Original Article Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-pt
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
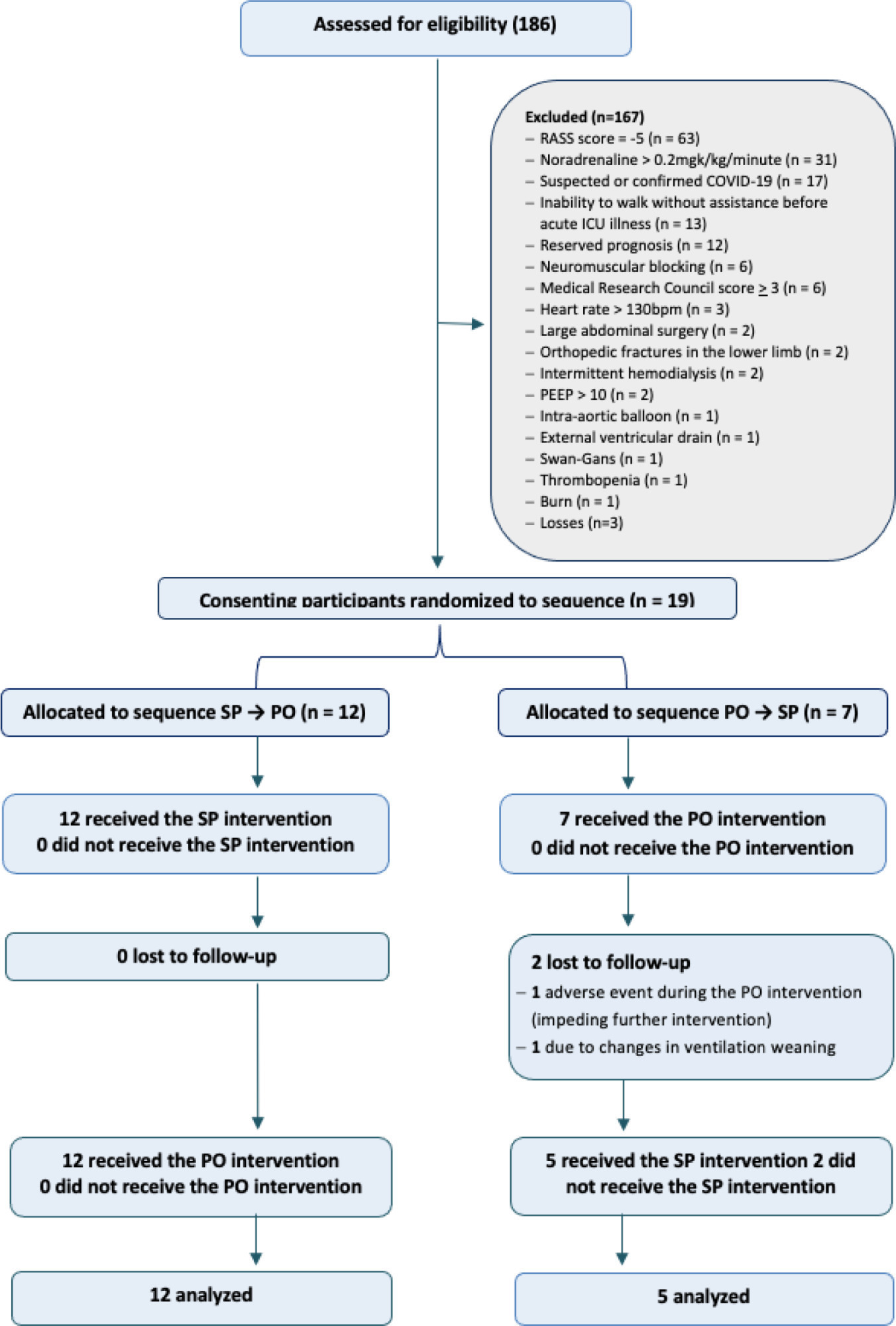
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Abstract
Crit Care Sci. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-pt
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Abstract
Crit Care Sci. 2023;35(4):377-385
DOI 10.5935/2965-2774.20230215-pt
To evaluate the occurrence of adverse events in the postoperative period of cardiac surgery in a pediatric intensive care unit and to find any patient characteristics that can predict such events.
This was a historical cohort study of patients recovering in the pediatric intensive care unit for the first 7 days after cardiac surgery between April and December 2019, by reviewing the medical records. The following were reviewed: demographic, clinical, and laboratory characteristics; patient severity scores; and selected adverse events, grouped into device-related, surgical, and nonsurgical.
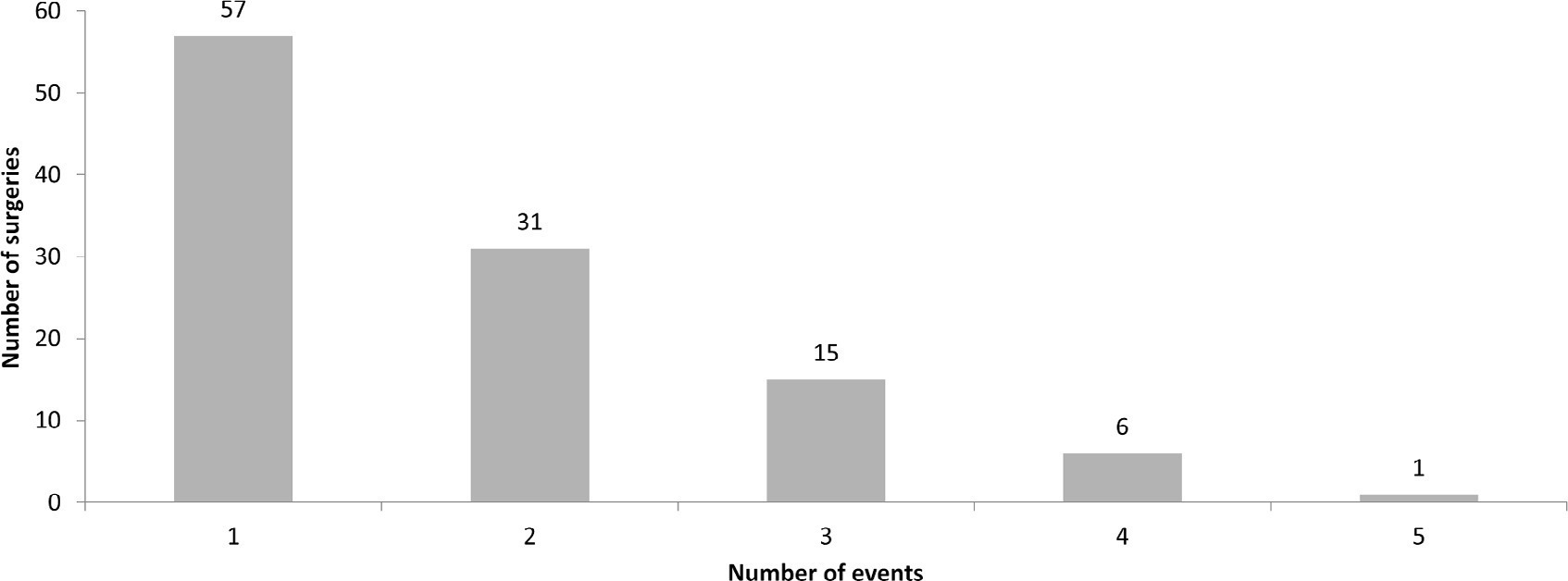
A total of 238 medical records were included. At least one adverse event occurred in 110 postoperative patients (46.2%). The total number of adverse events was 193 (81%). Vascular catheters were the most common cause, followed by cardiac arrest, bleeding, and surgical reexploration. In the univariate analysis, the vasoactive-inotropic score (VIS), Risk Adjustment in Congenital Heart Surgery (RACHS-1) score, age, Pediatric Index of Mortality (PIM-2), cardiopulmonary bypass and aortic clamping duration were significantly associated with adverse events. In the multivariate analysis, VIS ≥ 20 (OR 2.90; p = 0.004) and RACHS-1 ≥ 3 (OR 2.11; p = 0.019) were significant predictors, while age and delayed sternal closure showed only trends toward significance. To predict the occurrence of adverse events from VIS and RACHS-1, the area under the curve was 0.73 (95%CI 0.66 - 0.79).
Adverse events were quite frequent in children after cardiac surgery, especially those related to devices. The VIS and RACHS-1, used together, predicted the occurrence of adverse events well in this pediatric sample.
Abstract
Crit Care Sci. 2023;35(4):377-385
DOI 10.5935/2965-2774.20230215-pt
To evaluate the occurrence of adverse events in the postoperative period of cardiac surgery in a pediatric intensive care unit and to find any patient characteristics that can predict such events.
This was a historical cohort study of patients recovering in the pediatric intensive care unit for the first 7 days after cardiac surgery between April and December 2019, by reviewing the medical records. The following were reviewed: demographic, clinical, and laboratory characteristics; patient severity scores; and selected adverse events, grouped into device-related, surgical, and nonsurgical.
A total of 238 medical records were included. At least one adverse event occurred in 110 postoperative patients (46.2%). The total number of adverse events was 193 (81%). Vascular catheters were the most common cause, followed by cardiac arrest, bleeding, and surgical reexploration. In the univariate analysis, the vasoactive-inotropic score (VIS), Risk Adjustment in Congenital Heart Surgery (RACHS-1) score, age, Pediatric Index of Mortality (PIM-2), cardiopulmonary bypass and aortic clamping duration were significantly associated with adverse events. In the multivariate analysis, VIS ≥ 20 (OR 2.90; p = 0.004) and RACHS-1 ≥ 3 (OR 2.11; p = 0.019) were significant predictors, while age and delayed sternal closure showed only trends toward significance. To predict the occurrence of adverse events from VIS and RACHS-1, the area under the curve was 0.73 (95%CI 0.66 - 0.79).
Adverse events were quite frequent in children after cardiac surgery, especially those related to devices. The VIS and RACHS-1, used together, predicted the occurrence of adverse events well in this pediatric sample.
Abstract
Crit Care Sci. 2023;35(4):386-393
DOI 10.5935/2965-2774.20230190-pt
To assess the effect of atelectasis during mechanical ventilation on the periatelectatic and normal lung regions in a model of atelectasis in rats with acute lung injury induced by lipopolysaccharide.
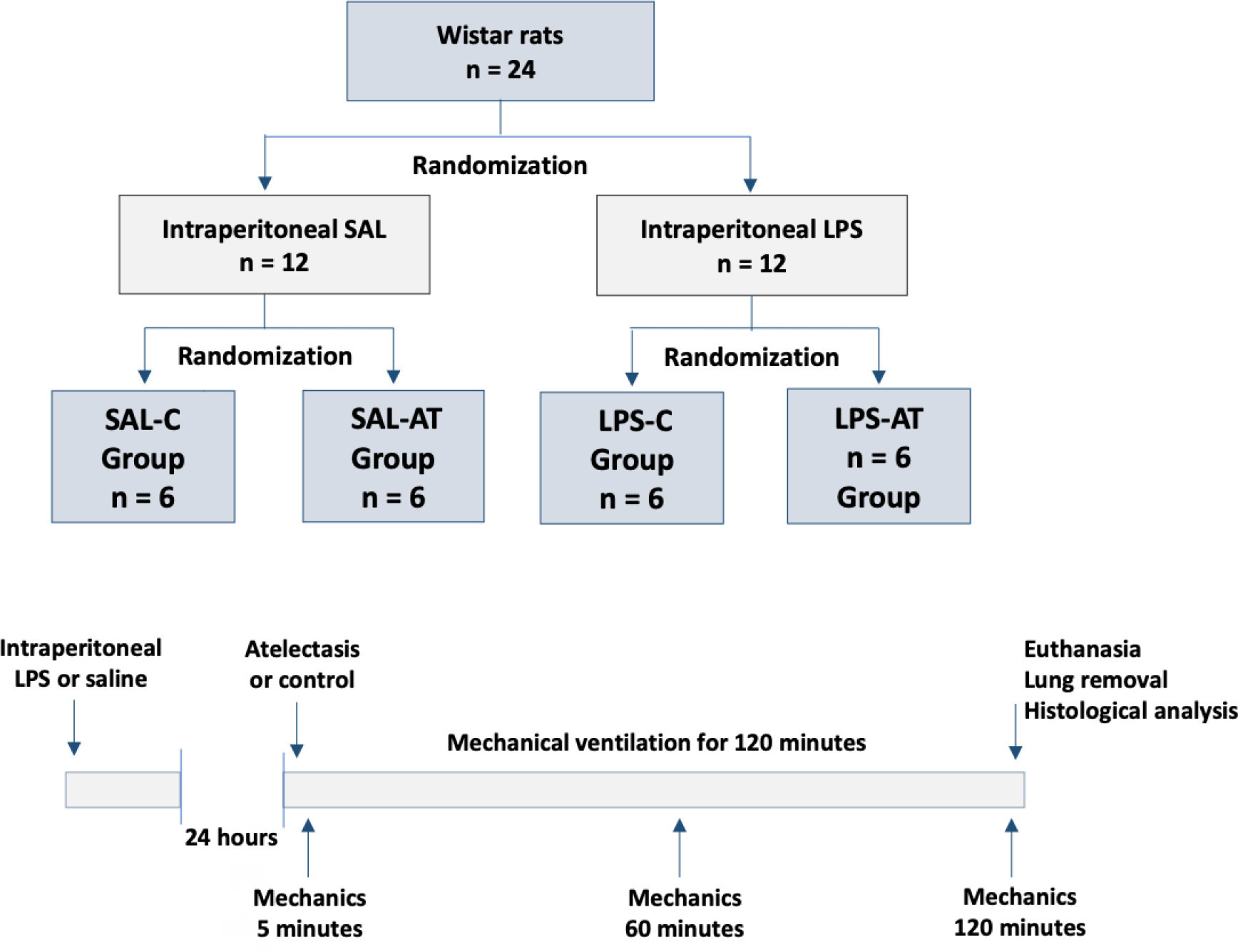
Twenty-four rats were randomized into the following four groups, each with 6 animals: the Saline-Control Group, Lipopolysaccharide Control Group, Saline-Atelectasis Group, and Lipopolysaccharide Atelectasis Group. Acute lung injury was induced by intraperitoneal injection of lipopolysaccharide. After 24 hours, atelectasis was induced by bronchial blocking. The animals underwent mechanical ventilation for two hours with protective parameters, and respiratory mechanics were monitored during this period. Thereafter, histologic analyses of two regions of interest, periatelectatic areas and the normally-aerated lung contralateral to the atelectatic areas, were performed.
The lung injury score was significantly higher in the Lipopolysaccharide Control Group (0.41 ± 0.13) than in the Saline Control Group (0.15 ± 0.51), p < 0.05. Periatelectatic regions showed higher lung injury scores than normally-aerated regions in both the Saline-Atelectasis (0.44 ± 0.06 x 0.27 ± 0.74 p < 0.05) and Lipopolysaccharide Atelectasis (0.56 ± 0.09 x 0.35 ± 0.04 p < 0.05) Groups. The lung injury score in the periatelectatic regions was higher in the Lipopolysaccharide Atelectasis Group (0.56 ± 0.09) than in the periatelectatic region of the Saline-Atelectasis Group (0.44 ± 0.06), p < 0.05.
Atelectasis may cause injury to the surrounding tissue after a period of mechanical ventilation with protective parameters. Its effect was more significant in previously injured lungs.
Abstract
Crit Care Sci. 2023;35(4):386-393
DOI 10.5935/2965-2774.20230190-pt
To assess the effect of atelectasis during mechanical ventilation on the periatelectatic and normal lung regions in a model of atelectasis in rats with acute lung injury induced by lipopolysaccharide.
Twenty-four rats were randomized into the following four groups, each with 6 animals: the Saline-Control Group, Lipopolysaccharide Control Group, Saline-Atelectasis Group, and Lipopolysaccharide Atelectasis Group. Acute lung injury was induced by intraperitoneal injection of lipopolysaccharide. After 24 hours, atelectasis was induced by bronchial blocking. The animals underwent mechanical ventilation for two hours with protective parameters, and respiratory mechanics were monitored during this period. Thereafter, histologic analyses of two regions of interest, periatelectatic areas and the normally-aerated lung contralateral to the atelectatic areas, were performed.
The lung injury score was significantly higher in the Lipopolysaccharide Control Group (0.41 ± 0.13) than in the Saline Control Group (0.15 ± 0.51), p < 0.05. Periatelectatic regions showed higher lung injury scores than normally-aerated regions in both the Saline-Atelectasis (0.44 ± 0.06 x 0.27 ± 0.74 p < 0.05) and Lipopolysaccharide Atelectasis (0.56 ± 0.09 x 0.35 ± 0.04 p < 0.05) Groups. The lung injury score in the periatelectatic regions was higher in the Lipopolysaccharide Atelectasis Group (0.56 ± 0.09) than in the periatelectatic region of the Saline-Atelectasis Group (0.44 ± 0.06), p < 0.05.
Atelectasis may cause injury to the surrounding tissue after a period of mechanical ventilation with protective parameters. Its effect was more significant in previously injured lungs.
Abstract
Crit Care Sci. 2023;35(4):394-401
DOI 10.5935/2965-2774.20230170-pt
To investigate the impact of delirium severity in critically ill COVID-19 patients and its association with outcomes.
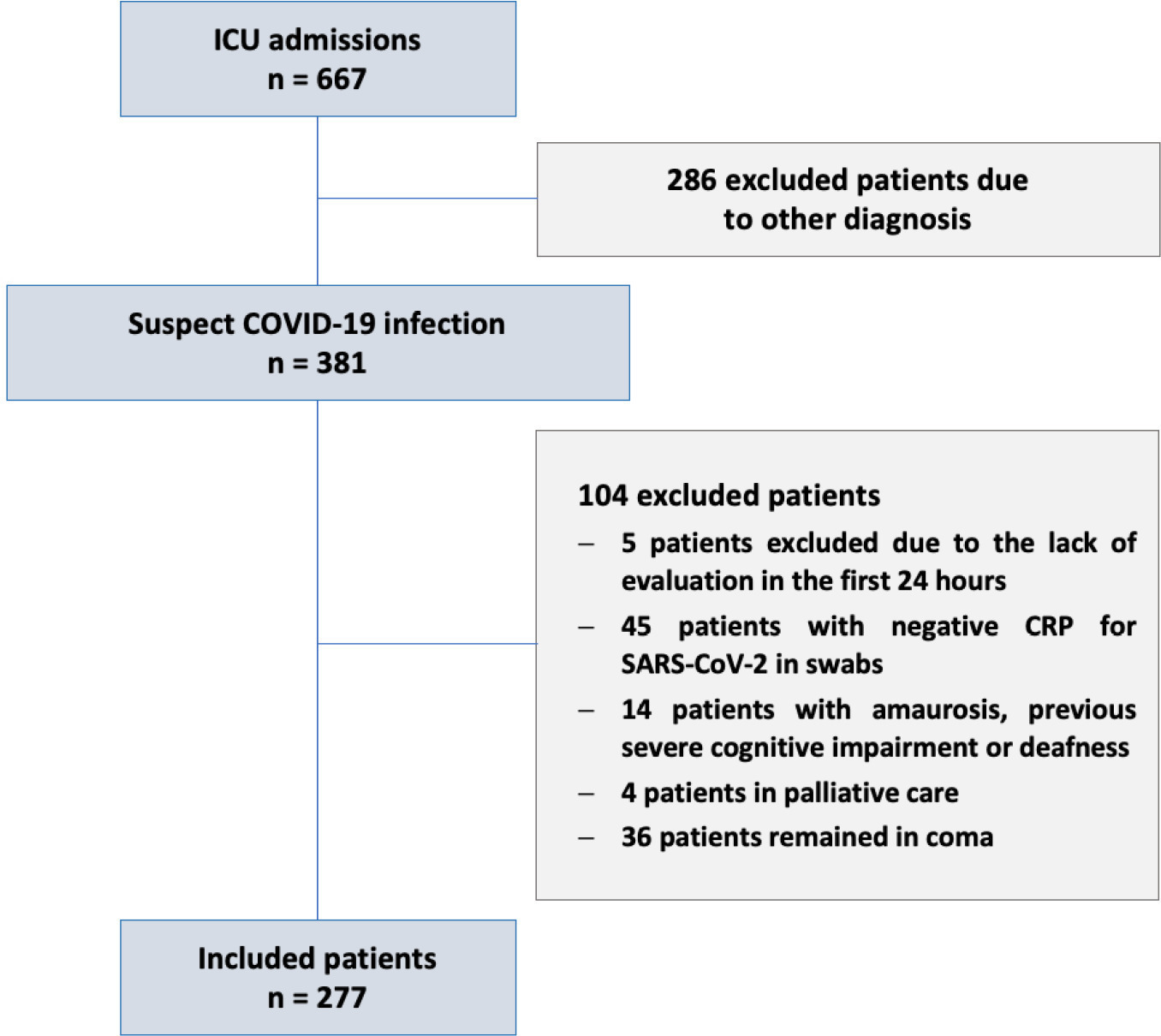
This prospective cohort study was performed in two tertiary intensive care units in Rio de Janeiro, Brazil. COVID-19 patients were evaluated daily during the first 7 days of intensive care unit stay using the Richmond Agitation Sedation Scale, Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Confusion Method Assessment for Intensive Care Unit-7 (CAM-ICU-7). Delirium severity was correlated with outcomes and one-year mortality.
Among the 277 COVID-19 patients included, delirium occurred in 101 (36.5%) during the first 7 days of intensive care unit stay, and it was associated with a higher length of intensive care unit stay in days (IQR 13 [7 - 25] versus 6 [4 - 12]; p < 0.001), higher hospital mortality (25.74% versus 5.11%; p < 0.001) and additional higher one-year mortality (5.3% versus 0.6%, p < 0.001). Delirium was classified by CAM-ICU-7 in terms of severity, and higher scores were associated with higher in-hospital mortality (17.86% versus 34.38% versus 38.46%, 95%CI, p value < 0.001). Severe delirium was associated with a higher risk of progression to coma (OR 7.1; 95%CI 1.9 - 31.0; p = 0.005) and to mechanical ventilation (OR 11.09; 95%CI 2.8 - 58.5; p = 0.002) in the multivariate analysis, adjusted by severity and frailty.
In patients admitted with COVID-19 in the intensive care unit, delirium was an independent risk factor for the worst prognosis, including mortality. The delirium severity assessed by the CAM-ICU-7 during the first week in the intensive care unit was associated with poor outcomes, including progression to coma and to mechanical ventilation.
Abstract
Crit Care Sci. 2023;35(4):394-401
DOI 10.5935/2965-2774.20230170-pt
To investigate the impact of delirium severity in critically ill COVID-19 patients and its association with outcomes.
This prospective cohort study was performed in two tertiary intensive care units in Rio de Janeiro, Brazil. COVID-19 patients were evaluated daily during the first 7 days of intensive care unit stay using the Richmond Agitation Sedation Scale, Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Confusion Method Assessment for Intensive Care Unit-7 (CAM-ICU-7). Delirium severity was correlated with outcomes and one-year mortality.
Among the 277 COVID-19 patients included, delirium occurred in 101 (36.5%) during the first 7 days of intensive care unit stay, and it was associated with a higher length of intensive care unit stay in days (IQR 13 [7 - 25] versus 6 [4 - 12]; p < 0.001), higher hospital mortality (25.74% versus 5.11%; p < 0.001) and additional higher one-year mortality (5.3% versus 0.6%, p < 0.001). Delirium was classified by CAM-ICU-7 in terms of severity, and higher scores were associated with higher in-hospital mortality (17.86% versus 34.38% versus 38.46%, 95%CI, p value < 0.001). Severe delirium was associated with a higher risk of progression to coma (OR 7.1; 95%CI 1.9 - 31.0; p = 0.005) and to mechanical ventilation (OR 11.09; 95%CI 2.8 - 58.5; p = 0.002) in the multivariate analysis, adjusted by severity and frailty.
In patients admitted with COVID-19 in the intensive care unit, delirium was an independent risk factor for the worst prognosis, including mortality. The delirium severity assessed by the CAM-ICU-7 during the first week in the intensive care unit was associated with poor outcomes, including progression to coma and to mechanical ventilation.
Abstract
Crit Care Sci. 2023;35(4):402-410
DOI 10.5935/2965-2774.20230174-pt
To describe, with a larger number of patients in a real-world scenario following routine implementation, intensivist-led ultrasound-guided percutaneous dilational tracheostomy and the possible risks and complications of the procedure not identified in clinical trials.
This was a phase IV cohort study of patients admitted to three intensive care units of a quaternary academic hospital who underwent intensivist-led ultrasound-guided percutaneous tracheostomy in Brazil from September 2017 to December 2021.
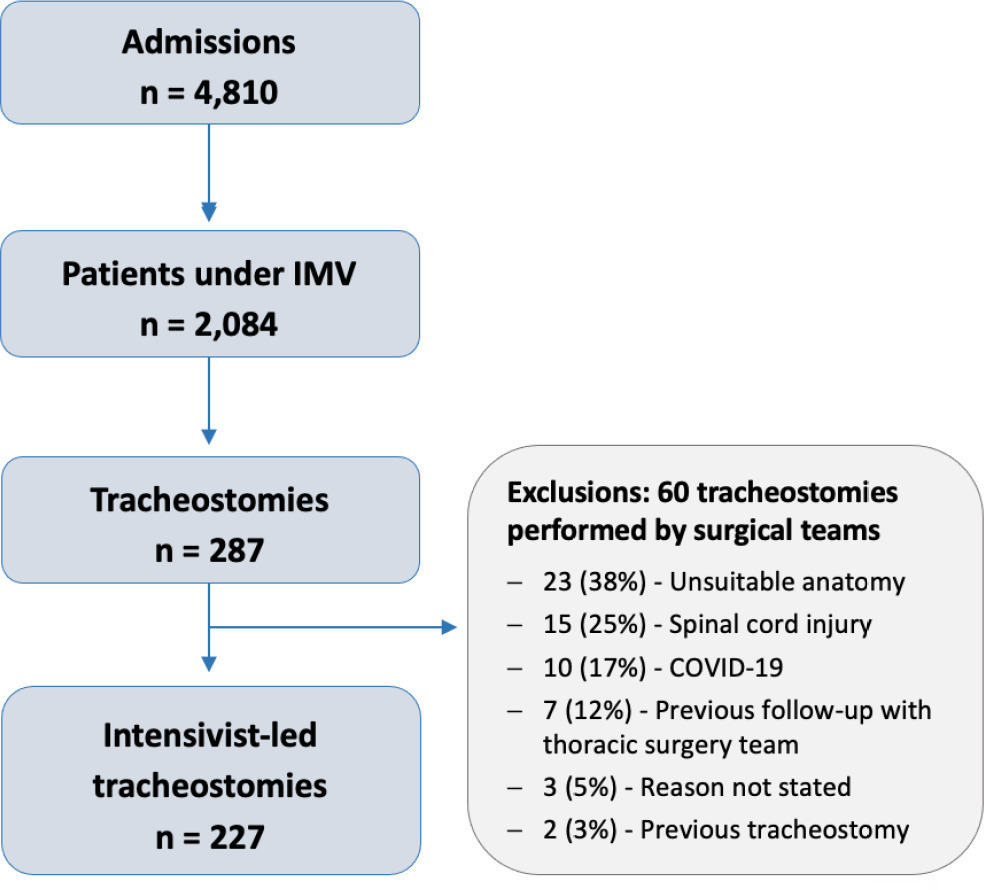
There were 4,810 intensive care unit admissions during the study period; 2,084 patients received mechanical ventilation, and 287 underwent tracheostomy, 227 of which were performed at bedside by the intensive care team. The main reason for intensive care unit admission was trauma, and for perform a tracheostomy it was a neurological impairment or an inability to protect the airways. The median time from intubation to tracheostomy was 14 days. Intensive care residents performed 76% of the procedures. At least one complication occurred in 29.5% of the procedures, the most common being hemodynamic instability and extubation during the procedure, with only 3 serious complications. The intensive care unit mortality was 29.1%, and the hospital mortality was 43.6%.
Intensivist-led ultrasound-guided percutaneous tracheostomy is feasible out of a clinical trial context with outcomes and complications comparable to those in the literature. Intensivists can acquire this competence during their training but should be aware of potential complications to enhance procedural safety.
Abstract
Crit Care Sci. 2023;35(4):402-410
DOI 10.5935/2965-2774.20230174-pt
To describe, with a larger number of patients in a real-world scenario following routine implementation, intensivist-led ultrasound-guided percutaneous dilational tracheostomy and the possible risks and complications of the procedure not identified in clinical trials.
This was a phase IV cohort study of patients admitted to three intensive care units of a quaternary academic hospital who underwent intensivist-led ultrasound-guided percutaneous tracheostomy in Brazil from September 2017 to December 2021.
There were 4,810 intensive care unit admissions during the study period; 2,084 patients received mechanical ventilation, and 287 underwent tracheostomy, 227 of which were performed at bedside by the intensive care team. The main reason for intensive care unit admission was trauma, and for perform a tracheostomy it was a neurological impairment or an inability to protect the airways. The median time from intubation to tracheostomy was 14 days. Intensive care residents performed 76% of the procedures. At least one complication occurred in 29.5% of the procedures, the most common being hemodynamic instability and extubation during the procedure, with only 3 serious complications. The intensive care unit mortality was 29.1%, and the hospital mortality was 43.6%.
Intensivist-led ultrasound-guided percutaneous tracheostomy is feasible out of a clinical trial context with outcomes and complications comparable to those in the literature. Intensivists can acquire this competence during their training but should be aware of potential complications to enhance procedural safety.
Abstract
Crit Care Sci. 2023;35(3):273-280
DOI 10.5935/2965-2774.20230359-pt
To describe the role of physiotherapists in assisting patients suspected to have or diagnosed with COVID-19 hospitalized in intensive care units in Brazil regarding technical training, working time, care practice, labor conditions and remuneration.
An analytical cross-sectional survey was carried out through an electronic questionnaire distributed to physiotherapists who worked in the care of patients with COVID-19 in Brazilian intensive care units.
A total of 657 questionnaires were completed by physiotherapists from the five regions of the country, with 85.3% working in adult, 5.4% in neonatal, 5.3% in pediatric and 3.8% in mixed intensive care units (pediatric and neonatal). In intensive care units with a physiotherapists available 24 hours/day, physiotherapists worked more frequently (90.6%) in the assembly, titration, and monitoring of noninvasive ventilation (p = 0.001). Most intensive care units with 12-hour/day physiotherapists (25.8%) did not apply any protocol compared to intensive care units with 18-hour/day physiotherapy (9.9%) versus 24 hours/day (10.2%) (p = 0.032). Most of the respondents (51.0%) received remuneration 2 or 3 times the minimum wage, and only 25.1% received an additional payment for working with patients suspected to have or diagnosed with COVID-19; 85.7% of them did not experience a lack of personal protective equipment.
Intensive care units with 24-hour/day physiotherapists had higher percentages of protocols and noninvasive ventilation for patients with COVID-19. The use of specific resources varied between the types of intensive care units and hospitals and in relation to the physiotherapists’ labor conditions. This study showed that most professionals had little experience in intensive care and low wages.
Abstract
Crit Care Sci. 2023;35(3):273-280
DOI 10.5935/2965-2774.20230359-pt
To describe the role of physiotherapists in assisting patients suspected to have or diagnosed with COVID-19 hospitalized in intensive care units in Brazil regarding technical training, working time, care practice, labor conditions and remuneration.
An analytical cross-sectional survey was carried out through an electronic questionnaire distributed to physiotherapists who worked in the care of patients with COVID-19 in Brazilian intensive care units.
A total of 657 questionnaires were completed by physiotherapists from the five regions of the country, with 85.3% working in adult, 5.4% in neonatal, 5.3% in pediatric and 3.8% in mixed intensive care units (pediatric and neonatal). In intensive care units with a physiotherapists available 24 hours/day, physiotherapists worked more frequently (90.6%) in the assembly, titration, and monitoring of noninvasive ventilation (p = 0.001). Most intensive care units with 12-hour/day physiotherapists (25.8%) did not apply any protocol compared to intensive care units with 18-hour/day physiotherapy (9.9%) versus 24 hours/day (10.2%) (p = 0.032). Most of the respondents (51.0%) received remuneration 2 or 3 times the minimum wage, and only 25.1% received an additional payment for working with patients suspected to have or diagnosed with COVID-19; 85.7% of them did not experience a lack of personal protective equipment.
Intensive care units with 24-hour/day physiotherapists had higher percentages of protocols and noninvasive ventilation for patients with COVID-19. The use of specific resources varied between the types of intensive care units and hospitals and in relation to the physiotherapists’ labor conditions. This study showed that most professionals had little experience in intensive care and low wages.
Abstract
Crit Care Sci. 2023;35(3):281-289
DOI 10.5935/2965-2774.20230041-pt
To evaluate if the reductions in systemic and renal oxygen consumption are associated with the development of evidence of anaerobic metabolism.
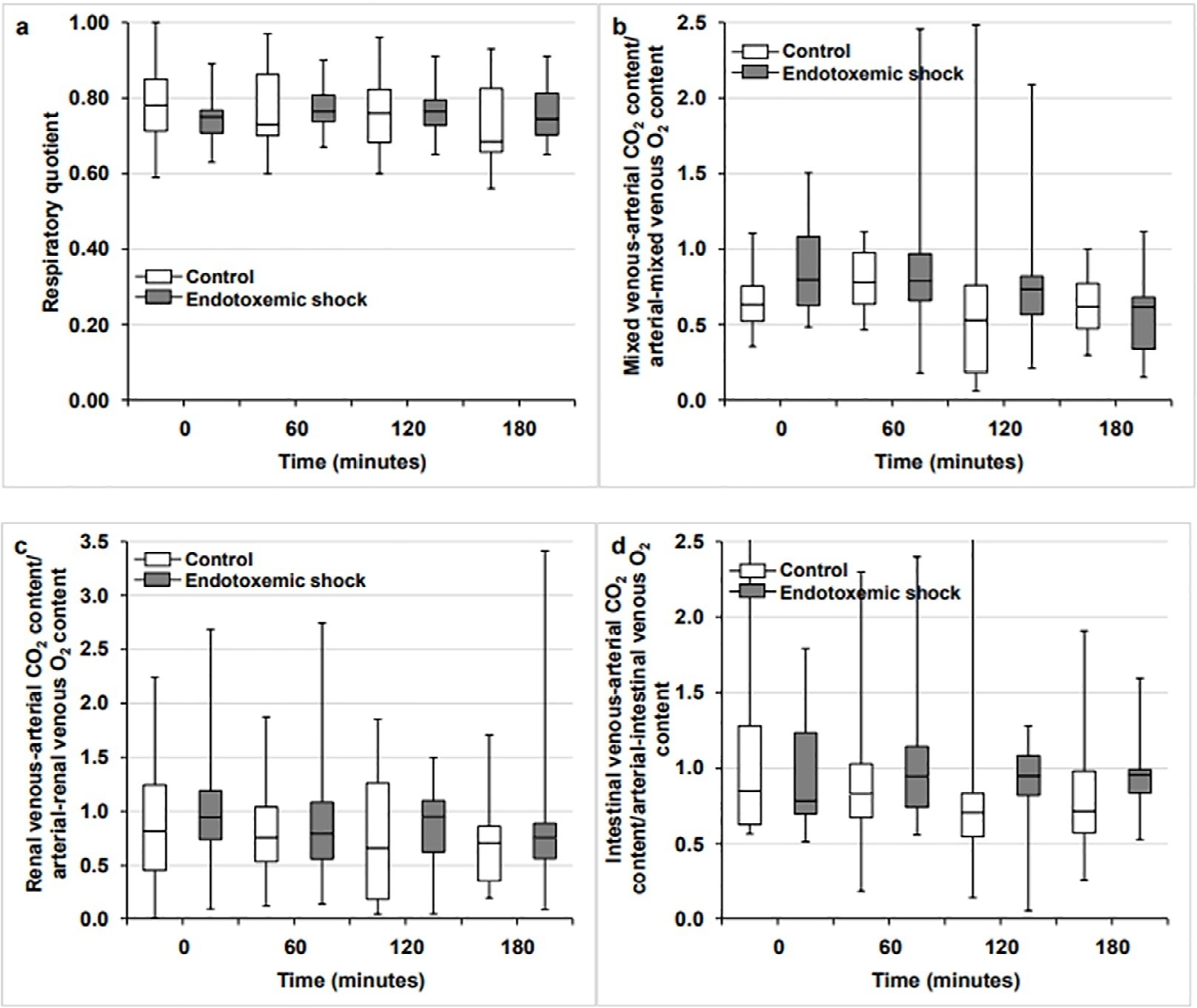
This is a subanalysis of a previously published study. In anesthetized and mechanically ventilated sheep, we measured the respiratory quotient by indirect calorimetry and its systemic, renal, and intestinal surrogates (the ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference. The Endotoxemic Shock Group (n = 12) was measured at baseline, after 60 minutes of endotoxemic shock, and after 60 and 120 minutes of fluid and norepinephrine resuscitation, and the values were compared with those of a Control Group (n = 12) without interventions.
Endotoxemic shock decreased systemic and renal oxygen consumption (6.3 [5.6 - 6.6] versus 7.4 [6.3 - 8.5] mL/minute/kg and 3.7 [3.3 - 4.5] versus 5.4 [4.6 - 9.4] mL/minute/100g; p < 0.05 for both). After 120 minutes of resuscitation, systemic oxygen consumption was normalized, but renal oxygen consumption remained decreased (6.3 [5.9 - 8.2] versus 7.1 [6.1 - 8.6] mL/minute/100g; p = not significance and 3.8 [1.9 - 4.8] versus 5.7 [4.5 - 7.1]; p < 0.05). The respiratory quotient and the systemic, renal and intestinal ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference did not change throughout the experiments.
In this experimental model of septic shock, oxygen supply dependence was not associated with increases in the respiratory quotient or its surrogates. Putative explanations for these findings are the absence of anaerobic metabolism or the poor sensitivity of these variables in detecting this condition.
Abstract
Crit Care Sci. 2023;35(3):281-289
DOI 10.5935/2965-2774.20230041-pt
To evaluate if the reductions in systemic and renal oxygen consumption are associated with the development of evidence of anaerobic metabolism.
This is a subanalysis of a previously published study. In anesthetized and mechanically ventilated sheep, we measured the respiratory quotient by indirect calorimetry and its systemic, renal, and intestinal surrogates (the ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference. The Endotoxemic Shock Group (n = 12) was measured at baseline, after 60 minutes of endotoxemic shock, and after 60 and 120 minutes of fluid and norepinephrine resuscitation, and the values were compared with those of a Control Group (n = 12) without interventions.
Endotoxemic shock decreased systemic and renal oxygen consumption (6.3 [5.6 - 6.6] versus 7.4 [6.3 - 8.5] mL/minute/kg and 3.7 [3.3 - 4.5] versus 5.4 [4.6 - 9.4] mL/minute/100g; p < 0.05 for both). After 120 minutes of resuscitation, systemic oxygen consumption was normalized, but renal oxygen consumption remained decreased (6.3 [5.9 - 8.2] versus 7.1 [6.1 - 8.6] mL/minute/100g; p = not significance and 3.8 [1.9 - 4.8] versus 5.7 [4.5 - 7.1]; p < 0.05). The respiratory quotient and the systemic, renal and intestinal ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference did not change throughout the experiments.
In this experimental model of septic shock, oxygen supply dependence was not associated with increases in the respiratory quotient or its surrogates. Putative explanations for these findings are the absence of anaerobic metabolism or the poor sensitivity of these variables in detecting this condition.
Abstract
Crit Care Sci. 2023;35(3):290-301
DOI 10.5935/2965-2774.20230388-pt
To determine the prevalence and factors associated with the physical rehabilitation of critically ill children in Brazilian pediatric intensive care units.
A 2-day, cross-sectional, multicenter point prevalence study comprising 27 pediatric intensive care units (out of 738) was conducted in Brazil in April and June 2019. This Brazilian study was part of a large multinational study called Prevalence of Acute Rehabilitation for Kids in the PICU (PARK-PICU). The primary outcome was the prevalence of mobility provided by physical therapy or occupational therapy. Clinical data on patient mobility, potential mobility safety events, and mobilization barriers were prospectively collected in patients admitted for ≥ 72 hours.
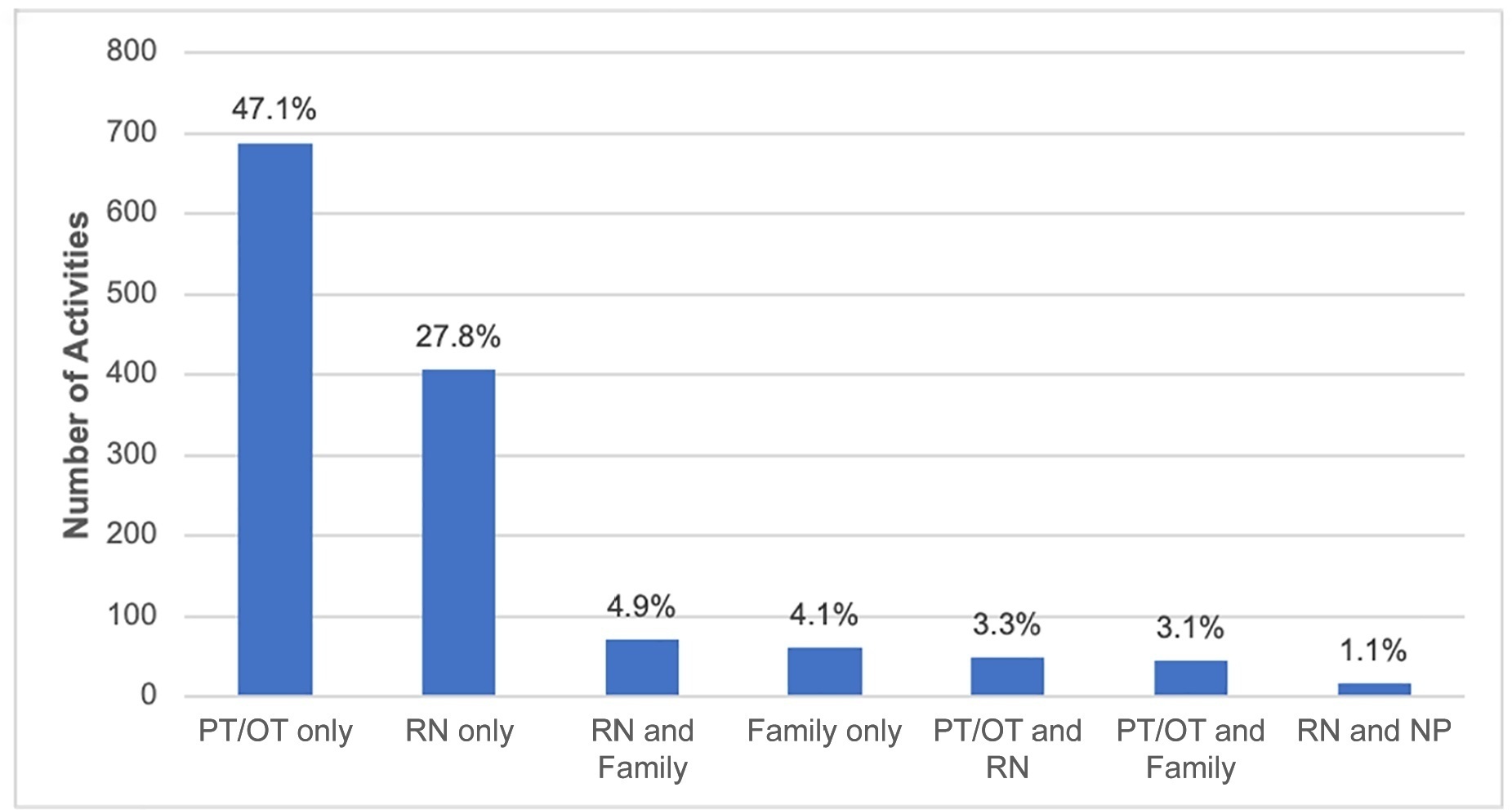
Children under the age of 3 years comprised 68% of the patient population. The prevalence of therapist-provided mobility was 74%, or 277 out of the 375 patient-days. Out-of-bed mobility was most positively associated with family presence (adjusted odds ratios 3.31;95%CI 1.70 - 6.43) and most negatively associated with arterial lines (adjusted odds ratios 0.16; 95%CI 0.05 - 0.57). Barriers to mobilization were reported on 27% of patient-days, the most common being lack of physician order (n = 18). Potential safety events occurred in 3% of all mobilization events.
Therapist-provided mobility in Brazilian pediatric intensive care units is frequent. Family presence was high and positively associated with out-of-bed mobility. The presence of physiotherapists 24 hours a day in Brazilian pediatric intensive care units may have a substantial impact on the mobilization of critically ill children.
Abstract
Crit Care Sci. 2023;35(3):290-301
DOI 10.5935/2965-2774.20230388-pt
To determine the prevalence and factors associated with the physical rehabilitation of critically ill children in Brazilian pediatric intensive care units.
A 2-day, cross-sectional, multicenter point prevalence study comprising 27 pediatric intensive care units (out of 738) was conducted in Brazil in April and June 2019. This Brazilian study was part of a large multinational study called Prevalence of Acute Rehabilitation for Kids in the PICU (PARK-PICU). The primary outcome was the prevalence of mobility provided by physical therapy or occupational therapy. Clinical data on patient mobility, potential mobility safety events, and mobilization barriers were prospectively collected in patients admitted for ≥ 72 hours.
Children under the age of 3 years comprised 68% of the patient population. The prevalence of therapist-provided mobility was 74%, or 277 out of the 375 patient-days. Out-of-bed mobility was most positively associated with family presence (adjusted odds ratios 3.31;95%CI 1.70 - 6.43) and most negatively associated with arterial lines (adjusted odds ratios 0.16; 95%CI 0.05 - 0.57). Barriers to mobilization were reported on 27% of patient-days, the most common being lack of physician order (n = 18). Potential safety events occurred in 3% of all mobilization events.
Therapist-provided mobility in Brazilian pediatric intensive care units is frequent. Family presence was high and positively associated with out-of-bed mobility. The presence of physiotherapists 24 hours a day in Brazilian pediatric intensive care units may have a substantial impact on the mobilization of critically ill children.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)