Human Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(4):544-548
DOI 10.5935/0103-507X.20210082
To evaluate whether there was any impact on the number of pediatric extracorporeal membrane oxygenation runs and survival rates in the years subsequent to the 2009 pandemic.
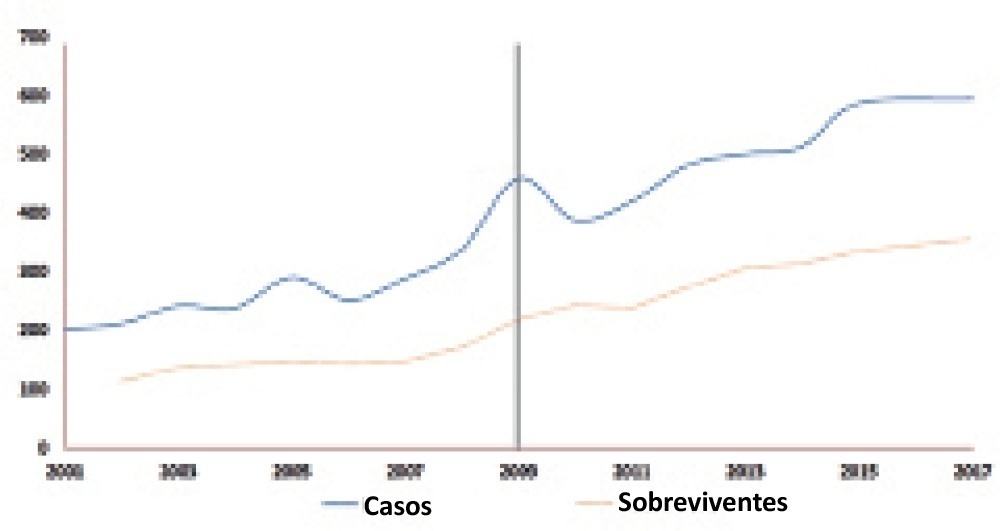
We studied two different periods of extracorporeal membrane oxygenation support for respiratory failure in children by analyzing datasets from the Extracorporeal Life Support Organization. Autoregressive integrated moving average models were constructed to estimate the effect of the pandemic. The year 2009 was the year of intervention (the H1N1 epidemic) in an interrupted time series model. Data collected from 2001 - 2010 were considered preintervention, and data collected from 2010 - 2017 were considered postintervention.
There was an increase in survival rates in the period 2010 - 2017 compared to 2001 - 2010 (p < 0.0001), with a significant improvement in survival when extracorporeal membrane oxygenation was performed for acute respiratory failure due to viral pneumonia. The autoregressive integrated moving average model shows an increase of 23 extracorporeal membrane oxygenation runs per year, prior to the point of the level effect (2009). In terms of survival, the preslope shows that there was no significant increase in survival rates before 2009 (p = 0.41), but the level effect was nearly significant after two years (p = 0.05), with a 6% increase in survival. In four years, there was an 8% (p = 0.03) increase in survival, and six years after 2009, there was up to a 10% (p = 0.026) increase in survival.
In the years following 2009, there was a significant, global incremental increase in the extracorporeal membrane oxygenation survival rates for all runs, mainly due to improvements in the technology and treatment protocols for acute respiratory failure related to viral pneumonia and other respiratory conditions.
Abstract
Rev Bras Ter Intensiva. 2021;33(4):544-548
DOI 10.5935/0103-507X.20210082
To evaluate whether there was any impact on the number of pediatric extracorporeal membrane oxygenation runs and survival rates in the years subsequent to the 2009 pandemic.
We studied two different periods of extracorporeal membrane oxygenation support for respiratory failure in children by analyzing datasets from the Extracorporeal Life Support Organization. Autoregressive integrated moving average models were constructed to estimate the effect of the pandemic. The year 2009 was the year of intervention (the H1N1 epidemic) in an interrupted time series model. Data collected from 2001 - 2010 were considered preintervention, and data collected from 2010 - 2017 were considered postintervention.
There was an increase in survival rates in the period 2010 - 2017 compared to 2001 - 2010 (p < 0.0001), with a significant improvement in survival when extracorporeal membrane oxygenation was performed for acute respiratory failure due to viral pneumonia. The autoregressive integrated moving average model shows an increase of 23 extracorporeal membrane oxygenation runs per year, prior to the point of the level effect (2009). In terms of survival, the preslope shows that there was no significant increase in survival rates before 2009 (p = 0.41), but the level effect was nearly significant after two years (p = 0.05), with a 6% increase in survival. In four years, there was an 8% (p = 0.03) increase in survival, and six years after 2009, there was up to a 10% (p = 0.026) increase in survival.
In the years following 2009, there was a significant, global incremental increase in the extracorporeal membrane oxygenation survival rates for all runs, mainly due to improvements in the technology and treatment protocols for acute respiratory failure related to viral pneumonia and other respiratory conditions.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):313-317
DOI 10.1590/S0103-507X2008000300015
Anesthetic management of patients with severe chronic obstructive pulmonary disease is extensively discussed, due to the high rates of complications in this subtype of patients submitted to medium and high complexity surgical procedures. The objective of this study is to report use of noninvasive positive pressure mechanical ventilation - bilevel positive airway pressure - and spinal anesthesia in a patient with severe chronic obstructive pulmonary disease during total hip arthroplasty. An 81 year old, male patient with severe chronic obstructive pulmonary disease (GOLD 4) was submitted to total hip arthroplasty due to a femoral bone fracture under spinal anestesia and noninvasive positive pressure mechanical ventilation-bilevel positive airway pressure with expiratory pressure of 7 cmH2O, inspiratory pressure of 15 cmH2O and O2 flow of 3 L/min. During the procedure, the patient had one episode of bronchospasm that was promptly reverted pharmacologically with no complications in the postoperative period. The combination of less invasive anesthetic and ventilation techniques is easy to apply and may be useful in the perioperative management of patients with high anesthetic morbidity. Interaction between clinical, surgical and anesthetic teams for these cases is very important to reduce the mortality associated with extensive procedures in severe patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):313-317
DOI 10.1590/S0103-507X2008000300015
Anesthetic management of patients with severe chronic obstructive pulmonary disease is extensively discussed, due to the high rates of complications in this subtype of patients submitted to medium and high complexity surgical procedures. The objective of this study is to report use of noninvasive positive pressure mechanical ventilation - bilevel positive airway pressure - and spinal anesthesia in a patient with severe chronic obstructive pulmonary disease during total hip arthroplasty. An 81 year old, male patient with severe chronic obstructive pulmonary disease (GOLD 4) was submitted to total hip arthroplasty due to a femoral bone fracture under spinal anestesia and noninvasive positive pressure mechanical ventilation-bilevel positive airway pressure with expiratory pressure of 7 cmH2O, inspiratory pressure of 15 cmH2O and O2 flow of 3 L/min. During the procedure, the patient had one episode of bronchospasm that was promptly reverted pharmacologically with no complications in the postoperative period. The combination of less invasive anesthetic and ventilation techniques is easy to apply and may be useful in the perioperative management of patients with high anesthetic morbidity. Interaction between clinical, surgical and anesthetic teams for these cases is very important to reduce the mortality associated with extensive procedures in severe patients.

Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)