-
Commentary
Prediction of intensive care units length of stay: a concise review
- Igor Tona Peres
 ,
, - Silvio Hamacher,
- Fernando Luiz Cyrino Oliveira ,
- Fernando Augusto Bozza,
- Jorge Ibrain Figueira Salluh
Abstract
CommentaryPrediction of intensive care units length of stay: a concise review
Rev Bras Ter Intensiva. 2021;33(2):183-187
DOI 10.5935/0103-507X.20210025
- Igor Tona Peres ,
- Silvio Hamacher,
- Fernando Luiz Cyrino Oliveira ,
- Fernando Augusto Bozza,
- Jorge Ibrain Figueira Salluh
Views2INTRODUCTION The length of stay (LOS) in the intensive care unit (ICU) is one of the most commonly used metrics for quality of care. Despite its potential limitations, ICU LOS is easy to measure, reproducible and can be used as a proxy for resource use, costs, and efficiency.() Moreover, it is a patient-centered outcome; therefore, […]See moreViews2

Abstract
CommentaryPrediction of intensive care units length of stay: a concise review
Rev Bras Ter Intensiva. 2021;33(2):183-187
DOI 10.5935/0103-507X.20210025
- Igor Tona Peres ,
- Silvio Hamacher,
- Fernando Luiz Cyrino Oliveira ,
- Fernando Augusto Bozza,
- Jorge Ibrain Figueira Salluh
Views2INTRODUCTIONThe length of stay (LOS) in the intensive care unit (ICU) is one of the most commonly used metrics for quality of care. Despite its potential limitations, ICU LOS is easy to measure, reproducible and can be used as a proxy for resource use, costs, and efficiency.() Moreover, it is a patient-centered outcome; therefore, it […]See more
- Igor Tona Peres
-
Original Article
Description of physical rehabilitation in intensive care units in Argentina: usual practice and during the COVID-19 pandemic. Online survey
Rev Bras Ter Intensiva. 2021;33(2):188-195
Abstract
Original ArticleDescription of physical rehabilitation in intensive care units in Argentina: usual practice and during the COVID-19 pandemic. Online survey
Rev Bras Ter Intensiva. 2021;33(2):188-195
DOI 10.5935/0103-507X.20210026
Views0Abstract
Objective:
To describe the usual practice of mobility therapy in the adult intensive care unit for patients with and without COVID-19.
Methods:
Online survey in which physical therapists working in an adult intensive care unit in Argentina participated. Sixteen multiple-choice or single-response questions grouped into three sections were asked. The first section addressed personal, professional and work environment data. The second section presented questions regarding usual care, and the third focused on practices under COVID-19 pandemic conditions.
Results:
Of 351 physical therapists, 76.1% answer that they were exclusively responsible for patient mobility. The highest motor-based goal varied according to four patient scenarios: Mechanically ventilated patients, patients weaned from mechanical ventilation, patients who had never required mechanical ventilation, and patients with COVID-19 under mechanical ventilation. In the first and last scenarios, the highest goal was to optimize muscle strength, while for the other two, it was to perform activities of daily living. Finally, the greatest limitation in working with patients with COVID-19 was respiratory and/or contact isolation.
Conclusion:
Physical therapists in Argentina reported being responsible for the mobility of patients in the intensive care unit. The highest motor-based therapeutic goals for four classic scenarios in the closed area were limited by the need for mechanical ventilation. The greatest limitation when mobilizing patients with COVID-19 was respiratory and contact isolation.
Keywords:Critical careEarly mobilizationPhysical therapy modalitiesRehabilitationRespiration, artificialSurvey and questionnairesSee moreViews0Abstract
Original ArticleDescription of physical rehabilitation in intensive care units in Argentina: usual practice and during the COVID-19 pandemic. Online survey
Rev Bras Ter Intensiva. 2021;33(2):188-195
DOI 10.5935/0103-507X.20210026
Views0Abstract
Objective:
To describe the usual practice of mobility therapy in the adult intensive care unit for patients with and without COVID-19.
Methods:
Online survey in which physical therapists working in an adult intensive care unit in Argentina participated. Sixteen multiple-choice or single-response questions grouped into three sections were asked. The first section addressed personal, professional and work environment data. The second section presented questions regarding usual care, and the third focused on practices under COVID-19 pandemic conditions.
Results:
Of 351 physical therapists, 76.1% answer that they were exclusively responsible for patient mobility. The highest motor-based goal varied according to four patient scenarios: Mechanically ventilated patients, patients weaned from mechanical ventilation, patients who had never required mechanical ventilation, and patients with COVID-19 under mechanical ventilation. In the first and last scenarios, the highest goal was to optimize muscle strength, while for the other two, it was to perform activities of daily living. Finally, the greatest limitation in working with patients with COVID-19 was respiratory and/or contact isolation.
Conclusion:
Physical therapists in Argentina reported being responsible for the mobility of patients in the intensive care unit. The highest motor-based therapeutic goals for four classic scenarios in the closed area were limited by the need for mechanical ventilation. The greatest limitation when mobilizing patients with COVID-19 was respiratory and contact isolation.
Keywords:Critical careEarly mobilizationPhysical therapy modalitiesRehabilitationRespiration, artificialSurvey and questionnairesSee more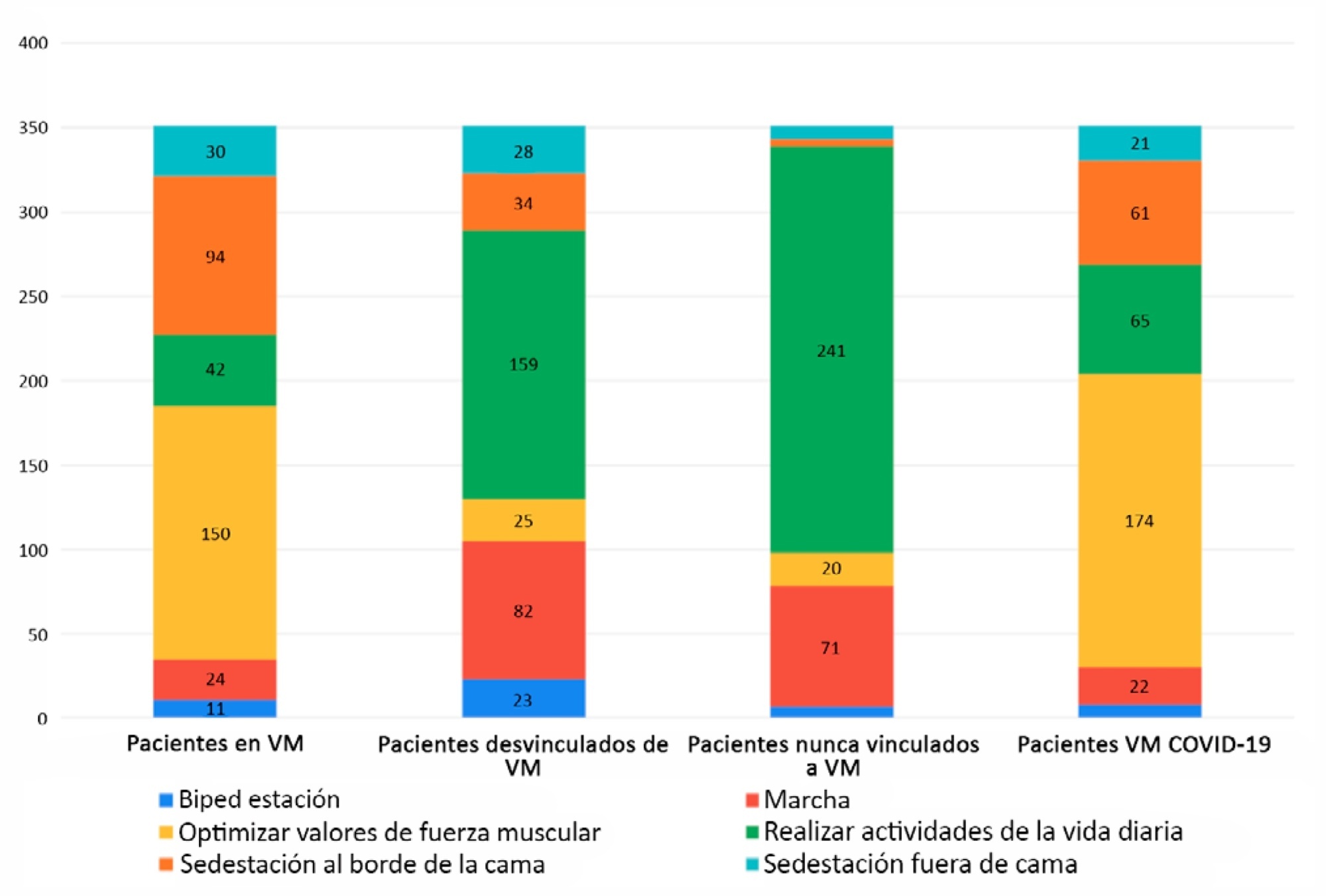
-
Original Article
Bedside clinical data subphenotypes of critically ill COVID-19 patients: a cohort study
- Raul dos Reis Ururahy ,
- César Albuquerque Gallo,
- Bruno Adler Maccagnan Pinheiro Besen,
- Marcelo Ticianelli de Carvalho,
- José Mauro Ribeiro, [ … ],
- Marcelo Park
Abstract
Original ArticleBedside clinical data subphenotypes of critically ill COVID-19 patients: a cohort study
Rev Bras Ter Intensiva. 2021;33(2):196-205
DOI 10.5935/0103-507X.20210027
- Raul dos Reis Ururahy ,
- César Albuquerque Gallo,
- Bruno Adler Maccagnan Pinheiro Besen,
- Marcelo Ticianelli de Carvalho,
- José Mauro Ribeiro,
- Rogério Zigaib,
- Pedro Vitale Mendes ,
- Marcelo Park
Views0See moreAbstract
Objective:
To identify more severe COVID-19 presentations.
Methods:
Consecutive intensive care unit-admitted patients were subjected to a stepwise clustering method.
Results:
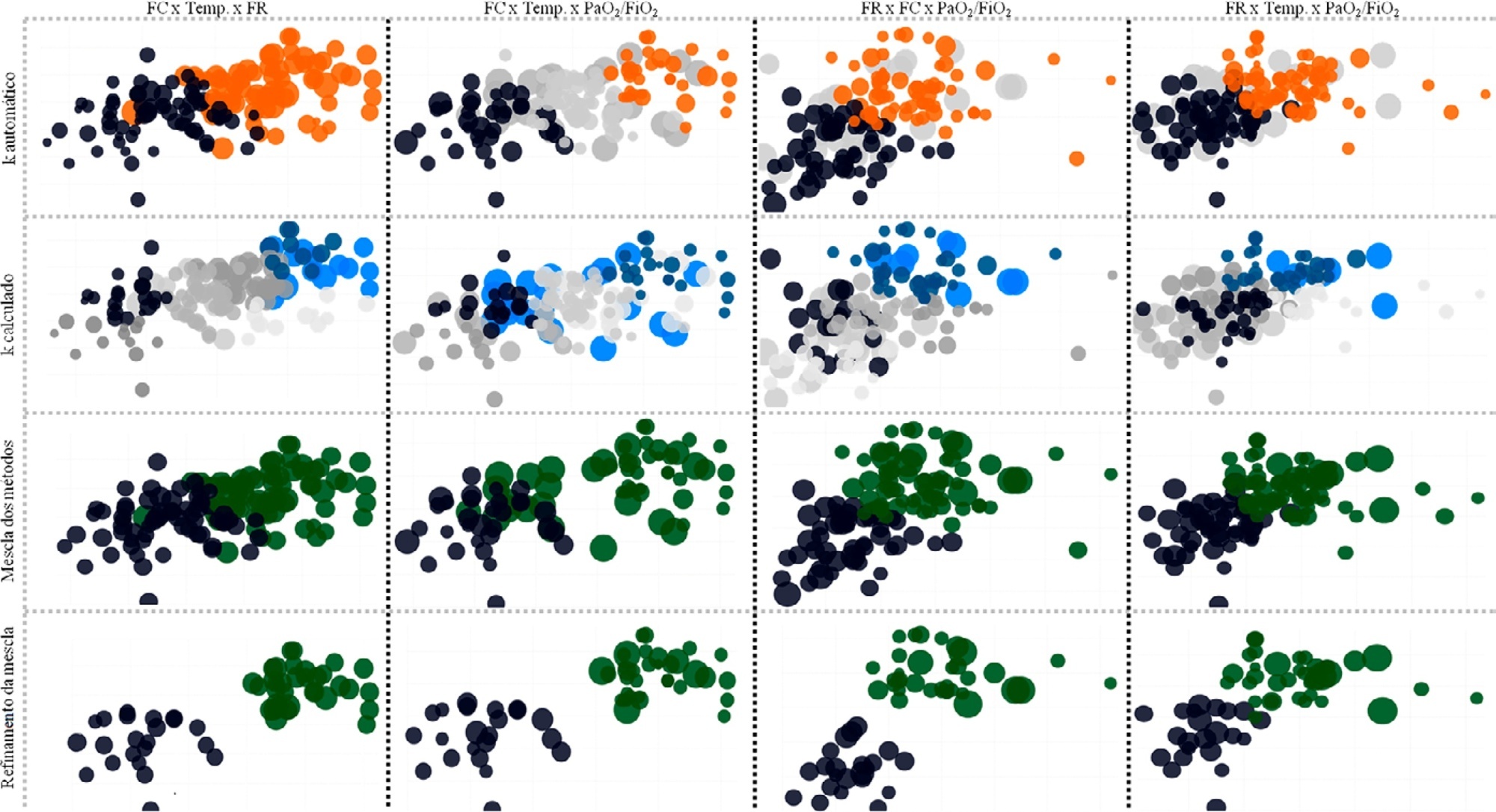
Data from 147 patients who were on average 56 ± 16 years old with a Simplified Acute Physiological Score 3 of 72 ± 18, of which 103 (70%) needed mechanical ventilation and 46 (31%) died in the intensive care unit, were analyzed. From the clustering algorithm, two well-defined groups were found based on maximal heart rate [Cluster A: 104 (95%CI 99 – 109) beats per minute versus Cluster B: 159 (95%CI 155 – 163) beats per minute], maximal respiratory rate [Cluster A: 33 (95%CI 31 – 35) breaths per minute versus Cluster B: 50 (95%CI 47 – 53) breaths per minute], and maximal body temperature [Cluster A: 37.4 (95%CI 37.1 – 37.7)°C versus Cluster B: 39.3 (95%CI 39.1 – 39.5)°C] during the intensive care unit stay, as well as the oxygen partial pressure in the blood over the oxygen inspiratory fraction at intensive care unit admission [Cluster A: 116 (95%CI 99 – 133) mmHg versus Cluster B: 78 (95%CI 63 – 93) mmHg]. Subphenotypes were distinct in inflammation profiles, organ dysfunction, organ support, intensive care unit length of stay, and intensive care unit mortality (with a ratio of 4.2 between the groups).
Conclusion:
Our findings, based on common clinical data, revealed two distinct subphenotypes with different disease courses. These results could help health professionals allocate resources and select patients for testing novel therapies.
Views0Abstract
Original ArticleBedside clinical data subphenotypes of critically ill COVID-19 patients: a cohort study
Rev Bras Ter Intensiva. 2021;33(2):196-205
DOI 10.5935/0103-507X.20210027
- Raul dos Reis Ururahy ,
- César Albuquerque Gallo,
- Bruno Adler Maccagnan Pinheiro Besen,
- Marcelo Ticianelli de Carvalho,
- José Mauro Ribeiro,
- Rogério Zigaib,
- Pedro Vitale Mendes ,
- Marcelo Park
Views0See moreAbstract
Objective:
To identify more severe COVID-19 presentations.
Methods:
Consecutive intensive care unit-admitted patients were subjected to a stepwise clustering method.
Results:
Data from 147 patients who were on average 56 ± 16 years old with a Simplified Acute Physiological Score 3 of 72 ± 18, of which 103 (70%) needed mechanical ventilation and 46 (31%) died in the intensive care unit, were analyzed. From the clustering algorithm, two well-defined groups were found based on maximal heart rate [Cluster A: 104 (95%CI 99 – 109) beats per minute versus Cluster B: 159 (95%CI 155 – 163) beats per minute], maximal respiratory rate [Cluster A: 33 (95%CI 31 – 35) breaths per minute versus Cluster B: 50 (95%CI 47 – 53) breaths per minute], and maximal body temperature [Cluster A: 37.4 (95%CI 37.1 – 37.7)°C versus Cluster B: 39.3 (95%CI 39.1 – 39.5)°C] during the intensive care unit stay, as well as the oxygen partial pressure in the blood over the oxygen inspiratory fraction at intensive care unit admission [Cluster A: 116 (95%CI 99 – 133) mmHg versus Cluster B: 78 (95%CI 63 – 93) mmHg]. Subphenotypes were distinct in inflammation profiles, organ dysfunction, organ support, intensive care unit length of stay, and intensive care unit mortality (with a ratio of 4.2 between the groups).
Conclusion:
Our findings, based on common clinical data, revealed two distinct subphenotypes with different disease courses. These results could help health professionals allocate resources and select patients for testing novel therapies.
- Raul dos Reis Ururahy
-
Original Article
Resuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti , [ … ],
- Flavia Ribeiro Machado
Abstract
Original ArticleResuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti ,
- Leandro Taniguchi ,
- André Gobatto,
- André Miguel Japiassú ,
- Antonio Tonete Bafi,
- Bruno Franco Mazza,
- Danilo Teixeira Noritomi,
- Felipe Dal-Pizzol ,
- Fernando Bozza ,
- Jorge Ibrahin Figueira Salluh ,
- Glauco Adrieno Westphal ,
- Márcio Soares ,
- Murillo Santucci César de Assunção ,
- Thiago Lisboa,
- Suzana Margarete Ajeje Lobo,
- Achilles Rohlfs Barbosa,
- Adriana Fonseca Ventura,
- Ailson Faria de Souza,
- Alexandre Francisco Silva,
- Alexandre Toledo,
- Aline Reis,
- Allan Cembranel,
- Alvaro Rea Neto,
- Ana Lúcia Gut,
- Ana Patricia Pierre Justo,
- Ana Paula Santos,
- André Campos D. de Albuquerque,
- André Scazufka,
- Antonio Babo Rodrigues,
- Bruno Bonaccorsi Fernandino,
- Bruno Goncalves Silva,
- Bruno Sarno Vidal,
- Bruno Valle Pinheiro,
- Bruno Vilela Costa Pinto,
- Carlos Augusto Ramos Feijo,
- Carlos de Abreu Filho,
- Carlos Eduardo da Costa Nunes Bosso,
- Carlos Eduardo Nassif Moreira,
- Carlos Henrique Ferreira Ramos,
- Carmen Tavares,
- Cidamaiá Arantes,
- Cintia Grion,
- Ciro Leite Mendes,
- Claudio Kmohan,
- Claudio Piras,
- Cristine Pilati Pileggi Castro,
- Cyntia Lins,
- Daniel Beraldo,
- Daniel Fontes,
- Daniela Boni,
- Débora Castiglioni,
- Denise de Moraes Paisani,
- Durval Ferreira Fonseca Pedroso,
- Ederson Roberto Mattos,
- Edgar de Brito Sobrinho,
- Edgar M. V. Troncoso,
- Edison Moraes Rodrigues Filho,
- Eduardo Enrico Ferrari Nogueira,
- Eduardo Leme Ferreira,
- Eduardo Souza Pacheco,
- Euzebio Jodar,
- Evandro L. A. Ferreira,
- Fabiana Fernandes de Araujo,
- Fabiana Schuelter Trevisol,
- Fábio Ferreira Amorim,
- Fabio Poianas Giannini,
- Fabrício Primitivo Matos Santos,
- Fátima Buarque,
- Felipe Gallego Lima,
- Fernando Antonio Alvares da Costa,
- Fernando Cesar dos Anjos Sad,
- Fernando G. Aranha,
- Fernando Ganem,
- Flavio Callil,
- Francisco Flávio Costa Filho,
- Frederico Toledo Campo Dall´Arto,
- Geovani Moreno,
- Gilberto Friedman,
- Giulliana Martines Moralez,
- Guilherme Abdalla da Silva,
- Guilherme Costa,
- Guilherme Silva Cavalcanti,
- Guilherme Silva Cavalcanti,
- Gustavo Navarro Betônico,
- Gustavo Navarro Betônico,
- Hélder Reis,
- Helia Beatriz N. Araujo,
- Helio Anjos Hortiz Júnior,
- Helio Penna Guimaraes,
- Hugo Urbano,
- Israel Maia,
- Ivan Lopes Santiago Filho,
- Jamil Farhat Júnior,
- Janu Rangel Alvarez,
- Joel Tavares Passos,
- Jorge Eduardo da Rocha Paranhos,
- José Aurelio Marques,
- José Gonçalves Moreira Filho,
- Jose Neto Andrade,
- José Onofre de C Sobrinho,
- Jose Terceiro de Paiva Bezerra,
- Juliana Apolônio Alves,
- Juliana Ferreira,
- Jussara Gomes,
- Karina Midori Sato,
- Karine Gerent,
- Kathia Margarida Costa Teixeira,
- Katia Aparecida Pessoa Conde,
- Laércia Ferreira Martins,
- Lanese Figueirêdo,
- Leila Rezegue,
- Leonardo Tcherniacovsk,
- Leone Oliveira Ferraz,
- Liane Cavalcante,
- Ligia Rabelo,
- Lilian Miilher,
- Lisiane Garcia,
- Luana Tannous,
- Ludhmila Abrahão Hajjar,
- Luís Eduardo Miranda Paciência,
- Luiz Monteiro da Cruz Neto,
- Macia Valeria Bley,
- Marcelo Ferreira Sousa,
- Marcelo Lourencini Puga,
- Marcelo Luz Pereira Romano,
- Marciano Nobrega,
- Marcio Arbex,
- Márcio Leite Rodrigues,
- Márcio Osório Guerreiro,
- Marcone Rocha,
- Maria Angela Pangoni Alves,
- Maria Angela Pangoni Alves,
- Maria Doroti Rosa,
- Mariza D’Agostino Dias,
- Miquéias Martins,
- Mirella de Oliveira,
- Miriane Melo Silveira Moretti,
- Mirna Matsui,
- Octavio Messender,
- Orlando Luís de Andrade Santarém,
- Patricio Júnior Henrique da Silveira,
- Paula Frizera Vassallo,
- Paulo Antoniazzi,
- Paulo César Gottardo,
- Paulo Correia,
- Paulo Ferreira,
- Paulo Torres,
- Pedro Gabrile M. de Barros e Silva,
- Rafael Foernges,
- Rafael Gomes,
- Rafael Moraes,
- Raimundo Nonato filho,
- Renato Luis Borba,
- Renato V Gomes,
- Ricardo Cordioli,
- Ricardo Lima,
- Ricardo Pérez López,
- Ricardo Rath de Oliveira Gargioni,
- Richard Rosenblat,
- Roberta Machado de Souza,
- Roberto Almeida,
- Roberto Camargo Narciso,
- Roberto Marco,
- Roberto waltrick,
- Rodrigo Biondi,
- Rodrigo Figueiredo,
- Rodrigo Santana Dutra,
- Roseane Batista,
- Rouge Felipe,
- Rubens Sergio da Silva Franco,
- Sandra Houly,
- Sara Socorro Faria,
- Sergio Felix Pinto,
- Sergio Luzzi,
- Sergio Sant’ana,
- Sergio Sonego Fernandes,
- Sérgio Yamada,
- Sérgio Zajac,
- Sidiner Mesquita Vaz,
- Silvia Aparecida Bezerra Bezerra,
- Tatiana Bueno Tardivo Farhat,
- Thiago Martins Santos,
- Tiago Smith,
- Ulysses V. A. Silva,
- Valnei Bento Damasceno,
- Vandack Nobre,
- Vicente Cés de Souza Dantas,
- Vivian Menezes Irineu,
- Viviane Bogado,
- Wagner Nedel,
- Walther Campos Filho,
- Weidson Dantas,
- William Viana,
- Wilson de Oliveira Filho,
- Wilson Martins Delgadinho,
- Simon Finfer,
- Flavia Ribeiro Machado
Views1See moreAbstract
Objective:
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
Methods:
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
Results:
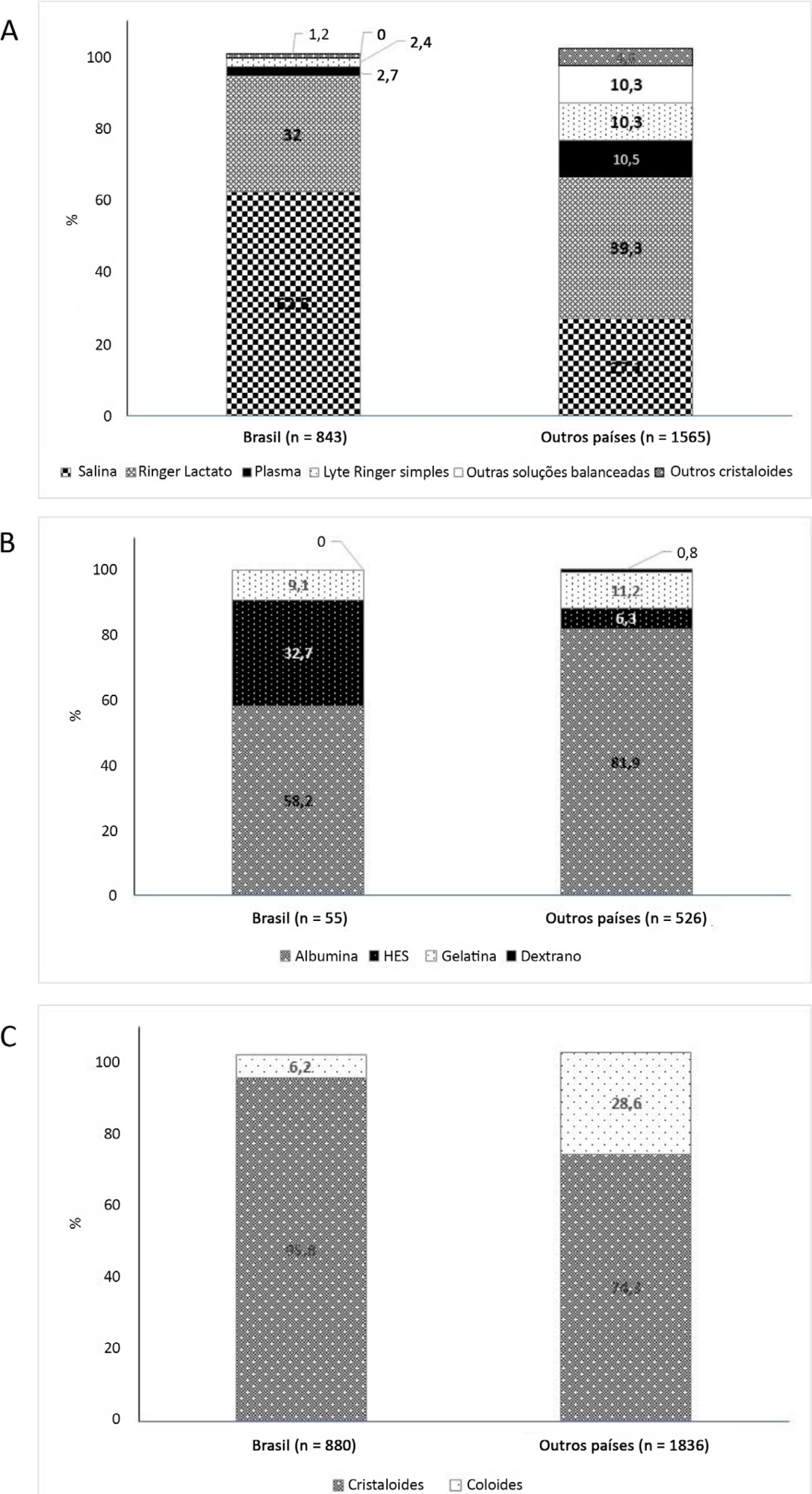
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Conclusion:
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
Views1Abstract
Original ArticleResuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti ,
- Leandro Taniguchi ,
- André Gobatto,
- André Miguel Japiassú ,
- Antonio Tonete Bafi,
- Bruno Franco Mazza,
- Danilo Teixeira Noritomi,
- Felipe Dal-Pizzol ,
- Fernando Bozza ,
- Jorge Ibrahin Figueira Salluh ,
- Glauco Adrieno Westphal ,
- Márcio Soares ,
- Murillo Santucci César de Assunção ,
- Thiago Lisboa,
- Suzana Margarete Ajeje Lobo,
- Achilles Rohlfs Barbosa,
- Adriana Fonseca Ventura,
- Ailson Faria de Souza,
- Alexandre Francisco Silva,
- Alexandre Toledo,
- Aline Reis,
- Allan Cembranel,
- Alvaro Rea Neto,
- Ana Lúcia Gut,
- Ana Patricia Pierre Justo,
- Ana Paula Santos,
- André Campos D. de Albuquerque,
- André Scazufka,
- Antonio Babo Rodrigues,
- Bruno Bonaccorsi Fernandino,
- Bruno Goncalves Silva,
- Bruno Sarno Vidal,
- Bruno Valle Pinheiro,
- Bruno Vilela Costa Pinto,
- Carlos Augusto Ramos Feijo,
- Carlos de Abreu Filho,
- Carlos Eduardo da Costa Nunes Bosso,
- Carlos Eduardo Nassif Moreira,
- Carlos Henrique Ferreira Ramos,
- Carmen Tavares,
- Cidamaiá Arantes,
- Cintia Grion,
- Ciro Leite Mendes,
- Claudio Kmohan,
- Claudio Piras,
- Cristine Pilati Pileggi Castro,
- Cyntia Lins,
- Daniel Beraldo,
- Daniel Fontes,
- Daniela Boni,
- Débora Castiglioni,
- Denise de Moraes Paisani,
- Durval Ferreira Fonseca Pedroso,
- Ederson Roberto Mattos,
- Edgar de Brito Sobrinho,
- Edgar M. V. Troncoso,
- Edison Moraes Rodrigues Filho,
- Eduardo Enrico Ferrari Nogueira,
- Eduardo Leme Ferreira,
- Eduardo Souza Pacheco,
- Euzebio Jodar,
- Evandro L. A. Ferreira,
- Fabiana Fernandes de Araujo,
- Fabiana Schuelter Trevisol,
- Fábio Ferreira Amorim,
- Fabio Poianas Giannini,
- Fabrício Primitivo Matos Santos,
- Fátima Buarque,
- Felipe Gallego Lima,
- Fernando Antonio Alvares da Costa,
- Fernando Cesar dos Anjos Sad,
- Fernando G. Aranha,
- Fernando Ganem,
- Flavio Callil,
- Francisco Flávio Costa Filho,
- Frederico Toledo Campo Dall´Arto,
- Geovani Moreno,
- Gilberto Friedman,
- Giulliana Martines Moralez,
- Guilherme Abdalla da Silva,
- Guilherme Costa,
- Guilherme Silva Cavalcanti,
- Guilherme Silva Cavalcanti,
- Gustavo Navarro Betônico,
- Gustavo Navarro Betônico,
- Hélder Reis,
- Helia Beatriz N. Araujo,
- Helio Anjos Hortiz Júnior,
- Helio Penna Guimaraes,
- Hugo Urbano,
- Israel Maia,
- Ivan Lopes Santiago Filho,
- Jamil Farhat Júnior,
- Janu Rangel Alvarez,
- Joel Tavares Passos,
- Jorge Eduardo da Rocha Paranhos,
- José Aurelio Marques,
- José Gonçalves Moreira Filho,
- Jose Neto Andrade,
- José Onofre de C Sobrinho,
- Jose Terceiro de Paiva Bezerra,
- Juliana Apolônio Alves,
- Juliana Ferreira,
- Jussara Gomes,
- Karina Midori Sato,
- Karine Gerent,
- Kathia Margarida Costa Teixeira,
- Katia Aparecida Pessoa Conde,
- Laércia Ferreira Martins,
- Lanese Figueirêdo,
- Leila Rezegue,
- Leonardo Tcherniacovsk,
- Leone Oliveira Ferraz,
- Liane Cavalcante,
- Ligia Rabelo,
- Lilian Miilher,
- Lisiane Garcia,
- Luana Tannous,
- Ludhmila Abrahão Hajjar,
- Luís Eduardo Miranda Paciência,
- Luiz Monteiro da Cruz Neto,
- Macia Valeria Bley,
- Marcelo Ferreira Sousa,
- Marcelo Lourencini Puga,
- Marcelo Luz Pereira Romano,
- Marciano Nobrega,
- Marcio Arbex,
- Márcio Leite Rodrigues,
- Márcio Osório Guerreiro,
- Marcone Rocha,
- Maria Angela Pangoni Alves,
- Maria Angela Pangoni Alves,
- Maria Doroti Rosa,
- Mariza D’Agostino Dias,
- Miquéias Martins,
- Mirella de Oliveira,
- Miriane Melo Silveira Moretti,
- Mirna Matsui,
- Octavio Messender,
- Orlando Luís de Andrade Santarém,
- Patricio Júnior Henrique da Silveira,
- Paula Frizera Vassallo,
- Paulo Antoniazzi,
- Paulo César Gottardo,
- Paulo Correia,
- Paulo Ferreira,
- Paulo Torres,
- Pedro Gabrile M. de Barros e Silva,
- Rafael Foernges,
- Rafael Gomes,
- Rafael Moraes,
- Raimundo Nonato filho,
- Renato Luis Borba,
- Renato V Gomes,
- Ricardo Cordioli,
- Ricardo Lima,
- Ricardo Pérez López,
- Ricardo Rath de Oliveira Gargioni,
- Richard Rosenblat,
- Roberta Machado de Souza,
- Roberto Almeida,
- Roberto Camargo Narciso,
- Roberto Marco,
- Roberto waltrick,
- Rodrigo Biondi,
- Rodrigo Figueiredo,
- Rodrigo Santana Dutra,
- Roseane Batista,
- Rouge Felipe,
- Rubens Sergio da Silva Franco,
- Sandra Houly,
- Sara Socorro Faria,
- Sergio Felix Pinto,
- Sergio Luzzi,
- Sergio Sant’ana,
- Sergio Sonego Fernandes,
- Sérgio Yamada,
- Sérgio Zajac,
- Sidiner Mesquita Vaz,
- Silvia Aparecida Bezerra Bezerra,
- Tatiana Bueno Tardivo Farhat,
- Thiago Martins Santos,
- Tiago Smith,
- Ulysses V. A. Silva,
- Valnei Bento Damasceno,
- Vandack Nobre,
- Vicente Cés de Souza Dantas,
- Vivian Menezes Irineu,
- Viviane Bogado,
- Wagner Nedel,
- Walther Campos Filho,
- Weidson Dantas,
- William Viana,
- Wilson de Oliveira Filho,
- Wilson Martins Delgadinho,
- Simon Finfer,
- Flavia Ribeiro Machado
Views1See moreAbstract
Objective:
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
Methods:
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
Results:
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Conclusion:
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
- Flavio Geraldo Rezende de Freitas
-
Original Article
Impact of nonclinical factors on intensive care unit admission decisions: a vignette-based randomized trial (V-TRIAGE)
Rev Bras Ter Intensiva. 2021;33(2):219-230
Abstract
Original ArticleImpact of nonclinical factors on intensive care unit admission decisions: a vignette-based randomized trial (V-TRIAGE)
Rev Bras Ter Intensiva. 2021;33(2):219-230
DOI 10.5935/0103-507X.20210029
Views1See moreAbstract
Objective:
To assess the impact of intensive care unit bed availability, distractors and choice framing on intensive care unit admission decisions.
Methods:
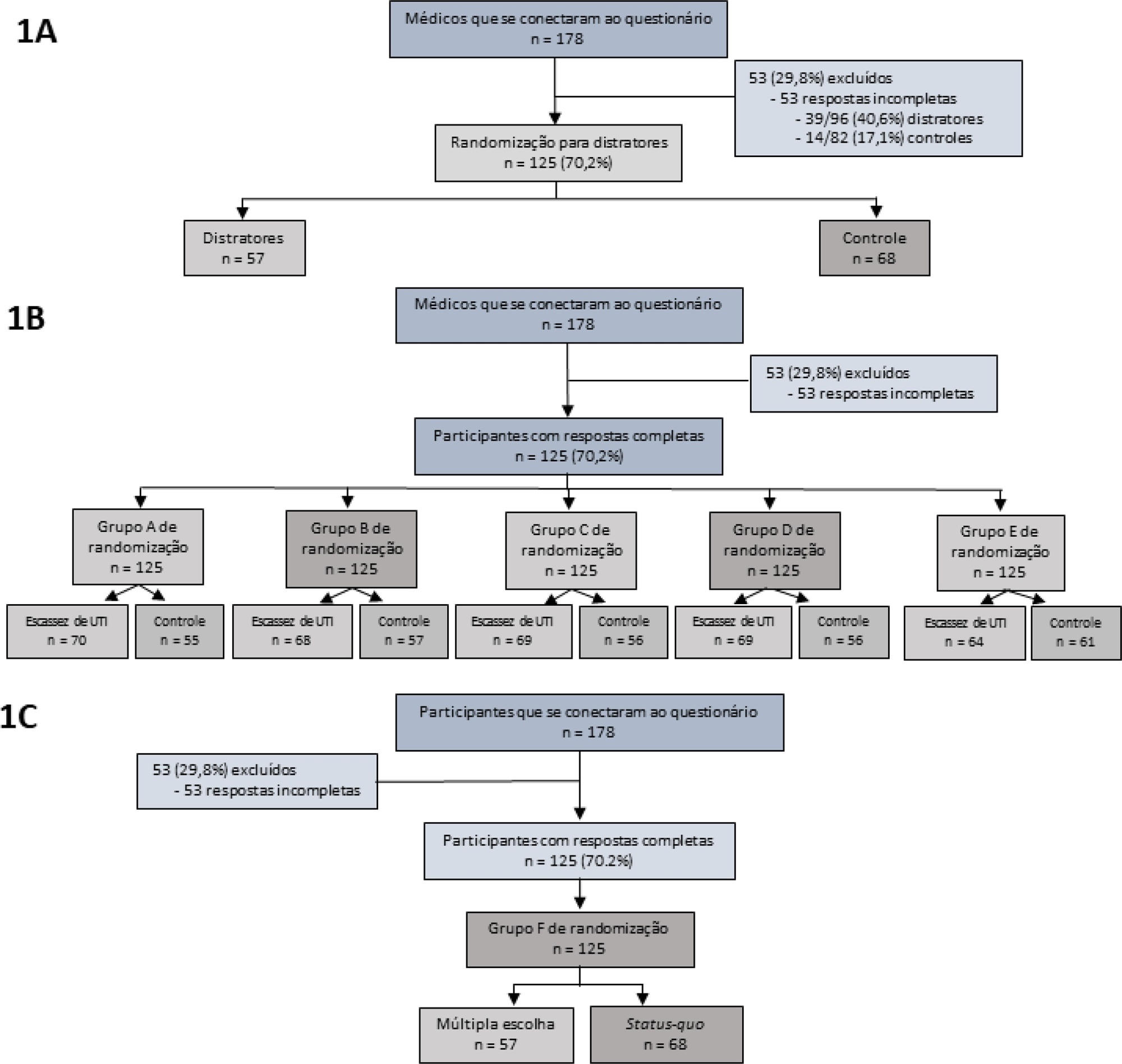
This study was a randomized factorial trial using patient-based vignettes. The vignettes were deemed archetypical for intensive care unit admission or refusal, as judged by a group of experts. Intensive care unit physicians were randomized to 1) an increased distraction (intervention) or a control group, 2) an intensive care unit bed scarcity or nonscarcity (availability) setting, and 3) a multiple-choice or omission (status quo) vignette scenario. The primary outcome was the proportion of appropriate intensive care unit allocations, defined as concordance with the allocation decision made by the group of experts.
Results:
We analyzed 125 physicians. Overall, distractors had no impact on the outcome; however, there was a differential drop-out rate, with fewer physicians in the intervention arm completing the questionnaire. Intensive care unit bed availability was associated with an inappropriate allocation of vignettes deemed inappropriate for intensive care unit admission (OR = 2.47; 95%CI 1.19 – 5.11) but not of vignettes appropriate for intensive care unit admission. There was a significant interaction with the presence of distractors (p = 0.007), with intensive care unit bed availability being associated with increased intensive care unit admission of vignettes inappropriate for intensive care unit admission in the distractor (intervention) arm (OR = 9.82; 95%CI 2.68 – 25.93) but not in the control group (OR = 1.02; 95%CI 0.38 – 2.72). Multiple choices were associated with increased inappropriate allocation in comparison to the omission group (OR = 5.18; 95%CI 1.37 – 19.61).
Conclusion:
Intensive care unit bed availability and cognitive biases were associated with inappropriate intensive care unit allocation decisions. These findings may have implications for intensive care unit admission policies.
Views1Abstract
Original ArticleImpact of nonclinical factors on intensive care unit admission decisions: a vignette-based randomized trial (V-TRIAGE)
Rev Bras Ter Intensiva. 2021;33(2):219-230
DOI 10.5935/0103-507X.20210029
Views1See moreAbstract
Objective:
To assess the impact of intensive care unit bed availability, distractors and choice framing on intensive care unit admission decisions.
Methods:
This study was a randomized factorial trial using patient-based vignettes. The vignettes were deemed archetypical for intensive care unit admission or refusal, as judged by a group of experts. Intensive care unit physicians were randomized to 1) an increased distraction (intervention) or a control group, 2) an intensive care unit bed scarcity or nonscarcity (availability) setting, and 3) a multiple-choice or omission (status quo) vignette scenario. The primary outcome was the proportion of appropriate intensive care unit allocations, defined as concordance with the allocation decision made by the group of experts.
Results:
We analyzed 125 physicians. Overall, distractors had no impact on the outcome; however, there was a differential drop-out rate, with fewer physicians in the intervention arm completing the questionnaire. Intensive care unit bed availability was associated with an inappropriate allocation of vignettes deemed inappropriate for intensive care unit admission (OR = 2.47; 95%CI 1.19 – 5.11) but not of vignettes appropriate for intensive care unit admission. There was a significant interaction with the presence of distractors (p = 0.007), with intensive care unit bed availability being associated with increased intensive care unit admission of vignettes inappropriate for intensive care unit admission in the distractor (intervention) arm (OR = 9.82; 95%CI 2.68 – 25.93) but not in the control group (OR = 1.02; 95%CI 0.38 – 2.72). Multiple choices were associated with increased inappropriate allocation in comparison to the omission group (OR = 5.18; 95%CI 1.37 – 19.61).
Conclusion:
Intensive care unit bed availability and cognitive biases were associated with inappropriate intensive care unit allocation decisions. These findings may have implications for intensive care unit admission policies.
-
Original Article
Prevalence and outcomes of sepsis in children admitted to public and private hospitals in Latin America: a multicenter observational study
- Daniela Carla Souza ,
- Eliane Roseli Barreira,
- Huei Hsin Shieh,
- Andrea Maria Cordeiro Ventura,
- Albert Bousso, [ … ],
- Eduardo Juan Troster
Abstract
Original ArticlePrevalence and outcomes of sepsis in children admitted to public and private hospitals in Latin America: a multicenter observational study
Rev Bras Ter Intensiva. 2021;33(2):231-242
DOI 10.5935/0103-507X.20210030
- Daniela Carla Souza ,
- Eliane Roseli Barreira,
- Huei Hsin Shieh,
- Andrea Maria Cordeiro Ventura,
- Albert Bousso,
- Eduardo Juan Troster
Views0ABSTRACT
Objective:
To report the prevalence and outcomes of sepsis in children admitted to public and private hospitals.
Methods:
Post hoc analysis of the Latin American Pediatric Sepsis Study (LAPSES) data, a cohort study that analyzed the prevalence and outcomes of sepsis in critically ill children with sepsis on admission at 21 pediatric intensive care units in five Latin American countries.
Results:
Of the 464 sepsis patients, 369 (79.5%) were admitted to public hospitals and 95 (20.5%) to private hospitals. Compared to those admitted to private hospitals, sepsis patients admitted to public hospitals did not differ in age, sex, immunization status, hospital length of stay or type of admission but had higher rates of septic shock, higher Pediatric Risk of Mortality (PRISM), Pediatric Index of Mortality 2 (PIM 2), and Pediatric Logistic Organ Dysfunction (PELOD) scores, and higher rates of underlying diseases and maternal illiteracy. The proportion of patients admitted from pediatric wards and sepsis-related mortality were higher in public hospitals. Multivariate analysis did not show any correlation between mortality and the type of hospital, but mortality was associated with greater severity on pediatric intensive care unit admission in patients from public hospitals.
Conclusion:
In this sample of critically ill children from five countries in Latin America, the prevalence of septic shock within the first 24 hours at admission and sepsis-related mortality were higher in public hospitals than in private hospitals. Higher sepsis-related mortality in children admitted to public pediatric intensive care units was associated with greater severity on pediatric intensive care unit admission but not with the type of hospital. New studies will be necessary to elucidate the causes of the higher prevalence and mortality of pediatric sepsis in public hospitals.
Keywords:ChildCritical illnessHospital, privateHospital, publicIntensive care unitsIntensive care units, pediatricLatin AmericaMortalityprevalenceSepsisSeptic shockSee moreViews0Abstract
Original ArticlePrevalence and outcomes of sepsis in children admitted to public and private hospitals in Latin America: a multicenter observational study
Rev Bras Ter Intensiva. 2021;33(2):231-242
DOI 10.5935/0103-507X.20210030
- Daniela Carla Souza ,
- Eliane Roseli Barreira,
- Huei Hsin Shieh,
- Andrea Maria Cordeiro Ventura,
- Albert Bousso,
- Eduardo Juan Troster
Views0ABSTRACT
Objective:
To report the prevalence and outcomes of sepsis in children admitted to public and private hospitals.
Methods:
Post hoc analysis of the Latin American Pediatric Sepsis Study (LAPSES) data, a cohort study that analyzed the prevalence and outcomes of sepsis in critically ill children with sepsis on admission at 21 pediatric intensive care units in five Latin American countries.
Results:
Of the 464 sepsis patients, 369 (79.5%) were admitted to public hospitals and 95 (20.5%) to private hospitals. Compared to those admitted to private hospitals, sepsis patients admitted to public hospitals did not differ in age, sex, immunization status, hospital length of stay or type of admission but had higher rates of septic shock, higher Pediatric Risk of Mortality (PRISM), Pediatric Index of Mortality 2 (PIM 2), and Pediatric Logistic Organ Dysfunction (PELOD) scores, and higher rates of underlying diseases and maternal illiteracy. The proportion of patients admitted from pediatric wards and sepsis-related mortality were higher in public hospitals. Multivariate analysis did not show any correlation between mortality and the type of hospital, but mortality was associated with greater severity on pediatric intensive care unit admission in patients from public hospitals.
Conclusion:
In this sample of critically ill children from five countries in Latin America, the prevalence of septic shock within the first 24 hours at admission and sepsis-related mortality were higher in public hospitals than in private hospitals. Higher sepsis-related mortality in children admitted to public pediatric intensive care units was associated with greater severity on pediatric intensive care unit admission but not with the type of hospital. New studies will be necessary to elucidate the causes of the higher prevalence and mortality of pediatric sepsis in public hospitals.
Keywords:ChildCritical illnessHospital, privateHospital, publicIntensive care unitsIntensive care units, pediatricLatin AmericaMortalityprevalenceSepsisSeptic shockSee more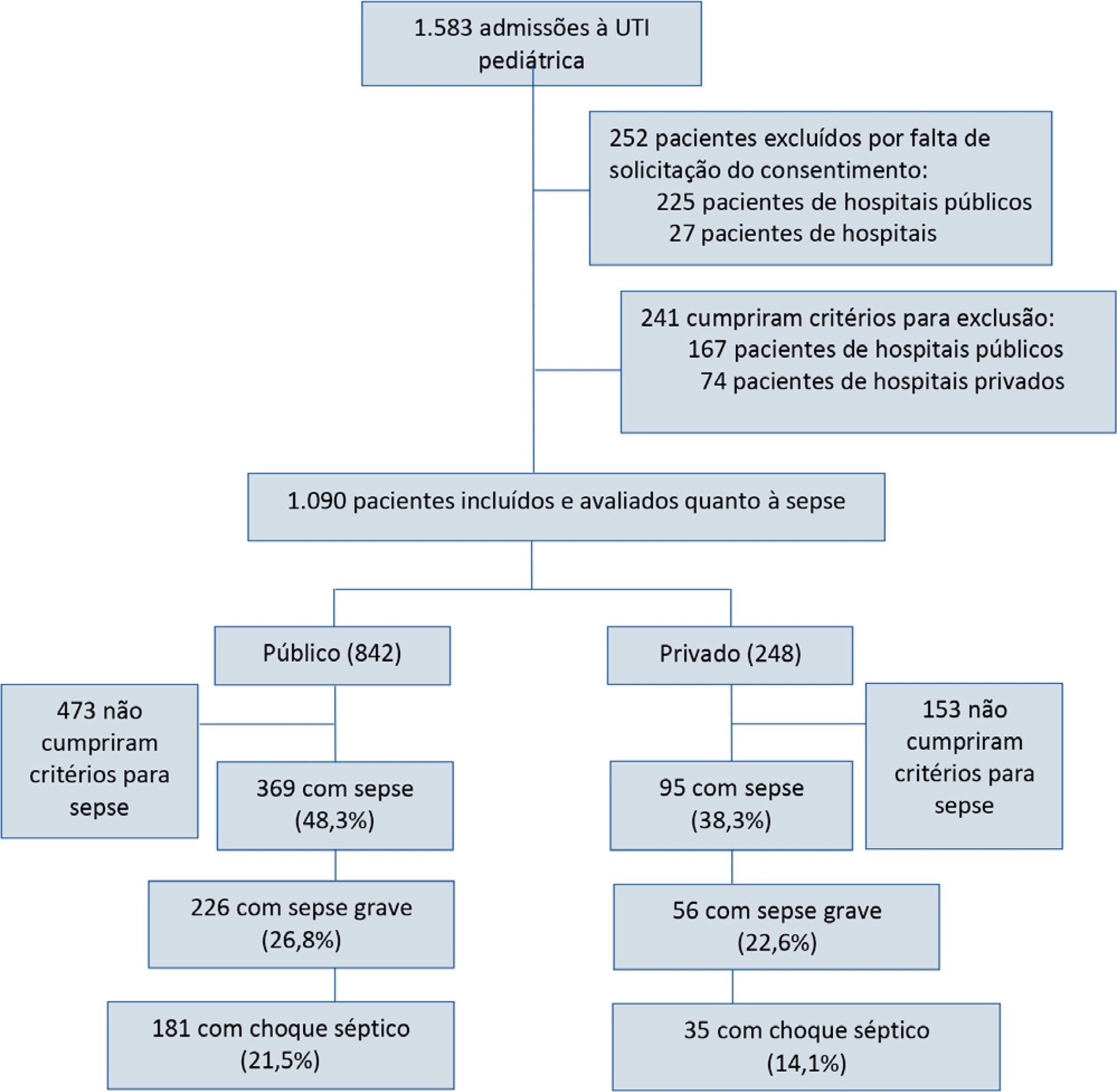
- Daniela Carla Souza
-
Original Article
Functional independence and spirometry in adult post-intensive care unit patients
- Lilian Regina Lengler Abentroth ,
- Erica Fernanda Osaku,
- Mayara Manzoni Marques da Silva,
- Jaiane Luiza Jaskowiak,
- Renata de Souza Zaponi, [ … ],
- Péricles Almeida Delfino Duarte
Abstract
Original ArticleFunctional independence and spirometry in adult post-intensive care unit patients
Rev Bras Ter Intensiva. 2021;33(2):243-250
DOI 10.5935/0103-507X.20210031
- Lilian Regina Lengler Abentroth ,
- Erica Fernanda Osaku,
- Mayara Manzoni Marques da Silva,
- Jaiane Luiza Jaskowiak,
- Renata de Souza Zaponi,
- Suely Mariko Ogasawara,
- Marcela Aparecida Leite,
- Cláudia Rejane Lima de Macedo Costa,
- Itamar Regazzo Pedreschi Porto,
- Amaury Cezar Jorge,
- Péricles Almeida Delfino Duarte
Views0ABSTRACT
Objective:
To relate functional independence to the degree of pulmonary impairment in adult patients 3 months after discharge from the intensive care unit.
Methods:
This was a retrospective cohort study conducted in one adult intensive care unit and a multi-professional post-intensive care unit outpatient clinic of a single center. Patients admitted to the intensive care unit from January 2012 to December 2013 who underwent (3 months later) spirometry and answered the Functional Independence Measure Questionnaire were included.
Results:
Patients were divided into groups according to the classification of functional independence and spirometry. The study included 197 patients who were divided into greater dependence (n = 4), lower dependence (n = 12) and independent (n = 181) groups. Comparing the three groups, regarding the classification of the Functional Independence Measure, patients with greater dependence had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment values at intensive care unit admission with more advanced age, more days on mechanical ventilation, and longer stay in the intensive care unit and hospital. The majority of patients presented with pulmonary impairment, which was the obstructive pattern observed most frequently. When comparing functional independence with pulmonary function, it was observed that the lower the functional status, the worse the pulmonary function, with a significant difference being observed in peak expiratory flow (p = 0.030).
Conclusion:
The majority of patients who returned to the outpatient clinic 3 months after discharge had good functional status but did present with pulmonary impairment, which is related to the degree of functional dependence.
Keywords:Ambulatory care facilities, hospitalCritical careIntensive care unitsMobility limitationPeak expiratory flow rateRespiration, artificialSpirometrySee moreViews0Abstract
Original ArticleFunctional independence and spirometry in adult post-intensive care unit patients
Rev Bras Ter Intensiva. 2021;33(2):243-250
DOI 10.5935/0103-507X.20210031
- Lilian Regina Lengler Abentroth ,
- Erica Fernanda Osaku,
- Mayara Manzoni Marques da Silva,
- Jaiane Luiza Jaskowiak,
- Renata de Souza Zaponi,
- Suely Mariko Ogasawara,
- Marcela Aparecida Leite,
- Cláudia Rejane Lima de Macedo Costa,
- Itamar Regazzo Pedreschi Porto,
- Amaury Cezar Jorge,
- Péricles Almeida Delfino Duarte
Views0ABSTRACT
Objective:
To relate functional independence to the degree of pulmonary impairment in adult patients 3 months after discharge from the intensive care unit.
Methods:
This was a retrospective cohort study conducted in one adult intensive care unit and a multi-professional post-intensive care unit outpatient clinic of a single center. Patients admitted to the intensive care unit from January 2012 to December 2013 who underwent (3 months later) spirometry and answered the Functional Independence Measure Questionnaire were included.
Results:
Patients were divided into groups according to the classification of functional independence and spirometry. The study included 197 patients who were divided into greater dependence (n = 4), lower dependence (n = 12) and independent (n = 181) groups. Comparing the three groups, regarding the classification of the Functional Independence Measure, patients with greater dependence had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment values at intensive care unit admission with more advanced age, more days on mechanical ventilation, and longer stay in the intensive care unit and hospital. The majority of patients presented with pulmonary impairment, which was the obstructive pattern observed most frequently. When comparing functional independence with pulmonary function, it was observed that the lower the functional status, the worse the pulmonary function, with a significant difference being observed in peak expiratory flow (p = 0.030).
Conclusion:
The majority of patients who returned to the outpatient clinic 3 months after discharge had good functional status but did present with pulmonary impairment, which is related to the degree of functional dependence.
Keywords:Ambulatory care facilities, hospitalCritical careIntensive care unitsMobility limitationPeak expiratory flow rateRespiration, artificialSpirometrySee more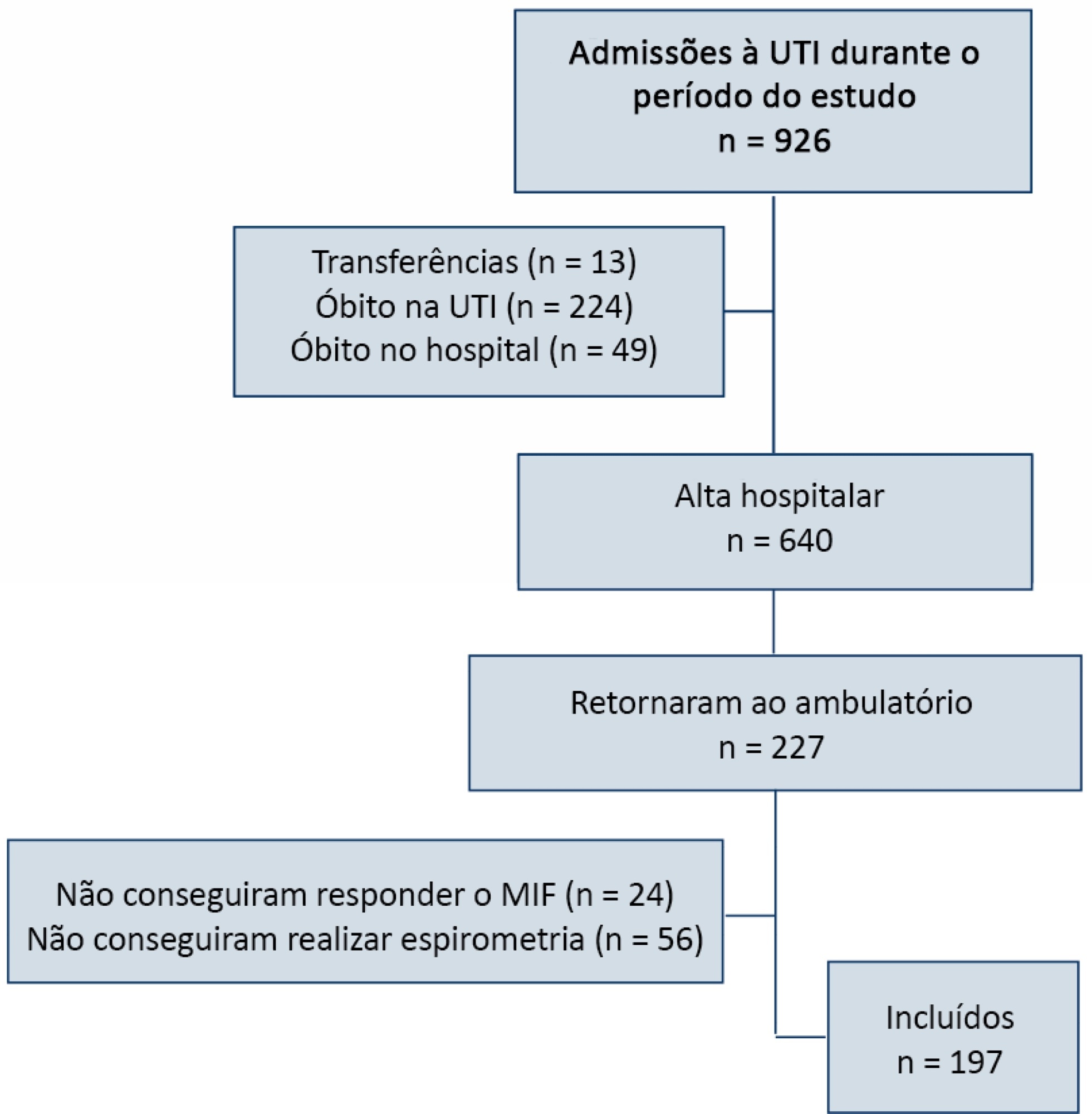
- Lilian Regina Lengler Abentroth
-
Original Article
Predictors of coronary artery disease in cardiac arrest survivors: coronary angiography for everyone? A single-center retrospective analysis
- Joana Rigueira ,
- Inês Aguiar-Ricardo,
- Pedro Carrilho-Ferreira,
- Miguel Nobre Menezes,
- Sara Pereira, [ … ],
- Fausto J. Pinto
Abstract
Original ArticlePredictors of coronary artery disease in cardiac arrest survivors: coronary angiography for everyone? A single-center retrospective analysis
Rev Bras Ter Intensiva. 2021;33(2):251-260
DOI 10.5935/0103-507X.20210032
- Joana Rigueira ,
- Inês Aguiar-Ricardo,
- Pedro Carrilho-Ferreira,
- Miguel Nobre Menezes,
- Sara Pereira,
- Pedro S. Morais,
- Pedro Canas da Silva,
- Fausto J. Pinto
Views0ABSTRACT
Objective:
To identify predictors of coronary artery disease in survivors of cardiac arrest, to define the best timing for coronary angiography and to establish the relationship between coronary artery disease and mortality.
Methods:
This was a single-center retrospective study including consecutive patients who underwent coronary angiography after cardiac arrest.
Results:
A total of 117 patients (63 ± 13 years, 77% men) were included. Most cardiac arrest incidents occurred with shockable rhythms (70.1%), and the median duration until the return of spontaneous circulation was 10 minutes. Significant coronary artery disease was found in 68.4% of patients, of whom 75% underwent percutaneous coronary intervention. ST-segment elevation (OR 6.5, 95%CI 2.2 – 19.6; p = 0.001), the presence of wall motion abnormalities (OR 22.0, 95%CI 5.7 – 84.6; p < 0.001), an left ventricular ejection fraction ≤ 40% (OR 6.2, 95%CI 1.8 - 21.8; p = 0.005) and elevated high sensitivity troponin T (OR 3.04, 95%CI 1.3 - 6.9; p = 0.008) were predictors of coronary artery disease; the latter had poor accuracy (area under the curve 0.64; p = 0.004), with an optimal cutoff of 170ng/L. Only ST-segment elevation and the presence of wall motion abnormalities were independent predictors of coronary artery disease. The duration of cardiac arrest (OR 1.015, 95%CI 1.0 - 1.05; p = 0.048) was an independent predictor of death, and shockable rhythm (OR 0.4, 95%CI 0.4 - 0.9; p = 0.031) was an independent predictor of survival. The presence of coronary artery disease and the performance of percutaneous coronary intervention had no impact on survival; it was not possible to establish the best cutoff for coronary angiography timing.
Conclusion:
In patients with cardiac arrest, ST-segment elevation, wall motion abnormalities, left ventricular dysfunction and elevated high sensitivity troponin T were predictive of coronary artery disease. Neither coronary artery disease nor percutaneous coronary intervention significantly impacted survival.
Keywords:Cardiac ArrestCoronary angiographyCoronary artery diseasepercutaneous coronary interventionSurvivalSee moreViews0Abstract
Original ArticlePredictors of coronary artery disease in cardiac arrest survivors: coronary angiography for everyone? A single-center retrospective analysis
Rev Bras Ter Intensiva. 2021;33(2):251-260
DOI 10.5935/0103-507X.20210032
- Joana Rigueira ,
- Inês Aguiar-Ricardo,
- Pedro Carrilho-Ferreira,
- Miguel Nobre Menezes,
- Sara Pereira,
- Pedro S. Morais,
- Pedro Canas da Silva,
- Fausto J. Pinto
Views0ABSTRACT
Objective:
To identify predictors of coronary artery disease in survivors of cardiac arrest, to define the best timing for coronary angiography and to establish the relationship between coronary artery disease and mortality.
Methods:
This was a single-center retrospective study including consecutive patients who underwent coronary angiography after cardiac arrest.
Results:
A total of 117 patients (63 ± 13 years, 77% men) were included. Most cardiac arrest incidents occurred with shockable rhythms (70.1%), and the median duration until the return of spontaneous circulation was 10 minutes. Significant coronary artery disease was found in 68.4% of patients, of whom 75% underwent percutaneous coronary intervention. ST-segment elevation (OR 6.5, 95%CI 2.2 – 19.6; p = 0.001), the presence of wall motion abnormalities (OR 22.0, 95%CI 5.7 – 84.6; p < 0.001), an left ventricular ejection fraction ≤ 40% (OR 6.2, 95%CI 1.8 - 21.8; p = 0.005) and elevated high sensitivity troponin T (OR 3.04, 95%CI 1.3 - 6.9; p = 0.008) were predictors of coronary artery disease; the latter had poor accuracy (area under the curve 0.64; p = 0.004), with an optimal cutoff of 170ng/L. Only ST-segment elevation and the presence of wall motion abnormalities were independent predictors of coronary artery disease. The duration of cardiac arrest (OR 1.015, 95%CI 1.0 - 1.05; p = 0.048) was an independent predictor of death, and shockable rhythm (OR 0.4, 95%CI 0.4 - 0.9; p = 0.031) was an independent predictor of survival. The presence of coronary artery disease and the performance of percutaneous coronary intervention had no impact on survival; it was not possible to establish the best cutoff for coronary angiography timing.
Conclusion:
In patients with cardiac arrest, ST-segment elevation, wall motion abnormalities, left ventricular dysfunction and elevated high sensitivity troponin T were predictive of coronary artery disease. Neither coronary artery disease nor percutaneous coronary intervention significantly impacted survival.
Keywords:Cardiac ArrestCoronary angiographyCoronary artery diseasepercutaneous coronary interventionSurvivalSee more - Joana Rigueira
-
Original Article
Driving pressure and mortality in trauma without acute respiratory distress syndrome: a prospective observational study
Rev Bras Ter Intensiva. 2021;33(2):261-265
Abstract
Original ArticleDriving pressure and mortality in trauma without acute respiratory distress syndrome: a prospective observational study
Rev Bras Ter Intensiva. 2021;33(2):261-265
DOI 10.5935/0103-507X.20210033
Views0ABSTRACT
Objective:
To identify the possible association between driving pressure and mechanical power values and oxygenation index on the first day of mechanical ventilation with the mortality of trauma patients without a diagnosis of acute respiratory distress syndrome.
Methods:
Patients under pressure-controlled or volume-controlled ventilation were included, with data collection 24 hours after orotracheal intubation. Patient follow-up was performed for 30 days to obtain the clinical outcome. The patients were admitted to two intensive care units of the Hospital de Pronto Socorro de Porto Alegre from June to September 2019.
Results:
A total of 24 patients were evaluated. Driving pressure, mechanical power and oxygenation index were similar among patients who survived and those who died, with no statistically significant difference between groups.
Conclusion:
Driving pressure, mechanical power and oxygenation index values obtained on the first day of mechanical ventilation were not associated with mortality of trauma patients without acute respiratory distress syndrome.
Keywords:Critical careIntensive care unitsMortalityRespiration, artificialRespiratory distress syndrome, adultRespiratory mechanicstraumaSee moreViews0Abstract
Original ArticleDriving pressure and mortality in trauma without acute respiratory distress syndrome: a prospective observational study
Rev Bras Ter Intensiva. 2021;33(2):261-265
DOI 10.5935/0103-507X.20210033
Views0ABSTRACT
Objective:
To identify the possible association between driving pressure and mechanical power values and oxygenation index on the first day of mechanical ventilation with the mortality of trauma patients without a diagnosis of acute respiratory distress syndrome.
Methods:
Patients under pressure-controlled or volume-controlled ventilation were included, with data collection 24 hours after orotracheal intubation. Patient follow-up was performed for 30 days to obtain the clinical outcome. The patients were admitted to two intensive care units of the Hospital de Pronto Socorro de Porto Alegre from June to September 2019.
Results:
A total of 24 patients were evaluated. Driving pressure, mechanical power and oxygenation index were similar among patients who survived and those who died, with no statistically significant difference between groups.
Conclusion:
Driving pressure, mechanical power and oxygenation index values obtained on the first day of mechanical ventilation were not associated with mortality of trauma patients without acute respiratory distress syndrome.
Keywords:Critical careIntensive care unitsMortalityRespiration, artificialRespiratory distress syndrome, adultRespiratory mechanicstraumaSee more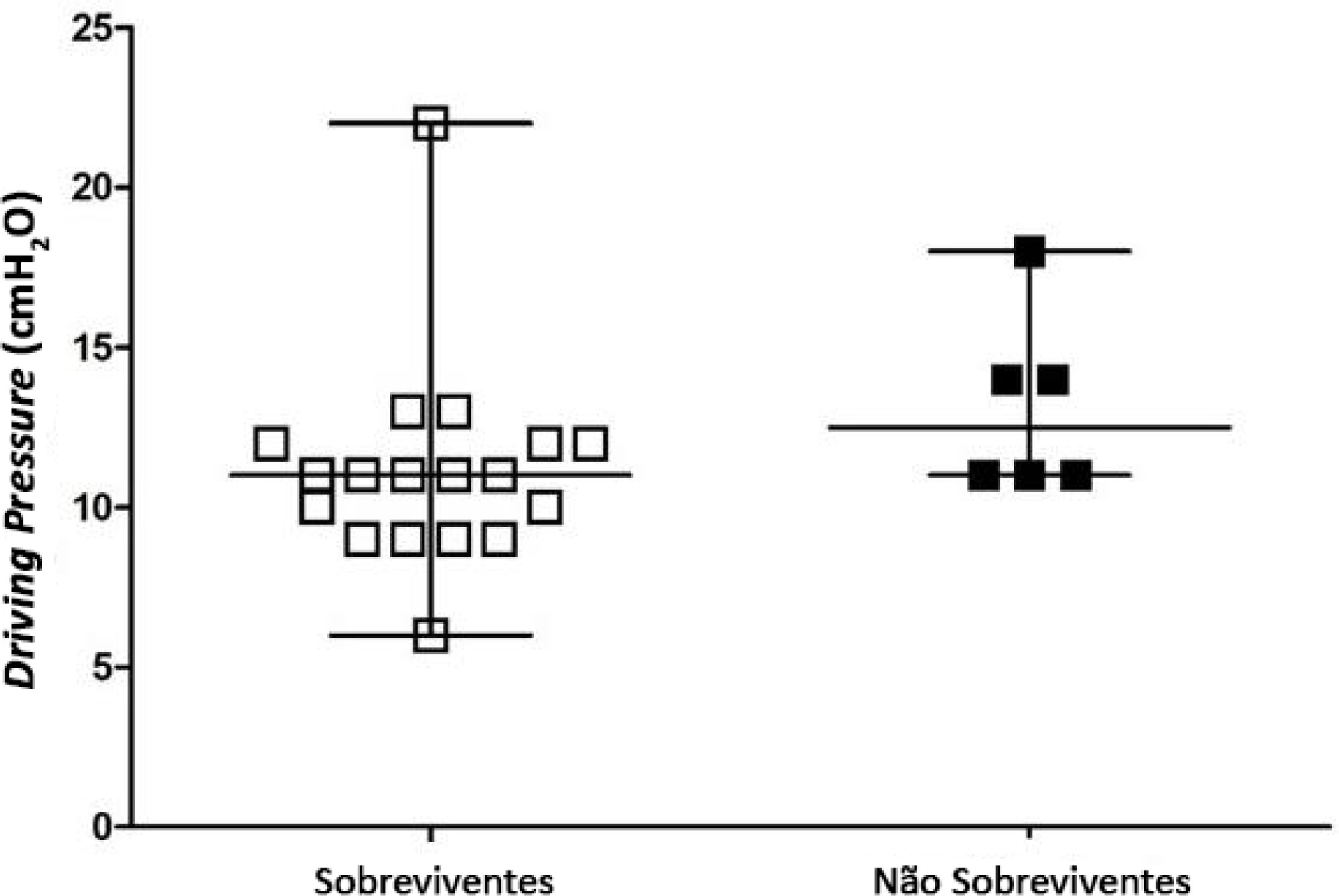
-
Original Article
Prescription of off-label and unlicensed drugs for preterm infants in a neonatal intensive care unit
- Verônica Cheles Vieira ,
- Renart Santos Costa,
- Raquel Cristina Gomes Lima ,
- Daiane Borges Queiroz,
- Danielle Souto de Medeiros
Abstract
Original ArticlePrescription of off-label and unlicensed drugs for preterm infants in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2021;33(2):266-275
DOI 10.5935/0103-507X.20210034
- Verônica Cheles Vieira ,
- Renart Santos Costa,
- Raquel Cristina Gomes Lima ,
- Daiane Borges Queiroz,
- Danielle Souto de Medeiros
Views0See moreABSTRACT
Objective:
To evaluate the use of off-label and unlicensed medications in preterm infants hospitalized in a neonatal intensive care unit.
Methods:
This nonconcurrent cohort study included preterm infants admitted to 3 neonatal intensive care units in 2016 and 2017 who were followed up during the neonatal period. The type and number of medications used were recorded for the entire period and classified based on the Anatomical Therapeutic Chemical. Descriptive and bivariate data analyses were performed to assess associations between the number of drugs used (total, off-label and unlicensed) and the explanatory variables of interest.
Results:
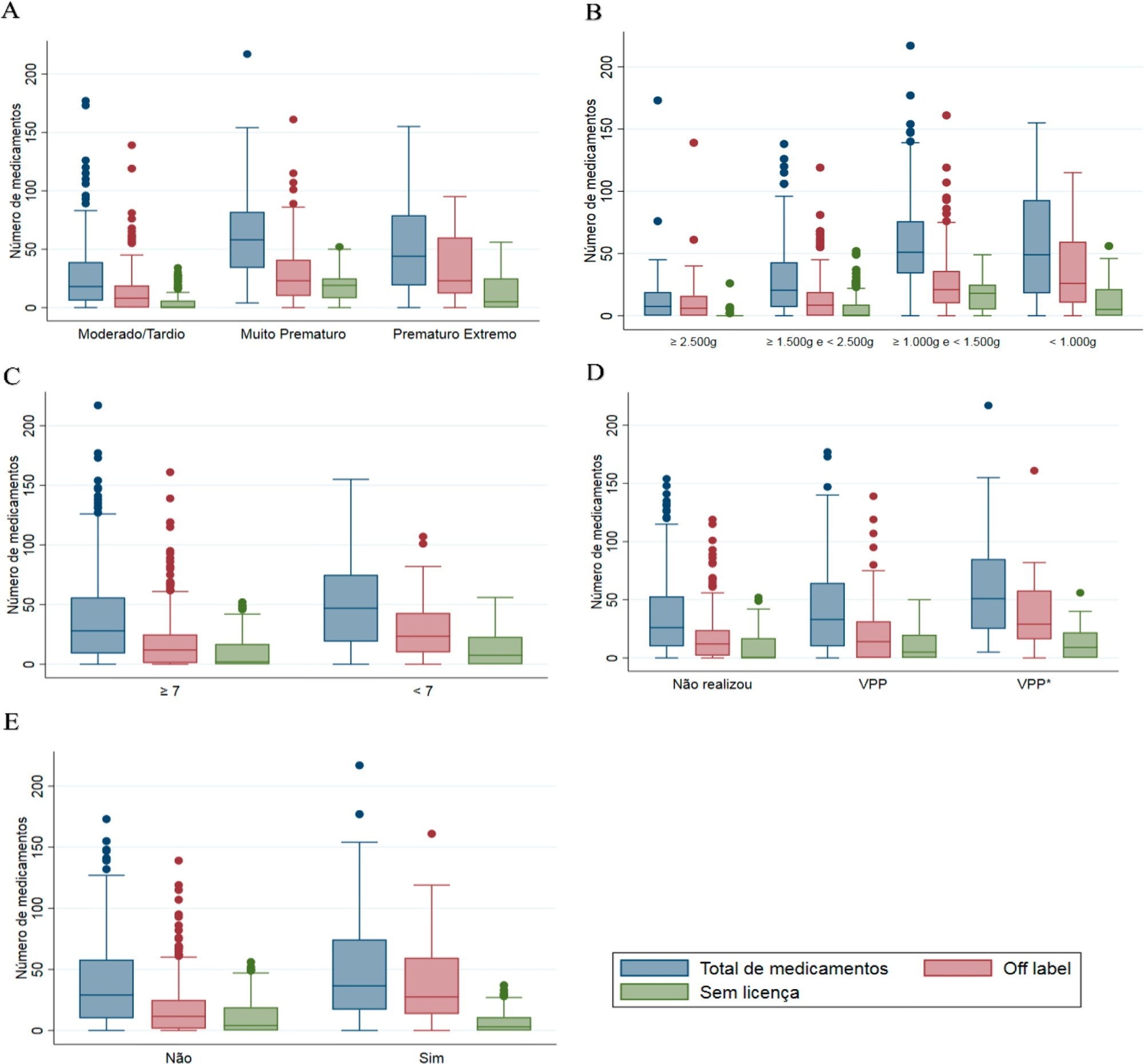
Four hundred preterm infants received 16,143 prescriptions for 86 different pharmaceuticals; 51.9% of these medications were classified as off-label and 23.5% as unlicensed. The most prescribed drugs were gentamicin and ampicillin (17.5% and 15.5% among off-label, respectively) and caffeine (75.5% among unlicensed). The results indicated significant associations between the use of off-label drugs and lower gestational age, low birth weight, lower 5-minute Apgar score, advanced resuscitation maneuver in the delivery room and death. The prescription of unlicensed drugs was associated with lower gestational age, low birth weight and 5-minute Apgar score below 7.
Conclusion:
Neonates admitted to neonatal intensive care units are highly exposed to off-label and unlicensed medications. Further studies are needed to achieve greater safety and quality of drug therapy used in neonatology.
Views0Abstract
Original ArticlePrescription of off-label and unlicensed drugs for preterm infants in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2021;33(2):266-275
DOI 10.5935/0103-507X.20210034
- Verônica Cheles Vieira ,
- Renart Santos Costa,
- Raquel Cristina Gomes Lima ,
- Daiane Borges Queiroz,
- Danielle Souto de Medeiros
Views0See moreABSTRACT
Objective:
To evaluate the use of off-label and unlicensed medications in preterm infants hospitalized in a neonatal intensive care unit.
Methods:
This nonconcurrent cohort study included preterm infants admitted to 3 neonatal intensive care units in 2016 and 2017 who were followed up during the neonatal period. The type and number of medications used were recorded for the entire period and classified based on the Anatomical Therapeutic Chemical. Descriptive and bivariate data analyses were performed to assess associations between the number of drugs used (total, off-label and unlicensed) and the explanatory variables of interest.
Results:
Four hundred preterm infants received 16,143 prescriptions for 86 different pharmaceuticals; 51.9% of these medications were classified as off-label and 23.5% as unlicensed. The most prescribed drugs were gentamicin and ampicillin (17.5% and 15.5% among off-label, respectively) and caffeine (75.5% among unlicensed). The results indicated significant associations between the use of off-label drugs and lower gestational age, low birth weight, lower 5-minute Apgar score, advanced resuscitation maneuver in the delivery room and death. The prescription of unlicensed drugs was associated with lower gestational age, low birth weight and 5-minute Apgar score below 7.
Conclusion:
Neonates admitted to neonatal intensive care units are highly exposed to off-label and unlicensed medications. Further studies are needed to achieve greater safety and quality of drug therapy used in neonatology.
- Verônica Cheles Vieira
-
Original Article
Association of uteroglobin-related protein 1 with smoke inhalation injury severity
- Sabrina Frighetto Henrich,
- Tatiana Helena Rech ,
- Cristiane Ritter,
- Monique Michels ,
- Felipe Dal-Pizzol , [ … ],
- Gilberto Friedman
Abstract
Original ArticleAssociation of uteroglobin-related protein 1 with smoke inhalation injury severity
Rev Bras Ter Intensiva. 2021;33(2):276-281
DOI 10.5935/0103-507X.20210035
- Sabrina Frighetto Henrich,
- Tatiana Helena Rech ,
- Cristiane Ritter,
- Monique Michels ,
- Felipe Dal-Pizzol ,
- Gilberto Friedman
Views1See moreABSTRACT
Objective:
To evaluate serum uteroglobin-related protein 1 expression early after smoke inhalation injuries and its association with the severity of inhalation injury in burned patients.
Methods:
Smoke or chemical inhalation injury is associated with morbidity and mortality. The consequences of inhalation result from an inflammatory response. Uteroglobin-related protein 1 is an anti-inflammatory protein and may improve lung inflammation. We hypothesized that uteroglobin-related protein 1 levels could reflect disease severity and predict outcome in patients with inhalation injury. Sixteen patients diagnosed with acute respiratory distress syndrome secondary to smoke inhalation injury were prospectively included in the study. Plasma was collected upon intensive care unit admission and within 24 hours of the inhalation injury. Bronchoscopies were carried out in all patients to assess the severity of inhalation injury within 72 hours. Uteroglobin-related protein 1 plasma levels were determined in duplicate with enzyme-linked immunosorbent assay.
Results:
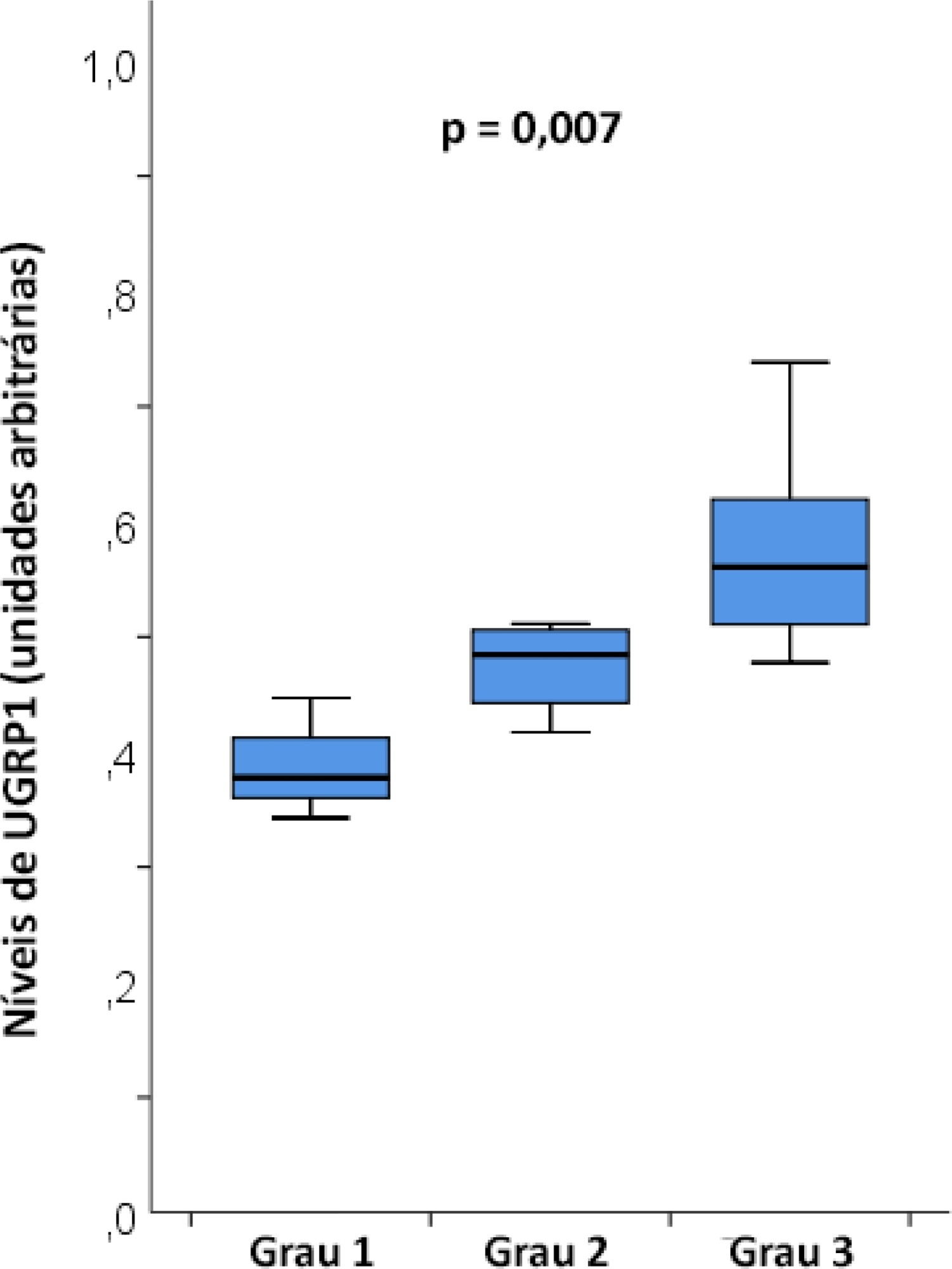
The mean age was 23 ± 5 years, and the inhalation injury distribution was as follows: three of grade 1, four of grade 2, and nine of grade 3. The level of uteroglobin-related protein 1 was related to inhalation severity (grade 1: 0.389 ± 0.053 arbitrary units versus grade 2: 0.474 ± 0.0423 arbitrary units versus grade 3: 0.580 ± 0.094 arbitrary units; p = 0.007).
Conclusion:
Plasma levels of uteroglobin-related protein 1 are associated with the degree of lung inhalation injury.
Views1Abstract
Original ArticleAssociation of uteroglobin-related protein 1 with smoke inhalation injury severity
Rev Bras Ter Intensiva. 2021;33(2):276-281
DOI 10.5935/0103-507X.20210035
- Sabrina Frighetto Henrich,
- Tatiana Helena Rech ,
- Cristiane Ritter,
- Monique Michels ,
- Felipe Dal-Pizzol ,
- Gilberto Friedman
Views1See moreABSTRACT
Objective:
To evaluate serum uteroglobin-related protein 1 expression early after smoke inhalation injuries and its association with the severity of inhalation injury in burned patients.
Methods:
Smoke or chemical inhalation injury is associated with morbidity and mortality. The consequences of inhalation result from an inflammatory response. Uteroglobin-related protein 1 is an anti-inflammatory protein and may improve lung inflammation. We hypothesized that uteroglobin-related protein 1 levels could reflect disease severity and predict outcome in patients with inhalation injury. Sixteen patients diagnosed with acute respiratory distress syndrome secondary to smoke inhalation injury were prospectively included in the study. Plasma was collected upon intensive care unit admission and within 24 hours of the inhalation injury. Bronchoscopies were carried out in all patients to assess the severity of inhalation injury within 72 hours. Uteroglobin-related protein 1 plasma levels were determined in duplicate with enzyme-linked immunosorbent assay.
Results:
The mean age was 23 ± 5 years, and the inhalation injury distribution was as follows: three of grade 1, four of grade 2, and nine of grade 3. The level of uteroglobin-related protein 1 was related to inhalation severity (grade 1: 0.389 ± 0.053 arbitrary units versus grade 2: 0.474 ± 0.0423 arbitrary units versus grade 3: 0.580 ± 0.094 arbitrary units; p = 0.007).
Conclusion:
Plasma levels of uteroglobin-related protein 1 are associated with the degree of lung inhalation injury.
-
Original Article
Traumatic brain injury hospital incidence in Brazil: an analysis of the past 10 years
Rev Bras Ter Intensiva. 2021;33(2):282-289
Abstract
Original ArticleTraumatic brain injury hospital incidence in Brazil: an analysis of the past 10 years
Rev Bras Ter Intensiva. 2021;33(2):282-289
DOI 10.5935/0103-507X.20210036
Views1Abstract
Objetivo:
Caracterizar os aspectos demográficos e sociais e o ônus econômico do traumatismo craniencefálico no sistema público de saúde brasileiro na última década.
Métodos:
Analisaram-se os dados provenientes da base de dados do Departamento de Informática do Sistema Único de Saúde referentes ao período entre janeiro de 2008 e dezembro de 2019.
Resultados:
Entre 2008 e 2019 ocorreram, em média, no Brasil, 131.014,83 internações por traumatismo craniencefálico ao ano, com incidência de 65,54 por 100 mil habitantes. Deve-se salientar a elevada incidência de traumatismo craniencefálico em adultos idosos (acima de 70 anos), acompanhada de altas taxas de mortalidade. Além disso, há também elevada incidência de traumatismo craniencefálico em adultos jovens (20 a 29 anos e 30 a 39 anos). Os dados aqui apresentados demonstram uma proporção de traumatismos craniencefálicos de 3,6 homens/mulheres.
Conclusão:
Embora se acredite que os dados apresentados subestimem a incidência e mortalidade associadas com o traumatismo craniencefálico no Brasil, este estudo pode ajudar na implantação de futuras estratégias de promoção da saúde para a população brasileira e mundial, com o objetivo de diminuir a incidência, a mortalidade e os custos do traumatismo craniencefálico.
Keywords:BrasilIncidênciaLesões encefálicas traumáticas/epidemiologiaLesões encefálicas traumáticas/mortalidadeSee moreViews1Abstract
Original ArticleTraumatic brain injury hospital incidence in Brazil: an analysis of the past 10 years
Rev Bras Ter Intensiva. 2021;33(2):282-289
DOI 10.5935/0103-507X.20210036
Views1Abstract
Objetivo:
Caracterizar os aspectos demográficos e sociais e o ônus econômico do traumatismo craniencefálico no sistema público de saúde brasileiro na última década.
Métodos:
Analisaram-se os dados provenientes da base de dados do Departamento de Informática do Sistema Único de Saúde referentes ao período entre janeiro de 2008 e dezembro de 2019.
Resultados:
Entre 2008 e 2019 ocorreram, em média, no Brasil, 131.014,83 internações por traumatismo craniencefálico ao ano, com incidência de 65,54 por 100 mil habitantes. Deve-se salientar a elevada incidência de traumatismo craniencefálico em adultos idosos (acima de 70 anos), acompanhada de altas taxas de mortalidade. Além disso, há também elevada incidência de traumatismo craniencefálico em adultos jovens (20 a 29 anos e 30 a 39 anos). Os dados aqui apresentados demonstram uma proporção de traumatismos craniencefálicos de 3,6 homens/mulheres.
Conclusão:
Embora se acredite que os dados apresentados subestimem a incidência e mortalidade associadas com o traumatismo craniencefálico no Brasil, este estudo pode ajudar na implantação de futuras estratégias de promoção da saúde para a população brasileira e mundial, com o objetivo de diminuir a incidência, a mortalidade e os custos do traumatismo craniencefálico.
Keywords:BrasilIncidênciaLesões encefálicas traumáticas/epidemiologiaLesões encefálicas traumáticas/mortalidadeSee more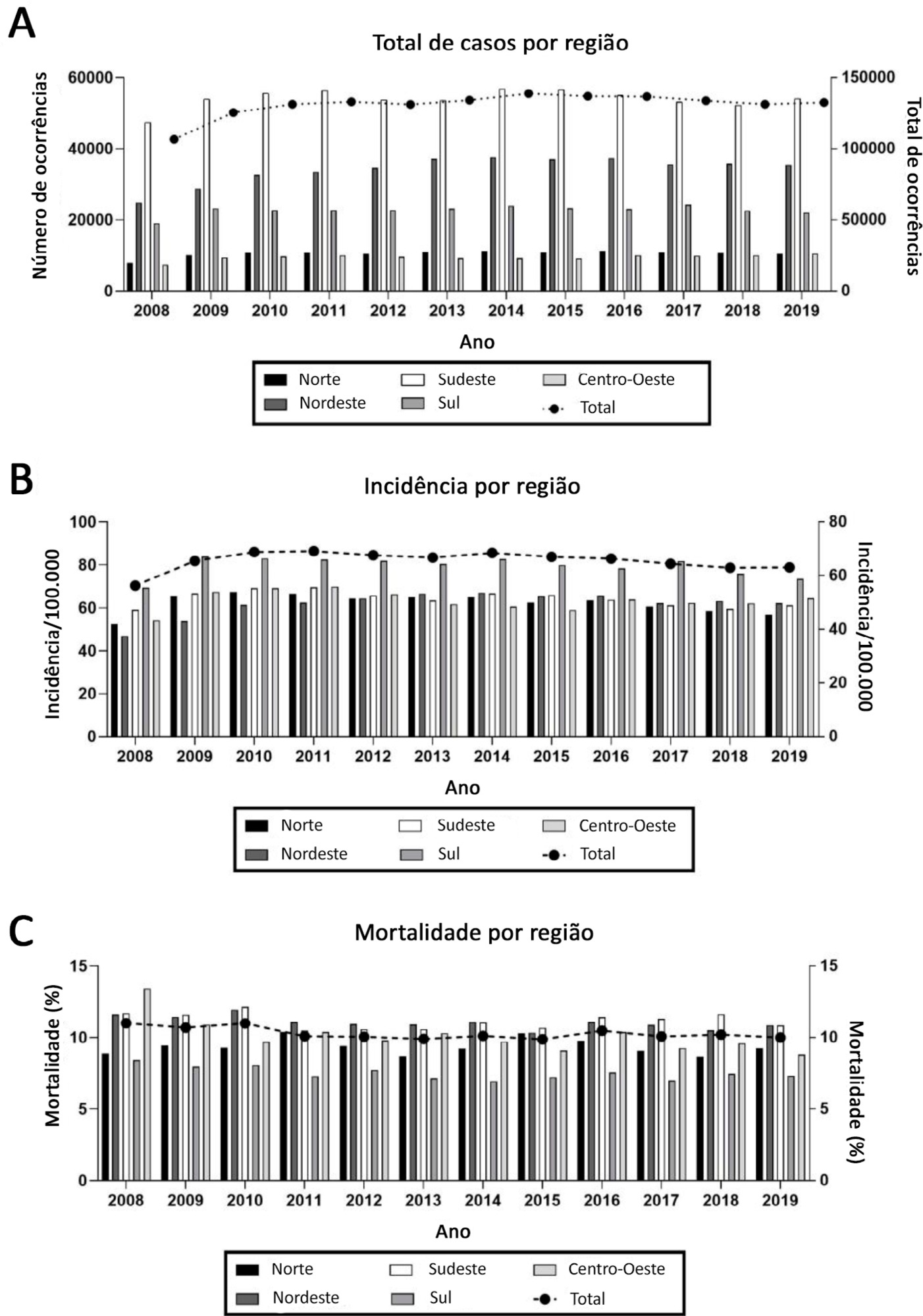
-
Original Article
New procedures for the confirmation of brain death in Brazil: results from the Central Estadual de Transplantes de Santa Catarina
Rev Bras Ter Intensiva. 2021;33(2):290-297
Abstract
Original ArticleNew procedures for the confirmation of brain death in Brazil: results from the Central Estadual de Transplantes de Santa Catarina
Rev Bras Ter Intensiva. 2021;33(2):290-297
DOI 10.5935/0103-507X.20210037
Views1See moreABSTRACT
Objective:
To analyze the impact of Resolution 2.173/2017 of the Federal Council of Medicine on results from the Central Estadual de Transplantes de Santa Catarina.
Methods:
This was a cross-sectional observational study of medical records of all patients (1,605) with suspected brain death notified to the Central Estadual de Transplantes de Santa Catarina; for this study, procedures to confirm this diagnosis were initiated between July 2016 and December 2017 and between January 2018 and June 2019. The median duration of the protocol in each period was considered for the comparison between the intervals. The collected data were transformed into rates (per million population). The mean rates for the periods before and after the implementation of the protocol were analyzed by Student’s t-test, and qualitative variables were analyzed by Pearson’s chi-squared test.
Results:
The mean duration of brain death confirmation procedures decreased more than 1 hour in the second period compared to the first period, with statistical significance (p = 0.001). The rates of harvested livers and transplanted pancreas, the number of notifications by hospital size and the rate of cardiac arrest in the macro-region of the Itajaí Valley were significantly different between the two periods.
Conclusion:
In the period after the new resolution on brain death, there was a reduction in the duration for diagnosis. However, other indicators did not change significantly, providing evidence for the multidimensional nature of the organ transplantation process in Santa Catarina and the need for further studies to better understand and optimize the process.
Views1Abstract
Original ArticleNew procedures for the confirmation of brain death in Brazil: results from the Central Estadual de Transplantes de Santa Catarina
Rev Bras Ter Intensiva. 2021;33(2):290-297
DOI 10.5935/0103-507X.20210037
Views1See moreABSTRACT
Objective:
To analyze the impact of Resolution 2.173/2017 of the Federal Council of Medicine on results from the Central Estadual de Transplantes de Santa Catarina.
Methods:
This was a cross-sectional observational study of medical records of all patients (1,605) with suspected brain death notified to the Central Estadual de Transplantes de Santa Catarina; for this study, procedures to confirm this diagnosis were initiated between July 2016 and December 2017 and between January 2018 and June 2019. The median duration of the protocol in each period was considered for the comparison between the intervals. The collected data were transformed into rates (per million population). The mean rates for the periods before and after the implementation of the protocol were analyzed by Student’s t-test, and qualitative variables were analyzed by Pearson’s chi-squared test.
Results:
The mean duration of brain death confirmation procedures decreased more than 1 hour in the second period compared to the first period, with statistical significance (p = 0.001). The rates of harvested livers and transplanted pancreas, the number of notifications by hospital size and the rate of cardiac arrest in the macro-region of the Itajaí Valley were significantly different between the two periods.
Conclusion:
In the period after the new resolution on brain death, there was a reduction in the duration for diagnosis. However, other indicators did not change significantly, providing evidence for the multidimensional nature of the organ transplantation process in Santa Catarina and the need for further studies to better understand and optimize the process.
-
Original Article
Performance status and acute organ dysfunction influence hospital mortality in critically ill patients with cancer and suspected infection: a retrospective cohort analysis
Rev Bras Ter Intensiva. 2021;33(2):298-303
Abstract
Original ArticlePerformance status and acute organ dysfunction influence hospital mortality in critically ill patients with cancer and suspected infection: a retrospective cohort analysis
Rev Bras Ter Intensiva. 2021;33(2):298-303
DOI 10.5935/0103-507X.20210038
Views1See moreABSTRACT
Objective:
To evaluate how performance status impairment and acute organ dysfunction influence hospital mortality in critically ill patients with cancer who were admitted with suspected sepsis.
Methods:
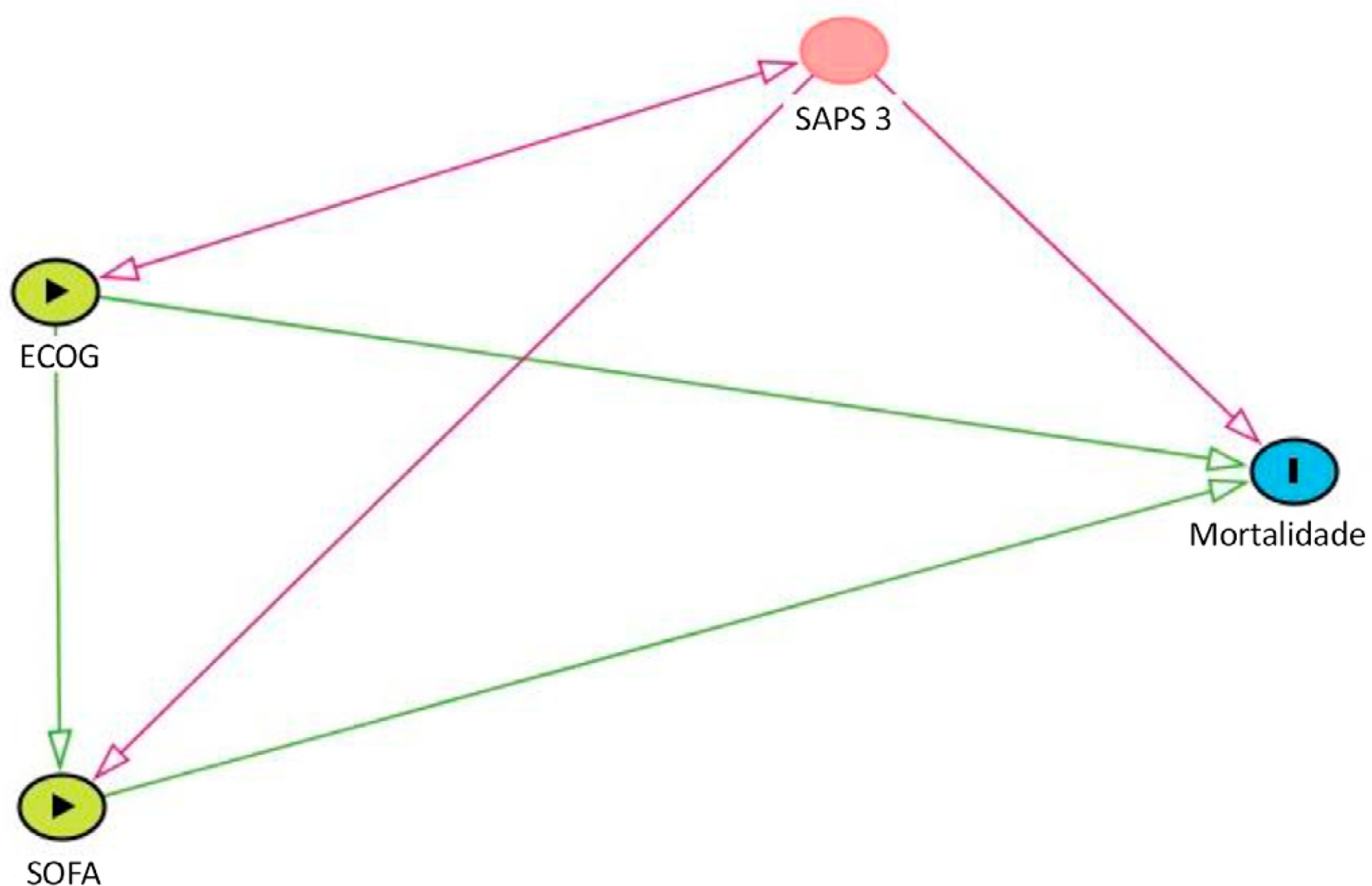
Data were obtained from a retrospective cohort of patients, admitted to an intensive care unit, with cancer and with a suspected infection who received parenteral antibiotics and underwent the collection of bodily fluid samples. We used logistic regression with hospital mortality as the outcome and the Sequential Organ Failure Assessment score, Eastern Cooperative Oncology Group status, and their interactions as predictors.
Results:
Of 450 patients included, 265 (58.9%) died in the hospital. For patients admitted to the intensive care unit with lower Sequential Organ Failure Assessment (≤ 6), performance status impairment influenced the in-hospital mortality, which was 32% among those with no and minor performance status impairment and 52% among those with moderate and severe performance status impairment, p < 0.01. However, for those with higher Sequential Organ Failure Assessment (> 6), performance status impairment did not influence the in-hospital mortality (73% among those with no and minor impairment and 84% among those with moderate and severe impairment; p = 0.1).
Conclusion:
Performance status impairment seems to influence hospital mortality in critically ill cancer patients with suspected sepsis when they have less severe acute organ dysfunction at the time of intensive care unit admission.
Views1Abstract
Original ArticlePerformance status and acute organ dysfunction influence hospital mortality in critically ill patients with cancer and suspected infection: a retrospective cohort analysis
Rev Bras Ter Intensiva. 2021;33(2):298-303
DOI 10.5935/0103-507X.20210038
Views1See moreABSTRACT
Objective:
To evaluate how performance status impairment and acute organ dysfunction influence hospital mortality in critically ill patients with cancer who were admitted with suspected sepsis.
Methods:
Data were obtained from a retrospective cohort of patients, admitted to an intensive care unit, with cancer and with a suspected infection who received parenteral antibiotics and underwent the collection of bodily fluid samples. We used logistic regression with hospital mortality as the outcome and the Sequential Organ Failure Assessment score, Eastern Cooperative Oncology Group status, and their interactions as predictors.
Results:
Of 450 patients included, 265 (58.9%) died in the hospital. For patients admitted to the intensive care unit with lower Sequential Organ Failure Assessment (≤ 6), performance status impairment influenced the in-hospital mortality, which was 32% among those with no and minor performance status impairment and 52% among those with moderate and severe performance status impairment, p < 0.01. However, for those with higher Sequential Organ Failure Assessment (> 6), performance status impairment did not influence the in-hospital mortality (73% among those with no and minor impairment and 84% among those with moderate and severe impairment; p = 0.1).
Conclusion:
Performance status impairment seems to influence hospital mortality in critically ill cancer patients with suspected sepsis when they have less severe acute organ dysfunction at the time of intensive care unit admission.
-
Review Article
Extubation in the pediatric intensive care unit: predictive methods. An integrative literature review
- Jéssica Cristina da Silva Moura ,
- Lívea Gianfrancesco,
- Tiago Henrique de Souza,
- Taís Daiene Russo Hortencio,
- Roberto José Negrão Nogueira
Abstract
Review ArticleExtubation in the pediatric intensive care unit: predictive methods. An integrative literature review
Rev Bras Ter Intensiva. 2021;33(2):304-311
DOI 10.5935/0103-507X.20210039
- Jéssica Cristina da Silva Moura ,
- Lívea Gianfrancesco,
- Tiago Henrique de Souza,
- Taís Daiene Russo Hortencio,
- Roberto José Negrão Nogueira
Views0See moreABSTRACT
For extubation in pediatric patients, the evaluation of readiness is strongly recommended. However, a device or practice that is superior to clinical judgment has not yet been accurately determined. Thus, it is important to conduct a review on the techniques of choice in clinical practice to predict extubation failure in pediatric patients. Based on a search in the PubMed®, Biblioteca Virtual em Saúde, Cochrane Library and Scopus databases, we conducted a survey of the predictive variables of extubation failure most commonly used in clinical practice in pediatric patients. Of the eight predictors described, the three most commonly used were the spontaneous breathing test, the rapid shallow breathing index and maximum inspiratory pressure. Although the disparity of the data presented in the studies prevented statistical treatment, it was still possible to describe and analyze the performance of these tests.
Views0Abstract
Review ArticleExtubation in the pediatric intensive care unit: predictive methods. An integrative literature review
Rev Bras Ter Intensiva. 2021;33(2):304-311
DOI 10.5935/0103-507X.20210039
- Jéssica Cristina da Silva Moura ,
- Lívea Gianfrancesco,
- Tiago Henrique de Souza,
- Taís Daiene Russo Hortencio,
- Roberto José Negrão Nogueira
Views0See moreABSTRACT
For extubation in pediatric patients, the evaluation of readiness is strongly recommended. However, a device or practice that is superior to clinical judgment has not yet been accurately determined. Thus, it is important to conduct a review on the techniques of choice in clinical practice to predict extubation failure in pediatric patients. Based on a search in the PubMed®, Biblioteca Virtual em Saúde, Cochrane Library and Scopus databases, we conducted a survey of the predictive variables of extubation failure most commonly used in clinical practice in pediatric patients. Of the eight predictors described, the three most commonly used were the spontaneous breathing test, the rapid shallow breathing index and maximum inspiratory pressure. Although the disparity of the data presented in the studies prevented statistical treatment, it was still possible to describe and analyze the performance of these tests.
- Jéssica Cristina da Silva Moura
-
Review Article
What outcomes should be evaluated in critically ill patients?
Rev Bras Ter Intensiva. 2021;33(2):312-319
Abstract
Review ArticleWhat outcomes should be evaluated in critically ill patients?
Rev Bras Ter Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Views2See moreABSTRACT
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
Views2Abstract
Review ArticleWhat outcomes should be evaluated in critically ill patients?
Rev Bras Ter Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Views2See moreABSTRACT
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
-
Case Report
Influenza B infection and Kawasaki disease in an adolescent during the COVID-19 pandemic: a case report
- Jéssica de Oliveira Silveira ,
- Mariana Grando Pegoraro,
- Juliana Ferreira Ferranti ,
- Albert Bousso,
- Tadeu Silveira Martins Renattini
Abstract
Case ReportInfluenza B infection and Kawasaki disease in an adolescent during the COVID-19 pandemic: a case report
Rev Bras Ter Intensiva. 2021;33(2):320-324
DOI 10.5935/0103-507X.20210041
- Jéssica de Oliveira Silveira ,
- Mariana Grando Pegoraro,
- Juliana Ferreira Ferranti ,
- Albert Bousso,
- Tadeu Silveira Martins Renattini
Views0ABSTRACT
We report a case of Influenza B infection and Kawasaki disease in an adolescent, diagnosed during the COVID-19 pandemic. An asthmatic female adolescent presented with fever and flu-like symptoms for 7 days and was admitted with acute respiratory failure requiring mechanical ventilation. She progressed with hemodynamic instability responsive to vasoactive drugs. Antibiotic therapy and support measures were introduced, showing progressive hemodynamics and respiratory improvement, however with persistent fever and increased inflammatory markers. During the hospitalization, she developed bilateral non-purulent conjunctivitis, hand and feet desquamation, strawberry tongue, and cervical adenopathy, and was diagnosed with Kawasaki disease. She was prescribed intravenous immunoglobulin and, due to the refractory clinical conditions, corticosteroid therapy was added; 24 hours later, the patient was afebrile. No coronary changes were found. A full viral panel including COVID-19 C-reactive protein and serology could only isolate the Influenza B virus. During the hospitalization, she was diagnosed with pulmonary thromboembolism; coagulopathies were investigated, and she was diagnosed with heterozygous factor V Leiden mutation. There is a potential association between Kawasaki disease and infection with Influenza B or with other viruses such as coronavirus. Therefore, this association should be considered in pediatric patients, adolescents included, with prolonged febrile conditions.
Keywords:adolescentCoronavirus infectionsCOVID-19Influenza B virusMucocutaneous lymph node syndromeRespiratory insufficiencySARS-CoV-2See moreViews0Abstract
Case ReportInfluenza B infection and Kawasaki disease in an adolescent during the COVID-19 pandemic: a case report
Rev Bras Ter Intensiva. 2021;33(2):320-324
DOI 10.5935/0103-507X.20210041
- Jéssica de Oliveira Silveira ,
- Mariana Grando Pegoraro,
- Juliana Ferreira Ferranti ,
- Albert Bousso,
- Tadeu Silveira Martins Renattini
Views0ABSTRACT
We report a case of Influenza B infection and Kawasaki disease in an adolescent, diagnosed during the COVID-19 pandemic. An asthmatic female adolescent presented with fever and flu-like symptoms for 7 days and was admitted with acute respiratory failure requiring mechanical ventilation. She progressed with hemodynamic instability responsive to vasoactive drugs. Antibiotic therapy and support measures were introduced, showing progressive hemodynamics and respiratory improvement, however with persistent fever and increased inflammatory markers. During the hospitalization, she developed bilateral non-purulent conjunctivitis, hand and feet desquamation, strawberry tongue, and cervical adenopathy, and was diagnosed with Kawasaki disease. She was prescribed intravenous immunoglobulin and, due to the refractory clinical conditions, corticosteroid therapy was added; 24 hours later, the patient was afebrile. No coronary changes were found. A full viral panel including COVID-19 C-reactive protein and serology could only isolate the Influenza B virus. During the hospitalization, she was diagnosed with pulmonary thromboembolism; coagulopathies were investigated, and she was diagnosed with heterozygous factor V Leiden mutation. There is a potential association between Kawasaki disease and infection with Influenza B or with other viruses such as coronavirus. Therefore, this association should be considered in pediatric patients, adolescents included, with prolonged febrile conditions.
Keywords:adolescentCoronavirus infectionsCOVID-19Influenza B virusMucocutaneous lymph node syndromeRespiratory insufficiencySARS-CoV-2See more
- Jéssica de Oliveira Silveira
-
Case Report
NEUROLOGICAL DYSFUNCTION ASSOCIATED WITH COVID-19
- Filipa Sofia Camacho Alves da Silva ,
- Alexei Bucur,
- Steeve Neves Rosado,
- Sílvia dos Santos Balhana,
- Carlos Manuel Meneses-Oliveira
Abstract
Case ReportNEUROLOGICAL DYSFUNCTION ASSOCIATED WITH COVID-19
Rev Bras Ter Intensiva. 2021;33(2):325-325
DOI 10.5935/0103-507X.20210042
- Filipa Sofia Camacho Alves da Silva ,
- Alexei Bucur,
- Steeve Neves Rosado,
- Sílvia dos Santos Balhana,
- Carlos Manuel Meneses-Oliveira
Views0ABSTRACT
COVID-19 was declared a pandemic by the World Health Organization on March 11, 2020. The clinical presentation is predominantly respiratory symptoms; however, in the current literature, several neurological manifestations associated with SARS-CoV-2 infection have been described. The authors present the clinical case of a 45-year-old man hospitalized for pneumonia with a positive test result for SARS-CoV-2, without a neurological history, who, on the sixteenth day of hospitalization, presented a sudden change in his state of consciousness accompanied by conjugated right gaze deviation and myoclonus of the face and thoracic region to the left, followed by generalized tonic-clonic seizures associated with persistent left hemiparesis. The present study highlights a positive RT-PCR test for SARS-CoV-2 in cerebrospinal fluid. The patient progressed with gradual improvement, and the outcome was favorable.
Keywords:Cerebrospinal fluidCoronavirus infectionsCOVID-19EncephalitisMeningoencephalitisNeurological manifestationsSARS-CoV-2See moreViews0Abstract
Case ReportNEUROLOGICAL DYSFUNCTION ASSOCIATED WITH COVID-19
Rev Bras Ter Intensiva. 2021;33(2):325-325
DOI 10.5935/0103-507X.20210042
- Filipa Sofia Camacho Alves da Silva ,
- Alexei Bucur,
- Steeve Neves Rosado,
- Sílvia dos Santos Balhana,
- Carlos Manuel Meneses-Oliveira
Views0ABSTRACT
COVID-19 was declared a pandemic by the World Health Organization on March 11, 2020. The clinical presentation is predominantly respiratory symptoms; however, in the current literature, several neurological manifestations associated with SARS-CoV-2 infection have been described. The authors present the clinical case of a 45-year-old man hospitalized for pneumonia with a positive test result for SARS-CoV-2, without a neurological history, who, on the sixteenth day of hospitalization, presented a sudden change in his state of consciousness accompanied by conjugated right gaze deviation and myoclonus of the face and thoracic region to the left, followed by generalized tonic-clonic seizures associated with persistent left hemiparesis. The present study highlights a positive RT-PCR test for SARS-CoV-2 in cerebrospinal fluid. The patient progressed with gradual improvement, and the outcome was favorable.
Keywords:Cerebrospinal fluidCoronavirus infectionsCOVID-19EncephalitisMeningoencephalitisNeurological manifestationsSARS-CoV-2See more - Filipa Sofia Camacho Alves da Silva
-
Case Report
Reversible contrast-induced encephalopathy after coil embolization of epistaxis
- Guilherme Menezes Mescolotte ,
- Fernando Rodrigues da Silva,
- Susana Afonso,
- Jaime Pamplona,
- Rui Moreno
Abstract
Case ReportReversible contrast-induced encephalopathy after coil embolization of epistaxis
Rev Bras Ter Intensiva. 2021;33(2):331-335
DOI 10.5935/0103-507X.20210043
- Guilherme Menezes Mescolotte ,
- Fernando Rodrigues da Silva,
- Susana Afonso,
- Jaime Pamplona,
- Rui Moreno
Views0ABSTRACT
A 37-year-old woman (35 weeks pregnant) was admitted to a local hospital due to severe epistaxis resulting in shock and the need for emergency cesarean section. After failure to tamponade the bleeding, angiographic treatment was provided. After the procedure, she was admitted to the neurocritical intensive care unit and was confused and agitated, requiring sedation and endotracheal intubation. In the intensive care unit, diagnostic investigations included brain magnetic resonance imaging, lumbar puncture with viral panel, electroencephalogram, tests for autoimmunity, and hydroelectrolytic and metabolic evaluations. Magnetic resonance imaging showed a puntiform restricted diffusion area on the left corona radiata on diffusion weighted imaging and mild cortical posterior edema (without restricted diffusion), and an electroencephalogram showed moderate diffuse slow activity and fronto-temporal slow activity of the left hemisphere with associated scarce paroxysmal components. The other exams did not show any relevant alterations. Due to the temporal relationship, the clinical history and the magnetic resonance imaging results, a diagnosis of contrast-induced encephalopathy was made. After 2 days in the intensive care unit, sedation was withdrawn, the patient was extubated, and total neurological recovery was verified within the next 24 hours.
Keywords:Brain diseases/chemically inducedContrast media/adverse effectsEpistaxisPregnancy complicationsSee moreViews0Abstract
Case ReportReversible contrast-induced encephalopathy after coil embolization of epistaxis
Rev Bras Ter Intensiva. 2021;33(2):331-335
DOI 10.5935/0103-507X.20210043
- Guilherme Menezes Mescolotte ,
- Fernando Rodrigues da Silva,
- Susana Afonso,
- Jaime Pamplona,
- Rui Moreno
Views0ABSTRACT
A 37-year-old woman (35 weeks pregnant) was admitted to a local hospital due to severe epistaxis resulting in shock and the need for emergency cesarean section. After failure to tamponade the bleeding, angiographic treatment was provided. After the procedure, she was admitted to the neurocritical intensive care unit and was confused and agitated, requiring sedation and endotracheal intubation. In the intensive care unit, diagnostic investigations included brain magnetic resonance imaging, lumbar puncture with viral panel, electroencephalogram, tests for autoimmunity, and hydroelectrolytic and metabolic evaluations. Magnetic resonance imaging showed a puntiform restricted diffusion area on the left corona radiata on diffusion weighted imaging and mild cortical posterior edema (without restricted diffusion), and an electroencephalogram showed moderate diffuse slow activity and fronto-temporal slow activity of the left hemisphere with associated scarce paroxysmal components. The other exams did not show any relevant alterations. Due to the temporal relationship, the clinical history and the magnetic resonance imaging results, a diagnosis of contrast-induced encephalopathy was made. After 2 days in the intensive care unit, sedation was withdrawn, the patient was extubated, and total neurological recovery was verified within the next 24 hours.
Keywords:Brain diseases/chemically inducedContrast media/adverse effectsEpistaxisPregnancy complicationsSee more
- Guilherme Menezes Mescolotte
-
Letter to the Editor
To: Memory box: possibilities to support grief in the intensive care unit during the COVID-19 pandemic
Rev Bras Ter Intensiva. 2021;33(2):336-336
Abstract
Letter to the EditorTo: Memory box: possibilities to support grief in the intensive care unit during the COVID-19 pandemic
Rev Bras Ter Intensiva. 2021;33(2):336-336
DOI 10.5935/0103-507X.20210044
Views0Dear editor, We would like to share ideas on the publication “Memory box: possibilities to support grief in the intensive care unit during the COVID-19 pandemic.”() Luiz et al. reported on the use of Memory box as a tool to support grief, and concluded that “Providing bereavement support is one of the possibilities we consider […]See moreViews0Abstract
Letter to the EditorTo: Memory box: possibilities to support grief in the intensive care unit during the COVID-19 pandemic
Rev Bras Ter Intensiva. 2021;33(2):336-336
DOI 10.5935/0103-507X.20210044
Views0Dear editor, We would like to share ideas on the publication “Memory box: possibilities to support grief in the intensive care unit during the COVID-19 pandemic.”() Luiz et al. reported on the use of Memory box as a tool to support grief, and concluded that “Providing bereavement support is one of the possibilities we consider […]See more -
Author’s Response
Reply to: Memory box: possibilities to support grief in the intensive care unit during the COVID-19 pandemic
- Thábata da Silva Cardoso Luiz ,
- Orli Carvalho da Silva Filho ,
- Tânia Cristina Camacho Ventura,
- Virginia Dresch
Abstract
Author’s ResponseReply to: Memory box: possibilities to support grief in the intensive care unit during the COVID-19 pandemic
Rev Bras Ter Intensiva. 2021;33(2):337-338
DOI 10.5935/0103-507X.20210045
- Thábata da Silva Cardoso Luiz ,
- Orli Carvalho da Silva Filho ,
- Tânia Cristina Camacho Ventura,
- Virginia Dresch
Views0Dear Editor, Regarding the comments related to the memory box intervention we described in our article,() we are confident that this dialogue can qualify and value the transversality of mental health during the coronavirus 2019 disease (COVID-19) pandemic, as recommended by the World Health Organization (WHO) in a technical note issued shortly after this current […]See moreViews0Abstract
Author’s ResponseReply to: Memory box: possibilities to support grief in the intensive care unit during the COVID-19 pandemic
Rev Bras Ter Intensiva. 2021;33(2):337-338
DOI 10.5935/0103-507X.20210045
- Thábata da Silva Cardoso Luiz ,
- Orli Carvalho da Silva Filho ,
- Tânia Cristina Camacho Ventura,
- Virginia Dresch
Views0Dear Editor, Regarding the comments related to the memory box intervention we described in our article,() we are confident that this dialogue can qualify and value the transversality of mental health during the coronavirus 2019 disease (COVID-19) pandemic, as recommended by the World Health Organization (WHO) in a technical note issued shortly after this current […]See more - Thábata da Silva Cardoso Luiz
Volume Articles - Critical Care Science (CCS)
