-
Final balance and “welcome”
Rev Bras Ter Intensiva. 2010;22(1):1-2
-
New challenges…
Rev Bras Ter Intensiva. 2010;22(1):3-4
-
Original Articles
Closed system for blood sampling and transfusion in critically ill patients
Rev Bras Ter Intensiva. 2010;22(1):5-10
Abstract
Original ArticlesClosed system for blood sampling and transfusion in critically ill patients
Rev Bras Ter Intensiva. 2010;22(1):5-10
DOI 10.1590/S0103-507X2010000100003
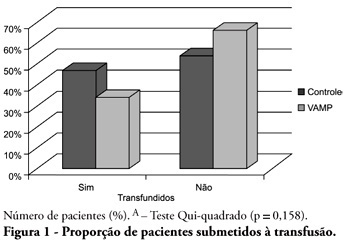
Views0See moreOBJECTIVE: Anemia is common in severely ill patients, and blood sampling plays a relevant causative role. Consequently, blood transfusions are frequent an related to several complications. Trying to reduce the transfusion-related risk, minimizing blood loss is mandatory. Thus, this work aimed to evaluate a closed blood sampling system as a strategy to spare unnecessary blood losses and transfusions. METHODS: This was a prospective, randomized, controlled, multicenter, 6 months, clinical trial. The patients were assigned to either VAMP (Venous Arterial Blood Management Protection) group, using a closed blood sampling system, or control group. The groups’ transfusion rate, as well as hemoglobin (Hb) and Hematocrit (Ht) changes were compared for 14 days. RESULTS: Were included 127 patients, 65 assigned to the control group, and 62 to VAMP. During the intensive care unit stay, both groups experienced both hemoglobin and hematocrit drops. However, when the final Ht and Hb were compared between the groups, a difference was identified with higher values in the VAMP group (p=0.03; p=0.006, respectively). No statistical difference was found for both groups transfusion rates, although the VAMP group had an absolute 12% blood transfusion reduction. CONCLUSION: The use of a closed blood sampling system was able to minimize blood count values changes, however failed to reduce transfusions rate.
Views0

Abstract
Original ArticlesClosed system for blood sampling and transfusion in critically ill patients
Rev Bras Ter Intensiva. 2010;22(1):5-10
DOI 10.1590/S0103-507X2010000100003
Views0See moreOBJECTIVE: Anemia is common in severely ill patients, and blood sampling plays a relevant causative role. Consequently, blood transfusions are frequent an related to several complications. Trying to reduce the transfusion-related risk, minimizing blood loss is mandatory. Thus, this work aimed to evaluate a closed blood sampling system as a strategy to spare unnecessary blood losses and transfusions. METHODS: This was a prospective, randomized, controlled, multicenter, 6 months, clinical trial. The patients were assigned to either VAMP (Venous Arterial Blood Management Protection) group, using a closed blood sampling system, or control group. The groups’ transfusion rate, as well as hemoglobin (Hb) and Hematocrit (Ht) changes were compared for 14 days. RESULTS: Were included 127 patients, 65 assigned to the control group, and 62 to VAMP. During the intensive care unit stay, both groups experienced both hemoglobin and hematocrit drops. However, when the final Ht and Hb were compared between the groups, a difference was identified with higher values in the VAMP group (p=0.03; p=0.006, respectively). No statistical difference was found for both groups transfusion rates, although the VAMP group had an absolute 12% blood transfusion reduction. CONCLUSION: The use of a closed blood sampling system was able to minimize blood count values changes, however failed to reduce transfusions rate.
-
Original Articles
Outcome of patients with cirrhosis admitted to intensive care
Rev Bras Ter Intensiva. 2010;22(1):11-18
Abstract
Original ArticlesOutcome of patients with cirrhosis admitted to intensive care
Rev Bras Ter Intensiva. 2010;22(1):11-18
DOI 10.1590/S0103-507X2010000100004
Views0See moreOBJECTIVE: This study aimed to evaluate the outcome of cirrhotic patients admitted to Intensive Care Unit. METHODS: We conducted a prospective cohort of cirrhotic patients admitted to two intensive care unit between June 1999 to September 2004. We collected demographic, comorbid conditions, diagnosis, vital signs, laboratory data, prognostic scores and evolution in intensive care unit and hospital. The patients were divided in groups: non surgical, non liver surgery, surgery for portal hypertension, liver surgery, liver transplantation, and urgent surgery. RESULTS: We studied 304 patients, which 190 (62.5%) were male. The median of age was 54 (47-61) years. The mortality rate in intensive care unit and hospital were 29.3 and 39.8%, respectively, more elevated than in the other patients admitted critically ill patients (19.6 and 28.3%; p<0.001). Non surgical patients and those submitted to urgent surgery presented high mortality rate in the intensive care unit (64.3 and 65.4%) and in the hospital (80.4 and 76.9%). The variables related to hospital mortality were [Odds ratio (confidence interval 95%)]: mean arterial pressure [0.985 (0.974-0.997)]; mechanical ventilation in the first 24 h [4.080 (1.990-8.364)]; confirmed infection in the first 24 h [7.899 (2.814-22.175)]; acute renal failure [5.509 (1.708-17.766)] and APACHE II score (points) [1.078 (1.017-1.143)]. CONCLUSIONS: Cirrhotic patients had higher mortality rate compared to non cirrhotic critically ill patients. Those admitted after urgent surgery and non surgical had higher mortality rate.
Views0Abstract
Original ArticlesOutcome of patients with cirrhosis admitted to intensive care
Rev Bras Ter Intensiva. 2010;22(1):11-18
DOI 10.1590/S0103-507X2010000100004
Views0See moreOBJECTIVE: This study aimed to evaluate the outcome of cirrhotic patients admitted to Intensive Care Unit. METHODS: We conducted a prospective cohort of cirrhotic patients admitted to two intensive care unit between June 1999 to September 2004. We collected demographic, comorbid conditions, diagnosis, vital signs, laboratory data, prognostic scores and evolution in intensive care unit and hospital. The patients were divided in groups: non surgical, non liver surgery, surgery for portal hypertension, liver surgery, liver transplantation, and urgent surgery. RESULTS: We studied 304 patients, which 190 (62.5%) were male. The median of age was 54 (47-61) years. The mortality rate in intensive care unit and hospital were 29.3 and 39.8%, respectively, more elevated than in the other patients admitted critically ill patients (19.6 and 28.3%; p<0.001). Non surgical patients and those submitted to urgent surgery presented high mortality rate in the intensive care unit (64.3 and 65.4%) and in the hospital (80.4 and 76.9%). The variables related to hospital mortality were [Odds ratio (confidence interval 95%)]: mean arterial pressure [0.985 (0.974-0.997)]; mechanical ventilation in the first 24 h [4.080 (1.990-8.364)]; confirmed infection in the first 24 h [7.899 (2.814-22.175)]; acute renal failure [5.509 (1.708-17.766)] and APACHE II score (points) [1.078 (1.017-1.143)]. CONCLUSIONS: Cirrhotic patients had higher mortality rate compared to non cirrhotic critically ill patients. Those admitted after urgent surgery and non surgical had higher mortality rate.
-
Original Articles
Risk factors for neonatal death in neonatal intensive care unit according to survival analysis
Rev Bras Ter Intensiva. 2010;22(1):19-26
Abstract
Original ArticlesRisk factors for neonatal death in neonatal intensive care unit according to survival analysis
Rev Bras Ter Intensiva. 2010;22(1):19-26
DOI 10.1590/S0103-507X2010000100005
Views0OBJECTIVE: To identify risk factors associated with death of infants admitted to neonatal intensive care unit of Taubaté University Hospital. METHODS: It is a longitudinal study with information obtained from medical records of newborns admitted to the neonatal intensive care unit of Taubaté University Hospital. Type of outcome, discharge or death, was dependent variable. The independent variables were maternal and gestational variables: maternal age, hypertension, diabetes, corticosteroid therapy and delivery; variables of the newborn: birth weight, gestation length, Apgar score in the first and fifth minutes of life, multiple birth, congenital malformations and sex; hospitalar variables: report of mechanical ventilation, positive pressure ventilation, reports of prolonged parenteral nutrition, sepsis, intubation, cardiac massage, phototherapy, hyaline membrane disease, oxygen and fraction of inspired oxygen. It was built a model in three hierarchical levels for the survival analysis by the Cox model; it was used the software Stata v9 and the final model contained variables with p <0.05. The risks were estimated by measure effect known as hazard ratio (HR) with confidence intervals of 95%. The newborns transferred during hospitalization to another service were excluded from the study. RESULTS: There were admitted during the study period 495 newborns, with 129 deaths (26.1%). In the final model, only the variables of steroid use (HR 1.64, 95% CI 1.02-2.70), malformation (HR 1.93, CI 95% 1,05-2,88), very low birth weight (HR 4.28, 95% CI 2,79-6,57) and Apgar scores lower than seven of no1 min (HR 1.87, 95% CI 1,19-2,93) and 5 min (HR 1.74, 95% CI 1,05-2,88) and the variables phototherapy (HR 0.34; 95% CI 0,22-0,53) and endotracheal intubation (HR 2.28, 95% CI 1 .41-3, 70). CONCLUSION: Factors related primarily to the newborn and the hospitalar internment (except therapy with corticosteroids) were identified as associated to mortality highlighting a possible protective factor of phototherapy and the risk of infants with very low birth weight.
Keywords:Congenital abnormalitiesInfantInfant mortalityIntensive careIntensive care unitslow birth weightneonatalSurvival analysisSee moreViews0Abstract
Original ArticlesRisk factors for neonatal death in neonatal intensive care unit according to survival analysis
Rev Bras Ter Intensiva. 2010;22(1):19-26
DOI 10.1590/S0103-507X2010000100005
Views0OBJECTIVE: To identify risk factors associated with death of infants admitted to neonatal intensive care unit of Taubaté University Hospital. METHODS: It is a longitudinal study with information obtained from medical records of newborns admitted to the neonatal intensive care unit of Taubaté University Hospital. Type of outcome, discharge or death, was dependent variable. The independent variables were maternal and gestational variables: maternal age, hypertension, diabetes, corticosteroid therapy and delivery; variables of the newborn: birth weight, gestation length, Apgar score in the first and fifth minutes of life, multiple birth, congenital malformations and sex; hospitalar variables: report of mechanical ventilation, positive pressure ventilation, reports of prolonged parenteral nutrition, sepsis, intubation, cardiac massage, phototherapy, hyaline membrane disease, oxygen and fraction of inspired oxygen. It was built a model in three hierarchical levels for the survival analysis by the Cox model; it was used the software Stata v9 and the final model contained variables with p <0.05. The risks were estimated by measure effect known as hazard ratio (HR) with confidence intervals of 95%. The newborns transferred during hospitalization to another service were excluded from the study. RESULTS: There were admitted during the study period 495 newborns, with 129 deaths (26.1%). In the final model, only the variables of steroid use (HR 1.64, 95% CI 1.02-2.70), malformation (HR 1.93, CI 95% 1,05-2,88), very low birth weight (HR 4.28, 95% CI 2,79-6,57) and Apgar scores lower than seven of no1 min (HR 1.87, 95% CI 1,19-2,93) and 5 min (HR 1.74, 95% CI 1,05-2,88) and the variables phototherapy (HR 0.34; 95% CI 0,22-0,53) and endotracheal intubation (HR 2.28, 95% CI 1 .41-3, 70). CONCLUSION: Factors related primarily to the newborn and the hospitalar internment (except therapy with corticosteroids) were identified as associated to mortality highlighting a possible protective factor of phototherapy and the risk of infants with very low birth weight.
Keywords:Congenital abnormalitiesInfantInfant mortalityIntensive careIntensive care unitslow birth weightneonatalSurvival analysisSee more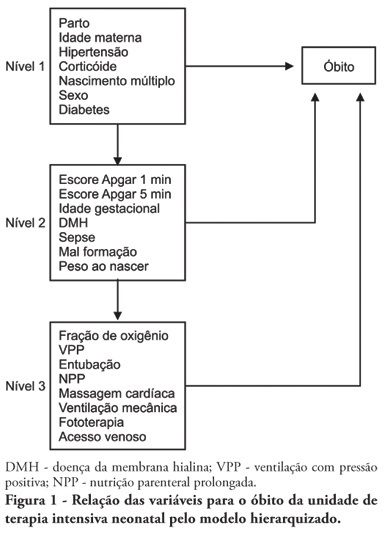
-
Original Articles Rev Bras Ter Intensiva. 2010;22(1):27-32
Abstract
Original ArticlesRev Bras Ter Intensiva. 2010;22(1):27-32
DOI 10.1590/S0103-507X2010000100006
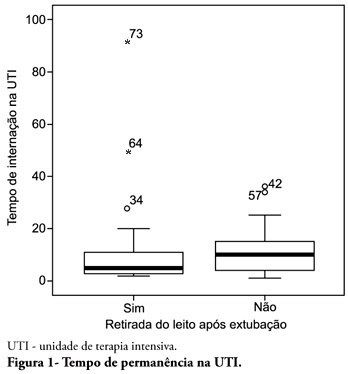
Views0See moreOBJECTIVE: To describe the withdrawal of the bed frequency in mechanic ventilation patients and its impact on mortality and length of stay in the intensive care unit. METHODS: This was a retrospective cohort study in mechanical ventilation patients. Clinical and epidemiological variables, withdrawal of bed related motor therapy, intensive care unit length of stay and mortality were evaluated. RESULTS: We studied 91 patients, mean age of 62.5± 18.8 years, predominantly female (52%) and mean intensive care unit length of stay of 07 days (95% CI, 8-13 days). Considering the withdrawal of the bed or not, no difference was observed between groups regarding length of stay in intensive care unit. Patients who were withdrawn of bed had a lower clinical severity. Their mortality rate was 29.7%. The not withdrawn of bed group had higher both actual and expected mortality. CONCLUSIONS: Patients withdrawn of bed following mechanical ventilation discontinuation showed lower mortality. It is suggested that early intensive care unit mobilization and withdrawal of bed should be stimulated.
Views0Abstract
Original ArticlesRev Bras Ter Intensiva. 2010;22(1):27-32
DOI 10.1590/S0103-507X2010000100006
Views0See moreOBJECTIVE: To describe the withdrawal of the bed frequency in mechanic ventilation patients and its impact on mortality and length of stay in the intensive care unit. METHODS: This was a retrospective cohort study in mechanical ventilation patients. Clinical and epidemiological variables, withdrawal of bed related motor therapy, intensive care unit length of stay and mortality were evaluated. RESULTS: We studied 91 patients, mean age of 62.5± 18.8 years, predominantly female (52%) and mean intensive care unit length of stay of 07 days (95% CI, 8-13 days). Considering the withdrawal of the bed or not, no difference was observed between groups regarding length of stay in intensive care unit. Patients who were withdrawn of bed had a lower clinical severity. Their mortality rate was 29.7%. The not withdrawn of bed group had higher both actual and expected mortality. CONCLUSIONS: Patients withdrawn of bed following mechanical ventilation discontinuation showed lower mortality. It is suggested that early intensive care unit mobilization and withdrawal of bed should be stimulated.
-
Original Articles
Comparison and effects of two different airway occlusion times during measurement of maximal inspiratory pressure in adult intensive care unit neurological patients
Rev Bras Ter Intensiva. 2010;22(1):33-39
Abstract
Original ArticlesComparison and effects of two different airway occlusion times during measurement of maximal inspiratory pressure in adult intensive care unit neurological patients
Rev Bras Ter Intensiva. 2010;22(1):33-39
DOI 10.1590/S0103-507X2010000100007
Views0See moreOBJECTIVE: To verify if the maximal inspiratory pressure values with 40 seconds occlusion time are greater than with the 20 seconds occlusion time, and the impacts on the following patient’s physiological variables: respiratory rate, pulse oxygen saturation, heart rate and blood pressure, before and after the measurements. METHODS: This was a transversal prospective randomized study. Fifty-one patients underwent maximal inspiratory pressure measurement, measured by one single investigator. The manometer was calibrated before each measurement, and then connected to the adapter and this to the unidirectional valve inspiratory branch for 20 or 40 seconds. RESULTS: The values with 40 seconds occlusion (57.6 ± 23.4 cmH2O) were significantly higher than the measurements taken with 20 seconds occlusion (40.5 ± 23.4 cmH2O; p=0.0001). The variables changes between the before and after measurement respiratory and hemodynamic parameters monitoring showed: heart rate variation for the 20 seconds occlusion 5.13 ± 8.56 beats per minute and after 40 seconds occlusion 7.94 ± 12.05 beats per minute (p = 0.053), versus baseline. The mean blood pressure change for 20 seconds occlusion was 9.29 ± 13.35 mmHg and for 40 seconds occlusion 15.52 ± 2.91 mmHg (p=0.021). The oxygen saturation change for 20 seconds occlusion was 1.66 ± 12.66%, and for 40 seconds 4.21 ± 5.53% (p=0.0001). The respiratory rate change for 20 seconds occlusion was 6.68 ± 12.66 movements per minute and for 40 seconds 6.94 ± 6.01 (p=0.883). CONCLUSION: The measurement of maximal inspiratory pressure using a longer occlusion (40 seconds) produced higher values, without triggering clinically significant stress according to the selected variables.
Views0Abstract
Original ArticlesComparison and effects of two different airway occlusion times during measurement of maximal inspiratory pressure in adult intensive care unit neurological patients
Rev Bras Ter Intensiva. 2010;22(1):33-39
DOI 10.1590/S0103-507X2010000100007
Views0See moreOBJECTIVE: To verify if the maximal inspiratory pressure values with 40 seconds occlusion time are greater than with the 20 seconds occlusion time, and the impacts on the following patient’s physiological variables: respiratory rate, pulse oxygen saturation, heart rate and blood pressure, before and after the measurements. METHODS: This was a transversal prospective randomized study. Fifty-one patients underwent maximal inspiratory pressure measurement, measured by one single investigator. The manometer was calibrated before each measurement, and then connected to the adapter and this to the unidirectional valve inspiratory branch for 20 or 40 seconds. RESULTS: The values with 40 seconds occlusion (57.6 ± 23.4 cmH2O) were significantly higher than the measurements taken with 20 seconds occlusion (40.5 ± 23.4 cmH2O; p=0.0001). The variables changes between the before and after measurement respiratory and hemodynamic parameters monitoring showed: heart rate variation for the 20 seconds occlusion 5.13 ± 8.56 beats per minute and after 40 seconds occlusion 7.94 ± 12.05 beats per minute (p = 0.053), versus baseline. The mean blood pressure change for 20 seconds occlusion was 9.29 ± 13.35 mmHg and for 40 seconds occlusion 15.52 ± 2.91 mmHg (p=0.021). The oxygen saturation change for 20 seconds occlusion was 1.66 ± 12.66%, and for 40 seconds 4.21 ± 5.53% (p=0.0001). The respiratory rate change for 20 seconds occlusion was 6.68 ± 12.66 movements per minute and for 40 seconds 6.94 ± 6.01 (p=0.883). CONCLUSION: The measurement of maximal inspiratory pressure using a longer occlusion (40 seconds) produced higher values, without triggering clinically significant stress according to the selected variables.
-
Original Articles
Effects of manual hyperinflation maneuver associated with positive end expiratory pressure in patients within coronary artery bypass grafting
Rev Bras Ter Intensiva. 2010;22(1):40-46
Abstract
Original ArticlesEffects of manual hyperinflation maneuver associated with positive end expiratory pressure in patients within coronary artery bypass grafting
Rev Bras Ter Intensiva. 2010;22(1):40-46
DOI 10.1590/S0103-507X2010000100008
Views1OBJECTIVE: To verify the effects of manual hyperinflation maneuver associated with positive end expiratory pressure in coronary artery bypass grafting patients. METHODS: This was a randomized trial, conducted from August 2007 to July 2008 in the intensive care unit of the Hospital Luterano (ULBRA). The patients were divided in the groups intervention – with manual hyperinflation plus positive end expiratory pressure – and controlThe ventilatory variables were measured before and after the manual hyperinflation. The t Student’s test was used for independent and paired samples as well as Fisher’s exact test and McNemar’s Chi-square test with 0.05 significance level. RESULTS: Eighteen patients were included. The mean age was 64± 11 years and 55.6% were female. The inspired tidal volume was 594± 112ml in the intervention group and 487± 51ml in the control group (p=0.024) and the expired tidal volume was 598± 105ml in the intervention group and 490± 58ml in the control group (p=0.02). The mean pre-maneuver static pulmonary compliance in the intervention group was 41.6± 12.1 ml/cmH2O and post maneuver it was 47.4± 16.6 ml/cmH2O (p=0.03). There was no significant between groups difference in the following variables: oxygen peripheral saturation, oxygen arterial pressure, extubation time and radiological changes. CONCLUSION: The results show that the manual hyperinflation associated with positive end expiratory pressure maneuver trends to promote increased lung volumes and static compliance, however these findings require further confirmation.
Keywords:Breathing exercisesMyocardial revascularizationPhysical therapy modalitiesPositive pressure respirationRehabilitationRespiration, artificialRespiratory therapySee moreViews1Abstract
Original ArticlesEffects of manual hyperinflation maneuver associated with positive end expiratory pressure in patients within coronary artery bypass grafting
Rev Bras Ter Intensiva. 2010;22(1):40-46
DOI 10.1590/S0103-507X2010000100008
Views1OBJECTIVE: To verify the effects of manual hyperinflation maneuver associated with positive end expiratory pressure in coronary artery bypass grafting patients. METHODS: This was a randomized trial, conducted from August 2007 to July 2008 in the intensive care unit of the Hospital Luterano (ULBRA). The patients were divided in the groups intervention – with manual hyperinflation plus positive end expiratory pressure – and controlThe ventilatory variables were measured before and after the manual hyperinflation. The t Student’s test was used for independent and paired samples as well as Fisher’s exact test and McNemar’s Chi-square test with 0.05 significance level. RESULTS: Eighteen patients were included. The mean age was 64± 11 years and 55.6% were female. The inspired tidal volume was 594± 112ml in the intervention group and 487± 51ml in the control group (p=0.024) and the expired tidal volume was 598± 105ml in the intervention group and 490± 58ml in the control group (p=0.02). The mean pre-maneuver static pulmonary compliance in the intervention group was 41.6± 12.1 ml/cmH2O and post maneuver it was 47.4± 16.6 ml/cmH2O (p=0.03). There was no significant between groups difference in the following variables: oxygen peripheral saturation, oxygen arterial pressure, extubation time and radiological changes. CONCLUSION: The results show that the manual hyperinflation associated with positive end expiratory pressure maneuver trends to promote increased lung volumes and static compliance, however these findings require further confirmation.
Keywords:Breathing exercisesMyocardial revascularizationPhysical therapy modalitiesPositive pressure respirationRehabilitationRespiration, artificialRespiratory therapySee more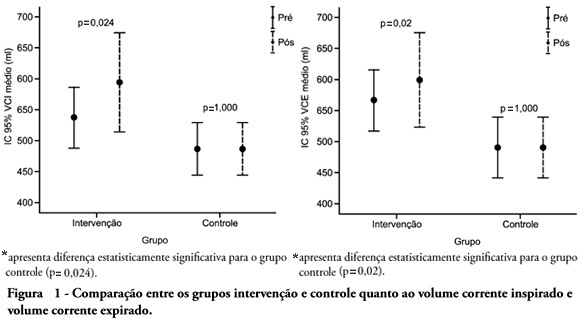
-
Original Articles
Epidemiological profile of patients with tracheotomy in a referral public hospital intensive care unit in Belo Horizonte
Rev Bras Ter Intensiva. 2010;22(1):47-52
Abstract
Original ArticlesEpidemiological profile of patients with tracheotomy in a referral public hospital intensive care unit in Belo Horizonte
Rev Bras Ter Intensiva. 2010;22(1):47-52
DOI 10.1590/S0103-507X2010000100009
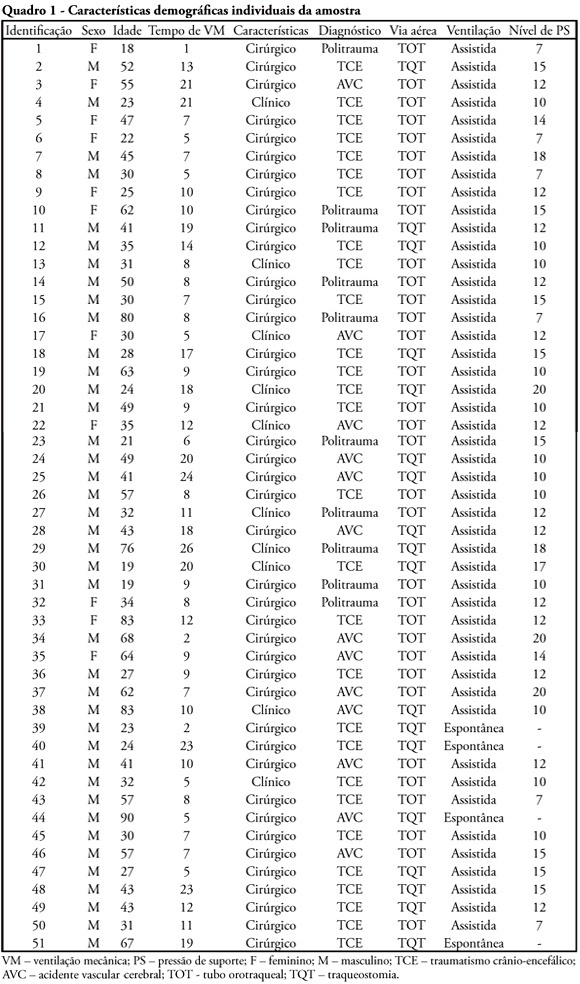
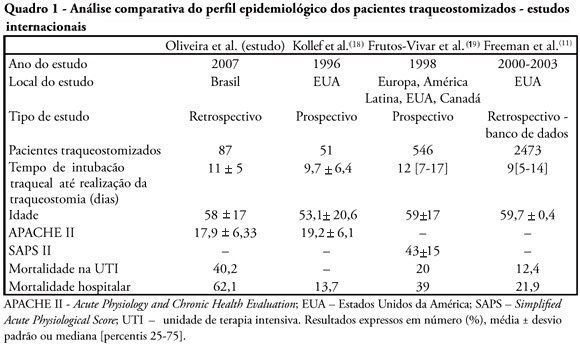
Views0See moreOBJECTIVES: Tracheostomy is a common procedure in intensive care unit to promote mechanical ventilation weaning. Despite tracheostomy is increasingly used there is no agreement of actual clinical practice of tracheostomy in different groups of patients in our environment. Objective of this study was to evaluate the epidemiological profile and outcomes of patients with tracheostomy at a clinical-surgical intensive care unit and compare this profile with the current literature. METHODS: Retrospective descriptive study through review of medical records and quality control database of “QuaTI” (Qualidade em Terapia Intensiva) of 87 patients with tracheostomy at Santa Casa de Belo Horizonte intensive care unit in 2007. We studied variables related to evolution aspects. RESULTS: The clinical and epidemiological analysis of the 87 patients showed: mean age 58 ± 17 years, mean Acute Physiology and Chronic Health Evaluation – APACHE II 18 ± 6, mean time of orotracheal intubation before tracheostomy of 11.17 ± 4.78 days. Intensive care unit mortality was 40.2% (35/87 patients), ward mortality was 36.5% (19/52) and overall hospital mortality 62.1% (54/87). Mean age of patients who died at intensive care unit (65 + 17 years) was greater than who were discharged to ward (53 ± 16 years) p = 0.003. Mean age of who died in hospital (intensive care unit and ward) (62 ± 17 years) was also higher than survivors (52 ± 16 years) p = 0.008. Old age (> 65 years) was related to intensive care unit mortality (OR 2.874, CI 1.165 a 7.088 p = 0.020) and also related to the overall hospital mortality (OR 3.202, CI 1.188 a 8.628 p = 0.019). There were not others variables related to mortality in this sample. CONCLUSIONS: The epidemiological profile of patients who underwent tracheotomy in the intensive care unit showed high mortality rate when compared to international series. Senility was related to worse outcome in these patients. Other issues were not related mortality in this group.
Views0Abstract
Original ArticlesEpidemiological profile of patients with tracheotomy in a referral public hospital intensive care unit in Belo Horizonte
Rev Bras Ter Intensiva. 2010;22(1):47-52
DOI 10.1590/S0103-507X2010000100009
Views0See moreOBJECTIVES: Tracheostomy is a common procedure in intensive care unit to promote mechanical ventilation weaning. Despite tracheostomy is increasingly used there is no agreement of actual clinical practice of tracheostomy in different groups of patients in our environment. Objective of this study was to evaluate the epidemiological profile and outcomes of patients with tracheostomy at a clinical-surgical intensive care unit and compare this profile with the current literature. METHODS: Retrospective descriptive study through review of medical records and quality control database of “QuaTI” (Qualidade em Terapia Intensiva) of 87 patients with tracheostomy at Santa Casa de Belo Horizonte intensive care unit in 2007. We studied variables related to evolution aspects. RESULTS: The clinical and epidemiological analysis of the 87 patients showed: mean age 58 ± 17 years, mean Acute Physiology and Chronic Health Evaluation – APACHE II 18 ± 6, mean time of orotracheal intubation before tracheostomy of 11.17 ± 4.78 days. Intensive care unit mortality was 40.2% (35/87 patients), ward mortality was 36.5% (19/52) and overall hospital mortality 62.1% (54/87). Mean age of patients who died at intensive care unit (65 + 17 years) was greater than who were discharged to ward (53 ± 16 years) p = 0.003. Mean age of who died in hospital (intensive care unit and ward) (62 ± 17 years) was also higher than survivors (52 ± 16 years) p = 0.008. Old age (> 65 years) was related to intensive care unit mortality (OR 2.874, CI 1.165 a 7.088 p = 0.020) and also related to the overall hospital mortality (OR 3.202, CI 1.188 a 8.628 p = 0.019). There were not others variables related to mortality in this sample. CONCLUSIONS: The epidemiological profile of patients who underwent tracheotomy in the intensive care unit showed high mortality rate when compared to international series. Senility was related to worse outcome in these patients. Other issues were not related mortality in this group.
-
Original Articles
Intensive care physicians’ attitudes and perceptions on nutrition therapy: a web-based survey
Rev Bras Ter Intensiva. 2010;22(1):53-63
Abstract
Original ArticlesIntensive care physicians’ attitudes and perceptions on nutrition therapy: a web-based survey
Rev Bras Ter Intensiva. 2010;22(1):53-63
DOI 10.1590/S0103-507X2010000100010
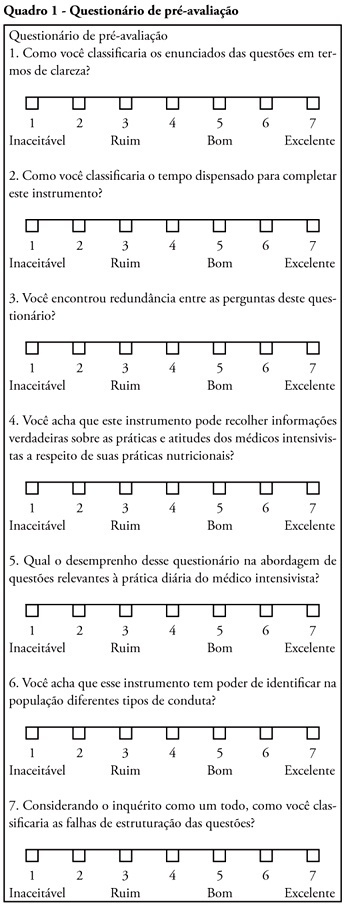
Views0See moreOBJECTIVE: Nutritional therapy is an important element in critical ill patient care. Although recognized as specialty, multidisciplinary teams in nutrition support are scarce in our country. Possibly, nutrition support therapy is applied by intensive care physicians and this may vary. The aim of the study is describe these specialists perceptions about theirs attitudes in enteral nutrition support. METHODS: A questionnaire was elaborated in an on-line platform. After pre-validation, it was sent by electronic mail to intensivists. In 30 days answers were collected, considering only the full-filled questionnaires. RESULTS: One hundred an fourteen forms were returned, 112 were analyzed. The responders were localized at majority in southeastern region. About beggining of nutritional support, the majority of answers reflect perceptions in accord to specialists societies recommendations. The responders’ perception the frequent utilization of assistentials protocols in nutrition care. After support beginning, the responders perceptions about theirs participation in changes in therapeutic plan seems to be lower. The self-knowledge about the theme among the responders was 6.0 (arithmetic media) in a 1 to 10 scale. CONCLUSIONS: More studies are necessary to evaluate nutritional support practices among intensive care physicians. Alternatives to on-line platform should be considered. Possibly, intensive care physicians do better in the initial phases of enteral support than in continuity of care. Intensive care physicians knowledge about the issue is suboptimal.
Views0Abstract
Original ArticlesIntensive care physicians’ attitudes and perceptions on nutrition therapy: a web-based survey
Rev Bras Ter Intensiva. 2010;22(1):53-63
DOI 10.1590/S0103-507X2010000100010
Views0See moreOBJECTIVE: Nutritional therapy is an important element in critical ill patient care. Although recognized as specialty, multidisciplinary teams in nutrition support are scarce in our country. Possibly, nutrition support therapy is applied by intensive care physicians and this may vary. The aim of the study is describe these specialists perceptions about theirs attitudes in enteral nutrition support. METHODS: A questionnaire was elaborated in an on-line platform. After pre-validation, it was sent by electronic mail to intensivists. In 30 days answers were collected, considering only the full-filled questionnaires. RESULTS: One hundred an fourteen forms were returned, 112 were analyzed. The responders were localized at majority in southeastern region. About beggining of nutritional support, the majority of answers reflect perceptions in accord to specialists societies recommendations. The responders’ perception the frequent utilization of assistentials protocols in nutrition care. After support beginning, the responders perceptions about theirs participation in changes in therapeutic plan seems to be lower. The self-knowledge about the theme among the responders was 6.0 (arithmetic media) in a 1 to 10 scale. CONCLUSIONS: More studies are necessary to evaluate nutritional support practices among intensive care physicians. Alternatives to on-line platform should be considered. Possibly, intensive care physicians do better in the initial phases of enteral support than in continuity of care. Intensive care physicians knowledge about the issue is suboptimal.
-
Review Articles
Understanding the PIRO concept: from theory to clinical practice – part 2
Rev Bras Ter Intensiva. 2010;22(1):64-68
Abstract
Review ArticlesUnderstanding the PIRO concept: from theory to clinical practice – part 2
Rev Bras Ter Intensiva. 2010;22(1):64-68
DOI 10.1590/S0103-507X2010000100011
Views0A sepsis staging system focused on predisposition, insult, host response and organ failure may provide a useful basis for risk stratification. Knowledge on interactions among predisposing factors, insult characteristics and host response might help us to improve our understanding on sepsis pathophysiology and allow more individual therapeutic approach. Recent clinical studies documented the clinical importance of PIRO approach for severity stratification in septic patients in intensive care unit, and also for specific conditions such as community acquired pneumonia and ventilator associated pneumonia , with a good performance for outcome prediction. In this review we describe how this new concept can be used in clinical practice and provide some insights on its usefulness to facilitate the stratification and potential for enrollment in clinical trials of sepsis therapies.
Keywords:Intensive careMultiple organ failureOutcome and process assessmentPrognosisRisk assessmentSepsisSee moreViews0Abstract
Review ArticlesUnderstanding the PIRO concept: from theory to clinical practice – part 2
Rev Bras Ter Intensiva. 2010;22(1):64-68
DOI 10.1590/S0103-507X2010000100011
Views0A sepsis staging system focused on predisposition, insult, host response and organ failure may provide a useful basis for risk stratification. Knowledge on interactions among predisposing factors, insult characteristics and host response might help us to improve our understanding on sepsis pathophysiology and allow more individual therapeutic approach. Recent clinical studies documented the clinical importance of PIRO approach for severity stratification in septic patients in intensive care unit, and also for specific conditions such as community acquired pneumonia and ventilator associated pneumonia , with a good performance for outcome prediction. In this review we describe how this new concept can be used in clinical practice and provide some insights on its usefulness to facilitate the stratification and potential for enrollment in clinical trials of sepsis therapies.
Keywords:Intensive careMultiple organ failureOutcome and process assessmentPrognosisRisk assessmentSepsisSee more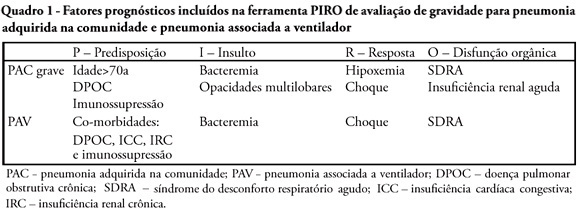
-
Review Articles
Topical anesthesia in preterm neonate: a reflection on the underutilization in clinical practice
Rev Bras Ter Intensiva. 2010;22(1):69-76
Abstract
Review ArticlesTopical anesthesia in preterm neonate: a reflection on the underutilization in clinical practice
Rev Bras Ter Intensiva. 2010;22(1):69-76
DOI 10.1590/S0103-507X2010000100012
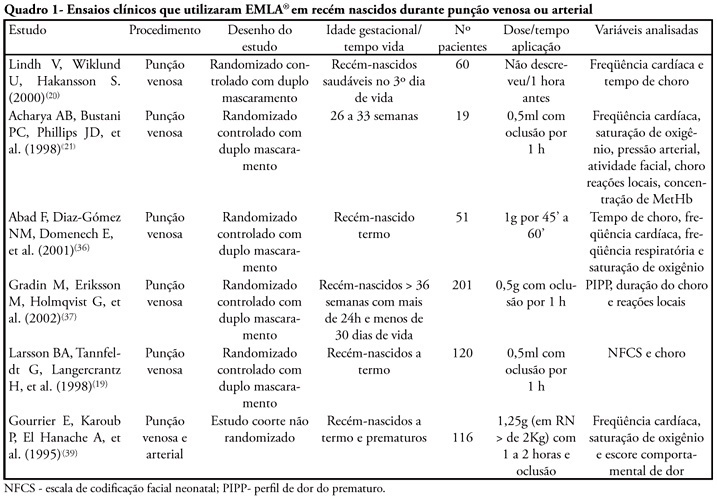
Views0See morePremature neonates are customarily submitted to invasive painful procedures during their stay in NICUs that are necessary to maintain their clinically stability. Topical anesthesia is a good option to be considered in the treatment of interventions that lead to mild to moderate pain and has the advantage of no systemic effects. In Brazil the most known topical anesthetic available for use is the eutectic mixture of local anesthetics (EMLA® cream). Its efficacy in the treatment of cutaneous painful procedures is well established for children and adults. Its utilization in neonates has been investigated also due to the risk to develop methemoglobinemia. The procedures in which topical anesthesia would be well indicated are those related to mild to moderate pain like: arterial and venous punction, hell lance puncture, lumbar puncture and percutaneous central catheter installation. The studies in the literature have so far lead to different conclusions, mainly depending on the type of the procedure and also due to the use of very different methodologies. The possibility of a direct pain evaluation may decrease the methodological bias leading to a more accurate evaluation of the efficacy of the topical anesthesia and also allowing comparisons among the indirect pain measures used so far.
Views0Abstract
Review ArticlesTopical anesthesia in preterm neonate: a reflection on the underutilization in clinical practice
Rev Bras Ter Intensiva. 2010;22(1):69-76
DOI 10.1590/S0103-507X2010000100012
Views0See morePremature neonates are customarily submitted to invasive painful procedures during their stay in NICUs that are necessary to maintain their clinically stability. Topical anesthesia is a good option to be considered in the treatment of interventions that lead to mild to moderate pain and has the advantage of no systemic effects. In Brazil the most known topical anesthetic available for use is the eutectic mixture of local anesthetics (EMLA® cream). Its efficacy in the treatment of cutaneous painful procedures is well established for children and adults. Its utilization in neonates has been investigated also due to the risk to develop methemoglobinemia. The procedures in which topical anesthesia would be well indicated are those related to mild to moderate pain like: arterial and venous punction, hell lance puncture, lumbar puncture and percutaneous central catheter installation. The studies in the literature have so far lead to different conclusions, mainly depending on the type of the procedure and also due to the use of very different methodologies. The possibility of a direct pain evaluation may decrease the methodological bias leading to a more accurate evaluation of the efficacy of the topical anesthesia and also allowing comparisons among the indirect pain measures used so far.
-
Review Articles
Post-traumatic stress disorder in intensive care unit patients
Rev Bras Ter Intensiva. 2010;22(1):77-84
Abstract
Review ArticlesPost-traumatic stress disorder in intensive care unit patients
Rev Bras Ter Intensiva. 2010;22(1):77-84
DOI 10.1590/S0103-507X2010000100013
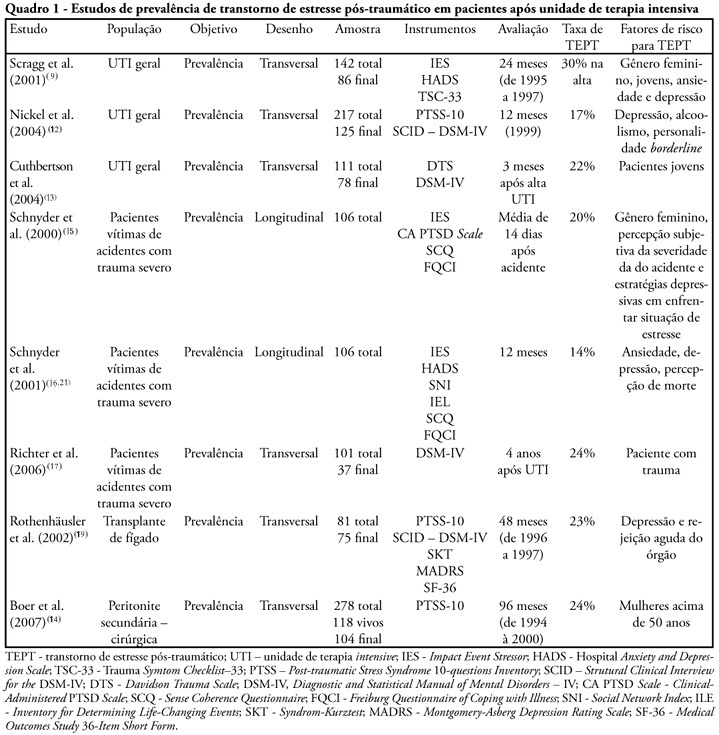
Views1See morePost-traumatic stress disorder has been detected in patients after treatment in intensive care unit. The main goal of this study is to review the psychological aspects and therapeutic interventions on those patients after their treatment on intensive care unit. Thirty eight articles have been included. The prevalence of post-traumatic stress disorder has varied from 17% up to 30% and the incidence from 14% to 24%. The risk factors were: previous anxiety historic, depression or panic, having delusional traumatic memories (derived from psychic formations as dreams and delirium), belief effects, depressive behavior, stressing experiences and mechanical ventilation. High doses of opiates, symptoms caused by sedation or analgesia reduction and the use of lorazepam were related with the increase of delirium and delusional memory. The disorder sintomatology can be reduced with hydrocortisone administration, with daily sedation interruption. No other effectiveness psychological intervention study was found.
Views1Abstract
Review ArticlesPost-traumatic stress disorder in intensive care unit patients
Rev Bras Ter Intensiva. 2010;22(1):77-84
DOI 10.1590/S0103-507X2010000100013
Views1See morePost-traumatic stress disorder has been detected in patients after treatment in intensive care unit. The main goal of this study is to review the psychological aspects and therapeutic interventions on those patients after their treatment on intensive care unit. Thirty eight articles have been included. The prevalence of post-traumatic stress disorder has varied from 17% up to 30% and the incidence from 14% to 24%. The risk factors were: previous anxiety historic, depression or panic, having delusional traumatic memories (derived from psychic formations as dreams and delirium), belief effects, depressive behavior, stressing experiences and mechanical ventilation. High doses of opiates, symptoms caused by sedation or analgesia reduction and the use of lorazepam were related with the increase of delirium and delusional memory. The disorder sintomatology can be reduced with hydrocortisone administration, with daily sedation interruption. No other effectiveness psychological intervention study was found.
-
Review Articles
Effects of motor physical therapy in critically ill patients: literature review
Rev Bras Ter Intensiva. 2010;22(1):85-91
Abstract
Review ArticlesEffects of motor physical therapy in critically ill patients: literature review
Rev Bras Ter Intensiva. 2010;22(1):85-91
DOI 10.1590/S0103-507X2010000100014
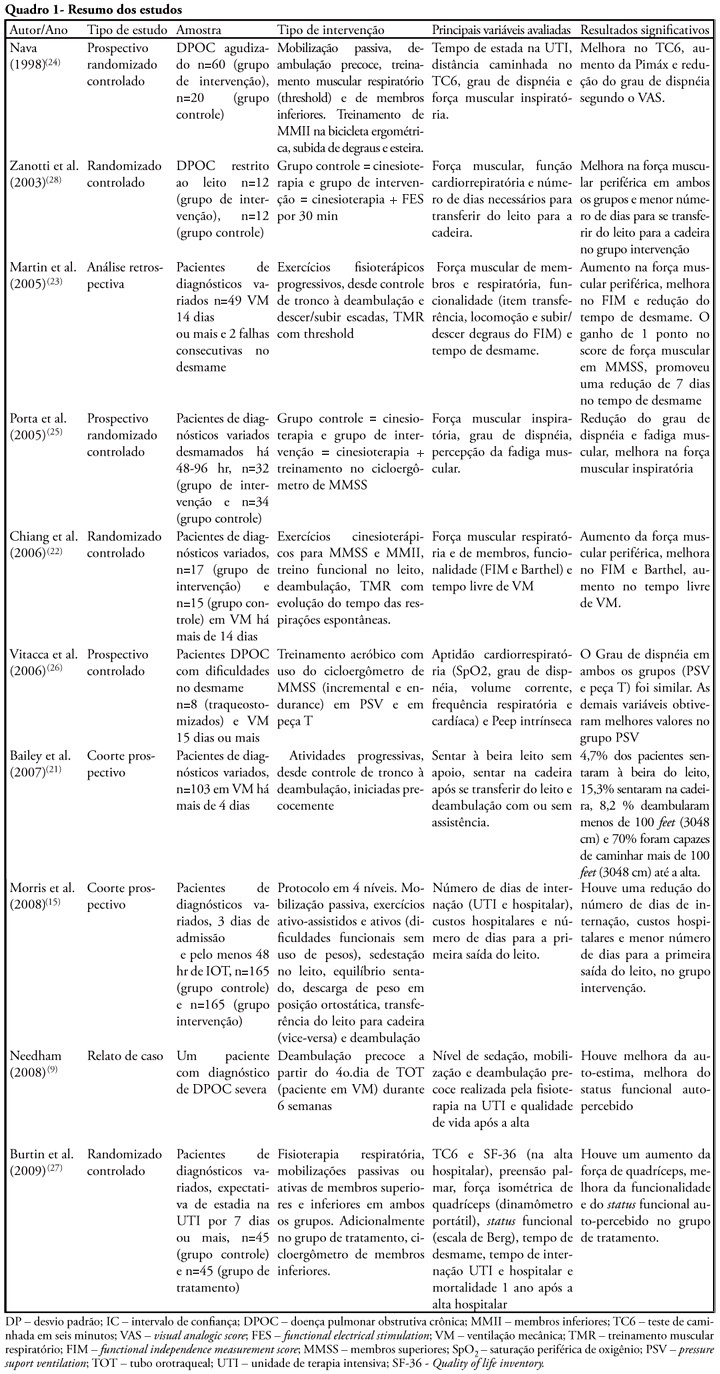
Views0See moreThe development of critical patient-related generalized weakness is a common complication in patients admitted to an intensive care unit. The reduced muscle strength increases the time for weaning, hospitalization, the risk of infections and consequent mortality. Physiotherapy is used in these patients as a resource for the prevention of muscle weakness, atrophy and functional capacity recovery. The aim of this study was to review the literature regarding the use of exercise alone in intensive care units staying patients. Literature searches were performed using the electronic databases Medline, LILACS, CINAHL, Cochrane, High Wire Press and SciELO, from January 1998 to July 2009 and book chapters, using keywords including “critical illness”, “cinesiotherapy”, “physical therapy”, “physiotherapy”, “exercises”, “training”, “force”, “active mobilization”, “mobilization”, “ICU”, “rehabilitation”, “mobility”, “muscle strength” and “weakness”. Despite the lack of studies and methodological diversity of studies found, confirming the use of exercise alone as a therapeutic resource, its use, including early seems an alternative to prevent and reverse muscle weakness intensive care unit ICU-acquired.
Views0Abstract
Review ArticlesEffects of motor physical therapy in critically ill patients: literature review
Rev Bras Ter Intensiva. 2010;22(1):85-91
DOI 10.1590/S0103-507X2010000100014
Views0See moreThe development of critical patient-related generalized weakness is a common complication in patients admitted to an intensive care unit. The reduced muscle strength increases the time for weaning, hospitalization, the risk of infections and consequent mortality. Physiotherapy is used in these patients as a resource for the prevention of muscle weakness, atrophy and functional capacity recovery. The aim of this study was to review the literature regarding the use of exercise alone in intensive care units staying patients. Literature searches were performed using the electronic databases Medline, LILACS, CINAHL, Cochrane, High Wire Press and SciELO, from January 1998 to July 2009 and book chapters, using keywords including “critical illness”, “cinesiotherapy”, “physical therapy”, “physiotherapy”, “exercises”, “training”, “force”, “active mobilization”, “mobilization”, “ICU”, “rehabilitation”, “mobility”, “muscle strength” and “weakness”. Despite the lack of studies and methodological diversity of studies found, confirming the use of exercise alone as a therapeutic resource, its use, including early seems an alternative to prevent and reverse muscle weakness intensive care unit ICU-acquired.
-
Review Articles
Clevidipine for hypertensive emergency
Rev Bras Ter Intensiva. 2010;22(1):92-95
Abstract
Review ArticlesClevidipine for hypertensive emergency
Rev Bras Ter Intensiva. 2010;22(1):92-95
DOI 10.1590/S0103-507X2010000100015
Views0See moreHypertensive emergency, is the most severe presentation of arterial hypertension, having high morbidity-mortality. Clevidipine is a calcium channel blocker. Its pharmacokinetics is favorable to use for hypertensive emergencies, rendering this drug a promising alternative to the restricted therapeutic armamentarium available both in the emergency room and intensive care unit. In this review we describe the pharmacodynamics, pharmacokinetics and clinical trials evaluating Clevidipine in emergency situations, comparing this drug to other traditionally used drugs in this condition.
Views0Abstract
Review ArticlesClevidipine for hypertensive emergency
Rev Bras Ter Intensiva. 2010;22(1):92-95
DOI 10.1590/S0103-507X2010000100015
Views0See moreHypertensive emergency, is the most severe presentation of arterial hypertension, having high morbidity-mortality. Clevidipine is a calcium channel blocker. Its pharmacokinetics is favorable to use for hypertensive emergencies, rendering this drug a promising alternative to the restricted therapeutic armamentarium available both in the emergency room and intensive care unit. In this review we describe the pharmacodynamics, pharmacokinetics and clinical trials evaluating Clevidipine in emergency situations, comparing this drug to other traditionally used drugs in this condition.
-
Case Report
Chryseobacterium indologenes infection: a case report
Rev Bras Ter Intensiva. 2010;22(1):96-98
Abstract
Case ReportChryseobacterium indologenes infection: a case report
Rev Bras Ter Intensiva. 2010;22(1):96-98
DOI 10.1590/S0103-507X2010000100016
Views0See moreA case of Chryseobacterium indologenes infection is reported, identified in an invasive mechanic ventilation patient’s tracheal aspiration material. Epidemiological, microbiological, and intensive care unit therapy aspects are discussed. The patient was a 30 years-old male, admitted with idiopathic medullary aplasia and febrile neutropenia, referred to the intensive care unit with severe bronchopneumonia and sepsis of pulmonary origin. Most of the previously reported Chryseobacterium indologenes infection cases were associated with severe diseases and polymicrobial infections which could make difficult interpreting antimicrobial therapy options against this agent.
Views0Abstract
Case ReportChryseobacterium indologenes infection: a case report
Rev Bras Ter Intensiva. 2010;22(1):96-98
DOI 10.1590/S0103-507X2010000100016
Views0See moreA case of Chryseobacterium indologenes infection is reported, identified in an invasive mechanic ventilation patient’s tracheal aspiration material. Epidemiological, microbiological, and intensive care unit therapy aspects are discussed. The patient was a 30 years-old male, admitted with idiopathic medullary aplasia and febrile neutropenia, referred to the intensive care unit with severe bronchopneumonia and sepsis of pulmonary origin. Most of the previously reported Chryseobacterium indologenes infection cases were associated with severe diseases and polymicrobial infections which could make difficult interpreting antimicrobial therapy options against this agent.
Volume Articles - Critical Care Science (CCS)
