Prognosis Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
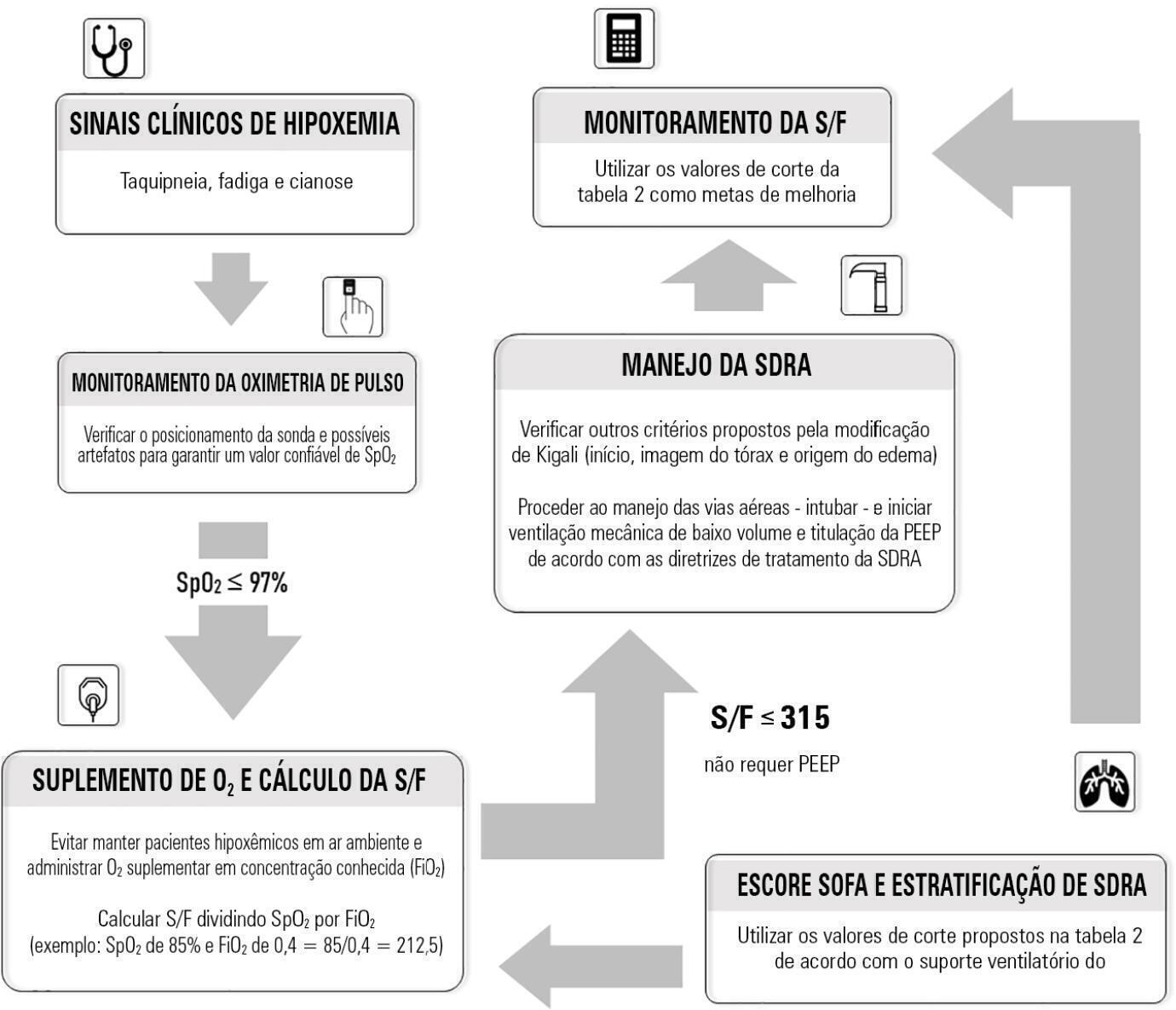
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):119-124
DOI 10.5935/0103-507X.20210013
To assess the performance of Pediatric Risk of Mortality (PRISM) III and Pediatric Index of Mortality (PIM) 2 scores in the pediatric intensive care unit.
A retrospective cohort study. Data were retrospectively collected from medical records of all patients admitted to the pediatric intensive care unit of a cancer hospital from January 2017 to June 2018.
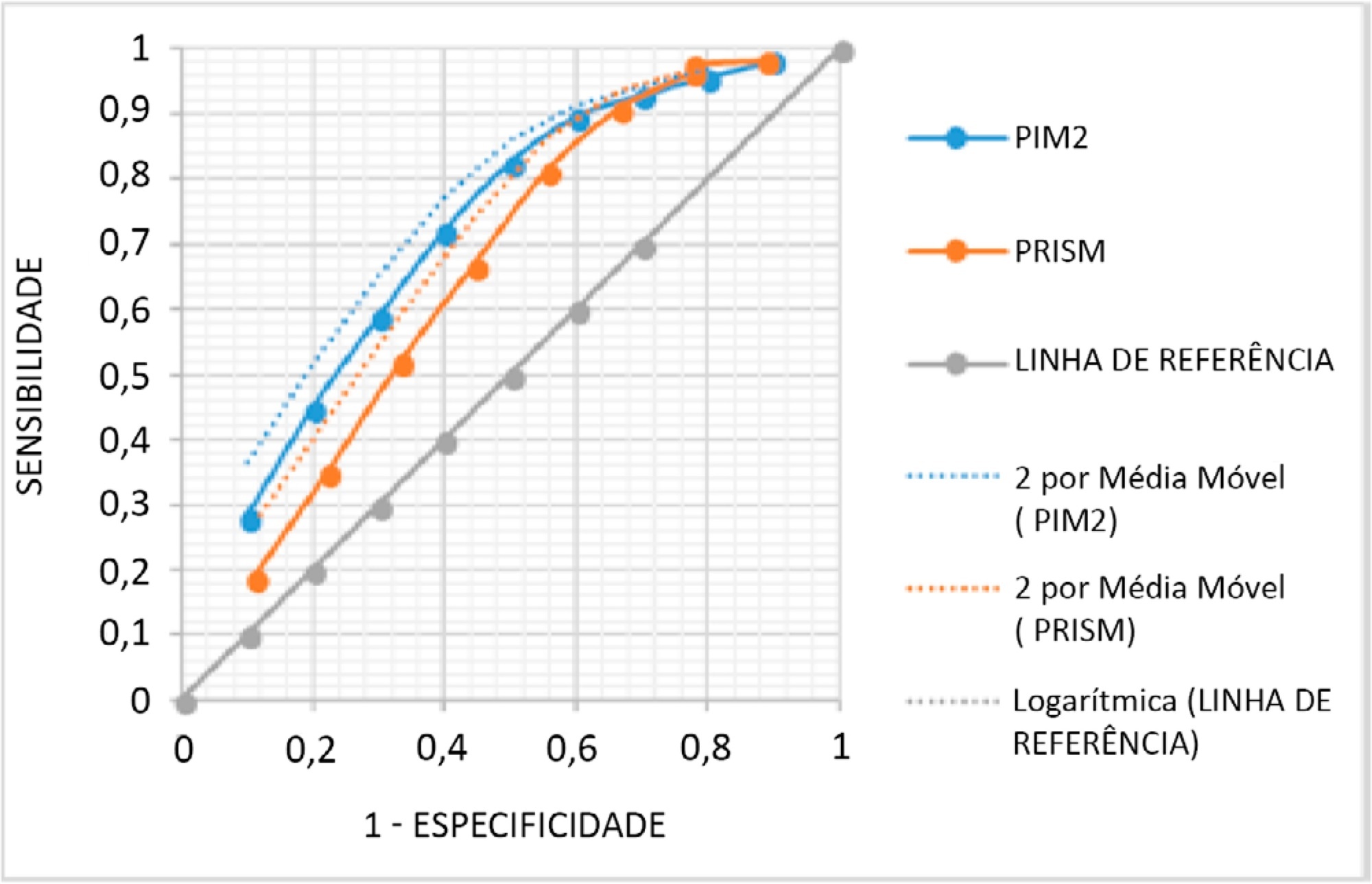
The mean PRISM III score was 15, and PIM 2, 24%. From the 338 studied patients, 62 (18.34%) died. The PRISM III estimated mortality was 79.52 patients (23.52%) and for PIM 2 80.19 patients (23.72%), corresponding to a standardized mortality ratio (95% confidence interval: 0.78 for PRISM II and 0.77 for PIM 2). The Hosmer-Lemeshow chi-square test was 11.56, 8df, 0.975 for PRISM II and 0.48, 8df, p = 0.999 for PIM 2. The area under the Receiver Operating Characteristic curve was 0.71 for PRISM III and 0.76 for PIM 2.
Both scores overestimated mortality and have shown a regular ability to discriminate between survivors and non-survivors. Models should be developed to quantify the severity of cancer pediatric patients in Pediatric Intensive Care Units and to predict the mortality risk accounting for their peculiarities.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):119-124
DOI 10.5935/0103-507X.20210013
To assess the performance of Pediatric Risk of Mortality (PRISM) III and Pediatric Index of Mortality (PIM) 2 scores in the pediatric intensive care unit.
A retrospective cohort study. Data were retrospectively collected from medical records of all patients admitted to the pediatric intensive care unit of a cancer hospital from January 2017 to June 2018.
The mean PRISM III score was 15, and PIM 2, 24%. From the 338 studied patients, 62 (18.34%) died. The PRISM III estimated mortality was 79.52 patients (23.52%) and for PIM 2 80.19 patients (23.72%), corresponding to a standardized mortality ratio (95% confidence interval: 0.78 for PRISM II and 0.77 for PIM 2). The Hosmer-Lemeshow chi-square test was 11.56, 8df, 0.975 for PRISM II and 0.48, 8df, p = 0.999 for PIM 2. The area under the Receiver Operating Characteristic curve was 0.71 for PRISM III and 0.76 for PIM 2.
Both scores overestimated mortality and have shown a regular ability to discriminate between survivors and non-survivors. Models should be developed to quantify the severity of cancer pediatric patients in Pediatric Intensive Care Units and to predict the mortality risk accounting for their peculiarities.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):514-520
DOI 10.5935/0103-507X.20200088
Low levels of thyroid hormones have been associated with poor clinical outcomes. This metabolic situation, designated euthyroid sick syndrome, has been interpreted as a state of adaptation to different pathological processes, characterized by the decrease in plasma triiodothyronine. The present study seeks to determine the incidence of this disorder in patients with septic shock and its relationship with other severity indices and clinical outcomes.
This prospective analytical study evaluated patients admitted to the intensive care unit with septic shock between April 2018 and July 2019. Variables associated with septic shock and thyroid profile were recorded at the time of the septic shock diagnosis and 7, 14, and 21 days later.
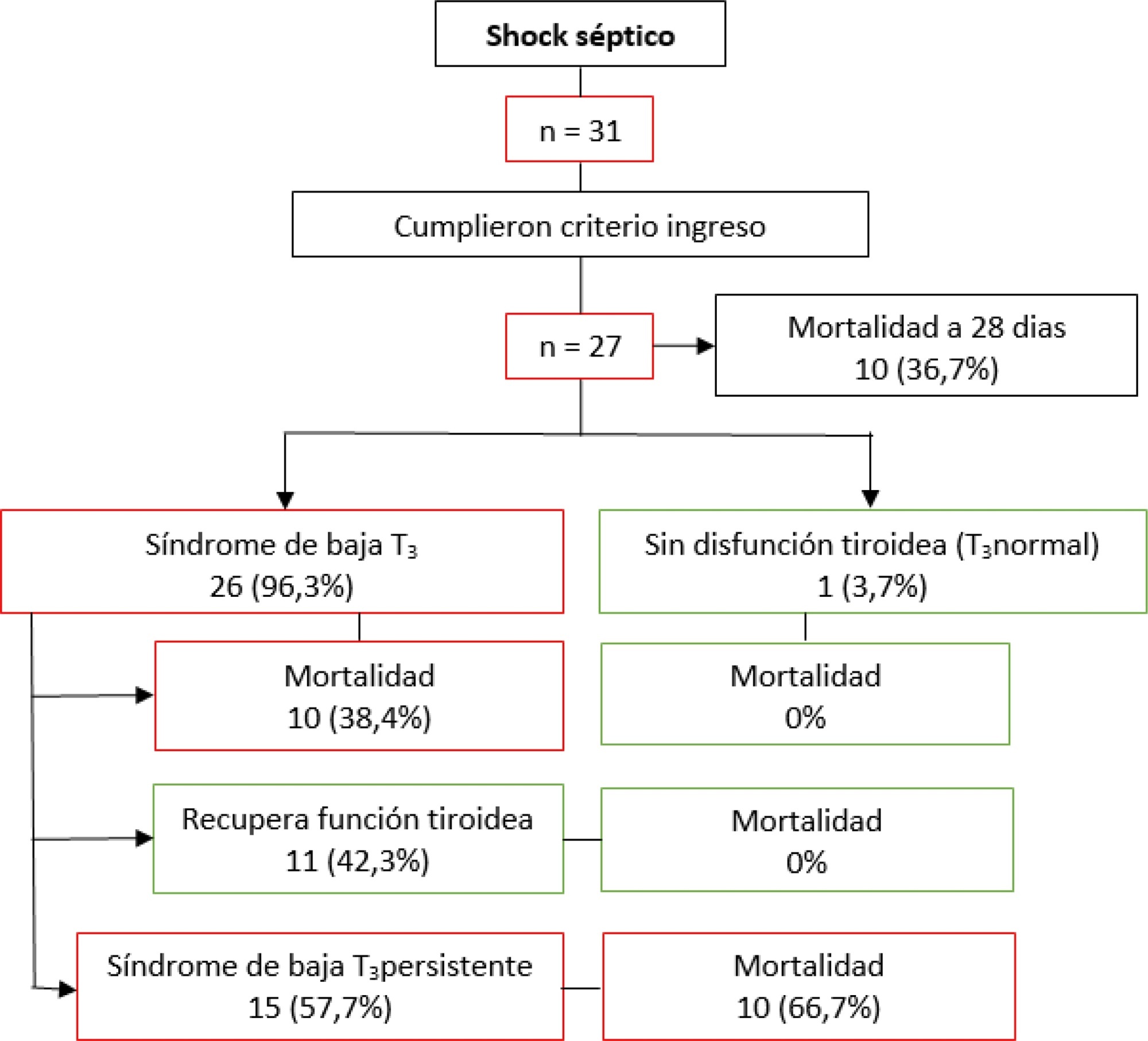
A total of 27 patients who met the inclusion criteria were analyzed. The incidence of an altered thyroid axis was 96.3%, with a mortality at 28 days of 36.7%. Patients without hormonal alteration did not present negative outcomes. Among those with low triiodothyronine, 42.3% recovered their thyroid function within 28 days, in whom mortality was 0%; 57.7% did not recover their thyroid function, in whom mortality was 66.7%. Those whose thyroid axis was altered and who did not normalize its function required more doses of vasoactives and had deteriorated lactate clearance.
Patients with septic shock have a high incidence of alteration of the thyroid axis, and this dysfunction is associated with higher mortality.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):514-520
DOI 10.5935/0103-507X.20200088
Low levels of thyroid hormones have been associated with poor clinical outcomes. This metabolic situation, designated euthyroid sick syndrome, has been interpreted as a state of adaptation to different pathological processes, characterized by the decrease in plasma triiodothyronine. The present study seeks to determine the incidence of this disorder in patients with septic shock and its relationship with other severity indices and clinical outcomes.
This prospective analytical study evaluated patients admitted to the intensive care unit with septic shock between April 2018 and July 2019. Variables associated with septic shock and thyroid profile were recorded at the time of the septic shock diagnosis and 7, 14, and 21 days later.
A total of 27 patients who met the inclusion criteria were analyzed. The incidence of an altered thyroid axis was 96.3%, with a mortality at 28 days of 36.7%. Patients without hormonal alteration did not present negative outcomes. Among those with low triiodothyronine, 42.3% recovered their thyroid function within 28 days, in whom mortality was 0%; 57.7% did not recover their thyroid function, in whom mortality was 66.7%. Those whose thyroid axis was altered and who did not normalize its function required more doses of vasoactives and had deteriorated lactate clearance.
Patients with septic shock have a high incidence of alteration of the thyroid axis, and this dysfunction is associated with higher mortality.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):229-234
DOI 10.5935/0103-507X.20200041
To depict the clinical presentation and outcomes of a cohort of critically ill patients with esophageal cancer.
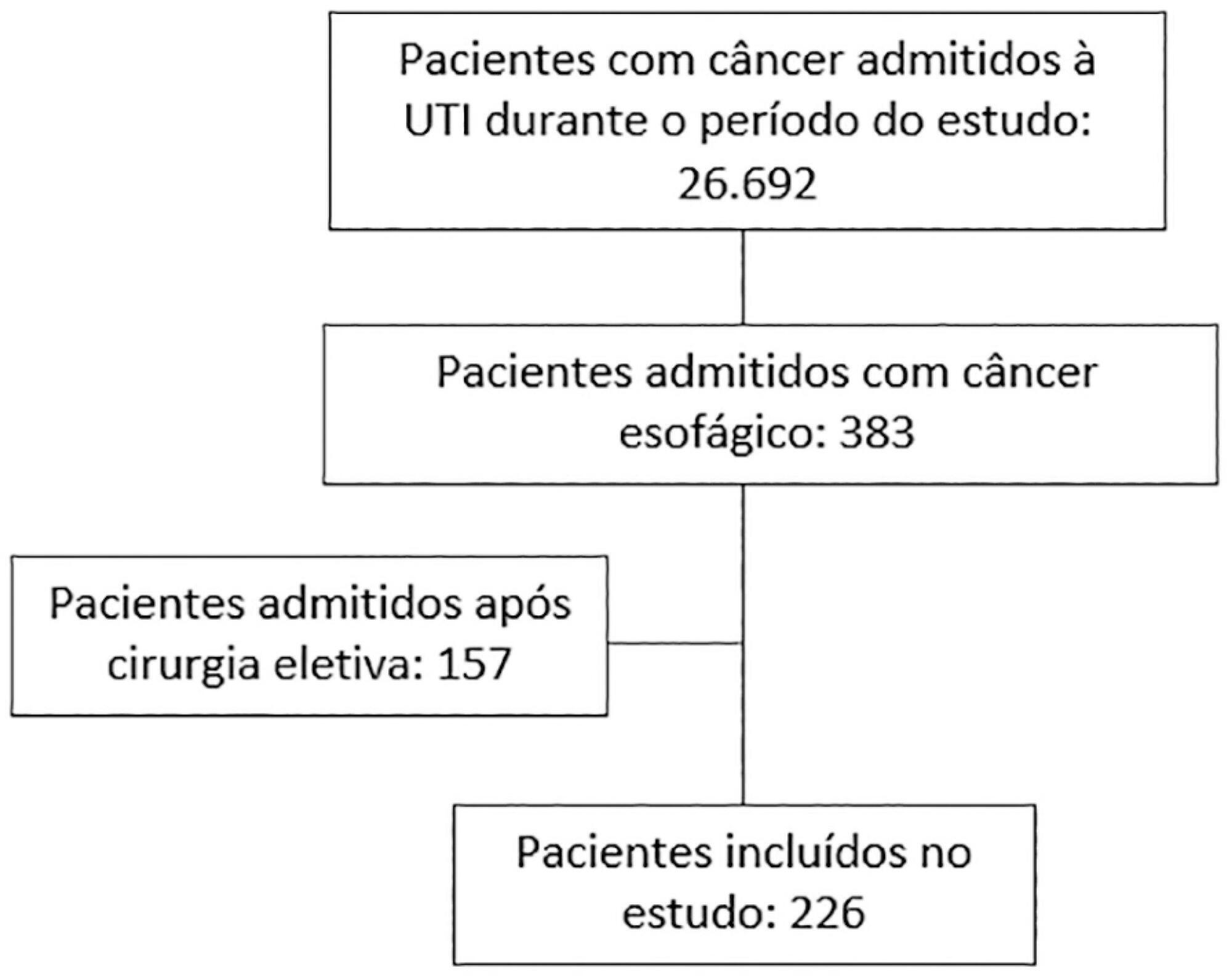
We carried out a multicenter retrospective study that included patients with esophageal cancer admitted to intensive care units with acute illness between September 2009 and December 2017. We collected the demographic and clinical characteristics of all included patients, as well as organ-support measures and hospital outcomes. We performed logistic regression analysis to identify independent factors associated with in-hospital mortality.
Of 226 patients included in the study, 131 (58.0%) patients died before hospital discharge. Squamous cell carcinoma was more frequent than adenocarcinoma, and 124 (54.9%) patients had metastatic cancer. The main reasons for admission were sepsis/septic shock and acute respiratory failure. Mechanical ventilation (OR = 6.18; 95%CI 2.86 - 13.35) and metastatic disease (OR = 7.10; 95%CI 3.35 - 15.05) were independently associated with in-hospital mortality.
In this cohort of patients with esophageal cancer admitted to intensive care units with acute illness, the in-hospital mortality rate was very high. The requirement for invasive mechanical ventilation and metastatic disease were independent prognostic factors and should be considered in discussions about the short-term outcomes of these patients.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):229-234
DOI 10.5935/0103-507X.20200041
To depict the clinical presentation and outcomes of a cohort of critically ill patients with esophageal cancer.
We carried out a multicenter retrospective study that included patients with esophageal cancer admitted to intensive care units with acute illness between September 2009 and December 2017. We collected the demographic and clinical characteristics of all included patients, as well as organ-support measures and hospital outcomes. We performed logistic regression analysis to identify independent factors associated with in-hospital mortality.
Of 226 patients included in the study, 131 (58.0%) patients died before hospital discharge. Squamous cell carcinoma was more frequent than adenocarcinoma, and 124 (54.9%) patients had metastatic cancer. The main reasons for admission were sepsis/septic shock and acute respiratory failure. Mechanical ventilation (OR = 6.18; 95%CI 2.86 - 13.35) and metastatic disease (OR = 7.10; 95%CI 3.35 - 15.05) were independently associated with in-hospital mortality.
In this cohort of patients with esophageal cancer admitted to intensive care units with acute illness, the in-hospital mortality rate was very high. The requirement for invasive mechanical ventilation and metastatic disease were independent prognostic factors and should be considered in discussions about the short-term outcomes of these patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):497-503
DOI 10.5935/0103-507X.20190087
To evaluate whether electromyographical findings could predict intensive care unit mortality among mechanically ventilated septic patients under profound sedation.
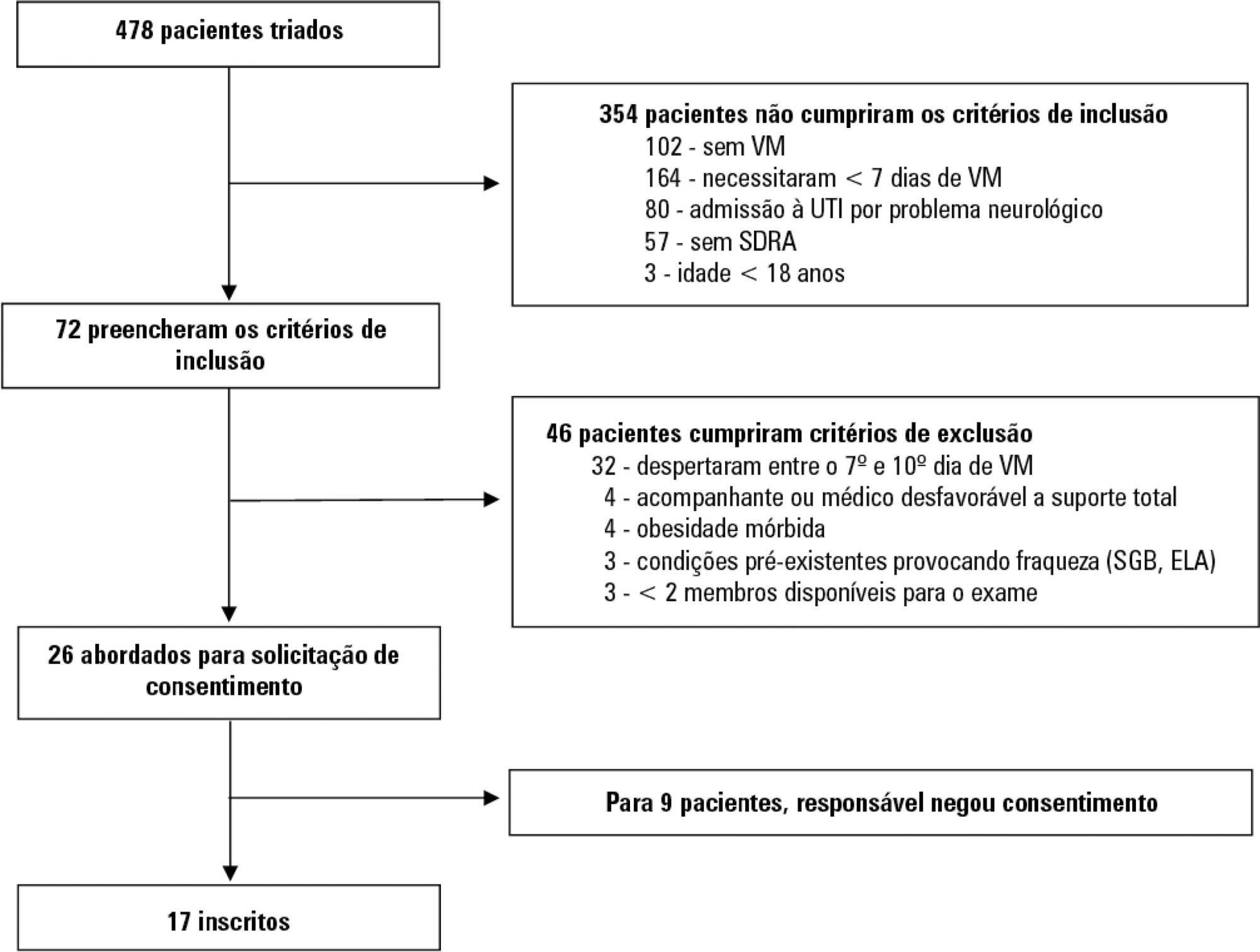
A prospective cohort study that consecutively enrolled moderate-severe acute respiratory distress syndrome (partial pressure of oxygen/fraction of inspired oxygen < 200) patients who were ≥ 18 years of age, dependent on mechanical ventilation for ≥ 7 days, and under profound sedation (Richmond Agitation Sedation Scale ≤ -4) was conducted. Electromyographic studies of the limbs were performed in all patients between the 7th and the 10th day of mechanical ventilation. Sensory nerve action potentials were recorded from the median and sural nerves. The compound muscle action potentials were recorded from the median (abductor pollicis brevis muscle) and common peroneal (extensor digitorum brevis muscle) nerves.
Seventeen patients were enrolled during the seven months of the study. Nine patients (53%) had electromyographic signs of critical illness myopathy or neuropathy. The risk of death during the intensive care unit stay was increased in patients with electromyographical signs of critical illness myopathy or neuropathy in comparison to those without these diagnostics (77.7% versus 12.5%, log-rank p = 0.02).
Electromyographical signs of critical illness myopathy or neuropathy between the 7th and the 10th day of mechanical ventilation may be associated with intensive care unit mortality among moderate-severe acute respiratory distress syndrome patients under profound sedation, in whom clinical strength assessment is not possible.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):497-503
DOI 10.5935/0103-507X.20190087
To evaluate whether electromyographical findings could predict intensive care unit mortality among mechanically ventilated septic patients under profound sedation.
A prospective cohort study that consecutively enrolled moderate-severe acute respiratory distress syndrome (partial pressure of oxygen/fraction of inspired oxygen < 200) patients who were ≥ 18 years of age, dependent on mechanical ventilation for ≥ 7 days, and under profound sedation (Richmond Agitation Sedation Scale ≤ -4) was conducted. Electromyographic studies of the limbs were performed in all patients between the 7th and the 10th day of mechanical ventilation. Sensory nerve action potentials were recorded from the median and sural nerves. The compound muscle action potentials were recorded from the median (abductor pollicis brevis muscle) and common peroneal (extensor digitorum brevis muscle) nerves.
Seventeen patients were enrolled during the seven months of the study. Nine patients (53%) had electromyographic signs of critical illness myopathy or neuropathy. The risk of death during the intensive care unit stay was increased in patients with electromyographical signs of critical illness myopathy or neuropathy in comparison to those without these diagnostics (77.7% versus 12.5%, log-rank p = 0.02).
Electromyographical signs of critical illness myopathy or neuropathy between the 7th and the 10th day of mechanical ventilation may be associated with intensive care unit mortality among moderate-severe acute respiratory distress syndrome patients under profound sedation, in whom clinical strength assessment is not possible.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):386-392
DOI 10.5935/0103-507X.20190051
The improvement in cardiopulmonary resuscitation quality has reduced the mortality of individuals treated for cardiac arrest. However, survivors have a high risk of severe brain damage in cases of return of spontaneous circulation. Data suggest that cases of cardiac arrest in critically ill patients with non-shockable rhythms have only a 6% chance of returning of spontaneous circulation, and of these, only one-third recover their autonomy. Should we, therefore, opt for a procedure in which the chance of survival is minimal and the risk of hospital death or severe and definitive brain damage is approximately 70%? Is it worth discussing patient resuscitation in cases of cardiac arrest? Would this discussion bring any benefit to the patients and their family members? Advanced discussions on do-not-resuscitate are based on the ethical principle of respect for patient autonomy, as the wishes of family members and physicians often do not match those of patients. In addition to the issue of autonomy, advanced discussions can help the medical and care team anticipate future problems and, thus, better plan patient care. Our opinion is that discussions regarding the resuscitation of critically ill patients should be performed for all patients within the first 24 to 48 hours after admission to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):386-392
DOI 10.5935/0103-507X.20190051
The improvement in cardiopulmonary resuscitation quality has reduced the mortality of individuals treated for cardiac arrest. However, survivors have a high risk of severe brain damage in cases of return of spontaneous circulation. Data suggest that cases of cardiac arrest in critically ill patients with non-shockable rhythms have only a 6% chance of returning of spontaneous circulation, and of these, only one-third recover their autonomy. Should we, therefore, opt for a procedure in which the chance of survival is minimal and the risk of hospital death or severe and definitive brain damage is approximately 70%? Is it worth discussing patient resuscitation in cases of cardiac arrest? Would this discussion bring any benefit to the patients and their family members? Advanced discussions on do-not-resuscitate are based on the ethical principle of respect for patient autonomy, as the wishes of family members and physicians often do not match those of patients. In addition to the issue of autonomy, advanced discussions can help the medical and care team anticipate future problems and, thus, better plan patient care. Our opinion is that discussions regarding the resuscitation of critically ill patients should be performed for all patients within the first 24 to 48 hours after admission to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 - 0.86); 0.70 (95%CI 0.61 - 0.79); 0.54 (95%CI 0.42 - 0.65); 0.48 (95%CI 0.36 - 0.58); and 0.68 (95%CI 0.58 - 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 - 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 - 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 - 2.022).
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 - 0.86); 0.70 (95%CI 0.61 - 0.79); 0.54 (95%CI 0.42 - 0.65); 0.48 (95%CI 0.36 - 0.58); and 0.68 (95%CI 0.58 - 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 - 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 - 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 - 2.022).
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)