-
Editorial
Fairness, not maleficence, in terminal critical patients care
Rev Bras Ter Intensiva. 2009;21(4):341-342
Abstract
EditorialFairness, not maleficence, in terminal critical patients care
Rev Bras Ter Intensiva. 2009;21(4):341-342
Views0

Abstract
EditorialFairness, not maleficence, in terminal critical patients care
Rev Bras Ter Intensiva. 2009;21(4):341-342
-
Original Articles
Lack of association between interleukin-1 gene polymorphism and prognosis in severe traumatic brain injury patients
Rev Bras Ter Intensiva. 2009;21(4):343-348
Abstract
Original ArticlesLack of association between interleukin-1 gene polymorphism and prognosis in severe traumatic brain injury patients
Rev Bras Ter Intensiva. 2009;21(4):343-348
DOI 10.1590/S0103-507X2009000400002
Views0See moreOBJECTIVE: Traumatic brain injury is the major cause of death among individuals between 1-45 years-old. The outcome of traumatic brain injury may be related to brain susceptibility to the injury and genetic factors. Genes that may affect traumatic brain injury outcome are being investigated, however there is still few data concerning the association between genetic polymorphisms and traumatic brain injury outcome. The interleukin-1 beta gene (IL-1B) is one of the most studied genes, because levels of this cytokine are raised after traumatic brain injury and this can affect worsen the prognosis. The aim of this study was to test whether the -31C/T polymorphism, located at the promoter region of the IL-1B gene, is associated with primary short-term outcome (death or intensive care unit discharge) in severe traumatic brain injury patients. METHODS: Were studied 69 patients admitted with severe traumatic brain injury in three hospitals of the metropolitan region of Porto Alegre. The polymorphism was analyzed by polymerase chain reaction, followed by restriction digestion. RESULTS: Severe traumatic brain injury was associated with a 45% mortality rate. No significant differences were observed in the allele and genotype frequencies between patients stratified by traumatic brain injury outcome. CONCLUSION: Our findings suggest that -31C/T IL-1B gene polymorphism have no significant impact on the outcome of patients after acute severe traumatic brain injury.
Views0Abstract
Original ArticlesLack of association between interleukin-1 gene polymorphism and prognosis in severe traumatic brain injury patients
Rev Bras Ter Intensiva. 2009;21(4):343-348
DOI 10.1590/S0103-507X2009000400002
Views0See moreOBJECTIVE: Traumatic brain injury is the major cause of death among individuals between 1-45 years-old. The outcome of traumatic brain injury may be related to brain susceptibility to the injury and genetic factors. Genes that may affect traumatic brain injury outcome are being investigated, however there is still few data concerning the association between genetic polymorphisms and traumatic brain injury outcome. The interleukin-1 beta gene (IL-1B) is one of the most studied genes, because levels of this cytokine are raised after traumatic brain injury and this can affect worsen the prognosis. The aim of this study was to test whether the -31C/T polymorphism, located at the promoter region of the IL-1B gene, is associated with primary short-term outcome (death or intensive care unit discharge) in severe traumatic brain injury patients. METHODS: Were studied 69 patients admitted with severe traumatic brain injury in three hospitals of the metropolitan region of Porto Alegre. The polymorphism was analyzed by polymerase chain reaction, followed by restriction digestion. RESULTS: Severe traumatic brain injury was associated with a 45% mortality rate. No significant differences were observed in the allele and genotype frequencies between patients stratified by traumatic brain injury outcome. CONCLUSION: Our findings suggest that -31C/T IL-1B gene polymorphism have no significant impact on the outcome of patients after acute severe traumatic brain injury.
-
Original Articles
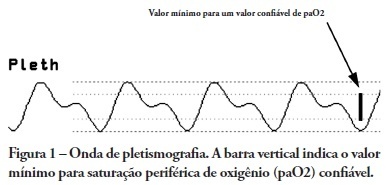
Comparison between respiratory pulse oximetry plethysmographic waveform amplitude and arterial pulse pressure variations among patients with and without norepinephrine use
Rev Bras Ter Intensiva. 2009;21(4):349-352
Abstract
Original ArticlesComparison between respiratory pulse oximetry plethysmographic waveform amplitude and arterial pulse pressure variations among patients with and without norepinephrine use
Rev Bras Ter Intensiva. 2009;21(4):349-352
DOI 10.1590/S0103-507X2009000400003
Views0See moreOBJECTIVES: Arterial pulse pressure respiratory variation is a good predictor of fluid response in ventilated patients. Recently, it was shown that respiratory variation in arterial pulse pressure correlates with variation in pulse oximetry plethysmographic waveform amplitude. We wanted to evaluate the correlation between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude, and to determine whether this correlation was influenced by norepinephrine administration. METHODS: Prospective study of sixty patients with normal sinus rhythm on mechanical ventilation, profoundly sedated and with stable hemodynamics. Oxygenation index and invasive arterial pressure were monitored. Respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude were recorded simultaneously in a beat-to-beat evaluation, and were compared using the Pearson coefficient of agreement and linear regression. RESULTS: Thirty patients (50%) required norepinephrine. There was a significant correlation (K = 0.66; p < 0.001) between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude. Area under the ROC curve was 0.88 (range, 0.79 - 0.97), with a best cutoff value of 14% to predict a respiratory variation in arterial pulse pressure of 13. The use of norepinephrine did not influence the correlation (K = 0.63, p = 0.001, respectively). CONCLUSIONS: Respiratory variation in arterial pulse pressure above 13% can be accurately predicted by a respiratory variation in pulse oximetry plethysmographic waveform amplitude of 14%. The use of norepinephrine does not alter this relationship.
Views0Abstract
Original ArticlesComparison between respiratory pulse oximetry plethysmographic waveform amplitude and arterial pulse pressure variations among patients with and without norepinephrine use
Rev Bras Ter Intensiva. 2009;21(4):349-352
DOI 10.1590/S0103-507X2009000400003
Views0See moreOBJECTIVES: Arterial pulse pressure respiratory variation is a good predictor of fluid response in ventilated patients. Recently, it was shown that respiratory variation in arterial pulse pressure correlates with variation in pulse oximetry plethysmographic waveform amplitude. We wanted to evaluate the correlation between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude, and to determine whether this correlation was influenced by norepinephrine administration. METHODS: Prospective study of sixty patients with normal sinus rhythm on mechanical ventilation, profoundly sedated and with stable hemodynamics. Oxygenation index and invasive arterial pressure were monitored. Respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude were recorded simultaneously in a beat-to-beat evaluation, and were compared using the Pearson coefficient of agreement and linear regression. RESULTS: Thirty patients (50%) required norepinephrine. There was a significant correlation (K = 0.66; p < 0.001) between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude. Area under the ROC curve was 0.88 (range, 0.79 - 0.97), with a best cutoff value of 14% to predict a respiratory variation in arterial pulse pressure of 13. The use of norepinephrine did not influence the correlation (K = 0.63, p = 0.001, respectively). CONCLUSIONS: Respiratory variation in arterial pulse pressure above 13% can be accurately predicted by a respiratory variation in pulse oximetry plethysmographic waveform amplitude of 14%. The use of norepinephrine does not alter this relationship.
-
Original Articles
Early predictive factors for intensive care unit readmission
Rev Bras Ter Intensiva. 2009;21(4):353-358
Abstract
Original ArticlesEarly predictive factors for intensive care unit readmission
Rev Bras Ter Intensiva. 2009;21(4):353-358
DOI 10.1590/S0103-507X2009000400004
Views0OBJECTIVE: To predict readmission in intensive care unit analyzing the first 24 hours data after intensive care unit admission. METHODS: The first intensive care unit admission of patients was analyzed from January to May 2009 in a mixed unit. Readmission to the unit was considered those during the same hospital stay or within 3 months after intensive care unit discharge. Deaths during the first admission were excluded. Demographic data, use of mechanical ventilation, and report of stay longer than 3 days were submitted to uni and multivariate analysis for readmission. RESULTS: Five hundred seventy-seven patients were included (33 excluded deaths). The readmission group had 59 patients, while 518 patients were not readmitted. The lead time between the index admission and readmission was 9 (3-28) days (18 were readmitted in less than 3 days), and 10 died. Patients readmitted at least once to the intensive care unit had the differences below in comparison to the control group: older age: 75 (67-81) versus 67 (56-78) years, P<0.01; admission for respiratory insufficiency or sepsis: 33 versus 13%, P<0.01; medical admission: 49 versus 32%, P<0.05; higher SAPS II score: 27 (21-35) versus 23 (18-29) points, P<0.01; Charlson index: 2 (1-2) versus 1 (0-2) points, P<0.01; first ICU stay longer than 3 days: 35 versus 23%, P<0.01. After logistic regression, higher age, Charlson index and admission for respiratory and sepsis were independently associated to readmissions in intensive care unit. CONCLUSION: Age, comorbidities and respiratory- and/or sepsis-related admission are associated with increased readmission risk in the studied sample.
Keywords:HospitalizationLength of staymorbidityPatient admissionPatient readmissionQuality of health careSee moreViews0Abstract
Original ArticlesEarly predictive factors for intensive care unit readmission
Rev Bras Ter Intensiva. 2009;21(4):353-358
DOI 10.1590/S0103-507X2009000400004
Views0OBJECTIVE: To predict readmission in intensive care unit analyzing the first 24 hours data after intensive care unit admission. METHODS: The first intensive care unit admission of patients was analyzed from January to May 2009 in a mixed unit. Readmission to the unit was considered those during the same hospital stay or within 3 months after intensive care unit discharge. Deaths during the first admission were excluded. Demographic data, use of mechanical ventilation, and report of stay longer than 3 days were submitted to uni and multivariate analysis for readmission. RESULTS: Five hundred seventy-seven patients were included (33 excluded deaths). The readmission group had 59 patients, while 518 patients were not readmitted. The lead time between the index admission and readmission was 9 (3-28) days (18 were readmitted in less than 3 days), and 10 died. Patients readmitted at least once to the intensive care unit had the differences below in comparison to the control group: older age: 75 (67-81) versus 67 (56-78) years, P<0.01; admission for respiratory insufficiency or sepsis: 33 versus 13%, P<0.01; medical admission: 49 versus 32%, P<0.05; higher SAPS II score: 27 (21-35) versus 23 (18-29) points, P<0.01; Charlson index: 2 (1-2) versus 1 (0-2) points, P<0.01; first ICU stay longer than 3 days: 35 versus 23%, P<0.01. After logistic regression, higher age, Charlson index and admission for respiratory and sepsis were independently associated to readmissions in intensive care unit. CONCLUSION: Age, comorbidities and respiratory- and/or sepsis-related admission are associated with increased readmission risk in the studied sample.
Keywords:HospitalizationLength of staymorbidityPatient admissionPatient readmissionQuality of health careSee more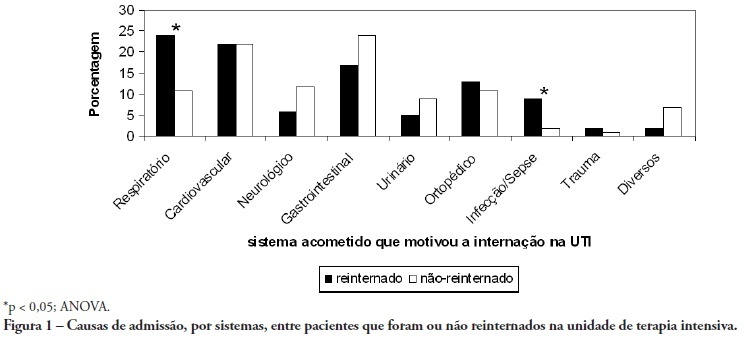
-
Original Articles
RIFLE: association with mortality and length of stay in critically ill acute kidney injury patients
Rev Bras Ter Intensiva. 2009;21(4):359-368
Abstract
Original ArticlesRIFLE: association with mortality and length of stay in critically ill acute kidney injury patients
Rev Bras Ter Intensiva. 2009;21(4):359-368
DOI 10.1590/S0103-507X2009000400005
Views0OBJECTIVE: To correlate the RIFLE classification with mortality and length of stay both in the intensive care unit and hospital. METHODS: A prospective, observational, longitudinal cohort study, approved by the Institution’s Ethics Committee. Data were collected for all patients staying longer than 24 hours in the intensive care unit of Hospital Universitário Polydoro Ernani de São Thiago – Universidade Federal de Santa Catarina from September 2007 to March 2008, followed-up either until discharge or death. Patients were divided in two groups: with or without acute kidney injury. The acute kidney injury group was additionally divided according to the RIFLE and sub-divided according to the maximal score in Risk, Injury of Failure. Loss and End-stage classes were not included in the study. APACHE II and SOFA were also evaluated. The t Student and Chi-Square tests were used. A P<0.05 was considered statistically significant. RESULTS: The sample included 129 patients, 52 (40.3%) with acute kidney injury according to RIFLE. Patients were more severely ill in this group, with higher APACHE and SOFA scores (P<0.05). Compared to the without kidney injury group, the kidney injury severity caused increased intensive care unity (Risk 25%; Injury 37.5%; Failure 62.5%) and in-hospital (Risk 50%; Injury 37.5%; Failure 62.5%) mortality, and longer intensive care unit stay (P<0.05). CONCLUSION: The RIFLE system, according to the severity class, was a marker for risk of increased intensive care unit and in-hospital mortality, and longer intensive care unit stay. No relationship with in-hospital length of stay was found.
Keywords:APACHECreatinineHospital mortalityIntensive care unitsLength of stayRenal insufficiency, acuteSee moreViews0Abstract
Original ArticlesRIFLE: association with mortality and length of stay in critically ill acute kidney injury patients
Rev Bras Ter Intensiva. 2009;21(4):359-368
DOI 10.1590/S0103-507X2009000400005
Views0OBJECTIVE: To correlate the RIFLE classification with mortality and length of stay both in the intensive care unit and hospital. METHODS: A prospective, observational, longitudinal cohort study, approved by the Institution’s Ethics Committee. Data were collected for all patients staying longer than 24 hours in the intensive care unit of Hospital Universitário Polydoro Ernani de São Thiago – Universidade Federal de Santa Catarina from September 2007 to March 2008, followed-up either until discharge or death. Patients were divided in two groups: with or without acute kidney injury. The acute kidney injury group was additionally divided according to the RIFLE and sub-divided according to the maximal score in Risk, Injury of Failure. Loss and End-stage classes were not included in the study. APACHE II and SOFA were also evaluated. The t Student and Chi-Square tests were used. A P<0.05 was considered statistically significant. RESULTS: The sample included 129 patients, 52 (40.3%) with acute kidney injury according to RIFLE. Patients were more severely ill in this group, with higher APACHE and SOFA scores (P<0.05). Compared to the without kidney injury group, the kidney injury severity caused increased intensive care unity (Risk 25%; Injury 37.5%; Failure 62.5%) and in-hospital (Risk 50%; Injury 37.5%; Failure 62.5%) mortality, and longer intensive care unit stay (P<0.05). CONCLUSION: The RIFLE system, according to the severity class, was a marker for risk of increased intensive care unit and in-hospital mortality, and longer intensive care unit stay. No relationship with in-hospital length of stay was found.
Keywords:APACHECreatinineHospital mortalityIntensive care unitsLength of stayRenal insufficiency, acuteSee more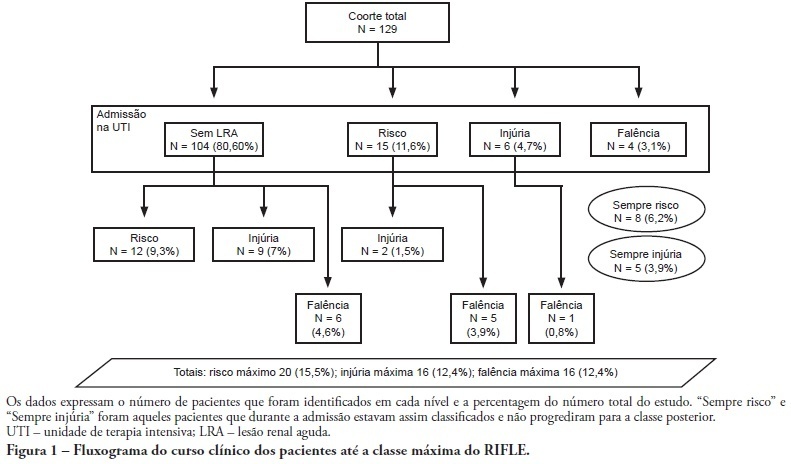
-
Original Articles
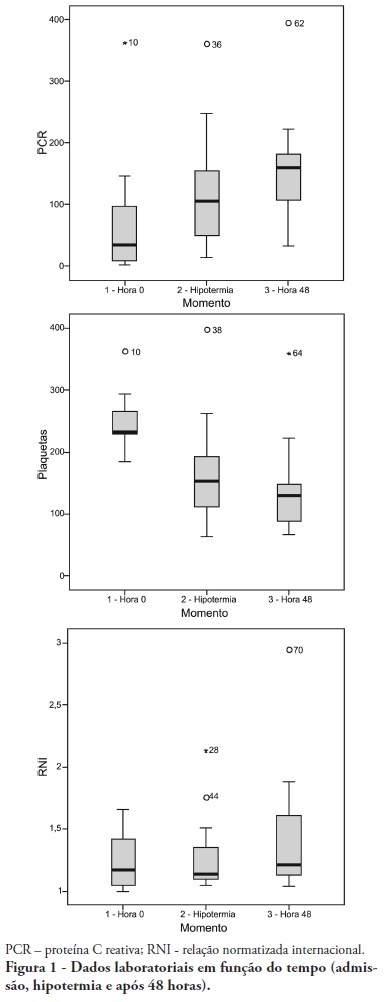
Study of resuscitated in- and out-hospital cardiorespiratory arrest patients undergoing therapeutic hypothermia
Rev Bras Ter Intensiva. 2009;21(4):369-375
Abstract
Original ArticlesStudy of resuscitated in- and out-hospital cardiorespiratory arrest patients undergoing therapeutic hypothermia
Rev Bras Ter Intensiva. 2009;21(4):369-375
DOI 10.1590/S0103-507X2009000400006
Views0See moreOBJECTIVE: To determine the characteristics of patients undergoing standard institutional protocol for management of resuscitated patients after a cardiac arrest episode, including therapeutic hypothermia. METHODS: This was a retrospective analysis of 26 consecutive patients admitted following cardiac arrest, between January 2007 and November 2008. RESULTS: All cases underwent therapeutic hypothermia. Average age was 63 years, and the patients were predominantly male. Cardiac arrest event was out-of-hospital in 8 cases, in the emergency room in 3 cases, in the wards in 13 cases and in the operation room in 2 cases. The cardiac arrest rhythm was ventricular fibrillation in seven patients, asystolia in 11, pulseless electrical activity in 5 cases, and was undetermined in 3 patients. The interval between the cardiac arrest and return of spontaneous circulation was 12 minutes (SD ± 5 min). The time to reach the target temperature was 5 ± 4 hours, the hypothermia time was 22 ± 6 hours and time to rewarming 9 ± 5.9 hours. Fourteen patients died in the intensive care unit, a 54% mortality, and three patients died during the in-hospital stay, a 66% in-hospital mortality. There was statistically significant reduction in hemoglobin (p<0.001), leukocytes (p=0.001), platelets (p<0.001), lactate (p<0.001) and potassium (p=0.009), values and increased C reactive protein (p=0.001) and INR (p=0.004) after hypothermia. CONCLUSIONS: The creation of a standard operative protocol for therapeutic hypothermia in post cardiac arrest patients management resulted in a high use of therapeutic hypothermia. The clinical results of this protocol adapted from randomized studies are similar to the literature.
Views0Abstract
Original ArticlesStudy of resuscitated in- and out-hospital cardiorespiratory arrest patients undergoing therapeutic hypothermia
Rev Bras Ter Intensiva. 2009;21(4):369-375
DOI 10.1590/S0103-507X2009000400006
Views0See moreOBJECTIVE: To determine the characteristics of patients undergoing standard institutional protocol for management of resuscitated patients after a cardiac arrest episode, including therapeutic hypothermia. METHODS: This was a retrospective analysis of 26 consecutive patients admitted following cardiac arrest, between January 2007 and November 2008. RESULTS: All cases underwent therapeutic hypothermia. Average age was 63 years, and the patients were predominantly male. Cardiac arrest event was out-of-hospital in 8 cases, in the emergency room in 3 cases, in the wards in 13 cases and in the operation room in 2 cases. The cardiac arrest rhythm was ventricular fibrillation in seven patients, asystolia in 11, pulseless electrical activity in 5 cases, and was undetermined in 3 patients. The interval between the cardiac arrest and return of spontaneous circulation was 12 minutes (SD ± 5 min). The time to reach the target temperature was 5 ± 4 hours, the hypothermia time was 22 ± 6 hours and time to rewarming 9 ± 5.9 hours. Fourteen patients died in the intensive care unit, a 54% mortality, and three patients died during the in-hospital stay, a 66% in-hospital mortality. There was statistically significant reduction in hemoglobin (p<0.001), leukocytes (p=0.001), platelets (p<0.001), lactate (p<0.001) and potassium (p=0.009), values and increased C reactive protein (p=0.001) and INR (p=0.004) after hypothermia. CONCLUSIONS: The creation of a standard operative protocol for therapeutic hypothermia in post cardiac arrest patients management resulted in a high use of therapeutic hypothermia. The clinical results of this protocol adapted from randomized studies are similar to the literature.
-
Original Articles
Enteral nutritional therapy: application of quality indicators
Rev Bras Ter Intensiva. 2009;21(4):376-383
Abstract
Original ArticlesEnteral nutritional therapy: application of quality indicators
Rev Bras Ter Intensiva. 2009;21(4):376-383
DOI 10.1590/S0103-507X2009000400007
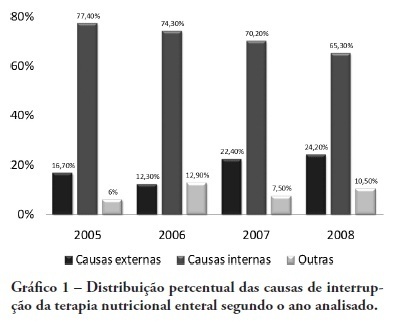
Views0See moreOBJECTIVE: Monitor the adequacy of enteral nutritional therapy at the intensive care unit aiming to improve the quality of nutritional assistance. METHODS: Prospective and observational study developed at the adult intensive care unit from 2005 to 2008. Patients over 18 years of age with exclusive enteral nutritional therapy for over 72h participated in the sample. The average values and the percentile adequacy of energy and proteins calculated, prescribed and administered in each year were analyzed. The factors responsible for the non-conformity of the administration planned were classified into intensive care unit extrinsic or intrinsic causes. The quality indicators proposed by the ILSI Brazil were applied, and expressed into percentile goals. In the statistic analyses, confidence interval and the t Student e Mann-Whitney (p<0.05) tests were used, according to the Epi Info program. RESULTS: One hundred and sixteen patients were followed up. There were statically difference in values of energy and protein administered in 2005 and in 2006, when compared to those in 2008. The adequacy calculated/prescribed remained close to 100% in all the surveys and the adequacy administered/prescribed increased from 74% in 2005, to 89% in 2008. An increase in interruptions of enteral nutritional therapy for external factors and the decrease in interruptions for intensive care unit internal factors were verified. The quality indicators equally reflect the evolution of the patient care. CONCLUSION: In the four yearly surveys, a progressive enhancement of nutritional support was verified. Quality indicators allow nutritional care evolution monitoring, the comparison to other services data, and are a new perspective for enteral nutritional therapy assessment.
Views0Abstract
Original ArticlesEnteral nutritional therapy: application of quality indicators
Rev Bras Ter Intensiva. 2009;21(4):376-383
DOI 10.1590/S0103-507X2009000400007
Views0See moreOBJECTIVE: Monitor the adequacy of enteral nutritional therapy at the intensive care unit aiming to improve the quality of nutritional assistance. METHODS: Prospective and observational study developed at the adult intensive care unit from 2005 to 2008. Patients over 18 years of age with exclusive enteral nutritional therapy for over 72h participated in the sample. The average values and the percentile adequacy of energy and proteins calculated, prescribed and administered in each year were analyzed. The factors responsible for the non-conformity of the administration planned were classified into intensive care unit extrinsic or intrinsic causes. The quality indicators proposed by the ILSI Brazil were applied, and expressed into percentile goals. In the statistic analyses, confidence interval and the t Student e Mann-Whitney (p<0.05) tests were used, according to the Epi Info program. RESULTS: One hundred and sixteen patients were followed up. There were statically difference in values of energy and protein administered in 2005 and in 2006, when compared to those in 2008. The adequacy calculated/prescribed remained close to 100% in all the surveys and the adequacy administered/prescribed increased from 74% in 2005, to 89% in 2008. An increase in interruptions of enteral nutritional therapy for external factors and the decrease in interruptions for intensive care unit internal factors were verified. The quality indicators equally reflect the evolution of the patient care. CONCLUSION: In the four yearly surveys, a progressive enhancement of nutritional support was verified. Quality indicators allow nutritional care evolution monitoring, the comparison to other services data, and are a new perspective for enteral nutritional therapy assessment.
-
Original Articles
Epidemiologic analysis of clinical isolates of Pseudomonas aeruginosa from an university hospital
Rev Bras Ter Intensiva. 2009;21(4):384-390
Abstract
Original ArticlesEpidemiologic analysis of clinical isolates of Pseudomonas aeruginosa from an university hospital
Rev Bras Ter Intensiva. 2009;21(4):384-390
DOI 10.1590/S0103-507X2009000400008
Views0OBJECTIVES: Pseudomonas aeruginosa is an increasingly prevalent opportunistic pathogen in hospital infection cases. Its high resistance rates to many antimicrobials has given this microorganism a relevant role among other highly prevalent bacteria involved in nosocomial infections. This study aimed to analyze epidemiologic characteristics of P. aeruginosa and to evaluate its susceptibility to antimicrobial agents at Hospital das Clínicas of the Universidade Federal de Pernambuco METHODS: A retrospective study was performed based on the registry book of miscellaneous secretions from the bacteriology laboratory of the Hospital das Clínicas involving the period between January and June 2008. Among the secretions registered, were identified the positives samples for P. aeruginosa, whose origin was analyzed, as well as its susceptibility profile to routinely used in our laboratory antimicrobials. RESULTS: The bacteria most frequently isolated from miscellaneous secretions bacteria were P. aeruginosa (26%) and S. aureus (25%). P. aeruginosa was mainly isolated from respiratory infections, with 33% of positive samples for this organism from tracheal secretions and 21% from nasal. The most effective antimicrobials against P. aeruginosa were: amikacin, imipenem, meropenem and aztreonam. CONCLUSIONS: These results show a high prevalence of P. aeruginosa in the Hospital das Clínicas of the Universidade Federal de Pernambuco. Despite featuring high resistance rates to older antimicrobials, as cephalosporins first and second generations and chloramphenicol, this pathogen showed good susceptibility to agents routinely used in this hospital.
Keywords:Antimicrobial drugs resistanceNosocomial infectionsPseudomonas aeruginosaPseudomonas infectionsSee moreViews0Abstract
Original ArticlesEpidemiologic analysis of clinical isolates of Pseudomonas aeruginosa from an university hospital
Rev Bras Ter Intensiva. 2009;21(4):384-390
DOI 10.1590/S0103-507X2009000400008
Views0OBJECTIVES: Pseudomonas aeruginosa is an increasingly prevalent opportunistic pathogen in hospital infection cases. Its high resistance rates to many antimicrobials has given this microorganism a relevant role among other highly prevalent bacteria involved in nosocomial infections. This study aimed to analyze epidemiologic characteristics of P. aeruginosa and to evaluate its susceptibility to antimicrobial agents at Hospital das Clínicas of the Universidade Federal de Pernambuco METHODS: A retrospective study was performed based on the registry book of miscellaneous secretions from the bacteriology laboratory of the Hospital das Clínicas involving the period between January and June 2008. Among the secretions registered, were identified the positives samples for P. aeruginosa, whose origin was analyzed, as well as its susceptibility profile to routinely used in our laboratory antimicrobials. RESULTS: The bacteria most frequently isolated from miscellaneous secretions bacteria were P. aeruginosa (26%) and S. aureus (25%). P. aeruginosa was mainly isolated from respiratory infections, with 33% of positive samples for this organism from tracheal secretions and 21% from nasal. The most effective antimicrobials against P. aeruginosa were: amikacin, imipenem, meropenem and aztreonam. CONCLUSIONS: These results show a high prevalence of P. aeruginosa in the Hospital das Clínicas of the Universidade Federal de Pernambuco. Despite featuring high resistance rates to older antimicrobials, as cephalosporins first and second generations and chloramphenicol, this pathogen showed good susceptibility to agents routinely used in this hospital.
Keywords:Antimicrobial drugs resistanceNosocomial infectionsPseudomonas aeruginosaPseudomonas infectionsSee more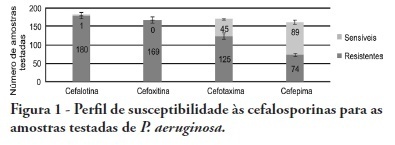
-
Original Articles
Red blood cells transfusion in intensive care unit
Rev Bras Ter Intensiva. 2009;21(4):391-397
Abstract
Original ArticlesRed blood cells transfusion in intensive care unit
Rev Bras Ter Intensiva. 2009;21(4):391-397
DOI 10.1590/S0103-507X2009000400009
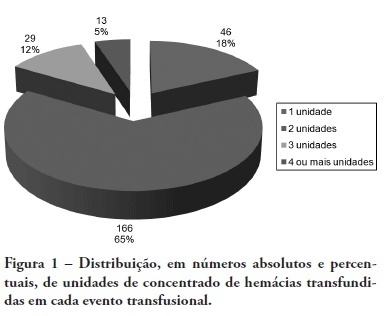
Views0See moreBACKGROUND: The anemia is a common problem upon admission of the patients in the intensive care unit being the red blood cell transfusion a frequent therapeutic. The causes of anemia in critical patients who under go red blood cell transfusion are several: acute loss of blood after trauma, gastrointestinal hemorrhage, surgery amongst others. Currently, few studies are available regarding the use of blood components in patients at intensive care unit. Although blood transfusions are frequent in intensive care unit, the optimized criteria for handling are not clearly defined, with no available guidelines. OBJECTIVES: To analyze the clinical indications of the use of the red blood cell in the intensive care unit. METHODS: The clinical history of the patients admitted in the intensive care unit were analyzed, revisiting which had have red blood cell transfusion in the period between January 1st 2005 and December 31 2005. The study was accepted by the Research Ethics Committee – Comitê de Ética em Pesquisa (CEP) – of the University of South of Santa Catarina (UNISUL). RESULTS: The transfusion rate was 19,33, and the majority of the patients were of the male gender. Their age prevalence was of 60 years old or older. The mortality rate among patients who under went red blood cell transfusion died was of 38,22%. The transfusions criterias were low serum hemoglobin (78%) and the hemoglobin pre – transfusion was 8,11 g/dL. CONCLUSIONS: Politrauma and sepsis/sepsis chock were the pre diagnosis criteria. A low hemoglobin level is the main clinical criteria with average hemoglobin pre – transfusion was 8,11 g/dL.
Views0Abstract
Original ArticlesRed blood cells transfusion in intensive care unit
Rev Bras Ter Intensiva. 2009;21(4):391-397
DOI 10.1590/S0103-507X2009000400009
Views0See moreBACKGROUND: The anemia is a common problem upon admission of the patients in the intensive care unit being the red blood cell transfusion a frequent therapeutic. The causes of anemia in critical patients who under go red blood cell transfusion are several: acute loss of blood after trauma, gastrointestinal hemorrhage, surgery amongst others. Currently, few studies are available regarding the use of blood components in patients at intensive care unit. Although blood transfusions are frequent in intensive care unit, the optimized criteria for handling are not clearly defined, with no available guidelines. OBJECTIVES: To analyze the clinical indications of the use of the red blood cell in the intensive care unit. METHODS: The clinical history of the patients admitted in the intensive care unit were analyzed, revisiting which had have red blood cell transfusion in the period between January 1st 2005 and December 31 2005. The study was accepted by the Research Ethics Committee – Comitê de Ética em Pesquisa (CEP) – of the University of South of Santa Catarina (UNISUL). RESULTS: The transfusion rate was 19,33, and the majority of the patients were of the male gender. Their age prevalence was of 60 years old or older. The mortality rate among patients who under went red blood cell transfusion died was of 38,22%. The transfusions criterias were low serum hemoglobin (78%) and the hemoglobin pre – transfusion was 8,11 g/dL. CONCLUSIONS: Politrauma and sepsis/sepsis chock were the pre diagnosis criteria. A low hemoglobin level is the main clinical criteria with average hemoglobin pre – transfusion was 8,11 g/dL.
-
Original Articles
Profile and long-term prognosis of glucose tight control in intensive care unit – patients: a cohort study
Rev Bras Ter Intensiva. 2009;21(4):398-403
Abstract
Original ArticlesProfile and long-term prognosis of glucose tight control in intensive care unit – patients: a cohort study
Rev Bras Ter Intensiva. 2009;21(4):398-403
DOI 10.1590/S0103-507X2009000400010
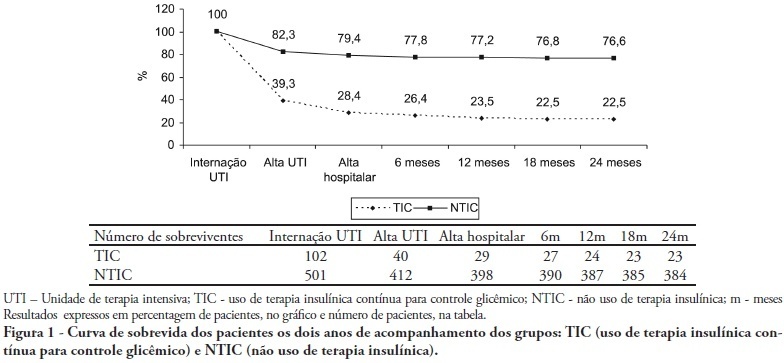
Views0See moreOBJECTIVES: Stress-induced hyperglycemia is frequent in critically ill patients and has been associated with increased mortality and morbidity (both in diabetic and non-diabetic patients). This study objective was to evaluate the profile and long-term prognosis of critically ill patients undergoing tight glucose-control. METHODS: Prospective cohort. All patients admitted to the intensive care unit over 1-year were enrolled. We analyzed demographic data, therapeutic intervention, and short- (during the stay) and long-term (2 years after discharge) mortality. The patients were categorized in 2 groups: tight glucose control and non-tight glucose-control, based on the unit staff decision. RESULTS: From the 603 enrolled patients, 102 (16.9%) underwent tight control (glucose <150 mg/dL) while 501 patients (83.1%) non-tight control. Patients in the TGC-group were more severely ill than those in the non-tight control group [APACHE II score (14 ± 3 versus 11 ± 4, P=0.04), SOFA (4.9 ± 3.2 versus 3.5 ± 3.4, P<0.001) and TISS-24h (25.7 ± 6.9 versus 21.1 ± 7.2, P< 0.001)]. The tight control group patients also had worse prognosis: [acute renal failure (51% versus 18.5%, P<0.001), critical illness neuropathy (16.7% versus 5.6%, P<0.001)] and increased mortality (during the ICU-stay [60.7% versus 17.7%, P<0.001] and within 2-years of the discharge [77.5% versus 23.4%; P<0.001]). CONCLUSION: Critically ill patients needing tight glucose control during the unit stay have more severe disease and have worse short and long-term prognosis.
Views0Abstract
Original ArticlesProfile and long-term prognosis of glucose tight control in intensive care unit – patients: a cohort study
Rev Bras Ter Intensiva. 2009;21(4):398-403
DOI 10.1590/S0103-507X2009000400010
Views0See moreOBJECTIVES: Stress-induced hyperglycemia is frequent in critically ill patients and has been associated with increased mortality and morbidity (both in diabetic and non-diabetic patients). This study objective was to evaluate the profile and long-term prognosis of critically ill patients undergoing tight glucose-control. METHODS: Prospective cohort. All patients admitted to the intensive care unit over 1-year were enrolled. We analyzed demographic data, therapeutic intervention, and short- (during the stay) and long-term (2 years after discharge) mortality. The patients were categorized in 2 groups: tight glucose control and non-tight glucose-control, based on the unit staff decision. RESULTS: From the 603 enrolled patients, 102 (16.9%) underwent tight control (glucose <150 mg/dL) while 501 patients (83.1%) non-tight control. Patients in the TGC-group were more severely ill than those in the non-tight control group [APACHE II score (14 ± 3 versus 11 ± 4, P=0.04), SOFA (4.9 ± 3.2 versus 3.5 ± 3.4, P<0.001) and TISS-24h (25.7 ± 6.9 versus 21.1 ± 7.2, P< 0.001)]. The tight control group patients also had worse prognosis: [acute renal failure (51% versus 18.5%, P<0.001), critical illness neuropathy (16.7% versus 5.6%, P<0.001)] and increased mortality (during the ICU-stay [60.7% versus 17.7%, P<0.001] and within 2-years of the discharge [77.5% versus 23.4%; P<0.001]). CONCLUSION: Critically ill patients needing tight glucose control during the unit stay have more severe disease and have worse short and long-term prognosis.
-
Review Articles
Controversies involving hypercapnic acidosis in acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2009;21(4):404-415
Abstract
Review ArticlesControversies involving hypercapnic acidosis in acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2009;21(4):404-415
DOI 10.1590/S0103-507X2009000400011
Views0See moreAcute respiratory distress syndrome is characterized by a diffuse inflammatory reaction of lung parenchyma induced by a direct insult to the alveolar epithelium (pulmonary acute respiratory distress syndrome) or an indirect lesion through the vascular endothelium (extrapulmonary acute respiratory distress syndrome). The main therapeutic strategy for acute respiratory distress syndrome is the ventilatory support. However, mechanical ventilation can worsen lung injury. In this context, a protective ventilatory strategy with low tidal volume has been proposed. The use of low tidal volume reduced the mortality rate of acute respiratory distress syndrome patients, but result in hypercapnic acidosis. The current article presents a review of literature on the effects of permissive hypercapnia in acute respiratory distress syndrome. To that end, we carried out a systematic review of scientific literature based on established criteria for documental analysis including clinical and experimental articles, using as data bases MedLine, LILACS, SciELO, PubMed, Cochrane. Hypercapnic acidosis has been considered by some authors as a modulator of the inflammatory process of acute respiratory distress syndrome. However, clinical and experimental studies on the effects of hypercapnic acidosis have shown controversial results. Therefore it is important to better elucidate the role of hypercapnic acidosis in acute respiratory distress syndrome.
Views0Abstract
Review ArticlesControversies involving hypercapnic acidosis in acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2009;21(4):404-415
DOI 10.1590/S0103-507X2009000400011
Views0See moreAcute respiratory distress syndrome is characterized by a diffuse inflammatory reaction of lung parenchyma induced by a direct insult to the alveolar epithelium (pulmonary acute respiratory distress syndrome) or an indirect lesion through the vascular endothelium (extrapulmonary acute respiratory distress syndrome). The main therapeutic strategy for acute respiratory distress syndrome is the ventilatory support. However, mechanical ventilation can worsen lung injury. In this context, a protective ventilatory strategy with low tidal volume has been proposed. The use of low tidal volume reduced the mortality rate of acute respiratory distress syndrome patients, but result in hypercapnic acidosis. The current article presents a review of literature on the effects of permissive hypercapnia in acute respiratory distress syndrome. To that end, we carried out a systematic review of scientific literature based on established criteria for documental analysis including clinical and experimental articles, using as data bases MedLine, LILACS, SciELO, PubMed, Cochrane. Hypercapnic acidosis has been considered by some authors as a modulator of the inflammatory process of acute respiratory distress syndrome. However, clinical and experimental studies on the effects of hypercapnic acidosis have shown controversial results. Therefore it is important to better elucidate the role of hypercapnic acidosis in acute respiratory distress syndrome.
-
Review Articles
Genetic susceptibility in acute lung injury and acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2009;21(4):416-424
Abstract
Review ArticlesGenetic susceptibility in acute lung injury and acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2009;21(4):416-424
DOI 10.1590/S0103-507X2009000400012
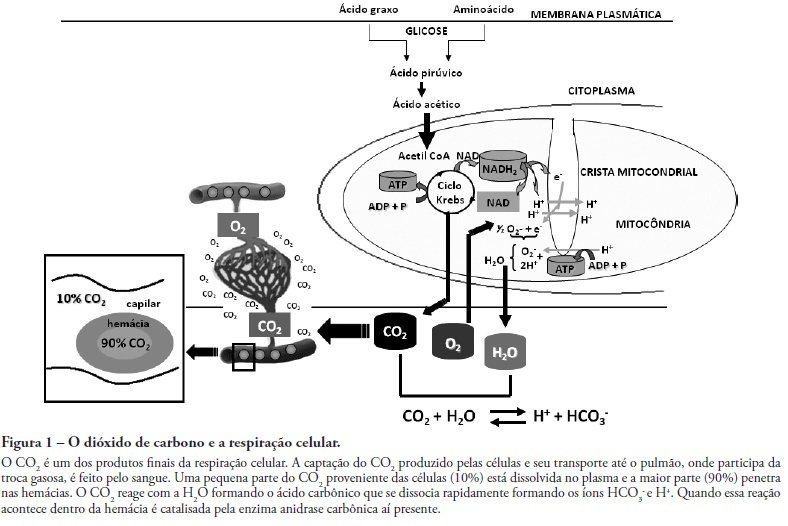
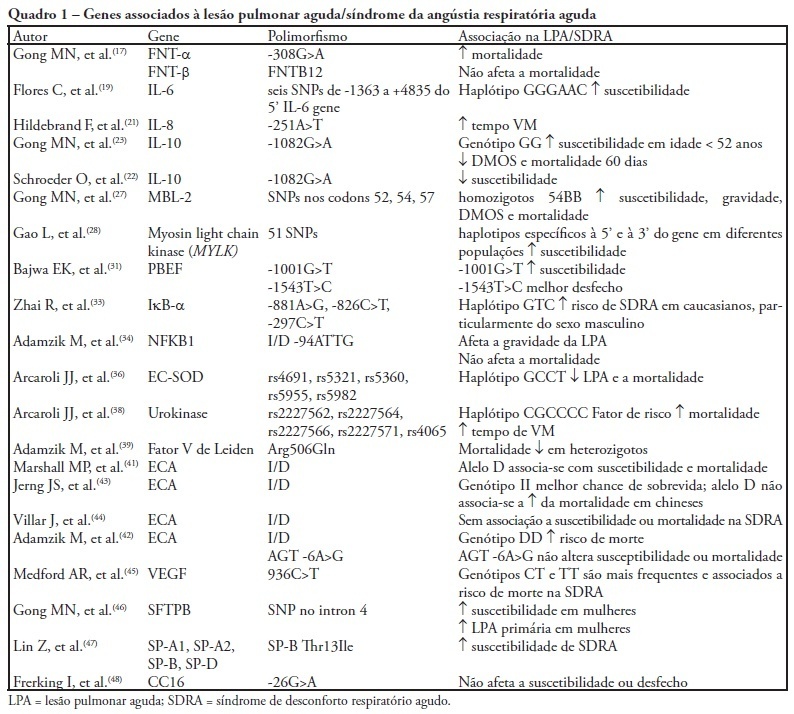
Views0See moreAcute lung injury and its most severe presentation, acute respiratory distress syndrome, are a common denominator for several diseases which can lead to exaggerated lung inflammation. In the last years this variability has been ascribed, at least partially, to genetic issues. This study aims to review the role of the main genes involved in acute lung injury and acute respiratory distress syndrome susceptibility, morbidity and mortality. By search on PubMed and LiLACS databases, using the key words acute lung injury, acute respiratory distress syndrome and adult acute respiratory distress syndrome in combination with genetic polymorphisms, 69 papers were selected, from which 38 were included in this review. Were also considered relevant articles extracted from the reference lists in the articles selected from the databases. Genetic polymorphisms are gene variations in at least 1% population. These gene variations may influence the inflammatory response mediators’ expression, directly affecting the susceptibility to acute lung injury, the intensity of lung parenchyma inflammation, the development clinical course and outcome. Association studies reproducible in large populations will definitely allow genomics to be included into the diagnostic and therapeutic armamentarium for acute lung injury/acute respiratory distress syndrome patients.
Views0Abstract
Review ArticlesGenetic susceptibility in acute lung injury and acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2009;21(4):416-424
DOI 10.1590/S0103-507X2009000400012
Views0See moreAcute lung injury and its most severe presentation, acute respiratory distress syndrome, are a common denominator for several diseases which can lead to exaggerated lung inflammation. In the last years this variability has been ascribed, at least partially, to genetic issues. This study aims to review the role of the main genes involved in acute lung injury and acute respiratory distress syndrome susceptibility, morbidity and mortality. By search on PubMed and LiLACS databases, using the key words acute lung injury, acute respiratory distress syndrome and adult acute respiratory distress syndrome in combination with genetic polymorphisms, 69 papers were selected, from which 38 were included in this review. Were also considered relevant articles extracted from the reference lists in the articles selected from the databases. Genetic polymorphisms are gene variations in at least 1% population. These gene variations may influence the inflammatory response mediators’ expression, directly affecting the susceptibility to acute lung injury, the intensity of lung parenchyma inflammation, the development clinical course and outcome. Association studies reproducible in large populations will definitely allow genomics to be included into the diagnostic and therapeutic armamentarium for acute lung injury/acute respiratory distress syndrome patients.
-
Review Articles
Understanding the PIRO concept: from theory to clinical practice – Part 1
Rev Bras Ter Intensiva. 2009;21(4):425-431
Abstract
Review ArticlesUnderstanding the PIRO concept: from theory to clinical practice – Part 1
Rev Bras Ter Intensiva. 2009;21(4):425-431
DOI 10.1590/S0103-507X2009000400013
Views0Despite recent advances in diagnosis and care of critically ill patients sepsis related mortality rate remains unacceptably high. Therefore, new methods of evaluation are necessary to provide an earlier and more accurate characterization of septic patients. Based on the (oncologic) TNM system, the PIRO concept was introduced as a new staging system for sepsis in order to assess risk and predict prognosis, with potential to assist in inclusion of patients in clinical studies and estimate the probability of response of patients to specific therapeutic interventions.
Keywords:Intensive careMultiple organ failureOutcome and process assessment (Health Care)PrognosisRisk assessmentSepsisSee moreViews0Abstract
Review ArticlesUnderstanding the PIRO concept: from theory to clinical practice – Part 1
Rev Bras Ter Intensiva. 2009;21(4):425-431
DOI 10.1590/S0103-507X2009000400013
Views0Despite recent advances in diagnosis and care of critically ill patients sepsis related mortality rate remains unacceptably high. Therefore, new methods of evaluation are necessary to provide an earlier and more accurate characterization of septic patients. Based on the (oncologic) TNM system, the PIRO concept was introduced as a new staging system for sepsis in order to assess risk and predict prognosis, with potential to assist in inclusion of patients in clinical studies and estimate the probability of response of patients to specific therapeutic interventions.
Keywords:Intensive careMultiple organ failureOutcome and process assessment (Health Care)PrognosisRisk assessmentSepsisSee more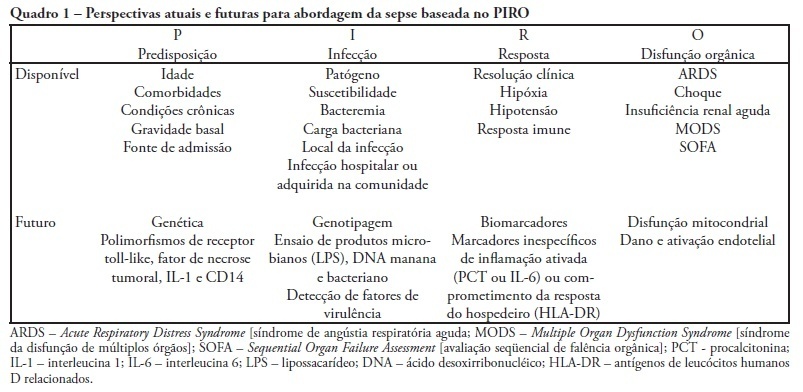
-
Review Articles
The morality of allocating resources to the elderly care in intensive care unit
Rev Bras Ter Intensiva. 2009;21(4):432-436
Abstract
Review ArticlesThe morality of allocating resources to the elderly care in intensive care unit
Rev Bras Ter Intensiva. 2009;21(4):432-436
DOI 10.1590/S0103-507X2009000400014
Views0See moreThe world is aging. In Brazil, and in several other countries in the world, changes in population’s age composition have been accompanied by an increase in demand for types of health care whose cost is high. Actually, some moral conflicts are arising from allocation of public resources for health, because the magnitude of social inequalities in health and limited resources require that priorities for public management are based on knowledge of the health situation and the impact of policies, programs, projects and actions on health. In this context, the intensive medicine, managers and physicians in intensive care are subject to moral conflicts, especially at the fair micro allocation resources for the elderly in the intensive care unit level. This paper attempts to review the situation of conflicts in the light of the tools of bioethics.
Views0Abstract
Review ArticlesThe morality of allocating resources to the elderly care in intensive care unit
Rev Bras Ter Intensiva. 2009;21(4):432-436
DOI 10.1590/S0103-507X2009000400014
Views0See moreThe world is aging. In Brazil, and in several other countries in the world, changes in population’s age composition have been accompanied by an increase in demand for types of health care whose cost is high. Actually, some moral conflicts are arising from allocation of public resources for health, because the magnitude of social inequalities in health and limited resources require that priorities for public management are based on knowledge of the health situation and the impact of policies, programs, projects and actions on health. In this context, the intensive medicine, managers and physicians in intensive care are subject to moral conflicts, especially at the fair micro allocation resources for the elderly in the intensive care unit level. This paper attempts to review the situation of conflicts in the light of the tools of bioethics.
-
Review Articles
Intensive care bedside echocardiography: true or a distant dream?
Rev Bras Ter Intensiva. 2009;21(4):437-445
Abstract
Review ArticlesIntensive care bedside echocardiography: true or a distant dream?
Rev Bras Ter Intensiva. 2009;21(4):437-445
DOI 10.1590/S0103-507X2009000400015
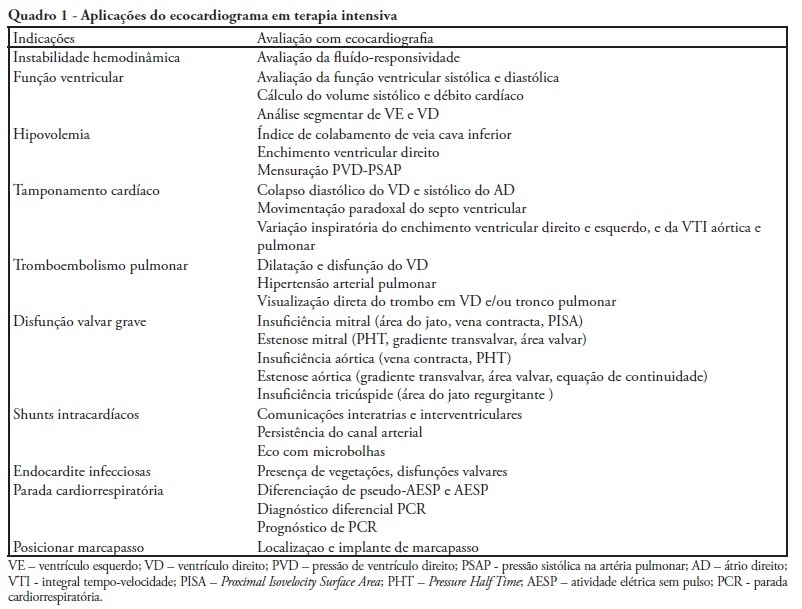
Views0See moreDuring the last few years, technological development and acquired experience advanced and the echocardiogram has become an important and useful tool in intensive care unit environment. Data obtained from semi quantitative Doppler echocardiography (transthoracic and transesophageal) evaluation has contributed to an appropriate patient monitoring and management. Echocardiography as a diagnostic, prognostic and monitoring method for fluid responsiveness assessment has become available nowadays since hand-carried ultrasound devices are portable and cheaper. Adequate training and development of appropriateness criteria for use of echocardiography in intensive care unit may lead to a standard use as a bedside tool.
Views0Abstract
Review ArticlesIntensive care bedside echocardiography: true or a distant dream?
Rev Bras Ter Intensiva. 2009;21(4):437-445
DOI 10.1590/S0103-507X2009000400015
Views0See moreDuring the last few years, technological development and acquired experience advanced and the echocardiogram has become an important and useful tool in intensive care unit environment. Data obtained from semi quantitative Doppler echocardiography (transthoracic and transesophageal) evaluation has contributed to an appropriate patient monitoring and management. Echocardiography as a diagnostic, prognostic and monitoring method for fluid responsiveness assessment has become available nowadays since hand-carried ultrasound devices are portable and cheaper. Adequate training and development of appropriateness criteria for use of echocardiography in intensive care unit may lead to a standard use as a bedside tool.
-
Review Articles
Motor physiotherapy in intensive care adult patients
Rev Bras Ter Intensiva. 2009;21(4):446-452
Abstract
Review ArticlesMotor physiotherapy in intensive care adult patients
Rev Bras Ter Intensiva. 2009;21(4):446-452
DOI 10.1590/S0103-507X2009000400016
Views0See moreThis study aimed to review the literature addressing motor physical therapy for intensive care unit adult patients. A literature search was conducted in the databases, PubMed, MedLine (International Literature and Health), LILACS (Latin American and Caribbean Health Sciences) and Cochrane between 1995 and December 2008 using the keywords: physical therapy, mobilization and intensive care unit. For comparison purposes we selected randomized controlled trials and prospective studies, addressing the subject motor physical therapy for intensive care unit adult patients. Pediatric and experimental studies, systematic reviews and meta-analysis were excluded. Of the 121 articles identified, only 4 met the inclusion criteria. Among these, three focused early motor physical therapy in patients with a range of diagnoses, showing that these patients left the bed and walked earlier, and stayed shorter both in the intensive care unit and hospital. Furthermore, patients on early motor physical therapy had shorter mechanical ventilation duration. Another paper compares the use of electrical stimulation associated with physical therapy in chronic obstructive pulmonary disease patients, showing increased muscle strength and shorter time for these patients bed to chair transference as compared with those only receiving physiotherapy. The risks of immobilization in mechanically ventilated critically ill patients are not fully understood. However, it is clear that the survivors show impaired quality of life due to persistent weakness and fatigue. Early mobilization is a new area, with little evidence so far. However, recent studies have confirmed that mechanically ventilated patients mobilization is safe and feasible, reducing both the intensive care unit and hospital stay. However, more studies are warranted to identify the exercise type, duration, intensity and impact for of early motor therapy in specific groups of patients.
Views0Abstract
Review ArticlesMotor physiotherapy in intensive care adult patients
Rev Bras Ter Intensiva. 2009;21(4):446-452
DOI 10.1590/S0103-507X2009000400016
Views0See moreThis study aimed to review the literature addressing motor physical therapy for intensive care unit adult patients. A literature search was conducted in the databases, PubMed, MedLine (International Literature and Health), LILACS (Latin American and Caribbean Health Sciences) and Cochrane between 1995 and December 2008 using the keywords: physical therapy, mobilization and intensive care unit. For comparison purposes we selected randomized controlled trials and prospective studies, addressing the subject motor physical therapy for intensive care unit adult patients. Pediatric and experimental studies, systematic reviews and meta-analysis were excluded. Of the 121 articles identified, only 4 met the inclusion criteria. Among these, three focused early motor physical therapy in patients with a range of diagnoses, showing that these patients left the bed and walked earlier, and stayed shorter both in the intensive care unit and hospital. Furthermore, patients on early motor physical therapy had shorter mechanical ventilation duration. Another paper compares the use of electrical stimulation associated with physical therapy in chronic obstructive pulmonary disease patients, showing increased muscle strength and shorter time for these patients bed to chair transference as compared with those only receiving physiotherapy. The risks of immobilization in mechanically ventilated critically ill patients are not fully understood. However, it is clear that the survivors show impaired quality of life due to persistent weakness and fatigue. Early mobilization is a new area, with little evidence so far. However, recent studies have confirmed that mechanically ventilated patients mobilization is safe and feasible, reducing both the intensive care unit and hospital stay. However, more studies are warranted to identify the exercise type, duration, intensity and impact for of early motor therapy in specific groups of patients.
-
Review Articles
Alveolar recruitment maneuver in mechanic ventilation pediatric intensive care unit children
Rev Bras Ter Intensiva. 2009;21(4):453-460
Abstract
Review ArticlesAlveolar recruitment maneuver in mechanic ventilation pediatric intensive care unit children
Rev Bras Ter Intensiva. 2009;21(4):453-460
DOI 10.1590/S0103-507X2009000400017
Views0See moreRecent changes were introduced in acute hypoxemic respiratory failure children ventilation methods. There are evidences that less aggressive ventilation strategies can improve severe pulmonary injury survival. Experimental trials evidenced a relationship between inappropriate ventilatory measures and delayed acute pulmonary injury improvement, or even worsening. From this, a protective ventilatory measure arises in combination with alveolar recruitment maneuver. This association is believed in clinical practice to determine importantly reduced morbidity and mortality as well as reduced mechanic ventilation-induced injuries. It is indicated for acute lung injury patients, generally from pneumonia or sepsis, with severe hypoxemia. Its main contraindications are homodynamic instability, pneumothorax and intracranial hypertension. Experimental trials showed beneficial maneuver effects on both oxygenation and alveolar collapse. Adult studies showed improved pulmonary function with hypoxemia reversion. In children, the maneuver lead to significant inspired oxygen fraction and alveolar collapse reductions, less oxygen dependency, improved pulmonary complacency, and reduced bronchopulmonary dysplasia. However, studies in children are limited. Additional investigation is warranted on this matter, and its clinical application evidence. A literature review was conducted based on textbooks and MEDLINE, Pubmed, Cochrane library, SciELO, and Ovid databases, from 1998 to 2009, both in Portuguese and English. Publications on alveolar recruitment maneuver both in adults and children, review articles, experimental and clinical trials were included using the key words: protective ventilatory strategy, alveolar recruitment maneuver, pediatrics and mechanic ventilation.
Views0Abstract
Review ArticlesAlveolar recruitment maneuver in mechanic ventilation pediatric intensive care unit children
Rev Bras Ter Intensiva. 2009;21(4):453-460
DOI 10.1590/S0103-507X2009000400017
Views0See moreRecent changes were introduced in acute hypoxemic respiratory failure children ventilation methods. There are evidences that less aggressive ventilation strategies can improve severe pulmonary injury survival. Experimental trials evidenced a relationship between inappropriate ventilatory measures and delayed acute pulmonary injury improvement, or even worsening. From this, a protective ventilatory measure arises in combination with alveolar recruitment maneuver. This association is believed in clinical practice to determine importantly reduced morbidity and mortality as well as reduced mechanic ventilation-induced injuries. It is indicated for acute lung injury patients, generally from pneumonia or sepsis, with severe hypoxemia. Its main contraindications are homodynamic instability, pneumothorax and intracranial hypertension. Experimental trials showed beneficial maneuver effects on both oxygenation and alveolar collapse. Adult studies showed improved pulmonary function with hypoxemia reversion. In children, the maneuver lead to significant inspired oxygen fraction and alveolar collapse reductions, less oxygen dependency, improved pulmonary complacency, and reduced bronchopulmonary dysplasia. However, studies in children are limited. Additional investigation is warranted on this matter, and its clinical application evidence. A literature review was conducted based on textbooks and MEDLINE, Pubmed, Cochrane library, SciELO, and Ovid databases, from 1998 to 2009, both in Portuguese and English. Publications on alveolar recruitment maneuver both in adults and children, review articles, experimental and clinical trials were included using the key words: protective ventilatory strategy, alveolar recruitment maneuver, pediatrics and mechanic ventilation.
-
Case Report
Tumoral pulmonary mass secondary to Schistosoma mansoni infection resembling neoplasia: case report
Rev Bras Ter Intensiva. 2009;21(4):461-464
Abstract
Case ReportTumoral pulmonary mass secondary to Schistosoma mansoni infection resembling neoplasia: case report
Rev Bras Ter Intensiva. 2009;21(4):461-464
DOI 10.1590/S0103-507X2009000400018
Views0See morePatients with chronic Schistosoma mansoni infection may feature a range of pulmonary symptoms and radiological findings. Eggs, and rarely adult worms, may passively enter the pulmonary circulation, usually via the portal system, where they may cause pulmonary inflammation, fibrosis, hypertension and cor pulmonale. A 25-year-old patient who lived in a schistosomiasis endemic area with a pulmonary mass suggestive of malignancy underwent exploratory thoracotomy. The mass was adherent, with no resection possibility. The lung-biopsy specimen evaluation showed several granulomas with Schistosoma mansoni eggs and hyperplasic connective tissue with no sign of malignancy. The patient had respiratory failure and hypotension immediately post-surgery. Specific treatment (praziquantel) and prednisone were given. The patient had pneumonia and septic shock. The patient was given antibiotics, vasopressors, mechanical ventilation and hemodialysis with no improvement, and subsequently died 28 days after the surgery.
Views0Abstract
Case ReportTumoral pulmonary mass secondary to Schistosoma mansoni infection resembling neoplasia: case report
Rev Bras Ter Intensiva. 2009;21(4):461-464
DOI 10.1590/S0103-507X2009000400018
Views0See morePatients with chronic Schistosoma mansoni infection may feature a range of pulmonary symptoms and radiological findings. Eggs, and rarely adult worms, may passively enter the pulmonary circulation, usually via the portal system, where they may cause pulmonary inflammation, fibrosis, hypertension and cor pulmonale. A 25-year-old patient who lived in a schistosomiasis endemic area with a pulmonary mass suggestive of malignancy underwent exploratory thoracotomy. The mass was adherent, with no resection possibility. The lung-biopsy specimen evaluation showed several granulomas with Schistosoma mansoni eggs and hyperplasic connective tissue with no sign of malignancy. The patient had respiratory failure and hypotension immediately post-surgery. Specific treatment (praziquantel) and prednisone were given. The patient had pneumonia and septic shock. The patient was given antibiotics, vasopressors, mechanical ventilation and hemodialysis with no improvement, and subsequently died 28 days after the surgery.
-
Erratum Rev Bras Ter Intensiva. 2009;21(4):465-465
Abstract
ErratumRev Bras Ter Intensiva. 2009;21(4):465-465
DOI 10.1590/S0103-507X2009000400019
Views0ERRATUM Regarding the article published on volume 21, number 3, pages 269-75 titled “Infections in patients submitted to hemodialysis: a systematic review,[…]See moreViews0Abstract
ErratumRev Bras Ter Intensiva. 2009;21(4):465-465
DOI 10.1590/S0103-507X2009000400019
Views0ERRATUM Regarding the article published on volume 21, number 3, pages 269-75 titled “Infections in patients submitted to hemodialysis: a systematic review,[…]See more
Volume Articles - Critical Care Science (CCS)
