Hypothermia Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(1):111-118
DOI 10.5935/0103-507X.20210012
To evaluate the incidence of hypothermia in patients undergoing continuous renal replacement therapy in the intensive care unit. As secondary objectives, we determined associated factors and compared the occurrence of hypothermia between two modalities of continuous renal replacement therapy.
A prospective cohort study was conducted with adult patients who were admitted to a clinical-surgical intensive care unit and underwent continuous renal replacement therapy in a high-complexity public university hospital in southern Brazil from April 2017 to July 2018. Hypothermia was defined as a body temperature ≤ 35ºC. The patients included in the study were followed for the first 48 hours of continuous renal replacement therapy. The researchers collected data from medical records and continuous renal replacement therapy records.
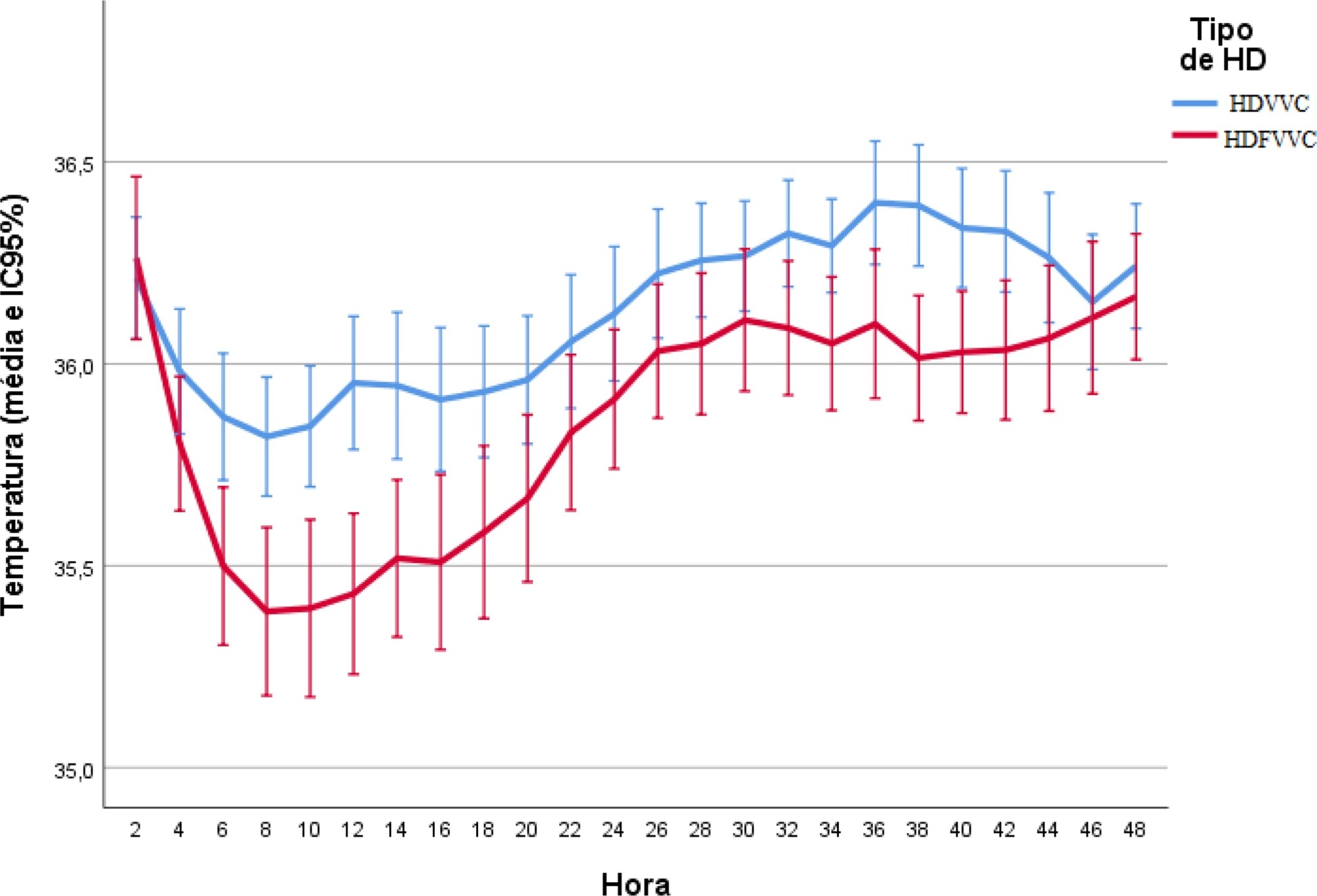
A total of 186 patients were equally distributed between two types of continuous renal replacement therapy: hemodialysis and hemodiafiltration. The incidence of hypothermia was 52.7% and was higher in patients admitted for shock (relative risk of 2.11; 95%CI 1.21 - 3.69; p = 0.009) and in those who underwent hemodiafiltration with heating in the return line (relative risk of 1.50; 95%CI 1.13 - 1.99; p = 0.005).
Hypothermia in critically ill patients with continuous renal replacement therapy is frequent, and the intensive care team should be attentive, especially when there are associated risk factors.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):111-118
DOI 10.5935/0103-507X.20210012
To evaluate the incidence of hypothermia in patients undergoing continuous renal replacement therapy in the intensive care unit. As secondary objectives, we determined associated factors and compared the occurrence of hypothermia between two modalities of continuous renal replacement therapy.
A prospective cohort study was conducted with adult patients who were admitted to a clinical-surgical intensive care unit and underwent continuous renal replacement therapy in a high-complexity public university hospital in southern Brazil from April 2017 to July 2018. Hypothermia was defined as a body temperature ≤ 35ºC. The patients included in the study were followed for the first 48 hours of continuous renal replacement therapy. The researchers collected data from medical records and continuous renal replacement therapy records.
A total of 186 patients were equally distributed between two types of continuous renal replacement therapy: hemodialysis and hemodiafiltration. The incidence of hypothermia was 52.7% and was higher in patients admitted for shock (relative risk of 2.11; 95%CI 1.21 - 3.69; p = 0.009) and in those who underwent hemodiafiltration with heating in the return line (relative risk of 1.50; 95%CI 1.13 - 1.99; p = 0.005).
Hypothermia in critically ill patients with continuous renal replacement therapy is frequent, and the intensive care team should be attentive, especially when there are associated risk factors.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):72-76
DOI 10.5935/0103-507X.20150012
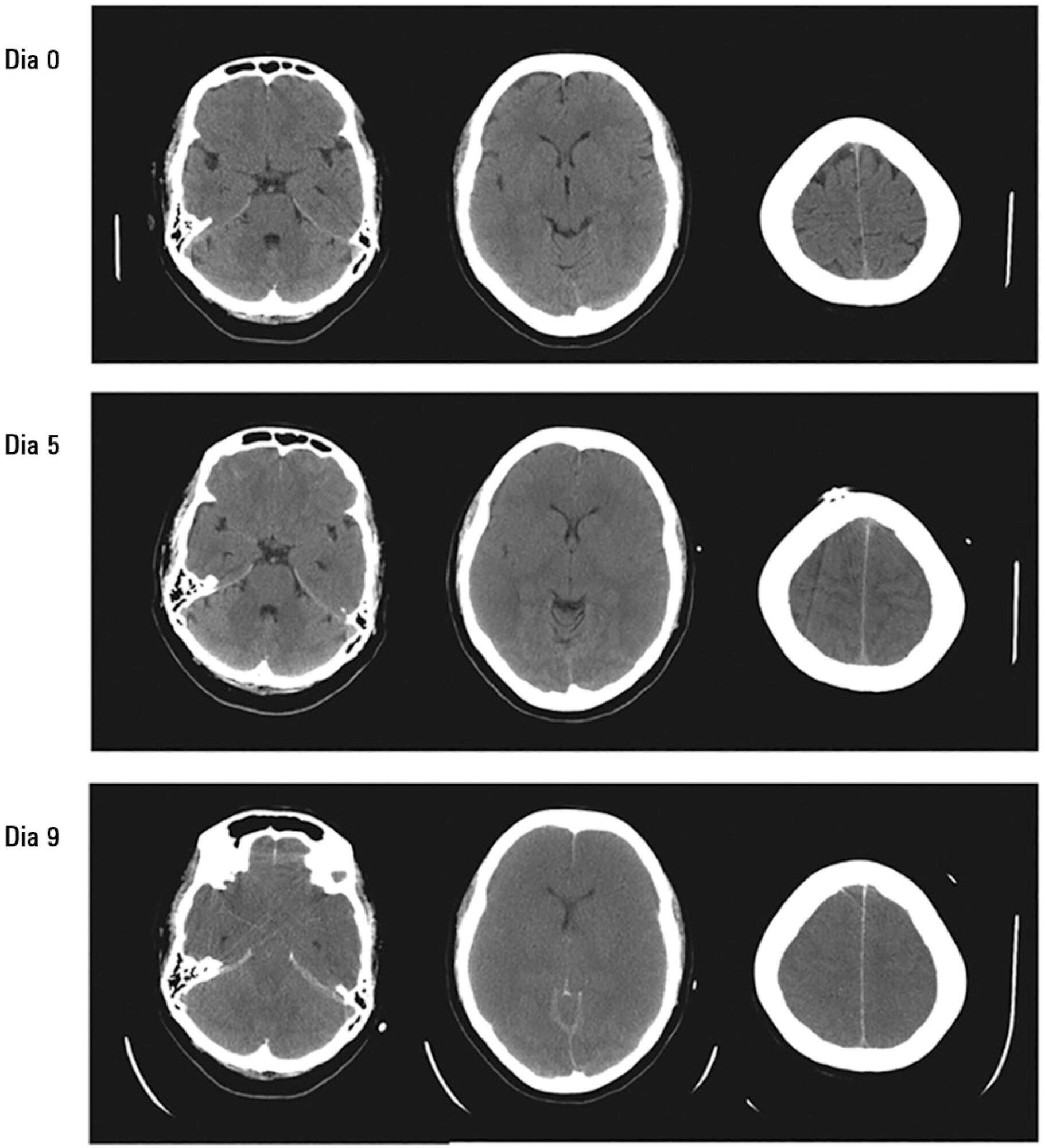
The most important topics in fulminant hepatic failure are cerebral edema and intracranial hypertension. Among all therapeutic options, systemic induced hypothermia to 33 - 34ºC has been reported to reduce the high pressure and increase the time during which patients can tolerate a graft. This review discusses the indications and adverse effects of hypothermia.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):72-76
DOI 10.5935/0103-507X.20150012
The most important topics in fulminant hepatic failure are cerebral edema and intracranial hypertension. Among all therapeutic options, systemic induced hypothermia to 33 - 34ºC has been reported to reduce the high pressure and increase the time during which patients can tolerate a graft. This review discusses the indications and adverse effects of hypothermia.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):369-375
DOI 10.1590/S0103-507X2009000400006
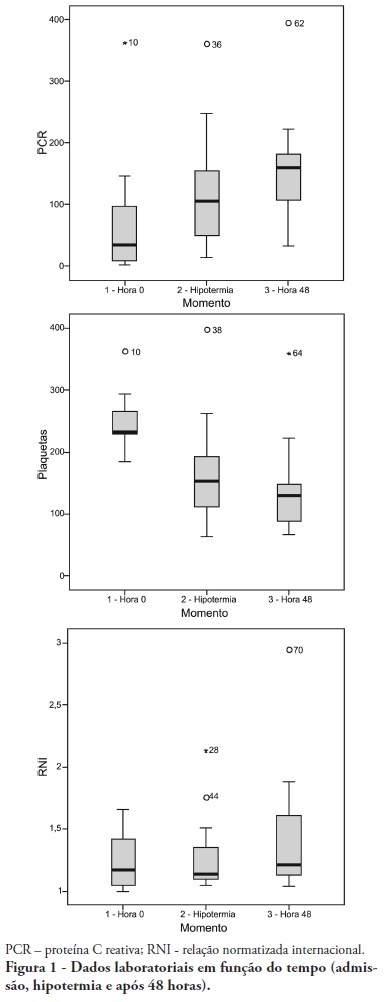
OBJECTIVE: To determine the characteristics of patients undergoing standard institutional protocol for management of resuscitated patients after a cardiac arrest episode, including therapeutic hypothermia. METHODS: This was a retrospective analysis of 26 consecutive patients admitted following cardiac arrest, between January 2007 and November 2008. RESULTS: All cases underwent therapeutic hypothermia. Average age was 63 years, and the patients were predominantly male. Cardiac arrest event was out-of-hospital in 8 cases, in the emergency room in 3 cases, in the wards in 13 cases and in the operation room in 2 cases. The cardiac arrest rhythm was ventricular fibrillation in seven patients, asystolia in 11, pulseless electrical activity in 5 cases, and was undetermined in 3 patients. The interval between the cardiac arrest and return of spontaneous circulation was 12 minutes (SD ± 5 min). The time to reach the target temperature was 5 ± 4 hours, the hypothermia time was 22 ± 6 hours and time to rewarming 9 ± 5.9 hours. Fourteen patients died in the intensive care unit, a 54% mortality, and three patients died during the in-hospital stay, a 66% in-hospital mortality. There was statistically significant reduction in hemoglobin (p<0.001), leukocytes (p=0.001), platelets (p<0.001), lactate (p<0.001) and potassium (p=0.009), values and increased C reactive protein (p=0.001) and INR (p=0.004) after hypothermia. CONCLUSIONS: The creation of a standard operative protocol for therapeutic hypothermia in post cardiac arrest patients management resulted in a high use of therapeutic hypothermia. The clinical results of this protocol adapted from randomized studies are similar to the literature.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):369-375
DOI 10.1590/S0103-507X2009000400006
OBJECTIVE: To determine the characteristics of patients undergoing standard institutional protocol for management of resuscitated patients after a cardiac arrest episode, including therapeutic hypothermia. METHODS: This was a retrospective analysis of 26 consecutive patients admitted following cardiac arrest, between January 2007 and November 2008. RESULTS: All cases underwent therapeutic hypothermia. Average age was 63 years, and the patients were predominantly male. Cardiac arrest event was out-of-hospital in 8 cases, in the emergency room in 3 cases, in the wards in 13 cases and in the operation room in 2 cases. The cardiac arrest rhythm was ventricular fibrillation in seven patients, asystolia in 11, pulseless electrical activity in 5 cases, and was undetermined in 3 patients. The interval between the cardiac arrest and return of spontaneous circulation was 12 minutes (SD ± 5 min). The time to reach the target temperature was 5 ± 4 hours, the hypothermia time was 22 ± 6 hours and time to rewarming 9 ± 5.9 hours. Fourteen patients died in the intensive care unit, a 54% mortality, and three patients died during the in-hospital stay, a 66% in-hospital mortality. There was statistically significant reduction in hemoglobin (p<0.001), leukocytes (p=0.001), platelets (p<0.001), lactate (p<0.001) and potassium (p=0.009), values and increased C reactive protein (p=0.001) and INR (p=0.004) after hypothermia. CONCLUSIONS: The creation of a standard operative protocol for therapeutic hypothermia in post cardiac arrest patients management resulted in a high use of therapeutic hypothermia. The clinical results of this protocol adapted from randomized studies are similar to the literature.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):190-196
DOI 10.1590/S0103-507X2008000200013
BACKGROUND AND OBJECTIVES: Out-of-hospital cardiac arrest is a major cause of death with survival rates as low as 5% to 35%. A large number of patients who survive resuscitation will face significant neurological damage, as a result of the ischemia that occurs both during cardiac arrest and reperfusion. However understanding of the mechanisms responsible for brain damage has not resulted in prognostic improvement. Therapeutic hypothermia after resuscitation may be a valid option associated to reduction of neurological damage. The purpose of this study was to review scientific evidence related to a therapy for patients resuscitated from cardiac arrest. CONTENTS: Description and analysis of the main risk factors associated with neurological damage after resuscitation from cardiac arrest as well as prognostic criteria was carried out. A non-systematic search was conducted in the PubMed data base for papers on a therapeutic approach for patients resuscitated from cardiac arrest. Bibliographic references of reviewed papers were also analyzed. Practical rules were drafted for such an approach. CONCLUSIONS: Patients resuscitated from cardiac arrest face a high level of risk of neurological damage. Therapeutic hypothermia and control of physiological parameters to optimise brain perfusion, may improve prognosis.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):190-196
DOI 10.1590/S0103-507X2008000200013
BACKGROUND AND OBJECTIVES: Out-of-hospital cardiac arrest is a major cause of death with survival rates as low as 5% to 35%. A large number of patients who survive resuscitation will face significant neurological damage, as a result of the ischemia that occurs both during cardiac arrest and reperfusion. However understanding of the mechanisms responsible for brain damage has not resulted in prognostic improvement. Therapeutic hypothermia after resuscitation may be a valid option associated to reduction of neurological damage. The purpose of this study was to review scientific evidence related to a therapy for patients resuscitated from cardiac arrest. CONTENTS: Description and analysis of the main risk factors associated with neurological damage after resuscitation from cardiac arrest as well as prognostic criteria was carried out. A non-systematic search was conducted in the PubMed data base for papers on a therapeutic approach for patients resuscitated from cardiac arrest. Bibliographic references of reviewed papers were also analyzed. Practical rules were drafted for such an approach. CONCLUSIONS: Patients resuscitated from cardiac arrest face a high level of risk of neurological damage. Therapeutic hypothermia and control of physiological parameters to optimise brain perfusion, may improve prognosis.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)