-
Special Article
Brazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19: Joint guideline of Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia, Sociedade Brasileira de Reumatologia
- Maicon Falavigna
 ,
, - Cinara Stein ,
- José Luiz Gomes do Amaral ,
- Luciano Cesar Pontes de Azevedo ,
- Karlyse Claudino Belli , [ … ],
- Carlos Roberto Ribeiro de Carvalho
Abstract
Special ArticleBrazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19: Joint guideline of Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia, Sociedade Brasileira de Reumatologia
Rev Bras Ter Intensiva. 2022;34(1):1-12
DOI 10.5935/0103-507X.20220001-en
- Maicon Falavigna ,
- Cinara Stein ,
- José Luiz Gomes do Amaral ,
- Luciano Cesar Pontes de Azevedo ,
- Karlyse Claudino Belli ,
- Verônica Colpani ,
- Clóvis Arns da Cunha ,
- Felipe Dal-Pizzol ,
- Maria Beatriz Souza Dias,
- Juliana Carvalho Ferreira ,
- Ana Paula da Rocha Freitas,
- Débora Dalmas Gräf ,
- Hélio Penna Guimarães ,
- Suzana Margareth Ajeje Lobo ,
- José Tadeu Monteiro ,
- Michelle Silva Nunes ,
- Maura Salaroli de Oliveira ,
- Clementina Corah Lucas Prado,
- Vania Cristina Canuto Santos ,
- Rosemeri Maurici da Silva ,
- Marcone Lima Sobreira ,
- Viviane Cordeiro Veiga ,
- Ávila Teixeira Vidal ,
- Ricardo Machado Xavier ,
- Alexandre Prehn Zavascki ,
- Flávia Ribeiro Machado ,
- Carlos Roberto Ribeiro de Carvalho
Views7See moreABSTRACT
Objective:
Several therapies are being used or proposed for COVID-19, and many lack appropriate evaluations of their effectiveness and safety. The purpose of this document is to develop recommendations to support decisions regarding the pharmacological treatment of patients hospitalized with COVID-19 in Brazil.
Methods:
A group of 27 experts, including representatives of the Ministry of Health and methodologists, created this guideline. The method used for the rapid development of guidelines was based on the adoption and/or adaptation of existing international guidelines (GRADE ADOLOPMENT) and supported by the e-COVID-19 RecMap platform. The quality of the evidence and the preparation of the recommendations followed the GRADE method.
Results:
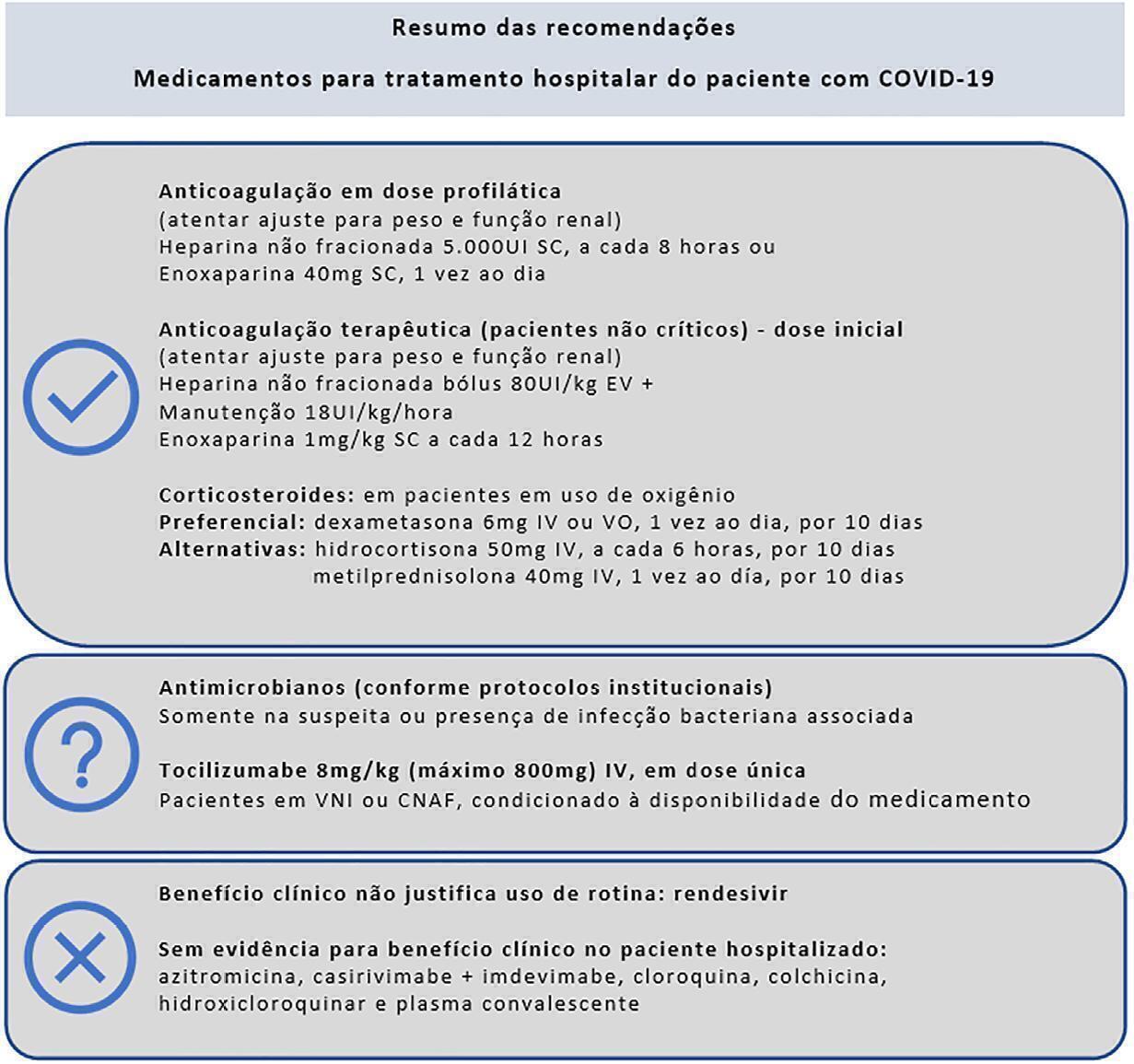
Sixteen recommendations were generated. They include strong recommendations for the use of corticosteroids in patients using supplemental oxygen, the use of anticoagulants at prophylactic doses to prevent thromboembolism and the nonuse of antibiotics in patients without suspected bacterial infection. It was not possible to make a recommendation regarding the use of tocilizumab in patients hospitalized with COVID-19 using oxygen due to uncertainties regarding the availability of and access to the drug. Strong recommendations against the use of hydroxychloroquine, convalescent plasma, colchicine, lopinavir + ritonavir and antibiotics in patients without suspected bacterial infection and also conditional recommendations against the use of casirivimab + imdevimab, ivermectin and rendesivir were made.
Conclusion:
To date, few therapies have proven effective in the treatment of hospitalized patients with COVID-19, and only corticosteroids and prophylaxis for thromboembolism are recommended. Several drugs were considered ineffective and should not be used to provide the best treatment according to the principles of evidence-based medicine and promote economical resource use.
Views7

Abstract
Special ArticleBrazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19: Joint guideline of Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia, Sociedade Brasileira de Reumatologia
Rev Bras Ter Intensiva. 2022;34(1):1-12
DOI 10.5935/0103-507X.20220001-en
- Maicon Falavigna ,
- Cinara Stein ,
- José Luiz Gomes do Amaral ,
- Luciano Cesar Pontes de Azevedo ,
- Karlyse Claudino Belli ,
- Verônica Colpani ,
- Clóvis Arns da Cunha ,
- Felipe Dal-Pizzol ,
- Maria Beatriz Souza Dias,
- Juliana Carvalho Ferreira ,
- Ana Paula da Rocha Freitas,
- Débora Dalmas Gräf ,
- Hélio Penna Guimarães ,
- Suzana Margareth Ajeje Lobo ,
- José Tadeu Monteiro ,
- Michelle Silva Nunes ,
- Maura Salaroli de Oliveira ,
- Clementina Corah Lucas Prado,
- Vania Cristina Canuto Santos ,
- Rosemeri Maurici da Silva ,
- Marcone Lima Sobreira ,
- Viviane Cordeiro Veiga ,
- Ávila Teixeira Vidal ,
- Ricardo Machado Xavier ,
- Alexandre Prehn Zavascki ,
- Flávia Ribeiro Machado ,
- Carlos Roberto Ribeiro de Carvalho
Views7See moreABSTRACT
Objective:
Several therapies are being used or proposed for COVID-19, and many lack appropriate evaluations of their effectiveness and safety. The purpose of this document is to develop recommendations to support decisions regarding the pharmacological treatment of patients hospitalized with COVID-19 in Brazil.
Methods:
A group of 27 experts, including representatives of the Ministry of Health and methodologists, created this guideline. The method used for the rapid development of guidelines was based on the adoption and/or adaptation of existing international guidelines (GRADE ADOLOPMENT) and supported by the e-COVID-19 RecMap platform. The quality of the evidence and the preparation of the recommendations followed the GRADE method.
Results:
Sixteen recommendations were generated. They include strong recommendations for the use of corticosteroids in patients using supplemental oxygen, the use of anticoagulants at prophylactic doses to prevent thromboembolism and the nonuse of antibiotics in patients without suspected bacterial infection. It was not possible to make a recommendation regarding the use of tocilizumab in patients hospitalized with COVID-19 using oxygen due to uncertainties regarding the availability of and access to the drug. Strong recommendations against the use of hydroxychloroquine, convalescent plasma, colchicine, lopinavir + ritonavir and antibiotics in patients without suspected bacterial infection and also conditional recommendations against the use of casirivimab + imdevimab, ivermectin and rendesivir were made.
Conclusion:
To date, few therapies have proven effective in the treatment of hospitalized patients with COVID-19, and only corticosteroids and prophylaxis for thromboembolism are recommended. Several drugs were considered ineffective and should not be used to provide the best treatment according to the principles of evidence-based medicine and promote economical resource use.
- Maicon Falavigna
-
Special Article
Antivirals for adult patients hospitalized with SARS-CoV-2 infection: A randomized, Phase II/III, multicenter, placebo-controlled, adaptive study, with multiple arms and stages. COALITION COVID-19 BRAZIL IX – REVOLUTIOn: protocol and statistical analysis plan
- Israel Silva Maia ,
- Aline Marcadenti ,
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Renato Hideo Nakagawa Santos , [ … ],
- Alexandre Biasi Cavalcanti
Abstract
Special ArticleAntivirals for adult patients hospitalized with SARS-CoV-2 infection: A randomized, Phase II/III, multicenter, placebo-controlled, adaptive study, with multiple arms and stages. COALITION COVID-19 BRAZIL IX – REVOLUTIOn: protocol and statistical analysis plan
Rev Bras Ter Intensiva. 2022;34(1):44-55
DOI 10.5935/0103-507X.20220002-en
- Israel Silva Maia ,
- Aline Marcadenti ,
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Renato Hideo Nakagawa Santos ,
- Karina Leal Negrelli ,
- Samara Pinheiro do Carmo Gomes ,
- Jaqueline Oliveira Gomes ,
- Mariana Barbosa dos Santos Carollo ,
- Tamiris Abait Miranda ,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira ,
- Glauco Adrieno Westphal ,
- Jacques Gabriel Alvares Horta ,
- Uri Adrian Prync Flato ,
- Camilo Fernandes ,
- Waldemar Carlos Barros ,
- Renata S Bolan ,
- Otávio Celso Eluf Gebara ,
- Meton Soares de Alencar Filho ,
- Victor Augusto Hamamoto ,
- Mauro Esteves Hernandes ,
- Nicole Alberti Golin ,
- Ronald Torres de Olinda ,
- Flávia Ribeiro Machado ,
- Régis Goulart Rosa ,
- Viviane Cordeiro Veiga ,
- Luciano César Pontes de Azevedo ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Tiago Moreno L Souza ,
- Otávio Berwanger ,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Repurposed drugs are important in resource-limited settings because the interventions are more rapidly available, have already been tested safely in other populations and are inexpensive. Repurposed drugs are an effective solution, especially for emerging diseases such as COVID-19. The REVOLUTIOn trial has the objective of evaluating three repurposed antiviral drugs, atazanavir, daclatasvir and sofosbuvir, already used for HIV- and hepatitis C virus-infected patients in a randomized, placebo-controlled, adaptive, multiarm, multistage study. The drugs will be tested simultaneously in a Phase II trial to first identify whether any of these drugs alone or in combination reduce the viral load. If they do, a Phase III trial will be initiated to investigate if these medications are capable of increasing the number of days free respiratory support. Participants must be hospitalized adults aged ≥ 18 years with initiation of symptoms ≤ 9 days and SpO2 ≤ 94% in room air or a need for supplemental oxygen to maintain an SpO2 > 94%. The expected total sample size ranges from 252 to 1,005 participants, depending on the number of stages that will be completed in the study. Hence, the protocol is described here in detail together with the statistical analysis plan. In conclusion, the REVOLUTIOn trial is designed to provide evidence on whether atazanavir, daclatasvir or sofosbuvir decrease the SARS-CoV-2 load in patients with COVID-19 and increase the number of days patients are free of respiratory support. In this protocol paper, we describe the rationale, design, and status of the trial.
ClinicalTrials.gov identifier:
Keywords:Antiviral agentsCoronavirus infectionsCOVID-19DaclatasvirprotocolRespiratory insufficiencySofosbuvirSee moreViews2Abstract
Special ArticleAntivirals for adult patients hospitalized with SARS-CoV-2 infection: A randomized, Phase II/III, multicenter, placebo-controlled, adaptive study, with multiple arms and stages. COALITION COVID-19 BRAZIL IX – REVOLUTIOn: protocol and statistical analysis plan
Rev Bras Ter Intensiva. 2022;34(1):44-55
DOI 10.5935/0103-507X.20220002-en
- Israel Silva Maia ,
- Aline Marcadenti ,
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Renato Hideo Nakagawa Santos ,
- Karina Leal Negrelli ,
- Samara Pinheiro do Carmo Gomes ,
- Jaqueline Oliveira Gomes ,
- Mariana Barbosa dos Santos Carollo ,
- Tamiris Abait Miranda ,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira ,
- Glauco Adrieno Westphal ,
- Jacques Gabriel Alvares Horta ,
- Uri Adrian Prync Flato ,
- Camilo Fernandes ,
- Waldemar Carlos Barros ,
- Renata S Bolan ,
- Otávio Celso Eluf Gebara ,
- Meton Soares de Alencar Filho ,
- Victor Augusto Hamamoto ,
- Mauro Esteves Hernandes ,
- Nicole Alberti Golin ,
- Ronald Torres de Olinda ,
- Flávia Ribeiro Machado ,
- Régis Goulart Rosa ,
- Viviane Cordeiro Veiga ,
- Luciano César Pontes de Azevedo ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Tiago Moreno L Souza ,
- Otávio Berwanger ,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Repurposed drugs are important in resource-limited settings because the interventions are more rapidly available, have already been tested safely in other populations and are inexpensive. Repurposed drugs are an effective solution, especially for emerging diseases such as COVID-19. The REVOLUTIOn trial has the objective of evaluating three repurposed antiviral drugs, atazanavir, daclatasvir and sofosbuvir, already used for HIV- and hepatitis C virus-infected patients in a randomized, placebo-controlled, adaptive, multiarm, multistage study. The drugs will be tested simultaneously in a Phase II trial to first identify whether any of these drugs alone or in combination reduce the viral load. If they do, a Phase III trial will be initiated to investigate if these medications are capable of increasing the number of days free respiratory support. Participants must be hospitalized adults aged ≥ 18 years with initiation of symptoms ≤ 9 days and SpO2 ≤ 94% in room air or a need for supplemental oxygen to maintain an SpO2 > 94%. The expected total sample size ranges from 252 to 1,005 participants, depending on the number of stages that will be completed in the study. Hence, the protocol is described here in detail together with the statistical analysis plan. In conclusion, the REVOLUTIOn trial is designed to provide evidence on whether atazanavir, daclatasvir or sofosbuvir decrease the SARS-CoV-2 load in patients with COVID-19 and increase the number of days patients are free of respiratory support. In this protocol paper, we describe the rationale, design, and status of the trial.
ClinicalTrials.gov identifier:
Keywords:Antiviral agentsCoronavirus infectionsCOVID-19DaclatasvirprotocolRespiratory insufficiencySofosbuvirSee more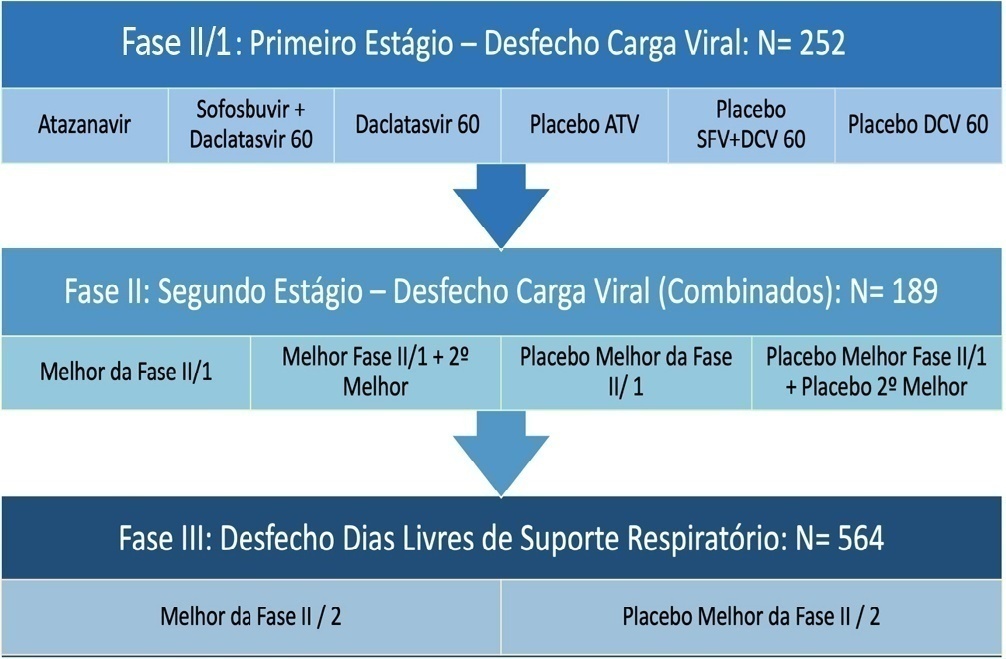
- Israel Silva Maia
-
Special Article
Statistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
- Otavio Ranzani ,
- Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz , [ … ],
- Danilo Teixeira Noritomi
Abstract
Special ArticleStatistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
- Otavio Ranzani ,
- Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz ,
- Eduardo Cordioli ,
- Renata Albaladejo Morbeck ,
- Otávio Berwanger ,
- Lúbia Caus de Morais ,
- Guilherme Schettino ,
- Alexandre Biasi Cavalcanti ,
- Regis Goulart Rosa ,
- Rodrigo Santos Biondi ,
- Jorge Ibrain Figueira Salluh ,
- Luciano César Pontes de Azevedo ,
- Ary Serpa Neto ,
- Danilo Teixeira Noritomi
Views2ABSTRACT
Objective:
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
Methods:
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
Conclusion:
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Keywords:BrazilCritical careData interpretation, statisticalHospital mortalityIntensive care unitsLength of stayPatient care teamResearch designTelemedicineSee moreViews2Abstract
Special ArticleStatistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
- Otavio Ranzani ,
- Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz ,
- Eduardo Cordioli ,
- Renata Albaladejo Morbeck ,
- Otávio Berwanger ,
- Lúbia Caus de Morais ,
- Guilherme Schettino ,
- Alexandre Biasi Cavalcanti ,
- Regis Goulart Rosa ,
- Rodrigo Santos Biondi ,
- Jorge Ibrain Figueira Salluh ,
- Luciano César Pontes de Azevedo ,
- Ary Serpa Neto ,
- Danilo Teixeira Noritomi
Views2ABSTRACT
Objective:
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
Methods:
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
Conclusion:
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Keywords:BrazilCritical careData interpretation, statisticalHospital mortalityIntensive care unitsLength of stayPatient care teamResearch designTelemedicineSee more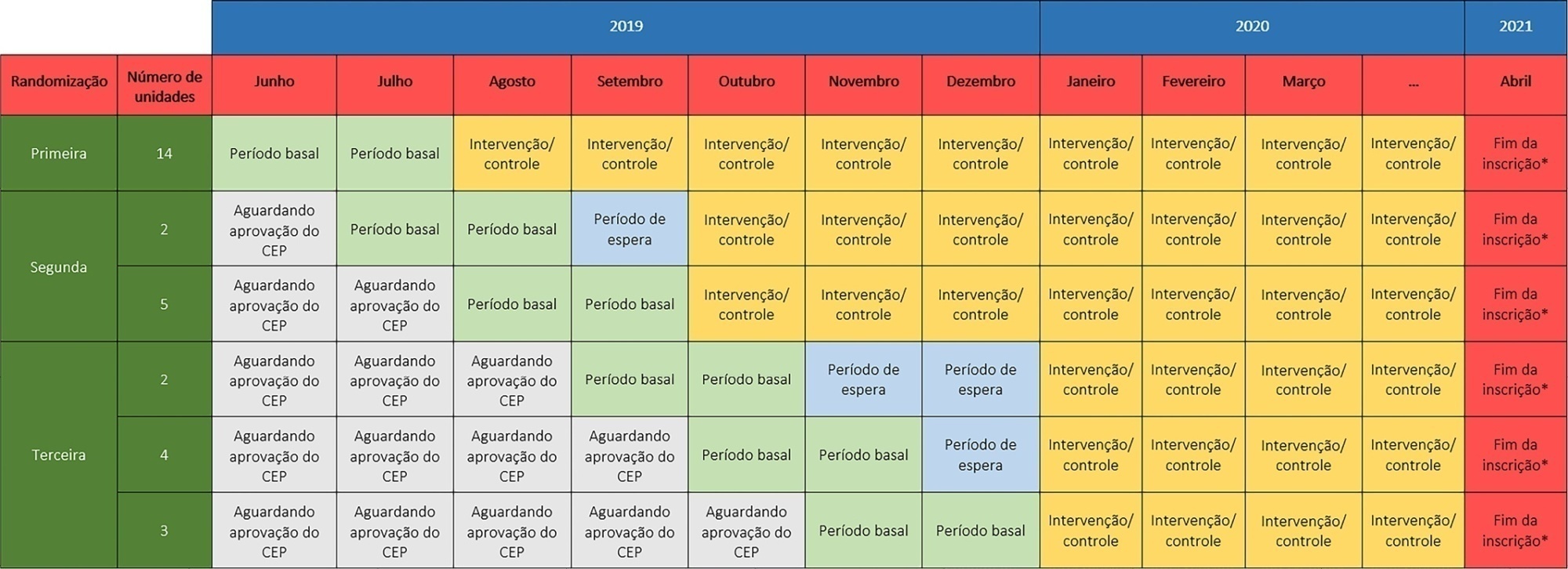
- Otavio Ranzani
-
Special Article
Hemodynamic phenotype-based, capillary refill time-targeted resuscitation in early septic shock: The ANDROMEDA-SHOCK-2 Randomized Clinical Trial study protocol
- Eduardo Kattan ,
- Jan Bakker ,
- Elisa Estenssoro ,
- Gustavo Adolfo Ospina-Tascón ,
- Alexandre Biasi Cavalcanti , [ … ],
- Glenn Hernández
Abstract
Special ArticleHemodynamic phenotype-based, capillary refill time-targeted resuscitation in early septic shock: The ANDROMEDA-SHOCK-2 Randomized Clinical Trial study protocol
Rev Bras Ter Intensiva. 2022;34(1):96-106
DOI 10.5935/0103-507X.20220004-en
- Eduardo Kattan ,
- Jan Bakker ,
- Elisa Estenssoro ,
- Gustavo Adolfo Ospina-Tascón ,
- Alexandre Biasi Cavalcanti ,
- Daniel De Backer ,
- Antoine Vieillard-Baron ,
- Jean-Louis Teboul ,
- Ricardo Castro ,
- Glenn Hernández
Views5ABSTRACT
Background:
Early reversion of sepsis-induced tissue hypoperfusion is essential for survival in septic shock. However, consensus regarding the best initial resuscitation strategy is lacking given that interventions designed for the entire population with septic shock might produce unnecessary fluid administration. This article reports the rationale, study design and analysis plan of the ANDROMEDA-2 study, which aims to determine whether a peripheral perfusion-guided strategy consisting of capillary refill time-targeted resuscitation based on clinical and hemodynamic phenotypes is associated with a decrease in a composite outcome of mortality, time to organ support cessation, and hospital length of stay compared to standard care in patients with early (< 4 hours of diagnosis) septic shock.
Methods:
The ANDROMEDA-2 study is a multicenter, multinational randomized controlled trial. In the intervention group, capillary refill time will be measured hourly for 6 hours. If abnormal, patients will enter an algorithm starting with pulse pressure assessment. Patients with pulse pressure less than 40mmHg will be tested for fluid responsiveness and receive fluids accordingly. In patients with pulse pressure > 40mmHg, norepinephrine will be titrated to maintain diastolic arterial pressure > 50mmHg. Patients who fail to normalize capillary refill time after the previous steps will be subjected to critical care echocardiography for cardiac dysfunction evaluation and subsequent management. Finally, vasopressor and inodilator tests will be performed to further optimize perfusion. A sample size of 1,500 patients will provide 88% power to demonstrate superiority of the capillary refill time-targeted strategy.
Conclusions:
If hemodynamic phenotype-based, capillary refill time-targeted resuscitation demonstrates to be a superior strategy, care processes in septic shock resuscitation can be optimized with bedside tools.
Keywords:AlgorithmCapillary refill timeCritical careEchocardiographyLength of staynorepinephrinePerfusionPhenotypeSepsisSeptic shockSee moreViews5Abstract
Special ArticleHemodynamic phenotype-based, capillary refill time-targeted resuscitation in early septic shock: The ANDROMEDA-SHOCK-2 Randomized Clinical Trial study protocol
Rev Bras Ter Intensiva. 2022;34(1):96-106
DOI 10.5935/0103-507X.20220004-en
- Eduardo Kattan ,
- Jan Bakker ,
- Elisa Estenssoro ,
- Gustavo Adolfo Ospina-Tascón ,
- Alexandre Biasi Cavalcanti ,
- Daniel De Backer ,
- Antoine Vieillard-Baron ,
- Jean-Louis Teboul ,
- Ricardo Castro ,
- Glenn Hernández
Views5ABSTRACT
Background:
Early reversion of sepsis-induced tissue hypoperfusion is essential for survival in septic shock. However, consensus regarding the best initial resuscitation strategy is lacking given that interventions designed for the entire population with septic shock might produce unnecessary fluid administration. This article reports the rationale, study design and analysis plan of the ANDROMEDA-2 study, which aims to determine whether a peripheral perfusion-guided strategy consisting of capillary refill time-targeted resuscitation based on clinical and hemodynamic phenotypes is associated with a decrease in a composite outcome of mortality, time to organ support cessation, and hospital length of stay compared to standard care in patients with early (< 4 hours of diagnosis) septic shock.
Methods:
The ANDROMEDA-2 study is a multicenter, multinational randomized controlled trial. In the intervention group, capillary refill time will be measured hourly for 6 hours. If abnormal, patients will enter an algorithm starting with pulse pressure assessment. Patients with pulse pressure less than 40mmHg will be tested for fluid responsiveness and receive fluids accordingly. In patients with pulse pressure > 40mmHg, norepinephrine will be titrated to maintain diastolic arterial pressure > 50mmHg. Patients who fail to normalize capillary refill time after the previous steps will be subjected to critical care echocardiography for cardiac dysfunction evaluation and subsequent management. Finally, vasopressor and inodilator tests will be performed to further optimize perfusion. A sample size of 1,500 patients will provide 88% power to demonstrate superiority of the capillary refill time-targeted strategy.
Conclusions:
If hemodynamic phenotype-based, capillary refill time-targeted resuscitation demonstrates to be a superior strategy, care processes in septic shock resuscitation can be optimized with bedside tools.
Keywords:AlgorithmCapillary refill timeCritical careEchocardiographyLength of staynorepinephrinePerfusionPhenotypeSepsisSeptic shockSee more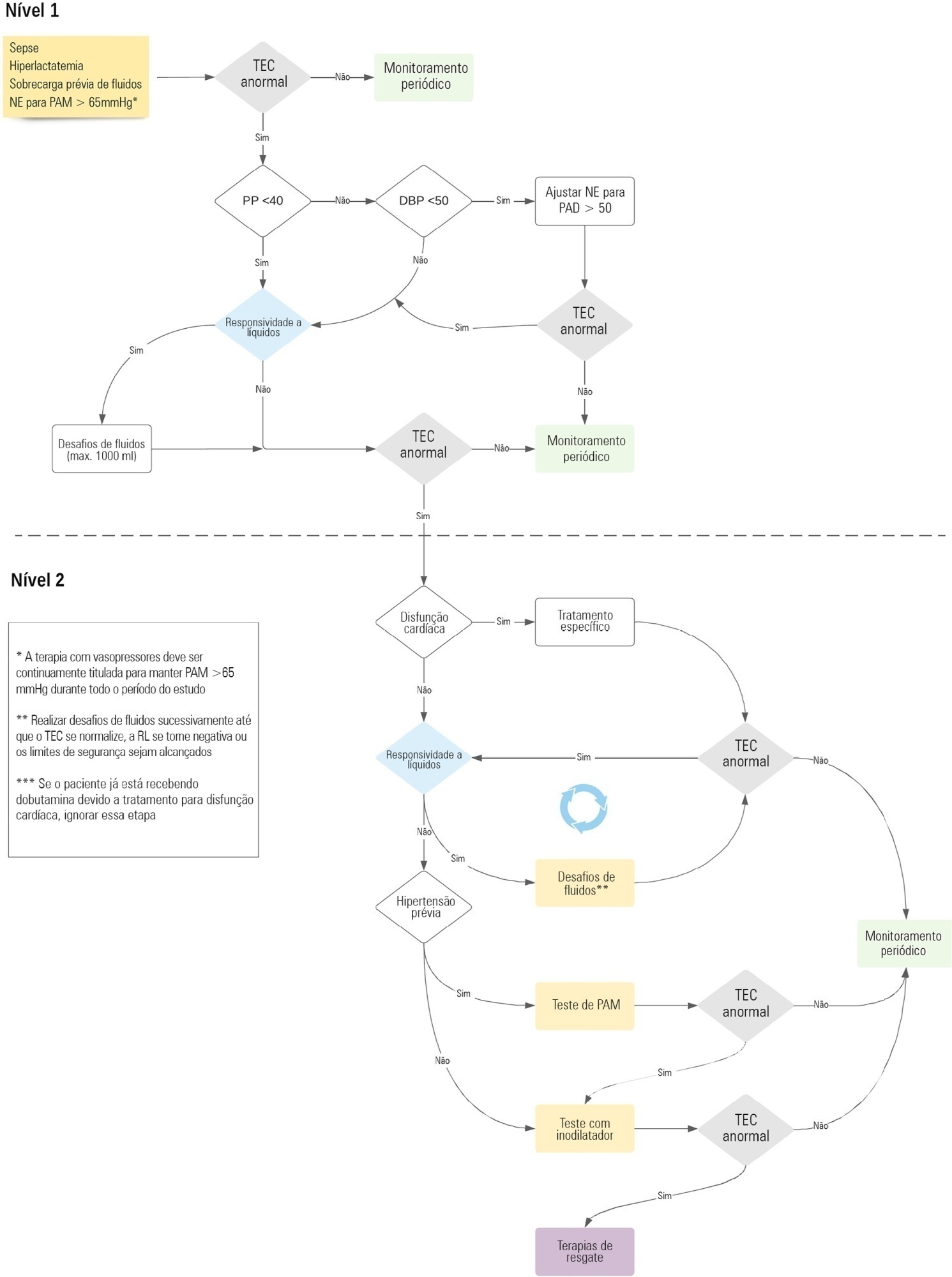
- Eduardo Kattan
-
Original Article
A nationwide survey on health resources and clinical practices during the early COVID-19 pandemic in Brazil
- Pedro Paulo Zanella do Amaral Campos ,
- Guilherme Martins de Souza ,
- Thais Midega ,
- Hélio Penna Guimarães ,
- Thiago Domingos Corrêa , [ … ],
- Ricardo Luiz Cordioli
Abstract
Original ArticleA nationwide survey on health resources and clinical practices during the early COVID-19 pandemic in Brazil
Rev Bras Ter Intensiva. 2022;34(1):107-115
DOI 10.5935/0103-507X.20220005-en
- Pedro Paulo Zanella do Amaral Campos ,
- Guilherme Martins de Souza ,
- Thais Midega ,
- Hélio Penna Guimarães ,
- Thiago Domingos Corrêa ,
- Ricardo Luiz Cordioli
Views1ABSTRACT
Objective:
To evaluate clinical practices and hospital resource organization during the early COVID-19 pandemic in Brazil.
Methods:
This was a multicenter, cross-sectional survey. An electronic questionnaire was provided to emergency department and intensive care unit physicians attending COVID-19 patients. The survey comprised four domains: characteristics of the participants, clinical practices, COVID-19 treatment protocols and hospital resource organization.
Results:
Between May and June 2020, 284 participants [median (interquartile ranges) age 39 (33 – 47) years, 56.3% men] responded to the survey; 33% were intensivists, and 9% were emergency medicine specialists. Half of the respondents worked in public hospitals. Noninvasive ventilation (89% versus 73%; p = 0.001) and highflow nasal cannula (49% versus 32%; p = 0.005) were reported to be more commonly available in private hospitals than in public hospitals. Mechanical ventilation was more commonly used in public hospitals than private hospitals (70% versus 50%; p = 0,024). In the Emergency Departments, positive endexpiratory pressure was most commonly adjusted according to SpO2, while in the intensive care units, positive end-expiratory pressure was adjusted according to the best lung compliance. In the Emergency Departments, 25% of the respondents did not know how to set positive end-expiratory pressure. Compared to private hospitals, public hospitals had a lower availability of protocols for personal protection equipment during tracheal intubation (82% versus 94%; p = 0.005), managing mechanical ventilation [64% versus 75%; p = 0.006] and weaning patients from mechanical ventilation [34% versus 54%; p = 0.002]. Finally, patients spent less time in the emergency department before being transferred to the intensive care unit in private hospitals than in public hospitals [2 (1 – 3) versus 5 (2 – 24) hours; p < 0.001].
Conclusion:
This survey revealed significant heterogeneity in the organization of hospital resources, clinical practices and treatments among physicians during the early COVID-19 pandemic in Brazil.
Keywords:BrazilCoronavirus infectionsCOVID-19Emergency servicehospitalHospital administrationIntensive care unitsPandemicsPhysiciansPractice patternsSurveys and questionnairesSee moreViews1Abstract
Original ArticleA nationwide survey on health resources and clinical practices during the early COVID-19 pandemic in Brazil
Rev Bras Ter Intensiva. 2022;34(1):107-115
DOI 10.5935/0103-507X.20220005-en
- Pedro Paulo Zanella do Amaral Campos ,
- Guilherme Martins de Souza ,
- Thais Midega ,
- Hélio Penna Guimarães ,
- Thiago Domingos Corrêa ,
- Ricardo Luiz Cordioli
Views1ABSTRACT
Objective:
To evaluate clinical practices and hospital resource organization during the early COVID-19 pandemic in Brazil.
Methods:
This was a multicenter, cross-sectional survey. An electronic questionnaire was provided to emergency department and intensive care unit physicians attending COVID-19 patients. The survey comprised four domains: characteristics of the participants, clinical practices, COVID-19 treatment protocols and hospital resource organization.
Results:
Between May and June 2020, 284 participants [median (interquartile ranges) age 39 (33 – 47) years, 56.3% men] responded to the survey; 33% were intensivists, and 9% were emergency medicine specialists. Half of the respondents worked in public hospitals. Noninvasive ventilation (89% versus 73%; p = 0.001) and highflow nasal cannula (49% versus 32%; p = 0.005) were reported to be more commonly available in private hospitals than in public hospitals. Mechanical ventilation was more commonly used in public hospitals than private hospitals (70% versus 50%; p = 0,024). In the Emergency Departments, positive endexpiratory pressure was most commonly adjusted according to SpO2, while in the intensive care units, positive end-expiratory pressure was adjusted according to the best lung compliance. In the Emergency Departments, 25% of the respondents did not know how to set positive end-expiratory pressure. Compared to private hospitals, public hospitals had a lower availability of protocols for personal protection equipment during tracheal intubation (82% versus 94%; p = 0.005), managing mechanical ventilation [64% versus 75%; p = 0.006] and weaning patients from mechanical ventilation [34% versus 54%; p = 0.002]. Finally, patients spent less time in the emergency department before being transferred to the intensive care unit in private hospitals than in public hospitals [2 (1 – 3) versus 5 (2 – 24) hours; p < 0.001].
Conclusion:
This survey revealed significant heterogeneity in the organization of hospital resources, clinical practices and treatments among physicians during the early COVID-19 pandemic in Brazil.
Keywords:BrazilCoronavirus infectionsCOVID-19Emergency servicehospitalHospital administrationIntensive care unitsPandemicsPhysiciansPractice patternsSurveys and questionnairesSee more - Pedro Paulo Zanella do Amaral Campos
-
Original Article
High-sensitivity troponin in the prognosis of patients hospitalized in intensive care for COVID-19: a Latin American longitudinal cohort study
- John Sprockel ,
- Anggie Murcia ,
- Juan Rincon ,
- Katherine Berrio ,
- Marisol Bejarano , [ … ],
- Jhon Parra
Abstract
Original ArticleHigh-sensitivity troponin in the prognosis of patients hospitalized in intensive care for COVID-19: a Latin American longitudinal cohort study
Rev Bras Ter Intensiva. 2022;34(1):124-130
DOI 10.5935/0103-507X.20220006-en
- John Sprockel ,
- Anggie Murcia ,
- Juan Rincon ,
- Katherine Berrio ,
- Marisol Bejarano ,
- Zulima Santofimio ,
- Hellen Cárdenas ,
- Diego Hernández ,
- Jhon Parra
Views1ABSTRACT
Objective:
The current study assessed the prevalence of troponin elevation and its capacity to predict 60day mortality in COVID-19 patients in intensive care.
Methods:
A longitudinal prospective single-center study was performed on a cohort of patients in intensive care due to a COVID-19 diagnosis confirmed using real-time test polymerase chain reaction from May to December 2020. A Receiver Operating Characteristic curve was constructed to predict death according to troponin level by calculating the area under the curve and its confidence intervals. A Cox proportional hazards model was generated to report the hazard ratios with confidence intervals of 95% and the p value for its association with 60day mortality.
Results:
A total of 296 patients were included with a 51% 60-day mortality rate. Troponin was positive in 39.9% (29.6% versus 49.7% in survivors and non-survivors, respectively). An area under the curve of 0.65 was found (95%CI: 0.59 – 0.71) to predict mortality. The Cox univariate model demonstrated a hazard ratio of 1.94 (95%CI: 1.41 – 2.67) and p < 0.001, but this relationship did not remain in the multivariate model, in which the hazard ratio was 1.387 (95%CI: 0.21 - 1.56) and the p value was 0.12.
Conclusion:
Troponin elevation is frequently found in patients in intensive care for COVID-19. Although its levels are higher in patients who die, no relationship was found in a multivariate model, which indicates that troponin should not be used as an only prognostic marker for mortality in this population.
Keywords:Coronavirus infectionsCOVID-19Critical careMortalityReverse transcriptase polymerase chain reactionTroponinSee moreViews1Abstract
Original ArticleHigh-sensitivity troponin in the prognosis of patients hospitalized in intensive care for COVID-19: a Latin American longitudinal cohort study
Rev Bras Ter Intensiva. 2022;34(1):124-130
DOI 10.5935/0103-507X.20220006-en
- John Sprockel ,
- Anggie Murcia ,
- Juan Rincon ,
- Katherine Berrio ,
- Marisol Bejarano ,
- Zulima Santofimio ,
- Hellen Cárdenas ,
- Diego Hernández ,
- Jhon Parra
Views1ABSTRACT
Objective:
The current study assessed the prevalence of troponin elevation and its capacity to predict 60day mortality in COVID-19 patients in intensive care.
Methods:
A longitudinal prospective single-center study was performed on a cohort of patients in intensive care due to a COVID-19 diagnosis confirmed using real-time test polymerase chain reaction from May to December 2020. A Receiver Operating Characteristic curve was constructed to predict death according to troponin level by calculating the area under the curve and its confidence intervals. A Cox proportional hazards model was generated to report the hazard ratios with confidence intervals of 95% and the p value for its association with 60day mortality.
Results:
A total of 296 patients were included with a 51% 60-day mortality rate. Troponin was positive in 39.9% (29.6% versus 49.7% in survivors and non-survivors, respectively). An area under the curve of 0.65 was found (95%CI: 0.59 – 0.71) to predict mortality. The Cox univariate model demonstrated a hazard ratio of 1.94 (95%CI: 1.41 – 2.67) and p < 0.001, but this relationship did not remain in the multivariate model, in which the hazard ratio was 1.387 (95%CI: 0.21 - 1.56) and the p value was 0.12.
Conclusion:
Troponin elevation is frequently found in patients in intensive care for COVID-19. Although its levels are higher in patients who die, no relationship was found in a multivariate model, which indicates that troponin should not be used as an only prognostic marker for mortality in this population.
Keywords:Coronavirus infectionsCOVID-19Critical careMortalityReverse transcriptase polymerase chain reactionTroponinSee more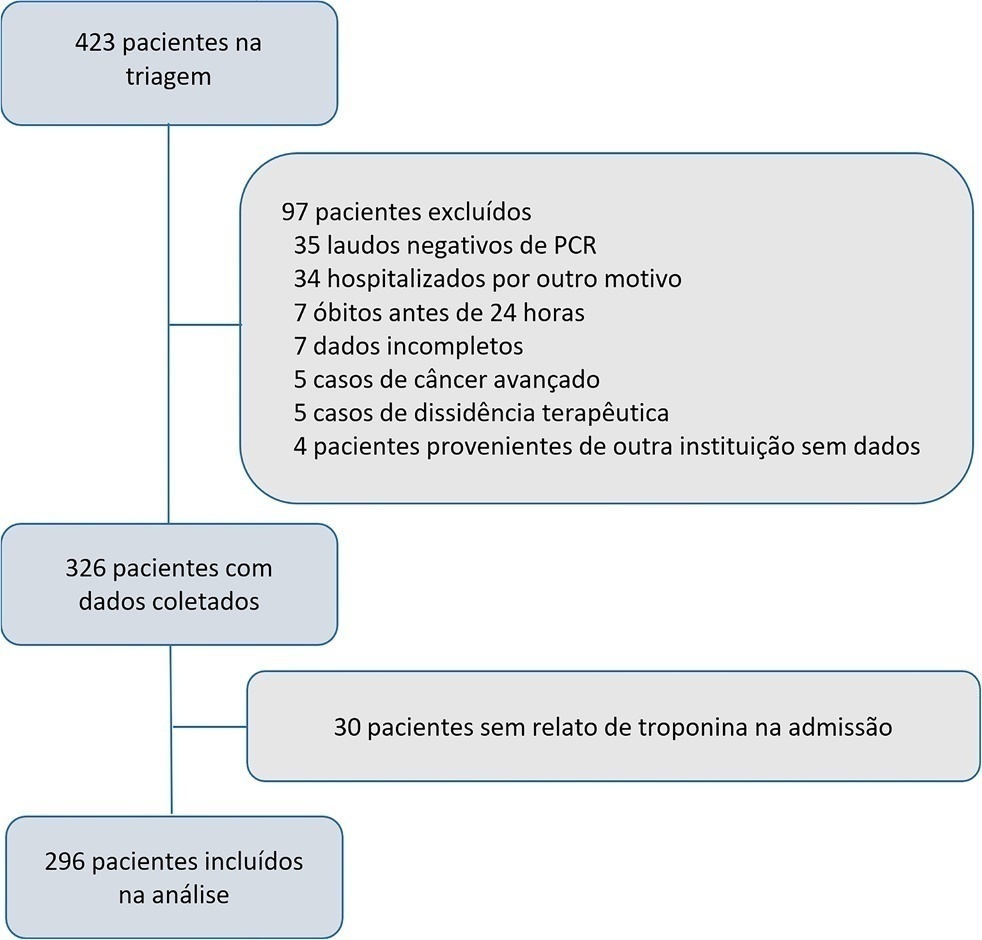
- John Sprockel
-
Original Article
Incidence of and risk factors for postintubation hypotension in critically ill patients with COVID-19
- Bişar Ergün ,
- Begüm Ergan ,
- Mehmet Nuri Yakar ,
- Murat Küçük ,
- Murat Özçelik , [ … ],
- Ali Necati Gökmen
Abstract
Original ArticleIncidence of and risk factors for postintubation hypotension in critically ill patients with COVID-19
Rev Bras Ter Intensiva. 2022;34(1):131-140
DOI 10.5935/0103-507X.20220007-en
- Bişar Ergün ,
- Begüm Ergan ,
- Mehmet Nuri Yakar ,
- Murat Küçük ,
- Murat Özçelik ,
- Erdem Yaka ,
- Ali Necati Gökmen
Views2ABSTRACT
Objective:
To evaluate the incidence of risk factors for postintubation hypotension in critically ill patients with COVID-19.
Methods:
We conducted a retrospective study of 141 patients with COVID-19 who were intubated in the intensive care unit. Postintubation hypotension was defined as the need for any vasopressor dose at any time within the 60 minutes following intubation. Patients with intubation-related cardiac arrest and hypotension before intubation were excluded from the study.
Results:
Of the 141 included patients, 53 patients (37.5%) had postintubation hypotension, and 43.6% of the patients (n = 17) were female. The median age of the postintubation hypotension group was 75.0 (interquartile range: 67.0 – 84.0). In the multivariate analysis, shock index ≥ 0.90 (OR = 7.76; 95%CI 3.14 – 19.21; p < 0.001), albumin levels < 2.92g/dL (OR = 3.65; 95%CI 1.49 - 8.96; p = 0.005), and procalcitonin levels (OR = 1.07, 95%CI 1.01 - 1.15; p = 0.045) were independent risk factors for postintubation hypotension. Hospital mortality was similar in patients with postintubation hypotension and patients without postintubation hypotension (92.5% versus 85.2%; p = 0.29).
Conclusion:
The incidence of postintubation hypotension was 37.5% in critically ill COVID-19 patients. A shock index ≥ 0.90 and albumin levels < 2.92g/dL were independently associated with postintubation hypotension. Furthermore, a shock index ≥ 0.90 may be a practical tool to predict the increased risk of postintubation hypotension in bedside scenarios before endotracheal intubation. In this study, postintubation hypotension was not associated with increased hospital mortality in COVID-19 patients.
Keywords:Coronavirus infectionsCOVID-19Critical illnessHospital mortalityHypotensionIntensive care unitsintratrachealIntubationrisk factorsSARS-CoV-2See moreViews2Abstract
Original ArticleIncidence of and risk factors for postintubation hypotension in critically ill patients with COVID-19
Rev Bras Ter Intensiva. 2022;34(1):131-140
DOI 10.5935/0103-507X.20220007-en
- Bişar Ergün ,
- Begüm Ergan ,
- Mehmet Nuri Yakar ,
- Murat Küçük ,
- Murat Özçelik ,
- Erdem Yaka ,
- Ali Necati Gökmen
Views2ABSTRACT
Objective:
To evaluate the incidence of risk factors for postintubation hypotension in critically ill patients with COVID-19.
Methods:
We conducted a retrospective study of 141 patients with COVID-19 who were intubated in the intensive care unit. Postintubation hypotension was defined as the need for any vasopressor dose at any time within the 60 minutes following intubation. Patients with intubation-related cardiac arrest and hypotension before intubation were excluded from the study.
Results:
Of the 141 included patients, 53 patients (37.5%) had postintubation hypotension, and 43.6% of the patients (n = 17) were female. The median age of the postintubation hypotension group was 75.0 (interquartile range: 67.0 – 84.0). In the multivariate analysis, shock index ≥ 0.90 (OR = 7.76; 95%CI 3.14 – 19.21; p < 0.001), albumin levels < 2.92g/dL (OR = 3.65; 95%CI 1.49 - 8.96; p = 0.005), and procalcitonin levels (OR = 1.07, 95%CI 1.01 - 1.15; p = 0.045) were independent risk factors for postintubation hypotension. Hospital mortality was similar in patients with postintubation hypotension and patients without postintubation hypotension (92.5% versus 85.2%; p = 0.29).
Conclusion:
The incidence of postintubation hypotension was 37.5% in critically ill COVID-19 patients. A shock index ≥ 0.90 and albumin levels < 2.92g/dL were independently associated with postintubation hypotension. Furthermore, a shock index ≥ 0.90 may be a practical tool to predict the increased risk of postintubation hypotension in bedside scenarios before endotracheal intubation. In this study, postintubation hypotension was not associated with increased hospital mortality in COVID-19 patients.
Keywords:Coronavirus infectionsCOVID-19Critical illnessHospital mortalityHypotensionIntensive care unitsintratrachealIntubationrisk factorsSARS-CoV-2See more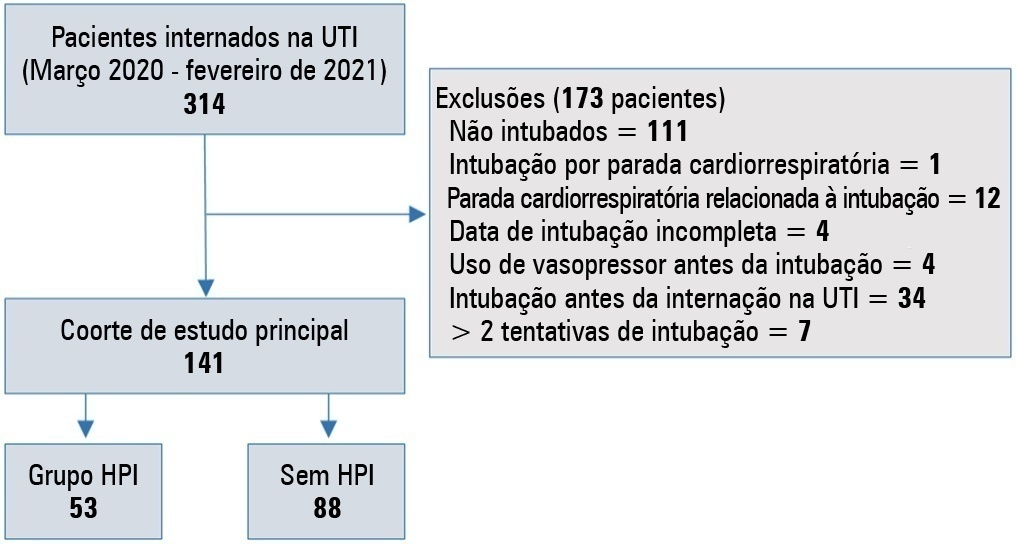
- Bişar Ergün
-
Original Article
The impact of severe COVID-19 on health-related quality of life and disability: an early follow-up perspective
- Liliana Cristina da Silva Ferreira Fontes ,
- Paulo Jorge Ribeiro Costa ,
- Joana Carolina João Fernandes ,
- Tatiana Santos Vieira ,
- Nuno Cruz Reis , [ … ],
- José Artur Osório Carvalho Paiva
Abstract
Original ArticleThe impact of severe COVID-19 on health-related quality of life and disability: an early follow-up perspective
Rev Bras Ter Intensiva. 2022;34(1):141-146
DOI 10.5935/0103-507X.20220008-en
- Liliana Cristina da Silva Ferreira Fontes ,
- Paulo Jorge Ribeiro Costa ,
- Joana Carolina João Fernandes ,
- Tatiana Santos Vieira ,
- Nuno Cruz Reis ,
- Isabel Maria Metelo Coimbra ,
- José Artur Osório Carvalho Paiva
Views1ABSTRACT
Objective:
To assess early postdischarge health-related quality of life and disability of all survivors of critical COVID-19 admitted for more than 24 hours to na intensive care unit..
Methods:
Study carried out at the Intensive Care Medicine Department of Centro Hospitalar Universitário São João from 8th October 2020 to 16th February 2021. Approximately 1 month after hospital discharge, an intensive care-trained nurse performed a telephone consultation with 99 survivors already at home applying the EuroQol Five-Dimensional Five-Level questionnaire and the 12-item World Health Organization Disability Assessment Schedule 2.0.
Results:
The mean age of the population studied was 63 ± 12 years, and 32.5% were submitted to invasive mechanical ventilation. Their mean Simplified Acute Physiologic Score was 35 ± 14, and the Charlson Comorbidity Index was 3 ± 2. Intensive care medicine and hospital lengths of stay were 13 ± 22 and 22 ± 25 days, respectively. The mean EuroQol Visual Analog Scale was 65% (± 21), and only 35.3% had no or slight problems performing their usual activities, most having some degree of pain/discomfort and anxiety/depression. The 12-item World Health Organization Disability Assessment Schedule 2.0 showed marked impairments in terms of reassuring usual work or community activities and mobility. The use of both tools suggested that their health status was worse than their perception of it.
Conclusion:
This early identification of sequelae may help define flows and priorities for rehabilitation and reinsertion after critical COVID-19.
Keywords:BetacoronavirusCoronavirus infectionsCOVID-19Critical careDisability evaluationPatient dischargeQuality of lifeRehabilitationSARS-CoV-2See moreViews1Abstract
Original ArticleThe impact of severe COVID-19 on health-related quality of life and disability: an early follow-up perspective
Rev Bras Ter Intensiva. 2022;34(1):141-146
DOI 10.5935/0103-507X.20220008-en
- Liliana Cristina da Silva Ferreira Fontes ,
- Paulo Jorge Ribeiro Costa ,
- Joana Carolina João Fernandes ,
- Tatiana Santos Vieira ,
- Nuno Cruz Reis ,
- Isabel Maria Metelo Coimbra ,
- José Artur Osório Carvalho Paiva
Views1ABSTRACT
Objective:
To assess early postdischarge health-related quality of life and disability of all survivors of critical COVID-19 admitted for more than 24 hours to na intensive care unit..
Methods:
Study carried out at the Intensive Care Medicine Department of Centro Hospitalar Universitário São João from 8th October 2020 to 16th February 2021. Approximately 1 month after hospital discharge, an intensive care-trained nurse performed a telephone consultation with 99 survivors already at home applying the EuroQol Five-Dimensional Five-Level questionnaire and the 12-item World Health Organization Disability Assessment Schedule 2.0.
Results:
The mean age of the population studied was 63 ± 12 years, and 32.5% were submitted to invasive mechanical ventilation. Their mean Simplified Acute Physiologic Score was 35 ± 14, and the Charlson Comorbidity Index was 3 ± 2. Intensive care medicine and hospital lengths of stay were 13 ± 22 and 22 ± 25 days, respectively. The mean EuroQol Visual Analog Scale was 65% (± 21), and only 35.3% had no or slight problems performing their usual activities, most having some degree of pain/discomfort and anxiety/depression. The 12-item World Health Organization Disability Assessment Schedule 2.0 showed marked impairments in terms of reassuring usual work or community activities and mobility. The use of both tools suggested that their health status was worse than their perception of it.
Conclusion:
This early identification of sequelae may help define flows and priorities for rehabilitation and reinsertion after critical COVID-19.
Keywords:BetacoronavirusCoronavirus infectionsCOVID-19Critical careDisability evaluationPatient dischargeQuality of lifeRehabilitationSARS-CoV-2See more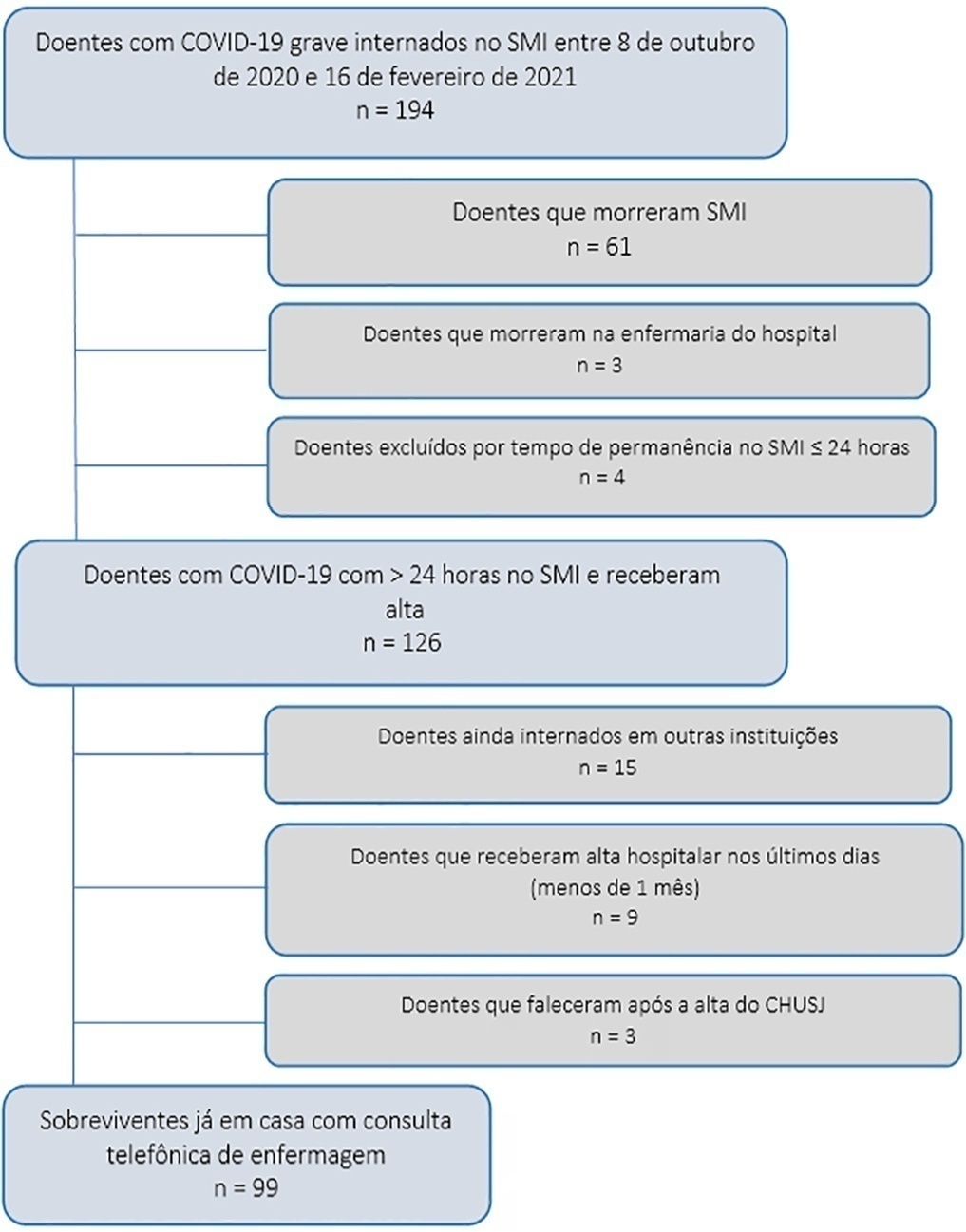
- Liliana Cristina da Silva Ferreira Fontes
-
Original Article
Vancomycin area under the curve-guided monitoring in pediatric patients
- Ronaldo Morales Junior ,
- Vanessa D’Amaro Juodinis ,
- Isabela Cristina Pinheiro de Freitas Santos ,
- Camila Canuto Campioni ,
- Flávia Gatto de Almeida Wirth , [ … ],
- Silvia Regina Cavani Jorge Santos
Abstract
Original ArticleVancomycin area under the curve-guided monitoring in pediatric patients
Rev Bras Ter Intensiva. 2022;34(1):147-153
DOI 10.5935/0103-507X.20220009-en
- Ronaldo Morales Junior ,
- Vanessa D’Amaro Juodinis ,
- Isabela Cristina Pinheiro de Freitas Santos ,
- Camila Canuto Campioni ,
- Flávia Gatto de Almeida Wirth ,
- Livia Maria Goncalves Barbosa ,
- Daniela Carla de Souza ,
- Silvia Regina Cavani Jorge Santos
Views1See moreABSTRACT
Objective:
To assess the percentage of vancomycin area under the curve/minimum inhibitory concentration target attainment in pediatric patients after the empirical dose regimen and to demonstrate the applicability of this method for vancomycin monitoring.
Methods:
A retrospective cohort study was performed including pediatric patients with normal renal function admitted between January 2020 and December 2020. The one-compartment model with first-order kinetics was used to estimate the pharmacokinetic parameters, and the area under the curve was calculated by the trapezoidal rule. The therapeutic target was defined as area under the curve/minimum inhibitory concentration ≥ 400 and < 600. The Chi-squared test was applied to compare the percentage of target attainment over age groups, while the pharmacokinetic parameters were compared by the Kruskal-Wallis test with Dunn’s test for post hoc analyses. We considered significant p-values < 0.05.
Results:
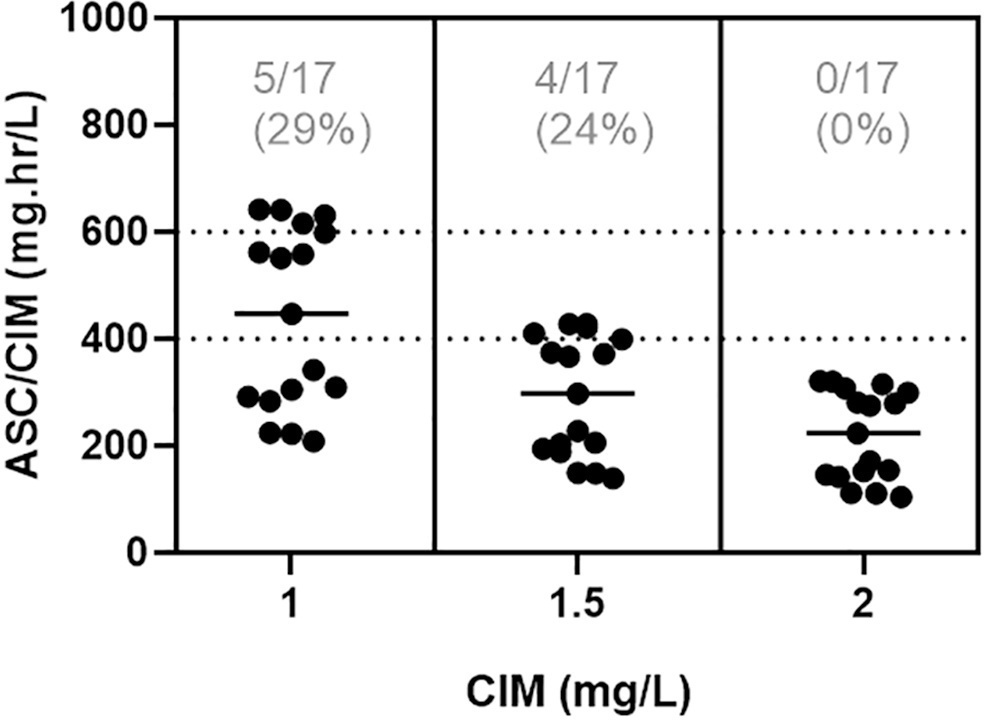
In total, 42 pairs of vancomycin levels were analyzed from 17 patients enrolled in this study. After empirical vancomycin daily dosing, the therapeutic target was achieved in five (29%) patients; four patients (24%) had a supratherapeutic initial area under the curve/minimum inhibitory concentration value (> 600mg.h/L), and eight (47%) patients had subtherapeutic values (< 400mg.h/L). The most identified pathogens were Staphylococcus spp. (n = 7). Trough levels and areas under the curve showed moderate correlation values (R2 = 0.73). Acute kidney injury occurred in one (6%) patient.
Conclusion:
Most patients did not reach the therapeutic target with a vancomycin empirical dose regimen, and the implementation of area under the curve-based dosing using two sample measurements allowed for real-time dose adjustments based on individuals’ pharmacokinetic parameters.
Views1Abstract
Original ArticleVancomycin area under the curve-guided monitoring in pediatric patients
Rev Bras Ter Intensiva. 2022;34(1):147-153
DOI 10.5935/0103-507X.20220009-en
- Ronaldo Morales Junior ,
- Vanessa D’Amaro Juodinis ,
- Isabela Cristina Pinheiro de Freitas Santos ,
- Camila Canuto Campioni ,
- Flávia Gatto de Almeida Wirth ,
- Livia Maria Goncalves Barbosa ,
- Daniela Carla de Souza ,
- Silvia Regina Cavani Jorge Santos
Views1See moreABSTRACT
Objective:
To assess the percentage of vancomycin area under the curve/minimum inhibitory concentration target attainment in pediatric patients after the empirical dose regimen and to demonstrate the applicability of this method for vancomycin monitoring.
Methods:
A retrospective cohort study was performed including pediatric patients with normal renal function admitted between January 2020 and December 2020. The one-compartment model with first-order kinetics was used to estimate the pharmacokinetic parameters, and the area under the curve was calculated by the trapezoidal rule. The therapeutic target was defined as area under the curve/minimum inhibitory concentration ≥ 400 and < 600. The Chi-squared test was applied to compare the percentage of target attainment over age groups, while the pharmacokinetic parameters were compared by the Kruskal-Wallis test with Dunn’s test for post hoc analyses. We considered significant p-values < 0.05.
Results:
In total, 42 pairs of vancomycin levels were analyzed from 17 patients enrolled in this study. After empirical vancomycin daily dosing, the therapeutic target was achieved in five (29%) patients; four patients (24%) had a supratherapeutic initial area under the curve/minimum inhibitory concentration value (> 600mg.h/L), and eight (47%) patients had subtherapeutic values (< 400mg.h/L). The most identified pathogens were Staphylococcus spp. (n = 7). Trough levels and areas under the curve showed moderate correlation values (R2 = 0.73). Acute kidney injury occurred in one (6%) patient.
Conclusion:
Most patients did not reach the therapeutic target with a vancomycin empirical dose regimen, and the implementation of area under the curve-based dosing using two sample measurements allowed for real-time dose adjustments based on individuals’ pharmacokinetic parameters.
- Ronaldo Morales Junior
-
Original Article
Prognostic value of hyperlactatemia in infected patients admitted to intensive care units: a multicenter study
- Catarina Mendes Silva ,
- João Pedro Baptista ,
- Paulo Mergulhão ,
- Filipe Froes ,
- João Gonçalves-Pereira , [ … ],
- José Artur Paiva
Abstract
Original ArticlePrognostic value of hyperlactatemia in infected patients admitted to intensive care units: a multicenter study
Rev Bras Ter Intensiva. 2022;34(1):154-162
DOI 10.5935/0103-507X.20220010-en
- Catarina Mendes Silva ,
- João Pedro Baptista ,
- Paulo Mergulhão ,
- Filipe Froes ,
- João Gonçalves-Pereira ,
- José Manuel Pereira,
- Claudia Camila Dias ,
- José Artur Paiva
Views1See moreABSTRACT
Objective:
To evaluate the influence of patient characteristics on hyperlactatemia in an infected population admitted to intensive care units and the influence of hyperlactatemia severity on hospital mortality.
Methods:
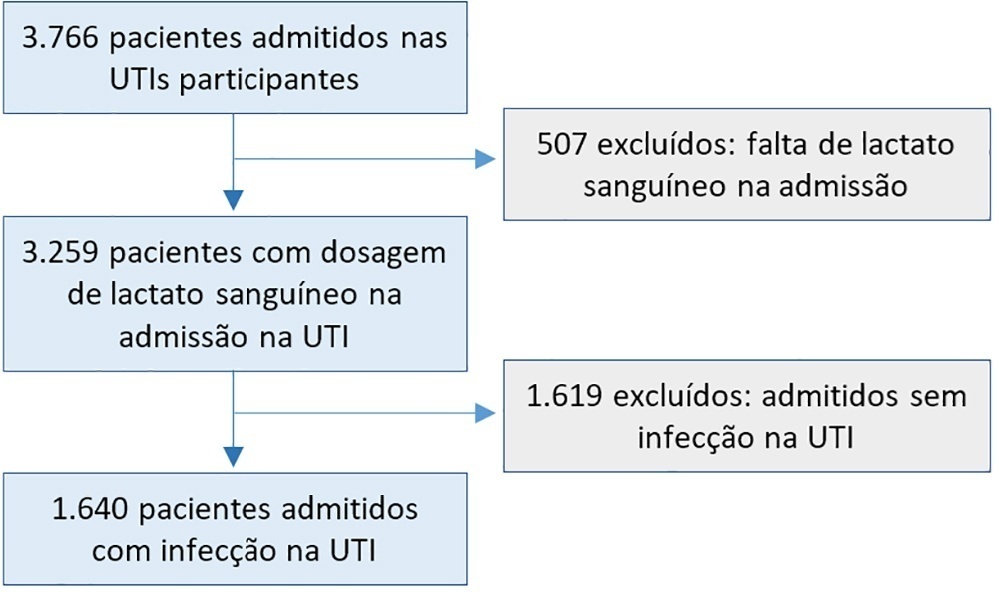
A post hoc analysis of hyperlactatemia in the INFAUCI study, a national prospective, observational, multicenter study, was conducted in 14 Portuguese intensive care units. Infected patients admitted to intensive care units with a lactate measurement in the first 12 hours of admission were selected. Sepsis was identified according to the Sepsis-2 definition accepted at the time of data collection. The severity of hyperlactatemia was classified as mild (2 – 3.9mmol/L), moderate (4.0 – 9.9mmol/L) or severe (> 10mmol/L).
Results:
In a total of 1,640 patients infected on admission, hyperlactatemia occurred in 934 patients (57%), classified as mild, moderate and severe in 57.0%, 34.4% and 8.7% of patients, respectively. The presence of hyperlactatemia and a higher degree of hyperlactatemia were both associated with a higher Simplified Acute Physiology Score II, a higher Charlson Comorbidity Index and the presence of septic shock. The lactate Receiver Operating Characteristic curve for hospital mortality had an area under the curve of 0.64 (95%CI 0.61 – 0.72), which increased to 0.71 (95%CI 0.68 – 0.74) when combined with Sequential Organ Failure Assessment score. In-hospital mortality with other covariates adjusted by Simplified Acute Physiology Score II was associated with moderate and severe hyperlactatemia, with odds ratio of 1.95 (95%CI 1.4 – 2.7; p < 0.001) and 4.54 (95%CI 2.4 - 8.5; p < 0.001), respectively.
Conclusion:
Blood lactate levels correlate independently with in-hospital mortality for moderate and severe degrees of hyperlactatemia.
Views1Abstract
Original ArticlePrognostic value of hyperlactatemia in infected patients admitted to intensive care units: a multicenter study
Rev Bras Ter Intensiva. 2022;34(1):154-162
DOI 10.5935/0103-507X.20220010-en
- Catarina Mendes Silva ,
- João Pedro Baptista ,
- Paulo Mergulhão ,
- Filipe Froes ,
- João Gonçalves-Pereira ,
- José Manuel Pereira,
- Claudia Camila Dias ,
- José Artur Paiva
Views1See moreABSTRACT
Objective:
To evaluate the influence of patient characteristics on hyperlactatemia in an infected population admitted to intensive care units and the influence of hyperlactatemia severity on hospital mortality.
Methods:
A post hoc analysis of hyperlactatemia in the INFAUCI study, a national prospective, observational, multicenter study, was conducted in 14 Portuguese intensive care units. Infected patients admitted to intensive care units with a lactate measurement in the first 12 hours of admission were selected. Sepsis was identified according to the Sepsis-2 definition accepted at the time of data collection. The severity of hyperlactatemia was classified as mild (2 – 3.9mmol/L), moderate (4.0 – 9.9mmol/L) or severe (> 10mmol/L).
Results:
In a total of 1,640 patients infected on admission, hyperlactatemia occurred in 934 patients (57%), classified as mild, moderate and severe in 57.0%, 34.4% and 8.7% of patients, respectively. The presence of hyperlactatemia and a higher degree of hyperlactatemia were both associated with a higher Simplified Acute Physiology Score II, a higher Charlson Comorbidity Index and the presence of septic shock. The lactate Receiver Operating Characteristic curve for hospital mortality had an area under the curve of 0.64 (95%CI 0.61 – 0.72), which increased to 0.71 (95%CI 0.68 – 0.74) when combined with Sequential Organ Failure Assessment score. In-hospital mortality with other covariates adjusted by Simplified Acute Physiology Score II was associated with moderate and severe hyperlactatemia, with odds ratio of 1.95 (95%CI 1.4 – 2.7; p < 0.001) and 4.54 (95%CI 2.4 - 8.5; p < 0.001), respectively.
Conclusion:
Blood lactate levels correlate independently with in-hospital mortality for moderate and severe degrees of hyperlactatemia.
- Catarina Mendes Silva
-
Original Article
Reduced physical functional performance before hospitalization predicts life support limitations and mortality in nonsurgical intensive care unit patients
- Jamile Caroline Garbuglio Araujo da Silva ,
- Tiago Giraldi ,
- Carolina Matida Gontijo Coutinho ,
- Marco Antonio Carvalho Filho ,
- Dario Cecílio Fernandes , [ … ],
- Thiago Martins Santos
Abstract
Original ArticleReduced physical functional performance before hospitalization predicts life support limitations and mortality in nonsurgical intensive care unit patients
Rev Bras Ter Intensiva. 2022;34(1):166-175
DOI 10.5935/0103-507X.20220011-en
- Jamile Caroline Garbuglio Araujo da Silva ,
- Tiago Giraldi ,
- Carolina Matida Gontijo Coutinho ,
- Marco Antonio Carvalho Filho ,
- Dario Cecílio Fernandes ,
- Thiago Martins Santos
Views2ABSTRACT
Objective:
To assess whether scales of physical functional performance and the surprise question (“Would I be surprised if this patient died in 6 months?”) predict life support limitations and mortality in critically ill nonsurgical patients.
Methods:
We included 114 patients admitted from the Emergency Department to an intensive care unit in this prospective cohort. Physical functional performance was assessed by the Palliative Prognostic Score, Karnofsky Performance Status, and the Katz Activities of Daily Living scale. Two intensivists responded to the surprise question.
Results:
The proposed physical functional performance scores were significantly lower in patients with life support limitations and those who died during the hospital stay. A negative response to the surprise question was more frequent in the same subset of patients. Adjusted univariable analysis showed an increased odds ratio for life support limitations and death regarding the activities of daily living scale (1.35 [1.01 – 1.78] and 1.34 [1.0 – 1.79], respectively) and a negative response for the surprise question (42.35 [11.62 – 154.43] and 47.79 [11.41 – 200.25], respectively); with a p < 0.05 for all results.
Conclusion:
All physical functional performance scales showed lower scores in nonsurvivors and patients with life support limitations. The activities of daily living score and the surprise question increased the odds of life support limitations and mortality in our cohort of nonsurgical intensive care unit patients admitted from the Emergency Department.
Keywords:Activities of daily livingIntensive care unitsKarnofsky Performance StatusPalliative CarePhysical functional performanceSee moreViews2Abstract
Original ArticleReduced physical functional performance before hospitalization predicts life support limitations and mortality in nonsurgical intensive care unit patients
Rev Bras Ter Intensiva. 2022;34(1):166-175
DOI 10.5935/0103-507X.20220011-en
- Jamile Caroline Garbuglio Araujo da Silva ,
- Tiago Giraldi ,
- Carolina Matida Gontijo Coutinho ,
- Marco Antonio Carvalho Filho ,
- Dario Cecílio Fernandes ,
- Thiago Martins Santos
Views2ABSTRACT
Objective:
To assess whether scales of physical functional performance and the surprise question (“Would I be surprised if this patient died in 6 months?”) predict life support limitations and mortality in critically ill nonsurgical patients.
Methods:
We included 114 patients admitted from the Emergency Department to an intensive care unit in this prospective cohort. Physical functional performance was assessed by the Palliative Prognostic Score, Karnofsky Performance Status, and the Katz Activities of Daily Living scale. Two intensivists responded to the surprise question.
Results:
The proposed physical functional performance scores were significantly lower in patients with life support limitations and those who died during the hospital stay. A negative response to the surprise question was more frequent in the same subset of patients. Adjusted univariable analysis showed an increased odds ratio for life support limitations and death regarding the activities of daily living scale (1.35 [1.01 – 1.78] and 1.34 [1.0 – 1.79], respectively) and a negative response for the surprise question (42.35 [11.62 – 154.43] and 47.79 [11.41 – 200.25], respectively); with a p < 0.05 for all results.
Conclusion:
All physical functional performance scales showed lower scores in nonsurvivors and patients with life support limitations. The activities of daily living score and the surprise question increased the odds of life support limitations and mortality in our cohort of nonsurgical intensive care unit patients admitted from the Emergency Department.
Keywords:Activities of daily livingIntensive care unitsKarnofsky Performance StatusPalliative CarePhysical functional performanceSee more - Jamile Caroline Garbuglio Araujo da Silva
-
Review Article
A deep look into the rib cage compression technique in mechanically ventilated patients: a narrative review
Rev Bras Ter Intensiva. 2022;34(1):176-184
Abstract
Review ArticleA deep look into the rib cage compression technique in mechanically ventilated patients: a narrative review
Rev Bras Ter Intensiva. 2022;34(1):176-184
DOI 10.5935/0103-507X.20220012-en
Views3ABSTRACT
Defective management of secretions is one of the most frequent complications in invasive mechanically ventilated patients. Clearance of secretions through chest physiotherapy is a critical aspect of the treatment of these patients. Manual rib cage compression is one of the most practiced chest physiotherapy techniques in ventilated patients; however, its impact on clinical outcomes remains controversial due to methodological issues and poor understanding of its action. In this review, we present a detailed analysis of the physical principles involved in rib cage compression technique performance, as well as the physiological effects observed in experimental and clinical studies, which show that the use of brief and vigorous rib cage compression, based on increased expiratory flows (expiratory-inspiratory airflow difference of > 33L/minute), can improve mucus movement toward the glottis. On the other hand, the use of soft and gradual rib cage compression throughout the whole expiratory phase does not impact the expiratory flows, resulting in ineffective or undesired effects in some cases. More physiological studies are needed to understand the principles of the rib cage compression technique in ventilated humans. However, according to the evidence, rib cage compression has more potential benefits than risks, so its implementation should be promoted.
Keywords:artificialCritical careMucociliary clearancePhysical therapy modalitiesPressureRespirationRespiratory therapyRib cageSee moreViews3Abstract
Review ArticleA deep look into the rib cage compression technique in mechanically ventilated patients: a narrative review
Rev Bras Ter Intensiva. 2022;34(1):176-184
DOI 10.5935/0103-507X.20220012-en
Views3ABSTRACT
Defective management of secretions is one of the most frequent complications in invasive mechanically ventilated patients. Clearance of secretions through chest physiotherapy is a critical aspect of the treatment of these patients. Manual rib cage compression is one of the most practiced chest physiotherapy techniques in ventilated patients; however, its impact on clinical outcomes remains controversial due to methodological issues and poor understanding of its action. In this review, we present a detailed analysis of the physical principles involved in rib cage compression technique performance, as well as the physiological effects observed in experimental and clinical studies, which show that the use of brief and vigorous rib cage compression, based on increased expiratory flows (expiratory-inspiratory airflow difference of > 33L/minute), can improve mucus movement toward the glottis. On the other hand, the use of soft and gradual rib cage compression throughout the whole expiratory phase does not impact the expiratory flows, resulting in ineffective or undesired effects in some cases. More physiological studies are needed to understand the principles of the rib cage compression technique in ventilated humans. However, according to the evidence, rib cage compression has more potential benefits than risks, so its implementation should be promoted.
Keywords:artificialCritical careMucociliary clearancePhysical therapy modalitiesPressureRespirationRespiratory therapyRib cageSee more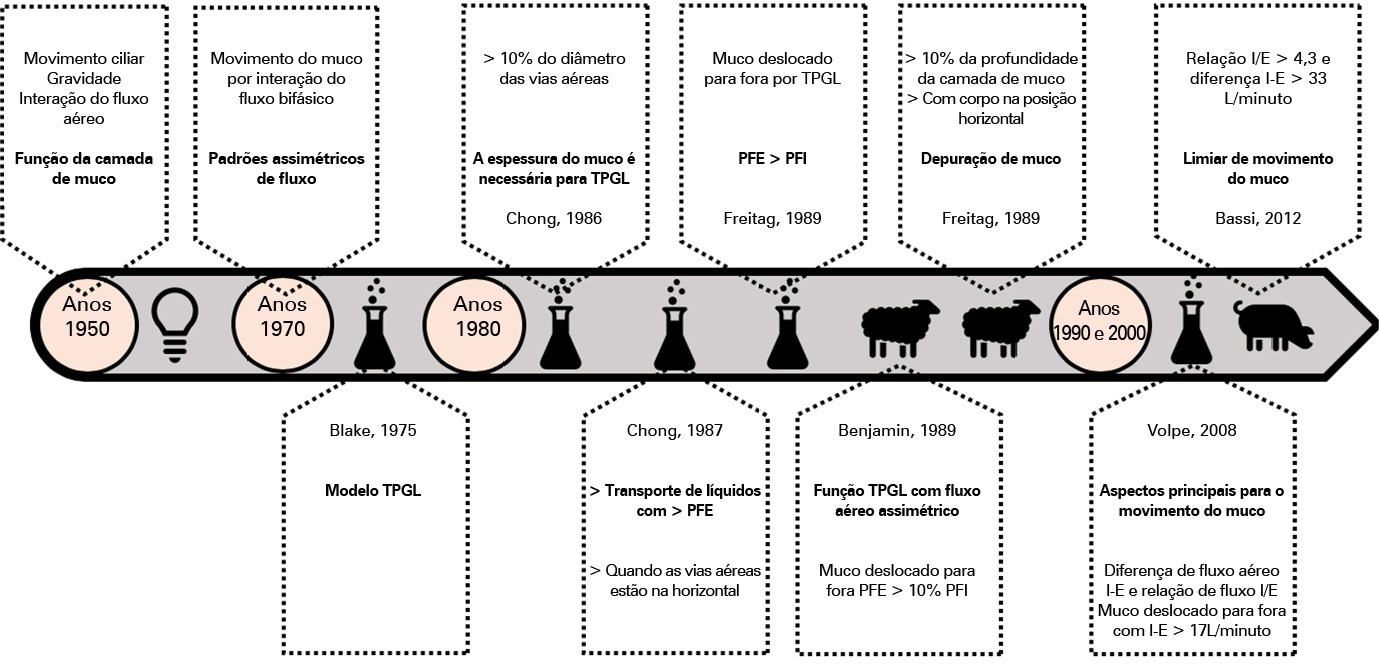
-
Review Article
Rationale and limitations of the SpO2/FiO2 as a possible substitute for PaO2/FiO2 in different preclinical and clinical scenarios
- Eduardo Butturini de Carvalho ,
- Thiago Ravache Sobreira Leite ,
- Raquel Ferreira de Magalhães Sacramento ,
- Paulo Roberto Loureiro do Nascimento ,
- Cynthia dos Santos Samary , [ … ],
- Pedro Leme Silva
Abstract
Review ArticleRationale and limitations of the SpO2/FiO2 as a possible substitute for PaO2/FiO2 in different preclinical and clinical scenarios
Rev Bras Ter Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
- Eduardo Butturini de Carvalho ,
- Thiago Ravache Sobreira Leite ,
- Raquel Ferreira de Magalhães Sacramento ,
- Paulo Roberto Loureiro do Nascimento ,
- Cynthia dos Santos Samary ,
- Patrícia Rieken Macedo Rocco ,
- Pedro Leme Silva
Views3ABSTRACT
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Keywords:Adultblood gas analysisCOVID-19InfantInfant, newbornOximetryOxygenOxygen saturationPrognosisRespiratory distress syndromeRespiratory insufficiencySARS-CoV-2See moreViews3Abstract
Review ArticleRationale and limitations of the SpO2/FiO2 as a possible substitute for PaO2/FiO2 in different preclinical and clinical scenarios
Rev Bras Ter Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
- Eduardo Butturini de Carvalho ,
- Thiago Ravache Sobreira Leite ,
- Raquel Ferreira de Magalhães Sacramento ,
- Paulo Roberto Loureiro do Nascimento ,
- Cynthia dos Santos Samary ,
- Patrícia Rieken Macedo Rocco ,
- Pedro Leme Silva
Views3ABSTRACT
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Keywords:Adultblood gas analysisCOVID-19InfantInfant, newbornOximetryOxygenOxygen saturationPrognosisRespiratory distress syndromeRespiratory insufficiencySARS-CoV-2See more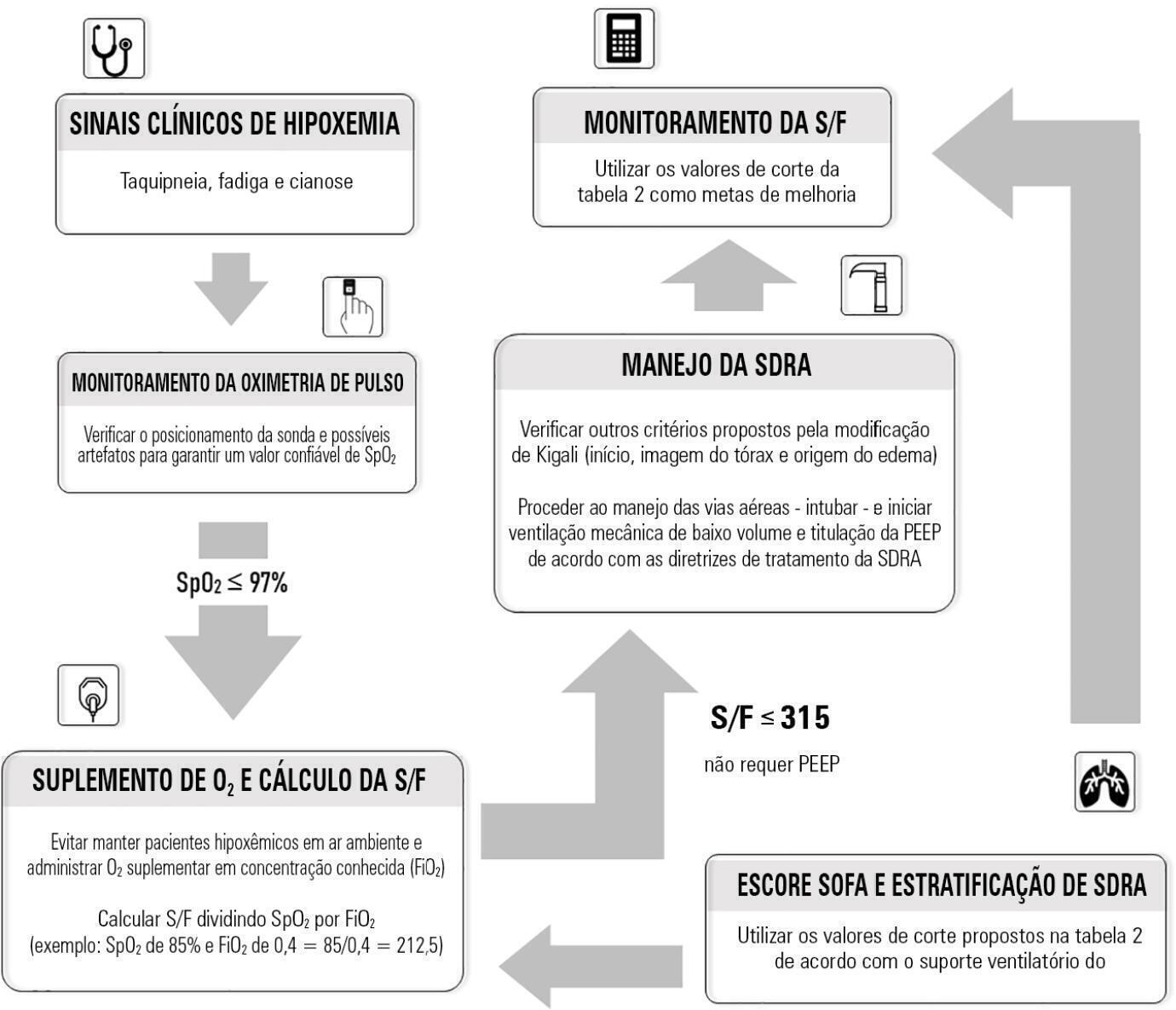
- Eduardo Butturini de Carvalho
-
Case Report
Valproate-associated hyperammonemic encephalopathy in subarachnoid hemorrhage: a diagnosis to consider
- Vivian Fuellis ,
- Pedro Grille ,
- Federico Verga ,
- Luis Urbán Alfaro ,
- Lucciano Grasiuso , [ … ],
- Marcelo Barbato
Abstract
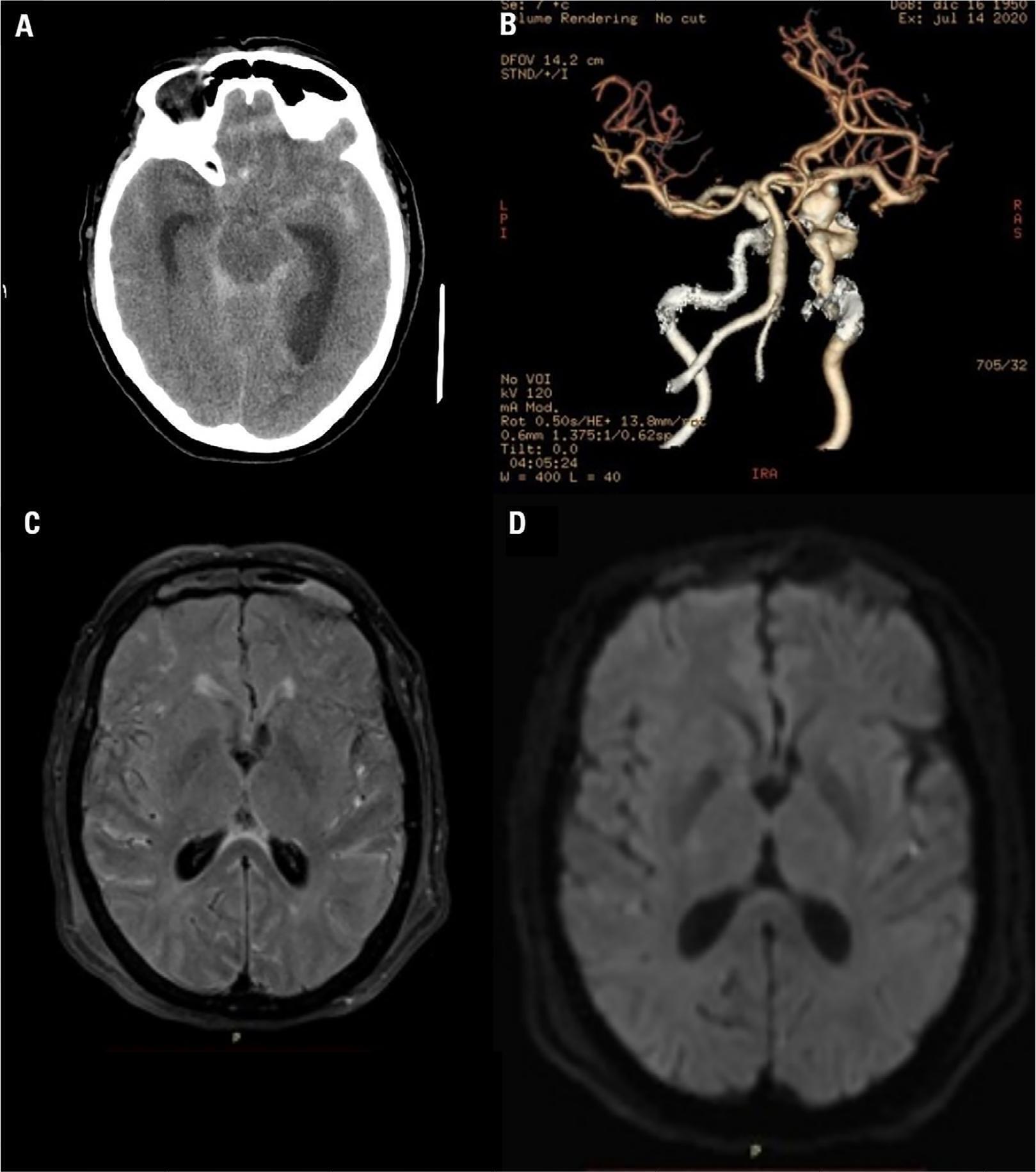
Case ReportValproate-associated hyperammonemic encephalopathy in subarachnoid hemorrhage: a diagnosis to consider
Rev Bras Ter Intensiva. 2022;34(1):197-201
Views2Abstract
Case ReportValproate-associated hyperammonemic encephalopathy in subarachnoid hemorrhage: a diagnosis to consider
Rev Bras Ter Intensiva. 2022;34(1):197-201
- Vivian Fuellis
-
Letter to the Editor
Endotracheal intubation in COVID-19 patients in Brazil: a nationwide survey
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fábio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Abstract
Letter to the EditorEndotracheal intubation in COVID-19 patients in Brazil: a nationwide survey
Rev Bras Ter Intensiva. 2022;34(1):202-204
DOI 10.5935/0103-507X.20220015-en
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fábio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Views2To the Editor Endotracheal intubation is a life-saving procedure in acute respiratory distress syndrome. However, complications such as hypoxia, hypotension and cardiovascular collapse may occur in almost 40% of the procedures in the intensive care unit (ICU).() Evidence regarding the best practice of endotracheal intubation in this context is scarce, and most data have been […]See moreViews2Abstract
Letter to the EditorEndotracheal intubation in COVID-19 patients in Brazil: a nationwide survey
Rev Bras Ter Intensiva. 2022;34(1):202-204
DOI 10.5935/0103-507X.20220015-en
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fábio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Views2To the Editor Endotracheal intubation is a life-saving procedure in acute respiratory distress syndrome. However, complications such as hypoxia, hypotension and cardiovascular collapse may occur in almost 40% of the procedures in the intensive care unit (ICU).() Evidence regarding the best practice of endotracheal intubation in this context is scarce, and most data have been […]See more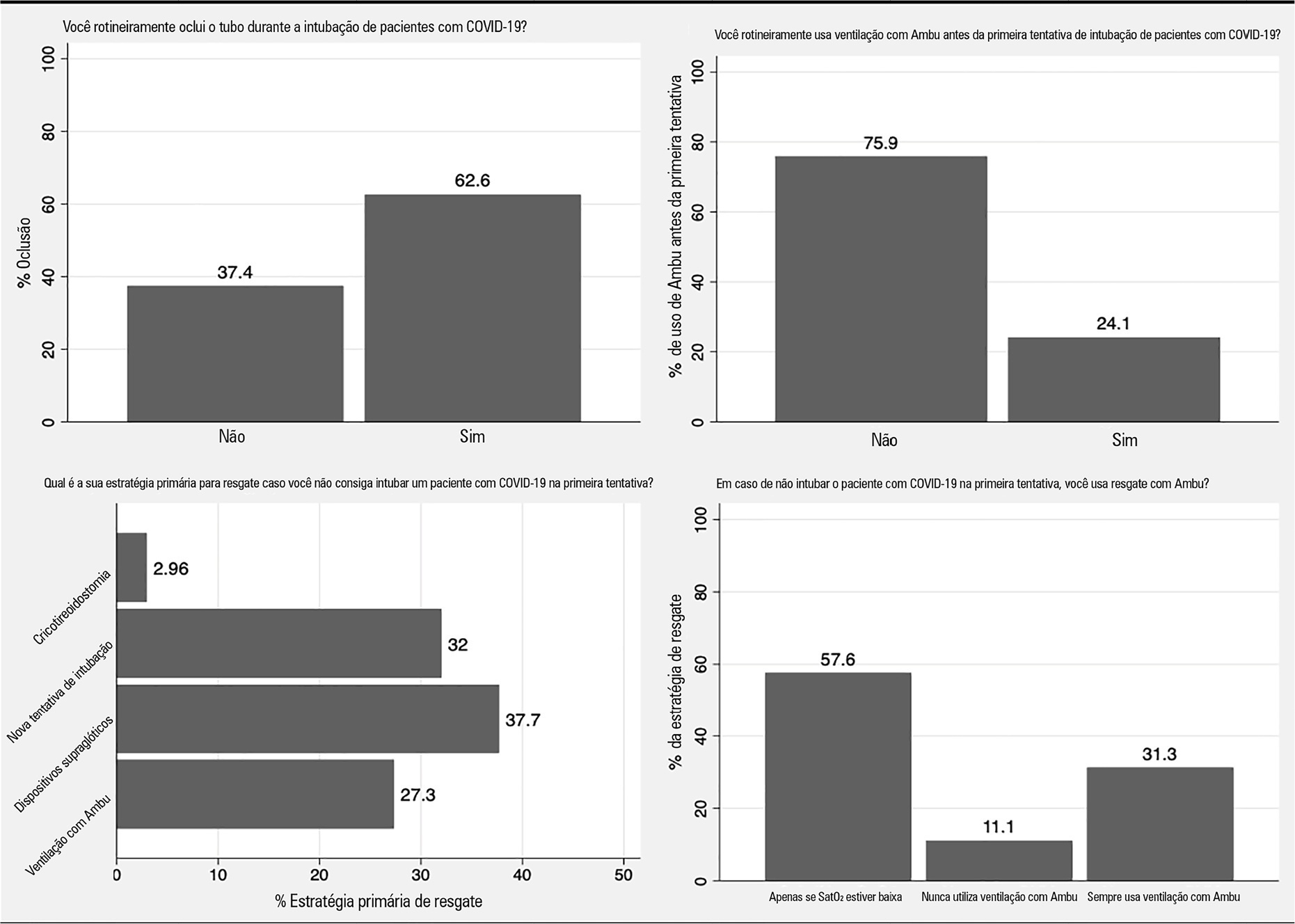
- Pedro Vitale Mendes
Volume Articles - Critical Care Science (CCS)
