-
Commentary
What every intensivist should know about light sedation for mechanically ventilated patients
Rev Bras Ter Intensiva. 2021;33(4):480-482
Abstract
CommentaryWhat every intensivist should know about light sedation for mechanically ventilated patients
Rev Bras Ter Intensiva. 2021;33(4):480-482
DOI 10.5935/0103-507X.20210069
Views3INTRODUCTION Pain, agitation and anxiety are frequently experienced by patients requiring intensive care unit (ICU) admission. These events are often associated with tracheal intubation, mechanical ventilation (MV) and bedside procedures. Sedatives and analgesics can be used to minimize distress, ensure comfort, and decrease the work of breathing to achieve better synchrony with the ventilator. A […]See moreViews3

Abstract
CommentaryWhat every intensivist should know about light sedation for mechanically ventilated patients
Rev Bras Ter Intensiva. 2021;33(4):480-482
DOI 10.5935/0103-507X.20210069
Views3INTRODUCTIONPain, agitation and anxiety are frequently experienced by patients requiring intensive care unit (ICU) admission. These events are often associated with tracheal intubation, mechanical ventilation (MV) and bedside procedures. Sedatives and analgesics can be used to minimize distress, ensure comfort, and decrease the work of breathing to achieve better synchrony with the ventilator. A number […]See more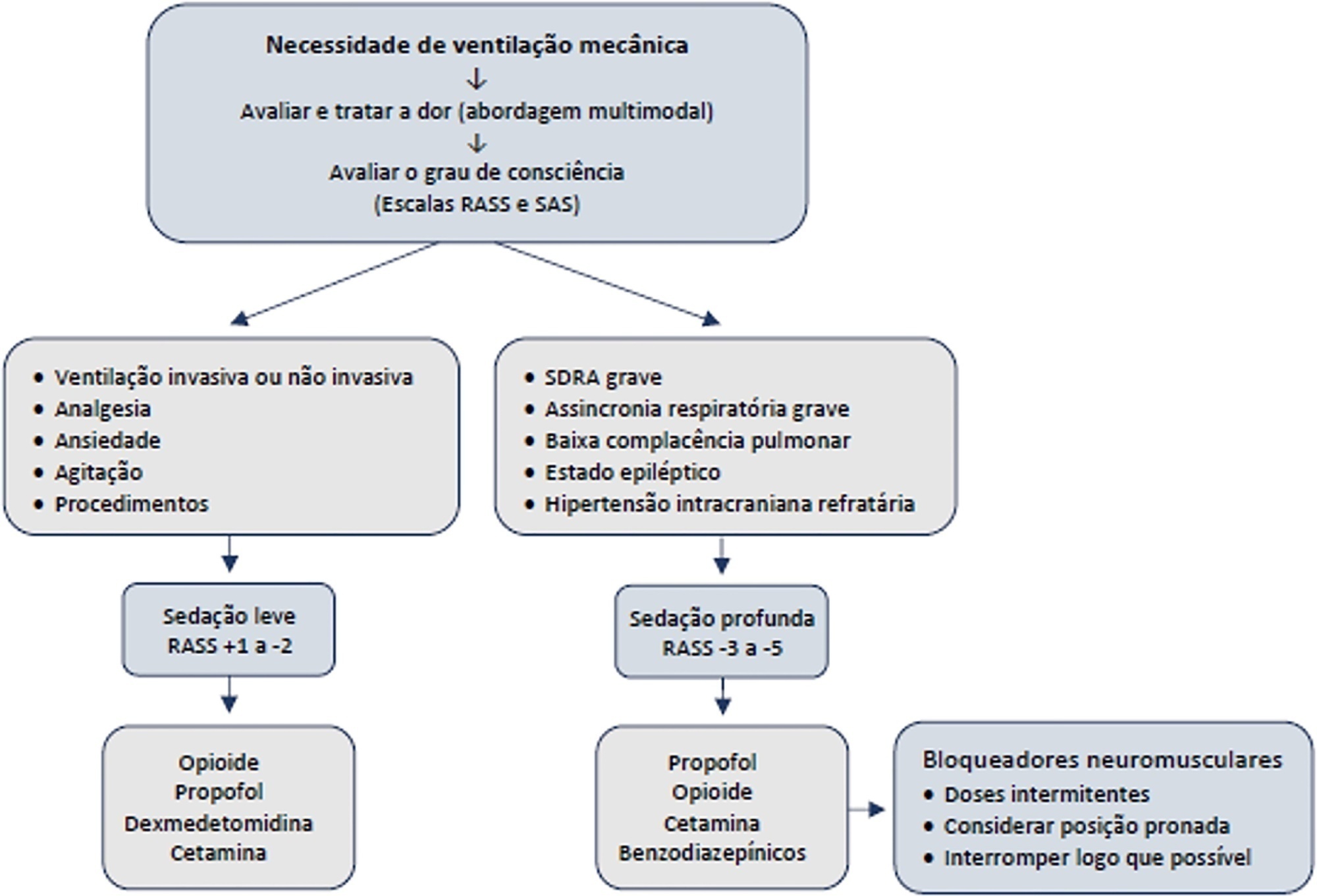
-
Commentary
Pediatric delirium in times of COVID-19
- Roberta Esteves Vieira de Castro
 ,
, - Miguel Rodríguez-Rubio,
- Maria Clara de Magalhães-Barbosa ,
- Arnaldo Prata-Barbosa
Abstract
CommentaryPediatric delirium in times of COVID-19
Rev Bras Ter Intensiva. 2021;33(4):483-486
DOI 10.5935/0103-507X.20210070
- Roberta Esteves Vieira de Castro ,
- Miguel Rodríguez-Rubio,
- Maria Clara de Magalhães-Barbosa ,
- Arnaldo Prata-Barbosa
Views0IntroductionDelirium is defined as a neurocognitive syndrome characterized by the acute onset of brain dysfunction with fluctuations in the basal mental state, inattention and disorganized thinking or altered levels of consciousness.(,) It is a frequent complication in intensive care units (ICUs).() Its occurrence is strongly predictive of an increase in the duration of mechanical ventilation […]See moreViews0Abstract
CommentaryPediatric delirium in times of COVID-19
Rev Bras Ter Intensiva. 2021;33(4):483-486
DOI 10.5935/0103-507X.20210070
- Roberta Esteves Vieira de Castro ,
- Miguel Rodríguez-Rubio,
- Maria Clara de Magalhães-Barbosa ,
- Arnaldo Prata-Barbosa
Views0IntroductionDelirium is defined as a neurocognitive syndrome characterized by the acute onset of brain dysfunction with fluctuations in the basal mental state, inattention and disorganized thinking or altered levels of consciousness.(,) It is a frequent complication in intensive care units (ICUs).() Its occurrence is strongly predictive of an increase in the duration of mechanical ventilation […]See more - Roberta Esteves Vieira de Castro
-
Special Article
Update of the recommendations of the Sociedade Portuguesa de Cuidados Intensivos and the Infection and Sepsis Group for the approach to COVID-19 in Intensive Care Medicine
- João João Mendes ,
- José Artur Paiva,
- Filipe Gonzalez,
- Paulo Mergulhão ,
- Filipe Froes, [ … ],
- João Gouveia
Abstract
Special ArticleUpdate of the recommendations of the Sociedade Portuguesa de Cuidados Intensivos and the Infection and Sepsis Group for the approach to COVID-19 in Intensive Care Medicine
Rev Bras Ter Intensiva. 2021;33(4):487-536
DOI 10.5935/0103-507X.0103-507X-rbti-20210080
- João João Mendes ,
- José Artur Paiva,
- Filipe Gonzalez,
- Paulo Mergulhão ,
- Filipe Froes,
- Roberto Roncon,
- João Gouveia
Views0ABSTRACT
Introduction:
The Sociedade Portuguesa de Cuidados Intensivos and the Infection and Sepsis Group have previously issued health service and management recommendations for critically ill patients with COVID-19. Due to the evolution of knowledge, the panel of experts was again convened to review the current evidence and issue updated recommendations.
Methods:
A national panel of experts who declared that they had no conflicts of interest regarding the development of the recommendations was assembled. Operational questions were developed based on the PICO methodology, and a rapid systematic review was conducted by consulting different bibliographic sources. The panel determined the direction and strength of the recommendations using two Delphi rounds, conducted in accordance with the principles of the GRADE system. A strong recommendation received the wording “is recommended”, and a weak recommendation was written as “is suggested.”
Results:
A total of 48 recommendations and 30 suggestions were issued, covering the following topics: diagnosis of SARS-CoV-2 infection, coinfection and superinfection; criteria for admission, cure and suspension of isolation; organization of services; personal protective equipment; and respiratory support and other specific therapies (antivirals, immunomodulators and anticoagulation).
Conclusion:
These recommendations, specifically oriented to the Portuguese reality but that may also apply to Portuguese-speaking African countries and East Timor, aim to support health professionals in the management of critically ill patients with COVID-19. They will be continuously reviewed to reflect the progress of our understanding and the treatment of this pathology.
Keywords:Coronavirus infectionsCOVID-19/diagnosisCOVID-19/therapyPractice guidelines as topicSARS-CoV-2See moreViews0Abstract
Special ArticleUpdate of the recommendations of the Sociedade Portuguesa de Cuidados Intensivos and the Infection and Sepsis Group for the approach to COVID-19 in Intensive Care Medicine
Rev Bras Ter Intensiva. 2021;33(4):487-536
DOI 10.5935/0103-507X.0103-507X-rbti-20210080
- João João Mendes ,
- José Artur Paiva,
- Filipe Gonzalez,
- Paulo Mergulhão ,
- Filipe Froes,
- Roberto Roncon,
- João Gouveia
Views0ABSTRACT
Introduction:
The Sociedade Portuguesa de Cuidados Intensivos and the Infection and Sepsis Group have previously issued health service and management recommendations for critically ill patients with COVID-19. Due to the evolution of knowledge, the panel of experts was again convened to review the current evidence and issue updated recommendations.
Methods:
A national panel of experts who declared that they had no conflicts of interest regarding the development of the recommendations was assembled. Operational questions were developed based on the PICO methodology, and a rapid systematic review was conducted by consulting different bibliographic sources. The panel determined the direction and strength of the recommendations using two Delphi rounds, conducted in accordance with the principles of the GRADE system. A strong recommendation received the wording “is recommended”, and a weak recommendation was written as “is suggested.”
Results:
A total of 48 recommendations and 30 suggestions were issued, covering the following topics: diagnosis of SARS-CoV-2 infection, coinfection and superinfection; criteria for admission, cure and suspension of isolation; organization of services; personal protective equipment; and respiratory support and other specific therapies (antivirals, immunomodulators and anticoagulation).
Conclusion:
These recommendations, specifically oriented to the Portuguese reality but that may also apply to Portuguese-speaking African countries and East Timor, aim to support health professionals in the management of critically ill patients with COVID-19. They will be continuously reviewed to reflect the progress of our understanding and the treatment of this pathology.
Keywords:Coronavirus infectionsCOVID-19/diagnosisCOVID-19/therapyPractice guidelines as topicSARS-CoV-2See more - João João Mendes
-
Original Article
Impact of liberal versus conservative saturation targets on gas exchange indices in COVID-19 related acute respiratory distress syndrome: a physiological study
- Javier Hernán Dorado ,
- Joaquín Pérez ,
- Emiliano Navarro,
- Emiliano Gogniat,
- Sebastían Torres, [ … ],
- Matías Accoce
Abstract
Original ArticleImpact of liberal versus conservative saturation targets on gas exchange indices in COVID-19 related acute respiratory distress syndrome: a physiological study
Rev Bras Ter Intensiva. 2021;33(4):537-543
DOI 10.5935/0103-507X.20210081
- Javier Hernán Dorado ,
- Joaquín Pérez ,
- Emiliano Navarro,
- Emiliano Gogniat,
- Sebastían Torres,
- Sabrina Cagide,
- Matías Accoce
Views0ABSTRACT
Objective:
To compare gas exchange indices behavior by using liberal versus conservative oxygenation targets in patients with moderate to severe acute respiratory distress syndrome secondary to COVID-19 under invasive mechanical ventilation. We also assessed the influence of high FiO2 on respiratory system mechanics.
Methods:
We prospectively included consecutive patients aged over 18 years old with a diagnosis of COVID-19 and moderate-severe acute respiratory distress syndrome. For each patient, we randomly applied two FiO2 protocols to achieve SpO2 88% – 92% or 96%. We assessed oxygenation indices and respiratory system mechanics.
Results:
We enrolled 15 patients. All the oxygenation indices were significantly affected by the FiO2 strategy (p < 0.05) selected. The PaO2/FiO2 deteriorated, PA-aO2 increased and Pa/AO2 decreased significantly when using FiO2 to achieve SpO2 96%. Conversely, the functional shunt fraction was reduced. Respiratory mechanics were not affected by the FiO2 strategy.
Conclusion:
A strategy aimed at liberal oxygenation targets significantly deteriorated gas exchange indices, except for functional shunt, in COVID-19-related acute respiratory distress syndrome. The respiratory system mechanics were not altered by the FiO2 strategy.
Keywords:artificialCOVID-19OxygenationPulmonary gas exchangeRespirationRespiratory distress syndromeRespiratory mechanicsSee moreViews0Abstract
Original ArticleImpact of liberal versus conservative saturation targets on gas exchange indices in COVID-19 related acute respiratory distress syndrome: a physiological study
Rev Bras Ter Intensiva. 2021;33(4):537-543
DOI 10.5935/0103-507X.20210081
- Javier Hernán Dorado ,
- Joaquín Pérez ,
- Emiliano Navarro,
- Emiliano Gogniat,
- Sebastían Torres,
- Sabrina Cagide,
- Matías Accoce
Views0ABSTRACT
Objective:
To compare gas exchange indices behavior by using liberal versus conservative oxygenation targets in patients with moderate to severe acute respiratory distress syndrome secondary to COVID-19 under invasive mechanical ventilation. We also assessed the influence of high FiO2 on respiratory system mechanics.
Methods:
We prospectively included consecutive patients aged over 18 years old with a diagnosis of COVID-19 and moderate-severe acute respiratory distress syndrome. For each patient, we randomly applied two FiO2 protocols to achieve SpO2 88% – 92% or 96%. We assessed oxygenation indices and respiratory system mechanics.
Results:
We enrolled 15 patients. All the oxygenation indices were significantly affected by the FiO2 strategy (p < 0.05) selected. The PaO2/FiO2 deteriorated, PA-aO2 increased and Pa/AO2 decreased significantly when using FiO2 to achieve SpO2 96%. Conversely, the functional shunt fraction was reduced. Respiratory mechanics were not affected by the FiO2 strategy.
Conclusion:
A strategy aimed at liberal oxygenation targets significantly deteriorated gas exchange indices, except for functional shunt, in COVID-19-related acute respiratory distress syndrome. The respiratory system mechanics were not altered by the FiO2 strategy.
Keywords:artificialCOVID-19OxygenationPulmonary gas exchangeRespirationRespiratory distress syndromeRespiratory mechanicsSee more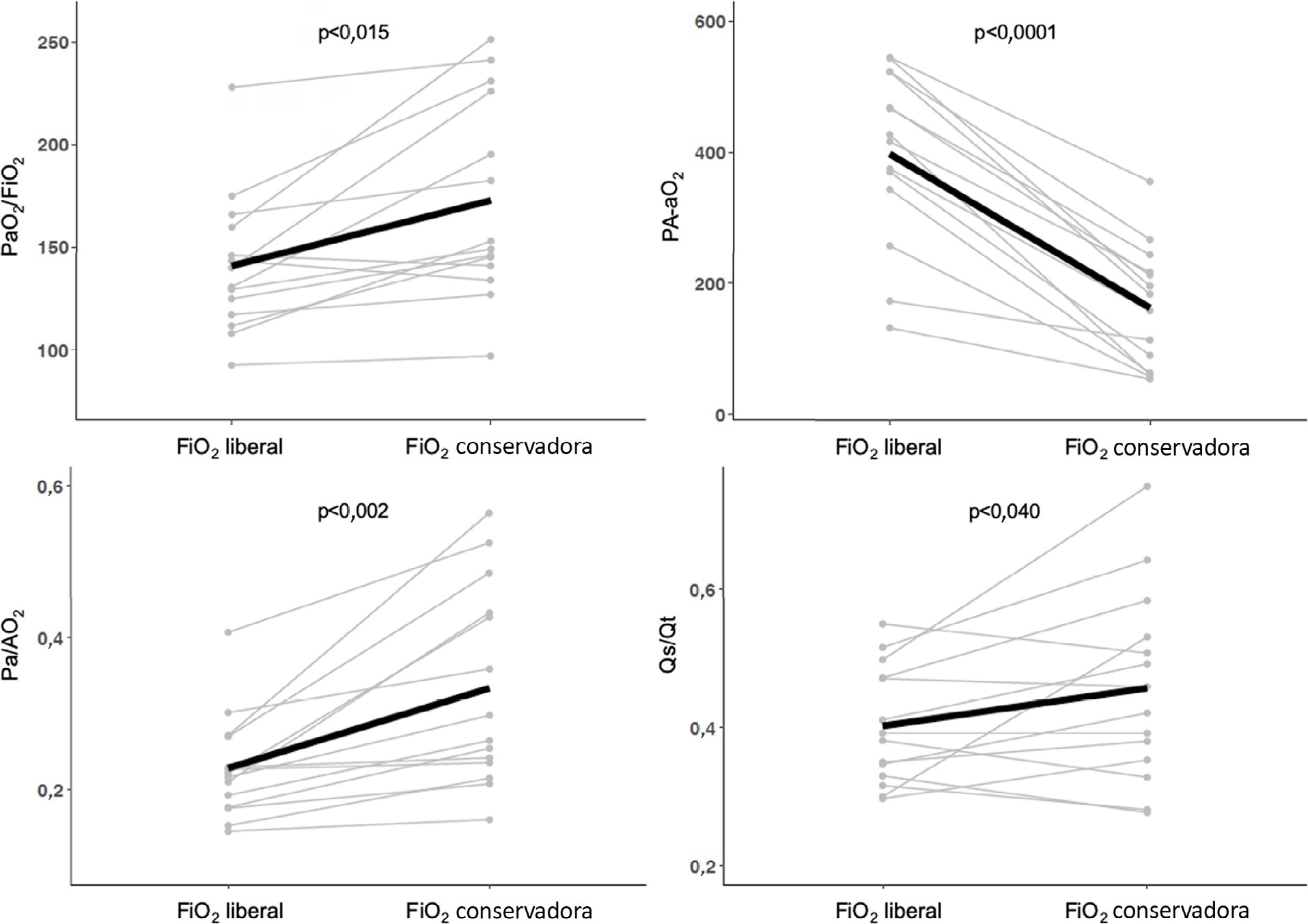
- Javier Hernán Dorado
-
Original Article
Extracorporeal membrane oxygenation for respiratory failure in children: the years before and after the 2009 H1N1 pandemic
- Felipe Rezende Caino de Oliveira ,
- Orlei Ribeiro de Araujo ,
- Daniel Garros,
- José Colleti Junior ,
- Werther Brunow de Carvalho , [ … ],
- Laurance Lequier
Abstract
Original ArticleExtracorporeal membrane oxygenation for respiratory failure in children: the years before and after the 2009 H1N1 pandemic
Rev Bras Ter Intensiva. 2021;33(4):544-548
DOI 10.5935/0103-507X.20210082
- Felipe Rezende Caino de Oliveira ,
- Orlei Ribeiro de Araujo ,
- Daniel Garros,
- José Colleti Junior ,
- Werther Brunow de Carvalho ,
- Laurance Lequier
Views0ABSTRACT
Objective:
To evaluate whether there was any impact on the number of pediatric extracorporeal membrane oxygenation runs and survival rates in the years subsequent to the 2009 pandemic.
Methods:
We studied two different periods of extracorporeal membrane oxygenation support for respiratory failure in children by analyzing datasets from the Extracorporeal Life Support Organization. Autoregressive integrated moving average models were constructed to estimate the effect of the pandemic. The year 2009 was the year of intervention (the H1N1 epidemic) in an interrupted time series model. Data collected from 2001 – 2010 were considered preintervention, and data collected from 2010 – 2017 were considered postintervention.
Results:
There was an increase in survival rates in the period 2010 – 2017 compared to 2001 – 2010 (p < 0.0001), with a significant improvement in survival when extracorporeal membrane oxygenation was performed for acute respiratory failure due to viral pneumonia. The autoregressive integrated moving average model shows an increase of 23 extracorporeal membrane oxygenation runs per year, prior to the point of the level effect (2009). In terms of survival, the preslope shows that there was no significant increase in survival rates before 2009 (p = 0.41), but the level effect was nearly significant after two years (p = 0.05), with a 6% increase in survival. In four years, there was an 8% (p = 0.03) increase in survival, and six years after 2009, there was up to a 10% (p = 0.026) increase in survival.
Conclusion:
In the years following 2009, there was a significant, global incremental increase in the extracorporeal membrane oxygenation survival rates for all runs, mainly due to improvements in the technology and treatment protocols for acute respiratory failure related to viral pneumonia and other respiratory conditions.
Keywords:ARDSChildExtracorporeal membrane oxygenationH1N1H1N1 SubtypeHumanInfluenzaInfluenza A virusPandemicsRespiratory distress syndromeRespiratory insufficiencySurvival rateSee moreViews0Abstract
Original ArticleExtracorporeal membrane oxygenation for respiratory failure in children: the years before and after the 2009 H1N1 pandemic
Rev Bras Ter Intensiva. 2021;33(4):544-548
DOI 10.5935/0103-507X.20210082
- Felipe Rezende Caino de Oliveira ,
- Orlei Ribeiro de Araujo ,
- Daniel Garros,
- José Colleti Junior ,
- Werther Brunow de Carvalho ,
- Laurance Lequier
Views0ABSTRACT
Objective:
To evaluate whether there was any impact on the number of pediatric extracorporeal membrane oxygenation runs and survival rates in the years subsequent to the 2009 pandemic.
Methods:
We studied two different periods of extracorporeal membrane oxygenation support for respiratory failure in children by analyzing datasets from the Extracorporeal Life Support Organization. Autoregressive integrated moving average models were constructed to estimate the effect of the pandemic. The year 2009 was the year of intervention (the H1N1 epidemic) in an interrupted time series model. Data collected from 2001 – 2010 were considered preintervention, and data collected from 2010 – 2017 were considered postintervention.
Results:
There was an increase in survival rates in the period 2010 – 2017 compared to 2001 – 2010 (p < 0.0001), with a significant improvement in survival when extracorporeal membrane oxygenation was performed for acute respiratory failure due to viral pneumonia. The autoregressive integrated moving average model shows an increase of 23 extracorporeal membrane oxygenation runs per year, prior to the point of the level effect (2009). In terms of survival, the preslope shows that there was no significant increase in survival rates before 2009 (p = 0.41), but the level effect was nearly significant after two years (p = 0.05), with a 6% increase in survival. In four years, there was an 8% (p = 0.03) increase in survival, and six years after 2009, there was up to a 10% (p = 0.026) increase in survival.
Conclusion:
In the years following 2009, there was a significant, global incremental increase in the extracorporeal membrane oxygenation survival rates for all runs, mainly due to improvements in the technology and treatment protocols for acute respiratory failure related to viral pneumonia and other respiratory conditions.
Keywords:ARDSChildExtracorporeal membrane oxygenationH1N1H1N1 SubtypeHumanInfluenzaInfluenza A virusPandemicsRespiratory distress syndromeRespiratory insufficiencySurvival rateSee more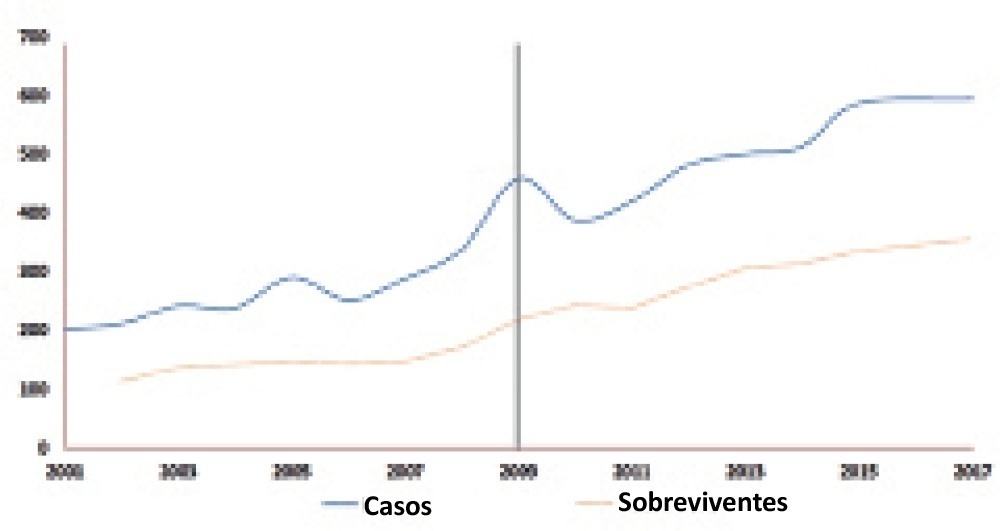
- Felipe Rezende Caino de Oliveira
-
Original Article
Correlation between syndecan-1 level and PELOD-2 score and mortality in pediatric sepsis
Rev Bras Ter Intensiva. 2021;33(4):549-556
Abstract
Original ArticleCorrelation between syndecan-1 level and PELOD-2 score and mortality in pediatric sepsis
Rev Bras Ter Intensiva. 2021;33(4):549-556
DOI 10.5935/0103-507X.20210083
Views0See moreABSTRACT
Objective:
To analyze the correlation between glycocalyx disruption measured via the serum syndecan-1 level and organ dysfunctions assessed by the PELOD-2 score and to evaluate its association with mortality in pediatric sepsis.
Methods:
We performed a prospective observational study in a tertiary public hospital. Sixty-eight pediatric patients diagnosed with sepsis according to International Pediatric Sepsis Consensus Conference criteria were consecutively recruited. We performed measurements of day 1 and day 5 serum syndecan-1 levels and PELOD-2 score components. Patients were followed up to 28 days following sepsis diagnosis.
Results:
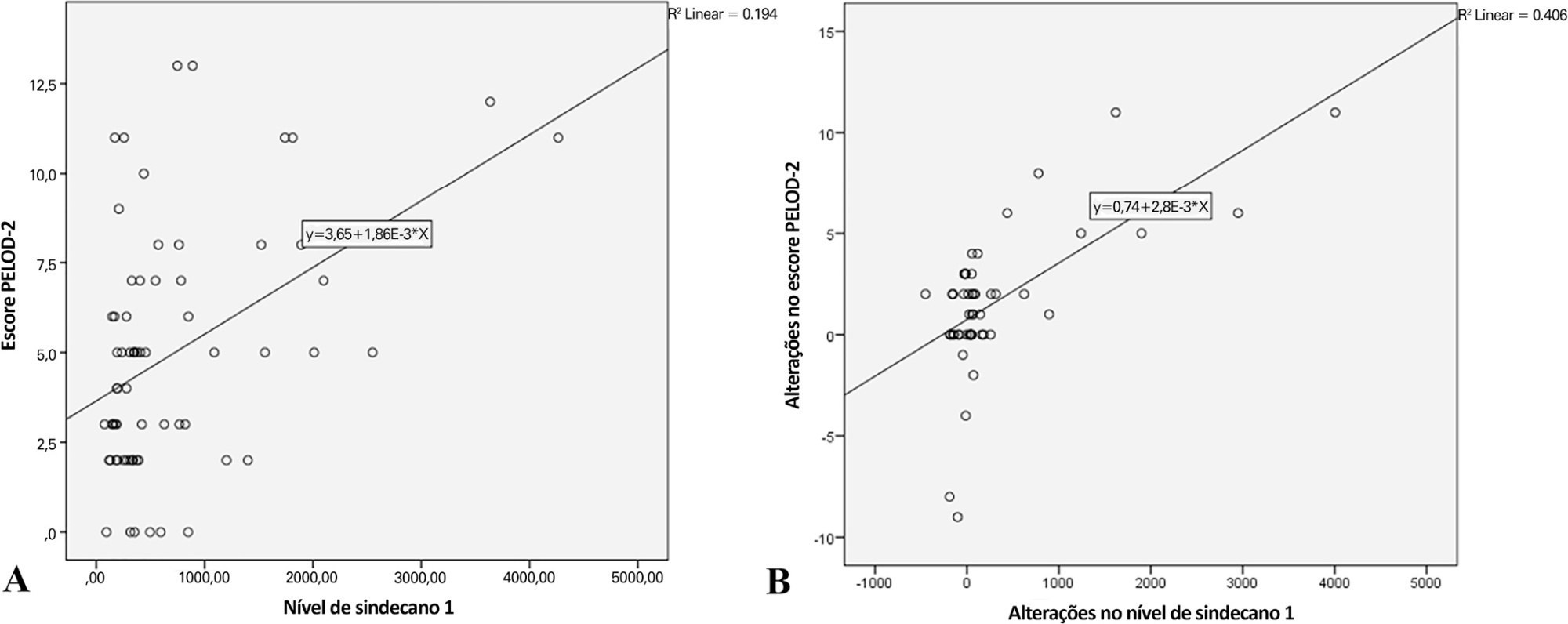
Overall, the syndecan-1 level was increased in all subjects, with a significantly higher level among septic shock patients (p = 0.01). The day 1 syndecan-1 level was positively correlated with the day 1 PELOD-2 score with a correlation coefficient of 0.35 (p = 0.003). Changes in syndecan-1 were positively correlated with changes in the PELOD-2 score, with a correlation coefficient of 0.499 (p < 0.001) during the first five days. Using the cutoff point of day 1 syndecan-1 ≥ 430ng/mL, organ dysfunction (PELOD-2 score of ≥ 8) could be predicted with an AUC of 74.3%, sensitivity of 78.6%, and specificity of 68.5% (p = 0.001).
Conclusion:
The day 1 syndecan-1 level was correlated with the day 1 PELOD-2 score but not 28-day mortality. Organ dysfunction (PELOD-2 ≥ 8) could be predicted by the syndecan-1 level in the first 24 hours of sepsis, suggesting its significant pathophysiological involvement in sepsis-associated organ dysfunction.
Views0Abstract
Original ArticleCorrelation between syndecan-1 level and PELOD-2 score and mortality in pediatric sepsis
Rev Bras Ter Intensiva. 2021;33(4):549-556
DOI 10.5935/0103-507X.20210083
Views0See moreABSTRACT
Objective:
To analyze the correlation between glycocalyx disruption measured via the serum syndecan-1 level and organ dysfunctions assessed by the PELOD-2 score and to evaluate its association with mortality in pediatric sepsis.
Methods:
We performed a prospective observational study in a tertiary public hospital. Sixty-eight pediatric patients diagnosed with sepsis according to International Pediatric Sepsis Consensus Conference criteria were consecutively recruited. We performed measurements of day 1 and day 5 serum syndecan-1 levels and PELOD-2 score components. Patients were followed up to 28 days following sepsis diagnosis.
Results:
Overall, the syndecan-1 level was increased in all subjects, with a significantly higher level among septic shock patients (p = 0.01). The day 1 syndecan-1 level was positively correlated with the day 1 PELOD-2 score with a correlation coefficient of 0.35 (p = 0.003). Changes in syndecan-1 were positively correlated with changes in the PELOD-2 score, with a correlation coefficient of 0.499 (p < 0.001) during the first five days. Using the cutoff point of day 1 syndecan-1 ≥ 430ng/mL, organ dysfunction (PELOD-2 score of ≥ 8) could be predicted with an AUC of 74.3%, sensitivity of 78.6%, and specificity of 68.5% (p = 0.001).
Conclusion:
The day 1 syndecan-1 level was correlated with the day 1 PELOD-2 score but not 28-day mortality. Organ dysfunction (PELOD-2 ≥ 8) could be predicted by the syndecan-1 level in the first 24 hours of sepsis, suggesting its significant pathophysiological involvement in sepsis-associated organ dysfunction.
-
Original Article
Lung donation and donor lung management: a survey among health care professionals in Argentina
- Vanesa Romina Ruiz ,
- Sergio Adrián Terrasa,
- Susana Bauque,
- Pablo Ezequiel Rodriguez,
- Verónica Celia Morozovsky, [ … ],
- Alejandro Daniel Midley
Abstract
Original ArticleLung donation and donor lung management: a survey among health care professionals in Argentina
Rev Bras Ter Intensiva. 2021;33(4):557-564
DOI 10.5935/0103-507X.20210072
- Vanesa Romina Ruiz ,
- Sergio Adrián Terrasa,
- Susana Bauque,
- Pablo Ezequiel Rodriguez,
- Verónica Celia Morozovsky,
- Alejandro Gabriel Da Lozzo ,
- Alejandro Daniel Midley
Views0See moreABSTRACT
Objective:
To describe health care providers’ knowledge about lung donation and donor lung management.
Methods:
A descriptive, cross-sectional study based on an anonymous survey was conducted between March and September 2018 among health care professionals registered to Sociedad Argentina de Terapia Intensiva.
Results:
Of the 736 respondents, the mean age was 40.5 years (standard deviation 8.9), and 61.3% were female. Sixty percent were physicians, 21.5% were nurses, and 17.9% were physiotherapists. Seventy-eight percent considered themselves appropriately informed about organ procurement, and 79.8% stated that they knew potential organ donor critical care management. The lung donor criteria were answered correctly by 71.3% of the respondents. However, after the donor’s brain death, 51% made no changes to ventilator parameters, 22.9% were not aware of which parameters to reprogram, and 44.5% selected tidal volume of 6 – 8mL/kg and positive end expiratory pressure of 5cmH2O. For 85% of the health care providers, the type of apnea test chosen was disconnection from the ventilator, and only 18.5% used a lung management protocol. The most frequent interventions used in the case of arterial oxygen partial pressure/fractional inspired oxygen < 300 were positive end expiratory pressure titration, closed-circuit endotracheal suctioning, and recruitment maneuvers.
Conclusion:
Health care professionals surveyed in Argentina correctly answered most of the questions related to lung donor criteria. However, they lacked detailed knowledge about ventilatory settings, ventilatory strategies, and protocols for lung donors. Educational programs are key to optimizing multiorgan donation and should be focused on protecting the donor lungs to increase the numbers of organs available for transplantation.
Views0Abstract
Original ArticleLung donation and donor lung management: a survey among health care professionals in Argentina
Rev Bras Ter Intensiva. 2021;33(4):557-564
DOI 10.5935/0103-507X.20210072
- Vanesa Romina Ruiz ,
- Sergio Adrián Terrasa,
- Susana Bauque,
- Pablo Ezequiel Rodriguez,
- Verónica Celia Morozovsky,
- Alejandro Gabriel Da Lozzo ,
- Alejandro Daniel Midley
Views0See moreABSTRACT
Objective:
To describe health care providers’ knowledge about lung donation and donor lung management.
Methods:
A descriptive, cross-sectional study based on an anonymous survey was conducted between March and September 2018 among health care professionals registered to Sociedad Argentina de Terapia Intensiva.
Results:
Of the 736 respondents, the mean age was 40.5 years (standard deviation 8.9), and 61.3% were female. Sixty percent were physicians, 21.5% were nurses, and 17.9% were physiotherapists. Seventy-eight percent considered themselves appropriately informed about organ procurement, and 79.8% stated that they knew potential organ donor critical care management. The lung donor criteria were answered correctly by 71.3% of the respondents. However, after the donor’s brain death, 51% made no changes to ventilator parameters, 22.9% were not aware of which parameters to reprogram, and 44.5% selected tidal volume of 6 – 8mL/kg and positive end expiratory pressure of 5cmH2O. For 85% of the health care providers, the type of apnea test chosen was disconnection from the ventilator, and only 18.5% used a lung management protocol. The most frequent interventions used in the case of arterial oxygen partial pressure/fractional inspired oxygen < 300 were positive end expiratory pressure titration, closed-circuit endotracheal suctioning, and recruitment maneuvers.
Conclusion:
Health care professionals surveyed in Argentina correctly answered most of the questions related to lung donor criteria. However, they lacked detailed knowledge about ventilatory settings, ventilatory strategies, and protocols for lung donors. Educational programs are key to optimizing multiorgan donation and should be focused on protecting the donor lungs to increase the numbers of organs available for transplantation.
- Vanesa Romina Ruiz
-
Original Article
Factors associated with functional decline in an intensive care unit: a prospective study on the level of physical activity and clinical factors
Rev Bras Ter Intensiva. 2021;33(4):565-571
Abstract
Original ArticleFactors associated with functional decline in an intensive care unit: a prospective study on the level of physical activity and clinical factors
Rev Bras Ter Intensiva. 2021;33(4):565-571
DOI 10.5935/0103-507X.20210073
Views1See moreABSTRACT
Objective:
To identify the factors associated with functional status decline in intensive care unit patients.
Methods:
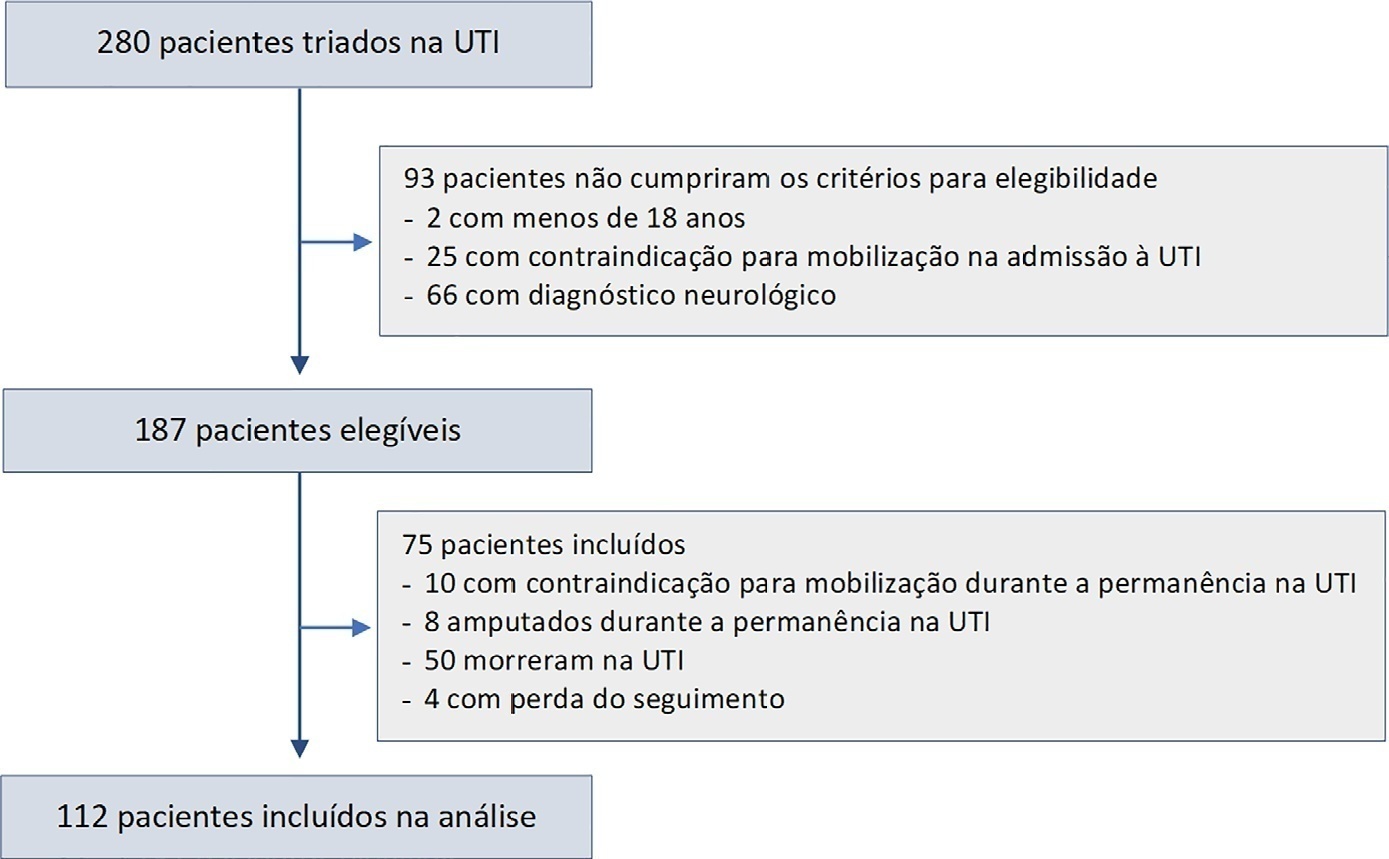
In this prospective study, patients in an intensive care unit aged 18 years or older without neurological disease or contraindications to mobilization were included. The exclusion criteria were patients who spent fewer than 4 days in the intensive care unit or died during the study period. Accelerometry was used to assess the physical activity level of patients. We recorded age, SAPS 3, days on mechanical ventilation, drugs used, comorbidities, and functional status after intensive care unit discharge. After intensive care unit discharge, the patients were assigned to a dependent group or an independent group according to their Barthel index. Logistic regression and the odds ratio were used in the analyses.
Results:
Sixty-three out of 112 included patients were assigned to the dependent group. The median Charlson comorbidity index was 3 (2 – 4). The mean SAPS 3 score was 53 ± 11. The patients spent 94 ± 4% of the time spent in inactivity and 4.8 ± 3.7% in light activities. The odds ratio showed that age (OR = 1.08; 95%CI 1.04 – 1.13) and time spent in inactivity (OR = 1.38; 95%CI 1.14 – 1.67) were factors associated with functional status decline. Time spent in light activity was associated with a better functional status (OR = 0.73; 95%CI 0.60 – 0.89).
Conclusions:
Age and time spent in inactivity during intensive care unit stay are associated with functional status decline. On the other hand, performing light activities seems to preserve the functional status of patients.
Views1Abstract
Original ArticleFactors associated with functional decline in an intensive care unit: a prospective study on the level of physical activity and clinical factors
Rev Bras Ter Intensiva. 2021;33(4):565-571
DOI 10.5935/0103-507X.20210073
Views1See moreABSTRACT
Objective:
To identify the factors associated with functional status decline in intensive care unit patients.
Methods:
In this prospective study, patients in an intensive care unit aged 18 years or older without neurological disease or contraindications to mobilization were included. The exclusion criteria were patients who spent fewer than 4 days in the intensive care unit or died during the study period. Accelerometry was used to assess the physical activity level of patients. We recorded age, SAPS 3, days on mechanical ventilation, drugs used, comorbidities, and functional status after intensive care unit discharge. After intensive care unit discharge, the patients were assigned to a dependent group or an independent group according to their Barthel index. Logistic regression and the odds ratio were used in the analyses.
Results:
Sixty-three out of 112 included patients were assigned to the dependent group. The median Charlson comorbidity index was 3 (2 – 4). The mean SAPS 3 score was 53 ± 11. The patients spent 94 ± 4% of the time spent in inactivity and 4.8 ± 3.7% in light activities. The odds ratio showed that age (OR = 1.08; 95%CI 1.04 – 1.13) and time spent in inactivity (OR = 1.38; 95%CI 1.14 – 1.67) were factors associated with functional status decline. Time spent in light activity was associated with a better functional status (OR = 0.73; 95%CI 0.60 – 0.89).
Conclusions:
Age and time spent in inactivity during intensive care unit stay are associated with functional status decline. On the other hand, performing light activities seems to preserve the functional status of patients.
-
Original Article
Influences of assisted breathing and mechanical ventilator settings on tidal volume and alveolar pressures in acute respiratory distress syndrome: a bench study
- Renata Santos Vasconcelos ,
- Raquel Pinto Sales,
- Juliana Arcanjo Lino,
- Luíza Gabriela de Carvalho Gomes,
- Nancy Delma Silva Vega Canjura Sousa, [ … ],
- Marcelo Alcantara Holanda
Abstract
Original ArticleInfluences of assisted breathing and mechanical ventilator settings on tidal volume and alveolar pressures in acute respiratory distress syndrome: a bench study
Rev Bras Ter Intensiva. 2021;33(4):572-582
DOI 10.5935/0103-507X.20210084
- Renata Santos Vasconcelos ,
- Raquel Pinto Sales,
- Juliana Arcanjo Lino,
- Luíza Gabriela de Carvalho Gomes,
- Nancy Delma Silva Vega Canjura Sousa,
- Liégina Silveira Marinho,
- Bruno do Valle Pinheiro ,
- Marcelo Alcantara Holanda
Views0ABSTRACT
Objective:
To evaluate the influences of respiratory muscle efforts and respiratory rate setting in the ventilator on tidal volume and alveolar distending pressures at end inspiration and expiration in volume-controlled ventilation and pressure-controlled ventilation modes in acute respiratory distress syndrome.
Methods:
An active test lung (ASL 5000™) connected to five intensive care unit ventilators was used in a model of acute respiratory distress syndrome. Respiratory muscle efforts (muscle pressure) were configured in three different ways: no effort (muscle pressure: 0cmH2O); inspiratory efforts only (muscle pressure:-5cmH2O, neural inspiratory time of 0.6s); and both inspiratory and expiratory muscle efforts (muscle pressure:-5/+5cmH2O). Volume-controlled and pressure-controlled ventilation modes were set to deliver a target tidal volume of 420mL and positive end-expiratory pressure of 10cmH2O. The tidal volume delivered to the lungs, alveolar pressures at the end of inspiration, and alveolar pressures at end expiration were evaluated.
Results:
When triggered by the simulated patient, the median tidal volume was 27mL lower than the set tidal volume (range-63 to +79mL), and there was variation in alveolar pressures with a median of 25.4cmH2O (range 20.5 to 30cmH2O). In the simulated scenarios with both spontaneous inspiratory and expiratory muscle efforts and with a mandatory respiratory rate lower than the simulated patient’s efforts, the median tidal volume was higher than controlled breathing.
Conclusion:
Adjusting respiratory muscle effort and pulmonary ventilator respiratory rate to a value above the patient’s respiratory rate in assisted/controlled modes generated large variations in tidal volume and pulmonary pressures, while the controlled mode showed no variations in these outcomes.
Keywords:artificialIntermittent positive-pressure breathingRespirationRespiratory distress syndromeVentilator-induced lung injurySee moreViews0Abstract
Original ArticleInfluences of assisted breathing and mechanical ventilator settings on tidal volume and alveolar pressures in acute respiratory distress syndrome: a bench study
Rev Bras Ter Intensiva. 2021;33(4):572-582
DOI 10.5935/0103-507X.20210084
- Renata Santos Vasconcelos ,
- Raquel Pinto Sales,
- Juliana Arcanjo Lino,
- Luíza Gabriela de Carvalho Gomes,
- Nancy Delma Silva Vega Canjura Sousa,
- Liégina Silveira Marinho,
- Bruno do Valle Pinheiro ,
- Marcelo Alcantara Holanda
Views0ABSTRACT
Objective:
To evaluate the influences of respiratory muscle efforts and respiratory rate setting in the ventilator on tidal volume and alveolar distending pressures at end inspiration and expiration in volume-controlled ventilation and pressure-controlled ventilation modes in acute respiratory distress syndrome.
Methods:
An active test lung (ASL 5000™) connected to five intensive care unit ventilators was used in a model of acute respiratory distress syndrome. Respiratory muscle efforts (muscle pressure) were configured in three different ways: no effort (muscle pressure: 0cmH2O); inspiratory efforts only (muscle pressure:-5cmH2O, neural inspiratory time of 0.6s); and both inspiratory and expiratory muscle efforts (muscle pressure:-5/+5cmH2O). Volume-controlled and pressure-controlled ventilation modes were set to deliver a target tidal volume of 420mL and positive end-expiratory pressure of 10cmH2O. The tidal volume delivered to the lungs, alveolar pressures at the end of inspiration, and alveolar pressures at end expiration were evaluated.
Results:
When triggered by the simulated patient, the median tidal volume was 27mL lower than the set tidal volume (range-63 to +79mL), and there was variation in alveolar pressures with a median of 25.4cmH2O (range 20.5 to 30cmH2O). In the simulated scenarios with both spontaneous inspiratory and expiratory muscle efforts and with a mandatory respiratory rate lower than the simulated patient’s efforts, the median tidal volume was higher than controlled breathing.
Conclusion:
Adjusting respiratory muscle effort and pulmonary ventilator respiratory rate to a value above the patient’s respiratory rate in assisted/controlled modes generated large variations in tidal volume and pulmonary pressures, while the controlled mode showed no variations in these outcomes.
Keywords:artificialIntermittent positive-pressure breathingRespirationRespiratory distress syndromeVentilator-induced lung injurySee more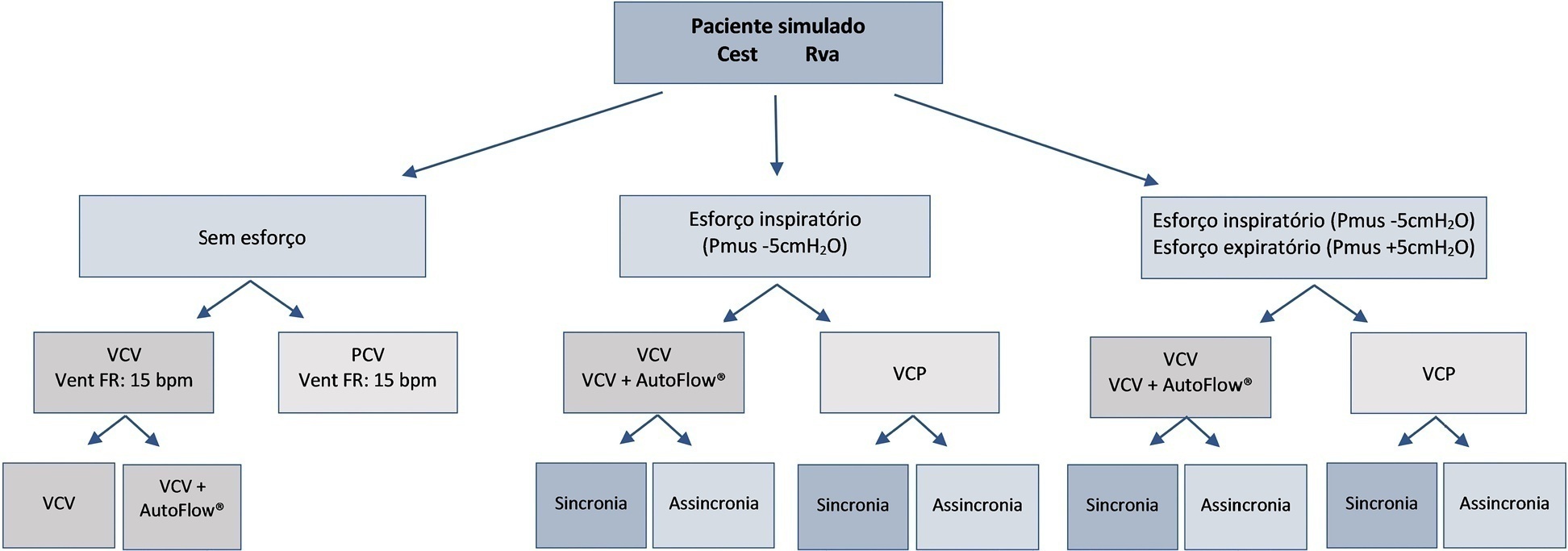
- Renata Santos Vasconcelos
-
Original Article
Acute organ failure and risk of admission to intensive medical care in cancer patients: a single center prospective cohort study
Rev Bras Ter Intensiva. 2021;33(4):583-591
Abstract
Original ArticleAcute organ failure and risk of admission to intensive medical care in cancer patients: a single center prospective cohort study
Rev Bras Ter Intensiva. 2021;33(4):583-591
DOI 10.5935/0103-507X.20210085
- Sara Coelho ,
- Teresa Ribeiro,
- Isabel Pereira,
- Delfim Duarte,
- Ana Afonso,
- Iolanda Meneses,
- Sofia Pinelas,
- Brigitte Pereira,
- Fernando Coelho,
- Anabela Martins,
- Nuno Sousa,
- Filomena Faria
Views1See moreABSTRACT
Objective:
To ascertain the cumulative incidence of acute organ failure and intensive care unit admission in cancer patients.
Methods:
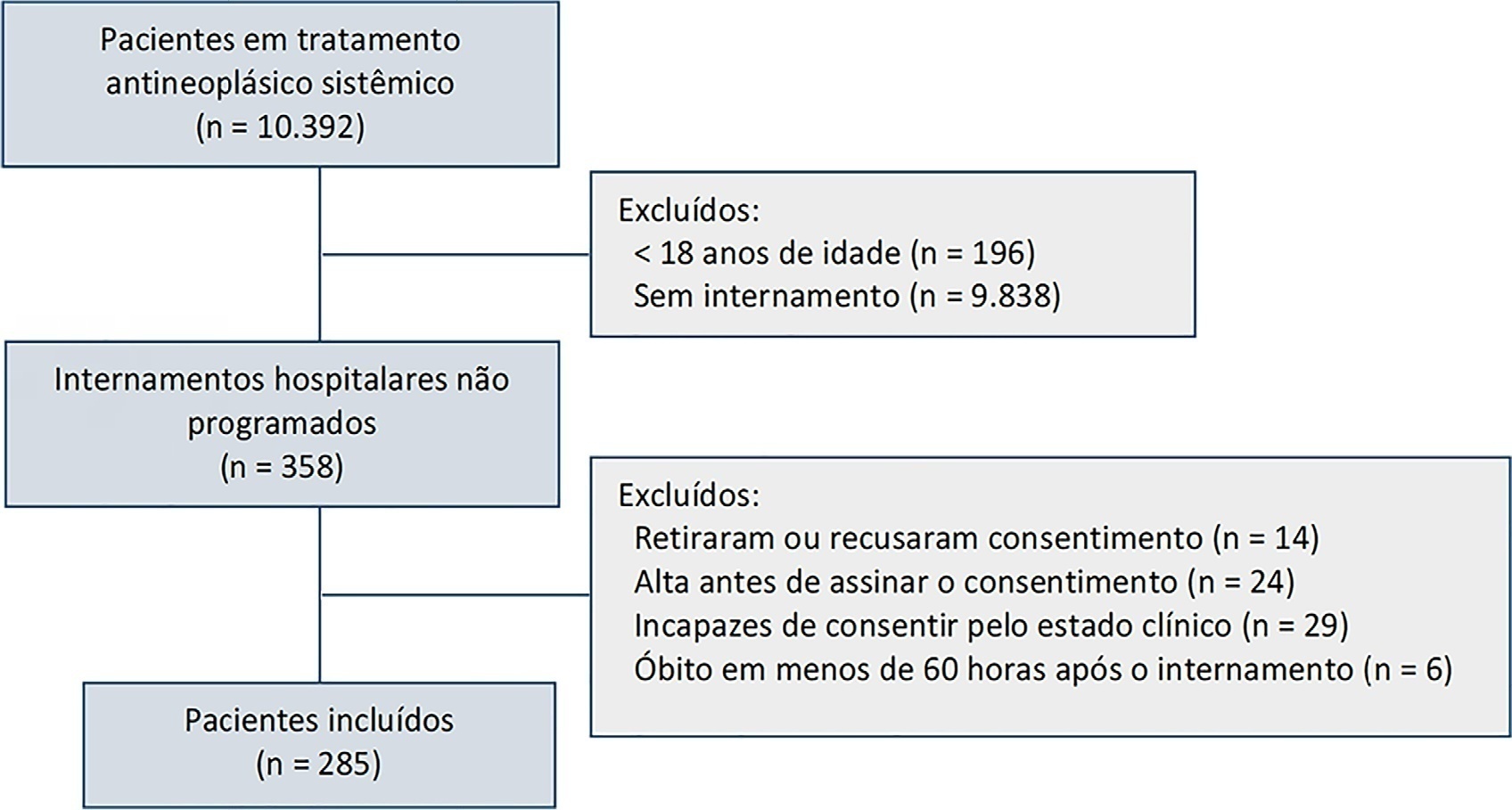
This was a single-center prospective cohort study of adult cancer patients admitted for unscheduled inpatient care while on systemic cancer treatment.
Results:
Between August 2018 and February 2019, 10,392 patients were on systemic treatment, 358 had unscheduled inpatient care and were eligible for inclusion, and 285 were included. The mean age was 60.9 years, 50.9% were male, and 17.9% of patients had hematologic cancers. The cumulative risk of acute organ failure was 39.6% (95%CI: 35 – 44), and that of intensive care unit admission among patients with acute organ failure was 15.0% (95%CI: 12 – 18). On admission, 62.1% of patients were considered not eligible for artificial organ replacement therapy. The median follow-up time was 9.5 months. Inpatient mortality was 17.5%, with an intensive care unit mortality rate of 58.8% and a median cohort survival of 134 days (95%CI: 106 – 162). In multivariate analysis, acute organ failure was associated with 6-month postdischarge mortality (HR 1.6; 95%CI: 1.2 – 2.2).
Conclusion:
The risk of acute organ failure in cancer patients admitted for unscheduled inpatient care while on systemic treatment was 39.6%, and the risk of intensive care unit admission was 15.0%. Acute organ failure in cancer patients was an independent poor prognostic factor for inpatient hospital mortality and 6-month survival.
Views1Abstract
Original ArticleAcute organ failure and risk of admission to intensive medical care in cancer patients: a single center prospective cohort study
Rev Bras Ter Intensiva. 2021;33(4):583-591
DOI 10.5935/0103-507X.20210085
- Sara Coelho ,
- Teresa Ribeiro,
- Isabel Pereira,
- Delfim Duarte,
- Ana Afonso,
- Iolanda Meneses,
- Sofia Pinelas,
- Brigitte Pereira,
- Fernando Coelho,
- Anabela Martins,
- Nuno Sousa,
- Filomena Faria
Views1See moreABSTRACT
Objective:
To ascertain the cumulative incidence of acute organ failure and intensive care unit admission in cancer patients.
Methods:
This was a single-center prospective cohort study of adult cancer patients admitted for unscheduled inpatient care while on systemic cancer treatment.
Results:
Between August 2018 and February 2019, 10,392 patients were on systemic treatment, 358 had unscheduled inpatient care and were eligible for inclusion, and 285 were included. The mean age was 60.9 years, 50.9% were male, and 17.9% of patients had hematologic cancers. The cumulative risk of acute organ failure was 39.6% (95%CI: 35 – 44), and that of intensive care unit admission among patients with acute organ failure was 15.0% (95%CI: 12 – 18). On admission, 62.1% of patients were considered not eligible for artificial organ replacement therapy. The median follow-up time was 9.5 months. Inpatient mortality was 17.5%, with an intensive care unit mortality rate of 58.8% and a median cohort survival of 134 days (95%CI: 106 – 162). In multivariate analysis, acute organ failure was associated with 6-month postdischarge mortality (HR 1.6; 95%CI: 1.2 – 2.2).
Conclusion:
The risk of acute organ failure in cancer patients admitted for unscheduled inpatient care while on systemic treatment was 39.6%, and the risk of intensive care unit admission was 15.0%. Acute organ failure in cancer patients was an independent poor prognostic factor for inpatient hospital mortality and 6-month survival.
- Sara Coelho
-
Original Article
Cross-cultural adaptation and translation of the Pediatric Intensive Care Unit-Quality of Dying and Death into Brazilian Portuguese
Rev Bras Ter Intensiva. 2021;33(4):592-599
Abstract
Original ArticleCross-cultural adaptation and translation of the Pediatric Intensive Care Unit-Quality of Dying and Death into Brazilian Portuguese
Rev Bras Ter Intensiva. 2021;33(4):592-599
DOI 10.5935/0103-507X.20210086
Views0See moreABSTRACT
Objectives:
To translate and culturally adapt the Pediatric Intensive Care Unit-Quality of Dying and Death questionnaire into Brazilian Portuguese.
Methods:
This was a cross-cultural adaptation process including conceptual, cultural, and semantic equivalence steps comprising three stages. Stage 1 involved authorization to perform the translation and cultural adaptation. Stage 2 entailed independent translation from English into Brazilian Portuguese, a synthesis of the translation, back-translation, and an expert panel. Stage 3 involved a pretest conducted with family caregivers and a multidisciplinary team.
Results:
The evaluation by the expert panel resulted in an average agreement of 0.8 in relation to semantic, cultural, and conceptual equivalence. The pretests of both versions of the questionnaire showed that the participants had adequate comprehension regarding the ease of understanding the items and response options.
Conclusion:
After going through the process of translation and cultural adaptation, the Pediatric Intensive Care Unit-Quality of Dying and Death caregiver and multidisciplinary team versions were considered culturally adapted, with both groups having a good understanding of the items. The questionnaires include relevant items to evaluate the process of death and dying in the intensive care setting, and suggest changes in care centered on patients and especially family caregivers, given the finitude of their children.
Views0Abstract
Original ArticleCross-cultural adaptation and translation of the Pediatric Intensive Care Unit-Quality of Dying and Death into Brazilian Portuguese
Rev Bras Ter Intensiva. 2021;33(4):592-599
DOI 10.5935/0103-507X.20210086
Views0See moreABSTRACT
Objectives:
To translate and culturally adapt the Pediatric Intensive Care Unit-Quality of Dying and Death questionnaire into Brazilian Portuguese.
Methods:
This was a cross-cultural adaptation process including conceptual, cultural, and semantic equivalence steps comprising three stages. Stage 1 involved authorization to perform the translation and cultural adaptation. Stage 2 entailed independent translation from English into Brazilian Portuguese, a synthesis of the translation, back-translation, and an expert panel. Stage 3 involved a pretest conducted with family caregivers and a multidisciplinary team.
Results:
The evaluation by the expert panel resulted in an average agreement of 0.8 in relation to semantic, cultural, and conceptual equivalence. The pretests of both versions of the questionnaire showed that the participants had adequate comprehension regarding the ease of understanding the items and response options.
Conclusion:
After going through the process of translation and cultural adaptation, the Pediatric Intensive Care Unit-Quality of Dying and Death caregiver and multidisciplinary team versions were considered culturally adapted, with both groups having a good understanding of the items. The questionnaires include relevant items to evaluate the process of death and dying in the intensive care setting, and suggest changes in care centered on patients and especially family caregivers, given the finitude of their children.
-
Review Article
How should dexmedetomidine and clonidine be prescribed in the critical care setting?
Rev Bras Ter Intensiva. 2021;33(4):600-615
Abstract
Review ArticleHow should dexmedetomidine and clonidine be prescribed in the critical care setting?
Rev Bras Ter Intensiva. 2021;33(4):600-615
DOI 10.5935/0103-507X.20210087
- Dan Longrois,
- Fabrice Petitjeans,
- Olivier Simonet,
- Marc de Kock,
- Marc Belliveau,
- Cyrille Pichot,
- Thomas Lieutaud,
- Marco Ghignone,
- Luc Quintin
Views3ABSTRACT
Cardiac, ventilatory and kidney management in the critical care setting has been optimized over the past decades. Cognition and sedation represent one of the last remaning challenges. As conventional sedation is suboptimal and as the sedation evoked by alpha-2 adrenergic agonists (“cooperative” sedation with dexmedetomidine, clonidine or guanfacine) represents a valuable alternative, this manuscript covers three practical topics for which evidence-based medicine is lacking: a) Switching from conventional to cooperative sedation (“switching”): the short answer is the abrupt withdrawal of conventional sedation, immediate implementation of alpha-2 agonist infusion and the use of “rescue sedation” (midazolam bolus[es]) or “breakthrough sedation” (haloperidol bolus[es]) to stabilize cooperative sedation. b) Switching from conventional to cooperative sedation in unstable patients (e.g., refractory delirium tremens, septic shock, acute respiratory distress syndrome, etc.): to avoid hypotension and bradycardia evoked by sympathetic deactivation, the short answer is to maintain the stroke volume through volume loading, vasopressors and inotropes. c) To avoid these switches and associated difficulties, alpha-2 agonists may be considered first-line sedatives. The short answer is to administer alpha-2 agonists slowly from admission or endotracheal intubation up to stabilized cooperative sedation. The “take home” message is as follows: a) alpha-2 agonists are jointly sympathetic deactivators and sedative agents; b) sympathetic deactivation implies maintaining the stroke volume and iterative assessment of volemia. Evidence-based medicine should document our propositions.
Keywords:Alpha-2 adrenergic agonistsclonidineCritical careDexmedetomidineGeneral anesthesiaGuanfacinesedationSee moreViews3Abstract
Review ArticleHow should dexmedetomidine and clonidine be prescribed in the critical care setting?
Rev Bras Ter Intensiva. 2021;33(4):600-615
DOI 10.5935/0103-507X.20210087
- Dan Longrois,
- Fabrice Petitjeans,
- Olivier Simonet,
- Marc de Kock,
- Marc Belliveau,
- Cyrille Pichot,
- Thomas Lieutaud,
- Marco Ghignone,
- Luc Quintin
Views3ABSTRACT
Cardiac, ventilatory and kidney management in the critical care setting has been optimized over the past decades. Cognition and sedation represent one of the last remaning challenges. As conventional sedation is suboptimal and as the sedation evoked by alpha-2 adrenergic agonists (“cooperative” sedation with dexmedetomidine, clonidine or guanfacine) represents a valuable alternative, this manuscript covers three practical topics for which evidence-based medicine is lacking: a) Switching from conventional to cooperative sedation (“switching”): the short answer is the abrupt withdrawal of conventional sedation, immediate implementation of alpha-2 agonist infusion and the use of “rescue sedation” (midazolam bolus[es]) or “breakthrough sedation” (haloperidol bolus[es]) to stabilize cooperative sedation. b) Switching from conventional to cooperative sedation in unstable patients (e.g., refractory delirium tremens, septic shock, acute respiratory distress syndrome, etc.): to avoid hypotension and bradycardia evoked by sympathetic deactivation, the short answer is to maintain the stroke volume through volume loading, vasopressors and inotropes. c) To avoid these switches and associated difficulties, alpha-2 agonists may be considered first-line sedatives. The short answer is to administer alpha-2 agonists slowly from admission or endotracheal intubation up to stabilized cooperative sedation. The “take home” message is as follows: a) alpha-2 agonists are jointly sympathetic deactivators and sedative agents; b) sympathetic deactivation implies maintaining the stroke volume and iterative assessment of volemia. Evidence-based medicine should document our propositions.
Keywords:Alpha-2 adrenergic agonistsclonidineCritical careDexmedetomidineGeneral anesthesiaGuanfacinesedationSee more
-
Review Article
Manual hyperinflation in children
Rev Bras Ter Intensiva. 2021;33(4):616-623
Abstract
Review ArticleManual hyperinflation in children
Rev Bras Ter Intensiva. 2021;33(4):616-623
DOI 10.5935/0103-507X.20210071
Views1ABSTRACT
Manual hyperinflation is used in neonatal and pediatric intensive care units to promote expiratory flow bias, but there is no consensus on the benefits of the technique. Thus, a review that presents supporting evidence is necessary. This study aims to review the literature on the manual hyperinflation maneuver in neonatal and pediatric intensive care units to analyze the evidence for this technique in terms of the forms of application (associated with other techniques or not), its safety, the performance of manual resuscitators and the influence of the physical therapist’s experience, in addition to evaluating the methodological quality of the identified articles. A search was performed in the following databases: Web of Science, ScienceDirect, PubMedⓇ, Scopus, CINAHL and SciELO. Two researchers independently selected the articles. Duplicate studies were assessed, evaluated by title and abstract and then read in full. The quality of the articles was analyzed using the PEDro scale. Six articles were included, two of which had high methodological quality. The main results provided information on the contribution of the positive end-expiratory pressure valve to increasing lung volumes and the use of chest compressions to optimize expiratory flow bias, the negative influence of operator experience on the increase in peak inspiratory flow, the performance of different manual resuscitators when used with the technique and the safety of application in terms of maintaining hemodynamic stability and increasing peripheral oxygen saturation. The available studies point to a positive effect of the manual hyperinflation maneuver in children who are admitted to intensive care units.
Registration PROSPERO: CRD42018108056.
Keywords:artificialChildInfantIntensive care unitsmechanicalNewbornpediatricPhysical therapy modalitiesRespirationRespiratory mechanicsRespiratory therapyventilatorsSee moreViews1Abstract
Review ArticleManual hyperinflation in children
Rev Bras Ter Intensiva. 2021;33(4):616-623
DOI 10.5935/0103-507X.20210071
Views1ABSTRACT
Manual hyperinflation is used in neonatal and pediatric intensive care units to promote expiratory flow bias, but there is no consensus on the benefits of the technique. Thus, a review that presents supporting evidence is necessary. This study aims to review the literature on the manual hyperinflation maneuver in neonatal and pediatric intensive care units to analyze the evidence for this technique in terms of the forms of application (associated with other techniques or not), its safety, the performance of manual resuscitators and the influence of the physical therapist’s experience, in addition to evaluating the methodological quality of the identified articles. A search was performed in the following databases: Web of Science, ScienceDirect, PubMedⓇ, Scopus, CINAHL and SciELO. Two researchers independently selected the articles. Duplicate studies were assessed, evaluated by title and abstract and then read in full. The quality of the articles was analyzed using the PEDro scale. Six articles were included, two of which had high methodological quality. The main results provided information on the contribution of the positive end-expiratory pressure valve to increasing lung volumes and the use of chest compressions to optimize expiratory flow bias, the negative influence of operator experience on the increase in peak inspiratory flow, the performance of different manual resuscitators when used with the technique and the safety of application in terms of maintaining hemodynamic stability and increasing peripheral oxygen saturation. The available studies point to a positive effect of the manual hyperinflation maneuver in children who are admitted to intensive care units.
Registration PROSPERO: CRD42018108056.
Keywords:artificialChildInfantIntensive care unitsmechanicalNewbornpediatricPhysical therapy modalitiesRespirationRespiratory mechanicsRespiratory therapyventilatorsSee more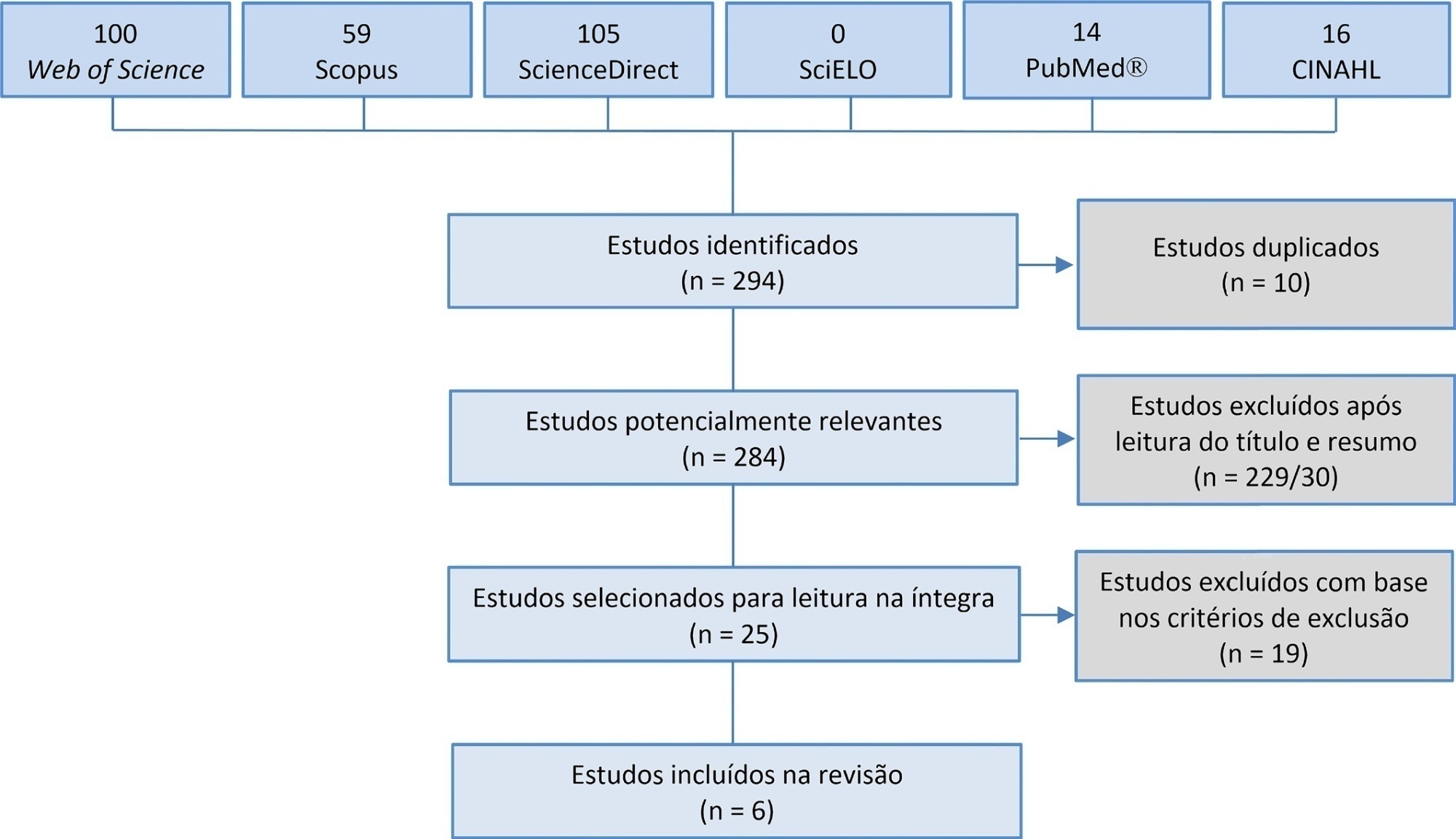
-
Review Article
Profile of adult intensive care units in Brazil: systematic review of observational studies
- Luciana Mara Meireles Aguiar ,
- Gabriela de Sousa Martins,
- Renato Valduga,
- André Paz Gerez,
- Eduardo Cunha do Carmo, [ … ],
- Marianne Lucena da Silva
Abstract
Review ArticleProfile of adult intensive care units in Brazil: systematic review of observational studies
Rev Bras Ter Intensiva. 2021;33(4):624-634
DOI 10.5935/0103-507X.20210088
- Luciana Mara Meireles Aguiar ,
- Gabriela de Sousa Martins,
- Renato Valduga,
- André Paz Gerez,
- Eduardo Cunha do Carmo,
- Katiane da Costa Cunha,
- Graziella França Bernardelli Cipriano,
- Marianne Lucena da Silva
Views1See moreABSTRACT
Objective:
To identify the clinical and epidemiological profile of adult intensive care units in Brazil.
Methods:
A systematic review was performed using a comprehensive strategy to search PubMed®, Embase, SciELO, and the Biblioteca Virtual em Saúde. The eligibility criteria for this review were observational studies that described the epidemiological and/or clinical profile of critically ill patients admitted to Brazilian intensive care units and were published between 2007 and 2020.
Results:
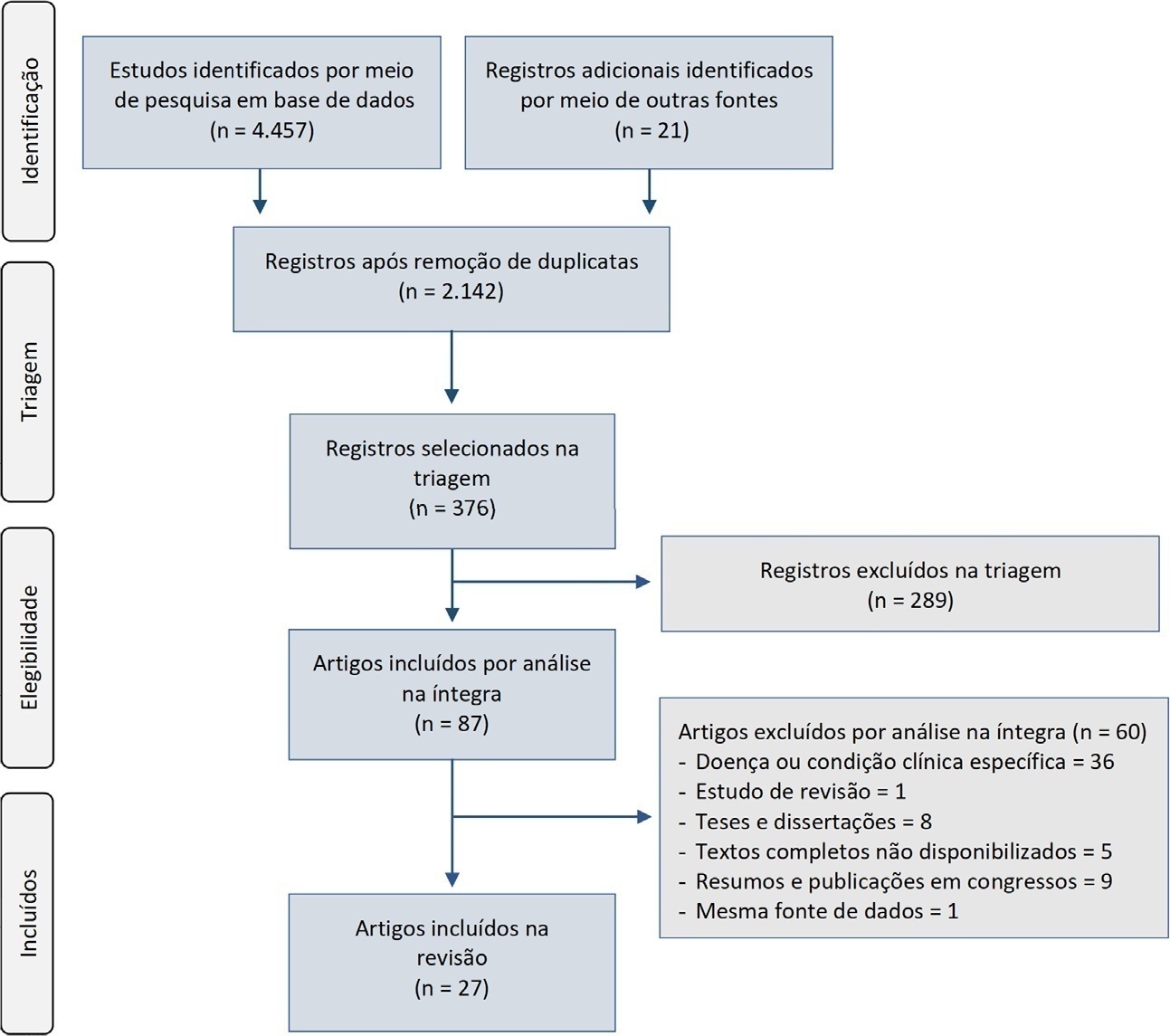
From the 4,457 identified studies, 27 were eligible for this review, constituting an analysis of 113 intensive care units and a final sample of 75,280 individuals. There was a predominance of male and elderly patients. Cardiovascular diseases were the main cause of admission to the intensive care unit. The Acute Physiology and Chronic Health Evaluation II score was the most widely used disease severity assessment system. The length of stay and mortality in the intensive care unit varied widely between institutions.
Conclusion:
These results can help guide the planning and organization of intensive care units, providing support for decision-making and the implementation of interventions that ensure better quality patient care.
Views1Abstract
Review ArticleProfile of adult intensive care units in Brazil: systematic review of observational studies
Rev Bras Ter Intensiva. 2021;33(4):624-634
DOI 10.5935/0103-507X.20210088
- Luciana Mara Meireles Aguiar ,
- Gabriela de Sousa Martins,
- Renato Valduga,
- André Paz Gerez,
- Eduardo Cunha do Carmo,
- Katiane da Costa Cunha,
- Graziella França Bernardelli Cipriano,
- Marianne Lucena da Silva
Views1See moreABSTRACT
Objective:
To identify the clinical and epidemiological profile of adult intensive care units in Brazil.
Methods:
A systematic review was performed using a comprehensive strategy to search PubMed®, Embase, SciELO, and the Biblioteca Virtual em Saúde. The eligibility criteria for this review were observational studies that described the epidemiological and/or clinical profile of critically ill patients admitted to Brazilian intensive care units and were published between 2007 and 2020.
Results:
From the 4,457 identified studies, 27 were eligible for this review, constituting an analysis of 113 intensive care units and a final sample of 75,280 individuals. There was a predominance of male and elderly patients. Cardiovascular diseases were the main cause of admission to the intensive care unit. The Acute Physiology and Chronic Health Evaluation II score was the most widely used disease severity assessment system. The length of stay and mortality in the intensive care unit varied widely between institutions.
Conclusion:
These results can help guide the planning and organization of intensive care units, providing support for decision-making and the implementation of interventions that ensure better quality patient care.
- Luciana Mara Meireles Aguiar
-
Case Report
Super-refractory status epilepticus and ketogenic diet in intensive care: a series report
Rev Bras Ter Intensiva. 2021;33(4):635-639
Abstract
Case ReportSuper-refractory status epilepticus and ketogenic diet in intensive care: a series report
Rev Bras Ter Intensiva. 2021;33(4):635-639
DOI 10.5935/0103-507X.20210089
Views0See moreAbstract
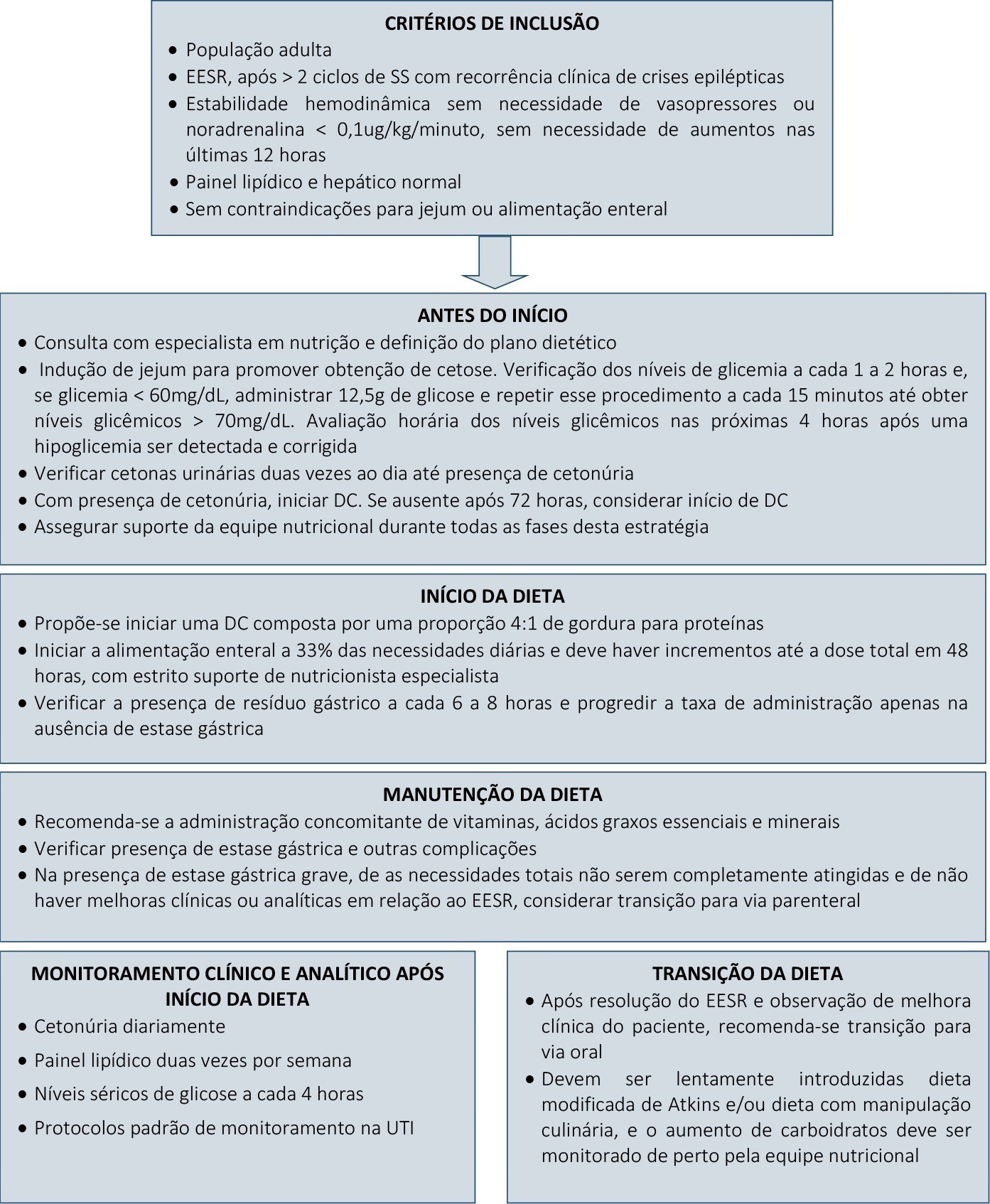
Super-refractory status epilepticus is defined as seizures that persist or reemerge in the setting of an intravenous anesthetic infusion for more than 24 hours. In recent years, attention has been driven to the potential benefits of a ketogenic diet in the management of these patients. However, the specific role of this strategy in the adult population, as well as its underlying mechanism of action and optimal time for the initiation and management of complications, remain widely debatable. We report a case series of three patients admitted to an intensive care unit due to super-refractory status epilepticus who were managed with a ketogenic diet and propose a clinical approach to its initiation, transition, and management of clinical intercurrences.
Views0Abstract
Case ReportSuper-refractory status epilepticus and ketogenic diet in intensive care: a series report
Rev Bras Ter Intensiva. 2021;33(4):635-639
DOI 10.5935/0103-507X.20210089
Views0See moreAbstract
Super-refractory status epilepticus is defined as seizures that persist or reemerge in the setting of an intravenous anesthetic infusion for more than 24 hours. In recent years, attention has been driven to the potential benefits of a ketogenic diet in the management of these patients. However, the specific role of this strategy in the adult population, as well as its underlying mechanism of action and optimal time for the initiation and management of complications, remain widely debatable. We report a case series of three patients admitted to an intensive care unit due to super-refractory status epilepticus who were managed with a ketogenic diet and propose a clinical approach to its initiation, transition, and management of clinical intercurrences.
-
Letter to the Editor
Epistaxis as a complication of high-flow nasal cannula therapy in adults
- Viviane Cordeiro Veiga ,
- Lígia Maria Coscrato Junqueira Silva,
- Érica Regina Ribeiro Sady ,
- Israel Silva Maia ,
- Alexandre Biasi Cavalcanti
Abstract
Letter to the EditorEpistaxis as a complication of high-flow nasal cannula therapy in adults
Rev Bras Ter Intensiva. 2021;33(4):640-643
DOI 10.5935/0103-507X.20210090
- Viviane Cordeiro Veiga ,
- Lígia Maria Coscrato Junqueira Silva,
- Érica Regina Ribeiro Sady ,
- Israel Silva Maia ,
- Alexandre Biasi Cavalcanti
Views1INTRODUCTIONHigh-flow nasal cannula (HFNC) therapy has emerged as a valuable therapy for adult patients with acute respiratory failure(,) or to prevent postextubation respiratory failure.(,) Currently, HFNC therapy is recommended in guidelines on the management of patients with coronavirus 2019 disease (COVID-19).() HFNC therapy delivers humidified and heated gas at a high flow that can exceed […]See moreViews1Abstract
Letter to the EditorEpistaxis as a complication of high-flow nasal cannula therapy in adults
Rev Bras Ter Intensiva. 2021;33(4):640-643
DOI 10.5935/0103-507X.20210090
- Viviane Cordeiro Veiga ,
- Lígia Maria Coscrato Junqueira Silva,
- Érica Regina Ribeiro Sady ,
- Israel Silva Maia ,
- Alexandre Biasi Cavalcanti
Views1INTRODUCTIONHigh-flow nasal cannula (HFNC) therapy has emerged as a valuable therapy for adult patients with acute respiratory failure(,) or to prevent postextubation respiratory failure.(,) Currently, HFNC therapy is recommended in guidelines on the management of patients with coronavirus 2019 disease (COVID-19).() HFNC therapy delivers humidified and heated gas at a high flow that can exceed […]See more - Viviane Cordeiro Veiga
Volume Articles - Critical Care Science (CCS)
