-
Editorial
Change the Qualis criteria!
Rev Bras Ter Intensiva. 2010;22(2):99-102
-
Original Articles
Orotracheal intubation: physicians knowledge assessment and clinical practices in intensive care units
Rev Bras Ter Intensiva. 2010;22(2):103-111
Abstract
Original ArticlesOrotracheal intubation: physicians knowledge assessment and clinical practices in intensive care units
Rev Bras Ter Intensiva. 2010;22(2):103-111
DOI 10.1590/S0103-507X2010000200002
Views0See moreOBJECTIVES: To assess the physician’s knowledge on intubation techniques and to identify the common practices. METHODS: This was a prospective study, involving three different intensive care units within a University hospital: Anesthesiology (ANEST), Pulmonology (PULMO) and Emergency Department (ED). All physicians working in these units and consenting to participate in the study completed a questionnaire with their demographic data and questions on orotracheal intubation. RESULTS: 85 completed questionnaires were retrieved (90.42% of the physicians). ANEST had the higher mean age (p=0.001), being 43.5% of them intensivists. The use of hypnotic and opioid association was reported by 97.6%, and pre-oxygenation by 91.8%, but only 44.6% reported sub-occipital pad use, with no difference between the ICUs. On ANEST an increased neuromuscular blockade use was reported (p<0.000) as well as increased caution with full stomach (p=0.002). The rapid sequence knowledge was restricted (mean 2.20 ± 0.89), p=0.06 between the different units. The Sellick maneuver was known by 97.6%, but 72% used it inappropriately. CONCLUSIONS: Physicians knowledge on orotracheal intubation in the intensive care unit is unsatisfactory, even among qualified professionals. It is necessary to check if the responses to the questionnaire and actual clinical practices agree.
Views0

Abstract
Original ArticlesOrotracheal intubation: physicians knowledge assessment and clinical practices in intensive care units
Rev Bras Ter Intensiva. 2010;22(2):103-111
DOI 10.1590/S0103-507X2010000200002
Views0See moreOBJECTIVES: To assess the physician’s knowledge on intubation techniques and to identify the common practices. METHODS: This was a prospective study, involving three different intensive care units within a University hospital: Anesthesiology (ANEST), Pulmonology (PULMO) and Emergency Department (ED). All physicians working in these units and consenting to participate in the study completed a questionnaire with their demographic data and questions on orotracheal intubation. RESULTS: 85 completed questionnaires were retrieved (90.42% of the physicians). ANEST had the higher mean age (p=0.001), being 43.5% of them intensivists. The use of hypnotic and opioid association was reported by 97.6%, and pre-oxygenation by 91.8%, but only 44.6% reported sub-occipital pad use, with no difference between the ICUs. On ANEST an increased neuromuscular blockade use was reported (p<0.000) as well as increased caution with full stomach (p=0.002). The rapid sequence knowledge was restricted (mean 2.20 ± 0.89), p=0.06 between the different units. The Sellick maneuver was known by 97.6%, but 72% used it inappropriately. CONCLUSIONS: Physicians knowledge on orotracheal intubation in the intensive care unit is unsatisfactory, even among qualified professionals. It is necessary to check if the responses to the questionnaire and actual clinical practices agree.
-
Original Articles
Appropriate medical professionals communication reduces intensive care unit mortality
Rev Bras Ter Intensiva. 2010;22(2):112-117
Abstract
Original ArticlesAppropriate medical professionals communication reduces intensive care unit mortality
Rev Bras Ter Intensiva. 2010;22(2):112-117
DOI 10.1590/S0103-507X2010000200003
Views0See moreOBJECTIVES: Communication issues between healthcare professionals in intensive care units may be related to critically ill patients’ increased mortality. This study aimed to evaluate if communication issues involving assistant physicians and routine intensive care unit physicians would impact critically ill patients’ morbidity and mortality. METHODS: This was a cohort study that included non-consecutive patients admitted to the intensive care unit for 18 months. The patients were categorized in 3 groups according to their assistant doctors’ versus routine doctors communication uses: DC – daily communication during the stay (>75% of the days); EC – eventual communication (25 to 75% of the days); RC – rare communication (< 25% of the days). Demographic data, severity scores, reason for admission to the intensive care unit and interventions were recorded. The consequences of the medical professionals communication failures (delayed procedures, diagnostic tests, antibiotics, ventilatory weaning, vasopressors) and medical prescriptions inadequacies (no bed head elevation, no stress ulceration and deep venous thrombosis drug prophylaxis), and their relationship with the patients outcomes were analyzed. RESULTS: 792 patients were included, and categorized as follows: DC (n=529); EC (n=187) and RC (n=76). The mortality was increased in the RC patients group (26.3%) versus the remainder groups (DC = 13.6% and EC = 17.1%; p<0.05). A multivariate analysis showed that delayed antibiotics [RR 1.83 (CI95%: 1.36 -2.25)], delayed ventilatory weaning [RR 1.63 (CI95%: 1.25-2.04)] and no deep venous thrombosis prophylaxis [RR 1.98 (CI95%: 1.43 - 3.12)] contributed independently for the increased mortality. CONCLUSION: The failure in the assistant and routine intensive care doctors communication may increase the patients’ mortality, particularly due to delayed antibiotics and ventilation weaning, and lack of deep venous thrombosis prophylaxis prescription.
Views0Abstract
Original ArticlesAppropriate medical professionals communication reduces intensive care unit mortality
Rev Bras Ter Intensiva. 2010;22(2):112-117
DOI 10.1590/S0103-507X2010000200003
Views0See moreOBJECTIVES: Communication issues between healthcare professionals in intensive care units may be related to critically ill patients’ increased mortality. This study aimed to evaluate if communication issues involving assistant physicians and routine intensive care unit physicians would impact critically ill patients’ morbidity and mortality. METHODS: This was a cohort study that included non-consecutive patients admitted to the intensive care unit for 18 months. The patients were categorized in 3 groups according to their assistant doctors’ versus routine doctors communication uses: DC – daily communication during the stay (>75% of the days); EC – eventual communication (25 to 75% of the days); RC – rare communication (< 25% of the days). Demographic data, severity scores, reason for admission to the intensive care unit and interventions were recorded. The consequences of the medical professionals communication failures (delayed procedures, diagnostic tests, antibiotics, ventilatory weaning, vasopressors) and medical prescriptions inadequacies (no bed head elevation, no stress ulceration and deep venous thrombosis drug prophylaxis), and their relationship with the patients outcomes were analyzed. RESULTS: 792 patients were included, and categorized as follows: DC (n=529); EC (n=187) and RC (n=76). The mortality was increased in the RC patients group (26.3%) versus the remainder groups (DC = 13.6% and EC = 17.1%; p<0.05). A multivariate analysis showed that delayed antibiotics [RR 1.83 (CI95%: 1.36 -2.25)], delayed ventilatory weaning [RR 1.63 (CI95%: 1.25-2.04)] and no deep venous thrombosis prophylaxis [RR 1.98 (CI95%: 1.43 - 3.12)] contributed independently for the increased mortality. CONCLUSION: The failure in the assistant and routine intensive care doctors communication may increase the patients’ mortality, particularly due to delayed antibiotics and ventilation weaning, and lack of deep venous thrombosis prophylaxis prescription.
-
Original Articles
Prolonged gastrointestinal dysfunction in critically ill patients
Rev Bras Ter Intensiva. 2010;22(2):118-124
Abstract
Original ArticlesProlonged gastrointestinal dysfunction in critically ill patients
Rev Bras Ter Intensiva. 2010;22(2):118-124
DOI 10.1590/S0103-507X2010000200004
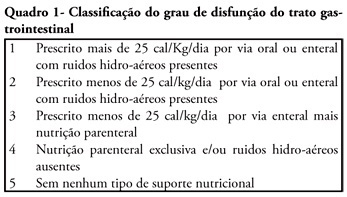
Views0See moreOBJECTIVE: We aimed to investigate the prevalence and independent predictors of prolonged gastrointestinal dysfunction in critically ill patients admitted to the intensive care unit. METHODS: Retrospective and observational cohort study performed in a mixed 24 beds intensive care unit in a tertiary center. Patients admitted in the intensive care unit between August 2003 and January 2004, who had a length of stay in the intensive care unit greater than 4 days were enrolled. Gastrointestinal function was evaluated daily according to a classification that considered physical examination (bowel sounds or distension) and the nutritional support progress. RESULTS: Were included 128 patients. The mean age was 56 ± 19 years, 63.3% were male and 77.3% were surgical patients. Prolonged gastrointestinal dysfunction occurred in 35% of patients, with prevalence 3.3 times higher in surgical patients (27%) than in medical patients (8%). Endoscopies were performed in 38 patients (29.7%), and in three quarters of them erosive lesions and or bleeding were observed. Gastrointestinal dysfunction was more frequent in patients presenting moderate or severe edema (51%) than in patients without edema (22.5%) (p<0.05). In the logistic regression analysis, a serum lactate level higher than 5.2 mEq/L (RR 6.69 95%CI 15-38.7, P = 0.034) and the presence of a low oxygenation index (RR 12.4 95%CI 2.18-70.8, p = 0.005) were predictive of gastrointestinal dysfunction. CONCLUSION: Prolonged gastrointestinal dysfunction was highly prevalent in this heterogeneous population of critically ill patients. Admission high serum lactate levels and a low oxygenation index were predictive of prolonged gastrointestinal dysfunction.
Views0Abstract
Original ArticlesProlonged gastrointestinal dysfunction in critically ill patients
Rev Bras Ter Intensiva. 2010;22(2):118-124
DOI 10.1590/S0103-507X2010000200004
Views0See moreOBJECTIVE: We aimed to investigate the prevalence and independent predictors of prolonged gastrointestinal dysfunction in critically ill patients admitted to the intensive care unit. METHODS: Retrospective and observational cohort study performed in a mixed 24 beds intensive care unit in a tertiary center. Patients admitted in the intensive care unit between August 2003 and January 2004, who had a length of stay in the intensive care unit greater than 4 days were enrolled. Gastrointestinal function was evaluated daily according to a classification that considered physical examination (bowel sounds or distension) and the nutritional support progress. RESULTS: Were included 128 patients. The mean age was 56 ± 19 years, 63.3% were male and 77.3% were surgical patients. Prolonged gastrointestinal dysfunction occurred in 35% of patients, with prevalence 3.3 times higher in surgical patients (27%) than in medical patients (8%). Endoscopies were performed in 38 patients (29.7%), and in three quarters of them erosive lesions and or bleeding were observed. Gastrointestinal dysfunction was more frequent in patients presenting moderate or severe edema (51%) than in patients without edema (22.5%) (p<0.05). In the logistic regression analysis, a serum lactate level higher than 5.2 mEq/L (RR 6.69 95%CI 15-38.7, P = 0.034) and the presence of a low oxygenation index (RR 12.4 95%CI 2.18-70.8, p = 0.005) were predictive of gastrointestinal dysfunction. CONCLUSION: Prolonged gastrointestinal dysfunction was highly prevalent in this heterogeneous population of critically ill patients. Admission high serum lactate levels and a low oxygenation index were predictive of prolonged gastrointestinal dysfunction.
-
Original Articles
Perceptions about end of life treatment in Argentina, Brazil and Uruguay intensive care units
Rev Bras Ter Intensiva. 2010;22(2):125-132
Abstract
Original ArticlesPerceptions about end of life treatment in Argentina, Brazil and Uruguay intensive care units
Rev Bras Ter Intensiva. 2010;22(2):125-132
DOI 10.1590/S0103-507X2010000200005
Views0ABSTRACT OBJECTIVE: To evaluate end-of-life procedures in intensive care units. METHODS: A questionnaire was prepared by the End-of-Life Study Group of the Argentinean, Brazilian and Uruguayan Intensive Care societies, collecting data on the participants’ demographics, institutions and limit therapeutic effort (LTE) decision making process. During this cross sectional study, the societies’ multidisciplinary teams members completed the questionnaire either during scientific meetings or online. The variables were analyzed with the Chi-square test, with a p<0.05 significance level. RESULTS: 420 professionals completed the questionnaire. The Brazilian units had more beds, unrestricted visit was less frequent, their professionals were younger and worked more recently in intensive care units, and more non-medical professionals completed the questionnaire. Three visits daily was the more usual number of visits for the three countries. The most influencing LTE factors were prognosis, co-morbidities, and therapeutic futility. In the three countries, more than 90% of the completers had already made LTE decisions. Cardiopulmonary resuscitation, vasoactive drugs administration, dialysis and parenteral nutrition were the most suspended/refused therapies in the three countries. Suspension of mechanic ventilation was more frequent in Argentina, followed by Uruguay. Sedation and analgesia were the less suspended therapies in the three countries. Legal definement and ethical issues were mentioned as the main barriers for the LTE decision making process. CONCLUSION: LTE decisions are frequent among the professionals working in the three countries’ intensive care units. We found a more proactive LTE decision making trend In Argentina, and more equity for decisions distribution in Uruguay. This difference appears to be related to the participants’ different ages, experiences, professional types and genders.
Keywords:Medical FutilityQuestionnairesTerminal careTerminally illTreatment refusalWithholding TreatmentSee moreViews0Abstract
Original ArticlesPerceptions about end of life treatment in Argentina, Brazil and Uruguay intensive care units
Rev Bras Ter Intensiva. 2010;22(2):125-132
DOI 10.1590/S0103-507X2010000200005
Views0ABSTRACT OBJECTIVE: To evaluate end-of-life procedures in intensive care units. METHODS: A questionnaire was prepared by the End-of-Life Study Group of the Argentinean, Brazilian and Uruguayan Intensive Care societies, collecting data on the participants’ demographics, institutions and limit therapeutic effort (LTE) decision making process. During this cross sectional study, the societies’ multidisciplinary teams members completed the questionnaire either during scientific meetings or online. The variables were analyzed with the Chi-square test, with a p<0.05 significance level. RESULTS: 420 professionals completed the questionnaire. The Brazilian units had more beds, unrestricted visit was less frequent, their professionals were younger and worked more recently in intensive care units, and more non-medical professionals completed the questionnaire. Three visits daily was the more usual number of visits for the three countries. The most influencing LTE factors were prognosis, co-morbidities, and therapeutic futility. In the three countries, more than 90% of the completers had already made LTE decisions. Cardiopulmonary resuscitation, vasoactive drugs administration, dialysis and parenteral nutrition were the most suspended/refused therapies in the three countries. Suspension of mechanic ventilation was more frequent in Argentina, followed by Uruguay. Sedation and analgesia were the less suspended therapies in the three countries. Legal definement and ethical issues were mentioned as the main barriers for the LTE decision making process. CONCLUSION: LTE decisions are frequent among the professionals working in the three countries’ intensive care units. We found a more proactive LTE decision making trend In Argentina, and more equity for decisions distribution in Uruguay. This difference appears to be related to the participants’ different ages, experiences, professional types and genders.
Keywords:Medical FutilityQuestionnairesTerminal careTerminally illTreatment refusalWithholding TreatmentSee more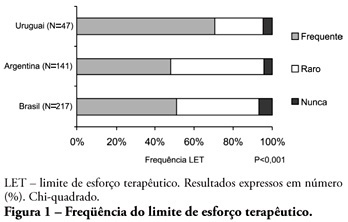
-
Original Articles
Impact of obesity on critical care treatment in adult patients
Rev Bras Ter Intensiva. 2010;22(2):133-137
Abstract
Original ArticlesImpact of obesity on critical care treatment in adult patients
Rev Bras Ter Intensiva. 2010;22(2):133-137
DOI 10.1590/S0103-507X2010000200006
Views0See moreSTUDY OBJECTIVE: Obese patients seem to have worse outcomes and more complications during intensive care unit (ICU) stay. This study describes the clinical course, complications and prognostic factors of obese patients admitted to an intensive care unit compared to a control group of nonobese patients. DESIGN: Retrospective observational study. SETTING: A 10-bed adult intensive care unit in a university-affiliated hospital. METHODS: All patients admitted to the intensive care unit over 52 months (April 01/2005 to November 30/2008) were included. Obese patients were defined as those with a body mass index (BMI) ≥ 30 Kg/M2. Demographic and intensive care unit related data were also collected. An clinical and demographical matching group of eutrophic patients selected from the data base as comparator for mortality and morbidity outcomes. The Mann-Whitney test was used for numeric data comparisons and the Chi Square test for categorical data comparisons. RESULTS: Two hundred nineteen patients were included. The obese group (n=73) was compared to the eutrophic group (n= 146). Most of this group BMI ranged between 30 – 35 Kg/M2. Only ten patients had body mass index ≥40 Kg/M2. Significant differences between the obese and eutrophic groups were observed in median APACHE II score (16 versus 12, respectively; p<0.05) and median intensive care unit length of stay (7 versus 5 days respectively; p<0,05). No significant differences were seen regarding risk of death, mortality rate, mechanical ventilation needs, days free of mechanical ventilation and tracheostomy rates. The observed mortality was higher than the APACHE II-predicted for both groups, but the larger differences were seen for morbid obese patients (BMI ≥40 Kg/M2). CONCLUSIONS: Obesity did not increase the mortality rate, but improved intensive care unit length of stay. The current prognostic scoring systems do not include BMI, possibly underestimating the risk of death, and other quality of care indexes in obese patients. New studies could be useful to clarify how body mass index impacts the mortality rate.
Views0Abstract
Original ArticlesImpact of obesity on critical care treatment in adult patients
Rev Bras Ter Intensiva. 2010;22(2):133-137
DOI 10.1590/S0103-507X2010000200006
Views0See moreSTUDY OBJECTIVE: Obese patients seem to have worse outcomes and more complications during intensive care unit (ICU) stay. This study describes the clinical course, complications and prognostic factors of obese patients admitted to an intensive care unit compared to a control group of nonobese patients. DESIGN: Retrospective observational study. SETTING: A 10-bed adult intensive care unit in a university-affiliated hospital. METHODS: All patients admitted to the intensive care unit over 52 months (April 01/2005 to November 30/2008) were included. Obese patients were defined as those with a body mass index (BMI) ≥ 30 Kg/M2. Demographic and intensive care unit related data were also collected. An clinical and demographical matching group of eutrophic patients selected from the data base as comparator for mortality and morbidity outcomes. The Mann-Whitney test was used for numeric data comparisons and the Chi Square test for categorical data comparisons. RESULTS: Two hundred nineteen patients were included. The obese group (n=73) was compared to the eutrophic group (n= 146). Most of this group BMI ranged between 30 – 35 Kg/M2. Only ten patients had body mass index ≥40 Kg/M2. Significant differences between the obese and eutrophic groups were observed in median APACHE II score (16 versus 12, respectively; p<0.05) and median intensive care unit length of stay (7 versus 5 days respectively; p<0,05). No significant differences were seen regarding risk of death, mortality rate, mechanical ventilation needs, days free of mechanical ventilation and tracheostomy rates. The observed mortality was higher than the APACHE II-predicted for both groups, but the larger differences were seen for morbid obese patients (BMI ≥40 Kg/M2). CONCLUSIONS: Obesity did not increase the mortality rate, but improved intensive care unit length of stay. The current prognostic scoring systems do not include BMI, possibly underestimating the risk of death, and other quality of care indexes in obese patients. New studies could be useful to clarify how body mass index impacts the mortality rate.
-
Original Articles
Risk factors for death among critically ill elderly patients
Rev Bras Ter Intensiva. 2010;22(2):138-143
Abstract
Original ArticlesRisk factors for death among critically ill elderly patients
Rev Bras Ter Intensiva. 2010;22(2):138-143
DOI 10.1590/S0103-507X2010000200007
Views0See moreBACKGROUND: The elderly population is increasing all over the world. The need of intensive care by the elderly is also increasing. There is a lack of studies investigating the risk factors for death among critically ill elderly patients. This study aims to investigate the factors associated with death in a population of critically ill elderly patients admitted to an intensive care unit in Brazil. METHODS: This is a retrospective cohort study including all elderly patients (>60 years) admitted to an intensive care unit in Fortaleza, Brazil, from January to December 2007. A comparison between survivors and nonsurvivors was done and the risk factors for death were investigated through univariate and multivariate analysis. RESULTS: A total of 84 patients were included, with an average age of 73 ± 7.6 years; 59% were female. Mortality was 62.8%. The main cause of death was multiple organ dysfunction (42.3%), followed by septic shock (36.5%) and cardiogenic shock (9.7%). Complications during intensive care unit ICU stay associated with death were respiratory failure (OR=61, p<0.001), acute kidney injury (OR=23, p<0.001), sepsis (OR=12, p<0.001), metabolic acidosis (OR=17, p<0.001), anemia (OR=8.6, p<0.005), coagulation disturbance (OR=5.9, p<0.001) and atrial fibrillation (OR=4.8, p<0.041). Independent risk factors for death were age (OR=1.15, p<0.005), coma (OR=7.51, p<0.003), hypotension (OR=21.75, p=0.003), respiratory failure (OR=9.93, p<0.0001) and acute kidney injury (OR=16.28, p<0.014). CONCLUSION: Mortality is high among critically ill elderly patients. Factors associated with death were age, coma, hypotension, respiratory failure and acute kidney injury.
Views0Abstract
Original ArticlesRisk factors for death among critically ill elderly patients
Rev Bras Ter Intensiva. 2010;22(2):138-143
DOI 10.1590/S0103-507X2010000200007
Views0See moreBACKGROUND: The elderly population is increasing all over the world. The need of intensive care by the elderly is also increasing. There is a lack of studies investigating the risk factors for death among critically ill elderly patients. This study aims to investigate the factors associated with death in a population of critically ill elderly patients admitted to an intensive care unit in Brazil. METHODS: This is a retrospective cohort study including all elderly patients (>60 years) admitted to an intensive care unit in Fortaleza, Brazil, from January to December 2007. A comparison between survivors and nonsurvivors was done and the risk factors for death were investigated through univariate and multivariate analysis. RESULTS: A total of 84 patients were included, with an average age of 73 ± 7.6 years; 59% were female. Mortality was 62.8%. The main cause of death was multiple organ dysfunction (42.3%), followed by septic shock (36.5%) and cardiogenic shock (9.7%). Complications during intensive care unit ICU stay associated with death were respiratory failure (OR=61, p<0.001), acute kidney injury (OR=23, p<0.001), sepsis (OR=12, p<0.001), metabolic acidosis (OR=17, p<0.001), anemia (OR=8.6, p<0.005), coagulation disturbance (OR=5.9, p<0.001) and atrial fibrillation (OR=4.8, p<0.041). Independent risk factors for death were age (OR=1.15, p<0.005), coma (OR=7.51, p<0.003), hypotension (OR=21.75, p=0.003), respiratory failure (OR=9.93, p<0.0001) and acute kidney injury (OR=16.28, p<0.014). CONCLUSION: Mortality is high among critically ill elderly patients. Factors associated with death were age, coma, hypotension, respiratory failure and acute kidney injury.
-
Original Articles
Patterns of antibacterials use in intensive care units
Rev Bras Ter Intensiva. 2010;22(2):144-152
Abstract
Original ArticlesPatterns of antibacterials use in intensive care units
Rev Bras Ter Intensiva. 2010;22(2):144-152
DOI 10.1590/S0103-507X2010000200008
Views0See moreOBJECTIVE: To know and compare the patterns of antimicrobials use in intensive care units (ICUs) based on the Anatomical Therapeutic Chemical/Defined Daily Dose (ATC/DDD) system. METHODS: a prospective cohort study was conducted in three medical-surgical intensive care units, two of them in public hospitals and one in a private hospital. Simple random, independent samples of patients admitted from 10/2004 to 09/2005 to the selected intensive care units were used. The antibiotics use was assessed using the ATC/DDD system. The amount of antibacterials used in each intensive care unit, in grams, was transformed in daily defined dose (DDD). The number of DDDs was divided by the number of patient-days, multiplied by one thousand, to obtain the average density of consumption (DC) per thousand patient-days (DDD1000). RESULTS: 1,728 patients-days and 2,918.6 DDDs were examined in the three intensive care units, corresponding to an average density of consumption of 1,689.0 DDD1000. The median number of DDDs of antibiotics use in the public hospitals’ intensive care units was significantly higher (p=0.002) versus the private hospital’s intensive care unit. The consumption of antibiotics in the private hospital’s intensive care unit (DC=2,191.7 DDD1000) was significantly higher (p<0.001) versus the intensive care units of public hospitals (1,499.5 DDD1000). The most used antibiotics groups in the three intensive care units were 3rd generation cephalosporins, penicillins/betalactamases inhibitors, carbapenems and fluorquinolones. CONCLUSION: The pattern of antibiotics use in the three examined intensive care units was not uniform. The private hospital’s intensive care unit used a significantly larger amount versus the public hospitals’ intensive care units. Nevertheless, the most used antibiotics groups were similar in the three intensive care units.
Views0Abstract
Original ArticlesPatterns of antibacterials use in intensive care units
Rev Bras Ter Intensiva. 2010;22(2):144-152
DOI 10.1590/S0103-507X2010000200008
Views0See moreOBJECTIVE: To know and compare the patterns of antimicrobials use in intensive care units (ICUs) based on the Anatomical Therapeutic Chemical/Defined Daily Dose (ATC/DDD) system. METHODS: a prospective cohort study was conducted in three medical-surgical intensive care units, two of them in public hospitals and one in a private hospital. Simple random, independent samples of patients admitted from 10/2004 to 09/2005 to the selected intensive care units were used. The antibiotics use was assessed using the ATC/DDD system. The amount of antibacterials used in each intensive care unit, in grams, was transformed in daily defined dose (DDD). The number of DDDs was divided by the number of patient-days, multiplied by one thousand, to obtain the average density of consumption (DC) per thousand patient-days (DDD1000). RESULTS: 1,728 patients-days and 2,918.6 DDDs were examined in the three intensive care units, corresponding to an average density of consumption of 1,689.0 DDD1000. The median number of DDDs of antibiotics use in the public hospitals’ intensive care units was significantly higher (p=0.002) versus the private hospital’s intensive care unit. The consumption of antibiotics in the private hospital’s intensive care unit (DC=2,191.7 DDD1000) was significantly higher (p<0.001) versus the intensive care units of public hospitals (1,499.5 DDD1000). The most used antibiotics groups in the three intensive care units were 3rd generation cephalosporins, penicillins/betalactamases inhibitors, carbapenems and fluorquinolones. CONCLUSION: The pattern of antibiotics use in the three examined intensive care units was not uniform. The private hospital’s intensive care unit used a significantly larger amount versus the public hospitals’ intensive care units. Nevertheless, the most used antibiotics groups were similar in the three intensive care units.
-
Original Articles
Cardiorespiratory arrest diagnosis and treatment: theoretical knowledge evaluation in a general hospital’s physicians
Rev Bras Ter Intensiva. 2010;22(2):153-158
Abstract
Original ArticlesCardiorespiratory arrest diagnosis and treatment: theoretical knowledge evaluation in a general hospital’s physicians
Rev Bras Ter Intensiva. 2010;22(2):153-158
DOI 10.1590/S0103-507X2010000200009
Views0BACKGROUND: The main causes of cardiopulmonary arrest are endemic, and require constant medical improvement on cardiopulmonary resuscitation techniques. Training and continued education are essential to skilled management of cardiopulmonary resuscitation. OBJECTIVE: This study aimed to evaluate the physicians’ theoretical knowledge on diagnosis and treatment of cardiopulmonary arrest. METHODS: This was a cross-sectional descriptive research conducted in a general hospital in Roraima, Brazil. The study population consisted of physicians who worked in the emergency department and intensive care units. The data were collected using a questionnaire addressing the subject. RESULTS: Forty four physicians answered the questionnaire. The mean score was 50% right answers. Most (88.5%) respondents committed “fatal errors”. Half of the sample was never trained in advanced life support skills. No correlation was found between the number of right answers and attendance to advanced life support training courses. An inverse correlation was found between performance and age, but no statistically significant correlation was seen regarding performance and time from medical graduation. CONCLUSION: The physicians’ theoretical knowledge on this field is worrisome. The results point to the importance of professional advanced life support training in order to assure quality standards for cardiac arrest management in this general hospital.
Keywords:Advanced life supportBasic life supportCardiopulmonary ResuscitationHealth knowledgeHeart arrestSee moreViews0Abstract
Original ArticlesCardiorespiratory arrest diagnosis and treatment: theoretical knowledge evaluation in a general hospital’s physicians
Rev Bras Ter Intensiva. 2010;22(2):153-158
DOI 10.1590/S0103-507X2010000200009
Views0BACKGROUND: The main causes of cardiopulmonary arrest are endemic, and require constant medical improvement on cardiopulmonary resuscitation techniques. Training and continued education are essential to skilled management of cardiopulmonary resuscitation. OBJECTIVE: This study aimed to evaluate the physicians’ theoretical knowledge on diagnosis and treatment of cardiopulmonary arrest. METHODS: This was a cross-sectional descriptive research conducted in a general hospital in Roraima, Brazil. The study population consisted of physicians who worked in the emergency department and intensive care units. The data were collected using a questionnaire addressing the subject. RESULTS: Forty four physicians answered the questionnaire. The mean score was 50% right answers. Most (88.5%) respondents committed “fatal errors”. Half of the sample was never trained in advanced life support skills. No correlation was found between the number of right answers and attendance to advanced life support training courses. An inverse correlation was found between performance and age, but no statistically significant correlation was seen regarding performance and time from medical graduation. CONCLUSION: The physicians’ theoretical knowledge on this field is worrisome. The results point to the importance of professional advanced life support training in order to assure quality standards for cardiac arrest management in this general hospital.
Keywords:Advanced life supportBasic life supportCardiopulmonary ResuscitationHealth knowledgeHeart arrestSee more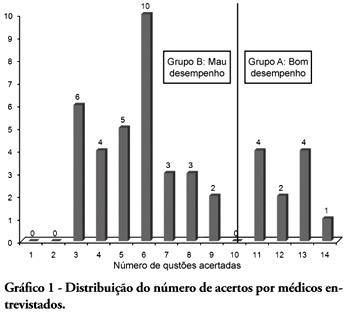
-
Original Articles
Spontaneous breathing trial evaluation in preterm newborns extubation
Rev Bras Ter Intensiva. 2010;22(2):159-165
Abstract
Original ArticlesSpontaneous breathing trial evaluation in preterm newborns extubation
Rev Bras Ter Intensiva. 2010;22(2):159-165
DOI 10.1590/S0103-507X2010000200010
Views0See moreOBJECTIVE: Neonates mechanic ventilation weaning has become a major clinical challenge, and constitutes a large portion of neonatal intensive care units workload. The spontaneous breathing trial (SBT), performed immediately before extubation, can provide useful information on the patient’s spontaneous breathing ability. This study aimed to assess the SBT effectiveness for extubation success prediction in mechanically ventilated preterm infants. METHODS: After Ethics Committee approval, an observational, longitudinal, prospective study was conducted. A sample of 60 preterm infants compliant with the weaning criteria was categorized in two groups: ‘SBT’ group (n=30), with the patients who underwent 30 minutes spontaneous breathing trial (SBT) with continuous positive pressure airway (CPAP), and the control group (n=30) where the extubation was performed without spontaneous breathing trial. The heart rate (HR), respiratory rate (RR), pulse oxymetry oxygen saturation (SpO2) and the Silverman-Andersen score were recorded before and 10, 20 and 30 minutes after the spontaneous breathing trial. Were also assessed for both groups, and versus extubation success or failure, the weight, gestational age, Apgar score, mean airway pressure, inspired oxygen concentration, and tracheal tube time. The Chi-square test was used for categorical variables and the Mann-Whitney test for non-normal distribution. Extubation success was defined as a 48 hours period with no reintubation requirement. RESULTS: No significant differences were identified between the groups for the analyzed variables, except for the mean airway pressure. A significant association was shown between spontaneous breathing trial and successful extubation. CONCLUSION: The significant association between SBT and extubation success may contribute for prediction of successful weaning in preterm infants.
Views0Abstract
Original ArticlesSpontaneous breathing trial evaluation in preterm newborns extubation
Rev Bras Ter Intensiva. 2010;22(2):159-165
DOI 10.1590/S0103-507X2010000200010
Views0See moreOBJECTIVE: Neonates mechanic ventilation weaning has become a major clinical challenge, and constitutes a large portion of neonatal intensive care units workload. The spontaneous breathing trial (SBT), performed immediately before extubation, can provide useful information on the patient’s spontaneous breathing ability. This study aimed to assess the SBT effectiveness for extubation success prediction in mechanically ventilated preterm infants. METHODS: After Ethics Committee approval, an observational, longitudinal, prospective study was conducted. A sample of 60 preterm infants compliant with the weaning criteria was categorized in two groups: ‘SBT’ group (n=30), with the patients who underwent 30 minutes spontaneous breathing trial (SBT) with continuous positive pressure airway (CPAP), and the control group (n=30) where the extubation was performed without spontaneous breathing trial. The heart rate (HR), respiratory rate (RR), pulse oxymetry oxygen saturation (SpO2) and the Silverman-Andersen score were recorded before and 10, 20 and 30 minutes after the spontaneous breathing trial. Were also assessed for both groups, and versus extubation success or failure, the weight, gestational age, Apgar score, mean airway pressure, inspired oxygen concentration, and tracheal tube time. The Chi-square test was used for categorical variables and the Mann-Whitney test for non-normal distribution. Extubation success was defined as a 48 hours period with no reintubation requirement. RESULTS: No significant differences were identified between the groups for the analyzed variables, except for the mean airway pressure. A significant association was shown between spontaneous breathing trial and successful extubation. CONCLUSION: The significant association between SBT and extubation success may contribute for prediction of successful weaning in preterm infants.
-
Original Articles
Acute kidney injury in children: incidence and prognostic factors in critical ill patients
Rev Bras Ter Intensiva. 2010;22(2):166-174
Abstract
Original ArticlesAcute kidney injury in children: incidence and prognostic factors in critical ill patients
Rev Bras Ter Intensiva. 2010;22(2):166-174
DOI 10.1590/S0103-507X2010000200011
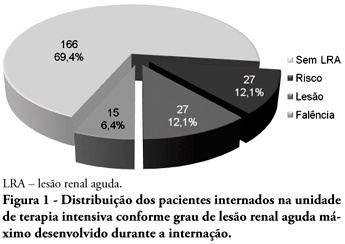
Views0See moreOBJECTIVES: Acute kidney injury is characterized by sudden and generally revertible renal function impairment involving inability to maintain homeostasis. In pediatrics, the main causes of acute kidney injury are sepsis, use of nephrotoxic drugs and renal ischemia in critically ill patients. The incidence of acute kidney injury in these patients ranges from 20 to 30%, resulting in increased morbid-mortality, a 40 to 90% rate. This study aimed to evaluate the incidence of acute kidney injury in intensive care unit patients, to categorize the severity of the acute kidney injury according to the Pediatric Risk, Injury, Failure, Loss, End-Stage (pRIFLE), examine the relationship between the acute kidney injury and severity using the Pediatric Index of Mortality (PIM) and to analyze outcome predictors. METHODS: A prospective study of the patients admitted to the intensive care unit of Hospital Infantil Joana de Gusmão – Florianópolis / SC – Brazil was conducted between July 2008 and January 2009. Were evaluated daily the urine output and serum creatinine, and the patients were categorized according to the pRIFLE criteria. RESULTS: During the follow-up period, 235 children were admitted. The incidence of acute kidney injury was 30.6%, and the maximal pRIFLE score during hospitalization was 12.1% for R, 12.1% for I and 6.4% for F. The mortality rate was 12.3%. The patients who developed acute kidney injury had a ten times bigger risk of death versus the not exposed patients. CONCLUSIONS: Acute kidney injury is frequent in critically ill patients. Early diagnosis and prompt and appropriate therapy for each clinical aspect may change this condition’s course and severity, and reduce the patients’ morbidity and mortality.
Views0Abstract
Original ArticlesAcute kidney injury in children: incidence and prognostic factors in critical ill patients
Rev Bras Ter Intensiva. 2010;22(2):166-174
DOI 10.1590/S0103-507X2010000200011
Views0See moreOBJECTIVES: Acute kidney injury is characterized by sudden and generally revertible renal function impairment involving inability to maintain homeostasis. In pediatrics, the main causes of acute kidney injury are sepsis, use of nephrotoxic drugs and renal ischemia in critically ill patients. The incidence of acute kidney injury in these patients ranges from 20 to 30%, resulting in increased morbid-mortality, a 40 to 90% rate. This study aimed to evaluate the incidence of acute kidney injury in intensive care unit patients, to categorize the severity of the acute kidney injury according to the Pediatric Risk, Injury, Failure, Loss, End-Stage (pRIFLE), examine the relationship between the acute kidney injury and severity using the Pediatric Index of Mortality (PIM) and to analyze outcome predictors. METHODS: A prospective study of the patients admitted to the intensive care unit of Hospital Infantil Joana de Gusmão – Florianópolis / SC – Brazil was conducted between July 2008 and January 2009. Were evaluated daily the urine output and serum creatinine, and the patients were categorized according to the pRIFLE criteria. RESULTS: During the follow-up period, 235 children were admitted. The incidence of acute kidney injury was 30.6%, and the maximal pRIFLE score during hospitalization was 12.1% for R, 12.1% for I and 6.4% for F. The mortality rate was 12.3%. The patients who developed acute kidney injury had a ten times bigger risk of death versus the not exposed patients. CONCLUSIONS: Acute kidney injury is frequent in critically ill patients. Early diagnosis and prompt and appropriate therapy for each clinical aspect may change this condition’s course and severity, and reduce the patients’ morbidity and mortality.
-
Original Articles
Applicability of the prevention protocol of pressure ulcers in intensive care unit
Rev Bras Ter Intensiva. 2010;22(2):175-185
Abstract
Original ArticlesApplicability of the prevention protocol of pressure ulcers in intensive care unit
Rev Bras Ter Intensiva. 2010;22(2):175-185
DOI 10.1590/S0103-507X2010000200012
Views0See moreOBJECTIVE: The avoidance of pressure ulcers development in critically ill patients is a major nursing challenge. Prevention is thus relevant for assurance of high quality care. This study aimed to evaluate the applicability of the Braden scale in intensive care unit patients. METHODS: This was a prospective study based which evaluated all adult patients staying in the intensive care unit from July 14 to August 10, 2009. The data were collected using the Braden’s scale by three examiners who identified the pressure ulcer development risk. The data were analyzed using the SAS Statistical Software. For determination of the examiners’ rates degree of coincidence, the Kappa value was used (95%CI). RESULTS: Regarding the related risk factors: 36.4% had mild sensory perception impairment; 50.9% had occasionally moist skin; 97.3% bedfast; 39.1% had very limited mobility; 45% probably had inappropriate nutrition; 61.8% had friction and shear problems. An agreement between the examiners was identified for nutrition and physical activity (38.1% to 100.0%); the Kappa population zero hypothesis was rejected; a paired examiners agreement (41.7% to 100.0%) was identified for the items humidity and physical activity, and the Kappa values ranged from 0.13 to 1. CONCLUSIONS: These intensive care patients were identified to have increased risk of developing pressure ulcers. This tool was considered appropriate to support the implementation of preventive measures.
Views0Abstract
Original ArticlesApplicability of the prevention protocol of pressure ulcers in intensive care unit
Rev Bras Ter Intensiva. 2010;22(2):175-185
DOI 10.1590/S0103-507X2010000200012
Views0See moreOBJECTIVE: The avoidance of pressure ulcers development in critically ill patients is a major nursing challenge. Prevention is thus relevant for assurance of high quality care. This study aimed to evaluate the applicability of the Braden scale in intensive care unit patients. METHODS: This was a prospective study based which evaluated all adult patients staying in the intensive care unit from July 14 to August 10, 2009. The data were collected using the Braden’s scale by three examiners who identified the pressure ulcer development risk. The data were analyzed using the SAS Statistical Software. For determination of the examiners’ rates degree of coincidence, the Kappa value was used (95%CI). RESULTS: Regarding the related risk factors: 36.4% had mild sensory perception impairment; 50.9% had occasionally moist skin; 97.3% bedfast; 39.1% had very limited mobility; 45% probably had inappropriate nutrition; 61.8% had friction and shear problems. An agreement between the examiners was identified for nutrition and physical activity (38.1% to 100.0%); the Kappa population zero hypothesis was rejected; a paired examiners agreement (41.7% to 100.0%) was identified for the items humidity and physical activity, and the Kappa values ranged from 0.13 to 1. CONCLUSIONS: These intensive care patients were identified to have increased risk of developing pressure ulcers. This tool was considered appropriate to support the implementation of preventive measures.
-
Original Articles
Applicability of bag squeezing and zeep maneuvers in mechanically ventilated patients
Rev Bras Ter Intensiva. 2010;22(2):186-191
Abstract
Original ArticlesApplicability of bag squeezing and zeep maneuvers in mechanically ventilated patients
Rev Bras Ter Intensiva. 2010;22(2):186-191
DOI 10.1590/S0103-507X2010000200013
Views0See moreOBJECTIVES: To evaluate the applicability of the bag squeezing and zeep maneuvers in mechanically ventilated patients. METHODS: Twenty stable mechanically ventilated patients were studied. All patients were randomly allocated to either bag squeezing techinique followed by zeep maneuver, or the reversed sequence. Each group crossed to the other sequence four hours later. Heart rate, respiratory rate, peripheral oxygen saturation and blood pressure were measured before, during and after each technique use. The suctioned secretions were collected and measured. The data were analyzed by pairwise statistical analysis for inter-group comparisons, and ANOVA for each group results analysis. RESULTS: The heart rate was significantly increased, from 92.6 ± 18.3 bpm to 99.8 ± 18.5 bpm and the peripheral oxygen saturation significantly decreased from 96.9 ± 3.0% to 94.5 ± 4.3% during the bag squeezing maneuver, although the values remained within the normal range. No significant changes were seen for the zeep maneuver. Peripheral oxygen saturation during the maneuvers was found to change when the techniques were compared. No differences were found for the suctionedsecretions amounts. CONCLUSION: The results suggest that both techniques are feasible as they cause few hemodynamic changes, and both are effective for bronchial secretions removal.
Views0Abstract
Original ArticlesApplicability of bag squeezing and zeep maneuvers in mechanically ventilated patients
Rev Bras Ter Intensiva. 2010;22(2):186-191
DOI 10.1590/S0103-507X2010000200013
Views0See moreOBJECTIVES: To evaluate the applicability of the bag squeezing and zeep maneuvers in mechanically ventilated patients. METHODS: Twenty stable mechanically ventilated patients were studied. All patients were randomly allocated to either bag squeezing techinique followed by zeep maneuver, or the reversed sequence. Each group crossed to the other sequence four hours later. Heart rate, respiratory rate, peripheral oxygen saturation and blood pressure were measured before, during and after each technique use. The suctioned secretions were collected and measured. The data were analyzed by pairwise statistical analysis for inter-group comparisons, and ANOVA for each group results analysis. RESULTS: The heart rate was significantly increased, from 92.6 ± 18.3 bpm to 99.8 ± 18.5 bpm and the peripheral oxygen saturation significantly decreased from 96.9 ± 3.0% to 94.5 ± 4.3% during the bag squeezing maneuver, although the values remained within the normal range. No significant changes were seen for the zeep maneuver. Peripheral oxygen saturation during the maneuvers was found to change when the techniques were compared. No differences were found for the suctionedsecretions amounts. CONCLUSION: The results suggest that both techniques are feasible as they cause few hemodynamic changes, and both are effective for bronchial secretions removal.
-
Original Articles
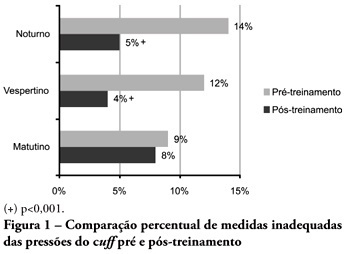
Cuff pressure control in intensive care unit: training effects
Rev Bras Ter Intensiva. 2010;22(2):192-195
Abstract
Original ArticlesCuff pressure control in intensive care unit: training effects
Rev Bras Ter Intensiva. 2010;22(2):192-195
DOI 10.1590/S0103-507X2010000200014
Views0See moreOBJECTIVES: Direct cuff pressure to the tracheal wall can cause damage. This paper aimed to verify the effectiveness of nursing team training on cuff pressure control. METHODS: A retrospective survey was initially made on the records of cuff pressure measurements from January 2007 to June 2008 and the inadequacy percent was verified. Next, a nursing team training program was provided involving all nursing shift teams during June 2008, and after the training the appropriate cuff pressures proportion was prospectively recorded between June and December 2008. The proportion of inappropriate cuff pressure was compared between the work shifts (morning, afternoon and evening-night) and between pre- and post-training, using the qualitative Chi-square test. The 5% limit (p<0.05) was considered for significant differences. RESULTS: For the pre-training period, inappropriate cuff pressure measures (over 30cmH2O) during morning, afternoon and evening-night shifts were 9.2%, 11.9% and 13.7%, respectively. For the post-training phase, 7.6%, 4.1% and 5.2% inappropriate cuff-pressures were identified for the morning, afternoon and evening-night shifts, respectively, with a significant reduction for the afternoon and evening-night shifts, respectively (p<0.001). CONCLUSION: Nursing team training was effective for inadequate cuff pressure harms awareness improvement, and resulted in safer pressure levels.
Views0Abstract
Original ArticlesCuff pressure control in intensive care unit: training effects
Rev Bras Ter Intensiva. 2010;22(2):192-195
DOI 10.1590/S0103-507X2010000200014
Views0See moreOBJECTIVES: Direct cuff pressure to the tracheal wall can cause damage. This paper aimed to verify the effectiveness of nursing team training on cuff pressure control. METHODS: A retrospective survey was initially made on the records of cuff pressure measurements from January 2007 to June 2008 and the inadequacy percent was verified. Next, a nursing team training program was provided involving all nursing shift teams during June 2008, and after the training the appropriate cuff pressures proportion was prospectively recorded between June and December 2008. The proportion of inappropriate cuff pressure was compared between the work shifts (morning, afternoon and evening-night) and between pre- and post-training, using the qualitative Chi-square test. The 5% limit (p<0.05) was considered for significant differences. RESULTS: For the pre-training period, inappropriate cuff pressure measures (over 30cmH2O) during morning, afternoon and evening-night shifts were 9.2%, 11.9% and 13.7%, respectively. For the post-training phase, 7.6%, 4.1% and 5.2% inappropriate cuff-pressures were identified for the morning, afternoon and evening-night shifts, respectively, with a significant reduction for the afternoon and evening-night shifts, respectively (p<0.001). CONCLUSION: Nursing team training was effective for inadequate cuff pressure harms awareness improvement, and resulted in safer pressure levels.
-
Review Articles
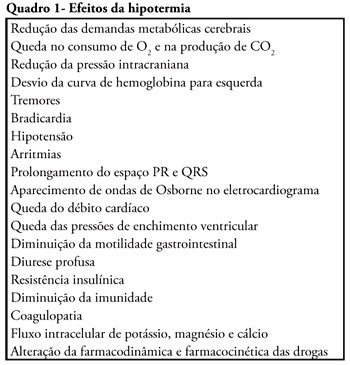
Mild therapeutic hypothermia after cardiac arrest: mechanism of action and protocol development
Rev Bras Ter Intensiva. 2010;22(2):196-205
Abstract
Review ArticlesMild therapeutic hypothermia after cardiac arrest: mechanism of action and protocol development
Rev Bras Ter Intensiva. 2010;22(2):196-205
DOI 10.1590/S0103-507X2010000200015
Views1See moreCardiac arrest is a high mortality event and the associated brain ischemia frequently causes severe neurological damage and persistent vegetative state. Therapeutic hypothermia is an important tool for the treatment of post-anoxic coma after cardiopulmonary resuscitation. It has been shown to reduce mortality and to improve neurological outcomes after cardiac arrest. Nevertheless, hypothermia is underused in critical care units. This manuscript aims to review the hypothermia mechanism of action in cardiac arrest survivors and to propose a simple protocol, feasible to be implemented in any critical care unit.
Views1Abstract
Review ArticlesMild therapeutic hypothermia after cardiac arrest: mechanism of action and protocol development
Rev Bras Ter Intensiva. 2010;22(2):196-205
DOI 10.1590/S0103-507X2010000200015
Views1See moreCardiac arrest is a high mortality event and the associated brain ischemia frequently causes severe neurological damage and persistent vegetative state. Therapeutic hypothermia is an important tool for the treatment of post-anoxic coma after cardiopulmonary resuscitation. It has been shown to reduce mortality and to improve neurological outcomes after cardiac arrest. Nevertheless, hypothermia is underused in critical care units. This manuscript aims to review the hypothermia mechanism of action in cardiac arrest survivors and to propose a simple protocol, feasible to be implemented in any critical care unit.
-
Review Articles
Mechanisms underlying uremic encephalopathy
Rev Bras Ter Intensiva. 2010;22(2):206-211
Abstract
Review ArticlesMechanisms underlying uremic encephalopathy
Rev Bras Ter Intensiva. 2010;22(2):206-211
DOI 10.1590/S0103-507X2010000200016
Views0See moreIn patients with renal failure, encephalopathy is a common problem that may be caused by uremia, thiamine deficiency, dialysis, transplant rejection, hypertension, fluid and electrolyte disturbances or drug toxicity. In general, encephalopathy presents with a symptom complex progressing from mild sensorial clouding to delirium and coma. This review discusses important issues regarding the mechanisms underlying the pathophysiology of uremic encephalopathy. The pathophysiology of uremic encephalopathy up to now is uncertain, but several factors have been postulated to be involved; it is a complex and probably multifactorial process. Hormonal disturbances, oxidative stress, accumulation of metabolites, imbalance in excitatory and inhibitory neurotransmitters, and disturbance of the intermediary metabolism have been identified as contributing factors. Despite continuous therapeutic progress, most neurological complications of uremia, like uremic encephalopathy, fail to fully respond to dialysis and many are elicited or aggravated by dialysis or renal transplantation. On the other hand, previous studies showed that antioxidant therapy could be used as an adjuvant therapy for the treatment of these neurological complications.
Views0Abstract
Review ArticlesMechanisms underlying uremic encephalopathy
Rev Bras Ter Intensiva. 2010;22(2):206-211
DOI 10.1590/S0103-507X2010000200016
Views0See moreIn patients with renal failure, encephalopathy is a common problem that may be caused by uremia, thiamine deficiency, dialysis, transplant rejection, hypertension, fluid and electrolyte disturbances or drug toxicity. In general, encephalopathy presents with a symptom complex progressing from mild sensorial clouding to delirium and coma. This review discusses important issues regarding the mechanisms underlying the pathophysiology of uremic encephalopathy. The pathophysiology of uremic encephalopathy up to now is uncertain, but several factors have been postulated to be involved; it is a complex and probably multifactorial process. Hormonal disturbances, oxidative stress, accumulation of metabolites, imbalance in excitatory and inhibitory neurotransmitters, and disturbance of the intermediary metabolism have been identified as contributing factors. Despite continuous therapeutic progress, most neurological complications of uremia, like uremic encephalopathy, fail to fully respond to dialysis and many are elicited or aggravated by dialysis or renal transplantation. On the other hand, previous studies showed that antioxidant therapy could be used as an adjuvant therapy for the treatment of these neurological complications.
Volume Articles - Critical Care Science (CCS)
