
About the Journal
The Critical Care Science (Crit Care Sci), ISSN 2965-2774 (formerly Revista Brasileira de Terapia Intensiva), is a continuous publication of the Associação de Medicina Intensiva Brasileira (AMIB) and the Sociedade Portuguesa de Cuidados Intensivos (SPCI) and has the objective to disseminate high-quality clinical, epidemiological, translational, and health services research related to adult and pediatric critical care medicine.
-
ORIGINAL ARTICLE
Identification of distinct phenotypes and improving prognosis using metabolic biomarkers in COVID-19 patients
- Andressa Santana,
- Gabriele da Silveira Prestes
 ,
, - Marinara Dagostin da Silva,
- Carolina Saibro Girardi ,
- Lucas dos Santos Silva , [ … ],
- Cristiane Ritter
Abstract
ORIGINAL ARTICLEIdentification of distinct phenotypes and improving prognosis using metabolic biomarkers in COVID-19 patients
Critical Care Science. 2024;36:e20240028en
DOI 10.62675/2965-2774.20240028-en
- Andressa Santana,
- Gabriele da Silveira Prestes ,
- Marinara Dagostin da Silva,
- Carolina Saibro Girardi ,
- Lucas dos Santos Silva ,
- José Cláudio Fonseca Moreira ,
- Daniel Pens Gelain ,
- Glauco Adrieno Westphal ,
- Emil Kupek ,
- Roger Walz ,
- Felipe Dal-Pizzol ,
- Cristiane Ritter
Views13See moreABSTRACT
Objective
To investigate the relationship between the levels of adipokines and other endocrine biomarkers and patient outcomes in hospitalized patients with COVID-19.
Methods
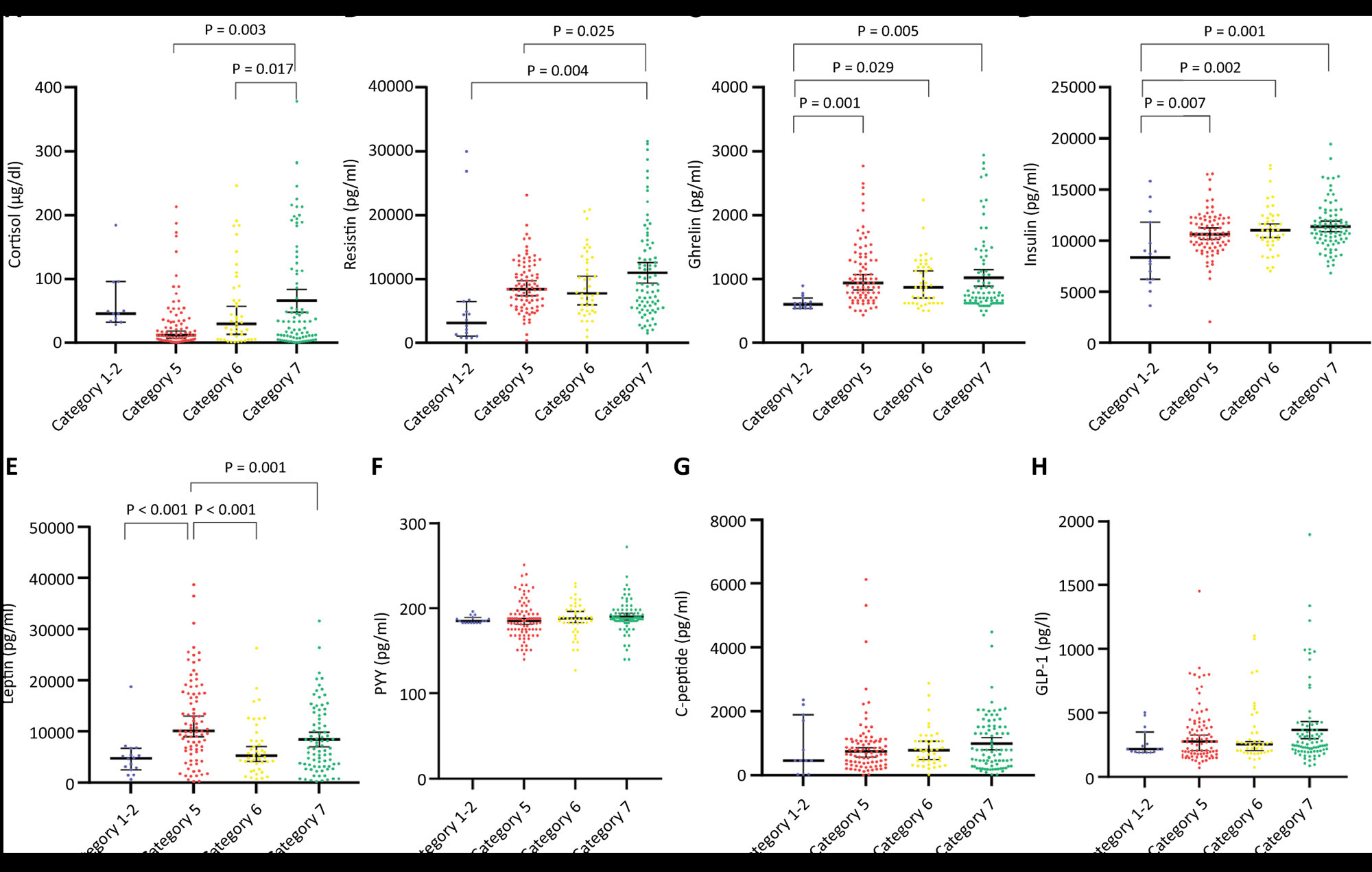
In a prospective study that included 213 subjects with COVID-19 admitted to the intensive care unit, we measured the levels of cortisol, C-peptide, glucagon-like peptide-1, insulin, peptide YY, ghrelin, leptin, and resistin.; their contributions to patient clustering, disease severity, and predicting in-hospital mortality were analyzed.
Results
Cortisol, resistin, leptin, insulin, and ghrelin levels significantly differed between severity groups, as defined by the World Health Organization severity scale. Additionally, lower ghrelin and higher cortisol levels were associated with mortality. Adding biomarkers to the clinical predictors of mortality significantly improved accuracy in determining prognosis. Phenotyping of subjects based on plasma biomarker levels yielded two different phenotypes that were associated with disease severity, but not mortality.
Conclusion
As a single biomarker, only cortisol was independently associated with mortality; however, metabolic biomarkers could improve mortality prediction when added to clinical parameters. Metabolic biomarker phenotypes were differentially distributed according to COVID-19 severity but were not associated with mortality.
Views13

Abstract
ORIGINAL ARTICLEIdentification of distinct phenotypes and improving prognosis using metabolic biomarkers in COVID-19 patients
Critical Care Science. 2024;36:e20240028en
DOI 10.62675/2965-2774.20240028-en
- Andressa Santana,
- Gabriele da Silveira Prestes ,
- Marinara Dagostin da Silva,
- Carolina Saibro Girardi ,
- Lucas dos Santos Silva ,
- José Cláudio Fonseca Moreira ,
- Daniel Pens Gelain ,
- Glauco Adrieno Westphal ,
- Emil Kupek ,
- Roger Walz ,
- Felipe Dal-Pizzol ,
- Cristiane Ritter
Views13See moreABSTRACT
Objective
To investigate the relationship between the levels of adipokines and other endocrine biomarkers and patient outcomes in hospitalized patients with COVID-19.
Methods
In a prospective study that included 213 subjects with COVID-19 admitted to the intensive care unit, we measured the levels of cortisol, C-peptide, glucagon-like peptide-1, insulin, peptide YY, ghrelin, leptin, and resistin.; their contributions to patient clustering, disease severity, and predicting in-hospital mortality were analyzed.
Results
Cortisol, resistin, leptin, insulin, and ghrelin levels significantly differed between severity groups, as defined by the World Health Organization severity scale. Additionally, lower ghrelin and higher cortisol levels were associated with mortality. Adding biomarkers to the clinical predictors of mortality significantly improved accuracy in determining prognosis. Phenotyping of subjects based on plasma biomarker levels yielded two different phenotypes that were associated with disease severity, but not mortality.
Conclusion
As a single biomarker, only cortisol was independently associated with mortality; however, metabolic biomarkers could improve mortality prediction when added to clinical parameters. Metabolic biomarker phenotypes were differentially distributed according to COVID-19 severity but were not associated with mortality.
-
Correspondence
To: Biomarkers of neuropsychiatric dysfunction in intensive care unit survivors: a prospective cohort study
Critical Care Science. 2024;36:e20240260en
Abstract
CorrespondenceTo: Biomarkers of neuropsychiatric dysfunction in intensive care unit survivors: a prospective cohort study
Critical Care Science. 2024;36:e20240260en
DOI 10.62675/2965-2774.20240260-en
Views1To the EditorWe read with interest the article by Rocha et al. on a long-term, prospective cohort study of the neuropsychiatric outcomes of 65 intensive care unit (ICU) survivors assessed using the Mini Mental State Examination (MMSE), Hospital Anxiety and Depression Scale (HADS), Impact of Event Scale-6 (IES-6), and several wet inflammatory biomarkers.() Delirium and […]See moreViews1Abstract
CorrespondenceTo: Biomarkers of neuropsychiatric dysfunction in intensive care unit survivors: a prospective cohort study
Critical Care Science. 2024;36:e20240260en
DOI 10.62675/2965-2774.20240260-en
Views1To the EditorWe read with interest the article by Rocha et al. on a long-term, prospective cohort study of the neuropsychiatric outcomes of 65 intensive care unit (ICU) survivors assessed using the Mini Mental State Examination (MMSE), Hospital Anxiety and Depression Scale (HADS), Impact of Event Scale-6 (IES-6), and several wet inflammatory biomarkers.() Delirium and […]See more -
Correspondence
To: Neurocritical care management supported by multimodal brain monitoring after acute brain injury
Critical Care Science. 2024;36:e20240276en
Abstract
CorrespondenceTo: Neurocritical care management supported by multimodal brain monitoring after acute brain injury
Critical Care Science. 2024;36:e20240276en
DOI 10.62675/2965-2774.20240276-en
Views2To the Editor We read with interest the article by Monteiro et al. on a retrospective single-center study of the outcomes and mortality of 389 patients with traumatic brain injury (TBI) or subarachnoid bleeding (SAB) depending on the level of neuro-monitoring (standard, advanced) in a neuro-critical care unit (NCCU, Group G1) and a general intensive […]See moreViews2Abstract
CorrespondenceTo: Neurocritical care management supported by multimodal brain monitoring after acute brain injury
Critical Care Science. 2024;36:e20240276en
DOI 10.62675/2965-2774.20240276-en
Views2To the Editor We read with interest the article by Monteiro et al. on a retrospective single-center study of the outcomes and mortality of 389 patients with traumatic brain injury (TBI) or subarachnoid bleeding (SAB) depending on the level of neuro-monitoring (standard, advanced) in a neuro-critical care unit (NCCU, Group G1) and a general intensive […]See more -
Viewpoint
A decade of the ORCHESTRA study: organizational characteristics, patient outcomes, performance and efficiency in critical care
- Marcio Soares ,
- Jorge Ibrain Figueira Salluh ,
- Fernando Godinho Zampieri ,
- Fernando Augusto Bozza ,
- Pedro Martins Pereira Kurtz
Abstract
ViewpointA decade of the ORCHESTRA study: organizational characteristics, patient outcomes, performance and efficiency in critical care
Critical Care Science. 2024;36:e20240118en
DOI 10.62675/2965-2774.20240118-en
- Marcio Soares ,
- Jorge Ibrain Figueira Salluh ,
- Fernando Godinho Zampieri ,
- Fernando Augusto Bozza ,
- Pedro Martins Pereira Kurtz
Views33INTRODUCTIONThe organization and structure of intensive care units (ICUs) affect the quality and efficiency of critical care.(,) Because acute care delivery varies significantly across countries, patient populations and local care practices, the associations of ICU structure, process and outcomes are also expected to differ depending on the context. Currently, most of the available information on […]See moreViews33Abstract
ViewpointA decade of the ORCHESTRA study: organizational characteristics, patient outcomes, performance and efficiency in critical care
Critical Care Science. 2024;36:e20240118en
DOI 10.62675/2965-2774.20240118-en
- Marcio Soares ,
- Jorge Ibrain Figueira Salluh ,
- Fernando Godinho Zampieri ,
- Fernando Augusto Bozza ,
- Pedro Martins Pereira Kurtz
Views33INTRODUCTIONThe organization and structure of intensive care units (ICUs) affect the quality and efficiency of critical care.(,) Because acute care delivery varies significantly across countries, patient populations and local care practices, the associations of ICU structure, process and outcomes are also expected to differ depending on the context. Currently, most of the available information on […]See more
- Marcio Soares
-
Editorial
Science over language: a plea to consider language bias in scientific publishing
- Sebastián González-Dambrauskas ,
- Jorge Ibrain Figueira Salluh ,
- Flávia Ribeiro Machado ,
- Alexandre Tellechea Rotta
Abstract
EditorialScience over language: a plea to consider language bias in scientific publishing
Critical Care Science. 2024;36:e20240084en
DOI 10.62675/2965-2774.20240084-en
- Sebastián González-Dambrauskas ,
- Jorge Ibrain Figueira Salluh ,
- Flávia Ribeiro Machado ,
- Alexandre Tellechea Rotta
Views3Language hegemony in scienceConsider the following fictional predicament: you have just finished writing the main manuscript for a study that, from conception to final analysis, took you more than four years to complete. You must now try to get it published in a respected scientific journal to disseminate your findings to a broad audience and […]See moreViews3Abstract
EditorialScience over language: a plea to consider language bias in scientific publishing
Critical Care Science. 2024;36:e20240084en
DOI 10.62675/2965-2774.20240084-en
- Sebastián González-Dambrauskas ,
- Jorge Ibrain Figueira Salluh ,
- Flávia Ribeiro Machado ,
- Alexandre Tellechea Rotta
Views3Language hegemony in scienceConsider the following fictional predicament: you have just finished writing the main manuscript for a study that, from conception to final analysis, took you more than four years to complete. You must now try to get it published in a respected scientific journal to disseminate your findings to a broad audience and […]See more - Sebastián González-Dambrauskas
-
Viewpoint
New Phoenix criteria for pediatric sepsis and septic shock: the strengths and the future of a comprehensive perspective
Critical Care Science. 2024;36:e20240058en
Abstract
ViewpointNew Phoenix criteria for pediatric sepsis and septic shock: the strengths and the future of a comprehensive perspective
Critical Care Science. 2024;36:e20240058en
DOI 10.62675/2965-2774.20240058-en
Views22In Greek mythology, the phoenix bird symbolizes life that overcomes death and the strength that accompanies transformation. Therefore, Phoenix is an appropriate name for the new Pediatric Sepsis Score owing to both the mythological reference and the location where it was first presented (Society of Critical Care Medicine – SCCM – Conference in Phoenix, Arizona).()The […]See moreViews22Abstract
ViewpointNew Phoenix criteria for pediatric sepsis and septic shock: the strengths and the future of a comprehensive perspective
Critical Care Science. 2024;36:e20240058en
DOI 10.62675/2965-2774.20240058-en
Views22In Greek mythology, the phoenix bird symbolizes life that overcomes death and the strength that accompanies transformation. Therefore, Phoenix is an appropriate name for the new Pediatric Sepsis Score owing to both the mythological reference and the location where it was first presented (Society of Critical Care Medicine – SCCM – Conference in Phoenix, Arizona).()The […]See more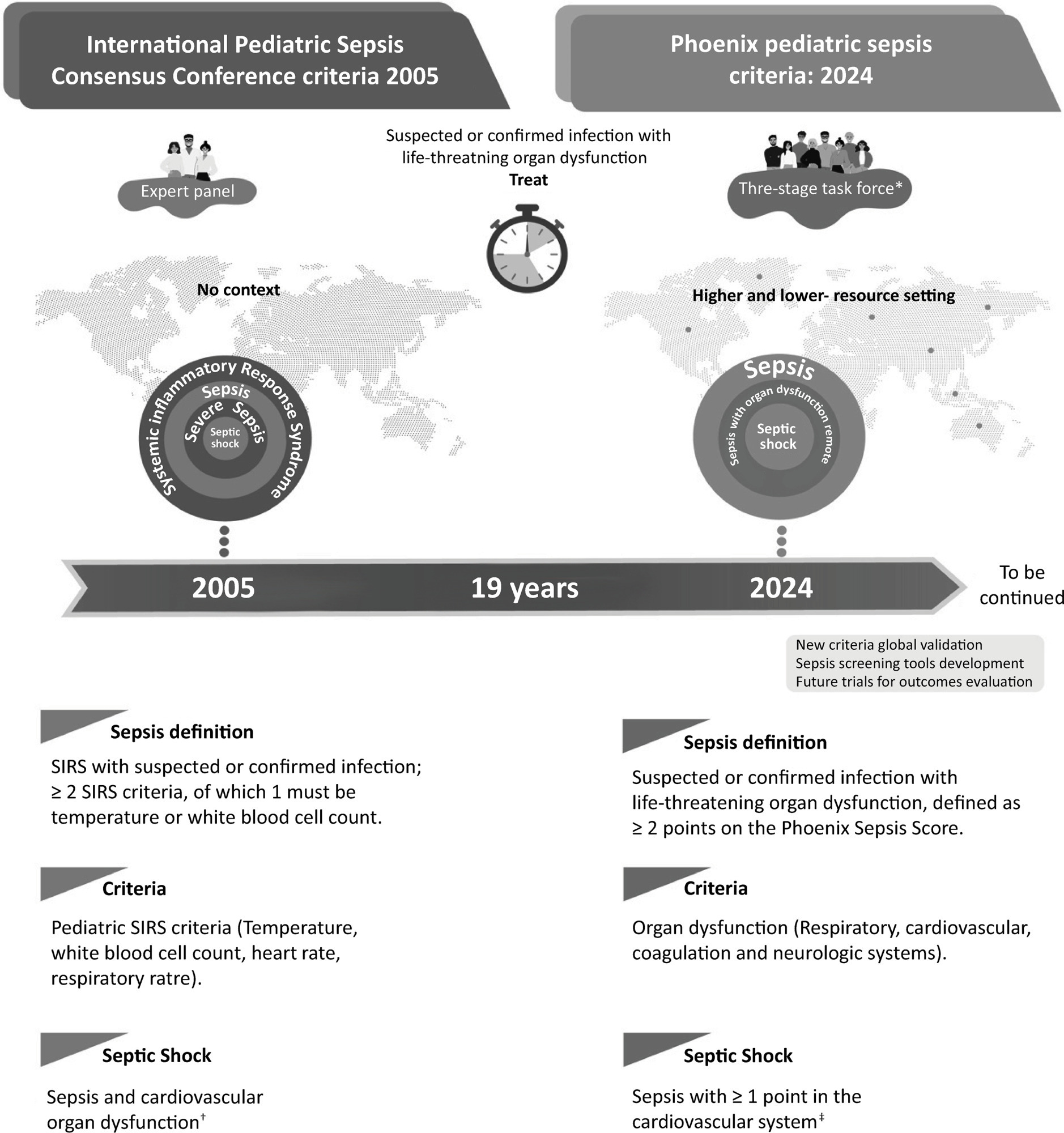
-
ORIGINAL ARTICLE
Analysis of factors associated with admission to the intensive care unit of children and adolescents with COVID-19: application of a multilevel model
- Lecidamia Cristina Leite Damascena ,
- Aline Roseane Queiroz de Paiva Faria ,
- Nyellisonn Nando Nóbrega de Lucena ,
- Ana Hermínia Andrade e Silva ,
- Talita Tavares Alves de Almeida , [ … ],
- Ana Maria Gondim Valença
Abstract
ORIGINAL ARTICLEAnalysis of factors associated with admission to the intensive care unit of children and adolescents with COVID-19: application of a multilevel model
Critical Care Science. 2024;36:e20240068en
DOI 10.62675/2965-2774.20240068-en
- Lecidamia Cristina Leite Damascena ,
- Aline Roseane Queiroz de Paiva Faria ,
- Nyellisonn Nando Nóbrega de Lucena ,
- Ana Hermínia Andrade e Silva ,
- Talita Tavares Alves de Almeida ,
- Diana de Fátima Alves Pinto ,
- Hemílio Fernandes Campos Coêlho ,
- Ana Maria Gondim Valença
Views6ABSTRACT
Objective
To identify factors associated with hospitalization in the intensive care unit in children and adolescents with COVID-19.
Methods
This was a retrospective cohort study using secondary data of hospitalized children and adolescents (zero to 18 years old) with COVID-19 reported in Paraíba from April 2020 to July 2021, totaling 486 records. Descriptive analysis, logistic regression and multilevel regression were performed, utilizing a significance level of 5%.
Results
According to logistic regression without hierarchical levels, there was an increased chance of admission to the intensive care unit for male patients (OR = 1.98; 95%CI 1.18 – 3.32), patients with respiratory distress (OR = 2.43; 95%CI 1.29 – 4.56), patients with dyspnea (OR = 3.57; 95%CI 1.77 – 7.18) and patients living in large cities (OR = 2.70; 95%CI 1.07 – 6.77). The likelihood of requiring intensive care was observed to decrease with increasing age (OR = 0.94; 95%CI = 0.90 – 0.97), the presence of cough (OR = 0.32; 95%CI 0.18 – 0.59) or fever (OR = 0.42; 95%CI 0.23 – 0.74) and increasing Gini index (OR = 0.003; 95%CI 0.000 – 0.243). According to the multilevel analysis, the odds of admission to the intensive care unit increased in male patients (OR = 1.70; 95%CI = 1.68-1.71) and with increasing population size of the municipality per 100,000 inhabitants (OR = 1.01; 95%CI 1.01-1.03); additionally, the odds of admission to the intensive care unit decreased for mixed-race versus non-brown-skinned patients (OR = 0.981; 95%CI 0.97 – 0.99) and increasing Gini index (OR = 0.02; 95%CI 0.02 – 0.02).
Conclusion
The effects of patient characteristics and social context on the need for intensive care in children and adolescents with SARS-CoV-2 infection were better estimated with the inclusion of a multilevel regression model.
Keywords:AdolescentChildCoronavirus infectionsCOVID-19Logistic modelsMultilevel analysisPediatric intensive care unitsSocial vulnerabilitySee moreViews6Abstract
ORIGINAL ARTICLEAnalysis of factors associated with admission to the intensive care unit of children and adolescents with COVID-19: application of a multilevel model
Critical Care Science. 2024;36:e20240068en
DOI 10.62675/2965-2774.20240068-en
- Lecidamia Cristina Leite Damascena ,
- Aline Roseane Queiroz de Paiva Faria ,
- Nyellisonn Nando Nóbrega de Lucena ,
- Ana Hermínia Andrade e Silva ,
- Talita Tavares Alves de Almeida ,
- Diana de Fátima Alves Pinto ,
- Hemílio Fernandes Campos Coêlho ,
- Ana Maria Gondim Valença
Views6ABSTRACT
Objective
To identify factors associated with hospitalization in the intensive care unit in children and adolescents with COVID-19.
Methods
This was a retrospective cohort study using secondary data of hospitalized children and adolescents (zero to 18 years old) with COVID-19 reported in Paraíba from April 2020 to July 2021, totaling 486 records. Descriptive analysis, logistic regression and multilevel regression were performed, utilizing a significance level of 5%.
Results
According to logistic regression without hierarchical levels, there was an increased chance of admission to the intensive care unit for male patients (OR = 1.98; 95%CI 1.18 – 3.32), patients with respiratory distress (OR = 2.43; 95%CI 1.29 – 4.56), patients with dyspnea (OR = 3.57; 95%CI 1.77 – 7.18) and patients living in large cities (OR = 2.70; 95%CI 1.07 – 6.77). The likelihood of requiring intensive care was observed to decrease with increasing age (OR = 0.94; 95%CI = 0.90 – 0.97), the presence of cough (OR = 0.32; 95%CI 0.18 – 0.59) or fever (OR = 0.42; 95%CI 0.23 – 0.74) and increasing Gini index (OR = 0.003; 95%CI 0.000 – 0.243). According to the multilevel analysis, the odds of admission to the intensive care unit increased in male patients (OR = 1.70; 95%CI = 1.68-1.71) and with increasing population size of the municipality per 100,000 inhabitants (OR = 1.01; 95%CI 1.01-1.03); additionally, the odds of admission to the intensive care unit decreased for mixed-race versus non-brown-skinned patients (OR = 0.981; 95%CI 0.97 – 0.99) and increasing Gini index (OR = 0.02; 95%CI 0.02 – 0.02).
Conclusion
The effects of patient characteristics and social context on the need for intensive care in children and adolescents with SARS-CoV-2 infection were better estimated with the inclusion of a multilevel regression model.
Keywords:AdolescentChildCoronavirus infectionsCOVID-19Logistic modelsMultilevel analysisPediatric intensive care unitsSocial vulnerabilitySee more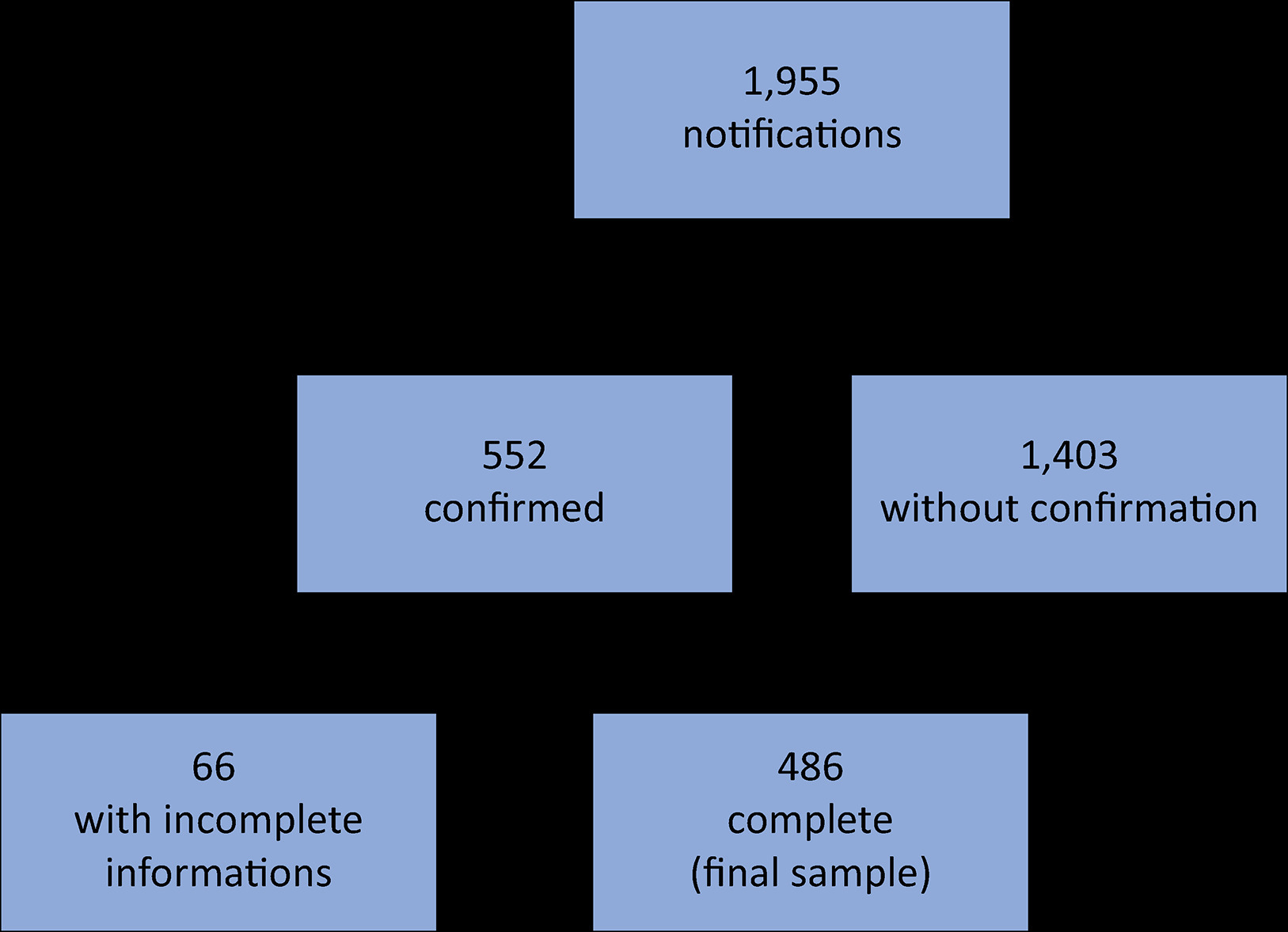
- Lecidamia Cristina Leite Damascena
-
Research Letter
Clinical outcomes of intensive care unit-acquired weakness in critically ill COVID-19 patients. A prospective cohort study
- Alessandra Preisig Werlang ,
- Viviane Martins Correa Boniatti ,
- Carolina Tarantino Neuenfeldt,
- Luciana Carcuchinski da Silva,
- Gabriela Machado Costa , [ … ],
- Wagner Luis Nedel
Abstract
Research LetterClinical outcomes of intensive care unit-acquired weakness in critically ill COVID-19 patients. A prospective cohort study
Critical Care Science. 2024;36:e20240003en
DOI 10.62675/2965-2774.20240003-en
- Alessandra Preisig Werlang ,
- Viviane Martins Correa Boniatti ,
- Carolina Tarantino Neuenfeldt,
- Luciana Carcuchinski da Silva,
- Gabriela Machado Costa ,
- Michelle Carneiro Teixeira ,
- Wagner Luis Nedel
Views2To the EditorIntensive care unit-acquired weakness (ICUAW) is one of the most common neurological complications in ICU patients,(,) and the prevalence of ICUAW after developing coronavirus disease 2019 (COVID-19)-related acute respiratory distress syndrome (ARDS) was 70 – 100%.() The risk factors for ICUAW, such as the frequent use of neuromuscular blockers (NMBs) and the regular […]See moreViews2Abstract
Research LetterClinical outcomes of intensive care unit-acquired weakness in critically ill COVID-19 patients. A prospective cohort study
Critical Care Science. 2024;36:e20240003en
DOI 10.62675/2965-2774.20240003-en
- Alessandra Preisig Werlang ,
- Viviane Martins Correa Boniatti ,
- Carolina Tarantino Neuenfeldt,
- Luciana Carcuchinski da Silva,
- Gabriela Machado Costa ,
- Michelle Carneiro Teixeira ,
- Wagner Luis Nedel
Views2To the EditorIntensive care unit-acquired weakness (ICUAW) is one of the most common neurological complications in ICU patients,(,) and the prevalence of ICUAW after developing coronavirus disease 2019 (COVID-19)-related acute respiratory distress syndrome (ARDS) was 70 – 100%.() The risk factors for ICUAW, such as the frequent use of neuromuscular blockers (NMBs) and the regular […]See more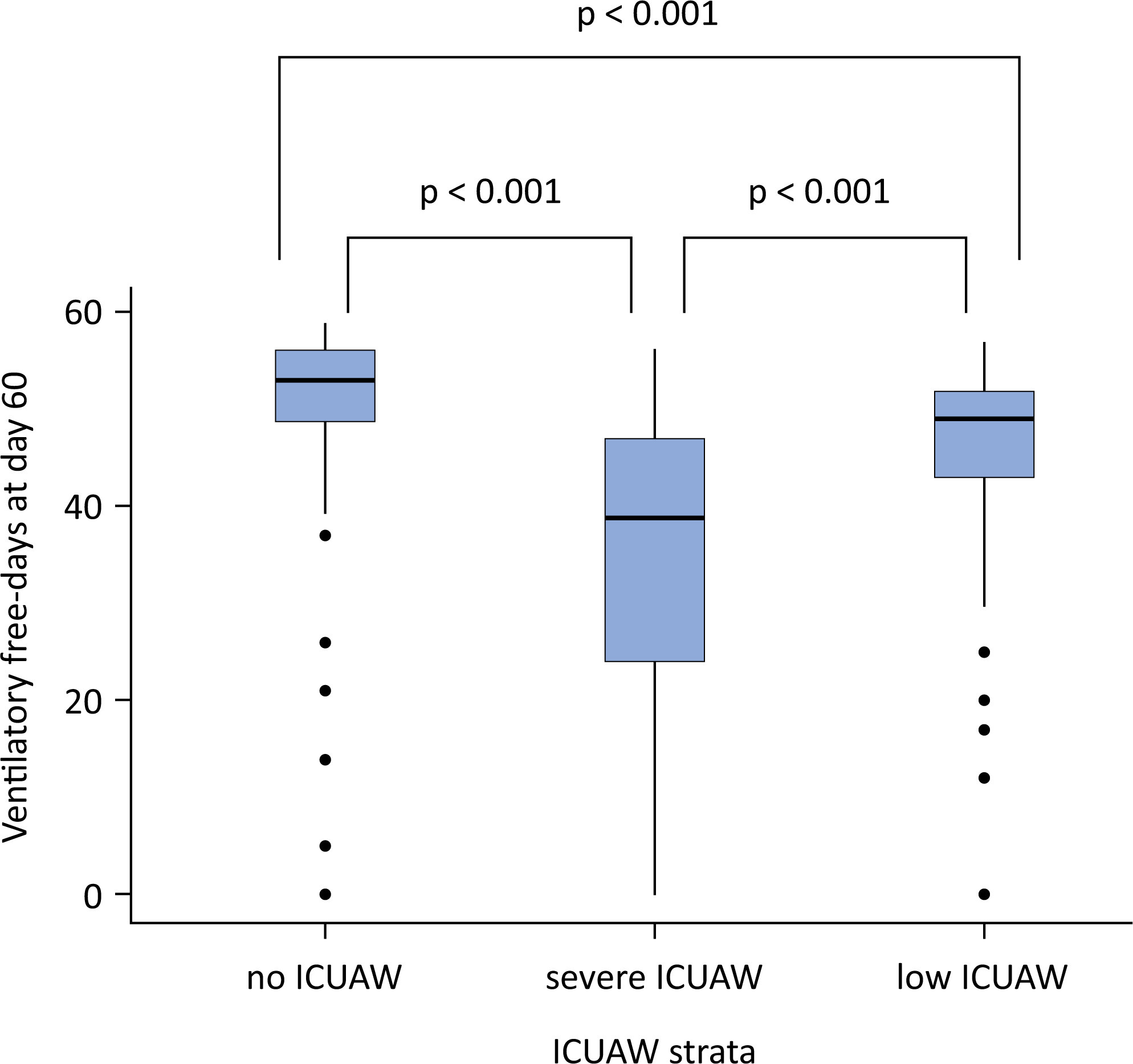
- Alessandra Preisig Werlang
-
Viewpoint
Revolutionizing care: unleashing the power of comprehensive geriatric assessment in tailoring treatment for frail postintensive care patients
Critical Care Science. 2024;36:e20240023en
Abstract
ViewpointRevolutionizing care: unleashing the power of comprehensive geriatric assessment in tailoring treatment for frail postintensive care patients
Critical Care Science. 2024;36:e20240023en
DOI 10.62675/2965-2774.20240023-en
Views2Frailty represents a condition of vulnerability leading to inadequate recovery following a stressful event, such as an acute illness or injury. This inadequate recovery results from cumulative, multisystem physiological depletion over a lifetime.() The frailty state implies that the available functional reserve is insufficient for complete recovery, often leading to a maladaptive response disproportionate to […]See moreViews2Abstract
ViewpointRevolutionizing care: unleashing the power of comprehensive geriatric assessment in tailoring treatment for frail postintensive care patients
Critical Care Science. 2024;36:e20240023en
DOI 10.62675/2965-2774.20240023-en
Views2Frailty represents a condition of vulnerability leading to inadequate recovery following a stressful event, such as an acute illness or injury. This inadequate recovery results from cumulative, multisystem physiological depletion over a lifetime.() The frailty state implies that the available functional reserve is insufficient for complete recovery, often leading to a maladaptive response disproportionate to […]See more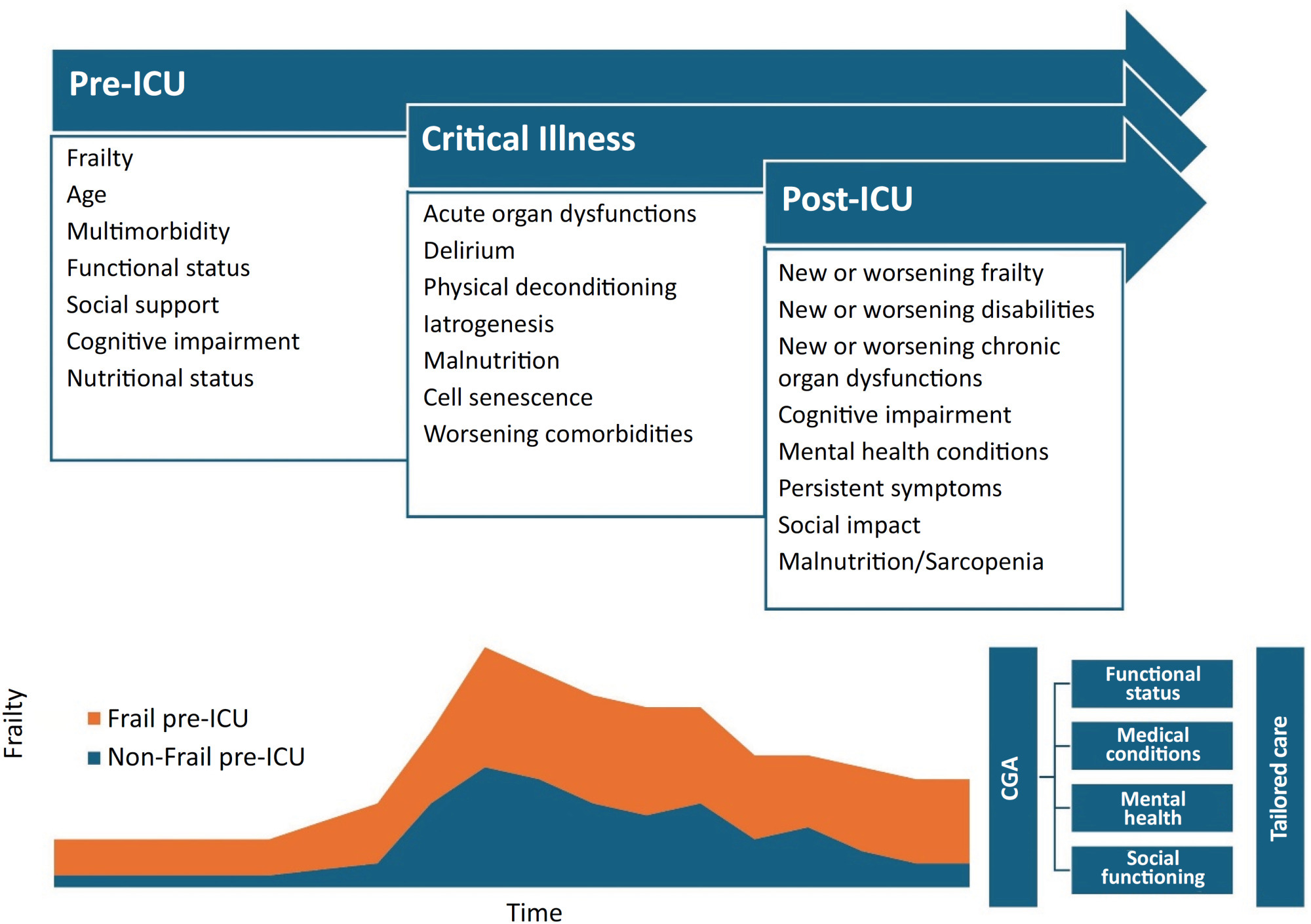
-
Clinical Report
Prospective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini , [ … ],
- Fernando Godinho Zampieri
Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Critical Care Science. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views3ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee moreViews3Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Critical Care Science. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views3ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee more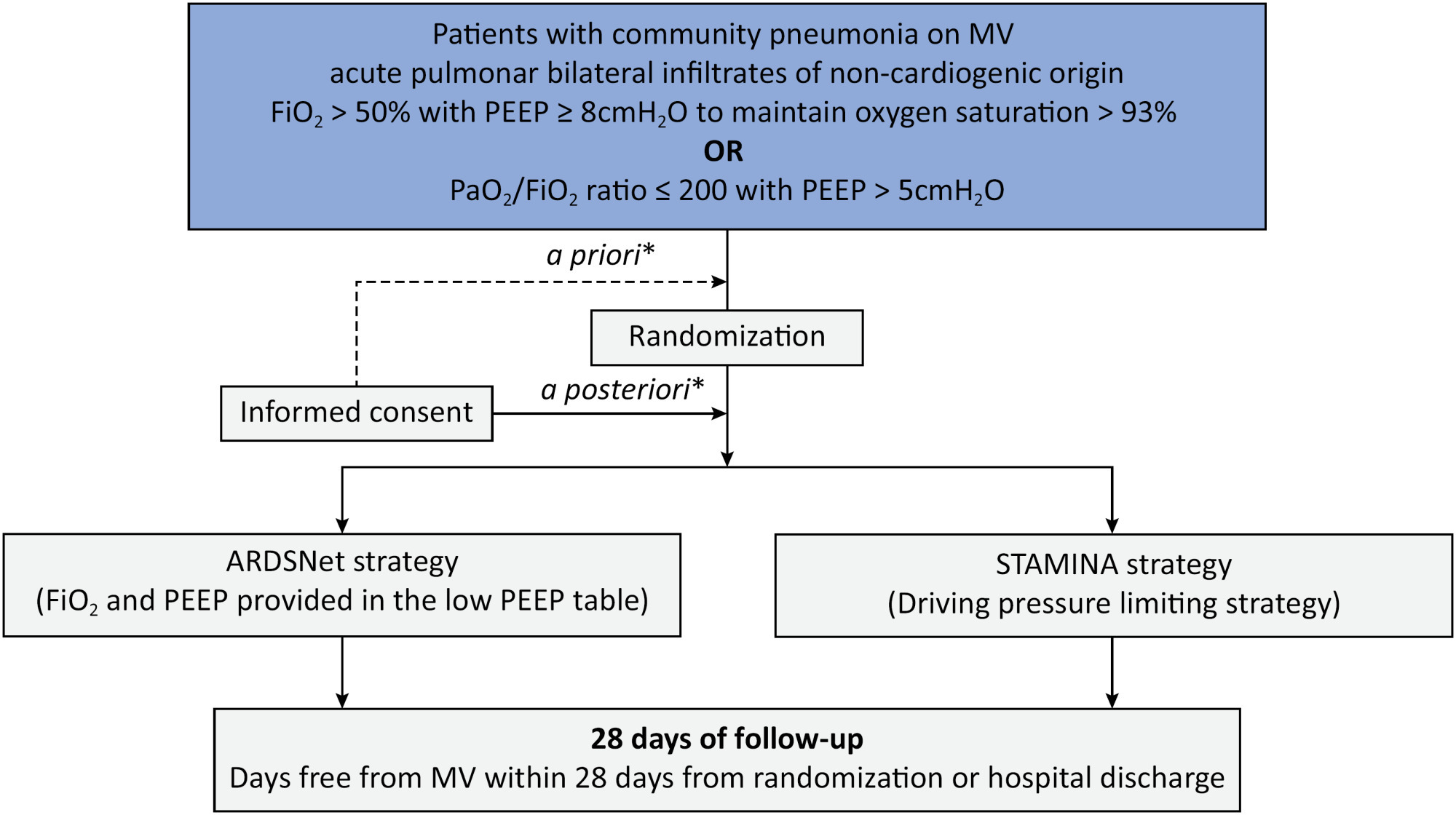
-
Viewpoint
New Phoenix criteria for pediatric sepsis and septic shock: the strengths and the future of a comprehensive perspective
Critical Care Science. 2024;36:e20240058en
Abstract
ViewpointNew Phoenix criteria for pediatric sepsis and septic shock: the strengths and the future of a comprehensive perspective
Critical Care Science. 2024;36:e20240058en
DOI 10.62675/2965-2774.20240058-en
Views22In Greek mythology, the phoenix bird symbolizes life that overcomes death and the strength that accompanies transformation. Therefore, Phoenix is an appropriate name for the new Pediatric Sepsis Score owing to both the mythological reference and the location where it was first presented (Society of Critical Care Medicine – SCCM – Conference in Phoenix, Arizona).()The […]See moreViews22Abstract
ViewpointNew Phoenix criteria for pediatric sepsis and septic shock: the strengths and the future of a comprehensive perspective
Critical Care Science. 2024;36:e20240058en
DOI 10.62675/2965-2774.20240058-en
Views22In Greek mythology, the phoenix bird symbolizes life that overcomes death and the strength that accompanies transformation. Therefore, Phoenix is an appropriate name for the new Pediatric Sepsis Score owing to both the mythological reference and the location where it was first presented (Society of Critical Care Medicine – SCCM – Conference in Phoenix, Arizona).()The […]See more -
ORIGINAL ARTICLE
Conscious prone positioning in nonintubated COVID-19 patients with acute respiratory distress syndrome: systematic review and meta-analysis
- Gustavo Adolfo Vásquez-Tirado ,
- Edinson Dante Meregildo-Rodríguez ,
- Martha Genara Asmat-Rubio ,
- María José Salazar-Castillo ,
- Claudia Vanessa Quispe-Castañeda , [ … ],
- María del Carmen Cuadra-Campos
Abstract
ORIGINAL ARTICLEConscious prone positioning in nonintubated COVID-19 patients with acute respiratory distress syndrome: systematic review and meta-analysis
Critical Care Science. 2024;36:e20240176en
DOI 10.62675/2965-2774.20240176-en
- Gustavo Adolfo Vásquez-Tirado ,
- Edinson Dante Meregildo-Rodríguez ,
- Martha Genara Asmat-Rubio ,
- María José Salazar-Castillo ,
- Claudia Vanessa Quispe-Castañeda ,
- María del Carmen Cuadra-Campos
Views2See moreABSTRACT
Objective:
To systematically review the effect of the prone position on endotracheal intubation and mortality in nonintubated COVID-19 patients with acute respiratory distress syndrome.
Methods:
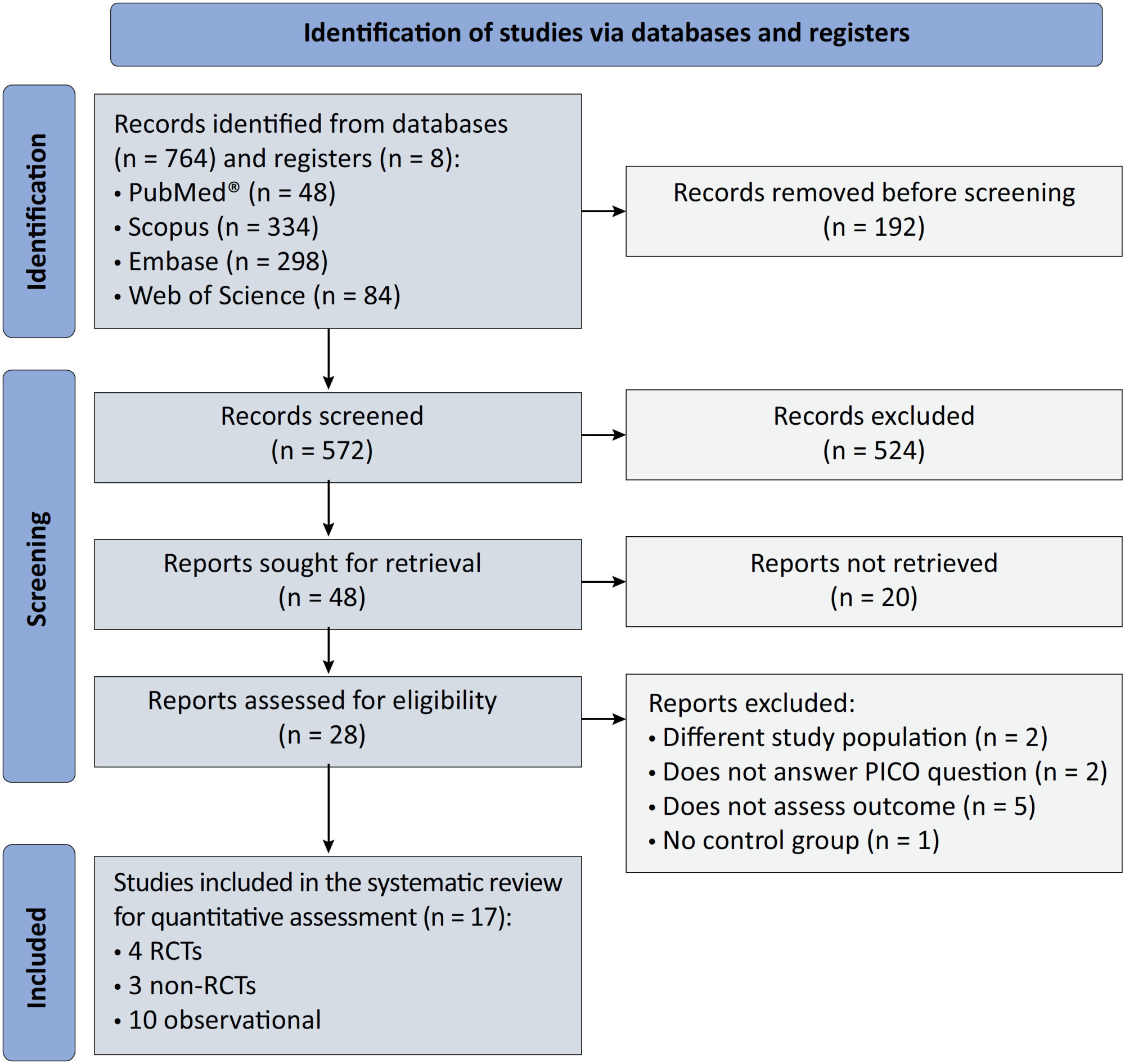
We registered the protocol (CRD42021286711) and searched for four databases and gray literature from inception to December 31, 2022. We included observational studies and clinical trials. There was no limit by date or the language of publication. We excluded case reports, case series, studies not available in full text, and those studies that included children < 18-years-old.
Results:
We included ten observational studies, eight clinical trials, 3,969 patients, 1,120 endotracheal intubation events, and 843 deaths. All of the studies had a low risk of bias (Newcastle-Ottawa Scale and Risk of Bias 2 tools). We found that the conscious prone position decreased the odds of endotracheal intubation by 44% (OR 0.56; 95%CI 0.40 – 0.78) and mortality by 43% (OR 0.57; 95%CI 0.39 – 0.84) in nonintubated COVID-19 patients with acute respiratory distress syndrome. This protective effect on endotracheal intubation and mortality was more robust in those who spent > 8 hours/day in the conscious prone position (OR 0.43; 95%CI 0.26 – 0.72 and OR 0.38; 95%CI 0.24 – 0.60, respectively). The certainty of the evidence according to the GRADE criteria was moderate.
Conclusion:
The conscious prone position decreased the odds of endotracheal intubation and mortality, especially when patients spent over 8 hours/day in the conscious prone position and treatment in the intensive care unit. However, our results should be cautiously interpreted due to limitations in evaluating randomized clinical trials, nonrandomized clinical trials and observational studies. However, despite systematic reviews with meta-analyses of randomized clinical trials, we must keep in mind that these studies remain heterogeneous from a clinical and methodological point of view.
Views2Abstract
ORIGINAL ARTICLEConscious prone positioning in nonintubated COVID-19 patients with acute respiratory distress syndrome: systematic review and meta-analysis
Critical Care Science. 2024;36:e20240176en
DOI 10.62675/2965-2774.20240176-en
- Gustavo Adolfo Vásquez-Tirado ,
- Edinson Dante Meregildo-Rodríguez ,
- Martha Genara Asmat-Rubio ,
- María José Salazar-Castillo ,
- Claudia Vanessa Quispe-Castañeda ,
- María del Carmen Cuadra-Campos
Views2See moreABSTRACT
Objective:
To systematically review the effect of the prone position on endotracheal intubation and mortality in nonintubated COVID-19 patients with acute respiratory distress syndrome.
Methods:
We registered the protocol (CRD42021286711) and searched for four databases and gray literature from inception to December 31, 2022. We included observational studies and clinical trials. There was no limit by date or the language of publication. We excluded case reports, case series, studies not available in full text, and those studies that included children < 18-years-old.
Results:
We included ten observational studies, eight clinical trials, 3,969 patients, 1,120 endotracheal intubation events, and 843 deaths. All of the studies had a low risk of bias (Newcastle-Ottawa Scale and Risk of Bias 2 tools). We found that the conscious prone position decreased the odds of endotracheal intubation by 44% (OR 0.56; 95%CI 0.40 – 0.78) and mortality by 43% (OR 0.57; 95%CI 0.39 – 0.84) in nonintubated COVID-19 patients with acute respiratory distress syndrome. This protective effect on endotracheal intubation and mortality was more robust in those who spent > 8 hours/day in the conscious prone position (OR 0.43; 95%CI 0.26 – 0.72 and OR 0.38; 95%CI 0.24 – 0.60, respectively). The certainty of the evidence according to the GRADE criteria was moderate.
Conclusion:
The conscious prone position decreased the odds of endotracheal intubation and mortality, especially when patients spent over 8 hours/day in the conscious prone position and treatment in the intensive care unit. However, our results should be cautiously interpreted due to limitations in evaluating randomized clinical trials, nonrandomized clinical trials and observational studies. However, despite systematic reviews with meta-analyses of randomized clinical trials, we must keep in mind that these studies remain heterogeneous from a clinical and methodological point of view.
- Gustavo Adolfo Vásquez-Tirado
-
Viewpoint
Why the Sequential Organ Failure Assessment score needs updating?
Critical Care Science. 2024;36:e20240296en
Abstract
ViewpointWhy the Sequential Organ Failure Assessment score needs updating?
Critical Care Science. 2024;36:e20240296en
DOI 10.62675/2965-2774.20240296-en
Views2The Sequential Organ Failure Assessment (SOFA) score was developed almost 30 years ago. It rapidly became one of the most widely used scoring systems in intensive care, both for clinical practice and research,(,) and remains one of the most cited scores in our speciality. Since its original description, there have been substantial changes in clinical […]See moreViews2Abstract
ViewpointWhy the Sequential Organ Failure Assessment score needs updating?
Critical Care Science. 2024;36:e20240296en
DOI 10.62675/2965-2774.20240296-en
Views2The Sequential Organ Failure Assessment (SOFA) score was developed almost 30 years ago. It rapidly became one of the most widely used scoring systems in intensive care, both for clinical practice and research,(,) and remains one of the most cited scores in our speciality. Since its original description, there have been substantial changes in clinical […]See more -
ORIGINAL ARTICLE
Driving pressure, as opposed to tidal volume based on predicted body weight, is associated with mortality: results from a prospective cohort of COVID-19 acute respiratory distress syndrome patients
- Erich Vidal Carvalho ,
- Maycon Moura Reboredo ,
- Edimar Pedrosa Gomes ,
- Pedro Nascimento Martins ,
- Gabriel Paz Souza Mota , [ … ],
- Bruno Valle Pinheiro
Abstract
ORIGINAL ARTICLEDriving pressure, as opposed to tidal volume based on predicted body weight, is associated with mortality: results from a prospective cohort of COVID-19 acute respiratory distress syndrome patients
Critical Care Science. 2024;36:e20240208en
DOI 10.62675/2965-2774.20240208-en
- Erich Vidal Carvalho ,
- Maycon Moura Reboredo ,
- Edimar Pedrosa Gomes ,
- Pedro Nascimento Martins ,
- Gabriel Paz Souza Mota ,
- Giovani Bernardo Costa ,
- Fernando Antonio Basile Colugnati ,
- Bruno Valle Pinheiro
Views2ABSTRACT
Objective:
To evaluate the association between driving pressure and tidal volume based on predicted body weight and mortality in a cohort of patients with acute respiratory distress syndrome caused by COVID-19.
Methods:
This was a prospective, observational study that included patients with acute respiratory distress syndrome due to COVID-19 admitted to two intensive care units. We performed multivariable analyses to determine whether driving pressure and tidal volume/kg predicted body weight on the first day of mechanical ventilation, as independent variables, are associated with hospital mortality.
Results:
We included 231 patients. The mean age was 64 (53 – 74) years, and the mean Simplified Acute and Physiology Score 3 score was 45 (39 – 54). The hospital mortality rate was 51.9%. Driving pressure was independently associated with hospital mortality (odds ratio 1.21, 95%CI 1.04 – 1.41 for each cm H2O increase in driving pressure, p = 0.01). Based on a double stratification analysis, we found that for the same level of tidal volume/kg predicted body weight, the risk of hospital death increased with increasing driving pressure. However, changes in tidal volume/kg predicted body weight were not associated with mortality when they did not lead to an increase in driving pressure.
Conclusion:
In patients with acute respiratory distress syndrome caused by COVID-19, exposure to higher driving pressure, as opposed to higher tidal volume/kg predicted body weight, is associated with greater mortality. These results suggest that driving pressure might be a primary target for lung-protective mechanical ventilation in these patients.
Keywords:Acute respiratory distress syndromeCoronavirus infectionsCOVID-19Intensive care unitsMortalityRespiration, artificialTidal volumeSee moreViews2Abstract
ORIGINAL ARTICLEDriving pressure, as opposed to tidal volume based on predicted body weight, is associated with mortality: results from a prospective cohort of COVID-19 acute respiratory distress syndrome patients
Critical Care Science. 2024;36:e20240208en
DOI 10.62675/2965-2774.20240208-en
- Erich Vidal Carvalho ,
- Maycon Moura Reboredo ,
- Edimar Pedrosa Gomes ,
- Pedro Nascimento Martins ,
- Gabriel Paz Souza Mota ,
- Giovani Bernardo Costa ,
- Fernando Antonio Basile Colugnati ,
- Bruno Valle Pinheiro
Views2ABSTRACT
Objective:
To evaluate the association between driving pressure and tidal volume based on predicted body weight and mortality in a cohort of patients with acute respiratory distress syndrome caused by COVID-19.
Methods:
This was a prospective, observational study that included patients with acute respiratory distress syndrome due to COVID-19 admitted to two intensive care units. We performed multivariable analyses to determine whether driving pressure and tidal volume/kg predicted body weight on the first day of mechanical ventilation, as independent variables, are associated with hospital mortality.
Results:
We included 231 patients. The mean age was 64 (53 – 74) years, and the mean Simplified Acute and Physiology Score 3 score was 45 (39 – 54). The hospital mortality rate was 51.9%. Driving pressure was independently associated with hospital mortality (odds ratio 1.21, 95%CI 1.04 – 1.41 for each cm H2O increase in driving pressure, p = 0.01). Based on a double stratification analysis, we found that for the same level of tidal volume/kg predicted body weight, the risk of hospital death increased with increasing driving pressure. However, changes in tidal volume/kg predicted body weight were not associated with mortality when they did not lead to an increase in driving pressure.
Conclusion:
In patients with acute respiratory distress syndrome caused by COVID-19, exposure to higher driving pressure, as opposed to higher tidal volume/kg predicted body weight, is associated with greater mortality. These results suggest that driving pressure might be a primary target for lung-protective mechanical ventilation in these patients.
Keywords:Acute respiratory distress syndromeCoronavirus infectionsCOVID-19Intensive care unitsMortalityRespiration, artificialTidal volumeSee more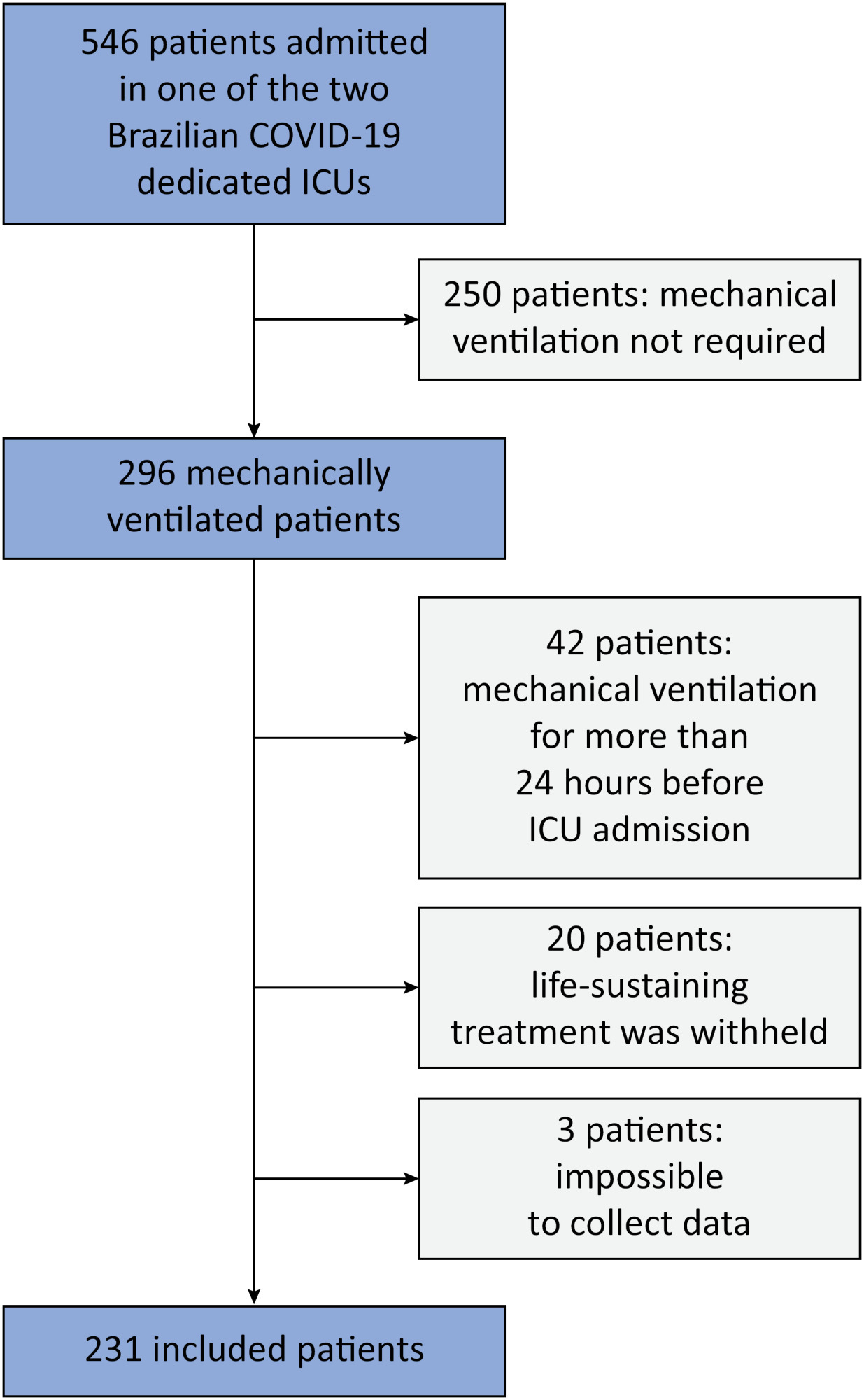
- Erich Vidal Carvalho
-
REVIEW
Unmasking the hidden aftermath: postintensive care unit sequelae, discharge preparedness, and long-term follow-up
Critical Care Science. 2024;36:e20240265en
Abstract
REVIEWUnmasking the hidden aftermath: postintensive care unit sequelae, discharge preparedness, and long-term follow-up
Critical Care Science. 2024;36:e20240265en
DOI 10.62675/2965-2774.20240265-en
Views5ABSTRACT
A significant portion of individuals who have experienced critical illness encounter new or exacerbated impairments in their physical, cognitive, or mental health, commonly referred to as postintensive care syndrome. Moreover, those who survive critical illness often face an increased risk of adverse consequences, including infections, major cardiovascular events, readmissions, and elevated mortality rates, during the months following hospitalization. These findings emphasize the critical necessity for effective prevention and management of long-term health deterioration in the critical care environment. Although conclusive evidence from well-designed randomized clinical trials is somewhat limited, potential interventions include strategies such as limiting sedation, early mobilization, maintaining family presence during the intensive care unit stay, implementing multicomponent transition programs (from intensive care unit to ward and from hospital to home), and offering specialized posthospital discharge follow-up. This review seeks to provide a concise summary of recent medical literature concerning long-term outcomes following critical illness and highlight potential approaches for preventing and addressing health decline in critical care survivors.
Keywords:Cardiovascular diseasesCognitionCritical illnessHospital-to-home transitionIntensive care unitsMental healthPatient dischargeSee moreViews5Abstract
REVIEWUnmasking the hidden aftermath: postintensive care unit sequelae, discharge preparedness, and long-term follow-up
Critical Care Science. 2024;36:e20240265en
DOI 10.62675/2965-2774.20240265-en
Views5ABSTRACT
A significant portion of individuals who have experienced critical illness encounter new or exacerbated impairments in their physical, cognitive, or mental health, commonly referred to as postintensive care syndrome. Moreover, those who survive critical illness often face an increased risk of adverse consequences, including infections, major cardiovascular events, readmissions, and elevated mortality rates, during the months following hospitalization. These findings emphasize the critical necessity for effective prevention and management of long-term health deterioration in the critical care environment. Although conclusive evidence from well-designed randomized clinical trials is somewhat limited, potential interventions include strategies such as limiting sedation, early mobilization, maintaining family presence during the intensive care unit stay, implementing multicomponent transition programs (from intensive care unit to ward and from hospital to home), and offering specialized posthospital discharge follow-up. This review seeks to provide a concise summary of recent medical literature concerning long-term outcomes following critical illness and highlight potential approaches for preventing and addressing health decline in critical care survivors.
Keywords:Cardiovascular diseasesCognitionCritical illnessHospital-to-home transitionIntensive care unitsMental healthPatient dischargeSee more
-
ORIGINAL ARTICLE
A comprehensive physical functional assessment of survivors of critical care unit stay due to COVID-19
- Marcia Souza Volpe ,
- Ana Carolina Cardoso dos Santos ,
- Sílvia Gaspar ,
- Jade Lara de Melo ,
- Gabriela Harada , [ … ],
- Carlos Roberto Ribeiro de Carvalho
Abstract
ORIGINAL ARTICLEA comprehensive physical functional assessment of survivors of critical care unit stay due to COVID-19
Critical Care Science. 2024;36:e20240284en
DOI 10.62675/2965-2774.20240284-en
- Marcia Souza Volpe ,
- Ana Carolina Cardoso dos Santos ,
- Sílvia Gaspar ,
- Jade Lara de Melo ,
- Gabriela Harada ,
- Patrícia Rocha Alves Ferreira ,
- Karina Ramiceli Soares da Silva ,
- Natália Tiemi Simokomaki Souza ,
- Carlos Toufen Junior ,
- Luciana Dias Chiavegato ,
- Marcelo Britto Passos Amato ,
- Maria Ignez Zanetti Feltrim ,
- Carlos Roberto Ribeiro de Carvalho
Views0See moreABSTRACT
Objective:
To examine the physical function and respiratory muscle strength of patients – who recovered from critical COVID-19 – after intensive care unit discharge to the ward on Days one (D1) and seven (D7), and to investigate variables associated with functional impairment.
Methods:
This was a prospective cohort study of adult patients with COVID-19 who needed invasive mechanical ventilation, non-invasive ventilation or high-flow nasal cannula and were discharged from the intensive care unit to the ward. Participants were submitted to Medical Research Council sum-score, handgrip strength, maximal inspiratory pressure, maximal expiratory pressure, and short physical performance battery tests. Participants were grouped into two groups according to their need for invasive ventilation: the Invasive Mechanical Ventilation Group (IMV Group) and the Non-Invasive Mechanical Ventilation Group (Non-IMV Group).
Results:
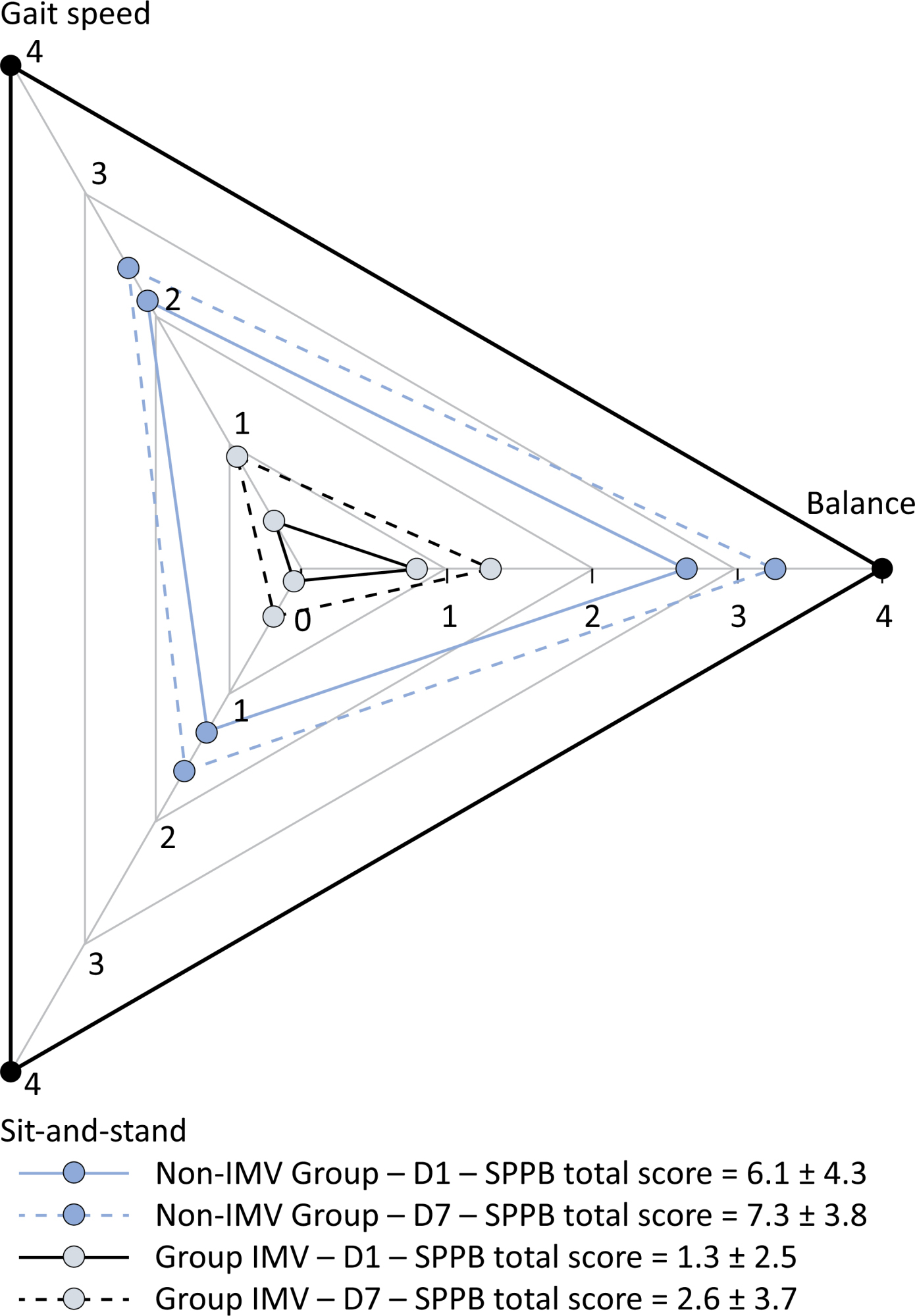
Patients in the IMV Group (n = 31) were younger and had higher Sequential Organ Failure Assessment scores than those in the Non-IMV Group (n = 33). The short physical performance battery scores (range 0 – 12) on D1 and D7 were 6.1 ± 4.3 and 7.3 ± 3.8, respectively for the Non-Invasive Mechanical Ventilation Group, and 1.3 ± 2.5 and 2.6 ± 3.7, respectively for the IMV Group. The prevalence of intensive care unit-acquired weakness on D7 was 13% for the Non-IMV Group and 72% for the IMV Group. The maximal inspiratory pressure, maximal expiratory pressure, and handgrip strength increased on D7 in both groups, but the maximal expiratory pressure and handgrip strength were still weak. Only maximal inspiratory pressure was recovered (i.e., > 80% of the predicted value) in the Non-IMV Group. Female sex, and the need and duration of invasive mechanical were independently and negatively associated with the short physical performance battery score and handgrip strength.
Conclusion:
Patients who recovered from critical COVID-19 and who received invasive mechanical ventilation presented greater disability than those who were not invasively ventilated. However, they both showed marginal functional improvement during early recovery, regardless of the need for invasive mechanical ventilation. This might highlight the severity of disability caused by SARS-CoV-2.
Views0Abstract
ORIGINAL ARTICLEA comprehensive physical functional assessment of survivors of critical care unit stay due to COVID-19
Critical Care Science. 2024;36:e20240284en
DOI 10.62675/2965-2774.20240284-en
- Marcia Souza Volpe ,
- Ana Carolina Cardoso dos Santos ,
- Sílvia Gaspar ,
- Jade Lara de Melo ,
- Gabriela Harada ,
- Patrícia Rocha Alves Ferreira ,
- Karina Ramiceli Soares da Silva ,
- Natália Tiemi Simokomaki Souza ,
- Carlos Toufen Junior ,
- Luciana Dias Chiavegato ,
- Marcelo Britto Passos Amato ,
- Maria Ignez Zanetti Feltrim ,
- Carlos Roberto Ribeiro de Carvalho
Views0See moreABSTRACT
Objective:
To examine the physical function and respiratory muscle strength of patients – who recovered from critical COVID-19 – after intensive care unit discharge to the ward on Days one (D1) and seven (D7), and to investigate variables associated with functional impairment.
Methods:
This was a prospective cohort study of adult patients with COVID-19 who needed invasive mechanical ventilation, non-invasive ventilation or high-flow nasal cannula and were discharged from the intensive care unit to the ward. Participants were submitted to Medical Research Council sum-score, handgrip strength, maximal inspiratory pressure, maximal expiratory pressure, and short physical performance battery tests. Participants were grouped into two groups according to their need for invasive ventilation: the Invasive Mechanical Ventilation Group (IMV Group) and the Non-Invasive Mechanical Ventilation Group (Non-IMV Group).
Results:
Patients in the IMV Group (n = 31) were younger and had higher Sequential Organ Failure Assessment scores than those in the Non-IMV Group (n = 33). The short physical performance battery scores (range 0 – 12) on D1 and D7 were 6.1 ± 4.3 and 7.3 ± 3.8, respectively for the Non-Invasive Mechanical Ventilation Group, and 1.3 ± 2.5 and 2.6 ± 3.7, respectively for the IMV Group. The prevalence of intensive care unit-acquired weakness on D7 was 13% for the Non-IMV Group and 72% for the IMV Group. The maximal inspiratory pressure, maximal expiratory pressure, and handgrip strength increased on D7 in both groups, but the maximal expiratory pressure and handgrip strength were still weak. Only maximal inspiratory pressure was recovered (i.e., > 80% of the predicted value) in the Non-IMV Group. Female sex, and the need and duration of invasive mechanical were independently and negatively associated with the short physical performance battery score and handgrip strength.
Conclusion:
Patients who recovered from critical COVID-19 and who received invasive mechanical ventilation presented greater disability than those who were not invasively ventilated. However, they both showed marginal functional improvement during early recovery, regardless of the need for invasive mechanical ventilation. This might highlight the severity of disability caused by SARS-CoV-2.
- Marcia Souza Volpe
-
Original Articles – Clinical Research
Influence of early mobilization on respiratory and peripheral muscle strength in critically ill patients
Revista Brasileira de Terapia Intensiva. 2012;24(2):173-178
Abstract
Original Articles – Clinical ResearchInfluence of early mobilization on respiratory and peripheral muscle strength in critically ill patients
Revista Brasileira de Terapia Intensiva. 2012;24(2):173-178
DOI 10.1590/S0103-507X2012000200013
Views0See moreOBJECTIVE:To evaluate the effects of an early mobilization protocol on respiratory and peripheral muscles in critically ill patients. METHODS: A randomized controlled clinical trial was conducted with 59 male and female patients on mechanical ventilation. The patients were divided into a conventional physical therapy group (control group, n=14) that received the sector’s standard physical therapy program and an early mobilization group (n=14) that received a systematic early mobilization protocol. Peripheral muscle strength was assessed with the Medical Research Council score, and respiratory muscle strength (determined by the maximal inspiratory and expiratory pressures) was measured using a vacuum manometer with a unidirectional valve. Systematic early mobilization was performed on five levels. RESULTS: Significant increases were observed for values for maximal inspiratory pressure and the Medical Research Council score in the early mobilization group. However, no statistically significant improvement was observed for maximal expiratory pressure or MV duration (days), length of stay in the intensive care unit (days), and length of hospital stay (days). CONCLUSION: The early mobilization group showed gains in inspiratory and peripheral muscle strength.
Views0Abstract
Original Articles – Clinical ResearchInfluence of early mobilization on respiratory and peripheral muscle strength in critically ill patients
Revista Brasileira de Terapia Intensiva. 2012;24(2):173-178
DOI 10.1590/S0103-507X2012000200013
Views0See moreOBJECTIVE:To evaluate the effects of an early mobilization protocol on respiratory and peripheral muscles in critically ill patients. METHODS: A randomized controlled clinical trial was conducted with 59 male and female patients on mechanical ventilation. The patients were divided into a conventional physical therapy group (control group, n=14) that received the sector’s standard physical therapy program and an early mobilization group (n=14) that received a systematic early mobilization protocol. Peripheral muscle strength was assessed with the Medical Research Council score, and respiratory muscle strength (determined by the maximal inspiratory and expiratory pressures) was measured using a vacuum manometer with a unidirectional valve. Systematic early mobilization was performed on five levels. RESULTS: Significant increases were observed for values for maximal inspiratory pressure and the Medical Research Council score in the early mobilization group. However, no statistically significant improvement was observed for maximal expiratory pressure or MV duration (days), length of stay in the intensive care unit (days), and length of hospital stay (days). CONCLUSION: The early mobilization group showed gains in inspiratory and peripheral muscle strength.
-
ARTIGOS ORIGINAIS
The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Revista Brasileira de Terapia Intensiva. 2017;29(4):418-426
Abstract
ARTIGOS ORIGINAISThe Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Revista Brasileira de Terapia Intensiva. 2017;29(4):418-426
DOI 10.5935/0103-507X.20170062
Views0See moreABSTRACT
Objective:
To describe the Epimed Monitor Database®, a Brazilian intensive care unit quality improvement database.
Methods:
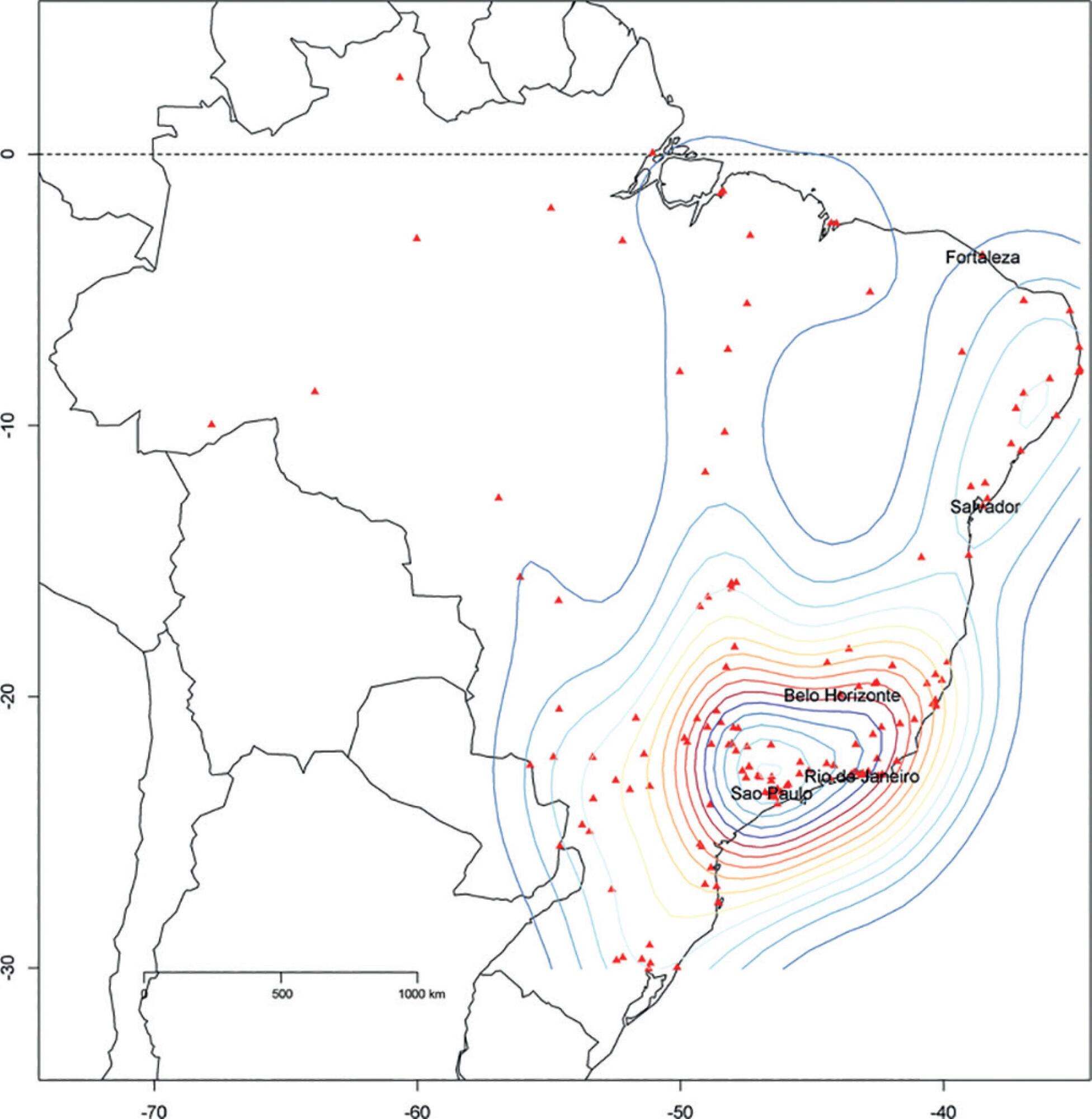
We described the Epimed Monitor® Database, including its structure and core data. We presented aggregated informative data from intensive care unit admissions from 2010 to 2016 using descriptive statistics. We also described the expansion and growth of the database along with the geographical distribution of participating units in Brazil.
Results:
The core data from the database includes demographic, administrative and physiological parameters, as well as specific report forms used to gather detailed data regarding the use of intensive care unit resources, infectious episodes, adverse events and checklists for adherence to best clinical practices. As of the end of 2016, 598 adult intensive care units in 318 hospitals totaling 8,160 intensive care unit beds were participating in the database. Most units were located at private hospitals in the southeastern region of the country. The number of yearly admissions rose during this period and included a predominance of medical admissions. The proportion of admissions due to cardiovascular disease declined, while admissions due to sepsis or infections became more common. Illness severity (Simplified Acute Physiology Score – SAPS 3 – 62 points), patient age (mean = 62 years) and hospital mortality (approximately 17%) remained reasonably stable during this time period.
Conclusion:
A large private database of critically ill patients is feasible and may provide relevant nationwide epidemiological data for quality improvement and benchmarking purposes among the participating intensive care units. This database is useful not only for administrative reasons but also for the improvement of daily care by facilitating the adoption of best practices and use for clinical research.
Views0Abstract
ARTIGOS ORIGINAISThe Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Revista Brasileira de Terapia Intensiva. 2017;29(4):418-426
DOI 10.5935/0103-507X.20170062
Views0See moreABSTRACT
Objective:
To describe the Epimed Monitor Database®, a Brazilian intensive care unit quality improvement database.
Methods:
We described the Epimed Monitor® Database, including its structure and core data. We presented aggregated informative data from intensive care unit admissions from 2010 to 2016 using descriptive statistics. We also described the expansion and growth of the database along with the geographical distribution of participating units in Brazil.
Results:
The core data from the database includes demographic, administrative and physiological parameters, as well as specific report forms used to gather detailed data regarding the use of intensive care unit resources, infectious episodes, adverse events and checklists for adherence to best clinical practices. As of the end of 2016, 598 adult intensive care units in 318 hospitals totaling 8,160 intensive care unit beds were participating in the database. Most units were located at private hospitals in the southeastern region of the country. The number of yearly admissions rose during this period and included a predominance of medical admissions. The proportion of admissions due to cardiovascular disease declined, while admissions due to sepsis or infections became more common. Illness severity (Simplified Acute Physiology Score – SAPS 3 – 62 points), patient age (mean = 62 years) and hospital mortality (approximately 17%) remained reasonably stable during this time period.
Conclusion:
A large private database of critically ill patients is feasible and may provide relevant nationwide epidemiological data for quality improvement and benchmarking purposes among the participating intensive care units. This database is useful not only for administrative reasons but also for the improvement of daily care by facilitating the adoption of best practices and use for clinical research.
-
Artigo Original Destaque
An epidemiological study of sepsis in Intensive Care Units: Sepsis Brazil study
Revista Brasileira de Terapia Intensiva. 2006;18(1):9-17
Abstract
Artigo Original DestaqueAn epidemiological study of sepsis in Intensive Care Units: Sepsis Brazil study
Revista Brasileira de Terapia Intensiva. 2006;18(1):9-17
DOI 10.1590/S0103-507X2006000100003
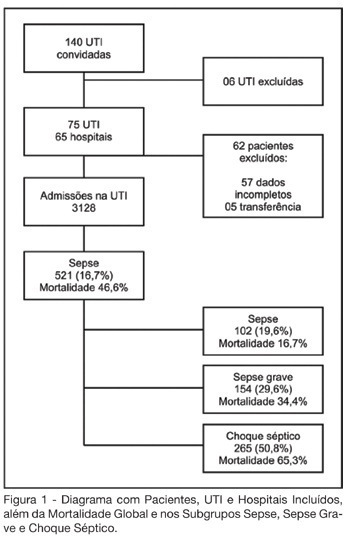
Views1See moreBACKGROUND AND OBJECTIVES: Sepsis represents the major cause of death in the ICUs all over the world. Many studies have shown an increasing incidence over time and only a slight reduce in mortality. Many new treatment strategies are arising and we should define the incidence and features of sepsis in Brazil. METHODS: Prospective cohort study in sixty-five hospitals all over Brazil. The patients who were admitted or who developed sepsis during the month of September, 2003 were enrolled. They were followed until the 28th day and/or until their discharge. The diagnoses were made in accordance to the criteria proposed by ACCP/SCCM. It were evaluated demographic features, APACHE II score, SOFA (Sepsis-related Organ Failure Assessment) score, mortality, sources of infections, microbiology, morbidities and length of stay (LOS). RESULTS: Seventy-five ICUs from all regions of Brazil took part in the study.3128 patients were identified and 521 (16.7%) filled the criteria of sepsis, severe sepsis or septic shock. Mean age was 61.7 (IQR 39-79), 293 (55.7%) were males, and the overall 28-day mortality rate was 46.6%. Average APACHE II score was 20 and SOFA score on the first day was 7 (IQR 4-10). SOFA score in the mortality group was higher on day 1 (8, IQR 5-11), and had increased on day 3 (9, IQR 6-12). The mortality rate for sepsis, severe sepsis and septic shock was 16.7%, 34.4% and 65.3%, respectively. The average LOS was 15 days (IQR 5-22). The two main sources of infection were the respiratory tract (69%) and the abdomen one (23.1%). Gram-negative bacilli were more prevalent (40.1%). Gram-positive cocci were identified in 32.8% and fungi infections in 5%. Mechanical ventilation was observed in 82.1% of the patients, Swan-Ganz catheter in 18.8%, vasopressors in 66.2% and hemotransfusion in 44.7%. CONCLUSIONS: It was observed a high mortality of sepsis in the ICUs in Brazil. The high frequency of septic shock demonstrated a group at high risk of death. In order to have a better use of the resources and reduce in mortality during the next 5 years, it is very important to identify our specific features related to this syndrome.
Views1Abstract
Artigo Original DestaqueAn epidemiological study of sepsis in Intensive Care Units: Sepsis Brazil study
Revista Brasileira de Terapia Intensiva. 2006;18(1):9-17
DOI 10.1590/S0103-507X2006000100003
Views1See moreBACKGROUND AND OBJECTIVES: Sepsis represents the major cause of death in the ICUs all over the world. Many studies have shown an increasing incidence over time and only a slight reduce in mortality. Many new treatment strategies are arising and we should define the incidence and features of sepsis in Brazil. METHODS: Prospective cohort study in sixty-five hospitals all over Brazil. The patients who were admitted or who developed sepsis during the month of September, 2003 were enrolled. They were followed until the 28th day and/or until their discharge. The diagnoses were made in accordance to the criteria proposed by ACCP/SCCM. It were evaluated demographic features, APACHE II score, SOFA (Sepsis-related Organ Failure Assessment) score, mortality, sources of infections, microbiology, morbidities and length of stay (LOS). RESULTS: Seventy-five ICUs from all regions of Brazil took part in the study.3128 patients were identified and 521 (16.7%) filled the criteria of sepsis, severe sepsis or septic shock. Mean age was 61.7 (IQR 39-79), 293 (55.7%) were males, and the overall 28-day mortality rate was 46.6%. Average APACHE II score was 20 and SOFA score on the first day was 7 (IQR 4-10). SOFA score in the mortality group was higher on day 1 (8, IQR 5-11), and had increased on day 3 (9, IQR 6-12). The mortality rate for sepsis, severe sepsis and septic shock was 16.7%, 34.4% and 65.3%, respectively. The average LOS was 15 days (IQR 5-22). The two main sources of infection were the respiratory tract (69%) and the abdomen one (23.1%). Gram-negative bacilli were more prevalent (40.1%). Gram-positive cocci were identified in 32.8% and fungi infections in 5%. Mechanical ventilation was observed in 82.1% of the patients, Swan-Ganz catheter in 18.8%, vasopressors in 66.2% and hemotransfusion in 44.7%. CONCLUSIONS: It was observed a high mortality of sepsis in the ICUs in Brazil. The high frequency of septic shock demonstrated a group at high risk of death. In order to have a better use of the resources and reduce in mortality during the next 5 years, it is very important to identify our specific features related to this syndrome.
-
SPECIAL ARTICLES
Physical therapy in critically ill adult patients: recommendations from the Brazilian Association of Intensive Care Medicine Department of Physical Therapy
Revista Brasileira de Terapia Intensiva. 2012;24(1):6-22
Abstract
SPECIAL ARTICLESPhysical therapy in critically ill adult patients: recommendations from the Brazilian Association of Intensive Care Medicine Department of Physical Therapy
Revista Brasileira de Terapia Intensiva. 2012;24(1):6-22
DOI 10.1590/S0103-507X2012000100003
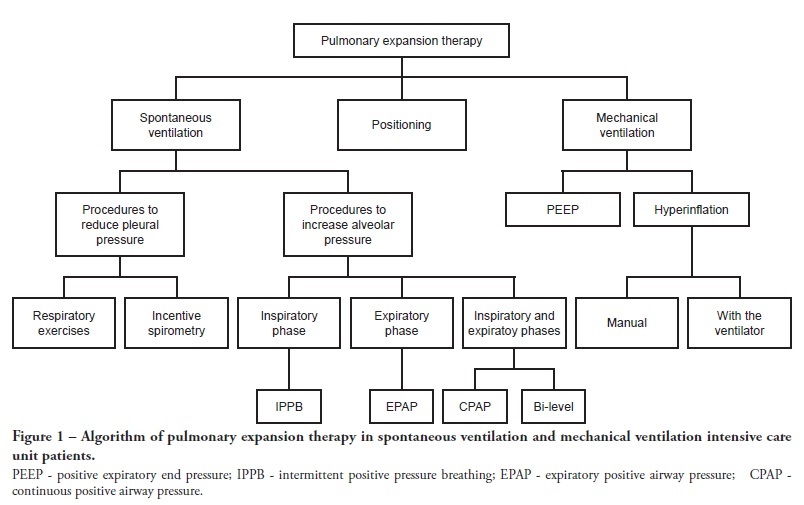
Views0See moreComplications from immobility in intensive care unit patients contribute to functional decline, increased healthcare costs, reduced quality of life and higher post-discharge mortality. Physical therapy focuses on promoting recovery and preserving function, and it may minimize the impact of these complications. A group of Brazilian Association of Intensive Care Medicine physical therapy experts developed this document that contains minimal physical therapy recommendations appropriate to the Brazilian real-world clinical situation. Prevention and treatment of atelectasis, procedures related to the removal of secretions and treatment of conditions related to physical deconditioning and functional decline are discussed. Equally important is the consideration that prescribing and executing activities, mobilizations and exercises are roles of the physical therapist, whose diagnosis should precede any intervention.
Views0Abstract
SPECIAL ARTICLESPhysical therapy in critically ill adult patients: recommendations from the Brazilian Association of Intensive Care Medicine Department of Physical Therapy
Revista Brasileira de Terapia Intensiva. 2012;24(1):6-22
DOI 10.1590/S0103-507X2012000100003
Views0See moreComplications from immobility in intensive care unit patients contribute to functional decline, increased healthcare costs, reduced quality of life and higher post-discharge mortality. Physical therapy focuses on promoting recovery and preserving function, and it may minimize the impact of these complications. A group of Brazilian Association of Intensive Care Medicine physical therapy experts developed this document that contains minimal physical therapy recommendations appropriate to the Brazilian real-world clinical situation. Prevention and treatment of atelectasis, procedures related to the removal of secretions and treatment of conditions related to physical deconditioning and functional decline are discussed. Equally important is the consideration that prescribing and executing activities, mobilizations and exercises are roles of the physical therapist, whose diagnosis should precede any intervention.
-
ORIGINAL ARTICLES
The reality of patients requiring prolonged mechanical ventilation: a multicenter study
Revista brasileira de terapia intensiva. 2015;27(1):26-35
Abstract
ORIGINAL ARTICLESThe reality of patients requiring prolonged mechanical ventilation: a multicenter study
Revista brasileira de terapia intensiva. 2015;27(1):26-35
DOI 10.5935/0103-507X.20150006
Views0See moreObjective:
The number of patients who require prolonged mechanical ventilation increased during the last decade, which generated a large population of chronically ill patients. This study established the incidence of prolonged mechanical ventilation in four intensive care units and reported different characteristics, hospital outcomes, and the impact of costs and services of prolonged mechanical ventilation patients (mechanical ventilation dependency ≥ 21 days) compared with non-prolonged mechanical ventilation patients (mechanical ventilation dependency < 21 days).
Methods:
This study was a multicenter cohort study of all patients who were admitted to four intensive care units. The main outcome measures were length of stay in the intensive care unit, hospital, complications during intensive care unit stay, and intensive care unit and hospital mortality.
Results:
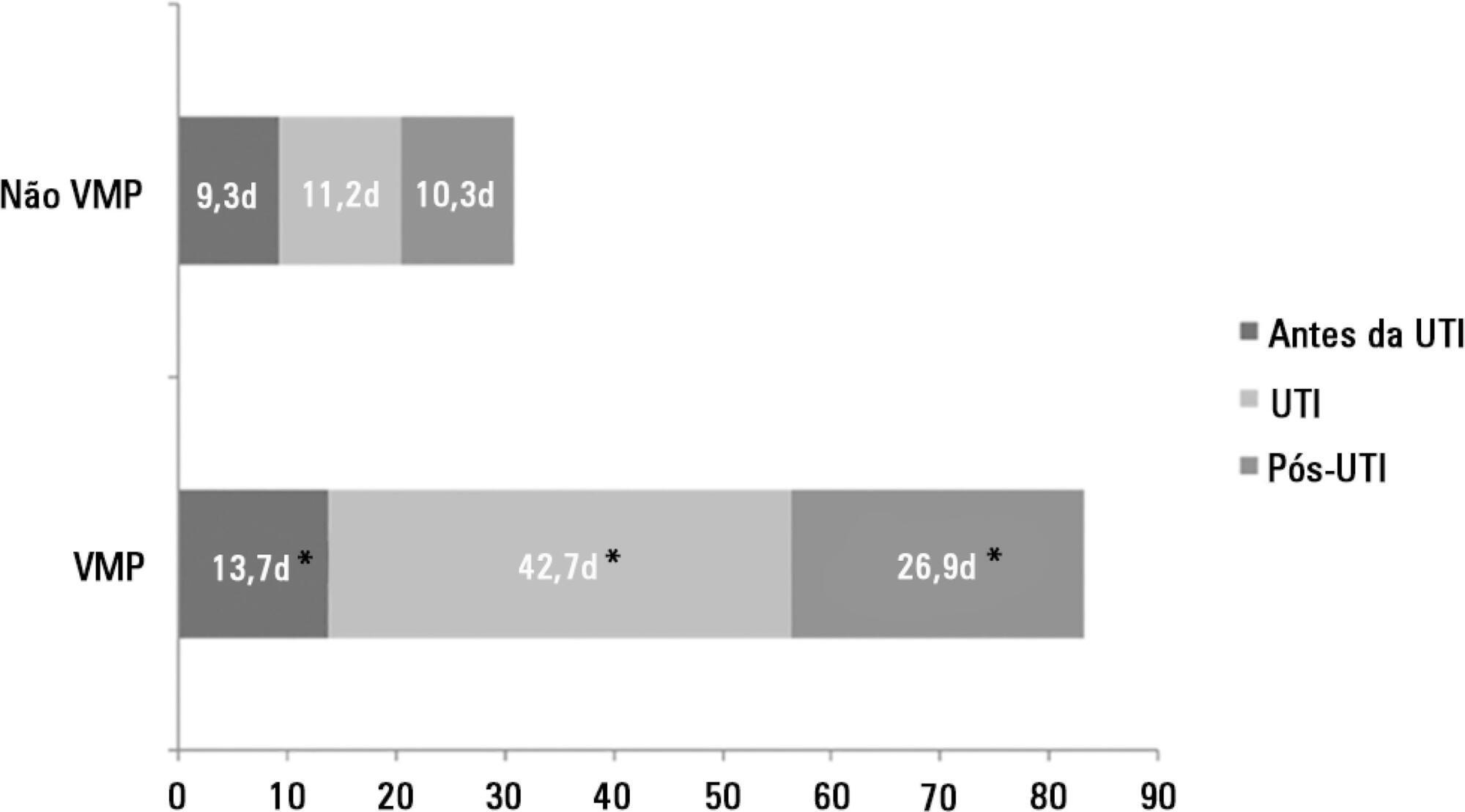
There were 5,287 admissions to the intensive care units during study period. Some of these patients (41.5%) needed ventilatory support (n = 2,197), and 218 of the patients met criteria for prolonged mechanical ventilation (9.9%). Some complications developed during intensive care unit stay, such as muscle weakness, pressure ulcers, bacterial nosocomial sepsis, candidemia, pulmonary embolism, and hyperactive delirium, were associated with a significantly higher risk of prolonged mechanical ventilation. Prolonged mechanical ventilation patients had a significant increase in intensive care unit mortality (absolute difference = 14.2%, p < 0.001) and hospital mortality (absolute difference = 19.1%, p < 0.001). The prolonged mechanical ventilation group spent more days in the hospital after intensive care unit discharge (26.9 ± 29.3 versus 10.3 ± 20.4 days, p < 0.001) with higher costs.
Conclusion:
The classification of chronically critically ill patients according to the definition of prolonged mechanical ventilation adopted by our study (mechanical ventilation dependency ≥ 21 days) identified patients with a high risk for complications during intensive care unit stay, longer intensive care unit and hospital stays, high death rates, and higher costs.
Views0Abstract
ORIGINAL ARTICLESThe reality of patients requiring prolonged mechanical ventilation: a multicenter study
Revista brasileira de terapia intensiva. 2015;27(1):26-35
DOI 10.5935/0103-507X.20150006
Views0See moreObjective:
The number of patients who require prolonged mechanical ventilation increased during the last decade, which generated a large population of chronically ill patients. This study established the incidence of prolonged mechanical ventilation in four intensive care units and reported different characteristics, hospital outcomes, and the impact of costs and services of prolonged mechanical ventilation patients (mechanical ventilation dependency ≥ 21 days) compared with non-prolonged mechanical ventilation patients (mechanical ventilation dependency < 21 days).
Methods:
This study was a multicenter cohort study of all patients who were admitted to four intensive care units. The main outcome measures were length of stay in the intensive care unit, hospital, complications during intensive care unit stay, and intensive care unit and hospital mortality.
Results:
There were 5,287 admissions to the intensive care units during study period. Some of these patients (41.5%) needed ventilatory support (n = 2,197), and 218 of the patients met criteria for prolonged mechanical ventilation (9.9%). Some complications developed during intensive care unit stay, such as muscle weakness, pressure ulcers, bacterial nosocomial sepsis, candidemia, pulmonary embolism, and hyperactive delirium, were associated with a significantly higher risk of prolonged mechanical ventilation. Prolonged mechanical ventilation patients had a significant increase in intensive care unit mortality (absolute difference = 14.2%, p < 0.001) and hospital mortality (absolute difference = 19.1%, p < 0.001). The prolonged mechanical ventilation group spent more days in the hospital after intensive care unit discharge (26.9 ± 29.3 versus 10.3 ± 20.4 days, p < 0.001) with higher costs.
Conclusion:
The classification of chronically critically ill patients according to the definition of prolonged mechanical ventilation adopted by our study (mechanical ventilation dependency ≥ 21 days) identified patients with a high risk for complications during intensive care unit stay, longer intensive care unit and hospital stays, high death rates, and higher costs.
-
SPECIAL ARTICLES
Brazilian recommendations of mechanical ventilation 2013. Part I
Revista brasileira de terapia intensiva. 2014;26(2):89-121
Abstract
SPECIAL ARTICLESBrazilian recommendations of mechanical ventilation 2013. Part I
Revista brasileira de terapia intensiva. 2014;26(2):89-121
DOI 10.5935/0103-507X.20140017
Views0See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
Views0Abstract
SPECIAL ARTICLESBrazilian recommendations of mechanical ventilation 2013. Part I
Revista brasileira de terapia intensiva. 2014;26(2):89-121
DOI 10.5935/0103-507X.20140017
Views0See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
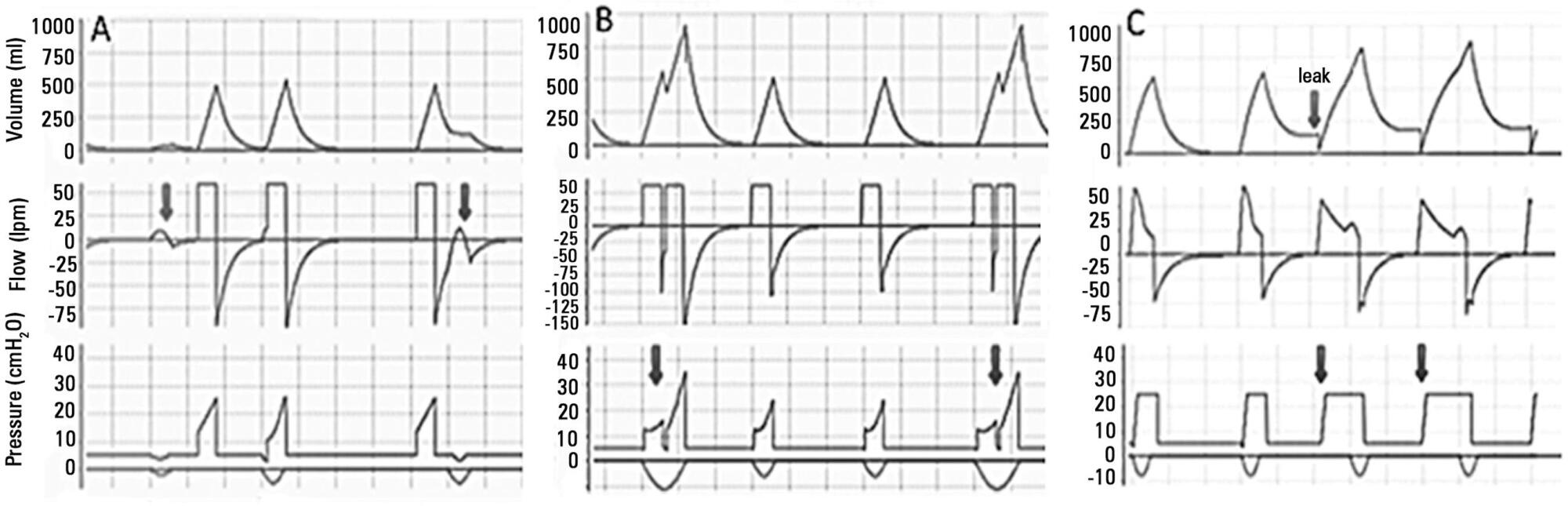
-
SPECIAL ARTICLES
Guidelines for the assessment and acceptance of potential brain-dead organ donors
Revista Brasileira de Terapia Intensiva. 2016;28(3):220-255
Abstract
SPECIAL ARTICLESGuidelines for the assessment and acceptance of potential brain-dead organ donors
Revista Brasileira de Terapia Intensiva. 2016;28(3):220-255
DOI 10.5935/0103-507X.20160049
Views1See moreABSTRACT
Organ transplantation is the only alternative for many patients with terminal diseases. The increasing disproportion between the high demand for organ transplants and the low rate of transplants actually performed is worrisome. Some of the causes of this disproportion are errors in the identification of potential organ donors and in the determination of contraindications by the attending staff. Therefore, the aim of the present document is to provide guidelines for intensive care multi-professional staffs for the recognition, assessment and acceptance of potential organ donors.
Views1Abstract
SPECIAL ARTICLESGuidelines for the assessment and acceptance of potential brain-dead organ donors
Revista Brasileira de Terapia Intensiva. 2016;28(3):220-255
DOI 10.5935/0103-507X.20160049
Views1See moreABSTRACT
Organ transplantation is the only alternative for many patients with terminal diseases. The increasing disproportion between the high demand for organ transplants and the low rate of transplants actually performed is worrisome. Some of the causes of this disproportion are errors in the identification of potential organ donors and in the determination of contraindications by the attending staff. Therefore, the aim of the present document is to provide guidelines for intensive care multi-professional staffs for the recognition, assessment and acceptance of potential organ donors.
-
ORIGINAL ARTICLES
Comparison of the RIFLE, AKIN and KDIGO criteria to predict mortality in critically ill patients
Revista brasileira de terapia intensiva. 2013;25(4):290-296
Abstract
ORIGINAL ARTICLESComparison of the RIFLE, AKIN and KDIGO criteria to predict mortality in critically ill patients
Revista brasileira de terapia intensiva. 2013;25(4):290-296
DOI 10.5935/0103-507X.20130050
Views3See moreObjective:
Acute kidney injury is a common complication in critically ill patients, and the RIFLE, AKIN and KDIGO criteria are used to classify these patients. The present study’s aim was to compare these criteria as predictors of mortality in critically ill patients.
Methods:
Prospective cohort study using medical records as the source of data. All patients admitted to the intensive care unit were included. The exclusion criteria were hospitalization for less than 24 hours and death. Patients were followed until discharge or death. Student’s t test, chi-squared analysis, a multivariate logistic regression and ROC curves were used for the data analysis.
Results:
The mean patient age was 64 years old, and the majority of patients were women of African descent. According to RIFLE, the mortality rates were 17.74%, 22.58%, 24.19% and 35.48% for patients without acute kidney injury (AKI) in stages of Risk, Injury and Failure, respectively. For AKIN, the mortality rates were 17.74%, 29.03%, 12.90% and 40.32% for patients without AKI and at stage I, stage II and stage III, respectively. For KDIGO 2012, the mortality rates were 17.74%, 29.03%, 11.29% and 41.94% for patients without AKI and at stage I, stage II and stage III, respectively. All three classification systems showed similar ROC curves for mortality.
Conclusion:
The RIFLE, AKIN and KDIGO criteria were good tools for predicting mortality in critically ill patients with no significant difference between them.
Views3Abstract
ORIGINAL ARTICLESComparison of the RIFLE, AKIN and KDIGO criteria to predict mortality in critically ill patients
Revista brasileira de terapia intensiva. 2013;25(4):290-296
DOI 10.5935/0103-507X.20130050
Views3See moreObjective:
Acute kidney injury is a common complication in critically ill patients, and the RIFLE, AKIN and KDIGO criteria are used to classify these patients. The present study’s aim was to compare these criteria as predictors of mortality in critically ill patients.
Methods:
Prospective cohort study using medical records as the source of data. All patients admitted to the intensive care unit were included. The exclusion criteria were hospitalization for less than 24 hours and death. Patients were followed until discharge or death. Student’s t test, chi-squared analysis, a multivariate logistic regression and ROC curves were used for the data analysis.
Results:
The mean patient age was 64 years old, and the majority of patients were women of African descent. According to RIFLE, the mortality rates were 17.74%, 22.58%, 24.19% and 35.48% for patients without acute kidney injury (AKI) in stages of Risk, Injury and Failure, respectively. For AKIN, the mortality rates were 17.74%, 29.03%, 12.90% and 40.32% for patients without AKI and at stage I, stage II and stage III, respectively. For KDIGO 2012, the mortality rates were 17.74%, 29.03%, 11.29% and 41.94% for patients without AKI and at stage I, stage II and stage III, respectively. All three classification systems showed similar ROC curves for mortality.
Conclusion:
The RIFLE, AKIN and KDIGO criteria were good tools for predicting mortality in critically ill patients with no significant difference between them.
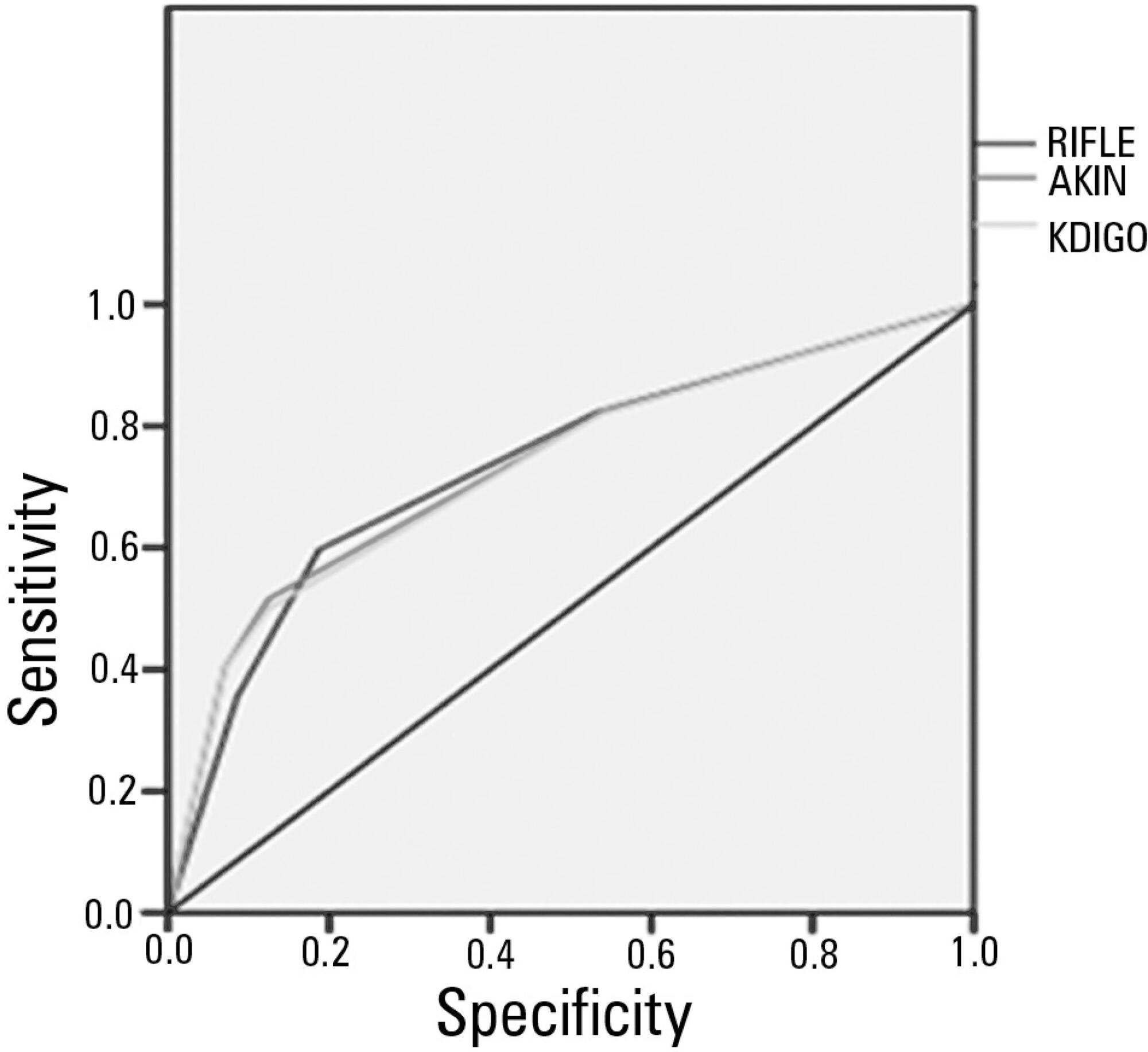
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric Mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency Risk factors SARS-CoV-2 Sepsis
Featured Articles
- ORIGINAL ARTICLE
Efficacy of melatonin in decreasing the incidence of delirium in critically ill adults: a randomized controlled trial
- Anjishnujit Bandyopadhyay ,
- Lakshmi Narayana Yaddanapudi ,
- Vikas Saini ,
- Neeru Sahni ,
- Sandeep Grover ,
- Sunaakshi Puri ,
- Vighnesh Ashok
Abstract
ORIGINAL ARTICLEEfficacy of melatonin in decreasing the incidence of delirium in critically ill adults: a randomized controlled trial
Critical Care Science. 2024;36:e20240144en
DOI 10.62675/2965-2774.20240144-en
- Anjishnujit Bandyopadhyay ,
- Lakshmi Narayana Yaddanapudi ,
- Vikas Saini ,
- Neeru Sahni ,
- Sandeep Grover ,
- Sunaakshi Puri ,
- Vighnesh Ashok
Views9See moreABSTRACT
Objective:
To determine whether enteral melatonin decreases the incidence of delirium in critically ill adults.
Methods:
In this randomized controlled trial, adults were admitted to the intensive care unit and received either usual standard care alone (Control Group) or in combination with 3mg of enteral melatonin once a day at 9 PM (Melatonin Group). Concealment of allocation was done by serially numbered opaque sealed envelopes. The intensivist assessing delirium and the investigator performing the data analysis were blinded to the group allocation. The primary outcome was the incidence of delirium within 24 hours of the intensive care unit stay. The secondary outcomes were the incidence of delirium on Days 3 and 7, intensive care unit mortality, length of intensive care unit stay, duration of mechanical ventilation and Glasgow outcome score (at discharge).
Results:
We included 108 patients in the final analysis, with 54 patients in each group. At 24 hours of intensive care unit stay, there was no difference in the incidence of delirium between Melatonin and Control Groups (29.6 versus 46.2%; RR = 0.6; 95%CI 0.38 – 1.05; p = 0.11). No secondary outcome showed a statistically significant difference.
Conclusion:
Enteral melatonin 3mg is not more effective at decreasing the incidence of delirium than standard care is in critically ill adults.
Views9Abstract
ORIGINAL ARTICLEEfficacy of melatonin in decreasing the incidence of delirium in critically ill adults: a randomized controlled trial
Critical Care Science. 2024;36:e20240144en
DOI 10.62675/2965-2774.20240144-en
- Anjishnujit Bandyopadhyay ,
- Lakshmi Narayana Yaddanapudi ,
- Vikas Saini ,
- Neeru Sahni ,
- Sandeep Grover ,
- Sunaakshi Puri ,
- Vighnesh Ashok
Views9See moreABSTRACT
Objective:
To determine whether enteral melatonin decreases the incidence of delirium in critically ill adults.
Methods:
In this randomized controlled trial, adults were admitted to the intensive care unit and received either usual standard care alone (Control Group) or in combination with 3mg of enteral melatonin once a day at 9 PM (Melatonin Group). Concealment of allocation was done by serially numbered opaque sealed envelopes. The intensivist assessing delirium and the investigator performing the data analysis were blinded to the group allocation. The primary outcome was the incidence of delirium within 24 hours of the intensive care unit stay. The secondary outcomes were the incidence of delirium on Days 3 and 7, intensive care unit mortality, length of intensive care unit stay, duration of mechanical ventilation and Glasgow outcome score (at discharge).
Results:
We included 108 patients in the final analysis, with 54 patients in each group. At 24 hours of intensive care unit stay, there was no difference in the incidence of delirium between Melatonin and Control Groups (29.6 versus 46.2%; RR = 0.6; 95%CI 0.38 – 1.05; p = 0.11). No secondary outcome showed a statistically significant difference.
Conclusion:
Enteral melatonin 3mg is not more effective at decreasing the incidence of delirium than standard care is in critically ill adults.
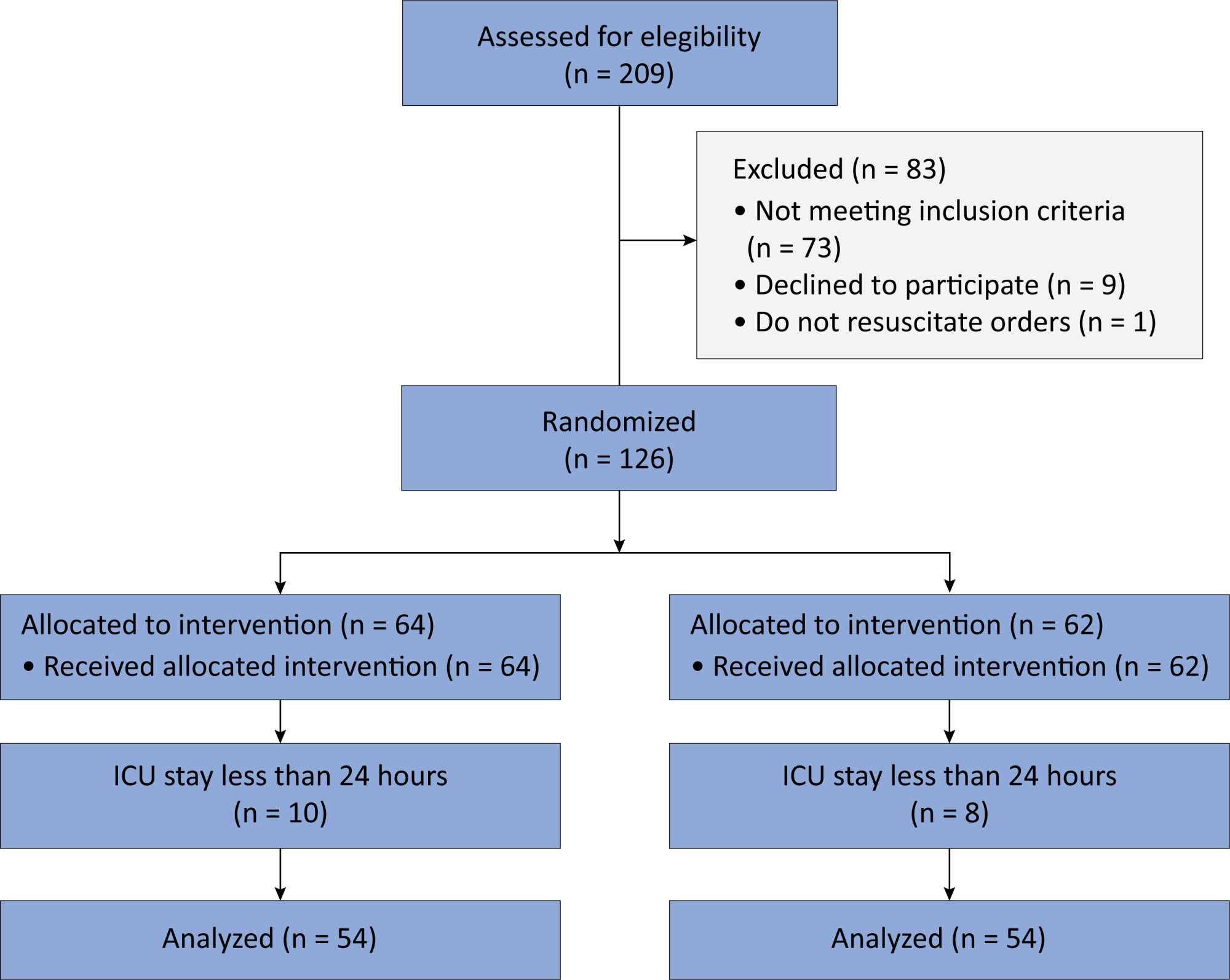
- Anjishnujit Bandyopadhyay
- SPECIAL ARTICLE
Intensive glucose control in critically ill adults: a protocol for a systematic review and individual patient data meta-analysis
- Derick Adigbli ,
- Li Yang,
- Naomi Hammond ,
- Djillali Annane,
- Yaseen Arabi ,
- Federico Bilotta ,
- Julien Bohé ,
- Frank Martin Brunkhorst ,
- Alexandre Biasi Cavalcanti ,
- Deborah Cook,
- Christoph Engel,
- Deborah Green-LaRoche ,
- Wei He,
- William Henderson,
- Cornelia Hoedemaekers ,
- Gaetano Iapichino ,
- Pierre Kalfon ,
- Gisela de La Rosa ,
- Iain MacKenzie,
- Christian Mélot ,
- Imogen Mitchell ,
- Tuomas Oksanen,
- Federico Polli ,
- Jean-Charles Preiser ,
- Francisco Garcia Soriano ,
- Ling-Cong Wang,
- Jiaxiang Yuan,
- Anthony Delaney ,
- Gian Luca Di Tanna ,
- Simon Finfer
Abstract
SPECIAL ARTICLEIntensive glucose control in critically ill adults: a protocol for a systematic review and individual patient data meta-analysis
Critical Care Science. 2023;35(4):345-354
DOI 10.5935/2965-2774.20230162-en
- Derick Adigbli ,
- Li Yang,
- Naomi Hammond ,
- Djillali Annane,
- Yaseen Arabi ,
- Federico Bilotta ,
- Julien Bohé ,
- Frank Martin Brunkhorst ,
- Alexandre Biasi Cavalcanti ,
- Deborah Cook,
- Christoph Engel,
- Deborah Green-LaRoche ,
- Wei He,
- William Henderson,
- Cornelia Hoedemaekers ,
- Gaetano Iapichino ,
- Pierre Kalfon ,
- Gisela de La Rosa ,
- Iain MacKenzie,
- Christian Mélot ,
- Imogen Mitchell ,
- Tuomas Oksanen,
- Federico Polli ,
- Jean-Charles Preiser ,
- Francisco Garcia Soriano ,
- Ling-Cong Wang,
- Jiaxiang Yuan,
- Anthony Delaney ,
- Gian Luca Di Tanna ,
- Simon Finfer
Views3ABSTRACT
Objective:
The optimal target for blood glucose concentration in critically ill patients is unclear. We will perform a systematic review and meta-analysis with aggregated and individual patient data from randomized controlled trials, comparing intensive glucose control with liberal glucose control in critically ill adults.
Data sources:
MEDLINE®, Embase, the Cochrane Central Register of Clinical Trials, and clinical trials registries (World Health Organization, clinical trials.gov). The authors of eligible trials will be invited to provide individual patient data. Published trial-level data from eligible trials that are not at high risk of bias will be included in an aggregated data meta-analysis if individual patient data are not available.
Methods:
Inclusion criteria: randomized controlled trials that recruited adult patients, targeting a blood glucose of ≤ 120mg/dL (≤ 6.6mmol/L) compared to a higher blood glucose concentration target using intravenous insulin in both groups. Excluded studies: those with an upper limit blood glucose target in the intervention group of > 120mg/dL (> 6.6mmol/L), or where intensive glucose control was only performed in the intraoperative period, and those where loss to follow-up exceeded 10% by hospital discharge.
Primary endpoint:
In-hospital mortality during index hospital admission. Secondary endpoints: mortality and survival at other timepoints, duration of invasive mechanical ventilation, vasoactive agents, and renal replacement therapy. A random effect Bayesian meta-analysis and hierarchical Bayesian models for individual patient data will be used.
Discussion:
This systematic review with aggregate and individual patient data will address the clinical question, ‘what is the best blood glucose target for critically ill patients overall?’
Keywords:Blood glucoseCritical illnessGlycemic controlInsulinIntraoperative periodMortalityPatient dischargeRegistriesSee moreViews3Abstract
SPECIAL ARTICLEIntensive glucose control in critically ill adults: a protocol for a systematic review and individual patient data meta-analysis
Critical Care Science. 2023;35(4):345-354
DOI 10.5935/2965-2774.20230162-en
- Derick Adigbli ,
- Li Yang,
- Naomi Hammond ,
- Djillali Annane,
- Yaseen Arabi ,
- Federico Bilotta ,
- Julien Bohé ,
- Frank Martin Brunkhorst ,
- Alexandre Biasi Cavalcanti ,
- Deborah Cook,
- Christoph Engel,
- Deborah Green-LaRoche ,
- Wei He,
- William Henderson,
- Cornelia Hoedemaekers ,
- Gaetano Iapichino ,
- Pierre Kalfon ,
- Gisela de La Rosa ,
- Iain MacKenzie,
- Christian Mélot ,
- Imogen Mitchell ,
- Tuomas Oksanen,
- Federico Polli ,
- Jean-Charles Preiser ,
- Francisco Garcia Soriano ,
- Ling-Cong Wang,
- Jiaxiang Yuan,
- Anthony Delaney ,
- Gian Luca Di Tanna ,
- Simon Finfer
Views3ABSTRACT
Objective:
The optimal target for blood glucose concentration in critically ill patients is unclear. We will perform a systematic review and meta-analysis with aggregated and individual patient data from randomized controlled trials, comparing intensive glucose control with liberal glucose control in critically ill adults.
Data sources:
MEDLINE®, Embase, the Cochrane Central Register of Clinical Trials, and clinical trials registries (World Health Organization, clinical trials.gov). The authors of eligible trials will be invited to provide individual patient data. Published trial-level data from eligible trials that are not at high risk of bias will be included in an aggregated data meta-analysis if individual patient data are not available.
Methods:
Inclusion criteria: randomized controlled trials that recruited adult patients, targeting a blood glucose of ≤ 120mg/dL (≤ 6.6mmol/L) compared to a higher blood glucose concentration target using intravenous insulin in both groups. Excluded studies: those with an upper limit blood glucose target in the intervention group of > 120mg/dL (> 6.6mmol/L), or where intensive glucose control was only performed in the intraoperative period, and those where loss to follow-up exceeded 10% by hospital discharge.
Primary endpoint:
In-hospital mortality during index hospital admission. Secondary endpoints: mortality and survival at other timepoints, duration of invasive mechanical ventilation, vasoactive agents, and renal replacement therapy. A random effect Bayesian meta-analysis and hierarchical Bayesian models for individual patient data will be used.
Discussion:
This systematic review with aggregate and individual patient data will address the clinical question, ‘what is the best blood glucose target for critically ill patients overall?’
Keywords:Blood glucoseCritical illnessGlycemic controlInsulinIntraoperative periodMortalityPatient dischargeRegistriesSee more - Derick Adigbli
- ARTIGO ORIGINAL
Impact of vertical positioning on lung aeration among mechanically ventilated intensive care unit patients: a randomized crossover clinical trial
- Douglas Neves ,
- Paulo Ricardo Marques Filho ,
- Raquel da Silva Townsend ,
- Cristiano dos Santos Rodrigues ,
- Luciana Tagliari ,
- Laura Cordeiro Madeira ,
- Mariana Fensterseifer Mattioni ,
- Márcio Luiz Ferreira de Camillis ,
- Clarissa Garcia Soares Leães ,
- Juliana Mara Stormovski de Andrade ,
- Caroline Cabral Robinson ,
- Daniel Sganzerla ,
- Laura Drehmer ,
- Denis Fernandes Madruga da Costa ,
- André Sant’Ana Machado ,
- Regis Goulart Rosa ,
- Pedro Dal Lago
Abstract
ARTIGO ORIGINALImpact of vertical positioning on lung aeration among mechanically ventilated intensive care unit patients: a randomized crossover clinical trial
Critical Care Science. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-en
- Douglas Neves ,
- Paulo Ricardo Marques Filho ,
- Raquel da Silva Townsend ,
- Cristiano dos Santos Rodrigues ,
- Luciana Tagliari ,
- Laura Cordeiro Madeira ,
- Mariana Fensterseifer Mattioni ,
- Márcio Luiz Ferreira de Camillis ,
- Clarissa Garcia Soares Leães ,
- Juliana Mara Stormovski de Andrade ,
- Caroline Cabral Robinson ,
- Daniel Sganzerla ,
- Laura Drehmer ,
- Denis Fernandes Madruga da Costa ,
- André Sant’Ana Machado ,
- Regis Goulart Rosa ,
- Pedro Dal Lago
Views5ABSTRACT
Objective:
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
Methods:
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
Results:
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
Conclusion:
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Keywords:AerationIntensive care unitsLungRespiration, artificialSitting positionStanding positionUltrasonographySee moreViews5Abstract
ARTIGO ORIGINALImpact of vertical positioning on lung aeration among mechanically ventilated intensive care unit patients: a randomized crossover clinical trial
Critical Care Science. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-en
- Douglas Neves ,
- Paulo Ricardo Marques Filho ,
- Raquel da Silva Townsend ,
- Cristiano dos Santos Rodrigues ,
- Luciana Tagliari ,
- Laura Cordeiro Madeira ,
- Mariana Fensterseifer Mattioni ,
- Márcio Luiz Ferreira de Camillis ,
- Clarissa Garcia Soares Leães ,
- Juliana Mara Stormovski de Andrade ,
- Caroline Cabral Robinson ,
- Daniel Sganzerla ,
- Laura Drehmer ,
- Denis Fernandes Madruga da Costa ,
- André Sant’Ana Machado ,
- Regis Goulart Rosa ,
- Pedro Dal Lago
Views5ABSTRACT
Objective:
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
Methods:
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
Results:
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
Conclusion:
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Keywords:AerationIntensive care unitsLungRespiration, artificialSitting positionStanding positionUltrasonographySee more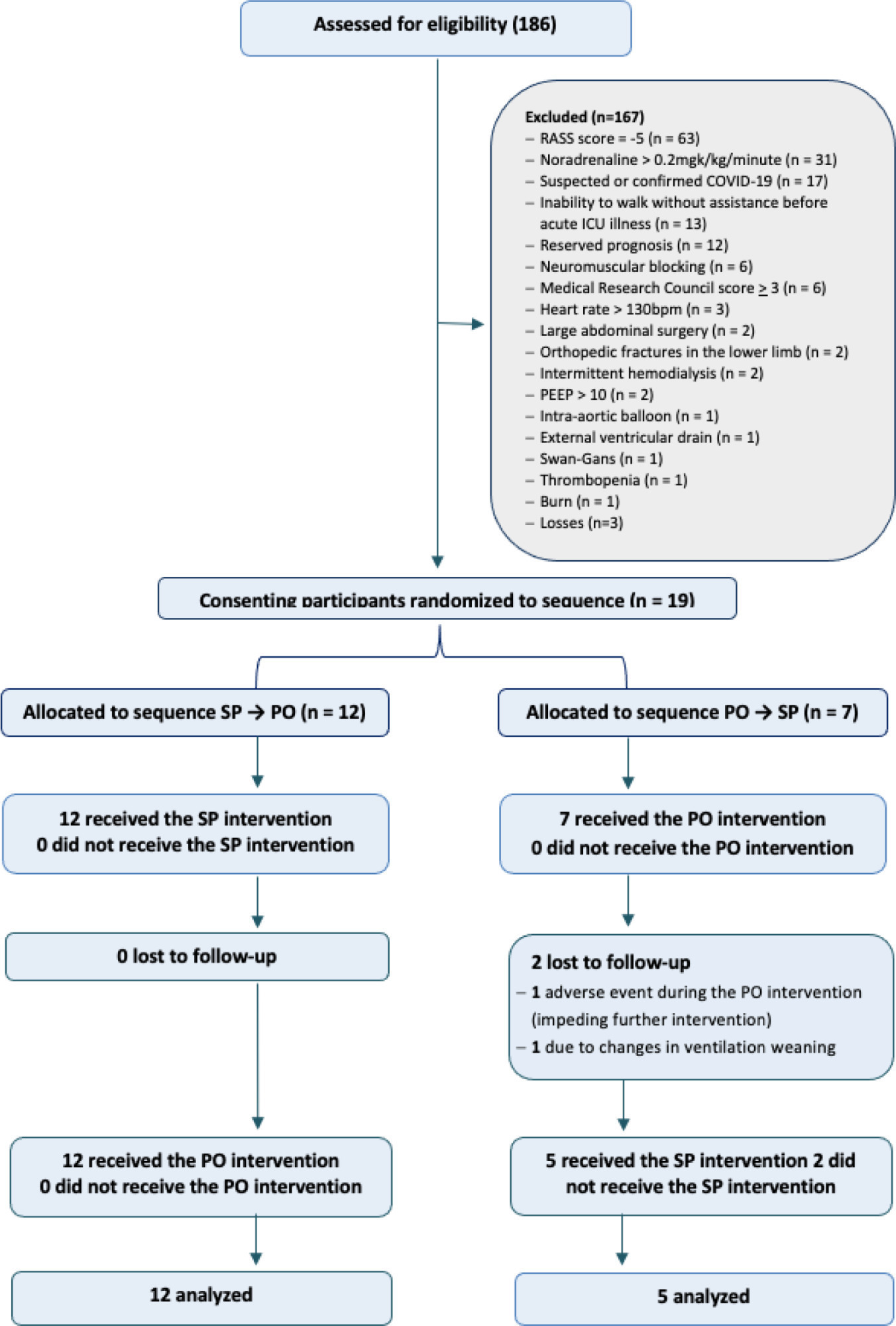
- Douglas Neves
Have your research published in our journal!
Publish your research in a full open access journal with credibility and high scientific and ethical standards.



