-
Outcome of influenza A (H1N1) patients admitted to intensive care units in the Paraná state, Brazil
Rev Bras Ter Intensiva. 2009;21(3):231-236
Abstract
Outcome of influenza A (H1N1) patients admitted to intensive care units in the Paraná state, Brazil
Rev Bras Ter Intensiva. 2009;21(3):231-236
DOI 10.1590/S0103-507X2009000300001
Views3See moreOBJECTIVE: This study aimed to analyze outcome, clinical and epidemiological characteristics and severity factors in adult patients admitted with a diagnosis of infection by virus A (H1N1) to public and private intensive care units, in Paraná, Brazil. METHODS: Cohort study of medical charts of patients older than 12 years admitted to 11 intensive care units in 6 cities in the state of Parana, Brazil, during a period of 45 days, with diagnosis of swine influenza. The diagnosis of infection with A (H1N1) was made by real time polymerase chain reaction (RT-PCR) of nasopharyngeal secretion, or strong clinical suspicion when other causes had been ruled out (even with negative RT-PCR). Descriptive statistics were performed, analysis by the Chi square test was used to compare percentages and the Student’s t test for continuous variables with univariate analysis, assuming a significance level of p <0.05. RESULTS: There were 63 adult patients admitted with a diagnosis of H1N1, 37 (58.7%) being RT-PCR positive. Most patients were young adults (65% under 40 years of age) with no gender predominance and high incidence of obesity (27.0% with Body Mass Index > 30). Mean of the Acute Physiologic Chronic Health Evaluation II (APACHE II) score was 15.0 + 8.1. Mortality in the intensive care unit was 39.7%. The main factors associated with mortality were: positive RT-PCR, low levels of initial PaO2/FiO2, high initial levels of urea and lactate dehydrogenase, required level of positive end expiratory pressure, need for the prone position and vasopressors. CONCLUSIONS: Adult patients with A (H1N1) virus infection admitted to intensive care units had a high risk of death, particularly due to respiratory impairment. Positive RT-PCR, urea and lactic dehydrogenase, low initial PaO2/FiO2 and high levels of PEEP were correlated with higher mortality.
Views3

Abstract
Outcome of influenza A (H1N1) patients admitted to intensive care units in the Paraná state, Brazil
Rev Bras Ter Intensiva. 2009;21(3):231-236
DOI 10.1590/S0103-507X2009000300001
Views3See moreOBJECTIVE: This study aimed to analyze outcome, clinical and epidemiological characteristics and severity factors in adult patients admitted with a diagnosis of infection by virus A (H1N1) to public and private intensive care units, in Paraná, Brazil. METHODS: Cohort study of medical charts of patients older than 12 years admitted to 11 intensive care units in 6 cities in the state of Parana, Brazil, during a period of 45 days, with diagnosis of swine influenza. The diagnosis of infection with A (H1N1) was made by real time polymerase chain reaction (RT-PCR) of nasopharyngeal secretion, or strong clinical suspicion when other causes had been ruled out (even with negative RT-PCR). Descriptive statistics were performed, analysis by the Chi square test was used to compare percentages and the Student’s t test for continuous variables with univariate analysis, assuming a significance level of p <0.05. RESULTS: There were 63 adult patients admitted with a diagnosis of H1N1, 37 (58.7%) being RT-PCR positive. Most patients were young adults (65% under 40 years of age) with no gender predominance and high incidence of obesity (27.0% with Body Mass Index > 30). Mean of the Acute Physiologic Chronic Health Evaluation II (APACHE II) score was 15.0 + 8.1. Mortality in the intensive care unit was 39.7%. The main factors associated with mortality were: positive RT-PCR, low levels of initial PaO2/FiO2, high initial levels of urea and lactate dehydrogenase, required level of positive end expiratory pressure, need for the prone position and vasopressors. CONCLUSIONS: Adult patients with A (H1N1) virus infection admitted to intensive care units had a high risk of death, particularly due to respiratory impairment. Positive RT-PCR, urea and lactic dehydrogenase, low initial PaO2/FiO2 and high levels of PEEP were correlated with higher mortality.
-
Pulmonary embolism: multicenter registry in tertiary hospitals
Rev Bras Ter Intensiva. 2009;21(3):237-246
Abstract
Pulmonary embolism: multicenter registry in tertiary hospitals
Rev Bras Ter Intensiva. 2009;21(3):237-246
DOI 10.1590/S0103-507X2009000300002
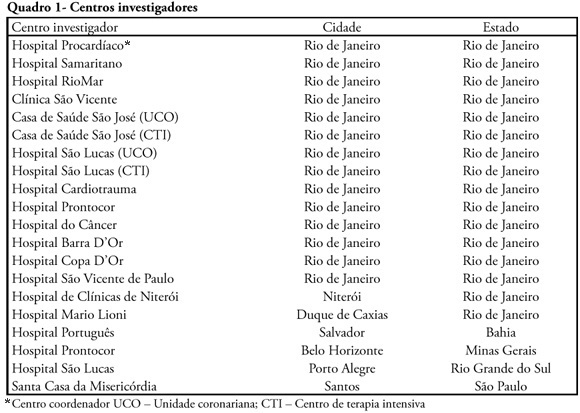
Views0See moreINTRODUCTION: The clinical profile as well as the therapeutic and diagnostic strategies for patients with pulmonary embolism, describes clinical practice in the approach of the disease. Such information, scarce in national studies, enables a better understanding of pulmonary embolism. METHODS: A multicenter trial included 727 patients with pulmonary embolism who were admitted in emergency or intensive care unit. Diagnostic criteria for inclusion were: 1. Visibility of thrombus in the pulmonary artery at pulmonary arteriography, helical computer tomography, magnetic resonance or echocardiogram. 2. High probability at pulmonary scintigraphy. 3. Venous duplex-scan with thrombus and clinical manifestations of pulmonary embolism. Clinical and complementary exams were analyzed. RESULTS: Mean age was 68 years, 42% were male. Most prevalent risk factors were: age>40 years, bed rest and neoplasm. More frequent signs and symptoms were: dyspnea, tachypnea, sinus tachycardia, and chest pain. Changes were observed at electrocardiogram in 30%, at chest X-ray in 45%, at venous duplex-scan in 67%, at transthoracic echocardiogram in 37%. . D-dimer, troponin I and CKMB were positive in, respectively, 93, 9 and 8%. Most frequently used methods to confirm diagnosis were helical computer tomography and non-fractioned heparin was the treatment most used. In-hospital mortality was 19.5%. CONCLUSIONS: It was observed that age>40 years, prolonged rest and neoplasms were the most prevalent risk factors and dyspnea and tachypnea were the more frequent clinical manifestations. Helical computer tomography was the most often used method to confirm diagnosis and non-fractioned heparin was the main form of treatment.
Views0Abstract
Pulmonary embolism: multicenter registry in tertiary hospitals
Rev Bras Ter Intensiva. 2009;21(3):237-246
DOI 10.1590/S0103-507X2009000300002
Views0See moreINTRODUCTION: The clinical profile as well as the therapeutic and diagnostic strategies for patients with pulmonary embolism, describes clinical practice in the approach of the disease. Such information, scarce in national studies, enables a better understanding of pulmonary embolism. METHODS: A multicenter trial included 727 patients with pulmonary embolism who were admitted in emergency or intensive care unit. Diagnostic criteria for inclusion were: 1. Visibility of thrombus in the pulmonary artery at pulmonary arteriography, helical computer tomography, magnetic resonance or echocardiogram. 2. High probability at pulmonary scintigraphy. 3. Venous duplex-scan with thrombus and clinical manifestations of pulmonary embolism. Clinical and complementary exams were analyzed. RESULTS: Mean age was 68 years, 42% were male. Most prevalent risk factors were: age>40 years, bed rest and neoplasm. More frequent signs and symptoms were: dyspnea, tachypnea, sinus tachycardia, and chest pain. Changes were observed at electrocardiogram in 30%, at chest X-ray in 45%, at venous duplex-scan in 67%, at transthoracic echocardiogram in 37%. . D-dimer, troponin I and CKMB were positive in, respectively, 93, 9 and 8%. Most frequently used methods to confirm diagnosis were helical computer tomography and non-fractioned heparin was the treatment most used. In-hospital mortality was 19.5%. CONCLUSIONS: It was observed that age>40 years, prolonged rest and neoplasms were the most prevalent risk factors and dyspnea and tachypnea were the more frequent clinical manifestations. Helical computer tomography was the most often used method to confirm diagnosis and non-fractioned heparin was the main form of treatment.
-
Individual prognostic assessment in the intensive care unit: can therapeutic persistence be distinguished from therapeutic obstinacy?
Rev Bras Ter Intensiva. 2009;21(3):247-254
Abstract
Individual prognostic assessment in the intensive care unit: can therapeutic persistence be distinguished from therapeutic obstinacy?
Rev Bras Ter Intensiva. 2009;21(3):247-254
DOI 10.1590/S0103-507X2009000300003
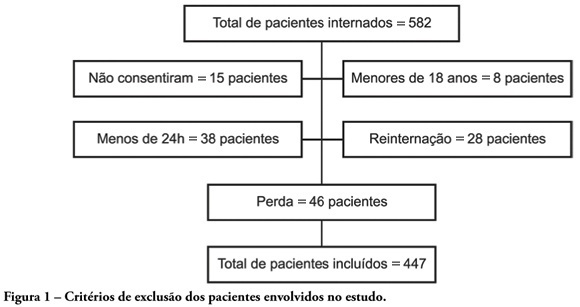
Views0See moreOBJECTIVES: Availability of state-of-the-art technology at intensive care units has often turned into a tool aggravating suffering by prolonging the end-of-life process. Distinguishing therapeutic persistence from therapeutic obstinacy has become a great challenge for present-day medicine. The aim of this study was to assess the benefit-harm relation in the use of life-sustaining therapies by means of an evolutionary system of individual prognostic assessment. METHODS: A cohort, prospective, observational study at the intensive care unit of the São Francisco De Paula University Hospital of UCPel, Pelotas RS from March 2006 to August 31, 2007. Individual prognostic assessments were recorded by using an evolutionary system, the UNICAMP II index, associated with albumin transferrin and lymphocytes serum levels, life- sustaining therapies and the outcome. Statistical analysis was carried out by the Student’s t-test, ANOVA test, Chi-square test, Fisher’s exact test, Spearman’s correlation test and area under the receiver-operating characteristic curve. A p value < 0.05 was considered statistically significant. RESULTS: Four hundred forty seven patients were assessed during the study. Prevalence of death was significantly higher among those who received life-sustaining therapies at a later stage of the intervention, and those whose prognostic index and nutritional status worsened at an early stage of intervention. CONCLUSION: Assessment of individual evolutionary prognostic proved to be a useful method to objectively subsidize ethical decisions related to therapeutic persistence and therapeutic obstinacy.
Views0Abstract
Individual prognostic assessment in the intensive care unit: can therapeutic persistence be distinguished from therapeutic obstinacy?
Rev Bras Ter Intensiva. 2009;21(3):247-254
DOI 10.1590/S0103-507X2009000300003
Views0See moreOBJECTIVES: Availability of state-of-the-art technology at intensive care units has often turned into a tool aggravating suffering by prolonging the end-of-life process. Distinguishing therapeutic persistence from therapeutic obstinacy has become a great challenge for present-day medicine. The aim of this study was to assess the benefit-harm relation in the use of life-sustaining therapies by means of an evolutionary system of individual prognostic assessment. METHODS: A cohort, prospective, observational study at the intensive care unit of the São Francisco De Paula University Hospital of UCPel, Pelotas RS from March 2006 to August 31, 2007. Individual prognostic assessments were recorded by using an evolutionary system, the UNICAMP II index, associated with albumin transferrin and lymphocytes serum levels, life- sustaining therapies and the outcome. Statistical analysis was carried out by the Student’s t-test, ANOVA test, Chi-square test, Fisher’s exact test, Spearman’s correlation test and area under the receiver-operating characteristic curve. A p value < 0.05 was considered statistically significant. RESULTS: Four hundred forty seven patients were assessed during the study. Prevalence of death was significantly higher among those who received life-sustaining therapies at a later stage of the intervention, and those whose prognostic index and nutritional status worsened at an early stage of intervention. CONCLUSION: Assessment of individual evolutionary prognostic proved to be a useful method to objectively subsidize ethical decisions related to therapeutic persistence and therapeutic obstinacy.
-
Prognostic factors in elderly patients admitted in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):255-261
Abstract
Prognostic factors in elderly patients admitted in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):255-261
DOI 10.1590/S0103-507X2009000300004
Views0See moreCurrently, aging of the population is a widespread global phenomenon. Therefore, the assessment of prognosis in elderly patients is needed. This study aims to identify risk factors in a population of elderly patients admitted in the intensive care unit METHODS: A prospective study in the intensive care unit of a general tertiary hospital was carried out for five months. Patients with 65 years or more of age, who stayed in the intensive care unit for 24 hours or more were included and those at the-end-of-life, patients readmitted to intensive care unit during the same hospital stay were excluded. RESULTS: In this study 199 patients were involved, with a mean age of 75.4±6.8 years, and 58.8% were female. Mortality was 57.3%. The mean APACHE II, SOFA, MODS and Katz index (assessment of daily activities) were respectively 20.0±5.8, 6.8±3.9, 2.4±1.9 and 5.3±1.6. Most patients were postoperative 59.3% and 41.6% were under invasive mechanical ventilation. At regression analysis, the independent determinants of higher mortality were: older age (76.9±6.7 years death versus 73.3±6.5 years discharge, P<0.001, OR=1.08, CI 95% 1.01-1. 16), the Katz index (4.9±1.9 deaths versus 5.7±0.9 discharge, p=0.001, OR=0.66, CI 95% 0.45-0.98), hyperglycemia (158.1±69.0 death versus 139.6±48.5 discharge p=0.041; OR=1.02; CI 95% 1.01-1.03) and need for mechanical ventilation at admission to the intensive care unit (57.0% death versus 20.5% discharge p <0.001, OR=3.57, CI 95% 1.24-10.3). CONCLUSION: Elderly patients admitted to the intensive care unit that have difficulties in performing daily activities, hyperglycemia and who are under invasive mechanical ventilation had a worse hospital prognosis.
Views0Abstract
Prognostic factors in elderly patients admitted in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):255-261
DOI 10.1590/S0103-507X2009000300004
Views0See moreCurrently, aging of the population is a widespread global phenomenon. Therefore, the assessment of prognosis in elderly patients is needed. This study aims to identify risk factors in a population of elderly patients admitted in the intensive care unit METHODS: A prospective study in the intensive care unit of a general tertiary hospital was carried out for five months. Patients with 65 years or more of age, who stayed in the intensive care unit for 24 hours or more were included and those at the-end-of-life, patients readmitted to intensive care unit during the same hospital stay were excluded. RESULTS: In this study 199 patients were involved, with a mean age of 75.4±6.8 years, and 58.8% were female. Mortality was 57.3%. The mean APACHE II, SOFA, MODS and Katz index (assessment of daily activities) were respectively 20.0±5.8, 6.8±3.9, 2.4±1.9 and 5.3±1.6. Most patients were postoperative 59.3% and 41.6% were under invasive mechanical ventilation. At regression analysis, the independent determinants of higher mortality were: older age (76.9±6.7 years death versus 73.3±6.5 years discharge, P<0.001, OR=1.08, CI 95% 1.01-1. 16), the Katz index (4.9±1.9 deaths versus 5.7±0.9 discharge, p=0.001, OR=0.66, CI 95% 0.45-0.98), hyperglycemia (158.1±69.0 death versus 139.6±48.5 discharge p=0.041; OR=1.02; CI 95% 1.01-1.03) and need for mechanical ventilation at admission to the intensive care unit (57.0% death versus 20.5% discharge p <0.001, OR=3.57, CI 95% 1.24-10.3). CONCLUSION: Elderly patients admitted to the intensive care unit that have difficulties in performing daily activities, hyperglycemia and who are under invasive mechanical ventilation had a worse hospital prognosis.
-
Aged patients with respiratory dysfunction: epidemiological profile and mortality risk factors
Rev Bras Ter Intensiva. 2009;21(3):262-268
Abstract
Aged patients with respiratory dysfunction: epidemiological profile and mortality risk factors
Rev Bras Ter Intensiva. 2009;21(3):262-268
DOI 10.1590/S0103-507X2009000300005
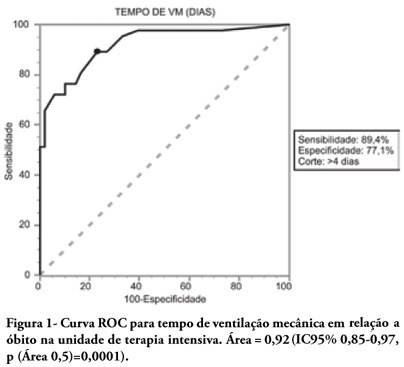
Views0See moreOBJECTIVES: To describe the population of aged as compared to young patients under mechanical ventilation and to analyze the mortality risk factors of this group in an intensive care unit. METHODS: This was a prospective observational trial in patients over 18 years of age, admitted in an intensive care unit and under mechanical ventilation, during one year. Patients were divided into two groups according to age: Group 1 – patients over 65 years old; and Group 2, 65 years old or younger. RESULTS: eighty one mechanic ventilation patients were included, 62 aged and 18 younger, mean ages from aged was 76 years, while in the younger it was 56 years. As compared to the control, aged patients had longer mechanic ventilation time , higher intensive care unit and hospital mortality: 63.1% versus 26.3% and 74.2% versus 47.4% (P<0.05), respectively. In addition, the aged under mechanic ventilation had increased desintubation failures, difficult ventilatory weaning and deaths directly related to respiratory dysfunction. The mechanic ventilation time was an independent risk factor for death in the intensive care unit in aged patients (OR= 2.7, p=0.02). The area under the ROC curve of mechanic ventilation about intensive care unit death was 0.92 (95% CI 0.85-0.97, p (area 0.5)=0.0001), cutoff point of 4 days, sensitivity 89.4% and specificity 77.1%. CONCLUSIONS: Mechanic ventilation patients over 65years of age have a worse prognosis than the younger, and the longer the mechanic ventilation time, the higher will be intensive care mortality.
Views0Abstract
Aged patients with respiratory dysfunction: epidemiological profile and mortality risk factors
Rev Bras Ter Intensiva. 2009;21(3):262-268
DOI 10.1590/S0103-507X2009000300005
Views0See moreOBJECTIVES: To describe the population of aged as compared to young patients under mechanical ventilation and to analyze the mortality risk factors of this group in an intensive care unit. METHODS: This was a prospective observational trial in patients over 18 years of age, admitted in an intensive care unit and under mechanical ventilation, during one year. Patients were divided into two groups according to age: Group 1 – patients over 65 years old; and Group 2, 65 years old or younger. RESULTS: eighty one mechanic ventilation patients were included, 62 aged and 18 younger, mean ages from aged was 76 years, while in the younger it was 56 years. As compared to the control, aged patients had longer mechanic ventilation time , higher intensive care unit and hospital mortality: 63.1% versus 26.3% and 74.2% versus 47.4% (P<0.05), respectively. In addition, the aged under mechanic ventilation had increased desintubation failures, difficult ventilatory weaning and deaths directly related to respiratory dysfunction. The mechanic ventilation time was an independent risk factor for death in the intensive care unit in aged patients (OR= 2.7, p=0.02). The area under the ROC curve of mechanic ventilation about intensive care unit death was 0.92 (95% CI 0.85-0.97, p (area 0.5)=0.0001), cutoff point of 4 days, sensitivity 89.4% and specificity 77.1%. CONCLUSIONS: Mechanic ventilation patients over 65years of age have a worse prognosis than the younger, and the longer the mechanic ventilation time, the higher will be intensive care mortality.
-
Infections in patients submitted to hemodialysis: a systematic review
Rev Bras Ter Intensiva. 2009;21(3):269-275
Abstract
Infections in patients submitted to hemodialysis: a systematic review
Rev Bras Ter Intensiva. 2009;21(3):269-275
DOI 10.1590/S0103-507X2009000300006
Views0OBJECTIVE: Infection is one of the main complications of dialysis procedures to correct renal injury, with a significant impact on morbidity mortality in chronic and critically acute dialysis patients. The objective of this work was to review literature on infection in patients submitted to hemodyalisis. METHODS: A survey of publications from 1990 to March 2008 was carried out in the database COCHRANE, PubMed/MEDLINE, Latin-American and Caribbean literature on Health Sciences and Nursing database. In Health Science (DECS) and Medical Subject Headings Section (MeSH) from |PubMed/MEDLINE the following descriptors were used: infection; cross infection; bacteremia; renal dialysis; renal failure;acute renal failure; hemofiltation; hemodiafiltration; renal replacement therapy. RESULTS: Thirty three articles were selected. Most publications were American, from 2001 to 2005 and mainly about vascular access-related infection. Studies diverged on the definition of infection and nomenclature, hindering comparisons. Fiver articles covered different infection topographies, 16 studied vascular access-related infections in the different types of vascular accesses, nine specifically focused on temporary central catheters for hemodialysis and only three studied infections in intensive care unit patients. Temporary central catheters for hemodialysis were identified as the principal risk factor. CONCLUSION: There is a need for studies about infection incidence in critically ill, submitted to dialysis with temporary catheters, due to acute renal injury to define a causal relationship and risk factors to orient adequate prevention and control measures.
Keywords:Bacteremiacross infectioninfectionRenal dialysisRenal insufficiency, acuteRenal insufficiency, chronicSee moreViews0Abstract
Infections in patients submitted to hemodialysis: a systematic review
Rev Bras Ter Intensiva. 2009;21(3):269-275
DOI 10.1590/S0103-507X2009000300006
Views0OBJECTIVE: Infection is one of the main complications of dialysis procedures to correct renal injury, with a significant impact on morbidity mortality in chronic and critically acute dialysis patients. The objective of this work was to review literature on infection in patients submitted to hemodyalisis. METHODS: A survey of publications from 1990 to March 2008 was carried out in the database COCHRANE, PubMed/MEDLINE, Latin-American and Caribbean literature on Health Sciences and Nursing database. In Health Science (DECS) and Medical Subject Headings Section (MeSH) from |PubMed/MEDLINE the following descriptors were used: infection; cross infection; bacteremia; renal dialysis; renal failure;acute renal failure; hemofiltation; hemodiafiltration; renal replacement therapy. RESULTS: Thirty three articles were selected. Most publications were American, from 2001 to 2005 and mainly about vascular access-related infection. Studies diverged on the definition of infection and nomenclature, hindering comparisons. Fiver articles covered different infection topographies, 16 studied vascular access-related infections in the different types of vascular accesses, nine specifically focused on temporary central catheters for hemodialysis and only three studied infections in intensive care unit patients. Temporary central catheters for hemodialysis were identified as the principal risk factor. CONCLUSION: There is a need for studies about infection incidence in critically ill, submitted to dialysis with temporary catheters, due to acute renal injury to define a causal relationship and risk factors to orient adequate prevention and control measures.
Keywords:Bacteremiacross infectioninfectionRenal dialysisRenal insufficiency, acuteRenal insufficiency, chronicSee more -
Nursing care adverse events at an intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):276-282
Abstract
Nursing care adverse events at an intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):276-282
DOI 10.1590/S0103-507X2009000300007
Views0See moreOBJECTIVE: The understanding of adverse events may simplify the inquiry regarding the quality of nursing care, presuming a foregrounding role in evaluating health services. The aim of the study was to identify adverse events in nursing care in an intensive care unit. METHODS: Data were collected using an appropriate form known as problem-oriented record (POR) over a 10-month period; patients were monitored throughout their intensive care unit stay. RESULTS: Over the study period, 550 adverse events were recorded as follows: 26 concerned the “five rights” related to drug administration; 23 to non-administered medication; 181 to inappropriate medication records; 28 to failure in infusion pump assembly; 17 to not performed inhalation; 8 to incorrect handling of needles and syringes; 53 to not performed nursing procedures; 46 to incorrect handling of therapeutic and diagnostic devices; 37 to alarms/warnings of devices used incorrectly; and 131 to failure in data recording by nurses. CONCLUSION: The occurrence of adverse events in the care given to patients by the nursing team are significant indicators that disclose the quality of nursing care. Therefore, these events should be analyzed to support in-service training of the nursing staff.
Views0Abstract
Nursing care adverse events at an intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):276-282
DOI 10.1590/S0103-507X2009000300007
Views0See moreOBJECTIVE: The understanding of adverse events may simplify the inquiry regarding the quality of nursing care, presuming a foregrounding role in evaluating health services. The aim of the study was to identify adverse events in nursing care in an intensive care unit. METHODS: Data were collected using an appropriate form known as problem-oriented record (POR) over a 10-month period; patients were monitored throughout their intensive care unit stay. RESULTS: Over the study period, 550 adverse events were recorded as follows: 26 concerned the “five rights” related to drug administration; 23 to non-administered medication; 181 to inappropriate medication records; 28 to failure in infusion pump assembly; 17 to not performed inhalation; 8 to incorrect handling of needles and syringes; 53 to not performed nursing procedures; 46 to incorrect handling of therapeutic and diagnostic devices; 37 to alarms/warnings of devices used incorrectly; and 131 to failure in data recording by nurses. CONCLUSION: The occurrence of adverse events in the care given to patients by the nursing team are significant indicators that disclose the quality of nursing care. Therefore, these events should be analyzed to support in-service training of the nursing staff.
-
Humanization of physiotherapy care: study with patients post-stay in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):283-291
Abstract
Humanization of physiotherapy care: study with patients post-stay in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):283-291
DOI 10.1590/S0103-507X2009000300008
Views0OBJECTIVES: The intensive care unit emerged to improve and concentrate material and human resources for the care of critical patients, and need for constant observation and continuous assistance. However, patients in intensive care unit requires exceptional care, directed not only to the physiopathological problem, but also towards the psychosocial issue, now intimately interlinked to the physical disease. In this ambient, very demanding for capability of the multiprofessional team, presence of the physiotherapist has become more frequent. This study aims to verify if the attitude of an experienced physiotherapist in the intensive care unit is humanized. METHODS: To evaluate physiotherapy care humanization, a questionnaire was prepared and patients over 18 years of age, lucid and staying in intensive care unit for 24 hours or more were included. RESULTS: Forty four patients were interviewed and 95.5% of these considered the physiotherapy care as humanized. Positive association was observed between dissatisfaction with the items of dignity, communication, warranty and empathy, and a dehumannized physiotherapy care. Patients who evaluated warranty as negative had a twofold greater chance (0.7 – 5.3) of perceiving care as dehumanized. Patients who evaluated empathy as negative had a 1.6 (0.8 – 3.4) times greater chance of perceiving care as dehumanized. CONCLUSION: Physiotherapy care given in the intensive care unit was marked by good assistance, attention provided to the patient and quality of treatment, characterizing humanized care.
Keywords:humanizationIntensive Care UnitPatient carePatient satisfactionPhysiotherapyProfessional-patient relationQuestionnairesSee moreViews0Abstract
Humanization of physiotherapy care: study with patients post-stay in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):283-291
DOI 10.1590/S0103-507X2009000300008
Views0OBJECTIVES: The intensive care unit emerged to improve and concentrate material and human resources for the care of critical patients, and need for constant observation and continuous assistance. However, patients in intensive care unit requires exceptional care, directed not only to the physiopathological problem, but also towards the psychosocial issue, now intimately interlinked to the physical disease. In this ambient, very demanding for capability of the multiprofessional team, presence of the physiotherapist has become more frequent. This study aims to verify if the attitude of an experienced physiotherapist in the intensive care unit is humanized. METHODS: To evaluate physiotherapy care humanization, a questionnaire was prepared and patients over 18 years of age, lucid and staying in intensive care unit for 24 hours or more were included. RESULTS: Forty four patients were interviewed and 95.5% of these considered the physiotherapy care as humanized. Positive association was observed between dissatisfaction with the items of dignity, communication, warranty and empathy, and a dehumannized physiotherapy care. Patients who evaluated warranty as negative had a twofold greater chance (0.7 – 5.3) of perceiving care as dehumanized. Patients who evaluated empathy as negative had a 1.6 (0.8 – 3.4) times greater chance of perceiving care as dehumanized. CONCLUSION: Physiotherapy care given in the intensive care unit was marked by good assistance, attention provided to the patient and quality of treatment, characterizing humanized care.
Keywords:humanizationIntensive Care UnitPatient carePatient satisfactionPhysiotherapyProfessional-patient relationQuestionnairesSee more -
Breathing pattern in weaning patients: comparison of two inspired oxygen fractions
Rev Bras Ter Intensiva. 2009;21(3):292-298
Abstract
Breathing pattern in weaning patients: comparison of two inspired oxygen fractions
Rev Bras Ter Intensiva. 2009;21(3):292-298
DOI 10.1590/S0103-507X2009000300009
Views0BACKGROUND AND OBJECTIVES: An inspired oxygen fraction (FiO2) of 40% is often used for weaning patients, but lower FiO2 values are also recommended, if arterial oxygen pressure (PaO2)/ FiO2 >150-200 mmHg. This study aimed to compare respiratory variables and vital data values recorded during use of sufficient FiO2 (ideal) to maintain peripheral oxygen saturation at 92% with values recorded during use of FiO2 established at 40% (baseline) in weaning patients. METHODS: Prospective cross-over study. Respiratory variables (respiratory frequency, tidal volume, occlusion pressure, inspiratory time/total time ratio) and vital data (blood pressure and heart rate) were collected sequentially at 30 and 60 minutes with baseline FiO2, followed by ideal FiO2. These were compared to a generalized linear model for repeated measurements. Comparisons between baseline and ideal FiO2 values, and arterial blood gases were evaluated by the Student’s t or Wilcoxon tests. RESULTS: In 30 adult patients the median of ideal FiO2 was 25% (IQ25%-75% 23-28). This was significantly lower than baseline FiO2 (40%) (p< 0.001). No significant difference was found in the PaO2/ FiO2 ratio between baseline FiO2 (269±53) and ideal FiO2 (268±47). Tidal volume was significantly lower during use of ideal FiO2 (p=0.003) and blood pressure was significantly higher during use of baseline FiO2 (p=0.041), but there was no clinical significance. The remaining variables were not affected by reduction in FiO2. The ideal FiO2 did not influence remaining variables. CONCLUSIONS: These results suggest that FiO2 levels sufficient to ensure a SpO2>92% did not alter breathing patterns or trigger clinical changes in weaning patients.
Keywords:mechanical ventilationOxygen inhalation therapyRespirationRespiratory mechanicsVentilator weaningSee moreViews0Abstract
Breathing pattern in weaning patients: comparison of two inspired oxygen fractions
Rev Bras Ter Intensiva. 2009;21(3):292-298
DOI 10.1590/S0103-507X2009000300009
Views0BACKGROUND AND OBJECTIVES: An inspired oxygen fraction (FiO2) of 40% is often used for weaning patients, but lower FiO2 values are also recommended, if arterial oxygen pressure (PaO2)/ FiO2 >150-200 mmHg. This study aimed to compare respiratory variables and vital data values recorded during use of sufficient FiO2 (ideal) to maintain peripheral oxygen saturation at 92% with values recorded during use of FiO2 established at 40% (baseline) in weaning patients. METHODS: Prospective cross-over study. Respiratory variables (respiratory frequency, tidal volume, occlusion pressure, inspiratory time/total time ratio) and vital data (blood pressure and heart rate) were collected sequentially at 30 and 60 minutes with baseline FiO2, followed by ideal FiO2. These were compared to a generalized linear model for repeated measurements. Comparisons between baseline and ideal FiO2 values, and arterial blood gases were evaluated by the Student’s t or Wilcoxon tests. RESULTS: In 30 adult patients the median of ideal FiO2 was 25% (IQ25%-75% 23-28). This was significantly lower than baseline FiO2 (40%) (p< 0.001). No significant difference was found in the PaO2/ FiO2 ratio between baseline FiO2 (269±53) and ideal FiO2 (268±47). Tidal volume was significantly lower during use of ideal FiO2 (p=0.003) and blood pressure was significantly higher during use of baseline FiO2 (p=0.041), but there was no clinical significance. The remaining variables were not affected by reduction in FiO2. The ideal FiO2 did not influence remaining variables. CONCLUSIONS: These results suggest that FiO2 levels sufficient to ensure a SpO2>92% did not alter breathing patterns or trigger clinical changes in weaning patients.
Keywords:mechanical ventilationOxygen inhalation therapyRespirationRespiratory mechanicsVentilator weaningSee more -
Occupational stress and repercussions on the quality of life of pediatric and neonatal intensivist physicians and nurses
Rev Bras Ter Intensiva. 2009;21(3):299-305
Abstract
Occupational stress and repercussions on the quality of life of pediatric and neonatal intensivist physicians and nurses
Rev Bras Ter Intensiva. 2009;21(3):299-305
DOI 10.1590/S0103-507X2009000300010
Views0OBJECTIVE: To investigate the relationship between work and quality of life of doctors and nurses in pediatric intensive care units and neonatal. METHODS: Cross-sectional study with 37 doctors and 20 nurses. The Job Content Questionnarie (JCQ) e Effort-Reward Imbalance (ERI), and World Health Organization Quality of Life (WHOQOL-100) were used. The correlation was estimated by Spearman correlation coefficient. RESULTS: The effort is inversely correlated with the areas physical, psychological, level of independence, environment (p<0.01) and social relationship (p<0.05). The reward is inversely correlated with the areas and psychological (p<0.05) level of independence (p<0.01). Control over the work is directly correlated with the physical domain (p<0.05). The psychological demands are inversely correlated with the areas physical (p<0.05), psychological (p<0.01) and level of independence (p<0.01). The physical demand is inversely correlated with physical areas, level of independence, environmental (p<0.01) and psychological (p<0.05). Job insecurity is inversely correlated with the psychological fields, level of independence (p<0.05) and the environment (p<0.01). Support the supervisor is directly correlated with degree of independence (p <0.05). CONCLUSION: Doctors and nurses showed high efforts, demands psychological, physical and job insecurity that impact on quality of life.
Keywords:Burnout, professionalIntensive care units, pediatricJob satisfactionQuality of lifeQuestionnairesSee moreViews0Abstract
Occupational stress and repercussions on the quality of life of pediatric and neonatal intensivist physicians and nurses
Rev Bras Ter Intensiva. 2009;21(3):299-305
DOI 10.1590/S0103-507X2009000300010
Views0OBJECTIVE: To investigate the relationship between work and quality of life of doctors and nurses in pediatric intensive care units and neonatal. METHODS: Cross-sectional study with 37 doctors and 20 nurses. The Job Content Questionnarie (JCQ) e Effort-Reward Imbalance (ERI), and World Health Organization Quality of Life (WHOQOL-100) were used. The correlation was estimated by Spearman correlation coefficient. RESULTS: The effort is inversely correlated with the areas physical, psychological, level of independence, environment (p<0.01) and social relationship (p<0.05). The reward is inversely correlated with the areas and psychological (p<0.05) level of independence (p<0.01). Control over the work is directly correlated with the physical domain (p<0.05). The psychological demands are inversely correlated with the areas physical (p<0.05), psychological (p<0.01) and level of independence (p<0.01). The physical demand is inversely correlated with physical areas, level of independence, environmental (p<0.01) and psychological (p<0.05). Job insecurity is inversely correlated with the psychological fields, level of independence (p<0.05) and the environment (p<0.01). Support the supervisor is directly correlated with degree of independence (p <0.05). CONCLUSION: Doctors and nurses showed high efforts, demands psychological, physical and job insecurity that impact on quality of life.
Keywords:Burnout, professionalIntensive care units, pediatricJob satisfactionQuality of lifeQuestionnairesSee more -
1st Forum of the Southern Cone End-of-Life Study Group: proposal for care of patients, bearers of terminal disease staying in the ICU
Rev Bras Ter Intensiva. 2009;21(3):306-309
Abstract
1st Forum of the Southern Cone End-of-Life Study Group: proposal for care of patients, bearers of terminal disease staying in the ICU
Rev Bras Ter Intensiva. 2009;21(3):306-309
DOI 10.1590/S0103-507X2009000300011
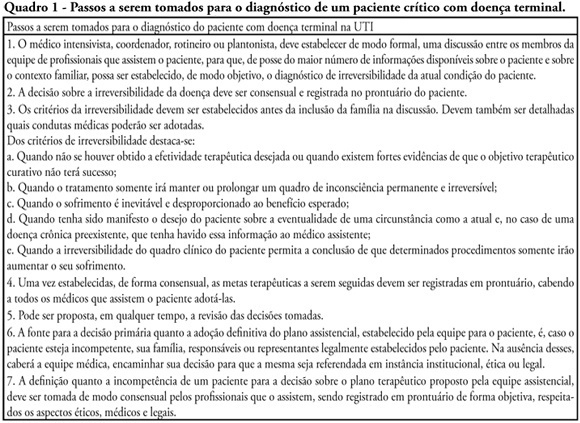
Views5See moreWithholding of treatment in patients with terminal disease is increasingly common in intensive care units, throughout the world. Notwithstanding, Brazilian intensivists still have a great difficulty to offer the best treatment to patients that have not benefited from curative care. The objective of this comment is to suggest an algorithm for the care of terminally ill patients. It was formulated based upon literature and the experience of experts, by members of the ethics committee and end-of-life of AMIB – Brazilian Association of Intensive Care.
Views5Abstract
1st Forum of the Southern Cone End-of-Life Study Group: proposal for care of patients, bearers of terminal disease staying in the ICU
Rev Bras Ter Intensiva. 2009;21(3):306-309
DOI 10.1590/S0103-507X2009000300011
Views5See moreWithholding of treatment in patients with terminal disease is increasingly common in intensive care units, throughout the world. Notwithstanding, Brazilian intensivists still have a great difficulty to offer the best treatment to patients that have not benefited from curative care. The objective of this comment is to suggest an algorithm for the care of terminally ill patients. It was formulated based upon literature and the experience of experts, by members of the ethics committee and end-of-life of AMIB – Brazilian Association of Intensive Care.
-
Glucose control in critically ill patients in 2009: no alarms and no surprises
Rev Bras Ter Intensiva. 2009;21(3):310-314
Abstract
Glucose control in critically ill patients in 2009: no alarms and no surprises
Rev Bras Ter Intensiva. 2009;21(3):310-314
DOI 10.1590/S0103-507X2009000300012
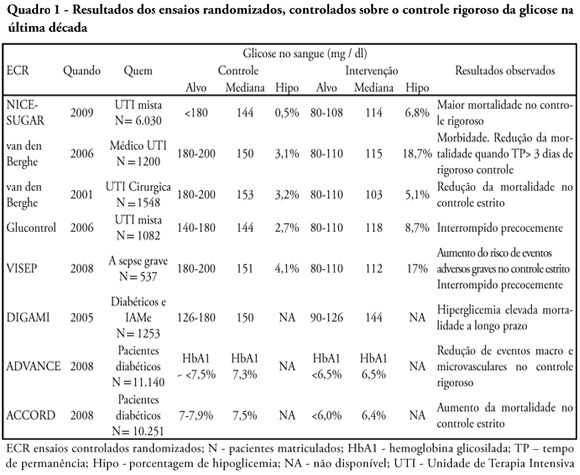
Views0See moreGlucose control is a major issue in critical care since landmark publications from the last decade leading to widespread use of strict glucose control in the clinical practice. Subsequent trials showed discordant results that lead to several questions and concerns about benefits and risks of implementing an intensive glucose control protocol. In the midst of all recent controversy, we propose that a new glycemic target -150mg/dl) should be aimed. This target glucose level could offer protection against the deleterious effects of hyperglycemia and at the same time keep patient’s safety avoiding hypoglicemia. The article presents a critical review of the current literature on intensive insulin therapy in critically ill patients.
Views0Abstract
Glucose control in critically ill patients in 2009: no alarms and no surprises
Rev Bras Ter Intensiva. 2009;21(3):310-314
DOI 10.1590/S0103-507X2009000300012
Views0See moreGlucose control is a major issue in critical care since landmark publications from the last decade leading to widespread use of strict glucose control in the clinical practice. Subsequent trials showed discordant results that lead to several questions and concerns about benefits and risks of implementing an intensive glucose control protocol. In the midst of all recent controversy, we propose that a new glycemic target -150mg/dl) should be aimed. This target glucose level could offer protection against the deleterious effects of hyperglycemia and at the same time keep patient’s safety avoiding hypoglicemia. The article presents a critical review of the current literature on intensive insulin therapy in critically ill patients.
-
Red blood cell transfusion in the intensive care setting: controversies amongst evidence
Rev Bras Ter Intensiva. 2009;21(3):315-323
Abstract
Red blood cell transfusion in the intensive care setting: controversies amongst evidence
Rev Bras Ter Intensiva. 2009;21(3):315-323
DOI 10.1590/S0103-507X2009000300013
Views0See moreAnemia is a prevalent issue in intensive care units. It appears in the first days, and may continue or worsen during hospital stay. Its etiology is generally multifactorial. Red blood cell transfusion is the most common intervention for treating anemia. Approximately 12 million blood units are used for transfusions in the United States, 25% to 30% in the intensive care units. Due to reduction of transfusion infections the increased safety has allowed an expansion of clinical indications. However, transfusion therapy is associated with other adverse effects such as nosocomial infections, immunological impairment, lung injury, hemolytic reactions and higher cancer incidence. Various papers have tried to show an association between correction of anemia and mortality-morbidity, but no consensus has been reached in literature. One of the current World Health Organization’s proposals is to reduce potentially unnecessary transfusions, promoting a rational transfusion attitude. The primary objective of this narrative review is to approach controversies regarding the transfusion threshold according to recent studies, and as a secondary objective, it aims to discuss iatrogenic anemia aspects and the different behaviors among intensivists on the best practices for implementation of transfusion practices. It is not within our objectives to discuss transfusion complications, although they are mentioned. A search was conducted on electronic literature databases (PubMed – Clinical Queries), and UpToDate 16.2, and additional consultation to textbooks. It became clear that transfusion practices are widely variable among intensive care units. Evidence is scarce that routine transfusion in non-hemorrhagic patients should be used in those with > 7 g/dL hemoglobin. There is no consensus on the transfusion threshold in critically ill patients. Cardiovascular disease patients seem to present a higher risk of death than non-cardiovascular patients, for any level of hemoglobin. Transfusion guided by hemoglobin levels and individual oxy-hemodynamic physiologic parameters and clinical context is apparently, the current best accepted strategy, rather than arbitrary and isolated hemoglobin correction.
Views0Abstract
Red blood cell transfusion in the intensive care setting: controversies amongst evidence
Rev Bras Ter Intensiva. 2009;21(3):315-323
DOI 10.1590/S0103-507X2009000300013
Views0See moreAnemia is a prevalent issue in intensive care units. It appears in the first days, and may continue or worsen during hospital stay. Its etiology is generally multifactorial. Red blood cell transfusion is the most common intervention for treating anemia. Approximately 12 million blood units are used for transfusions in the United States, 25% to 30% in the intensive care units. Due to reduction of transfusion infections the increased safety has allowed an expansion of clinical indications. However, transfusion therapy is associated with other adverse effects such as nosocomial infections, immunological impairment, lung injury, hemolytic reactions and higher cancer incidence. Various papers have tried to show an association between correction of anemia and mortality-morbidity, but no consensus has been reached in literature. One of the current World Health Organization’s proposals is to reduce potentially unnecessary transfusions, promoting a rational transfusion attitude. The primary objective of this narrative review is to approach controversies regarding the transfusion threshold according to recent studies, and as a secondary objective, it aims to discuss iatrogenic anemia aspects and the different behaviors among intensivists on the best practices for implementation of transfusion practices. It is not within our objectives to discuss transfusion complications, although they are mentioned. A search was conducted on electronic literature databases (PubMed – Clinical Queries), and UpToDate 16.2, and additional consultation to textbooks. It became clear that transfusion practices are widely variable among intensive care units. Evidence is scarce that routine transfusion in non-hemorrhagic patients should be used in those with > 7 g/dL hemoglobin. There is no consensus on the transfusion threshold in critically ill patients. Cardiovascular disease patients seem to present a higher risk of death than non-cardiovascular patients, for any level of hemoglobin. Transfusion guided by hemoglobin levels and individual oxy-hemodynamic physiologic parameters and clinical context is apparently, the current best accepted strategy, rather than arbitrary and isolated hemoglobin correction.
-
Intestinal constipation in intensive care units
Rev Bras Ter Intensiva. 2009;21(3):324-331
Abstract
Intestinal constipation in intensive care units
Rev Bras Ter Intensiva. 2009;21(3):324-331
DOI 10.1590/S0103-507X2009000300014
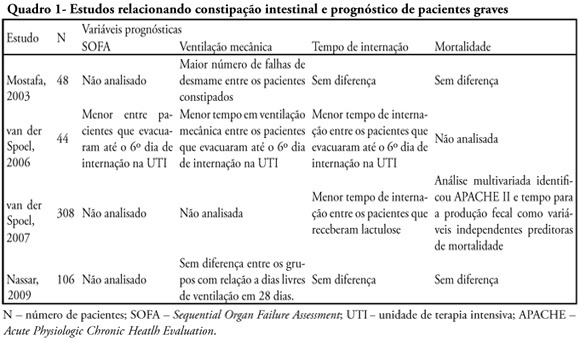
Views0See moreConstipation is a common complication identified among critically ill patients. Its incidence is highly variable due to lack of definition of such patients. Besides the already known consequences of constipation, in recent years it was observed that this complication may also be related to worse prognosis of critically ill patients. This review endeavors to describe the main available scientific evidence showing that constipation is a prognostic marker and a clinical representation of intestinal dysfunction, in addition to eventually interfering in the prognosis with treatment. Ogilvie syndrome, a major cause of morbidity and mortality in intensive care units was also reviewed. Considering the above cases it was concluded that more attention to this disorder is required in intensive care units as well as development of protocols for diagnosis and management of critically ill patients.
Views0Abstract
Intestinal constipation in intensive care units
Rev Bras Ter Intensiva. 2009;21(3):324-331
DOI 10.1590/S0103-507X2009000300014
Views0See moreConstipation is a common complication identified among critically ill patients. Its incidence is highly variable due to lack of definition of such patients. Besides the already known consequences of constipation, in recent years it was observed that this complication may also be related to worse prognosis of critically ill patients. This review endeavors to describe the main available scientific evidence showing that constipation is a prognostic marker and a clinical representation of intestinal dysfunction, in addition to eventually interfering in the prognosis with treatment. Ogilvie syndrome, a major cause of morbidity and mortality in intensive care units was also reviewed. Considering the above cases it was concluded that more attention to this disorder is required in intensive care units as well as development of protocols for diagnosis and management of critically ill patients.
-
Use of automated external defibrillator in Peruvian out-of-hospital environment: improving emergency response in Latin America
Rev Bras Ter Intensiva. 2009;21(3):332-335
Abstract
Use of automated external defibrillator in Peruvian out-of-hospital environment: improving emergency response in Latin America
Rev Bras Ter Intensiva. 2009;21(3):332-335
DOI 10.1590/S0103-507X2009000300015
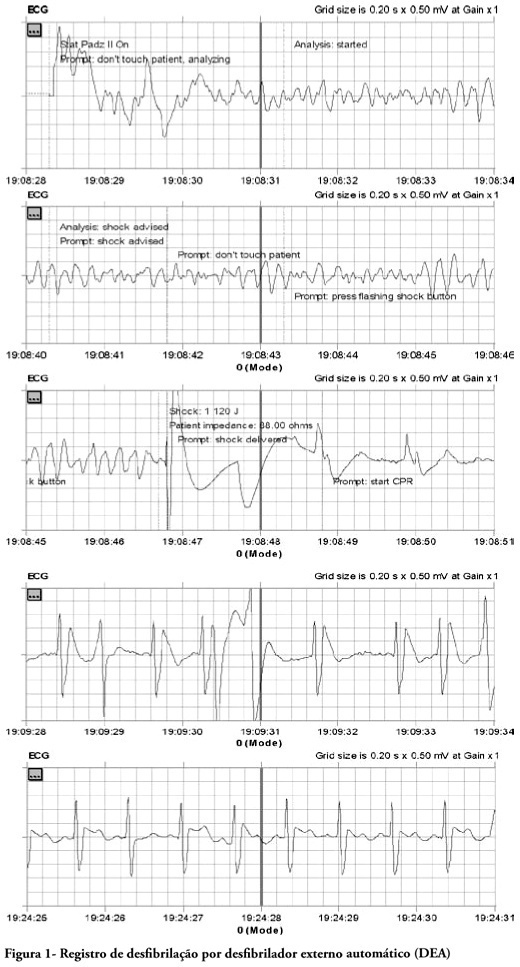
Views0See moreThis case report relates out-of-hospital care to a patient with risk factors treated in the out-of-hospital services after cardiac arrest and ventricular fibrillation. The patient was treated according to the standards of basic life support and advanced cardiovascular life support; by applying an automated external defibrillator (AED) with favorable outcome and successful recovery of the patient from his risk of life condition. This is the first documented report with a favorable outcome in Peru, in out-of-hospital services and stresses the desirability of adopting policies for public access to early defibrillation.
Views0Abstract
Use of automated external defibrillator in Peruvian out-of-hospital environment: improving emergency response in Latin America
Rev Bras Ter Intensiva. 2009;21(3):332-335
DOI 10.1590/S0103-507X2009000300015
Views0See moreThis case report relates out-of-hospital care to a patient with risk factors treated in the out-of-hospital services after cardiac arrest and ventricular fibrillation. The patient was treated according to the standards of basic life support and advanced cardiovascular life support; by applying an automated external defibrillator (AED) with favorable outcome and successful recovery of the patient from his risk of life condition. This is the first documented report with a favorable outcome in Peru, in out-of-hospital services and stresses the desirability of adopting policies for public access to early defibrillation.
-
Thrombotic thrombocytopenic purpura associated with pregnancy: case report
Rev Bras Ter Intensiva. 2009;21(3):336-339
Abstract
Thrombotic thrombocytopenic purpura associated with pregnancy: case report
Rev Bras Ter Intensiva. 2009;21(3):336-339
DOI 10.1590/S0103-507X2009000300016
Views0Case report of a patient with 37-week gestational age admitted to an obstetric intensive care unit with an altered level of consciousness, related primarily to the pregnancy-induced hypertension. The patient presented a worsening clinical course characterized by, anemia and severe thrombocytopenia, Investigation led to a diagnostic of thrombotic thrombocytopenic purpura after the hematological profile was assessed. The authors emphasize the importance of the disease recognition as a prognostic marker for obstetric patients, in view of the similarity with other common morbidities during pregnancy and the importance of timely diagnosis and early treatment as determinant factors for the outcome.
Keywords:Case reportsIntensive carePlasmapheresisPregnancy complications, hematologicPurpurathrombotic thrombocytopenicSee moreViews0Abstract
Thrombotic thrombocytopenic purpura associated with pregnancy: case report
Rev Bras Ter Intensiva. 2009;21(3):336-339
DOI 10.1590/S0103-507X2009000300016
Views0Case report of a patient with 37-week gestational age admitted to an obstetric intensive care unit with an altered level of consciousness, related primarily to the pregnancy-induced hypertension. The patient presented a worsening clinical course characterized by, anemia and severe thrombocytopenia, Investigation led to a diagnostic of thrombotic thrombocytopenic purpura after the hematological profile was assessed. The authors emphasize the importance of the disease recognition as a prognostic marker for obstetric patients, in view of the similarity with other common morbidities during pregnancy and the importance of timely diagnosis and early treatment as determinant factors for the outcome.
Keywords:Case reportsIntensive carePlasmapheresisPregnancy complications, hematologicPurpurathrombotic thrombocytopenicSee more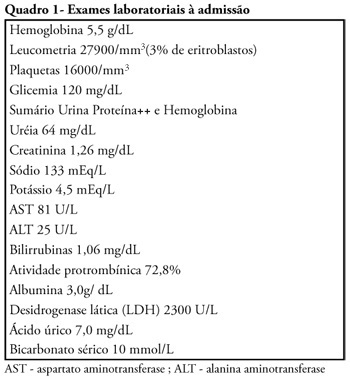
Volume Articles - Critical Care Science (CCS)
