Oxygen consumption Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(3):281-289
DOI 10.5935/2965-2774.20230041-pt
To evaluate if the reductions in systemic and renal oxygen consumption are associated with the development of evidence of anaerobic metabolism.
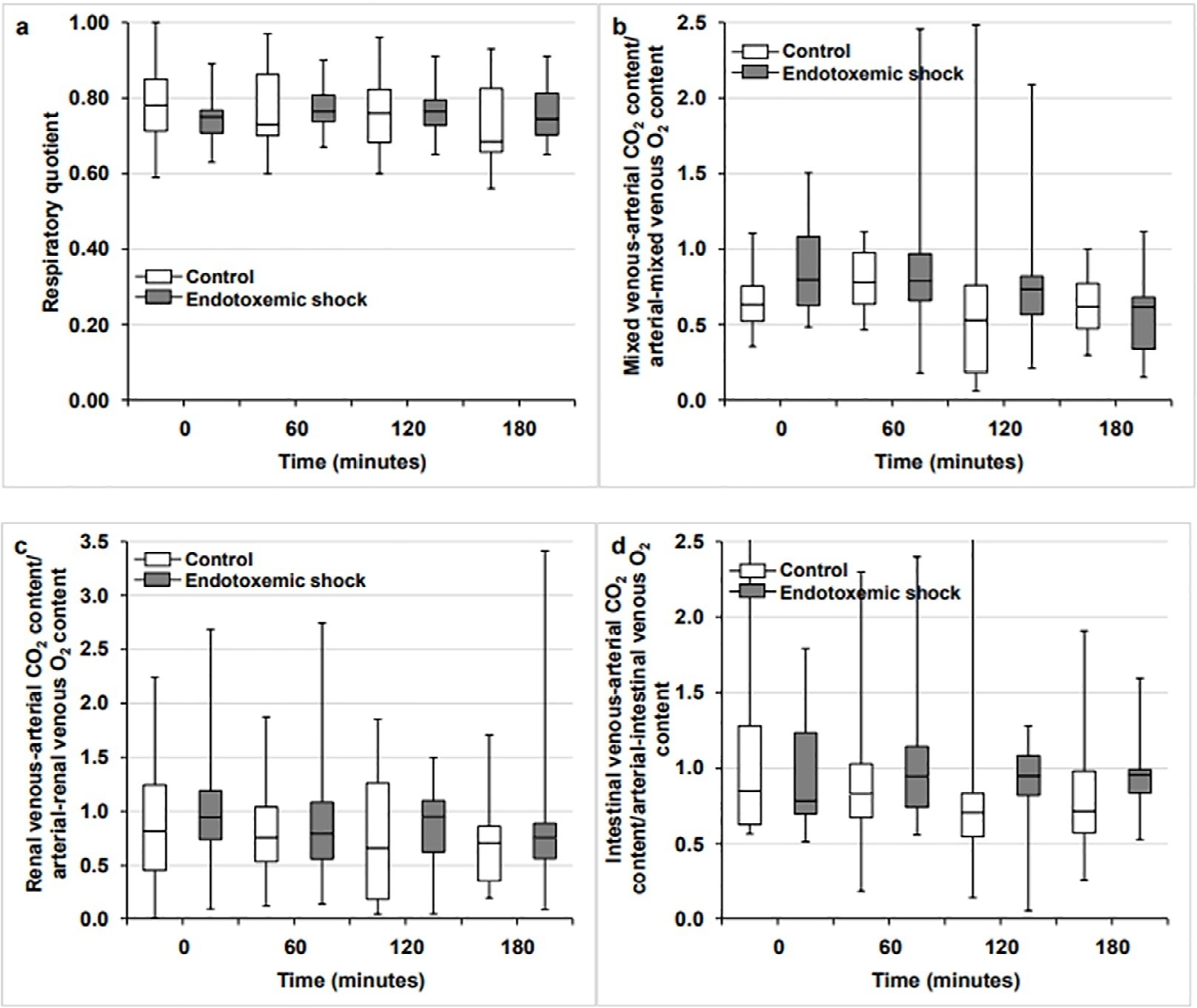
This is a subanalysis of a previously published study. In anesthetized and mechanically ventilated sheep, we measured the respiratory quotient by indirect calorimetry and its systemic, renal, and intestinal surrogates (the ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference. The Endotoxemic Shock Group (n = 12) was measured at baseline, after 60 minutes of endotoxemic shock, and after 60 and 120 minutes of fluid and norepinephrine resuscitation, and the values were compared with those of a Control Group (n = 12) without interventions.
Endotoxemic shock decreased systemic and renal oxygen consumption (6.3 [5.6 - 6.6] versus 7.4 [6.3 - 8.5] mL/minute/kg and 3.7 [3.3 - 4.5] versus 5.4 [4.6 - 9.4] mL/minute/100g; p < 0.05 for both). After 120 minutes of resuscitation, systemic oxygen consumption was normalized, but renal oxygen consumption remained decreased (6.3 [5.9 - 8.2] versus 7.1 [6.1 - 8.6] mL/minute/100g; p = not significance and 3.8 [1.9 - 4.8] versus 5.7 [4.5 - 7.1]; p < 0.05). The respiratory quotient and the systemic, renal and intestinal ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference did not change throughout the experiments.
In this experimental model of septic shock, oxygen supply dependence was not associated with increases in the respiratory quotient or its surrogates. Putative explanations for these findings are the absence of anaerobic metabolism or the poor sensitivity of these variables in detecting this condition.
Abstract
Crit Care Sci. 2023;35(3):281-289
DOI 10.5935/2965-2774.20230041-pt
To evaluate if the reductions in systemic and renal oxygen consumption are associated with the development of evidence of anaerobic metabolism.
This is a subanalysis of a previously published study. In anesthetized and mechanically ventilated sheep, we measured the respiratory quotient by indirect calorimetry and its systemic, renal, and intestinal surrogates (the ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference. The Endotoxemic Shock Group (n = 12) was measured at baseline, after 60 minutes of endotoxemic shock, and after 60 and 120 minutes of fluid and norepinephrine resuscitation, and the values were compared with those of a Control Group (n = 12) without interventions.
Endotoxemic shock decreased systemic and renal oxygen consumption (6.3 [5.6 - 6.6] versus 7.4 [6.3 - 8.5] mL/minute/kg and 3.7 [3.3 - 4.5] versus 5.4 [4.6 - 9.4] mL/minute/100g; p < 0.05 for both). After 120 minutes of resuscitation, systemic oxygen consumption was normalized, but renal oxygen consumption remained decreased (6.3 [5.9 - 8.2] versus 7.1 [6.1 - 8.6] mL/minute/100g; p = not significance and 3.8 [1.9 - 4.8] versus 5.7 [4.5 - 7.1]; p < 0.05). The respiratory quotient and the systemic, renal and intestinal ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference did not change throughout the experiments.
In this experimental model of septic shock, oxygen supply dependence was not associated with increases in the respiratory quotient or its surrogates. Putative explanations for these findings are the absence of anaerobic metabolism or the poor sensitivity of these variables in detecting this condition.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):255-261
DOI 10.5935/0103-507X.20220023-en
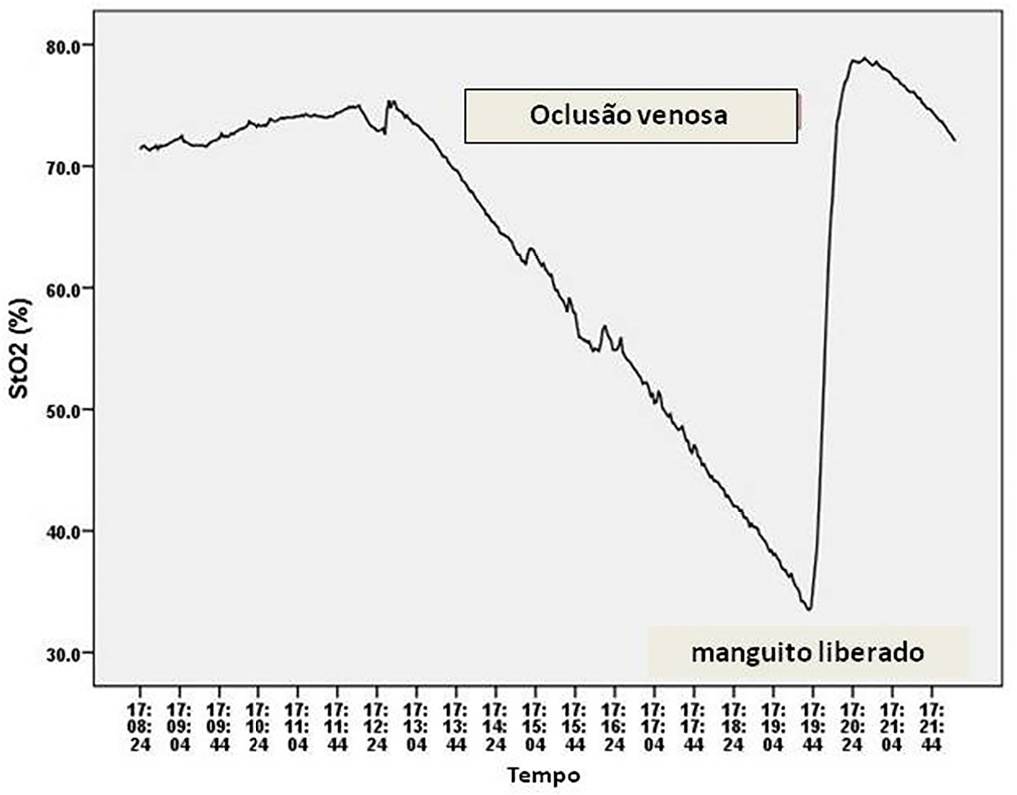
To test whether tissue oxygen saturation (StO2) after a venous occlusion test estimates central venous oxygen saturation (ScvO2).
Observational study in intensive care unit patients. Tissue oxygen saturation was monitored (InSpectra Tissue Spectrometer Model 650, Hutchinson Technology Inc., MN, USA) with a multiprobe (15/25mm) in the thenar position. A venous occlusion test in volunteers was applied in the upper arm to test the tolerability and pattern of StO2 changes during the venous occlusion test. A sphygmomanometer cuff was inflated to a pressure 30mmHg above diastolic pressure until StO2 reached a plateau and deflated to 0mmHg. Tissue oxygen saturation parameters were divided into resting StO2 (r-StO2) and minimal StO2 (m-StO2) at the end of the venous occlusion test. In patients, the cuff was inflated to a pressure 30mmHg above diastolic pressure for 5 min (volunteers’ time derived) or until a StO2 plateau was reached. Tissue oxygen saturation parameters were divided into r-StO2, m-StO2, and the mean time that StO2 reached ScvO2. The StO2 value at the mean time was compared to ScvO2.
All 9 volunteers tolerated the venous occlusion test. The time for tolerability or the StO2 plateau was 7 ± 1 minutes. We studied 22 patients. The mean time for StO2 equalized ScvO2 was 100 sec and 95 sec (15/25mm probes). The StO2 value at 100 sec ([100-StO2] 15mm: 74 ± 7%; 25mm: 74 ± 6%) was then compared with ScvO2 (75 ± 6%). The StO2 value at 100 sec correlated with ScvO2 (15 mm: R2 = 0.63, 25mm: R2 = 0.67, p < 0.01) without discrepancy (Bland Altman).
Central venous oxygen saturation can be estimated from StO2 during a venous occlusion test.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):255-261
DOI 10.5935/0103-507X.20220023-en
To test whether tissue oxygen saturation (StO2) after a venous occlusion test estimates central venous oxygen saturation (ScvO2).
Observational study in intensive care unit patients. Tissue oxygen saturation was monitored (InSpectra Tissue Spectrometer Model 650, Hutchinson Technology Inc., MN, USA) with a multiprobe (15/25mm) in the thenar position. A venous occlusion test in volunteers was applied in the upper arm to test the tolerability and pattern of StO2 changes during the venous occlusion test. A sphygmomanometer cuff was inflated to a pressure 30mmHg above diastolic pressure until StO2 reached a plateau and deflated to 0mmHg. Tissue oxygen saturation parameters were divided into resting StO2 (r-StO2) and minimal StO2 (m-StO2) at the end of the venous occlusion test. In patients, the cuff was inflated to a pressure 30mmHg above diastolic pressure for 5 min (volunteers’ time derived) or until a StO2 plateau was reached. Tissue oxygen saturation parameters were divided into r-StO2, m-StO2, and the mean time that StO2 reached ScvO2. The StO2 value at the mean time was compared to ScvO2.
All 9 volunteers tolerated the venous occlusion test. The time for tolerability or the StO2 plateau was 7 ± 1 minutes. We studied 22 patients. The mean time for StO2 equalized ScvO2 was 100 sec and 95 sec (15/25mm probes). The StO2 value at 100 sec ([100-StO2] 15mm: 74 ± 7%; 25mm: 74 ± 6%) was then compared with ScvO2 (75 ± 6%). The StO2 value at 100 sec correlated with ScvO2 (15 mm: R2 = 0.63, 25mm: R2 = 0.67, p < 0.01) without discrepancy (Bland Altman).
Central venous oxygen saturation can be estimated from StO2 during a venous occlusion test.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):154-166
DOI 10.5935/0103-507X.20210017
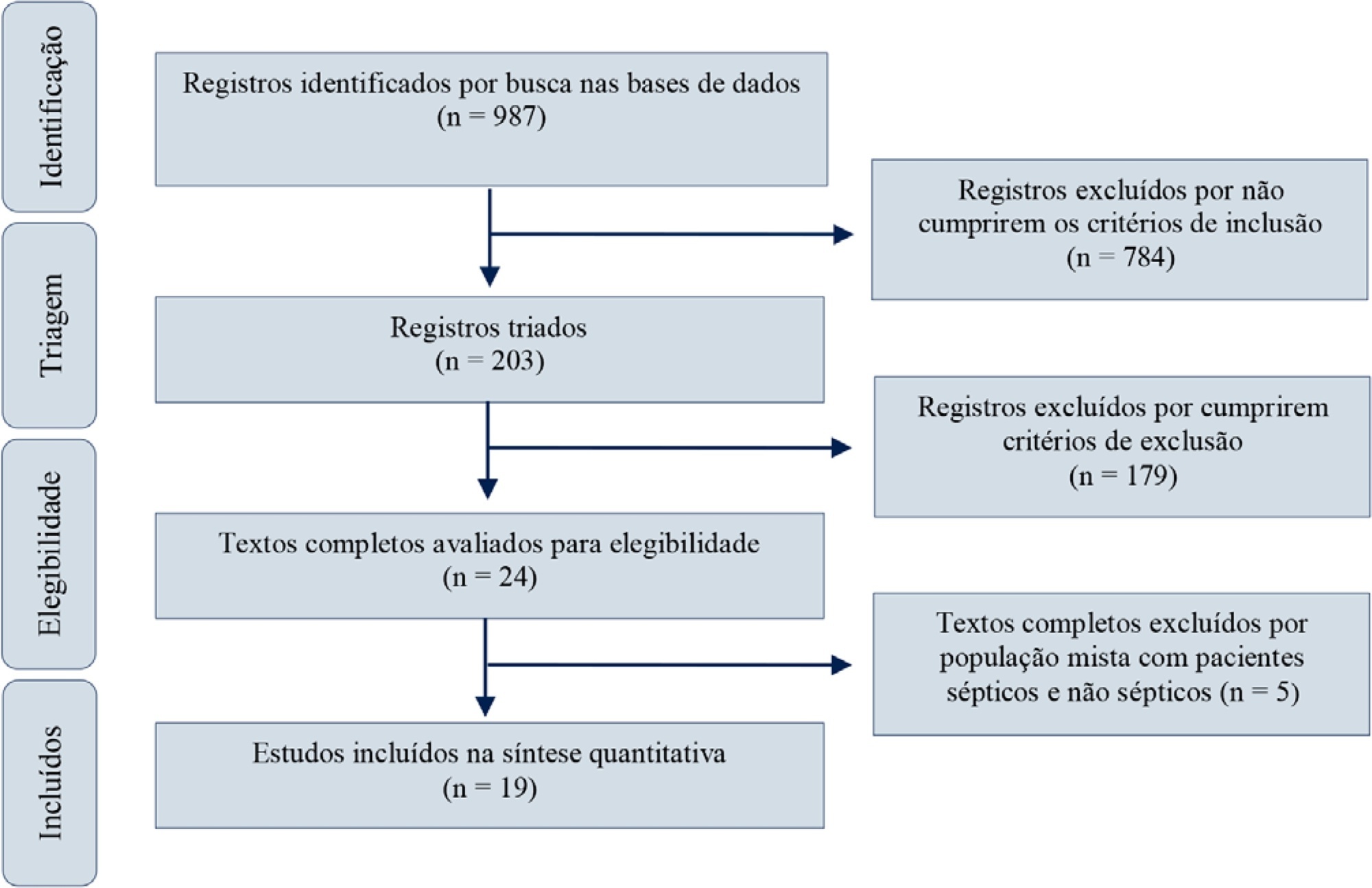
Red blood cell transfusion is thought to improve cell respiration during septic shock. Nevertheless, its acute impact on oxygen transport and metabolism in this condition remains highly debatable. The objective of this study was to evaluate the impact of red blood cell transfusion on microcirculation and oxygen metabolism in patients with sepsis and septic shock. We conducted a search in the MEDLINE®, Elsevier and Scopus databases. We included studies conducted in adult humans with sepsis and septic shock. A systematic review and meta-analysis were performed using the DerSimonian and Laird random-effects model. A p value < 0.05 was considered significant. Nineteen manuscripts with 428 patients were included in the analysis. Red blood cell transfusions were associated with an increase in the pooled mean venous oxygen saturation of 3.7% (p < 0.001), a decrease in oxygen extraction ratio of -6.98 (p < 0.001) and had no significant effect on the cardiac index (0.02L/minute; p = 0,96). Similar results were obtained in studies including simultaneous measurements of venous oxygen saturation, oxygen extraction ratio, and cardiac index. Red blood cell transfusions led to a significant increase in the proportion of perfused small vessels (2.85%; p = 0.553), while tissue oxygenation parameters revealed a significant increase in the tissue hemoglobin index (1.66; p = 0.018). Individual studies reported significant improvements in tissue oxygenation and sublingual microcirculatory parameters in patients with deranged microcirculation at baseline. Red blood cell transfusions seemed to improve systemic oxygen metabolism with apparent independence from cardiac index variations. Some beneficial effects have been observed for tissue oxygenation and microcirculation parameters, particularly in patients with more severe alterations at baseline. More studies are necessary to evaluate their clinical impact and to individualize transfusion decisions.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):154-166
DOI 10.5935/0103-507X.20210017
Red blood cell transfusion is thought to improve cell respiration during septic shock. Nevertheless, its acute impact on oxygen transport and metabolism in this condition remains highly debatable. The objective of this study was to evaluate the impact of red blood cell transfusion on microcirculation and oxygen metabolism in patients with sepsis and septic shock. We conducted a search in the MEDLINE®, Elsevier and Scopus databases. We included studies conducted in adult humans with sepsis and septic shock. A systematic review and meta-analysis were performed using the DerSimonian and Laird random-effects model. A p value < 0.05 was considered significant. Nineteen manuscripts with 428 patients were included in the analysis. Red blood cell transfusions were associated with an increase in the pooled mean venous oxygen saturation of 3.7% (p < 0.001), a decrease in oxygen extraction ratio of -6.98 (p < 0.001) and had no significant effect on the cardiac index (0.02L/minute; p = 0,96). Similar results were obtained in studies including simultaneous measurements of venous oxygen saturation, oxygen extraction ratio, and cardiac index. Red blood cell transfusions led to a significant increase in the proportion of perfused small vessels (2.85%; p = 0.553), while tissue oxygenation parameters revealed a significant increase in the tissue hemoglobin index (1.66; p = 0.018). Individual studies reported significant improvements in tissue oxygenation and sublingual microcirculatory parameters in patients with deranged microcirculation at baseline. Red blood cell transfusions seemed to improve systemic oxygen metabolism with apparent independence from cardiac index variations. Some beneficial effects have been observed for tissue oxygenation and microcirculation parameters, particularly in patients with more severe alterations at baseline. More studies are necessary to evaluate their clinical impact and to individualize transfusion decisions.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)