-
Original Articles
Early detection strategy and mortality reduction in severe sepsis
Rev Bras Ter Intensiva. 2009;21(2):113-123
Abstract
Original ArticlesEarly detection strategy and mortality reduction in severe sepsis
Rev Bras Ter Intensiva. 2009;21(2):113-123
DOI 10.1590/S0103-507X2009000200001
Views0OBJECTIVE: To evaluate the impact of implementing an institutional policy for detection of severe sepsis and septic shock. METHODS: Study before (stage I), after (stage II) with prospective data collection in a 195 bed public hospital.. Stage I: Patients with severe sepsis or septic shock were included consecutively over 15 months and treated according to the Surviving Sepsis Campaign guidelines. Stage II: In the 10 subsequent months, patients with severe sepsis or septic shock were enrolled based on an active search for signs suggesting infection (SSI) in hospitalized patients. The two stages were compared for demographic variables, time needed for recognition of at least two signs suggesting infection (SSI-Δt), compliance to the bundles of 6 and 24 hours and mortality. RESULTS: We identified 124 patients with severe sepsis or septic shock, 68 in stage I and 56 in stage II. The demographic variables were similar in both stages. The Δt-SSI was 34 ± 54 hours in stage I and 7 ± 8.4 hours in stage II (p <0.001). There was no difference in compliance to the bundles. In parallel there was significant reduction of mortality rates at 28 days (54.4% versus 30%, p <0.02) and hospital (67.6% versus 41%, p <0.003). CONCLUSION: The strategy used helped to identify early risk of sepsis and resulted in decreased mortality associated with severe sepsis and septic shock.
Keywords:SepsisShock, septicSee moreViews0

Abstract
Original ArticlesEarly detection strategy and mortality reduction in severe sepsis
Rev Bras Ter Intensiva. 2009;21(2):113-123
DOI 10.1590/S0103-507X2009000200001
Views0OBJECTIVE: To evaluate the impact of implementing an institutional policy for detection of severe sepsis and septic shock. METHODS: Study before (stage I), after (stage II) with prospective data collection in a 195 bed public hospital.. Stage I: Patients with severe sepsis or septic shock were included consecutively over 15 months and treated according to the Surviving Sepsis Campaign guidelines. Stage II: In the 10 subsequent months, patients with severe sepsis or septic shock were enrolled based on an active search for signs suggesting infection (SSI) in hospitalized patients. The two stages were compared for demographic variables, time needed for recognition of at least two signs suggesting infection (SSI-Δt), compliance to the bundles of 6 and 24 hours and mortality. RESULTS: We identified 124 patients with severe sepsis or septic shock, 68 in stage I and 56 in stage II. The demographic variables were similar in both stages. The Δt-SSI was 34 ± 54 hours in stage I and 7 ± 8.4 hours in stage II (p <0.001). There was no difference in compliance to the bundles. In parallel there was significant reduction of mortality rates at 28 days (54.4% versus 30%, p <0.02) and hospital (67.6% versus 41%, p <0.003). CONCLUSION: The strategy used helped to identify early risk of sepsis and resulted in decreased mortality associated with severe sepsis and septic shock.
Keywords:SepsisShock, septicSee more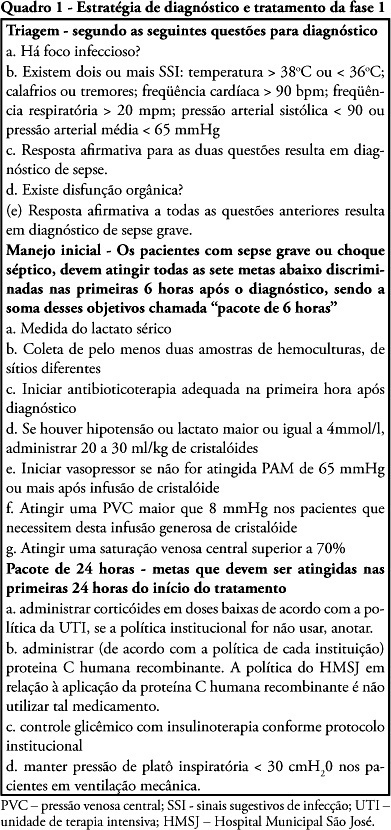
-
Original Articles
Nutritional assessment of the critically ill patients with cardiac disease under renal replacement therapy: diagnostic difficulty
Rev Bras Ter Intensiva. 2009;21(2):124-128
Abstract
Original ArticlesNutritional assessment of the critically ill patients with cardiac disease under renal replacement therapy: diagnostic difficulty
Rev Bras Ter Intensiva. 2009;21(2):124-128
DOI 10.1590/S0103-507X2009000200002
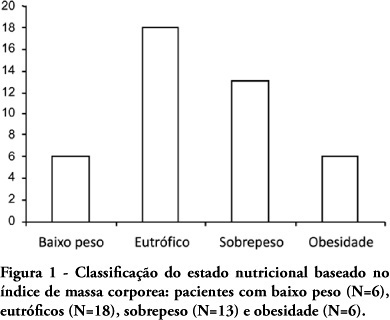
Views0See moreOBJECTIVE: Evaluate the nutritional status of patients with cardiac disease and concomitant renal dysfunction requiring renal replacement therapy. METHODS: Patients with cardiac disease and renal failure receiving renal replacement therapy, admitted to an intensive care unit, were submitted to nutritional evaluation, by use of anthropometric measurements and laboratory data. RESULTS: We studied 43 patients, mean age 64±15 years, 26 were men. The mean left ventricular ejection fraction was 0.36±0.16. Analysis of anthropometric measurements, based on body mass index disclosed that, 18 patients were normal, 6 were underweight and 19 were overweight or obese. Based on measurement of triceps skinfold thickness, 16 patients were considered normal and 27 had some degree of depletion. Measurements of midarm circumference and midarm muscular circumference showed 41 patients with some degree of depletion. Laboratory data revealed 28 patients with depletion based on albumin levels and 27 with depletion based on lymphocyte count. CONCLUSIONS: Malnutrition is common in critically ill patients with cardiac disease and renal failure receiving renal replacement therapy. Nutritional assessment based on body mass index did not prove to be a good index for diagnosis of nutritional disorders. The nutritional evaluation must be complemented in order to identify malnutrition and introduce early nutritional support.
Views0Abstract
Original ArticlesNutritional assessment of the critically ill patients with cardiac disease under renal replacement therapy: diagnostic difficulty
Rev Bras Ter Intensiva. 2009;21(2):124-128
DOI 10.1590/S0103-507X2009000200002
Views0See moreOBJECTIVE: Evaluate the nutritional status of patients with cardiac disease and concomitant renal dysfunction requiring renal replacement therapy. METHODS: Patients with cardiac disease and renal failure receiving renal replacement therapy, admitted to an intensive care unit, were submitted to nutritional evaluation, by use of anthropometric measurements and laboratory data. RESULTS: We studied 43 patients, mean age 64±15 years, 26 were men. The mean left ventricular ejection fraction was 0.36±0.16. Analysis of anthropometric measurements, based on body mass index disclosed that, 18 patients were normal, 6 were underweight and 19 were overweight or obese. Based on measurement of triceps skinfold thickness, 16 patients were considered normal and 27 had some degree of depletion. Measurements of midarm circumference and midarm muscular circumference showed 41 patients with some degree of depletion. Laboratory data revealed 28 patients with depletion based on albumin levels and 27 with depletion based on lymphocyte count. CONCLUSIONS: Malnutrition is common in critically ill patients with cardiac disease and renal failure receiving renal replacement therapy. Nutritional assessment based on body mass index did not prove to be a good index for diagnosis of nutritional disorders. The nutritional evaluation must be complemented in order to identify malnutrition and introduce early nutritional support.
-
Original Articles
Energy expenditure in mechanical ventilation: is there an agreement between the Ireton-Jones equation and indirect calorimetry?
Rev Bras Ter Intensiva. 2009;21(2):129-134
Abstract
Original ArticlesEnergy expenditure in mechanical ventilation: is there an agreement between the Ireton-Jones equation and indirect calorimetry?
Rev Bras Ter Intensiva. 2009;21(2):129-134
DOI 10.1590/S0103-507X2009000200003
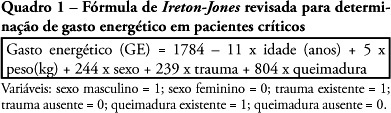
Views0See moreOBJECTIVE: Assess the agreement between the energy expenditure measured by indirect calorimetry and that estimated by the Ireton-Jones formula of critically ill patients under assisted mechanical ventilation. METHODS: Participated in the study individuals able to interrupt ventilation support, admitted at the center of intensive care of the Hospital de Clínicas de Porto Alegre – RS, between August 2006 and January 2007. Energy expenditure was measured by indirect calorimetry using a specific monitor, as well as estimated by the Ireton-Jones formula. Values found were analyzed using the Student’s t test and the Bland and Altman method and expressed in mean, ± standard deviation with a significance level of p<0.05. RESULTS: The study included forty patients with a mean age of 56±16 years and APACHE II score of 23±8. Energy expenditure measured by indirect calorimetry was of 1558±304kcal/24h, while that estimated by Ireton-Jones was of 1689±246kcal/24h. There was a significant statistical difference between means of energy expenditure measured and estimated of the same individual (p<0.004). The agreement thresholds between indirect calorimetry and the Ireton-Jones equation were of -680.51 to 417.81 kcal. CONCLUSION: Energy expenditure estimated by the Ireton-Jones formula did not present good agreement with that measured by indirect calorimetry, however, considering aspects related to availability of the equipment, this equation may be useful in the nutritional planning for critically ill patients.
Views0Abstract
Original ArticlesEnergy expenditure in mechanical ventilation: is there an agreement between the Ireton-Jones equation and indirect calorimetry?
Rev Bras Ter Intensiva. 2009;21(2):129-134
DOI 10.1590/S0103-507X2009000200003
Views0See moreOBJECTIVE: Assess the agreement between the energy expenditure measured by indirect calorimetry and that estimated by the Ireton-Jones formula of critically ill patients under assisted mechanical ventilation. METHODS: Participated in the study individuals able to interrupt ventilation support, admitted at the center of intensive care of the Hospital de Clínicas de Porto Alegre – RS, between August 2006 and January 2007. Energy expenditure was measured by indirect calorimetry using a specific monitor, as well as estimated by the Ireton-Jones formula. Values found were analyzed using the Student’s t test and the Bland and Altman method and expressed in mean, ± standard deviation with a significance level of p<0.05. RESULTS: The study included forty patients with a mean age of 56±16 years and APACHE II score of 23±8. Energy expenditure measured by indirect calorimetry was of 1558±304kcal/24h, while that estimated by Ireton-Jones was of 1689±246kcal/24h. There was a significant statistical difference between means of energy expenditure measured and estimated of the same individual (p<0.004). The agreement thresholds between indirect calorimetry and the Ireton-Jones equation were of -680.51 to 417.81 kcal. CONCLUSION: Energy expenditure estimated by the Ireton-Jones formula did not present good agreement with that measured by indirect calorimetry, however, considering aspects related to availability of the equipment, this equation may be useful in the nutritional planning for critically ill patients.
-
Original Articles
Reasons related to the choice of critical care medicine as a specialty by medical residents
Rev Bras Ter Intensiva. 2009;21(2):135-140
Abstract
Original ArticlesReasons related to the choice of critical care medicine as a specialty by medical residents
Rev Bras Ter Intensiva. 2009;21(2):135-140
DOI 10.1590/S0103-507X2009000200004
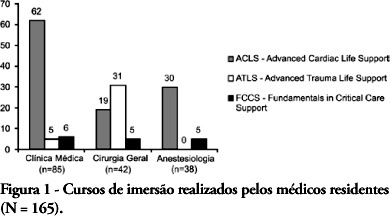
Views1See moreOBJECTIVES: Critical Care Medicine is a relatively new specialty, which in recent years has made significant progress in Brazil. However, few physicians are willing to acquire this specialization. The main objective of this study was to describe the factors associated with choice of Critical Care Medicine as a specialty by medical residents of Salvador-BA. METHODS: A cross-sectional and descriptive study, in which a questionnaire was submitted to all residents of the specialties that are a prerequisite for Critical Care Medicine (Clinical Medicine, General Surgery and Anesthesiology), between October and December 2007. RESULTS: The study included 165 residents (89.7% of the total), in which 51.5% were clinical medicine residents, 25.5% were general surgery residents, and 23.0% were anesthesiology residents. Of the respondents, 14 (9.1%) intended to enter Critical Care Medicine residency, although 90 (54.5%) were willing to become intensive care unit physicians after their regular residency. The main reason stated to specialize in critical care medicine was to like work with critically ill patients (92.9%). The main reasons stated not to specialize in critical care medicine, however were related with the poorer quality of life and work. Residents who did intensive care unit initernship during medical studies were more likely to work in an intensive care units after residency. CONCLUSIONS: This population showed little interest to specialize in critical care medicine. The main reasons given for this limited interest were factors related to quality of life and intensive care unit environment. A national survey is required to identify the interventions needed to favor this specialization.
Views1Abstract
Original ArticlesReasons related to the choice of critical care medicine as a specialty by medical residents
Rev Bras Ter Intensiva. 2009;21(2):135-140
DOI 10.1590/S0103-507X2009000200004
Views1See moreOBJECTIVES: Critical Care Medicine is a relatively new specialty, which in recent years has made significant progress in Brazil. However, few physicians are willing to acquire this specialization. The main objective of this study was to describe the factors associated with choice of Critical Care Medicine as a specialty by medical residents of Salvador-BA. METHODS: A cross-sectional and descriptive study, in which a questionnaire was submitted to all residents of the specialties that are a prerequisite for Critical Care Medicine (Clinical Medicine, General Surgery and Anesthesiology), between October and December 2007. RESULTS: The study included 165 residents (89.7% of the total), in which 51.5% were clinical medicine residents, 25.5% were general surgery residents, and 23.0% were anesthesiology residents. Of the respondents, 14 (9.1%) intended to enter Critical Care Medicine residency, although 90 (54.5%) were willing to become intensive care unit physicians after their regular residency. The main reason stated to specialize in critical care medicine was to like work with critically ill patients (92.9%). The main reasons stated not to specialize in critical care medicine, however were related with the poorer quality of life and work. Residents who did intensive care unit initernship during medical studies were more likely to work in an intensive care units after residency. CONCLUSIONS: This population showed little interest to specialize in critical care medicine. The main reasons given for this limited interest were factors related to quality of life and intensive care unit environment. A national survey is required to identify the interventions needed to favor this specialization.
-
Original Articles
Evaluation of medical decisions at the end-of-life process
Rev Bras Ter Intensiva. 2009;21(2):141-147
Abstract
Original ArticlesEvaluation of medical decisions at the end-of-life process
Rev Bras Ter Intensiva. 2009;21(2):141-147
DOI 10.1590/S0103-507X2009000200005
Views0See moreOBJECTIVES: To evaluate the medical decisions at end-of-life of patients admitted at HU/UFSC and to compare these decisions and the profile of patients who died in the intensive care unit (ICU) to those who died in medical (MW) and surgical wards (SW). METHODS: This is a retrospective and observational study. Demographic data, clinical features, treatment and the end-of-life care decisions of adult patients who died in wards and the intensive care unit of HU/UFSC from July/2004 to December/2008 were analyzed . For statistical analysis the Student’s t, χ2 and ANOVA tests were used: (significance p <0.05). RESULTS: An analysis was made of 1124 deaths: 404 occurred in ICU, 607 in MW and 113 in SW. The overall hospital mortality rate was 5.9% (ICU=24.49%, MW=7.2%, SW=1.69%). Mean ages of patients were: ICU=56.7, MW=69.3 and SW=70.4 years (p <0.01). Withholding/withdrawing life support was performed prior to 30.7% of deaths in the intensive care unit and 10% in the wards (p <0.01). Cardiopulmonary resuscitation was not carried out in 65% of cases in ICU, 79% in MW and 62% in SW. Besides cardiopulmonary resuscitation, the more frequent withholding/withdrawing life support in the intensive care unit were vasoactive drugs and in the wards refusal of admission to intensive care unit . Do-not-resuscitate order was documented in 2.4% of cases in ICU and 2.6% in MW. Palliative and comfort care were provided to 2% of patients in ICU, 11.5% in MW and 8% in SW. Terminality of the disease was recognized in 40% of cases in ICU, 34.6% in MW and 16.8% in SW. CONCLUSIONS: The profile of patients who died and medical decisions during the end-of-life process were different in the intensive care unit, clinical and surgical wards.
Views0Abstract
Original ArticlesEvaluation of medical decisions at the end-of-life process
Rev Bras Ter Intensiva. 2009;21(2):141-147
DOI 10.1590/S0103-507X2009000200005
Views0See moreOBJECTIVES: To evaluate the medical decisions at end-of-life of patients admitted at HU/UFSC and to compare these decisions and the profile of patients who died in the intensive care unit (ICU) to those who died in medical (MW) and surgical wards (SW). METHODS: This is a retrospective and observational study. Demographic data, clinical features, treatment and the end-of-life care decisions of adult patients who died in wards and the intensive care unit of HU/UFSC from July/2004 to December/2008 were analyzed . For statistical analysis the Student’s t, χ2 and ANOVA tests were used: (significance p <0.05). RESULTS: An analysis was made of 1124 deaths: 404 occurred in ICU, 607 in MW and 113 in SW. The overall hospital mortality rate was 5.9% (ICU=24.49%, MW=7.2%, SW=1.69%). Mean ages of patients were: ICU=56.7, MW=69.3 and SW=70.4 years (p <0.01). Withholding/withdrawing life support was performed prior to 30.7% of deaths in the intensive care unit and 10% in the wards (p <0.01). Cardiopulmonary resuscitation was not carried out in 65% of cases in ICU, 79% in MW and 62% in SW. Besides cardiopulmonary resuscitation, the more frequent withholding/withdrawing life support in the intensive care unit were vasoactive drugs and in the wards refusal of admission to intensive care unit . Do-not-resuscitate order was documented in 2.4% of cases in ICU and 2.6% in MW. Palliative and comfort care were provided to 2% of patients in ICU, 11.5% in MW and 8% in SW. Terminality of the disease was recognized in 40% of cases in ICU, 34.6% in MW and 16.8% in SW. CONCLUSIONS: The profile of patients who died and medical decisions during the end-of-life process were different in the intensive care unit, clinical and surgical wards.
-
Original Articles
Intensivist nurses perception of intensive care unit dysthanasia
Rev Bras Ter Intensiva. 2009;21(2):148-154
Abstract
Original ArticlesIntensivist nurses perception of intensive care unit dysthanasia
Rev Bras Ter Intensiva. 2009;21(2):148-154
DOI 10.1590/S0103-507X2009000200006
Views0See morePURPOSE: Identify and evaluate the perception of Intensivist Nurses in a University Hospital in Londrina, of dysthanasia in terminal patients at the Intensive Care Unit. METHODS: Qualitative study. Data were collected by semi-structured recorded interview involving nine nurses working in a university hospital intensive care units, during January 2009. A thematic analysis was used to evaluate subjects’ speech and identify discussion categories. RESULTS: Five categories were identified, discussed based on the authors’ experience and literature, namely: measures prolonging life of patients with no chance of cure in the intensive care unit; nurses’ actions/reactions when facing dysthanasia; reasons leading to prolonging life of patients with no chance of cure; nurses’ feelings about dysthanasia and life prolongation; care measures as opposed to dysthanasia. CONCLUSION: Experiencing of nurses when facing dysthanasia actions was shown to be complex, a factor of suffering, frustration and discomfort for these professionals. In the nurses’ view, lack of communication stands out as an important factor for dysthanasia, and measures to replace dysthanasia are those relieving suffering.
Views0Abstract
Original ArticlesIntensivist nurses perception of intensive care unit dysthanasia
Rev Bras Ter Intensiva. 2009;21(2):148-154
DOI 10.1590/S0103-507X2009000200006
Views0See morePURPOSE: Identify and evaluate the perception of Intensivist Nurses in a University Hospital in Londrina, of dysthanasia in terminal patients at the Intensive Care Unit. METHODS: Qualitative study. Data were collected by semi-structured recorded interview involving nine nurses working in a university hospital intensive care units, during January 2009. A thematic analysis was used to evaluate subjects’ speech and identify discussion categories. RESULTS: Five categories were identified, discussed based on the authors’ experience and literature, namely: measures prolonging life of patients with no chance of cure in the intensive care unit; nurses’ actions/reactions when facing dysthanasia; reasons leading to prolonging life of patients with no chance of cure; nurses’ feelings about dysthanasia and life prolongation; care measures as opposed to dysthanasia. CONCLUSION: Experiencing of nurses when facing dysthanasia actions was shown to be complex, a factor of suffering, frustration and discomfort for these professionals. In the nurses’ view, lack of communication stands out as an important factor for dysthanasia, and measures to replace dysthanasia are those relieving suffering.
-
Original Articles
Effects of manual rib-cage compression versus PEEP-ZEEP maneuver on respiratory system compliance and oxygenation in patients receiving mechanical ventilation
Rev Bras Ter Intensiva. 2009;21(2):155-161
Abstract
Original ArticlesEffects of manual rib-cage compression versus PEEP-ZEEP maneuver on respiratory system compliance and oxygenation in patients receiving mechanical ventilation
Rev Bras Ter Intensiva. 2009;21(2):155-161
DOI 10.1590/S0103-507X2009000200007
Views0OBJECTIVES: Patients unable to perform breathing functions may be submitted to invasive mechanical ventilation. Chest physiotherapy acts directly on the treatment of these patients for the purpose of improving their lung function. The objective of this study was to evaluate the effects of manual rib-cage compression versus the positive end expiratory pressure-zero end expiratory pressure (PEEP-ZEEP) maneuver, on compliance of the respiratory system and oxygenation in patients under invasive mechanical ventilation. METHODS: A double centric, prospective, randomized and crossover study, with patients under invasive mechanical ventilation, in controlled mode for more than 48 hours was carried out. The protocols of chest physiothe-rapy were randomly applied at an interval of 24 hours. Data of respiratory system compliance and oxygenation were collected before application of the protocols and 30 minutes after. RESULTS: Twelve patients completed the study. Intragroup analysis, for both techniques showed a statistically significant difference in tidal volume (p=0.002), static compliance (p=0.002) and dynamic compliance (p=0.002). In relation to oxygenation, in the group of manual rib-cage compression, peripheral oxygen saturation increased with a significant difference (p=0.011). CONCLUSIONS: Manual rib-cage compression and PEEP-ZEEP maneuver have positive clinical effects. In relation to oxygenation we found a favorable behavior of peripheral oxygen saturation in the group of manual rib-cage compression.
Keywords:Continuous positive airway pressurePhysical therapy modalitiesPositive pressure respirationRespiration, artificialRespiratory therapySee moreViews0Abstract
Original ArticlesEffects of manual rib-cage compression versus PEEP-ZEEP maneuver on respiratory system compliance and oxygenation in patients receiving mechanical ventilation
Rev Bras Ter Intensiva. 2009;21(2):155-161
DOI 10.1590/S0103-507X2009000200007
Views0OBJECTIVES: Patients unable to perform breathing functions may be submitted to invasive mechanical ventilation. Chest physiotherapy acts directly on the treatment of these patients for the purpose of improving their lung function. The objective of this study was to evaluate the effects of manual rib-cage compression versus the positive end expiratory pressure-zero end expiratory pressure (PEEP-ZEEP) maneuver, on compliance of the respiratory system and oxygenation in patients under invasive mechanical ventilation. METHODS: A double centric, prospective, randomized and crossover study, with patients under invasive mechanical ventilation, in controlled mode for more than 48 hours was carried out. The protocols of chest physiothe-rapy were randomly applied at an interval of 24 hours. Data of respiratory system compliance and oxygenation were collected before application of the protocols and 30 minutes after. RESULTS: Twelve patients completed the study. Intragroup analysis, for both techniques showed a statistically significant difference in tidal volume (p=0.002), static compliance (p=0.002) and dynamic compliance (p=0.002). In relation to oxygenation, in the group of manual rib-cage compression, peripheral oxygen saturation increased with a significant difference (p=0.011). CONCLUSIONS: Manual rib-cage compression and PEEP-ZEEP maneuver have positive clinical effects. In relation to oxygenation we found a favorable behavior of peripheral oxygen saturation in the group of manual rib-cage compression.
Keywords:Continuous positive airway pressurePhysical therapy modalitiesPositive pressure respirationRespiration, artificialRespiratory therapySee more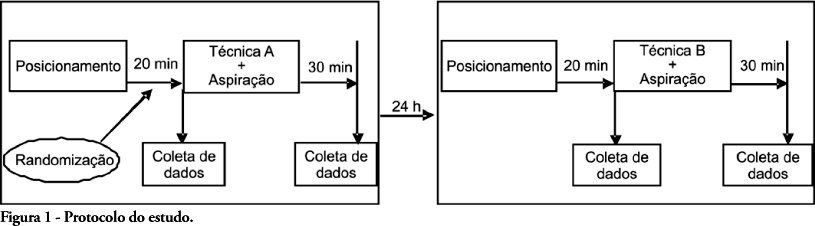
-
Original Articles
Bariatric surgery: is admission to the intensive care unit necessary?
Rev Bras Ter Intensiva. 2009;21(2):162-168
Abstract
Original ArticlesBariatric surgery: is admission to the intensive care unit necessary?
Rev Bras Ter Intensiva. 2009;21(2):162-168
DOI 10.1590/S0103-507X2009000200008
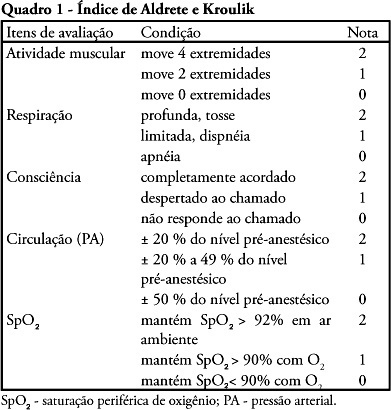
Views0See moreOBJECTIVE: The purpose of this study was to determine the place of stay at postoperative and to verify medical-surgical complications that would justify admission to the intensive care unit, including death. METHODS: Cross-over, prospective, open study that evaluated 120 patients who were submitted to primary bariatric surgery by video laparoscopy from May 2007 to April 2008 in a tertiary hospital. The Aldrete Kroulik index was used for release from the post-anesthesia recovery room and to define where the patient should be routinely referred for postoperative. RESULTS: Among the 120 patients, 83 were women and 37 men with a mean age ranging from 35.4 ± 10.5 years (18 to 66 years), body mass index 45.6 ± 10.5. The time between hospital admission and start of surgery was 140.7 ± 81.8 minutes, surgery time was 105 ± 28.6 minutes, time of post-anesthesia recovery room was between 125 ± 38 minutes and length of hospital stay was 47.7 ± 12.4 hours, with 100% of the patients walking in 24 hours. The Aldrete and Kroulik index in the post-anesthesia recovery room achieved scores of 10 to 120 minutes in all patients, with a 100% survival . CONCLUSION: Using the Aldrete and Kroulik index in the post-anesthesia of gastric bypass by video laparoscopy in primary bariatric surgery, no patient was admitted in intensive care unit and no major complication was observed.
Views0Abstract
Original ArticlesBariatric surgery: is admission to the intensive care unit necessary?
Rev Bras Ter Intensiva. 2009;21(2):162-168
DOI 10.1590/S0103-507X2009000200008
Views0See moreOBJECTIVE: The purpose of this study was to determine the place of stay at postoperative and to verify medical-surgical complications that would justify admission to the intensive care unit, including death. METHODS: Cross-over, prospective, open study that evaluated 120 patients who were submitted to primary bariatric surgery by video laparoscopy from May 2007 to April 2008 in a tertiary hospital. The Aldrete Kroulik index was used for release from the post-anesthesia recovery room and to define where the patient should be routinely referred for postoperative. RESULTS: Among the 120 patients, 83 were women and 37 men with a mean age ranging from 35.4 ± 10.5 years (18 to 66 years), body mass index 45.6 ± 10.5. The time between hospital admission and start of surgery was 140.7 ± 81.8 minutes, surgery time was 105 ± 28.6 minutes, time of post-anesthesia recovery room was between 125 ± 38 minutes and length of hospital stay was 47.7 ± 12.4 hours, with 100% of the patients walking in 24 hours. The Aldrete and Kroulik index in the post-anesthesia recovery room achieved scores of 10 to 120 minutes in all patients, with a 100% survival . CONCLUSION: Using the Aldrete and Kroulik index in the post-anesthesia of gastric bypass by video laparoscopy in primary bariatric surgery, no patient was admitted in intensive care unit and no major complication was observed.
-
Original Articles
Management of emergency situations in patients undergoing tracheostomy
Rev Bras Ter Intensiva. 2009;21(2):169-172
Abstract
Original ArticlesManagement of emergency situations in patients undergoing tracheostomy
Rev Bras Ter Intensiva. 2009;21(2):169-172
DOI 10.1590/S0103-507X2009000200009
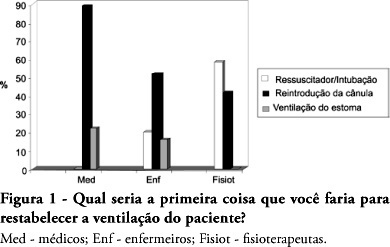
Views1See moreOBJECTIVES: The aim of this study was to evaluate the level of knowledge of health care professionals in an emergency situation related to tracheostomy tube displacement METHODS: a descriptive and exploratory study was carried out with the intensive care unit health professionals of a university hospital in Salvador, Brazil, from July to September 2007. For this purpose, a questionnaire was translated and adapted from a previous study. Questions were: 1- Have you dealt with this emergency? 2 – What is the first thing you do? 3- Do you know what the stay sutures are for? 4 – How are they used in an emergency setting? 5 -Do you know what to do with the introducer? RESULTS: the sample comprised 41 professionals (nine physicians, 20 nurses and 12 physiotherapists). A descriptive analysis showed that 63% of professionals had never experienced such complications. Analysis of a subgroup showed that 42% of physiotherapists, 56% of physicians and 69% of nurses would act inappropriately. Analyzing the level of knowledge about the importance of stay sutures, the study showed that 78% of the sample did not know what they were or how to use them, and 63.4% did not know how to use the introducer correctly. CONCLUSIONS: , regarding the use of a tracheostomy tube in a situation of emergency, the level of knowledge of the professionals evaluated was insufficient. The greatest shortcoming was detected in the level of knowledge about stay sutures.
Views1Abstract
Original ArticlesManagement of emergency situations in patients undergoing tracheostomy
Rev Bras Ter Intensiva. 2009;21(2):169-172
DOI 10.1590/S0103-507X2009000200009
Views1See moreOBJECTIVES: The aim of this study was to evaluate the level of knowledge of health care professionals in an emergency situation related to tracheostomy tube displacement METHODS: a descriptive and exploratory study was carried out with the intensive care unit health professionals of a university hospital in Salvador, Brazil, from July to September 2007. For this purpose, a questionnaire was translated and adapted from a previous study. Questions were: 1- Have you dealt with this emergency? 2 – What is the first thing you do? 3- Do you know what the stay sutures are for? 4 – How are they used in an emergency setting? 5 -Do you know what to do with the introducer? RESULTS: the sample comprised 41 professionals (nine physicians, 20 nurses and 12 physiotherapists). A descriptive analysis showed that 63% of professionals had never experienced such complications. Analysis of a subgroup showed that 42% of physiotherapists, 56% of physicians and 69% of nurses would act inappropriately. Analyzing the level of knowledge about the importance of stay sutures, the study showed that 78% of the sample did not know what they were or how to use them, and 63.4% did not know how to use the introducer correctly. CONCLUSIONS: , regarding the use of a tracheostomy tube in a situation of emergency, the level of knowledge of the professionals evaluated was insufficient. The greatest shortcoming was detected in the level of knowledge about stay sutures.
-
Artigo Original – Pediatria
Outcome and characteristics of infants with acute viral bronchiolitis submitted to mechanical ventilation in a Brazilian pediatric intensive care
Rev Bras Ter Intensiva. 2009;21(2):174-182
Abstract
Artigo Original – PediatriaOutcome and characteristics of infants with acute viral bronchiolitis submitted to mechanical ventilation in a Brazilian pediatric intensive care
Rev Bras Ter Intensiva. 2009;21(2):174-182
DOI 10.1590/S0103-507X2009000200010
Views0OBJECTIVE: To describe the characteristics and the outcome of infants with acute viral bronchiolitis submitted to mechanical ventilation. METHODS: We performed a retrospective study enrolling all infants (less than 12 months old) admitted with the diagnosis of acute viral bronchiolitis and submitted to mechanical ventilation in an university affiliated Brazilian pediatric intensive care unit between March, 2004 and September, 2006 (3 consecutives winters). The mechanical ventilation parameters’ employed on 1st, 2nd, 3rd, 7th day and before extubation were evaluated as well as the evolution (mortality rate, presence of acute respiratory distress syndrome and the prevalence of complications). The groups were compared using the Student t test, the Mann-Whitney U test and the Chi-square test. RESULTS: Fifty-nine infants were included (3.8 ± 2.7 months old, 59% male), with 9.0 ± 9.4 days on mechanical ventilation. Prior mechanical ventilation, non invasive ventilation was instituted in 71% of children. Anemia was observed in 78% of the sample. In 51 infants (86.5%) the lower airway obstructive pattern was maintained up to tracheal extubation with a nil mortality and low prevalence of pneumothorax (7.8%). Acute respiratory distress syndrome occurred in 8 infants (13.5%), with higher mortality and a higher prevalence of pneumothorax (62.5%). CONCLUSIONS: The declining mortality in acute viral bronchiolitis is observed even in non developed regions, involving children with high rates of anemia and premature labor. The low mortality is associated with the maintenance of the lower airway obstructive pattern during the period on mechanical ventilation. The development of acute respiratory distress syndrome is associated with increased mortality and higher prevalence of complications, representing the actual challenge in the management of children with severe acute viral bronchiolitis.
Keywords:acute respiratory distress syndromeBronchiolitis, viralIntubation, intratrachealRespiration, artificialSee moreViews0Abstract
Artigo Original – PediatriaOutcome and characteristics of infants with acute viral bronchiolitis submitted to mechanical ventilation in a Brazilian pediatric intensive care
Rev Bras Ter Intensiva. 2009;21(2):174-182
DOI 10.1590/S0103-507X2009000200010
Views0OBJECTIVE: To describe the characteristics and the outcome of infants with acute viral bronchiolitis submitted to mechanical ventilation. METHODS: We performed a retrospective study enrolling all infants (less than 12 months old) admitted with the diagnosis of acute viral bronchiolitis and submitted to mechanical ventilation in an university affiliated Brazilian pediatric intensive care unit between March, 2004 and September, 2006 (3 consecutives winters). The mechanical ventilation parameters’ employed on 1st, 2nd, 3rd, 7th day and before extubation were evaluated as well as the evolution (mortality rate, presence of acute respiratory distress syndrome and the prevalence of complications). The groups were compared using the Student t test, the Mann-Whitney U test and the Chi-square test. RESULTS: Fifty-nine infants were included (3.8 ± 2.7 months old, 59% male), with 9.0 ± 9.4 days on mechanical ventilation. Prior mechanical ventilation, non invasive ventilation was instituted in 71% of children. Anemia was observed in 78% of the sample. In 51 infants (86.5%) the lower airway obstructive pattern was maintained up to tracheal extubation with a nil mortality and low prevalence of pneumothorax (7.8%). Acute respiratory distress syndrome occurred in 8 infants (13.5%), with higher mortality and a higher prevalence of pneumothorax (62.5%). CONCLUSIONS: The declining mortality in acute viral bronchiolitis is observed even in non developed regions, involving children with high rates of anemia and premature labor. The low mortality is associated with the maintenance of the lower airway obstructive pattern during the period on mechanical ventilation. The development of acute respiratory distress syndrome is associated with increased mortality and higher prevalence of complications, representing the actual challenge in the management of children with severe acute viral bronchiolitis.
Keywords:acute respiratory distress syndromeBronchiolitis, viralIntubation, intratrachealRespiration, artificialSee more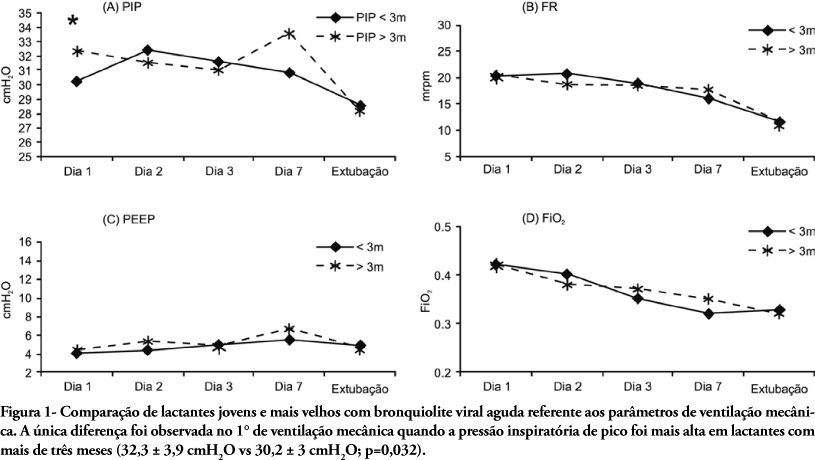
-
Original Article – Neonatologia
Results of airway clearance techniques in respiratory mechanics of preterm neonates under mechanical ventilation
Rev Bras Ter Intensiva. 2009;21(2):183-189
Abstract
Original Article – NeonatologiaResults of airway clearance techniques in respiratory mechanics of preterm neonates under mechanical ventilation
Rev Bras Ter Intensiva. 2009;21(2):183-189
DOI 10.1590/S0103-507X2009000200011
Views0See moreOBJECTIVES: This research aimed to evaluate the repercussions of specific chest physiotherapy procedures in mean airway resistance and in dynamic compliance in preterm infants in mechanical ventilation. METHODS: Eighteen preterm infants in conventional mechanical ventilation were submitted to one session of chest physiotherapy (manual chest compression during expiration + intermittent aspiration of intratracheal cannula). Mean airway resistance and dynamic compliance measurements were taken prior to, 10, 40 and 70 minutes after intervention using a pneumotachograph with graphic display (Newport Navigator GM-250®), coupled to a flow transducer (Varfley-Bicore®). For analysis of results the infants were divided into 2 groups; less than 5 days (group mechanical ventilation <5) and 5 days or more (group mechanical ventilation >5) on mechanical ventilation. Values were analyzed by Friedman Test, with Dunn’s Multiple Comparisons Test (p<0,05 significant). RESULTS: In group mechanical ventilation <5 a significant reduction of mean airway resistance was observed at the 10th minute after intervention (p<0,05). There were no significant alterations in dynamic compliance. The group mechanical ventilation >5 mean airway resistance had a significant reduction at the 10th (p<0,001), 40th (p<0,05) and 70th (p<0,05) minute after intervention. The dynamic compliance improved significantly only at the 10th minute (p<0,05). CONCLUSIONS: The airway clearance techniques used in preterm neonates under conventional mechanical ventilation >5 improved mean airway resistance and dynamic compliance, with best results for the mean airway resistance.
Views0Abstract
Original Article – NeonatologiaResults of airway clearance techniques in respiratory mechanics of preterm neonates under mechanical ventilation
Rev Bras Ter Intensiva. 2009;21(2):183-189
DOI 10.1590/S0103-507X2009000200011
Views0See moreOBJECTIVES: This research aimed to evaluate the repercussions of specific chest physiotherapy procedures in mean airway resistance and in dynamic compliance in preterm infants in mechanical ventilation. METHODS: Eighteen preterm infants in conventional mechanical ventilation were submitted to one session of chest physiotherapy (manual chest compression during expiration + intermittent aspiration of intratracheal cannula). Mean airway resistance and dynamic compliance measurements were taken prior to, 10, 40 and 70 minutes after intervention using a pneumotachograph with graphic display (Newport Navigator GM-250®), coupled to a flow transducer (Varfley-Bicore®). For analysis of results the infants were divided into 2 groups; less than 5 days (group mechanical ventilation <5) and 5 days or more (group mechanical ventilation >5) on mechanical ventilation. Values were analyzed by Friedman Test, with Dunn’s Multiple Comparisons Test (p<0,05 significant). RESULTS: In group mechanical ventilation <5 a significant reduction of mean airway resistance was observed at the 10th minute after intervention (p<0,05). There were no significant alterations in dynamic compliance. The group mechanical ventilation >5 mean airway resistance had a significant reduction at the 10th (p<0,001), 40th (p<0,05) and 70th (p<0,05) minute after intervention. The dynamic compliance improved significantly only at the 10th minute (p<0,05). CONCLUSIONS: The airway clearance techniques used in preterm neonates under conventional mechanical ventilation >5 improved mean airway resistance and dynamic compliance, with best results for the mean airway resistance.
-
Review Articles
Ultrasound-guided venous cannullation in critical care unit
Rev Bras Ter Intensiva. 2009;21(2):190-196
Abstract
Review ArticlesUltrasound-guided venous cannullation in critical care unit
Rev Bras Ter Intensiva. 2009;21(2):190-196
DOI 10.1590/S0103-507X2009000200012
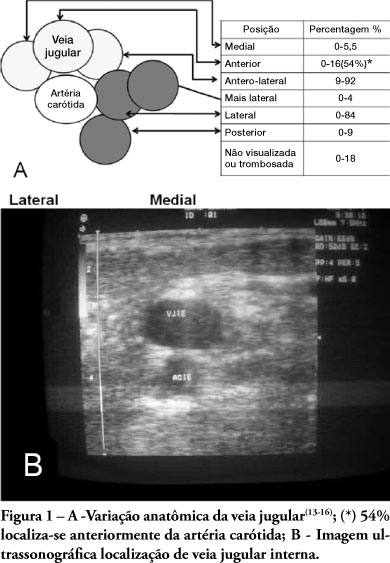
Views0See moreUse of ultrasound introduced as part of intensive care therapy makes viable bedside invasive procedures and diagnosis. Due to portability, combined with team training, its use guarantees less complications related to insertion, as well as patients’ safety. It also reduces severe conditions related to the catheter, such as pneumothorax among others. Probably, in a near future, as purchase of ultrasound equipment becomes easier and team training more adequate, this tool will become essential in daily clinical practice.
Views0Abstract
Review ArticlesUltrasound-guided venous cannullation in critical care unit
Rev Bras Ter Intensiva. 2009;21(2):190-196
DOI 10.1590/S0103-507X2009000200012
Views0See moreUse of ultrasound introduced as part of intensive care therapy makes viable bedside invasive procedures and diagnosis. Due to portability, combined with team training, its use guarantees less complications related to insertion, as well as patients’ safety. It also reduces severe conditions related to the catheter, such as pneumothorax among others. Probably, in a near future, as purchase of ultrasound equipment becomes easier and team training more adequate, this tool will become essential in daily clinical practice.
-
Review Articles
Association of alveolar recruitment maneuvers and prone position in acute respiratory disease syndrome patients
Rev Bras Ter Intensiva. 2009;21(2):197-203
Abstract
Review ArticlesAssociation of alveolar recruitment maneuvers and prone position in acute respiratory disease syndrome patients
Rev Bras Ter Intensiva. 2009;21(2):197-203
DOI 10.1590/S0103-507X2009000200013
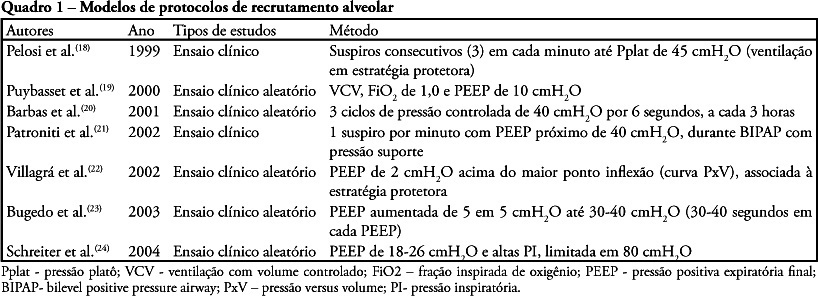
Views0See moreThe acute respiratory distress syndrome is the clinical presentation of acute lung injury characterized by diffuse alveolar damage and development of non-cardiogenic pulmonary edema due to increased pulmonary alveolar-capillary membrane permeability. Alveolar recruitment maneuvers and prone position can be used in the treatment of acute respiratory distress syndrome. The objective of this review of literature was to identify possible benefits, indications, complications and care of the associated recruitment maneuvers and prone position for treatment of the acute respiratory distress syndrome. This national and international scientific literature review was developed according to the established criteria for searching the databases MedLine, LILACS, SciElo, PubMed, Cochrane, from 1994 to 2008 in Portuguese and English, with the key words: acute respiratory distress syndrome, alveolar recruitment maneuver and prone position. Despite advances in the understanding of acute respiratory distress syndrome pathophysiology, mortality is still expressive. Alveolar recruitment maneuvers and prone position significantly contribute to treatment of acute respiratory distress syndrome patient aiming to improve oxygenation and minimizing complications of refractory hypoxemia and reduction of pulmonary compliance. However,as there are few studies in literature associating alveolar recruitment maneuvers and prone position for treatment of acute respiratory distress syndrome, additional research and evidences of clinical application are required.
Views0Abstract
Review ArticlesAssociation of alveolar recruitment maneuvers and prone position in acute respiratory disease syndrome patients
Rev Bras Ter Intensiva. 2009;21(2):197-203
DOI 10.1590/S0103-507X2009000200013
Views0See moreThe acute respiratory distress syndrome is the clinical presentation of acute lung injury characterized by diffuse alveolar damage and development of non-cardiogenic pulmonary edema due to increased pulmonary alveolar-capillary membrane permeability. Alveolar recruitment maneuvers and prone position can be used in the treatment of acute respiratory distress syndrome. The objective of this review of literature was to identify possible benefits, indications, complications and care of the associated recruitment maneuvers and prone position for treatment of the acute respiratory distress syndrome. This national and international scientific literature review was developed according to the established criteria for searching the databases MedLine, LILACS, SciElo, PubMed, Cochrane, from 1994 to 2008 in Portuguese and English, with the key words: acute respiratory distress syndrome, alveolar recruitment maneuver and prone position. Despite advances in the understanding of acute respiratory distress syndrome pathophysiology, mortality is still expressive. Alveolar recruitment maneuvers and prone position significantly contribute to treatment of acute respiratory distress syndrome patient aiming to improve oxygenation and minimizing complications of refractory hypoxemia and reduction of pulmonary compliance. However,as there are few studies in literature associating alveolar recruitment maneuvers and prone position for treatment of acute respiratory distress syndrome, additional research and evidences of clinical application are required.
-
Review Articles
Will use of exhaled breath condensate be useful for the intensive care unit routine?
Rev Bras Ter Intensiva. 2009;21(2):204-211
Abstract
Review ArticlesWill use of exhaled breath condensate be useful for the intensive care unit routine?
Rev Bras Ter Intensiva. 2009;21(2):204-211
DOI 10.1590/S0103-507X2009000200014
Views0See moreEndogenous production of nitric oxide can be detected and monitored in exhaled air of men and animals. The main objective of this review was to discuss if nitric oxide in exhaled breath condensate is a useful tool when investigating respiratory dysfunctions in intensive care units. Specialized literature reveals an increasing interest in the use of exhaled breath condensate as a non-invasive method to investigate pulmonary disease. However, a standardized method for its collection is lacking, and use of different methods of respiratory support complicates comparison among different studies. In addition, the same specialized literature review emphasized possible difficulties for routine use of the exhaled breath condensate in intensive care patients, mainly under mechanical ventilation. Until exhaled breath condensate becomes a routine tool of research and monitoring of intensive care patients, more specific studies and technologies are still necessary. Its importance has been related to physiological control of the pulmonary function and to physiopathology of pulmonary disease involving chronic inflammation and oxidative stress.
Views0Abstract
Review ArticlesWill use of exhaled breath condensate be useful for the intensive care unit routine?
Rev Bras Ter Intensiva. 2009;21(2):204-211
DOI 10.1590/S0103-507X2009000200014
Views0See moreEndogenous production of nitric oxide can be detected and monitored in exhaled air of men and animals. The main objective of this review was to discuss if nitric oxide in exhaled breath condensate is a useful tool when investigating respiratory dysfunctions in intensive care units. Specialized literature reveals an increasing interest in the use of exhaled breath condensate as a non-invasive method to investigate pulmonary disease. However, a standardized method for its collection is lacking, and use of different methods of respiratory support complicates comparison among different studies. In addition, the same specialized literature review emphasized possible difficulties for routine use of the exhaled breath condensate in intensive care patients, mainly under mechanical ventilation. Until exhaled breath condensate becomes a routine tool of research and monitoring of intensive care patients, more specific studies and technologies are still necessary. Its importance has been related to physiological control of the pulmonary function and to physiopathology of pulmonary disease involving chronic inflammation and oxidative stress.
-
Review Articles
Assessment of fluid responsiveness in patients under spontaneous breathing activity
Rev Bras Ter Intensiva. 2009;21(2):212-218
Abstract
Review ArticlesAssessment of fluid responsiveness in patients under spontaneous breathing activity
Rev Bras Ter Intensiva. 2009;21(2):212-218
DOI 10.1590/S0103-507X2009000200015
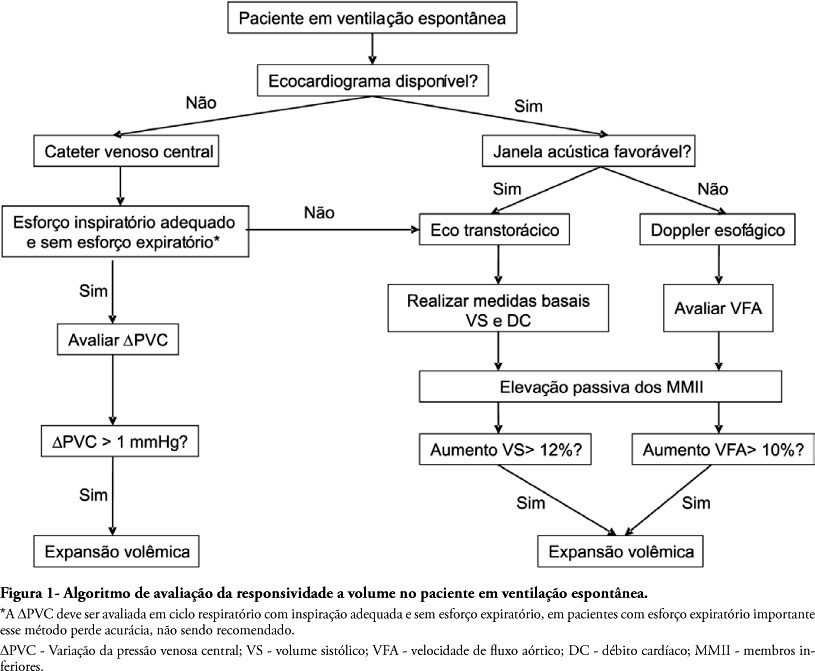
Views0See moreTo assess fluid responsiveness in patients under spontaneous breathing activity ventilation remains a challenge for intensive care physicians. Much of the knowledge on heart-lung interactions and dynamic indexes of fluid responsiveness may not be useful for these patients. Historically, the most frequently used variables to guide fluid responsiveness on this population have been the static preload indexes. However, more recently, dynamic indexes from less invasive devices are being often used, even though their usefulness on spontaneously-breathing subjects remains controversial. The purpose of this article was to review evidences on the assessment of fluid responsiveness in patients under spontaneous ventilation. A search in literature showed poor evidence for use of static variables, such as filling pressures and ventricular end-diastolic volumes. Dynamic indexes, such as pulse pressure variation and other indexes had not been appropriately tested during spontaneous ventilation. Favorable results were found with central venous pressure variation and with transthoracic echocardiography or transesophageal Doppler dynamic indexes, especially when associated to passive lower limb elevation. We conclude that although central venous pressure variation and echocardiography variables could aid bedside clinicians in assessing fluid responsiveness during spontaneous ventilation, more studies on this subject are definitely required.
Views0Abstract
Review ArticlesAssessment of fluid responsiveness in patients under spontaneous breathing activity
Rev Bras Ter Intensiva. 2009;21(2):212-218
DOI 10.1590/S0103-507X2009000200015
Views0See moreTo assess fluid responsiveness in patients under spontaneous breathing activity ventilation remains a challenge for intensive care physicians. Much of the knowledge on heart-lung interactions and dynamic indexes of fluid responsiveness may not be useful for these patients. Historically, the most frequently used variables to guide fluid responsiveness on this population have been the static preload indexes. However, more recently, dynamic indexes from less invasive devices are being often used, even though their usefulness on spontaneously-breathing subjects remains controversial. The purpose of this article was to review evidences on the assessment of fluid responsiveness in patients under spontaneous ventilation. A search in literature showed poor evidence for use of static variables, such as filling pressures and ventricular end-diastolic volumes. Dynamic indexes, such as pulse pressure variation and other indexes had not been appropriately tested during spontaneous ventilation. Favorable results were found with central venous pressure variation and with transthoracic echocardiography or transesophageal Doppler dynamic indexes, especially when associated to passive lower limb elevation. We conclude that although central venous pressure variation and echocardiography variables could aid bedside clinicians in assessing fluid responsiveness during spontaneous ventilation, more studies on this subject are definitely required.
-
How to assess intensive care randomized trials
Rev Bras Ter Intensiva. 2009;21(2):219-225
Abstract
How to assess intensive care randomized trials
Rev Bras Ter Intensiva. 2009;21(2):219-225
DOI 10.1590/S0103-507X2009000200016
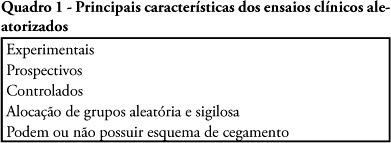
Views0See moreRandomized controlled trials are scientific investigations considered as the gold-standard to evaluate therapeutic interventions. Randomized controlled trials may examine the safety and efficacy of new drugs and therapeutic procedures or compare the effects of two or more drugs or any other intervention. In this article, we present the essential features of these studies, as well as, factors which may bias randomized controlled trials. We also present criteria to critically appraise articles reporting randomized controlled trials, explain how to interpret the results and how to apply them to clinical practice.
Views0Abstract
How to assess intensive care randomized trials
Rev Bras Ter Intensiva. 2009;21(2):219-225
DOI 10.1590/S0103-507X2009000200016
Views0See moreRandomized controlled trials are scientific investigations considered as the gold-standard to evaluate therapeutic interventions. Randomized controlled trials may examine the safety and efficacy of new drugs and therapeutic procedures or compare the effects of two or more drugs or any other intervention. In this article, we present the essential features of these studies, as well as, factors which may bias randomized controlled trials. We also present criteria to critically appraise articles reporting randomized controlled trials, explain how to interpret the results and how to apply them to clinical practice.
-
Case Report
Pulmonary artery rupture by the Swan-Ganz catheter: case report
Rev Bras Ter Intensiva. 2009;21(2):226-230
Abstract
Case ReportPulmonary artery rupture by the Swan-Ganz catheter: case report
Rev Bras Ter Intensiva. 2009;21(2):226-230
DOI 10.1590/S0103-507X2009000200017
Views0See morePulmonary artery catheter is frequently used to monitor patients during liver transplantation. Recently developed less invasive methods for estimating cardiac output and pulmonary capillary wedge pressure together with the failure of randomized studies to demonstrate reduced mortality in pulmonary artery catheter-monitored patients, has restricted its applicability. Pulmonary artery rupture by pulmonary artery catheter is a rare, but dangerous complication. The purpose of this report is to describe a pulmonary artery rupture caused by monitorization with a pulmonary artery catheter, reviewing the clinical approach and discussing hemodynamic monitoring with the pulmonary artery catheter during liver transplantation. A 56 year old female patient, with cirrhosis caused by hepatitis C virus (MELD score 26) presented with acute hepatic encephalopathy. She was medicated and received a liver transplantation with invasive monitoring with a pulmonary artery catheter. In the first 24 hours after surgery, the patient presented with hemodynamic instability, low hematocrit, and cardiorespiratory arrest. After cardiopulmonary resuscitation, hemopericardium was diagnosed by transthoracic echocardiography and even after pericardiocentesis the patient developed recurrent hemopericardium. Pulmonary angiography did not disclose large vessellesions. The pulmonary artery rupture diagnosis was only made after sternotomy and direct lesion observation. Complications from use of pulmonary artery catheter are infrequent, however, due to their clinical severity, can cause high morbidity and mortality. A decreased use of pulmonary artery catheter reduced the number of complications observed. New clinical studies comparing pulmonary artery catheter with non-invasive methods for pulmonary capillary wedge pressure measurement must be conducted in liver transplantation.
Views0Abstract
Case ReportPulmonary artery rupture by the Swan-Ganz catheter: case report
Rev Bras Ter Intensiva. 2009;21(2):226-230
DOI 10.1590/S0103-507X2009000200017
Views0See morePulmonary artery catheter is frequently used to monitor patients during liver transplantation. Recently developed less invasive methods for estimating cardiac output and pulmonary capillary wedge pressure together with the failure of randomized studies to demonstrate reduced mortality in pulmonary artery catheter-monitored patients, has restricted its applicability. Pulmonary artery rupture by pulmonary artery catheter is a rare, but dangerous complication. The purpose of this report is to describe a pulmonary artery rupture caused by monitorization with a pulmonary artery catheter, reviewing the clinical approach and discussing hemodynamic monitoring with the pulmonary artery catheter during liver transplantation. A 56 year old female patient, with cirrhosis caused by hepatitis C virus (MELD score 26) presented with acute hepatic encephalopathy. She was medicated and received a liver transplantation with invasive monitoring with a pulmonary artery catheter. In the first 24 hours after surgery, the patient presented with hemodynamic instability, low hematocrit, and cardiorespiratory arrest. After cardiopulmonary resuscitation, hemopericardium was diagnosed by transthoracic echocardiography and even after pericardiocentesis the patient developed recurrent hemopericardium. Pulmonary angiography did not disclose large vessellesions. The pulmonary artery rupture diagnosis was only made after sternotomy and direct lesion observation. Complications from use of pulmonary artery catheter are infrequent, however, due to their clinical severity, can cause high morbidity and mortality. A decreased use of pulmonary artery catheter reduced the number of complications observed. New clinical studies comparing pulmonary artery catheter with non-invasive methods for pulmonary capillary wedge pressure measurement must be conducted in liver transplantation.
Volume Articles - Critical Care Science (CCS)
