bariatric surgery Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2009;21(2):162-168
DOI 10.1590/S0103-507X2009000200008
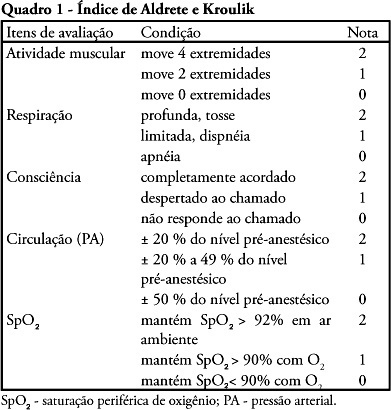
OBJECTIVE: The purpose of this study was to determine the place of stay at postoperative and to verify medical-surgical complications that would justify admission to the intensive care unit, including death. METHODS: Cross-over, prospective, open study that evaluated 120 patients who were submitted to primary bariatric surgery by video laparoscopy from May 2007 to April 2008 in a tertiary hospital. The Aldrete Kroulik index was used for release from the post-anesthesia recovery room and to define where the patient should be routinely referred for postoperative. RESULTS: Among the 120 patients, 83 were women and 37 men with a mean age ranging from 35.4 ± 10.5 years (18 to 66 years), body mass index 45.6 ± 10.5. The time between hospital admission and start of surgery was 140.7 ± 81.8 minutes, surgery time was 105 ± 28.6 minutes, time of post-anesthesia recovery room was between 125 ± 38 minutes and length of hospital stay was 47.7 ± 12.4 hours, with 100% of the patients walking in 24 hours. The Aldrete and Kroulik index in the post-anesthesia recovery room achieved scores of 10 to 120 minutes in all patients, with a 100% survival . CONCLUSION: Using the Aldrete and Kroulik index in the post-anesthesia of gastric bypass by video laparoscopy in primary bariatric surgery, no patient was admitted in intensive care unit and no major complication was observed.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):162-168
DOI 10.1590/S0103-507X2009000200008
OBJECTIVE: The purpose of this study was to determine the place of stay at postoperative and to verify medical-surgical complications that would justify admission to the intensive care unit, including death. METHODS: Cross-over, prospective, open study that evaluated 120 patients who were submitted to primary bariatric surgery by video laparoscopy from May 2007 to April 2008 in a tertiary hospital. The Aldrete Kroulik index was used for release from the post-anesthesia recovery room and to define where the patient should be routinely referred for postoperative. RESULTS: Among the 120 patients, 83 were women and 37 men with a mean age ranging from 35.4 ± 10.5 years (18 to 66 years), body mass index 45.6 ± 10.5. The time between hospital admission and start of surgery was 140.7 ± 81.8 minutes, surgery time was 105 ± 28.6 minutes, time of post-anesthesia recovery room was between 125 ± 38 minutes and length of hospital stay was 47.7 ± 12.4 hours, with 100% of the patients walking in 24 hours. The Aldrete and Kroulik index in the post-anesthesia recovery room achieved scores of 10 to 120 minutes in all patients, with a 100% survival . CONCLUSION: Using the Aldrete and Kroulik index in the post-anesthesia of gastric bypass by video laparoscopy in primary bariatric surgery, no patient was admitted in intensive care unit and no major complication was observed.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):429-434
DOI 10.1590/S0103-507X2008000400017
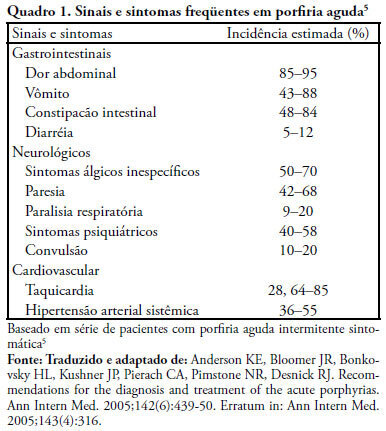
Acute intermittent porphyria is an unusual pathology with potentially severe consequences when not early detected. Among the possible causes of porphyric crises decrease of caloric intake has been described. A case of acute intermittent porphyria in the late postoperative period of a bariatric surgery performed for treatment of obesity is reported. A review of the diagnostic aspects and management of this pathology in the intensive care unit follows. A 31 year old woman was admitted in the intensive care unit three weeks after a bariatric surgery, with decreased level of consciousness and respiratory distress. The patient evolved with psychomotor agitation, mental confusion, abdominal pain and proximal tetraparesis. Diagnosis investigation disclosed severe hyponatremia (92mEq/L), hypomagnesemia, hypophosfatemia and hypocalcemia and cloudy urine without hematuria. Acute porphyria was suspected and the urine test detected high delta amino-levulinic acid and porphobilinogen. Treatment consisted of a correction of electrolyte disturbances and high carbohydrate intake. Hematin and heme arginate were not used, due to the difficulty to acquire the medication. After 8 months the patient progressed with full recovery of muscle strength and a clinical improvement. Acute intermittent porphyria has signs and symptoms common to several clinical, neurological, psychiatric and gastroenterological pathologies, which complicate diagnosis. Therefore, acute intermittent porphyria should be included in the differential diagnosis of neurological, psychiatric and gastroenterological alterations when results of all other exams are normal. Attention must be given to patients undergoing surgery mainly bariatric that, in addition to procedure stress, substantially limit the total caloric intake, potentially triggering crises. Review of literature did not disclose any report of acute intermittent porphyria crisis induced by bariatric surgery.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):429-434
DOI 10.1590/S0103-507X2008000400017
Acute intermittent porphyria is an unusual pathology with potentially severe consequences when not early detected. Among the possible causes of porphyric crises decrease of caloric intake has been described. A case of acute intermittent porphyria in the late postoperative period of a bariatric surgery performed for treatment of obesity is reported. A review of the diagnostic aspects and management of this pathology in the intensive care unit follows. A 31 year old woman was admitted in the intensive care unit three weeks after a bariatric surgery, with decreased level of consciousness and respiratory distress. The patient evolved with psychomotor agitation, mental confusion, abdominal pain and proximal tetraparesis. Diagnosis investigation disclosed severe hyponatremia (92mEq/L), hypomagnesemia, hypophosfatemia and hypocalcemia and cloudy urine without hematuria. Acute porphyria was suspected and the urine test detected high delta amino-levulinic acid and porphobilinogen. Treatment consisted of a correction of electrolyte disturbances and high carbohydrate intake. Hematin and heme arginate were not used, due to the difficulty to acquire the medication. After 8 months the patient progressed with full recovery of muscle strength and a clinical improvement. Acute intermittent porphyria has signs and symptoms common to several clinical, neurological, psychiatric and gastroenterological pathologies, which complicate diagnosis. Therefore, acute intermittent porphyria should be included in the differential diagnosis of neurological, psychiatric and gastroenterological alterations when results of all other exams are normal. Attention must be given to patients undergoing surgery mainly bariatric that, in addition to procedure stress, substantially limit the total caloric intake, potentially triggering crises. Review of literature did not disclose any report of acute intermittent porphyria crisis induced by bariatric surgery.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):205-209
DOI 10.1590/S0103-507X2007000200011
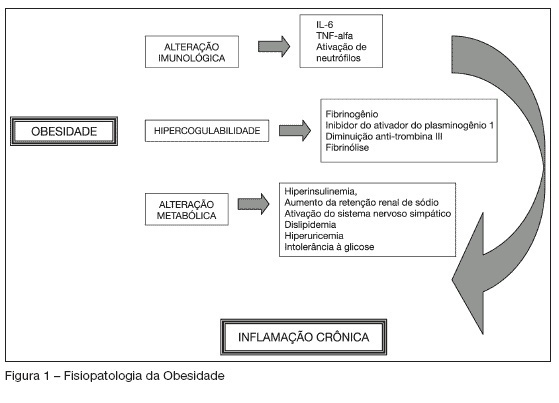
BACKGROUND AND OBJECTIVES: Obesity is an epidemic disease reaching more than 300 million people all over the world. Its prevalence has increased during the past few years and according to some studies its mortality in the critically ill patient seems to be much higher, especially among patients who were submitted to surgery. This study has as objective to discuss some particularities of managing obese patients in the intensive care unit after bariatric surgery. CONTENTS: The rate of obese patient in the ICU ranges from 9% to 26% and the increase in the number of bariatric surgeries has raised the number of obese patients in the ICU. It is important to know the physiopathology of obesity and to treat its particularities during the postoperative care. Such as pulmonary restriction, that causes an increase in pulmonary complications, coronary artery disease and thromboembolic events. CONCLUSIONS: The number of patients that undergo to bariatric surgery has increased; therefore, the number of obese patients in the ICU has also risen. Different physiological events and complications in obese patients are challenges to clinical practice. The knowledge of obese physiopathology helps in the managing routine procedures and complications after bariatric surgery.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):205-209
DOI 10.1590/S0103-507X2007000200011
BACKGROUND AND OBJECTIVES: Obesity is an epidemic disease reaching more than 300 million people all over the world. Its prevalence has increased during the past few years and according to some studies its mortality in the critically ill patient seems to be much higher, especially among patients who were submitted to surgery. This study has as objective to discuss some particularities of managing obese patients in the intensive care unit after bariatric surgery. CONTENTS: The rate of obese patient in the ICU ranges from 9% to 26% and the increase in the number of bariatric surgeries has raised the number of obese patients in the ICU. It is important to know the physiopathology of obesity and to treat its particularities during the postoperative care. Such as pulmonary restriction, that causes an increase in pulmonary complications, coronary artery disease and thromboembolic events. CONCLUSIONS: The number of patients that undergo to bariatric surgery has increased; therefore, the number of obese patients in the ICU has also risen. Different physiological events and complications in obese patients are challenges to clinical practice. The knowledge of obese physiopathology helps in the managing routine procedures and complications after bariatric surgery.