-
Commentary
Challenges of the coronavirus pandemic for Brazilian intensivists: present and future
Rev Bras Ter Intensiva. 2021;33(3):339-340
Abstract
CommentaryChallenges of the coronavirus pandemic for Brazilian intensivists: present and future
Rev Bras Ter Intensiva. 2021;33(3):339-340
DOI 10.5935/0103-507X.20210052
Views0Comments The first cases of severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) in Brazil was reported in February 2020. Despite the extensive reach of the Brazilian public health system and its impressive capillarity capacity throughout the entire country, not a single county or community was spared from coronavirus disease 2019 (COVID-19). The mitigation phase of […]See moreViews0

Abstract
CommentaryChallenges of the coronavirus pandemic for Brazilian intensivists: present and future
Rev Bras Ter Intensiva. 2021;33(3):339-340
DOI 10.5935/0103-507X.20210052
Views0CommentsThe first cases of severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) in Brazil was reported in February 2020. Despite the extensive reach of the Brazilian public health system and its impressive capillarity capacity throughout the entire country, not a single county or community was spared from coronavirus disease 2019 (COVID-19). The mitigation phase of the […]See more -
Commentary
Pediatric sepsis research in low- and middle-income countries: overcoming challenges
Rev Bras Ter Intensiva. 2021;33(3):341-345
Abstract
CommentaryPediatric sepsis research in low- and middle-income countries: overcoming challenges
Rev Bras Ter Intensiva. 2021;33(3):341-345
Views0Abstract
CommentaryPediatric sepsis research in low- and middle-income countries: overcoming challenges
Rev Bras Ter Intensiva. 2021;33(3):341-345
-
Original Article
Pulmonary embolism risk factors for intensive care unit anticoagulated COVID-19 patients undergoing computed tomography angiography
- Gonzalo Patricio Briceño-Mayorga
 ,
, - Rocío Gutiérrez ,
- Celine Sotomayor,
- Matías Ebner,
- Felipe Allende , [ … ],
- Rodrigo Assar
Abstract
Original ArticlePulmonary embolism risk factors for intensive care unit anticoagulated COVID-19 patients undergoing computed tomography angiography
Rev Bras Ter Intensiva. 2021;33(3):346-352
DOI 10.5935/0103-507X.20210053
- Gonzalo Patricio Briceño-Mayorga ,
- Rocío Gutiérrez ,
- Celine Sotomayor,
- Matías Ebner,
- Felipe Allende ,
- Rodrigo Assar
Views0Abstract
Objective:
To assess pulmonary embolism incidence, its relationship with D-dimer levels and other possible associated factors in addition to anticoagulation and contrast medium adverse effects.
Methods:
A retrospective observational cohort study at a Chilean public hospital was performed. Intensive care unit mechanically ventilated COVID-19 patients older than 18 years old between March and June 2020 were included. All patients received heparin thromboprophylaxis, which was increased to the anticoagulation dose with D-dimer greater than 3µg/mL.
Results:
A total of 127 patients were followed up, of whom 73 underwent pulmonary computed tomography angiography (mean age, 54 ± 12 years; 49 men). Sixty-two of the 73 patients (84.9%) received full anticoagulation before computed tomography angiography. In addition, 18 of the 73 patients had pulmonary embolism (24.7%). When comparing patients with and without pulmonary embolism, no significant differences were observed in age, sex, obesity, smoking, Wells and revised Geneva scores, D-dimer or mortality. Anticoagulant use was similar in both groups. Days from the start of anticoagulation until computed tomography angiography were significantly lower in the pulmonary embolism group (p = 0.002). Three patients presented post contrast-acute kidney injury (4.1%), and one patient had major bleeding.
Conclusion:
Despite anticoagulation, one in four COVID-19 patients connected to mechanical ventilation and evaluated with pulmonary computed tomography angiography had pulmonary embolism. With a longer the delay in performing computed tomography angiography once empirical anticoagulation was started, significantly less pulmonary embolism was identified.
Keywords:Blood coagulationComputed tomography angiographyContrast media/adverse effectsCOVID-19InfectionsIntensive care unitspulmonary embolismRespiration, artificialRespiratory insufficiencySee moreViews0Abstract
Original ArticlePulmonary embolism risk factors for intensive care unit anticoagulated COVID-19 patients undergoing computed tomography angiography
Rev Bras Ter Intensiva. 2021;33(3):346-352
DOI 10.5935/0103-507X.20210053
- Gonzalo Patricio Briceño-Mayorga ,
- Rocío Gutiérrez ,
- Celine Sotomayor,
- Matías Ebner,
- Felipe Allende ,
- Rodrigo Assar
Views0Abstract
Objective:
To assess pulmonary embolism incidence, its relationship with D-dimer levels and other possible associated factors in addition to anticoagulation and contrast medium adverse effects.
Methods:
A retrospective observational cohort study at a Chilean public hospital was performed. Intensive care unit mechanically ventilated COVID-19 patients older than 18 years old between March and June 2020 were included. All patients received heparin thromboprophylaxis, which was increased to the anticoagulation dose with D-dimer greater than 3µg/mL.
Results:
A total of 127 patients were followed up, of whom 73 underwent pulmonary computed tomography angiography (mean age, 54 ± 12 years; 49 men). Sixty-two of the 73 patients (84.9%) received full anticoagulation before computed tomography angiography. In addition, 18 of the 73 patients had pulmonary embolism (24.7%). When comparing patients with and without pulmonary embolism, no significant differences were observed in age, sex, obesity, smoking, Wells and revised Geneva scores, D-dimer or mortality. Anticoagulant use was similar in both groups. Days from the start of anticoagulation until computed tomography angiography were significantly lower in the pulmonary embolism group (p = 0.002). Three patients presented post contrast-acute kidney injury (4.1%), and one patient had major bleeding.
Conclusion:
Despite anticoagulation, one in four COVID-19 patients connected to mechanical ventilation and evaluated with pulmonary computed tomography angiography had pulmonary embolism. With a longer the delay in performing computed tomography angiography once empirical anticoagulation was started, significantly less pulmonary embolism was identified.
Keywords:Blood coagulationComputed tomography angiographyContrast media/adverse effectsCOVID-19InfectionsIntensive care unitspulmonary embolismRespiration, artificialRespiratory insufficiencySee more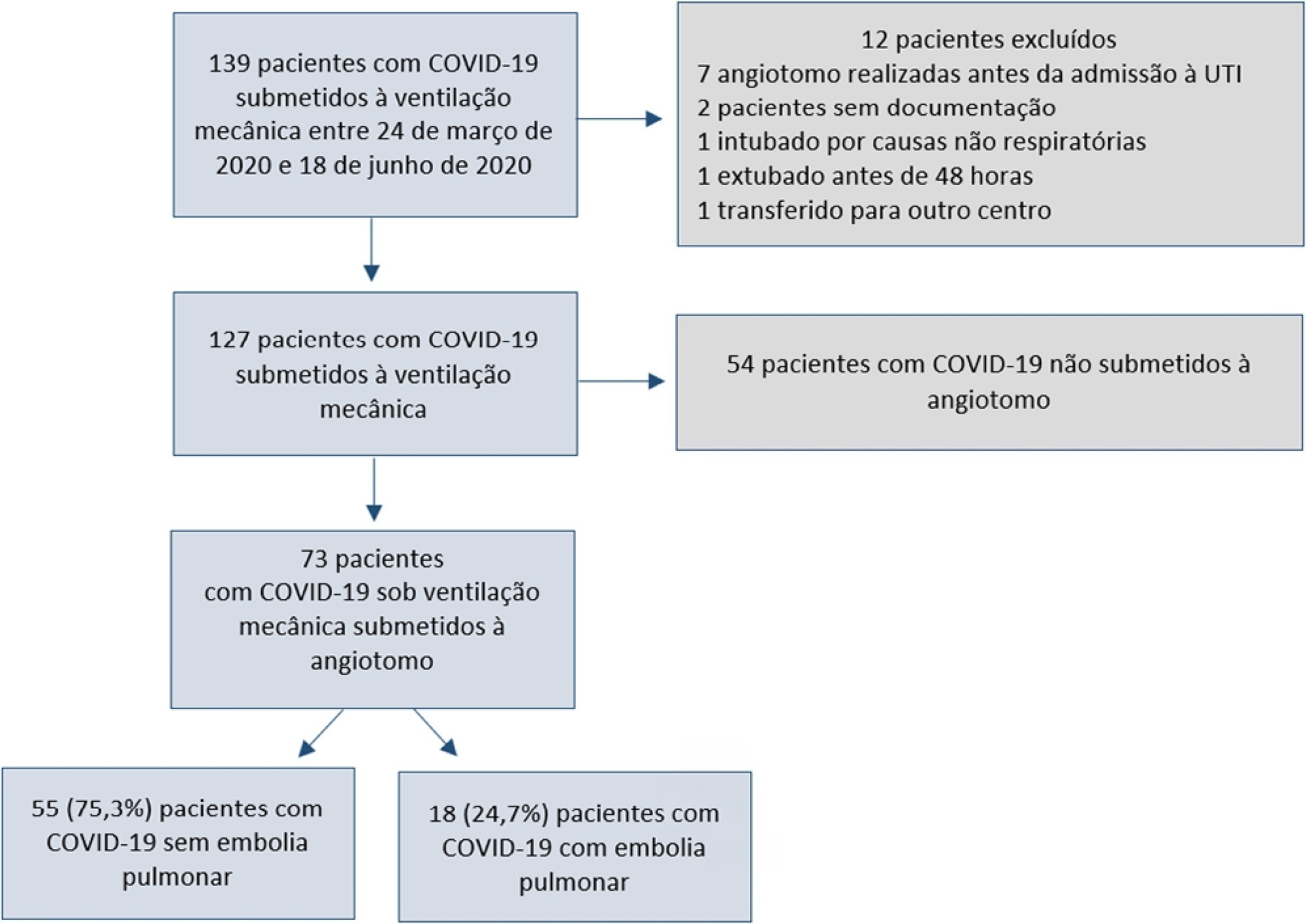
- Gonzalo Patricio Briceño-Mayorga
-
Original Article
Early Rehabilitation Index: translation and cross-cultural adaptation to Brazilian Portuguese; and Early Rehabilitation Barthel Index: validation for use in the intensive care unit
- Nair Fritzen dos Reis ,
- Roberta Rodolfo Mazzali Biscaro,
- Fernanda Cabral Xavier Sarmento Figueiredo ,
- Elizabeth Cristiane Buss Lunardelli ,
- Rosemeri Maurici da Silva
Abstract
Original ArticleEarly Rehabilitation Index: translation and cross-cultural adaptation to Brazilian Portuguese; and Early Rehabilitation Barthel Index: validation for use in the intensive care unit
Rev Bras Ter Intensiva. 2021;33(3):353-361
DOI 10.5935/0103-507X.20210051
- Nair Fritzen dos Reis ,
- Roberta Rodolfo Mazzali Biscaro,
- Fernanda Cabral Xavier Sarmento Figueiredo ,
- Elizabeth Cristiane Buss Lunardelli ,
- Rosemeri Maurici da Silva
Views0ABSTRACT
Objective:
To translate and cross-culturally adapt the Early Rehabilitation Index to Brazilian Portuguese and validate the Early Rehabilitation Barthel Index for use in the intensive care unit to assess functional status.
Methods:
The following steps were performed: preparation, translation, reconciliation, back-translation, revision, harmonization, pretesting, and psychometric evaluation. After this initial process, the Portuguese version was applied by two evaluators to patients hospitalized in the intensive care unit for at least 48 hours. The reliability of the scale was assessed by internal consistency, interrater reliability, and floor and ceiling effects. To measure construct validity, the Early Rehabilitation Barthel Index was correlated with instruments typically used to assess functional status in the intensive care unit.
Results:
A total of 122 patients with a median age of 56 (46.8 – 66) years participated in the study. The Early Rehabilitation Barthel Index had adequate reliability, with a Cronbach’s alpha coefficient of 0.65. The interrater reliability was excellent, with an intraclass correlation coefficient of 0.94 (95%CI 0.92 – 0.96), and agreement was moderate to excellent, with a kappa agreement index of 0.54 to 1.0. The floor and ceiling effects were minimal. The validity of the Early Rehabilitation Barthel Index was observed through its correlations with the total Perme score (rho = 0.72), the Functional Status Score for the ICU (rho = 0.77), the Physical Function in the Intensive Care Test score (rho = 0.69), and the Medical Research Council sum score (rho = 0.58), in addition to handgrip strength (rho = 0.58) and knee extensor strength measured by hand-held dynamometry (rho = 0.55), all with p < 0.001.
Conclusion:
The adapted versions of the Early Rehabilitation Index for Brazilian Portuguese and, in its entirety, the Early Rehabilitation Barthel Index are reliable and valid for assessing the functional status of patients at discharge from the intensive care unit.
Keywords:Critical careFunctional statusIntensive care unitsPsychometricsRehabilitationValidation studySee moreViews0Abstract
Original ArticleEarly Rehabilitation Index: translation and cross-cultural adaptation to Brazilian Portuguese; and Early Rehabilitation Barthel Index: validation for use in the intensive care unit
Rev Bras Ter Intensiva. 2021;33(3):353-361
DOI 10.5935/0103-507X.20210051
- Nair Fritzen dos Reis ,
- Roberta Rodolfo Mazzali Biscaro,
- Fernanda Cabral Xavier Sarmento Figueiredo ,
- Elizabeth Cristiane Buss Lunardelli ,
- Rosemeri Maurici da Silva
Views0ABSTRACT
Objective:
To translate and cross-culturally adapt the Early Rehabilitation Index to Brazilian Portuguese and validate the Early Rehabilitation Barthel Index for use in the intensive care unit to assess functional status.
Methods:
The following steps were performed: preparation, translation, reconciliation, back-translation, revision, harmonization, pretesting, and psychometric evaluation. After this initial process, the Portuguese version was applied by two evaluators to patients hospitalized in the intensive care unit for at least 48 hours. The reliability of the scale was assessed by internal consistency, interrater reliability, and floor and ceiling effects. To measure construct validity, the Early Rehabilitation Barthel Index was correlated with instruments typically used to assess functional status in the intensive care unit.
Results:
A total of 122 patients with a median age of 56 (46.8 – 66) years participated in the study. The Early Rehabilitation Barthel Index had adequate reliability, with a Cronbach’s alpha coefficient of 0.65. The interrater reliability was excellent, with an intraclass correlation coefficient of 0.94 (95%CI 0.92 – 0.96), and agreement was moderate to excellent, with a kappa agreement index of 0.54 to 1.0. The floor and ceiling effects were minimal. The validity of the Early Rehabilitation Barthel Index was observed through its correlations with the total Perme score (rho = 0.72), the Functional Status Score for the ICU (rho = 0.77), the Physical Function in the Intensive Care Test score (rho = 0.69), and the Medical Research Council sum score (rho = 0.58), in addition to handgrip strength (rho = 0.58) and knee extensor strength measured by hand-held dynamometry (rho = 0.55), all with p < 0.001.
Conclusion:
The adapted versions of the Early Rehabilitation Index for Brazilian Portuguese and, in its entirety, the Early Rehabilitation Barthel Index are reliable and valid for assessing the functional status of patients at discharge from the intensive care unit.
Keywords:Critical careFunctional statusIntensive care unitsPsychometricsRehabilitationValidation studySee more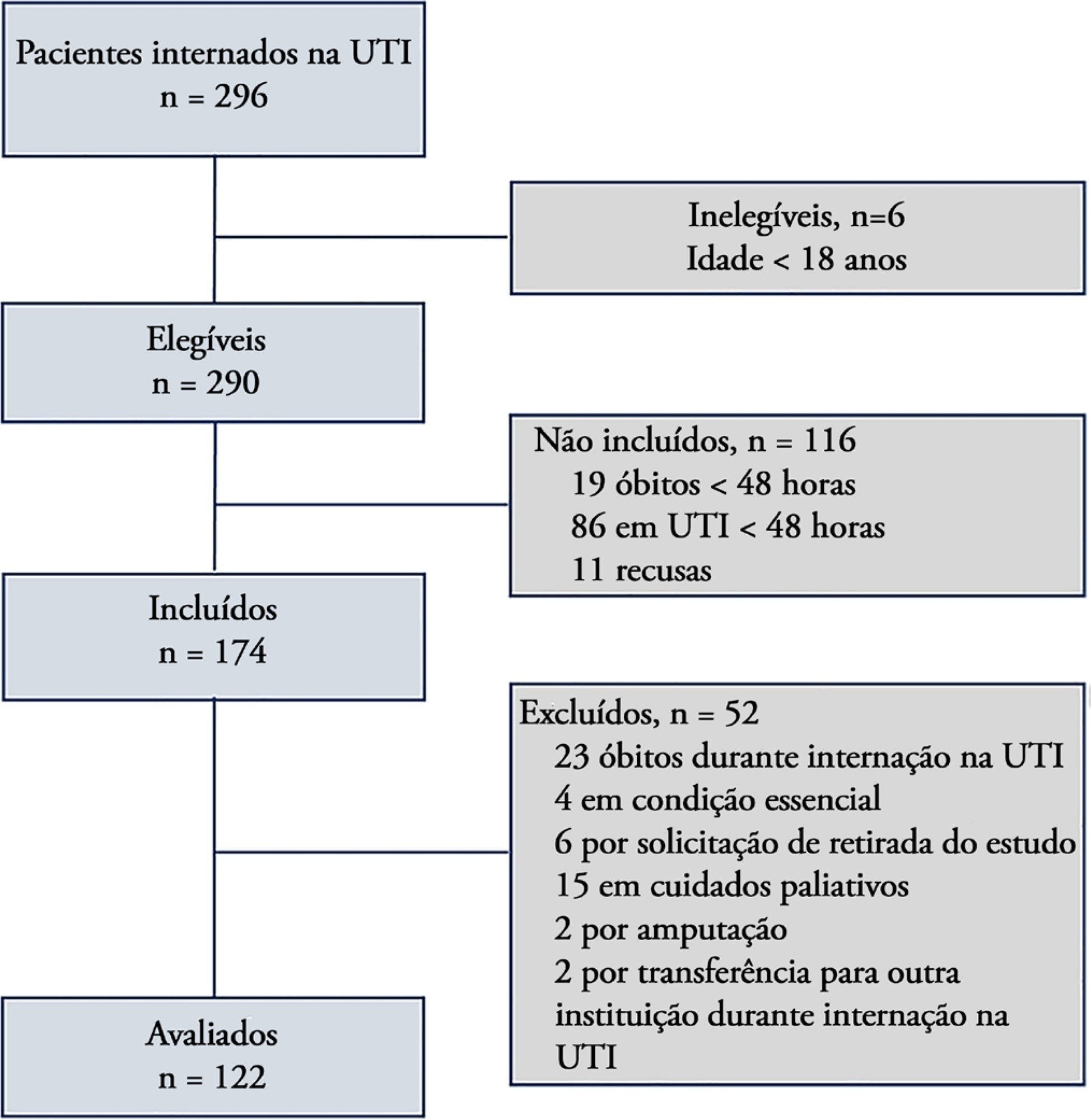
- Nair Fritzen dos Reis
-
Original Article
Noninvasive ventilation versus conventional oxygen therapy after extubation failure in high-risk patients in an intensive care unit: a pragmatic clinical trial
- Alberto Belenguer-Muncharaz ,
- Maria-Lidón Mateu-Campos,
- Bárbara Vidal-Tegedor,
- María-Desamparados Ferrándiz-Sellés,
- Maria-Luisa Micó-Gómez, [ … ],
- Jairo Rodríguez-Portillo
Abstract
Original ArticleNoninvasive ventilation versus conventional oxygen therapy after extubation failure in high-risk patients in an intensive care unit: a pragmatic clinical trial
Rev Bras Ter Intensiva. 2021;33(3):362-373
DOI 10.5935/0103-507X.20210059
- Alberto Belenguer-Muncharaz ,
- Maria-Lidón Mateu-Campos,
- Bárbara Vidal-Tegedor,
- María-Desamparados Ferrándiz-Sellés,
- Maria-Luisa Micó-Gómez,
- Susana Altaba-Tena ,
- María Arlandis-Tomás,
- Rosa Álvaro-Sánchez,
- Enver Rodríguez-Martínez,
- Jairo Rodríguez-Portillo
Views1ABSTRACT
Objective:
To determine the effectiveness of noninvasive ventilation versus conventional oxygen therapy in patients with acute respiratory failure after extubation failure.
Methods:
A pragmatic clinical trial was conducted in an intensive care unit from March 2009 to September 2016. Patients on mechanical ventilation > 24 hours who developed acute respiratory failure after scheduled extubation were included and were assigned to noninvasive ventilation or conventional oxygen therapy. The primary objective was to reduce the reintubation rate. The secondary objectives were to improve respiratory parameters and reduce complications, the duration of mechanical ventilation, the intensive care unit stay, the hospital stay, and mortality in the intensive care unit, in the hospital, and 90 days after discharge. Factors correlated with reintubation were also analyzed.
Results:
Of a total of 2,574 patients, 77 were analyzed (38 in the noninvasive ventilation group and 39 in the conventional oxygen therapy group). Noninvasive ventilation reduced the respiratory and cardiac rates more rapidly than conventional oxygen therapy. Reintubation was less common in the noninvasive ventilation group [12 (32%) versus 22 (56%) in the conventional oxygen therapy group, relative risk 0.58 (95%CI 0.34 – 0.97), p = 0.039]. The rest of the parameters did not show significant differences. In the multivariate analysis, noninvasive ventilation protected against reintubation [OR 0.17 (95%CI 0.05 – 0.56), p = 0.004], while liver failure before extubation and the inability to maintain airway patency predisposed patients to reintubation.
Conclusion:
The use of noninvasive ventilation in patients who failed extubation could be beneficial compared to conventional oxygen therapy.
Keywords:extubationNoninvasive ventilationOxygen inhalation therapyRespiration, artificialRespiratory insufficiencyWeaningSee moreViews1Abstract
Original ArticleNoninvasive ventilation versus conventional oxygen therapy after extubation failure in high-risk patients in an intensive care unit: a pragmatic clinical trial
Rev Bras Ter Intensiva. 2021;33(3):362-373
DOI 10.5935/0103-507X.20210059
- Alberto Belenguer-Muncharaz ,
- Maria-Lidón Mateu-Campos,
- Bárbara Vidal-Tegedor,
- María-Desamparados Ferrándiz-Sellés,
- Maria-Luisa Micó-Gómez,
- Susana Altaba-Tena ,
- María Arlandis-Tomás,
- Rosa Álvaro-Sánchez,
- Enver Rodríguez-Martínez,
- Jairo Rodríguez-Portillo
Views1ABSTRACT
Objective:
To determine the effectiveness of noninvasive ventilation versus conventional oxygen therapy in patients with acute respiratory failure after extubation failure.
Methods:
A pragmatic clinical trial was conducted in an intensive care unit from March 2009 to September 2016. Patients on mechanical ventilation > 24 hours who developed acute respiratory failure after scheduled extubation were included and were assigned to noninvasive ventilation or conventional oxygen therapy. The primary objective was to reduce the reintubation rate. The secondary objectives were to improve respiratory parameters and reduce complications, the duration of mechanical ventilation, the intensive care unit stay, the hospital stay, and mortality in the intensive care unit, in the hospital, and 90 days after discharge. Factors correlated with reintubation were also analyzed.
Results:
Of a total of 2,574 patients, 77 were analyzed (38 in the noninvasive ventilation group and 39 in the conventional oxygen therapy group). Noninvasive ventilation reduced the respiratory and cardiac rates more rapidly than conventional oxygen therapy. Reintubation was less common in the noninvasive ventilation group [12 (32%) versus 22 (56%) in the conventional oxygen therapy group, relative risk 0.58 (95%CI 0.34 – 0.97), p = 0.039]. The rest of the parameters did not show significant differences. In the multivariate analysis, noninvasive ventilation protected against reintubation [OR 0.17 (95%CI 0.05 – 0.56), p = 0.004], while liver failure before extubation and the inability to maintain airway patency predisposed patients to reintubation.
Conclusion:
The use of noninvasive ventilation in patients who failed extubation could be beneficial compared to conventional oxygen therapy.
Keywords:extubationNoninvasive ventilationOxygen inhalation therapyRespiration, artificialRespiratory insufficiencyWeaningSee more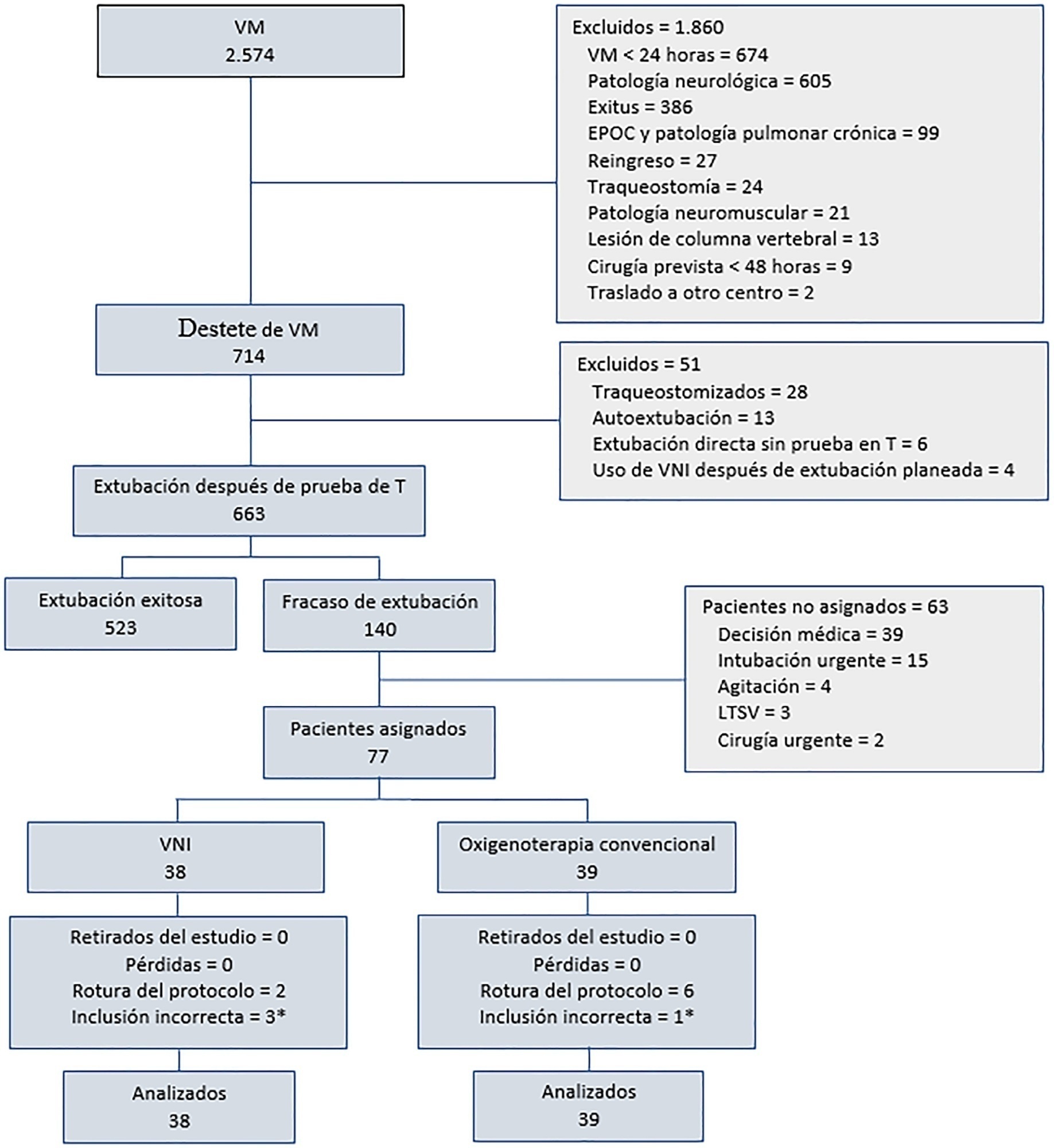
- Alberto Belenguer-Muncharaz
-
Original Article
The 6-Minute Walk Test predicts long-term physical improvement among intensive care unit survivors: a prospective cohort study
- Regis Goulart Rosa ,
- Camila Dietrich,
- Enio Luiz Tschiedel do Valle,
- Denise Souza,
- Luciana Tagliari, [ … ],
- Cassiano Teixeira
Abstract
Original ArticleThe 6-Minute Walk Test predicts long-term physical improvement among intensive care unit survivors: a prospective cohort study
Rev Bras Ter Intensiva. 2021;33(3):374-383
DOI 10.5935/0103-507X.20210056
- Regis Goulart Rosa ,
- Camila Dietrich,
- Enio Luiz Tschiedel do Valle,
- Denise Souza,
- Luciana Tagliari,
- Mariana Mattioni,
- Túlio Frederico Tonietto,
- Rosa da Rosa,
- Mirceli Goulart Barbosa,
- Gisele Agustini Lovatel,
- Pedro Dal Lago,
- Eubrando Silvestre Oliveira,
- Daniel Sganzerla,
- Juliana M. S. Andrade ,
- Paula Berto,
- Paulo Ricardo Cardoso,
- Evelin Carneiro Sanchez,
- Maicon Falavigna ,
- Juçara G. Maccari,
- Gabriela Rech,
- Caroline Robinson,
- Daniel Schneider,
- Patrícia de Leon,
- Lívia Biason,
- Cassiano Teixeira
Views1See moreABSTRACT
Objective:
To evaluate the ability of the 6-Minute Walk Test to predict long-term physical functional status improvement among intensive care unit survivors.
Methods:
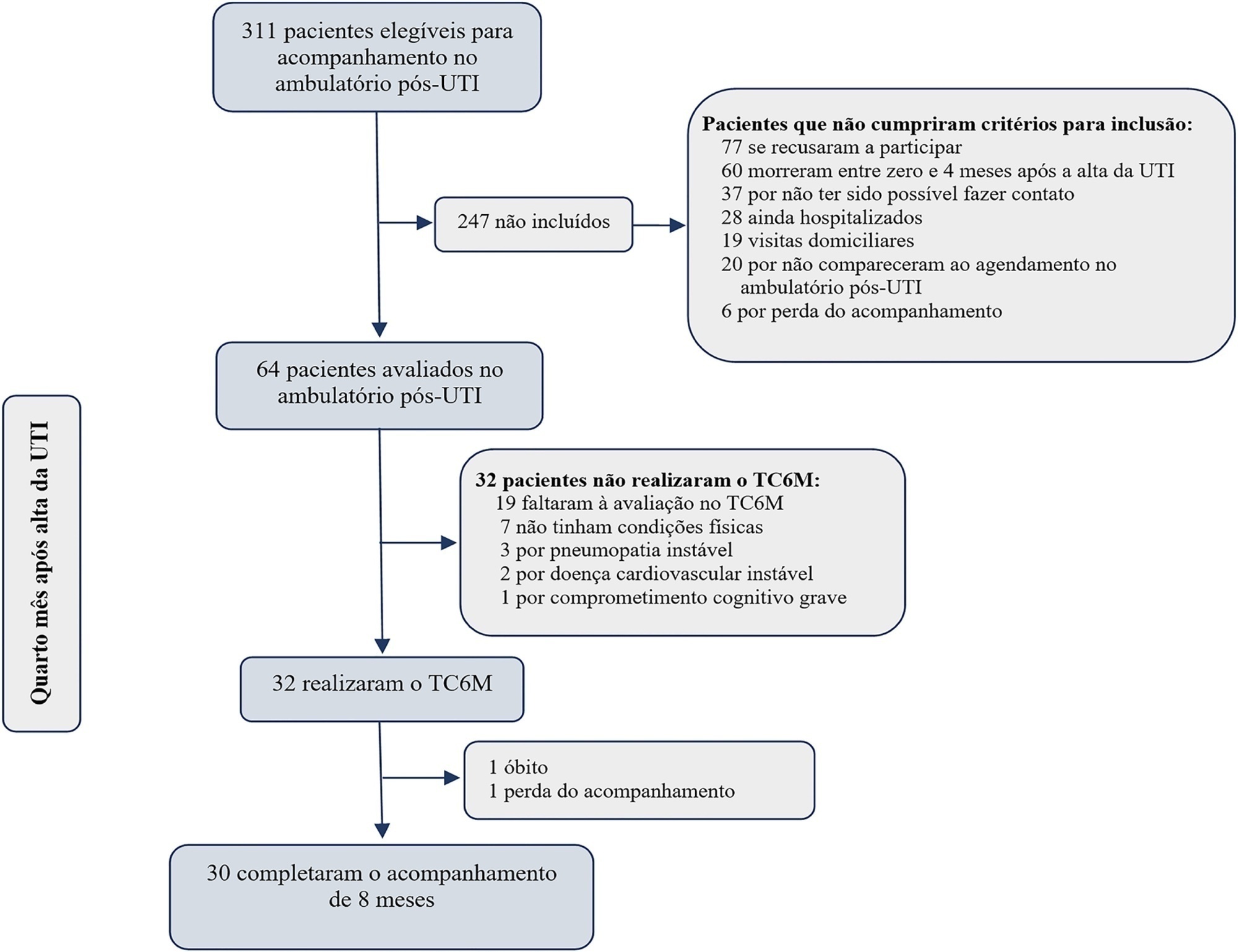
Thirty-two intensive care unit survivors were prospectively evaluated from February 2017 to August 2018 in a post-intensive care unit outpatient clinic in Brazil. Individuals with intensive care unit stays > 72 hours (emergency admissions) or > 120 hours (elective admissions) attending the post-intensive care unit clinic four months after intensive care unit discharge were consecutively enrolled. The association between the 6-Minute Walk Test distance at baseline and physical functional status was assessed over 8 months using the Barthel Index.
Results:
The mean 6-Minute Walk Test distance was significantly lower in intensive care unit survivors than in the general population (405m versus 557m; p < 0.001). Age (β = -4.0; p < 0.001) and muscle weakness (β = -99.7; p = 0.02) were associated with the 6-Minute Walk Test distance. A 6-Minute Walk Test distance was associated with improvement in physical functional status over the 8-month follow-up (odds ratio for each 10m of 1.07; 95%CI 1.01 - 1.16; p = 0.03). The area under the Receiver Operating Characteristic curve for the 6-Minute Walk Test prediction of physical functional status improvement was 0.72 (95%CI 0.53 - 0.88).
Conclusion:
The 6-Minute Walk Test performed 4 months after intensive care unit discharge predicted long-term physical functional status among intensive care unit survivors with moderate accuracy.
Views1Abstract
Original ArticleThe 6-Minute Walk Test predicts long-term physical improvement among intensive care unit survivors: a prospective cohort study
Rev Bras Ter Intensiva. 2021;33(3):374-383
DOI 10.5935/0103-507X.20210056
- Regis Goulart Rosa ,
- Camila Dietrich,
- Enio Luiz Tschiedel do Valle,
- Denise Souza,
- Luciana Tagliari,
- Mariana Mattioni,
- Túlio Frederico Tonietto,
- Rosa da Rosa,
- Mirceli Goulart Barbosa,
- Gisele Agustini Lovatel,
- Pedro Dal Lago,
- Eubrando Silvestre Oliveira,
- Daniel Sganzerla,
- Juliana M. S. Andrade ,
- Paula Berto,
- Paulo Ricardo Cardoso,
- Evelin Carneiro Sanchez,
- Maicon Falavigna ,
- Juçara G. Maccari,
- Gabriela Rech,
- Caroline Robinson,
- Daniel Schneider,
- Patrícia de Leon,
- Lívia Biason,
- Cassiano Teixeira
Views1See moreABSTRACT
Objective:
To evaluate the ability of the 6-Minute Walk Test to predict long-term physical functional status improvement among intensive care unit survivors.
Methods:
Thirty-two intensive care unit survivors were prospectively evaluated from February 2017 to August 2018 in a post-intensive care unit outpatient clinic in Brazil. Individuals with intensive care unit stays > 72 hours (emergency admissions) or > 120 hours (elective admissions) attending the post-intensive care unit clinic four months after intensive care unit discharge were consecutively enrolled. The association between the 6-Minute Walk Test distance at baseline and physical functional status was assessed over 8 months using the Barthel Index.
Results:
The mean 6-Minute Walk Test distance was significantly lower in intensive care unit survivors than in the general population (405m versus 557m; p < 0.001). Age (β = -4.0; p < 0.001) and muscle weakness (β = -99.7; p = 0.02) were associated with the 6-Minute Walk Test distance. A 6-Minute Walk Test distance was associated with improvement in physical functional status over the 8-month follow-up (odds ratio for each 10m of 1.07; 95%CI 1.01 - 1.16; p = 0.03). The area under the Receiver Operating Characteristic curve for the 6-Minute Walk Test prediction of physical functional status improvement was 0.72 (95%CI 0.53 - 0.88).
Conclusion:
The 6-Minute Walk Test performed 4 months after intensive care unit discharge predicted long-term physical functional status among intensive care unit survivors with moderate accuracy.
- Regis Goulart Rosa
-
Original Article
Clinical practices related to high-flow nasal cannulas in pediatric critical care in Brazil compared to other countries: a Brazilian survey
Rev Bras Ter Intensiva. 2021;33(3):384-393
Abstract
Original ArticleClinical practices related to high-flow nasal cannulas in pediatric critical care in Brazil compared to other countries: a Brazilian survey
Rev Bras Ter Intensiva. 2021;33(3):384-393
DOI 10.5935/0103-507X.20210055
Views1ABSTRACT
Objective:
To describe current clinical practices related to the use of high-flow nasal cannula therapy by Brazilian pediatric intensivists and compare them with those in other countries.
Methods:
A questionnaire was administered to pediatric intensivists in North and South America, Asia, Europe, and Australia/New Zealand for the main study. We compared the Brazilian cohort with cohorts in the United States of America, Canada, the United Kingdom, and India
Results:
Overall, 501 physicians responded, 127 of which were in Brazil. Only 63.8% of respondents in Brazil had a high-flow nasal cannula available, in contrast to 100% of respondents in the United Kingdom, Canada, and the United States. The attending physician was responsible for the decision to start a high-flow nasal cannula according to 61.2% respondents in Brazil, 95.5% in the United Kingdom, 96.6% in the United States, 96.8% in Canada, and 84.7% in India. A total of 62% of respondents in Brazil, 96.3% in the United Kingdom, 96.6% in the United States, 96.8% in Canada, and 84.7% in India reported that the attending physician was responsible for the decision to wean or modify the high-flow nasal cannula settings. When high-flow nasal cannula therapy failed due to respiratory distress/failure, 82% of respondents in Brazil would consider a trial of noninvasive ventilation before endotracheal intubation, compared to 93% in the United Kingdom, 88% in the United States, 91.5% in Canada, and 76.8% in India. More Brazilian intensivists (6.5%) than intensivists in the United Kingdom, United States, and India (1.6% for all) affirmed using sedatives frequently with high-flow nasal cannulas.
Conclusion:
The availability of high-flow nasal cannulas in Brazil is still not widespread. There are some divergences in clinical practices between Brazilian intensivists and their colleagues abroad, mainly in processes and decision-making about starting and weaning high-flow nasal cannula therapy.
Keywords:BrazilCanadaCannulaIndiaIntensive careIntensive care units, pediatricNoninvasive ventilationOxygen inhalation therapyRespiratory insufficiencySurveys and questionnairesUnited KingdomUnited StatesSee moreViews1Abstract
Original ArticleClinical practices related to high-flow nasal cannulas in pediatric critical care in Brazil compared to other countries: a Brazilian survey
Rev Bras Ter Intensiva. 2021;33(3):384-393
DOI 10.5935/0103-507X.20210055
Views1ABSTRACT
Objective:
To describe current clinical practices related to the use of high-flow nasal cannula therapy by Brazilian pediatric intensivists and compare them with those in other countries.
Methods:
A questionnaire was administered to pediatric intensivists in North and South America, Asia, Europe, and Australia/New Zealand for the main study. We compared the Brazilian cohort with cohorts in the United States of America, Canada, the United Kingdom, and India
Results:
Overall, 501 physicians responded, 127 of which were in Brazil. Only 63.8% of respondents in Brazil had a high-flow nasal cannula available, in contrast to 100% of respondents in the United Kingdom, Canada, and the United States. The attending physician was responsible for the decision to start a high-flow nasal cannula according to 61.2% respondents in Brazil, 95.5% in the United Kingdom, 96.6% in the United States, 96.8% in Canada, and 84.7% in India. A total of 62% of respondents in Brazil, 96.3% in the United Kingdom, 96.6% in the United States, 96.8% in Canada, and 84.7% in India reported that the attending physician was responsible for the decision to wean or modify the high-flow nasal cannula settings. When high-flow nasal cannula therapy failed due to respiratory distress/failure, 82% of respondents in Brazil would consider a trial of noninvasive ventilation before endotracheal intubation, compared to 93% in the United Kingdom, 88% in the United States, 91.5% in Canada, and 76.8% in India. More Brazilian intensivists (6.5%) than intensivists in the United Kingdom, United States, and India (1.6% for all) affirmed using sedatives frequently with high-flow nasal cannulas.
Conclusion:
The availability of high-flow nasal cannulas in Brazil is still not widespread. There are some divergences in clinical practices between Brazilian intensivists and their colleagues abroad, mainly in processes and decision-making about starting and weaning high-flow nasal cannula therapy.
Keywords:BrazilCanadaCannulaIndiaIntensive careIntensive care units, pediatricNoninvasive ventilationOxygen inhalation therapyRespiratory insufficiencySurveys and questionnairesUnited KingdomUnited StatesSee more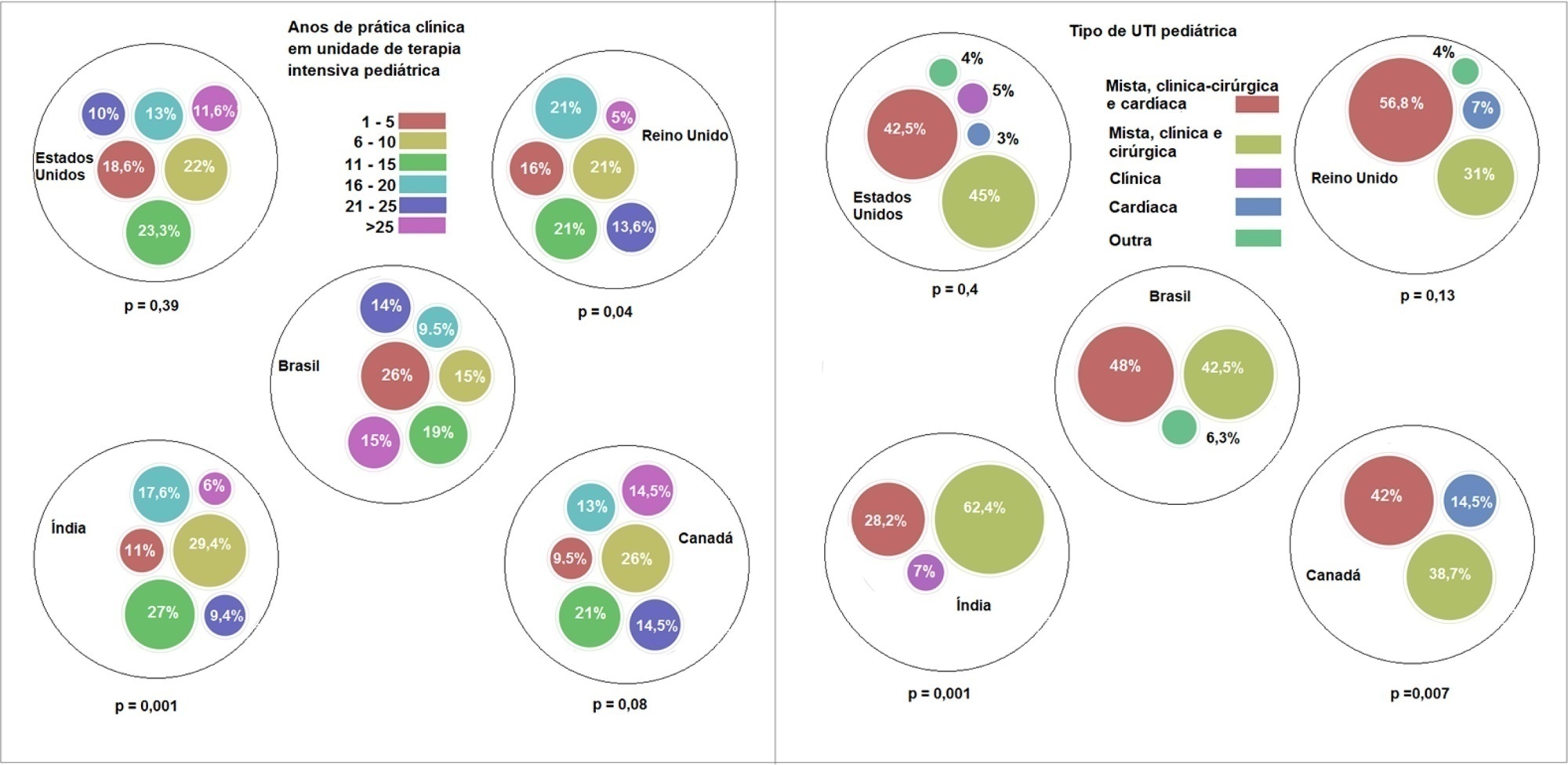
-
Original Article
SAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
- Valeska Fernandes Pasinato ,
- Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto, [ … ],
- Silvia Regina Rios Vieira
Abstract
Original ArticleSAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
Rev Bras Ter Intensiva. 2021;33(3):394-400
DOI 10.5935/0103-507X.20210064
- Valeska Fernandes Pasinato ,
- Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto,
- Gabriela Soranço Salazar,
- Silvia Regina Rios Vieira
Views2ABSTRACT
Objective:
To evaluate the substitution of Acute Physiology and Chronic Health Evaluation II (APACHE II) by Simplified Acute Physiology Score 3 (SAPS 3) as a severity marker in the modified version of the NUTrition RIsk in the Critically ill score (mNUTRIC); without interleukin 6) based on an analysis of its discriminative ability for in-hospital mortality prediction.
Methods:
This retrospective cohort study evaluated 1,516 adult patients admitted to an intensive care unit of a private general hospital from April 2017 to January 2018. Performance evaluation included Fleiss’ Kappa and Pearson correlation analysis. The discriminative ability for estimating in-hospital mortality was assessed with the Receiver Operating Characteristic curve.
Results:
The sample was randomly divided into two-thirds for model development (n = 1,025; age 72 [57 – 83]; 52.4% male) and one-third for performance evaluation (n = 490; age 72 [57 – 83]; 50.8% male). The agreement with mNUTRIC was Kappa of 0.563 (p < 0.001), and the correlation between the instruments was Pearson correlation of 0.804 (p < 0.001). The tool showed good performance in predicting in-hospital mortality (area under the curve 0.825 [0.787 - 0.863] p < 0.001).
Conclusion:
The substitution of APACHE II by SAPS 3 as a severity marker in the mNUTRIC score showed good performance in predicting in-hospital mortality. These data provide the first evidence regarding the validity of the substitution of APACHE II by SAPS 3 in the mNUTRIC as a marker of severity. Multicentric studies and additional analyses of nutritional adequacy parameters are required.
Keywords:APACHECritical careMortalitynutritional assessmentSeverity of illness indexSimplified acute physiology scoreSee moreViews2Abstract
Original ArticleSAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
Rev Bras Ter Intensiva. 2021;33(3):394-400
DOI 10.5935/0103-507X.20210064
- Valeska Fernandes Pasinato ,
- Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto,
- Gabriela Soranço Salazar,
- Silvia Regina Rios Vieira
Views2ABSTRACT
Objective:
To evaluate the substitution of Acute Physiology and Chronic Health Evaluation II (APACHE II) by Simplified Acute Physiology Score 3 (SAPS 3) as a severity marker in the modified version of the NUTrition RIsk in the Critically ill score (mNUTRIC); without interleukin 6) based on an analysis of its discriminative ability for in-hospital mortality prediction.
Methods:
This retrospective cohort study evaluated 1,516 adult patients admitted to an intensive care unit of a private general hospital from April 2017 to January 2018. Performance evaluation included Fleiss’ Kappa and Pearson correlation analysis. The discriminative ability for estimating in-hospital mortality was assessed with the Receiver Operating Characteristic curve.
Results:
The sample was randomly divided into two-thirds for model development (n = 1,025; age 72 [57 – 83]; 52.4% male) and one-third for performance evaluation (n = 490; age 72 [57 – 83]; 50.8% male). The agreement with mNUTRIC was Kappa of 0.563 (p < 0.001), and the correlation between the instruments was Pearson correlation of 0.804 (p < 0.001). The tool showed good performance in predicting in-hospital mortality (area under the curve 0.825 [0.787 - 0.863] p < 0.001).
Conclusion:
The substitution of APACHE II by SAPS 3 as a severity marker in the mNUTRIC score showed good performance in predicting in-hospital mortality. These data provide the first evidence regarding the validity of the substitution of APACHE II by SAPS 3 in the mNUTRIC as a marker of severity. Multicentric studies and additional analyses of nutritional adequacy parameters are required.
Keywords:APACHECritical careMortalitynutritional assessmentSeverity of illness indexSimplified acute physiology scoreSee more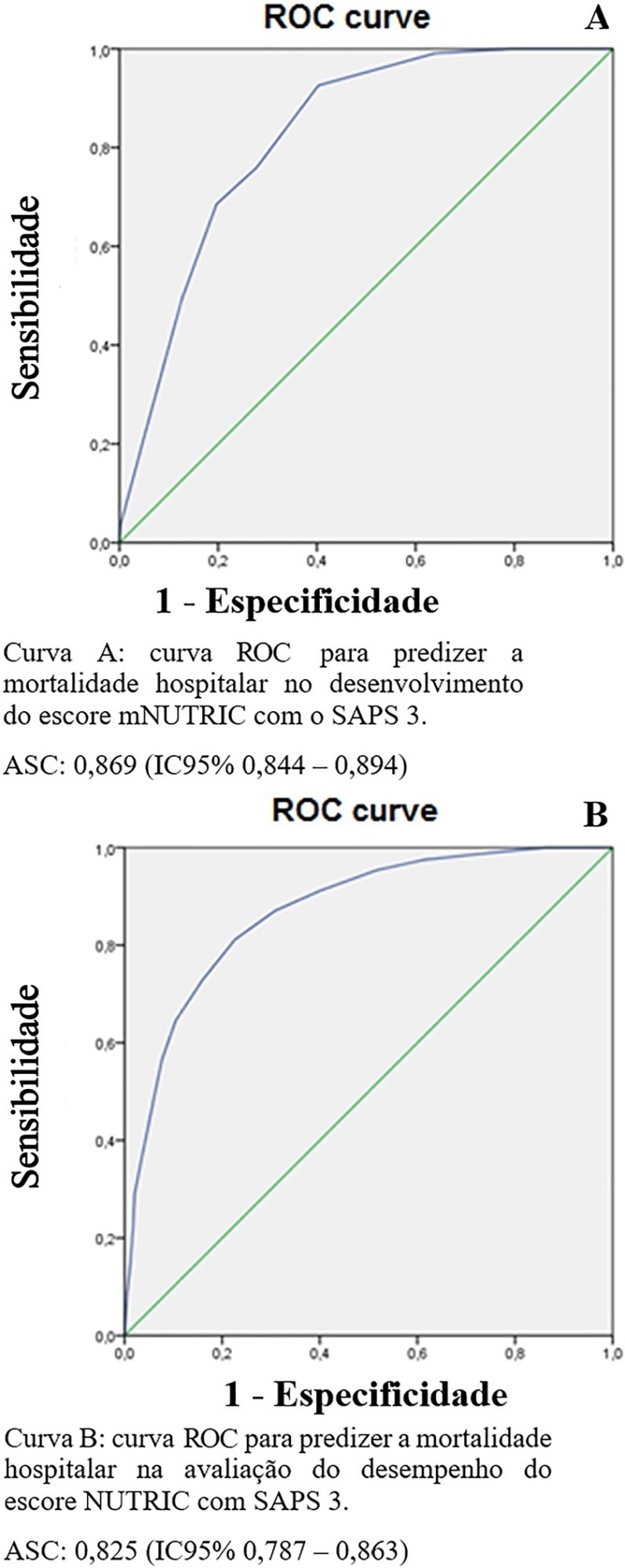
- Valeska Fernandes Pasinato
-
Original Article
Patients’ perception of medical communication and their needs during the stay in the intensive care unit
Rev Bras Ter Intensiva. 2021;33(3):401-411
Abstract
Original ArticlePatients’ perception of medical communication and their needs during the stay in the intensive care unit
Rev Bras Ter Intensiva. 2021;33(3):401-411
DOI 10.5935/0103-507X.20210050
Views0ABSTRACT
Objective:
To understand the perception of patients about medical communication as well as their needs during hospitalization in the intensive care unit.
Methods:
This study was cross-sectional descriptive and qualitative exploratory including 103 patients admitted to or recently discharged from the intensive care units of four hospitals in Greater Florianópolis, Santa Catarina state, Brazil. The patients’ sociodemographic and clinical variables were studied, as were the score they gave to the quality of medical communication through the Quality of Communication Questionnaire and their spontaneous comments with reflections or justifications for the scores given, and their responses on how they felt and what complementary help they would have liked to receive. The quantitative data were analyzed by descriptive and analytical statistics, and the qualitative data were analyzed by thematic content analysis.
Results:
The mean Quality of Communication Questionnaire score was 5.1 (standard deviation – SD = 1.3), with 8.6 (SD = 1.3) on the general communication subscale and 2.1 (SD = 1.8) on the end-of-life communication subscale. The patients had a variable understanding of medical language. Some physicians seemed to be “rushed”, according to some patients. Other patients would like to receive more frequent and detailed information and/or be respected and taken “more seriously” when they reported pain. Anxiety, sadness, and fear were among the reported feelings. Other needs included silence, more time for visits, the presence of a companion, psychological and social-work care, a bathroom that they could use, and better food in the intensive care unit.
Conclusion:
The quality of medical communication with patients is good but could improve if physicians and the healthcare team had more time for patients. Other felt needs included respect, pain relief, and adjustments in the intensive care unit dynamics and environment.
Keywords:CommunicationCritical carePatient comfortPatient preferencePatient satisfactionPhysician-patient relationsSee moreViews0Abstract
Original ArticlePatients’ perception of medical communication and their needs during the stay in the intensive care unit
Rev Bras Ter Intensiva. 2021;33(3):401-411
DOI 10.5935/0103-507X.20210050
Views0ABSTRACT
Objective:
To understand the perception of patients about medical communication as well as their needs during hospitalization in the intensive care unit.
Methods:
This study was cross-sectional descriptive and qualitative exploratory including 103 patients admitted to or recently discharged from the intensive care units of four hospitals in Greater Florianópolis, Santa Catarina state, Brazil. The patients’ sociodemographic and clinical variables were studied, as were the score they gave to the quality of medical communication through the Quality of Communication Questionnaire and their spontaneous comments with reflections or justifications for the scores given, and their responses on how they felt and what complementary help they would have liked to receive. The quantitative data were analyzed by descriptive and analytical statistics, and the qualitative data were analyzed by thematic content analysis.
Results:
The mean Quality of Communication Questionnaire score was 5.1 (standard deviation – SD = 1.3), with 8.6 (SD = 1.3) on the general communication subscale and 2.1 (SD = 1.8) on the end-of-life communication subscale. The patients had a variable understanding of medical language. Some physicians seemed to be “rushed”, according to some patients. Other patients would like to receive more frequent and detailed information and/or be respected and taken “more seriously” when they reported pain. Anxiety, sadness, and fear were among the reported feelings. Other needs included silence, more time for visits, the presence of a companion, psychological and social-work care, a bathroom that they could use, and better food in the intensive care unit.
Conclusion:
The quality of medical communication with patients is good but could improve if physicians and the healthcare team had more time for patients. Other felt needs included respect, pain relief, and adjustments in the intensive care unit dynamics and environment.
Keywords:CommunicationCritical carePatient comfortPatient preferencePatient satisfactionPhysician-patient relationsSee more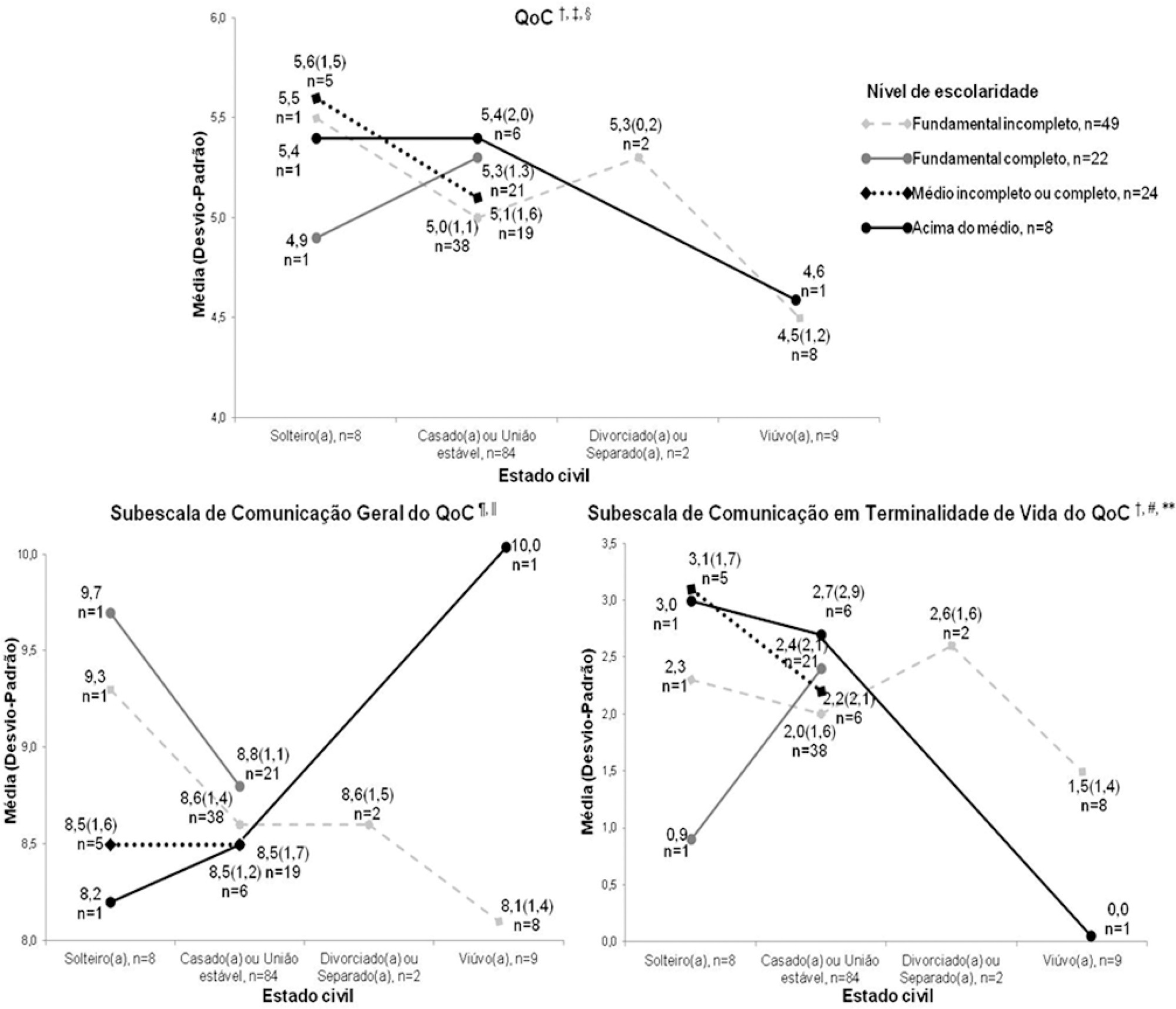
-
Original Article
Identification of abnormal pupil dilation velocity as a biomarker of cerebral injury in neurocritically ill patients
- Prachi Singh ,
- Sonia E. Stutzman,
- Aardhra Venkatachalam,
- DaiWai M. Olson,
- Arianna Barnes, [ … ],
- Folefac D. Atem
Abstract
Original ArticleIdentification of abnormal pupil dilation velocity as a biomarker of cerebral injury in neurocritically ill patients
Rev Bras Ter Intensiva. 2021;33(3):412-421
DOI 10.5935/0103-507X.20210065
- Prachi Singh ,
- Sonia E. Stutzman,
- Aardhra Venkatachalam,
- DaiWai M. Olson,
- Arianna Barnes,
- Folefac D. Atem
Views1ABSTRACT
Objective:
To calculate mean dilation velocities for Glasgow coma scale-derived injury severity classifications stratified by multiple confounding variables.
Methods:
In this study, we examined 68,813 pupil readings from 3,595 patients to determine normal dilation velocity with brain injury categorized based upon a Glasgow coma scale as mild (13 – 15), moderate (9 – 12), or severe (3 – 8). The variables age, sex, race, pupil size, intensive care unit length of stay, intracranial pressure, use of narcotics, Glasgow coma scale, and diagnosis were considered as confounding and controlled for in statistical analysis. Machine learning classification algorithm-based logistic regression was employed to identify dilation velocity cutoffs for Glasgow coma scale categories.
Results:
The odds ratios and confidence intervals of these factors were shown to be statistically significant in their influence on dilation velocity. Classification based on the area under the curve showed that for the mild Glasgow coma scale, the dilation velocity threshold value was 1.2mm/s, with false probability rates of 0.1602 and 0.1902 and areas under the curve of 0.8380 and 0.8080 in the left and right eyes, respectively. For the moderate Glasgow coma scale, the dilation velocity was 1.1mm/s, with false probability rates of 0.1880 and 0.1940 and areas under the curve of 0.8120 and 0.8060 in the left and right eyes, respectively. Furthermore, for the severe Glasgow coma scale, the dilation velocity was 0.9mm/s, with false probability rates of 0.1980 and 0.2060 and areas under the curve of 0.8020 and 0.7940 in the left and right eyes, respectively. These values were different from the previous method of subjective description and from previously estimated normal dilation velocities.
Conclusion:
Slower dilation velocities were observed in patients with lower Glasgow coma scores, indicating that decreasing velocities may indicate a higher degree of neuronal injury.
Keywords:Glasgow coma scaleNeurologic manifestationsNeuroscience/statistics and numerical dataOculomotor nerve injuriesOptic nerve injuriesPupil disordersSee moreViews1Abstract
Original ArticleIdentification of abnormal pupil dilation velocity as a biomarker of cerebral injury in neurocritically ill patients
Rev Bras Ter Intensiva. 2021;33(3):412-421
DOI 10.5935/0103-507X.20210065
- Prachi Singh ,
- Sonia E. Stutzman,
- Aardhra Venkatachalam,
- DaiWai M. Olson,
- Arianna Barnes,
- Folefac D. Atem
Views1ABSTRACT
Objective:
To calculate mean dilation velocities for Glasgow coma scale-derived injury severity classifications stratified by multiple confounding variables.
Methods:
In this study, we examined 68,813 pupil readings from 3,595 patients to determine normal dilation velocity with brain injury categorized based upon a Glasgow coma scale as mild (13 – 15), moderate (9 – 12), or severe (3 – 8). The variables age, sex, race, pupil size, intensive care unit length of stay, intracranial pressure, use of narcotics, Glasgow coma scale, and diagnosis were considered as confounding and controlled for in statistical analysis. Machine learning classification algorithm-based logistic regression was employed to identify dilation velocity cutoffs for Glasgow coma scale categories.
Results:
The odds ratios and confidence intervals of these factors were shown to be statistically significant in their influence on dilation velocity. Classification based on the area under the curve showed that for the mild Glasgow coma scale, the dilation velocity threshold value was 1.2mm/s, with false probability rates of 0.1602 and 0.1902 and areas under the curve of 0.8380 and 0.8080 in the left and right eyes, respectively. For the moderate Glasgow coma scale, the dilation velocity was 1.1mm/s, with false probability rates of 0.1880 and 0.1940 and areas under the curve of 0.8120 and 0.8060 in the left and right eyes, respectively. Furthermore, for the severe Glasgow coma scale, the dilation velocity was 0.9mm/s, with false probability rates of 0.1980 and 0.2060 and areas under the curve of 0.8020 and 0.7940 in the left and right eyes, respectively. These values were different from the previous method of subjective description and from previously estimated normal dilation velocities.
Conclusion:
Slower dilation velocities were observed in patients with lower Glasgow coma scores, indicating that decreasing velocities may indicate a higher degree of neuronal injury.
Keywords:Glasgow coma scaleNeurologic manifestationsNeuroscience/statistics and numerical dataOculomotor nerve injuriesOptic nerve injuriesPupil disordersSee more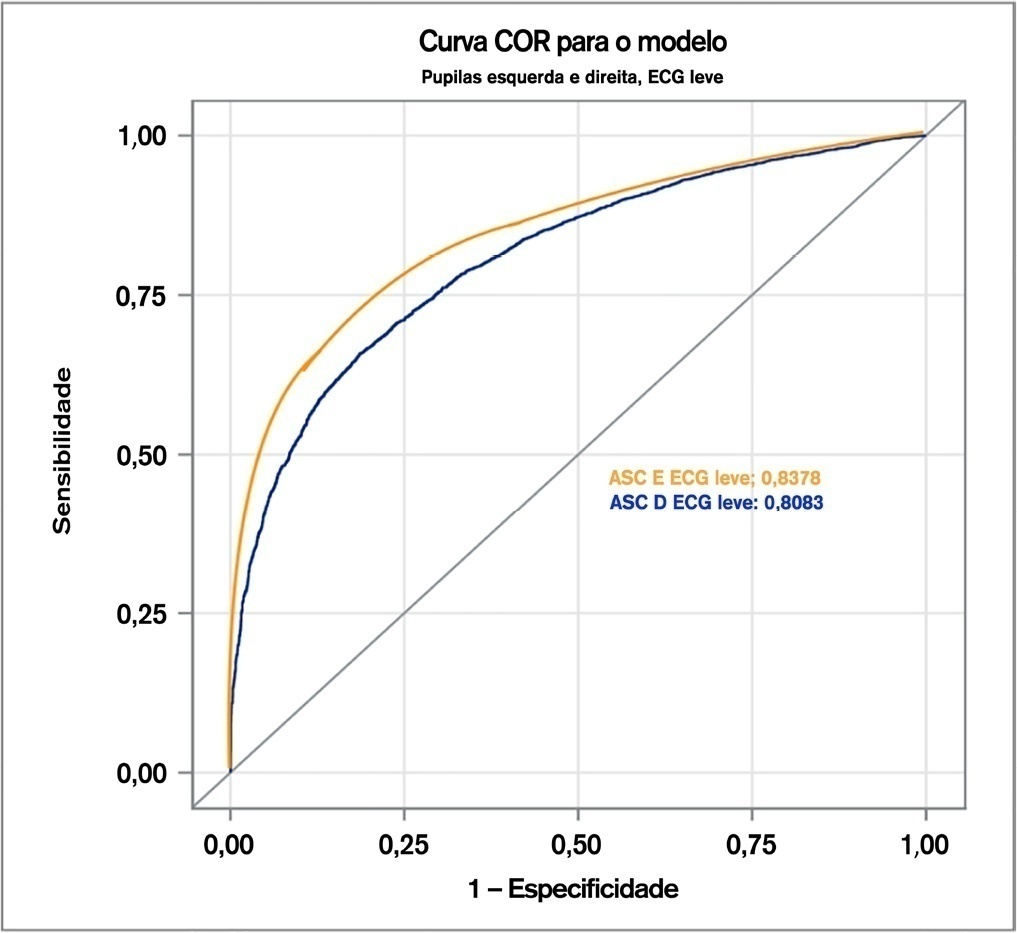
- Prachi Singh
-
Original Article
Postextubation fluid balance is associated with extubation failure: a cohort study
- Priscila Albrecht dos Santos,
- Alexandre Ribas,
- Thiele Cabral Coelho Quadros ,
- Clarissa Netto Blattner,
- Márcio Manozzo Boniatti
Abstract
Original ArticlePostextubation fluid balance is associated with extubation failure: a cohort study
Rev Bras Ter Intensiva. 2021;33(3):422-427
DOI 10.5935/0103-507X.20210057
- Priscila Albrecht dos Santos,
- Alexandre Ribas,
- Thiele Cabral Coelho Quadros ,
- Clarissa Netto Blattner,
- Márcio Manozzo Boniatti
Views1ABSTRACT
Objective:
To assess whether there is an association between 48-hour postextubation fluid balance and extubation failure.
Methods:
This was a prospective cohort study that included patients admitted to the intensive care unit of a tertiary hospital in southern Brazil from March 2019 to December 2019. Patients who required mechanical ventilation for at least 24 hours and who were extubated during the study period were included. The primary outcome was extubation failure, considered as the need for reintubation in the first 72 hours after extubation. The secondary outcome was a combined outcome with extubation failure or the need for therapeutic noninvasive ventilation.
Results:
A total of 101 patients were included. Extubation failure was observed in 29 (28.7%) patients. In univariate analysis, patients with a negative 48-hour postextubation fluid balance higher than one liter had a lower rate of extubation failure (12.0%) than patients with a negative 48-hour postextubation fluid balance lower than 1L (34.2%; p = 0.033). Mechanical ventilation duration and negative 48-hour postextubation fluid balance lower than one liter were associated with extubation failure when corrected for Simplified Acute Physiology Score 3 in multivariate analysis. When we evaluated the combined outcome, only negative 48-hour postextubation lower than 1L maintained an association when corrected for for Simplified Acute Physiology Score 3 and mechanical ventilation duration.
Conclusion:
The 48-hour postextubation fluid balance is associated with extubation failure. Further studies are necessary to assess whether avoiding positive fluid balance in this period might improve weaning outcomes.
Keywords:Airway extubationNoninvasive ventilationRespiration, artificialWater-electrolyte balanceWeaningSee moreViews1Abstract
Original ArticlePostextubation fluid balance is associated with extubation failure: a cohort study
Rev Bras Ter Intensiva. 2021;33(3):422-427
DOI 10.5935/0103-507X.20210057
- Priscila Albrecht dos Santos,
- Alexandre Ribas,
- Thiele Cabral Coelho Quadros ,
- Clarissa Netto Blattner,
- Márcio Manozzo Boniatti
Views1ABSTRACT
Objective:
To assess whether there is an association between 48-hour postextubation fluid balance and extubation failure.
Methods:
This was a prospective cohort study that included patients admitted to the intensive care unit of a tertiary hospital in southern Brazil from March 2019 to December 2019. Patients who required mechanical ventilation for at least 24 hours and who were extubated during the study period were included. The primary outcome was extubation failure, considered as the need for reintubation in the first 72 hours after extubation. The secondary outcome was a combined outcome with extubation failure or the need for therapeutic noninvasive ventilation.
Results:
A total of 101 patients were included. Extubation failure was observed in 29 (28.7%) patients. In univariate analysis, patients with a negative 48-hour postextubation fluid balance higher than one liter had a lower rate of extubation failure (12.0%) than patients with a negative 48-hour postextubation fluid balance lower than 1L (34.2%; p = 0.033). Mechanical ventilation duration and negative 48-hour postextubation fluid balance lower than one liter were associated with extubation failure when corrected for Simplified Acute Physiology Score 3 in multivariate analysis. When we evaluated the combined outcome, only negative 48-hour postextubation lower than 1L maintained an association when corrected for for Simplified Acute Physiology Score 3 and mechanical ventilation duration.
Conclusion:
The 48-hour postextubation fluid balance is associated with extubation failure. Further studies are necessary to assess whether avoiding positive fluid balance in this period might improve weaning outcomes.
Keywords:Airway extubationNoninvasive ventilationRespiration, artificialWater-electrolyte balanceWeaningSee more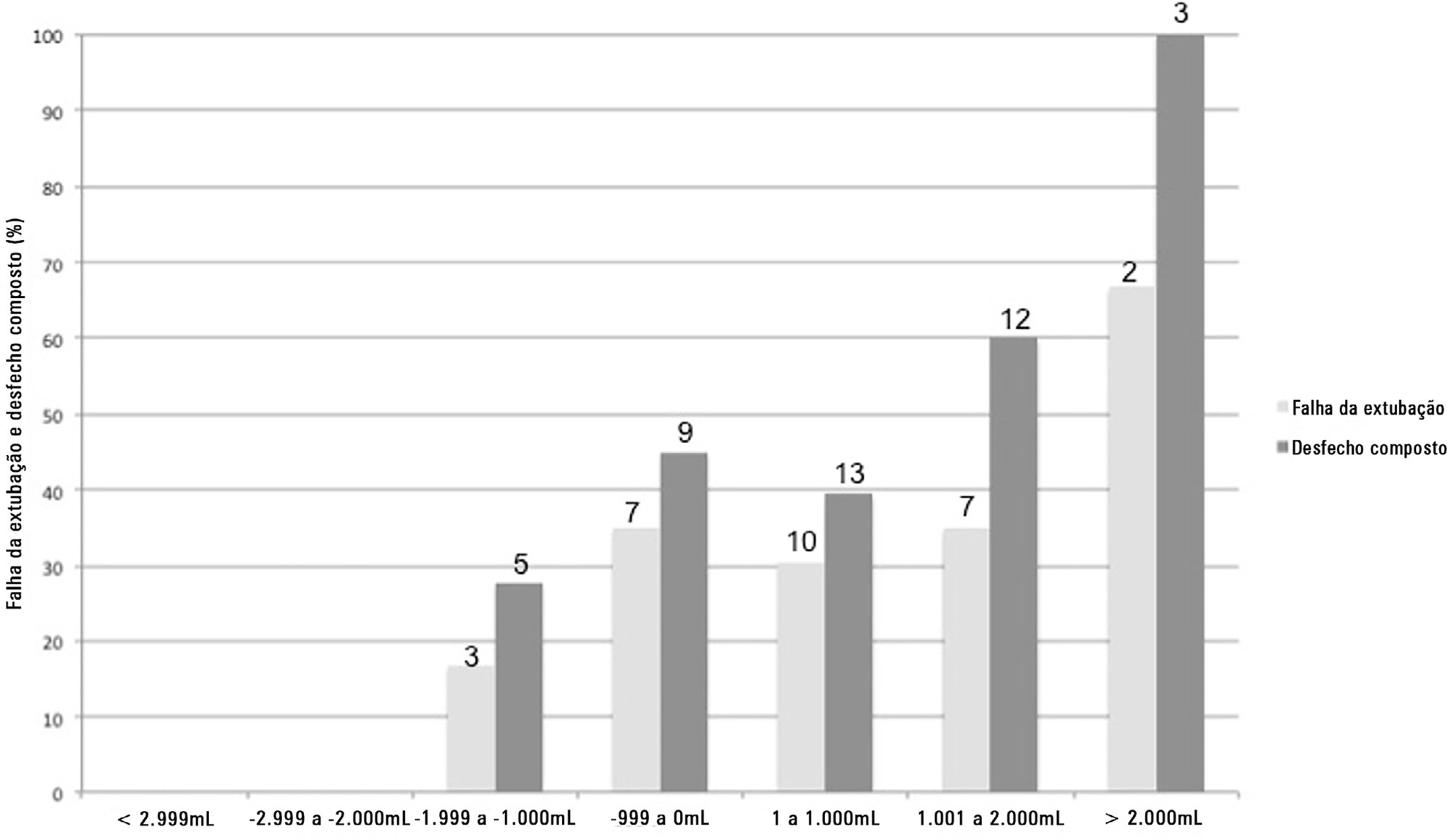
-
Original Article
A cost-effectiveness analysis of propofol versus midazolam for the sedation of adult patients admitted to the intensive care unit
- Teresa Raquel Andrade,
- Jorge Ibrain Figueira Salluh ,
- Raphaela Garcia,
- Daniela Farah,
- Paulo Sérgio Lucas da Silva, [ … ],
- Marcelo Cunio Machado Fonseca
Abstract
Original ArticleA cost-effectiveness analysis of propofol versus midazolam for the sedation of adult patients admitted to the intensive care unit
Rev Bras Ter Intensiva. 2021;33(3):428-433
DOI 10.5935/0103-507X.20210068
- Teresa Raquel Andrade,
- Jorge Ibrain Figueira Salluh ,
- Raphaela Garcia,
- Daniela Farah,
- Paulo Sérgio Lucas da Silva,
- Danielle F. Bastos,
- Marcelo Cunio Machado Fonseca
Views1ABSTRACT
Objective:
To build a cost-effectiveness model to compare the use of propofol versus midazolam in critically ill adult patients under mechanical ventilation.
Methods:
We built a decision tree model for critically ill patients submitted to mechanical ventilation and analyzed it from the Brazilian private health care system perspective. The time horizon was that of intensive care unit hospitalization. The outcomes were cost-effectiveness per hour of intensive care unit stay avoided and cost-effectiveness per hour of mechanical ventilation avoided. We retrieved data for the model from a previous meta-analysis. We assumed that the cost of medication was embedded in the intensive care unit cost. We conducted univariate and probabilistic sensitivity analyses.
Results:
Mechanically ventilated patients using propofol had their intensive care unit stay and the duration of mechanical ventilation decreased by 47.97 hours and 21.65 hours, respectively. There was an average cost reduction of US$ 2,998.971 for propofol when compared to midazolam. The cost-effectiveness per hour of intensive care unit stay and mechanical ventilation avoided were dominant 94.40% and 80.8% of the time, respectively.
Conclusion:
There was a significant reduction in costs associated with propofol use related to intensive care unit stay and duration of mechanical ventilation for critically ill adult patients.
Keywords:AdultartificialCost-effectivenessCritical illnessIntensive care unitsMidazolamPropofolRespirationSee moreViews1Abstract
Original ArticleA cost-effectiveness analysis of propofol versus midazolam for the sedation of adult patients admitted to the intensive care unit
Rev Bras Ter Intensiva. 2021;33(3):428-433
DOI 10.5935/0103-507X.20210068
- Teresa Raquel Andrade,
- Jorge Ibrain Figueira Salluh ,
- Raphaela Garcia,
- Daniela Farah,
- Paulo Sérgio Lucas da Silva,
- Danielle F. Bastos,
- Marcelo Cunio Machado Fonseca
Views1ABSTRACT
Objective:
To build a cost-effectiveness model to compare the use of propofol versus midazolam in critically ill adult patients under mechanical ventilation.
Methods:
We built a decision tree model for critically ill patients submitted to mechanical ventilation and analyzed it from the Brazilian private health care system perspective. The time horizon was that of intensive care unit hospitalization. The outcomes were cost-effectiveness per hour of intensive care unit stay avoided and cost-effectiveness per hour of mechanical ventilation avoided. We retrieved data for the model from a previous meta-analysis. We assumed that the cost of medication was embedded in the intensive care unit cost. We conducted univariate and probabilistic sensitivity analyses.
Results:
Mechanically ventilated patients using propofol had their intensive care unit stay and the duration of mechanical ventilation decreased by 47.97 hours and 21.65 hours, respectively. There was an average cost reduction of US$ 2,998.971 for propofol when compared to midazolam. The cost-effectiveness per hour of intensive care unit stay and mechanical ventilation avoided were dominant 94.40% and 80.8% of the time, respectively.
Conclusion:
There was a significant reduction in costs associated with propofol use related to intensive care unit stay and duration of mechanical ventilation for critically ill adult patients.
Keywords:AdultartificialCost-effectivenessCritical illnessIntensive care unitsMidazolamPropofolRespirationSee more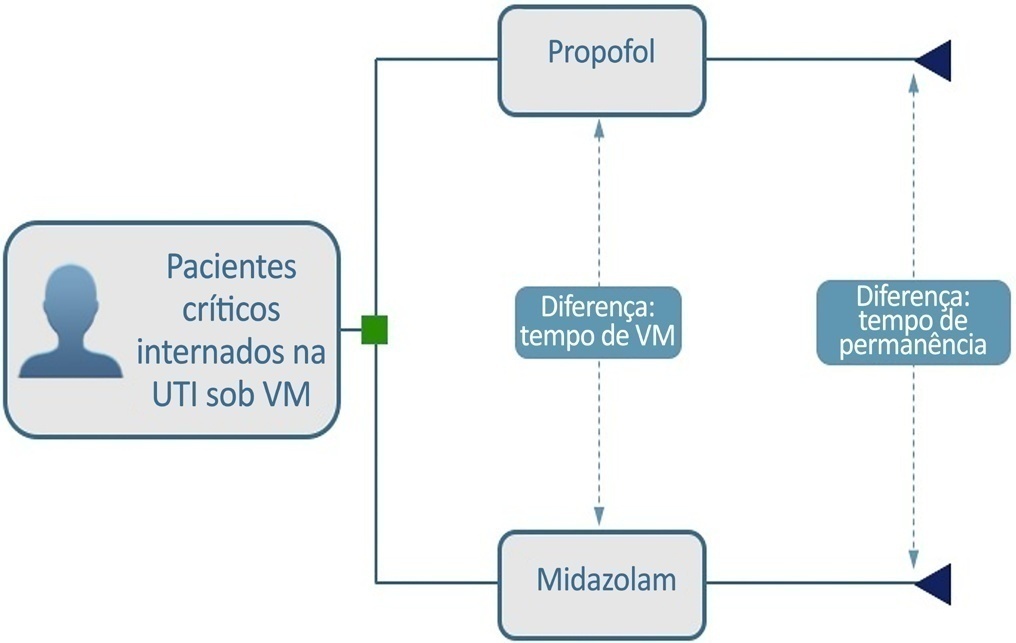
-
Original Article
Assessment of newborn pain during arterial puncture: an observational analytical study
- Rayanne Marques Costa Alberice ,
- Silvia Cristina Oliveira da Silva,
- Anna Caroline Costa Leite ,
- Bruna Figueiredo Manzo,
- Delma Aurélia da Silva Simão, [ … ],
- Juliana de Oliveira Marcatto
Abstract
Original ArticleAssessment of newborn pain during arterial puncture: an observational analytical study
Rev Bras Ter Intensiva. 2021;33(3):434-439
DOI 10.5935/0103-507X.20210058
- Rayanne Marques Costa Alberice ,
- Silvia Cristina Oliveira da Silva,
- Anna Caroline Costa Leite ,
- Bruna Figueiredo Manzo,
- Delma Aurélia da Silva Simão,
- Juliana de Oliveira Marcatto
Views0See moreABSTRACT
Objective:
To evaluate pain intensity during arterial puncture performed in newborns admitted to a neonatal progressive care unit and to evaluate the perception of health professionals regarding neonatal pain.
Methods:
This was an observational analytical study in which 62 arterial punctures were performed in 35 neonates. Pain was assessed during collection using the Premature Infant Pain Profile scale. The health professionals responsible for collection evaluated pain using a verbal numerical scale ranging from zero to ten. The data were subjected to descriptive statistical analysis using the Statistical Package for the Social Science software.
Results:
Among the newborns, 30.6% (n = 19) had no pain or mild pain (0 – 6), 24.2% (n = 15) had mild to moderate pain (7 – 11) and 45.2% (28) had severe pain (12 – 21). It was found that health professionals identified pain during the procedure.
Conclusion:
Arterial puncture is considered a painful procedure that can result in mild to severe pain. The adoption of systematic evaluation strategies is necessary to enable appropriate therapeutic intervention.
Views0Abstract
Original ArticleAssessment of newborn pain during arterial puncture: an observational analytical study
Rev Bras Ter Intensiva. 2021;33(3):434-439
DOI 10.5935/0103-507X.20210058
- Rayanne Marques Costa Alberice ,
- Silvia Cristina Oliveira da Silva,
- Anna Caroline Costa Leite ,
- Bruna Figueiredo Manzo,
- Delma Aurélia da Silva Simão,
- Juliana de Oliveira Marcatto
Views0See moreABSTRACT
Objective:
To evaluate pain intensity during arterial puncture performed in newborns admitted to a neonatal progressive care unit and to evaluate the perception of health professionals regarding neonatal pain.
Methods:
This was an observational analytical study in which 62 arterial punctures were performed in 35 neonates. Pain was assessed during collection using the Premature Infant Pain Profile scale. The health professionals responsible for collection evaluated pain using a verbal numerical scale ranging from zero to ten. The data were subjected to descriptive statistical analysis using the Statistical Package for the Social Science software.
Results:
Among the newborns, 30.6% (n = 19) had no pain or mild pain (0 – 6), 24.2% (n = 15) had mild to moderate pain (7 – 11) and 45.2% (28) had severe pain (12 – 21). It was found that health professionals identified pain during the procedure.
Conclusion:
Arterial puncture is considered a painful procedure that can result in mild to severe pain. The adoption of systematic evaluation strategies is necessary to enable appropriate therapeutic intervention.
- Rayanne Marques Costa Alberice
-
Review Article
Efficacy of topiramate as an add-on therapy in patients with refractory status epilepticus: a short systematic review
- Leonardo Christiaan Welling,
- Nícollas Nunes Rabelo,
- Marcia Harumy Yoshikawa,
- João Paulo Mota Telles ,
- Manoel Jacobsen Teixeira, [ … ],
- Eberval Gadelha Figueiredo
Abstract
Review ArticleEfficacy of topiramate as an add-on therapy in patients with refractory status epilepticus: a short systematic review
Rev Bras Ter Intensiva. 2021;33(3):440-444
DOI 10.5935/0103-507X.20210054
- Leonardo Christiaan Welling,
- Nícollas Nunes Rabelo,
- Marcia Harumy Yoshikawa,
- João Paulo Mota Telles ,
- Manoel Jacobsen Teixeira,
- Eberval Gadelha Figueiredo
Views0See moreABSTRACT
Objective:
To identify current evidence on the use of topiramate for refractory status epilepticus.
Methods:
We reviewed the literature to investigate the efficacy of topiramate in the treatment of refractory status epilepticus. The search terms used were “status epilepticus”, “refractory”, “treatment” and “topiramate”. No restrictions were used.
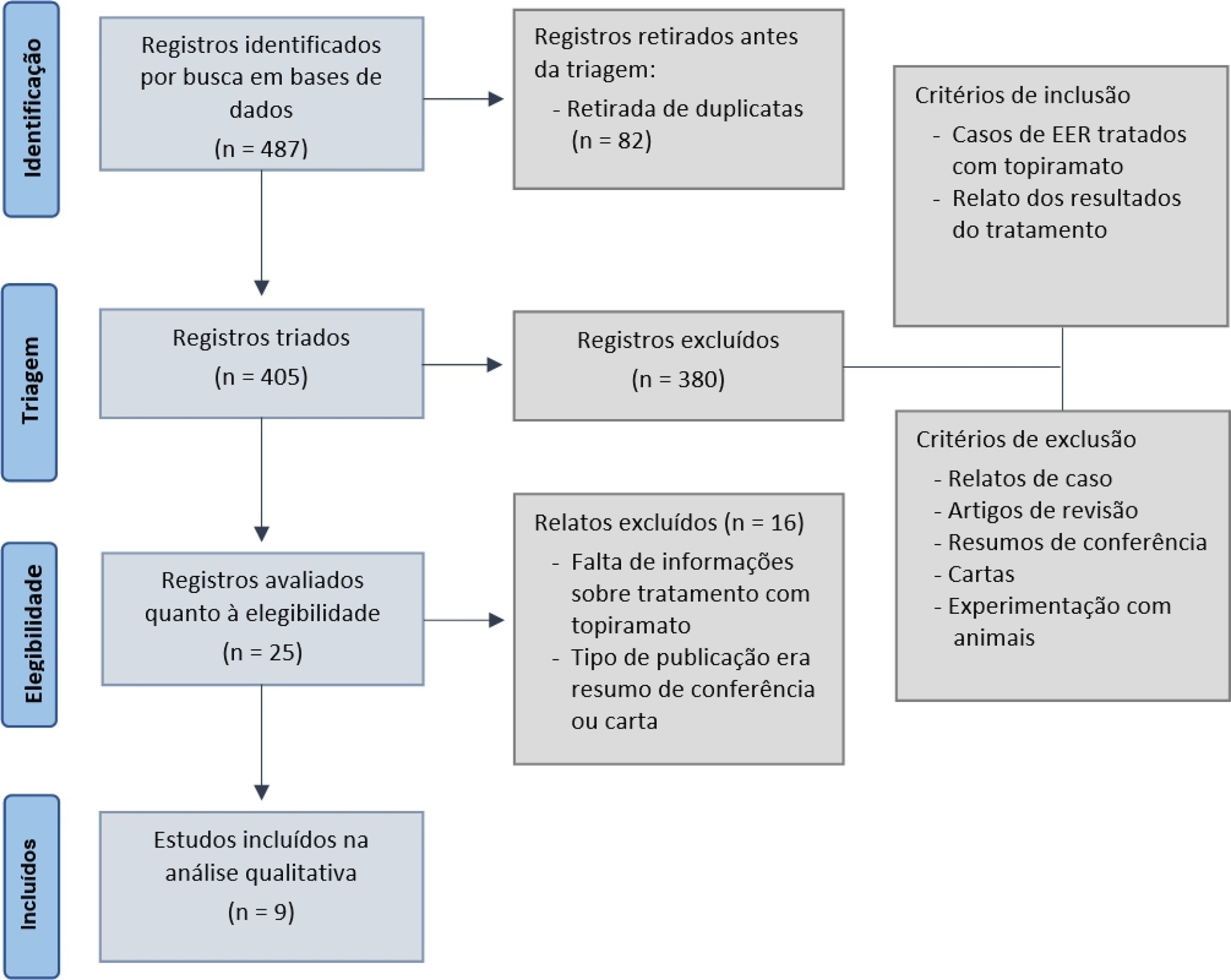
Results:
The search yielded 487 articles that reported using topiramate as a treatment for refractory status epilepticus and its outcomes. Case reports, review articles, and animal experiments were excluded. After excluding duplicates and applying inclusion and exclusion criteria, nine studies were included for analyses. Descriptive and qualitative analyses were performed, and the results were as follows: response rates (defined as termination in-hospital until 72 hours after the administration of topiramate) varied from 27% to 100%. The mortality rate varied from 5.9% to 68%. Positive functional long-term outcomes, defined as discharge, back to baseline or rehabilitation, were documented by seven studies, and the rates ranged between 4% and 55%. Most studies reported no or mild adverse effects.
Conclusion:
Topiramate was effective in terminating refractory status epilepticus, presented relatively low mortality and was well tolerated. Therefore, topiramate could be a good option as a third-line therapy for refractory status epilepticus, but further studies are necessary.
Views0Abstract
Review ArticleEfficacy of topiramate as an add-on therapy in patients with refractory status epilepticus: a short systematic review
Rev Bras Ter Intensiva. 2021;33(3):440-444
DOI 10.5935/0103-507X.20210054
- Leonardo Christiaan Welling,
- Nícollas Nunes Rabelo,
- Marcia Harumy Yoshikawa,
- João Paulo Mota Telles ,
- Manoel Jacobsen Teixeira,
- Eberval Gadelha Figueiredo
Views0See moreABSTRACT
Objective:
To identify current evidence on the use of topiramate for refractory status epilepticus.
Methods:
We reviewed the literature to investigate the efficacy of topiramate in the treatment of refractory status epilepticus. The search terms used were “status epilepticus”, “refractory”, “treatment” and “topiramate”. No restrictions were used.
Results:
The search yielded 487 articles that reported using topiramate as a treatment for refractory status epilepticus and its outcomes. Case reports, review articles, and animal experiments were excluded. After excluding duplicates and applying inclusion and exclusion criteria, nine studies were included for analyses. Descriptive and qualitative analyses were performed, and the results were as follows: response rates (defined as termination in-hospital until 72 hours after the administration of topiramate) varied from 27% to 100%. The mortality rate varied from 5.9% to 68%. Positive functional long-term outcomes, defined as discharge, back to baseline or rehabilitation, were documented by seven studies, and the rates ranged between 4% and 55%. Most studies reported no or mild adverse effects.
Conclusion:
Topiramate was effective in terminating refractory status epilepticus, presented relatively low mortality and was well tolerated. Therefore, topiramate could be a good option as a third-line therapy for refractory status epilepticus, but further studies are necessary.
-
Review Article
Cough peak flow to predict extubation outcome: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2021;33(3):445-456
Abstract
Review ArticleCough peak flow to predict extubation outcome: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2021;33(3):445-456
DOI 10.5935/0103-507X.20210060
Views0See moreAbstract
Objective:
This systematic review was designed to assess the usefulness of cough peak flow to predict the extubation outcome in subjects who passed a spontaneous breathing trial.
Methods:
The search covered the scientific databases MEDLINE, Lilacs, Ibecs, Cinahl, SciELO, Cochrane, Scopus, Web of Science and gray literature. The Quality Assessment of Diagnostic Accuracy Studies was used to assess the methodological quality and risk of study bias. The statistical heterogeneity of the likelihood (LR) and diagnostic odds ratios were evaluated using forest plots and Cochran’s Q statistic, and a crosshair summary Receiver Operating Characteristic plot using the multiple cutoffs model was calculated.
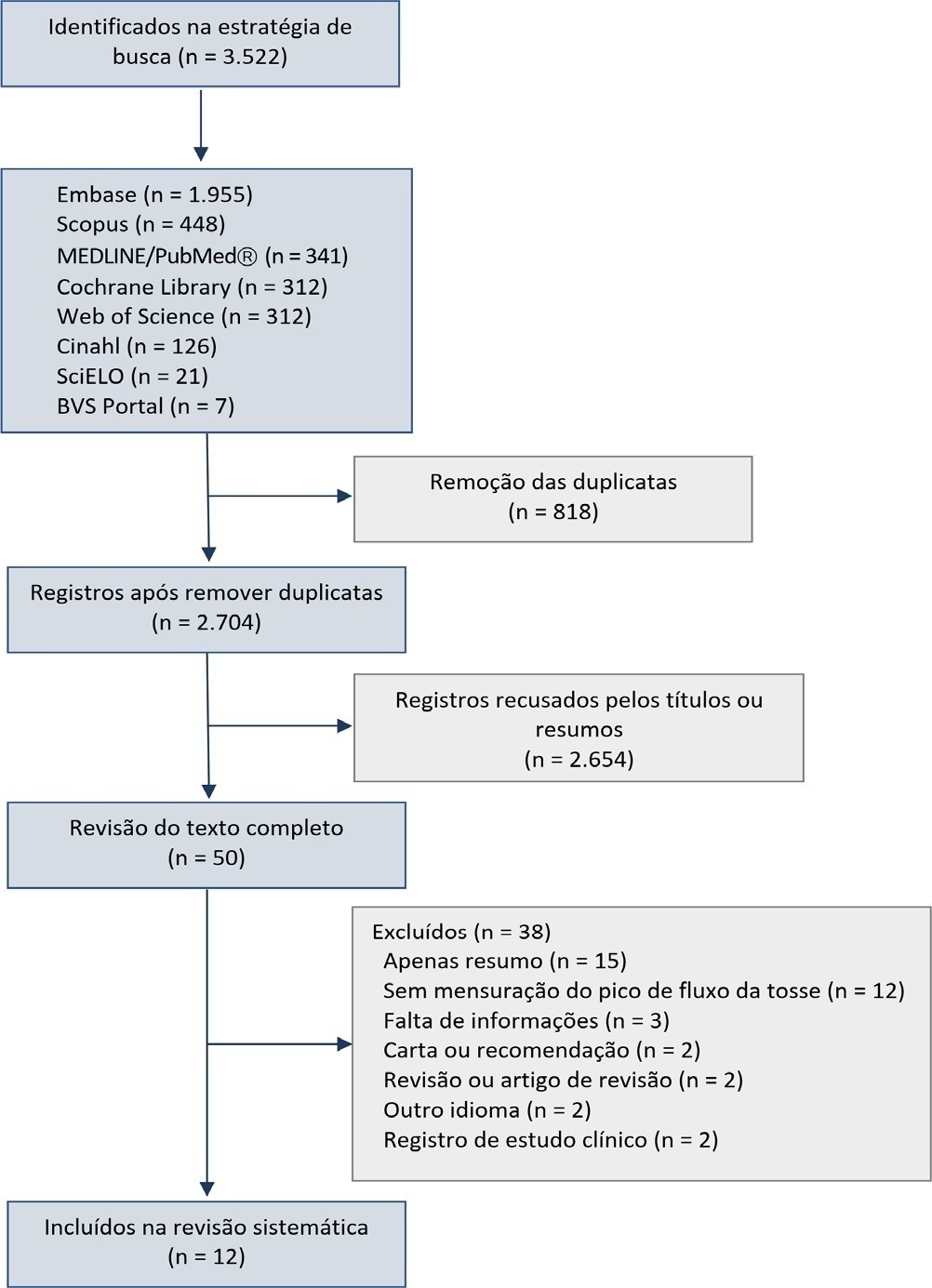
Results:
We initially retrieved 3,522 references from the databases; among these, 12 studies including 1,757 subjects were selected for the qualitative analysis. Many studies presented an unclear risk of bias in the “patient selection” and “flow and time” criteria. Among the 12 included studies, seven presented “high risk” and five “unclear risk” for the item “reference standard.” The diagnostic performance of the cough peak flow for the extubation outcome was low to moderate when we considered the results from all included studies, with a +LR of 1.360 (95%CI 1.240 – 1.530), -LR of 0.218 (95%CI 0.159 – 0.293) and a diagnostic odds ratio of 6.450 (95%CI 4.490 – 9.090). A subgroup analysis including only the studies with a cutoff between 55 and 65 L/minute showed a slightly better, although still moderate, performance.
Conclusion:
A cough peak flow assessment considering a cutoff between 55 and 65L/minute may be useful as a complementary measurement prior to extubation. Additional well-designed studies are necessary to identify the best method and equipment to record the cough peak flow as well as the best cutoff.
Views0Abstract
Review ArticleCough peak flow to predict extubation outcome: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2021;33(3):445-456
DOI 10.5935/0103-507X.20210060
Views0See moreAbstract
Objective:
This systematic review was designed to assess the usefulness of cough peak flow to predict the extubation outcome in subjects who passed a spontaneous breathing trial.
Methods:
The search covered the scientific databases MEDLINE, Lilacs, Ibecs, Cinahl, SciELO, Cochrane, Scopus, Web of Science and gray literature. The Quality Assessment of Diagnostic Accuracy Studies was used to assess the methodological quality and risk of study bias. The statistical heterogeneity of the likelihood (LR) and diagnostic odds ratios were evaluated using forest plots and Cochran’s Q statistic, and a crosshair summary Receiver Operating Characteristic plot using the multiple cutoffs model was calculated.
Results:
We initially retrieved 3,522 references from the databases; among these, 12 studies including 1,757 subjects were selected for the qualitative analysis. Many studies presented an unclear risk of bias in the “patient selection” and “flow and time” criteria. Among the 12 included studies, seven presented “high risk” and five “unclear risk” for the item “reference standard.” The diagnostic performance of the cough peak flow for the extubation outcome was low to moderate when we considered the results from all included studies, with a +LR of 1.360 (95%CI 1.240 – 1.530), -LR of 0.218 (95%CI 0.159 – 0.293) and a diagnostic odds ratio of 6.450 (95%CI 4.490 – 9.090). A subgroup analysis including only the studies with a cutoff between 55 and 65 L/minute showed a slightly better, although still moderate, performance.
Conclusion:
A cough peak flow assessment considering a cutoff between 55 and 65L/minute may be useful as a complementary measurement prior to extubation. Additional well-designed studies are necessary to identify the best method and equipment to record the cough peak flow as well as the best cutoff.
-
Case Report
Posterior reversible encephalopathy syndrome in a patient submitted to extracorporeal membrane oxygenation for COVID-19
Rev Bras Ter Intensiva. 2021;33(3):457-460
Abstract
Case ReportPosterior reversible encephalopathy syndrome in a patient submitted to extracorporeal membrane oxygenation for COVID-19
Rev Bras Ter Intensiva. 2021;33(3):457-460
DOI 10.5935/0103-507X.20210067
Views0ABSTRACT
A 63-year-old woman presented to the emergency department with an acute history of fever, prostration and dyspnea. She was diagnosed with severe COVID-19 acute respiratory distress syndrome and, despite optimized critical care support, met the indications for veno-venous extracorporeal membrane oxygenation. On day 34, after 7 days of wean sedation with a positive evolution of neurologic status, she presented a limited generalized tonic-clonic seizure not related to hydroelectrolytic or metabolic imbalance, which led to a diagnostic investigation; her brain imaging tests showed a posterior reversible encephalopathy syndrome. This case emphasizes the issue of neurological complications in patients with severe COVID-19 infection and the importance of early diagnosis and support.
Keywords:Acute distress syndromeBrain diseasesCoronavirus infectionsCOVID-19Extracorporeal membrane oxygenationNeurologic manifestationsSee moreViews0Abstract
Case ReportPosterior reversible encephalopathy syndrome in a patient submitted to extracorporeal membrane oxygenation for COVID-19
Rev Bras Ter Intensiva. 2021;33(3):457-460
DOI 10.5935/0103-507X.20210067
Views0ABSTRACT
A 63-year-old woman presented to the emergency department with an acute history of fever, prostration and dyspnea. She was diagnosed with severe COVID-19 acute respiratory distress syndrome and, despite optimized critical care support, met the indications for veno-venous extracorporeal membrane oxygenation. On day 34, after 7 days of wean sedation with a positive evolution of neurologic status, she presented a limited generalized tonic-clonic seizure not related to hydroelectrolytic or metabolic imbalance, which led to a diagnostic investigation; her brain imaging tests showed a posterior reversible encephalopathy syndrome. This case emphasizes the issue of neurological complications in patients with severe COVID-19 infection and the importance of early diagnosis and support.
Keywords:Acute distress syndromeBrain diseasesCoronavirus infectionsCOVID-19Extracorporeal membrane oxygenationNeurologic manifestationsSee more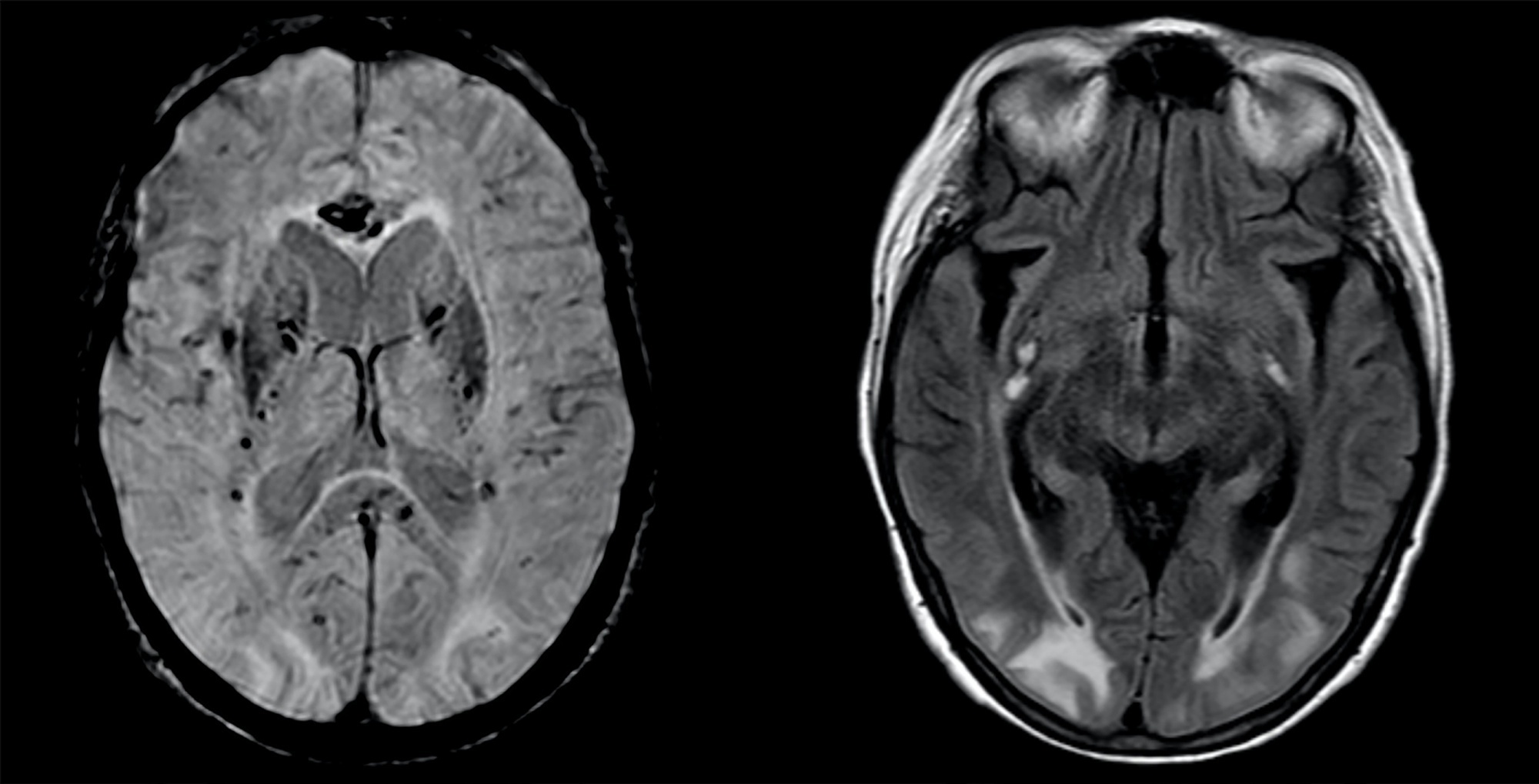
-
Case Report
Self-inflicted lung injury: is it possible to identify the risk? A case report
Rev Bras Ter Intensiva. 2021;33(3):461-468
Abstract
Case ReportSelf-inflicted lung injury: is it possible to identify the risk? A case report
Rev Bras Ter Intensiva. 2021;33(3):461-468
DOI 10.5935/0103-507X.20210061
Views0ABSTRACT
Spontaneous breathing can be deleterious in patients with previously injured lungs, especially in acute respiratory distress syndrome. Moreover, the failure to assume spontaneous breathing during mechanical ventilation and the need to switch back to controlled mechanical ventilation are associated with higher mortality. There is a gap of knowledge regarding which parameters might be useful to predict the risk of patient self-inflicted lung injury and to detect the inability to assume spontaneous breathing. We report a case of patient self-inflicted lung injury, the corresponding basic and advanced monitoring of the respiratory system mechanics and physiological and clinical results related to spontaneous breathing. The patient was a 33-year-old Caucasian man with a medical history of AIDS who developed acute respiratory distress syndrome and needed invasive mechanical ventilation after noninvasive ventilatory support failure. During the controlled ventilation periods, a protective ventilation strategy was adopted, and the patient showed clear clinical and radiographic improvement. However, during each spontaneous breathing period under pressure support ventilation, despite adequate initial parameters and a strictly adjusted ventilatory setting and monitoring, the patient developed progressive hypoxemia and worsening of respiratory system mechanics with a clearly correlated radiographic deterioration (patient self-inflicted lung injury). After failing three spontaneous breathing assumption trials, he died on day 29 due to refractory hypoxemia. Conventional basic and advanced monitoring variables in this case were not sufficient to identify the aptitude to breathe spontaneously or to predict the risk and development of patient self-inflicted lung injury during partial support ventilation.
Keywords:artificialInteractive ventilatory supportmonitoringRespirationRespiratory distress syndromeVentilator-induced lung injurySee moreViews0Abstract
Case ReportSelf-inflicted lung injury: is it possible to identify the risk? A case report
Rev Bras Ter Intensiva. 2021;33(3):461-468
DOI 10.5935/0103-507X.20210061
Views0ABSTRACT
Spontaneous breathing can be deleterious in patients with previously injured lungs, especially in acute respiratory distress syndrome. Moreover, the failure to assume spontaneous breathing during mechanical ventilation and the need to switch back to controlled mechanical ventilation are associated with higher mortality. There is a gap of knowledge regarding which parameters might be useful to predict the risk of patient self-inflicted lung injury and to detect the inability to assume spontaneous breathing. We report a case of patient self-inflicted lung injury, the corresponding basic and advanced monitoring of the respiratory system mechanics and physiological and clinical results related to spontaneous breathing. The patient was a 33-year-old Caucasian man with a medical history of AIDS who developed acute respiratory distress syndrome and needed invasive mechanical ventilation after noninvasive ventilatory support failure. During the controlled ventilation periods, a protective ventilation strategy was adopted, and the patient showed clear clinical and radiographic improvement. However, during each spontaneous breathing period under pressure support ventilation, despite adequate initial parameters and a strictly adjusted ventilatory setting and monitoring, the patient developed progressive hypoxemia and worsening of respiratory system mechanics with a clearly correlated radiographic deterioration (patient self-inflicted lung injury). After failing three spontaneous breathing assumption trials, he died on day 29 due to refractory hypoxemia. Conventional basic and advanced monitoring variables in this case were not sufficient to identify the aptitude to breathe spontaneously or to predict the risk and development of patient self-inflicted lung injury during partial support ventilation.
Keywords:artificialInteractive ventilatory supportmonitoringRespirationRespiratory distress syndromeVentilator-induced lung injurySee more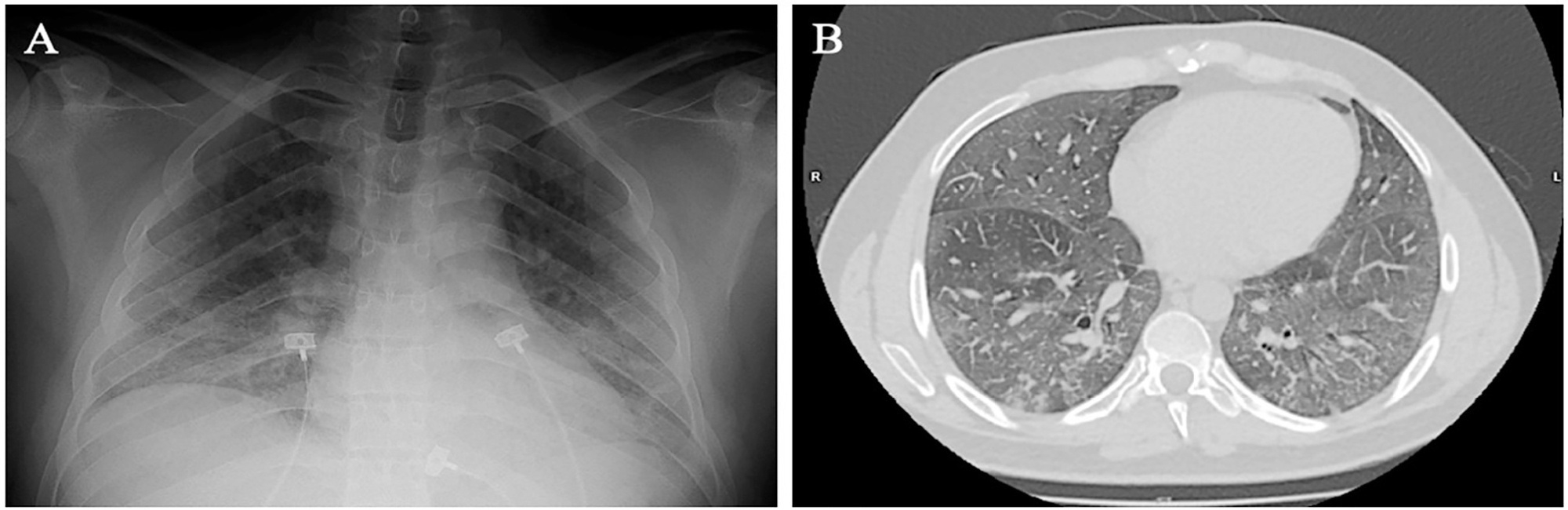
-
Case Report
The use of a noninvasive intracranial pressure monitoring method in the intensive care unit to improve neuroprotection in postoperative cardiac surgery patients after extracorporeal circulation
- Salomón Soriano Ordinola Rojas ,
- Amanda Ayako Minemura Ordinola,
- Viviane Cordeiro Veiga ,
- Januário Manoel de Souza
Abstract
Case ReportThe use of a noninvasive intracranial pressure monitoring method in the intensive care unit to improve neuroprotection in postoperative cardiac surgery patients after extracorporeal circulation
Rev Bras Ter Intensiva. 2021;33(3):469-476
DOI 10.5935/0103-507X.20210066
- Salomón Soriano Ordinola Rojas ,
- Amanda Ayako Minemura Ordinola,
- Viviane Cordeiro Veiga ,
- Januário Manoel de Souza
Views0ABSTRACT
Brain injury caused by extracorporeal circulation during cardiovascular surgical procedures has been a recurring complication since the implementation of extracorporeal circulation five decades ago. There is no unique cause of brain injury due to the use of extracorporeal circulation, but it is known that brain injury affects about 70% of patients who undergo this procedure. Intracranial pressure assessment is one method that can guide the management of patients undergoing procedures associated with neurological disturbances. This study describes two cases of patients who underwent cardiovascular surgery with extracorporeal circulation in whom clinical protocols for neuroprotection in the postoperative phase were guided by intracranial pressure waveform findings obtained with a novel noninvasive intracranial pressure monitoring method.
Keywords:Brain injuriesCardiovascular surgical proceduresCritical careExtracorporeal circulationIntracranial pressureNeuroprotectionSee moreViews0Abstract
Case ReportThe use of a noninvasive intracranial pressure monitoring method in the intensive care unit to improve neuroprotection in postoperative cardiac surgery patients after extracorporeal circulation
Rev Bras Ter Intensiva. 2021;33(3):469-476
DOI 10.5935/0103-507X.20210066
- Salomón Soriano Ordinola Rojas ,
- Amanda Ayako Minemura Ordinola,
- Viviane Cordeiro Veiga ,
- Januário Manoel de Souza
Views0ABSTRACT
Brain injury caused by extracorporeal circulation during cardiovascular surgical procedures has been a recurring complication since the implementation of extracorporeal circulation five decades ago. There is no unique cause of brain injury due to the use of extracorporeal circulation, but it is known that brain injury affects about 70% of patients who undergo this procedure. Intracranial pressure assessment is one method that can guide the management of patients undergoing procedures associated with neurological disturbances. This study describes two cases of patients who underwent cardiovascular surgery with extracorporeal circulation in whom clinical protocols for neuroprotection in the postoperative phase were guided by intracranial pressure waveform findings obtained with a novel noninvasive intracranial pressure monitoring method.
Keywords:Brain injuriesCardiovascular surgical proceduresCritical careExtracorporeal circulationIntracranial pressureNeuroprotectionSee more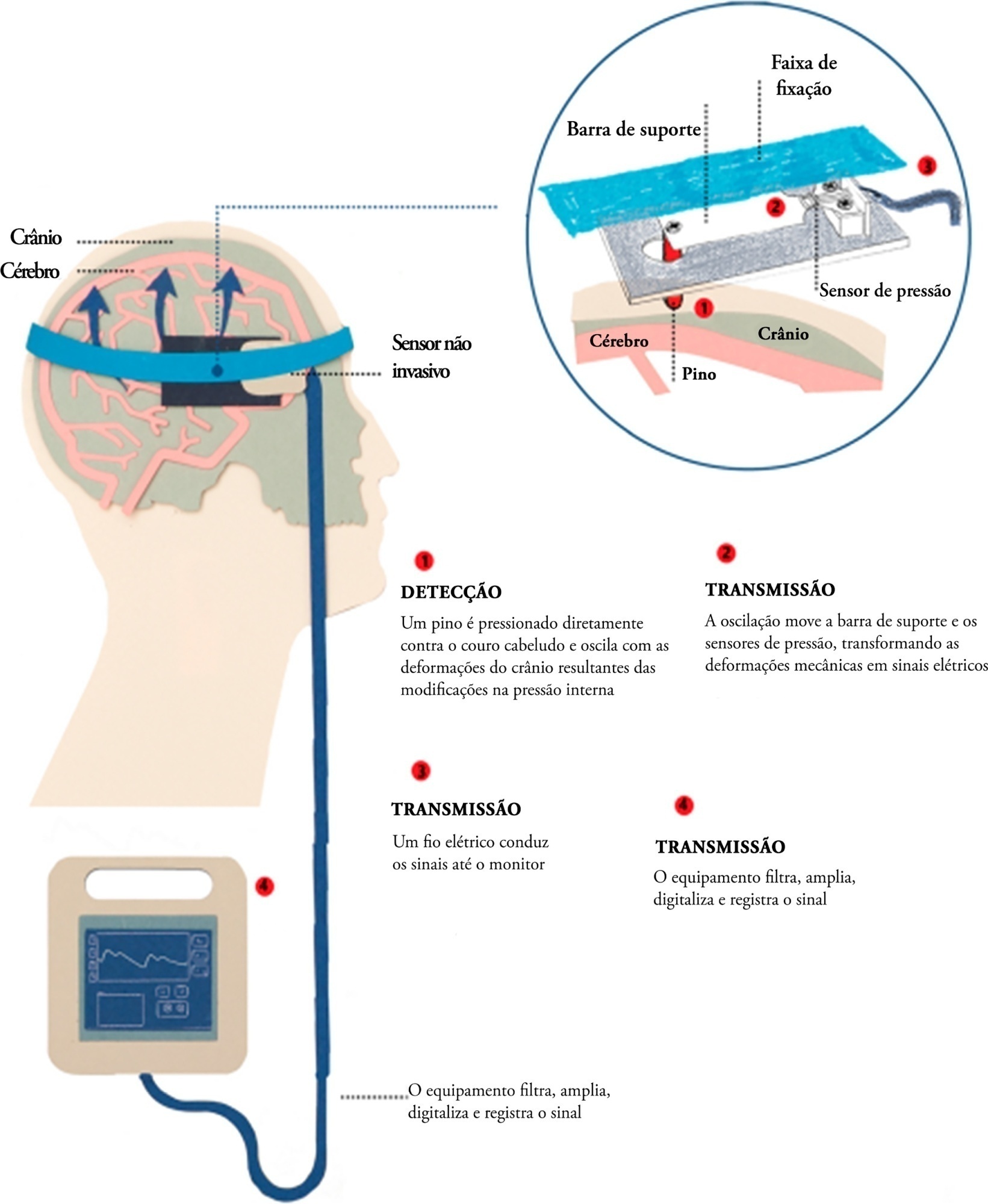
- Salomón Soriano Ordinola Rojas
-
Letter to the Editor
Perception of professionals in critical patient units about brain death
Rev Bras Ter Intensiva. 2021;33(3):477-479
Abstract
Letter to the EditorPerception of professionals in critical patient units about brain death
Rev Bras Ter Intensiva. 2021;33(3):477-479
DOI 10.5935/0103-507X.20210063
Views0To the Editor The health teams in critical patient units (intensive care units, emergency services and units with critically ill patients) experience the initial process of organ donation in their hospital routines. In these units, patients with clinical signs of brain death (BD) are diagnosed and approved or not for donation, depending on the wishes […]See moreViews0Abstract
Letter to the EditorPerception of professionals in critical patient units about brain death
Rev Bras Ter Intensiva. 2021;33(3):477-479
DOI 10.5935/0103-507X.20210063
Views0To the Editor The health teams in critical patient units (intensive care units, emergency services and units with critically ill patients) experience the initial process of organ donation in their hospital routines. In these units, patients with clinical signs of brain death (BD) are diagnosed and approved or not for donation, depending on the wishes […]See more
Volume Articles - Critical Care Science (CCS)
