
You searched for:"Vitor Mendes"
We found (3) results for your search.-
Original Article
What changed between the peak and plateau periods of the first COVID-19 pandemic wave? A multicentric Portuguese cohort study in intensive care
- Rui Antunes Pereira
 ,
, - Marta Sousa ,
- José Pedro Cidade ,
- Luís Melo ,
- Diogo Lopes , [ … ],
- Susana Mendes Fernandes
Abstract
Original ArticleWhat changed between the peak and plateau periods of the first COVID-19 pandemic wave? A multicentric Portuguese cohort study in intensive care
Rev Bras Ter Intensiva. 2022;34(4):433-442
DOI 10.5935/0103-507X.20210037-en
- Rui Antunes Pereira ,
- Marta Sousa ,
- José Pedro Cidade ,
- Luís Melo ,
- Diogo Lopes ,
- Sara Ventura ,
- Irene Aragão ,
- Raul Miguel de Freitas Lima Neto ,
- Elena Molinos ,
- Ana Marques ,
- Nelson Cardoso ,
- Flávio Marino ,
- Filipa Brás Monteiro ,
- Ana Pinho Oliveira ,
- Rogério C Silva ,
- André Miguel Neto Real ,
- Bruno Sarmento Banheiro ,
- Renato Reis ,
- Maria Adão-Serrano ,
- Ana Cracium ,
- Ana Valadas ,
- João Miguel Ribeiro ,
- Pedro Póvoa ,
- Camila Tapadinhas ,
- Vítor Mendes ,
- Luís Coelho ,
- Raquel Maia ,
- Paulo Telles Freitas ,
- Isabel Amorim Ferreira ,
- Tiago Ramires ,
- Luís Silva Val-Flores ,
- Mariana Cascão ,
- Rita Alves ,
- Simão C Rodeia ,
- Cleide Barrigoto ,
- Rosa Cardiga ,
- Maria João Ferreira da Silva ,
- Bruno Vale ,
- Tatiana Fonseca ,
- Ana Lúcia Rios,
- João Camões ,
- Danay Pérez,
- Susana Cabral ,
- Maria Inês Ribeiro,
- João João Mendes ,
- João Gouveia ,
- Susana Mendes Fernandes
Views1ABSTRACT
Objective:
To analyze and compare COVID-19 patient characteristics, clinical management and outcomes between the peak and plateau periods of the first pandemic wave in Portugal.
Methods:
This was a multicentric ambispective cohort study including consecutive severe COVID-19 patients between March and August 2020 from 16 Portuguese intensive care units. The peak and plateau periods, respectively, weeks 10 – 16 and 17 – 34, were defined.
Results:
Five hundred forty-one adult patients with a median age of 65 [57 – 74] years, mostly male (71.2%), were included. There were no significant differences in median age (p = 0.3), Simplified Acute Physiology Score II (40 versus 39; p = 0.8), partial arterial oxygen pressure/fraction of inspired oxygen ratio (139 versus 136; p = 0.6), antibiotic therapy (57% versus 64%; p = 0.2) at admission, or 28-day mortality (24.4% versus 22.8%; p = 0.7) between the peak and plateau periods. During the peak period, patients had fewer comorbidities (1 [0 – 3] versus 2 [0 – 5]; p = 0.002) and presented a higher use of vasopressors (47% versus 36%; p < 0.001) and invasive mechanical ventilation (58.1 versus 49.2%; p < 0.001) at admission, prone positioning (45% versus 36%; p = 0.04), and hydroxychloroquine (59% versus 10%; p < 0.001) and lopinavir/ritonavir (41% versus 10%; p < 0.001) prescriptions. However, a greater use of high-flow nasal cannulas (5% versus 16%, p < 0.001) on admission, remdesivir (0.3% versus 15%; p < 0.001) and corticosteroid (29% versus 52%, p < 0.001) therapy, and a shorter ICU length of stay (12 days versus 8, p < 0.001) were observed during the plateau.
Conclusion:
There were significant changes in patient comorbidities, intensive care unit therapies and length of stay between the peak and plateau periods of the first COVID-19 wave.
Keywords:acute respiratory distress syndromeAdrenal cortex hormonesCoronavirus infectionsCOVID-19Critical care outcomesCritical illnessIntensive carePandemicsSARS-CoV-2See moreViews1

Abstract
Original ArticleWhat changed between the peak and plateau periods of the first COVID-19 pandemic wave? A multicentric Portuguese cohort study in intensive care
Rev Bras Ter Intensiva. 2022;34(4):433-442
DOI 10.5935/0103-507X.20210037-en
- Rui Antunes Pereira ,
- Marta Sousa ,
- José Pedro Cidade ,
- Luís Melo ,
- Diogo Lopes ,
- Sara Ventura ,
- Irene Aragão ,
- Raul Miguel de Freitas Lima Neto ,
- Elena Molinos ,
- Ana Marques ,
- Nelson Cardoso ,
- Flávio Marino ,
- Filipa Brás Monteiro ,
- Ana Pinho Oliveira ,
- Rogério C Silva ,
- André Miguel Neto Real ,
- Bruno Sarmento Banheiro ,
- Renato Reis ,
- Maria Adão-Serrano ,
- Ana Cracium ,
- Ana Valadas ,
- João Miguel Ribeiro ,
- Pedro Póvoa ,
- Camila Tapadinhas ,
- Vítor Mendes ,
- Luís Coelho ,
- Raquel Maia ,
- Paulo Telles Freitas ,
- Isabel Amorim Ferreira ,
- Tiago Ramires ,
- Luís Silva Val-Flores ,
- Mariana Cascão ,
- Rita Alves ,
- Simão C Rodeia ,
- Cleide Barrigoto ,
- Rosa Cardiga ,
- Maria João Ferreira da Silva ,
- Bruno Vale ,
- Tatiana Fonseca ,
- Ana Lúcia Rios,
- João Camões ,
- Danay Pérez,
- Susana Cabral ,
- Maria Inês Ribeiro,
- João João Mendes ,
- João Gouveia ,
- Susana Mendes Fernandes
Views1ABSTRACT
Objective:
To analyze and compare COVID-19 patient characteristics, clinical management and outcomes between the peak and plateau periods of the first pandemic wave in Portugal.
Methods:
This was a multicentric ambispective cohort study including consecutive severe COVID-19 patients between March and August 2020 from 16 Portuguese intensive care units. The peak and plateau periods, respectively, weeks 10 – 16 and 17 – 34, were defined.
Results:
Five hundred forty-one adult patients with a median age of 65 [57 – 74] years, mostly male (71.2%), were included. There were no significant differences in median age (p = 0.3), Simplified Acute Physiology Score II (40 versus 39; p = 0.8), partial arterial oxygen pressure/fraction of inspired oxygen ratio (139 versus 136; p = 0.6), antibiotic therapy (57% versus 64%; p = 0.2) at admission, or 28-day mortality (24.4% versus 22.8%; p = 0.7) between the peak and plateau periods. During the peak period, patients had fewer comorbidities (1 [0 – 3] versus 2 [0 – 5]; p = 0.002) and presented a higher use of vasopressors (47% versus 36%; p < 0.001) and invasive mechanical ventilation (58.1 versus 49.2%; p < 0.001) at admission, prone positioning (45% versus 36%; p = 0.04), and hydroxychloroquine (59% versus 10%; p < 0.001) and lopinavir/ritonavir (41% versus 10%; p < 0.001) prescriptions. However, a greater use of high-flow nasal cannulas (5% versus 16%, p < 0.001) on admission, remdesivir (0.3% versus 15%; p < 0.001) and corticosteroid (29% versus 52%, p < 0.001) therapy, and a shorter ICU length of stay (12 days versus 8, p < 0.001) were observed during the plateau.
Conclusion:
There were significant changes in patient comorbidities, intensive care unit therapies and length of stay between the peak and plateau periods of the first COVID-19 wave.
Keywords:acute respiratory distress syndromeAdrenal cortex hormonesCoronavirus infectionsCOVID-19Critical care outcomesCritical illnessIntensive carePandemicsSARS-CoV-2See more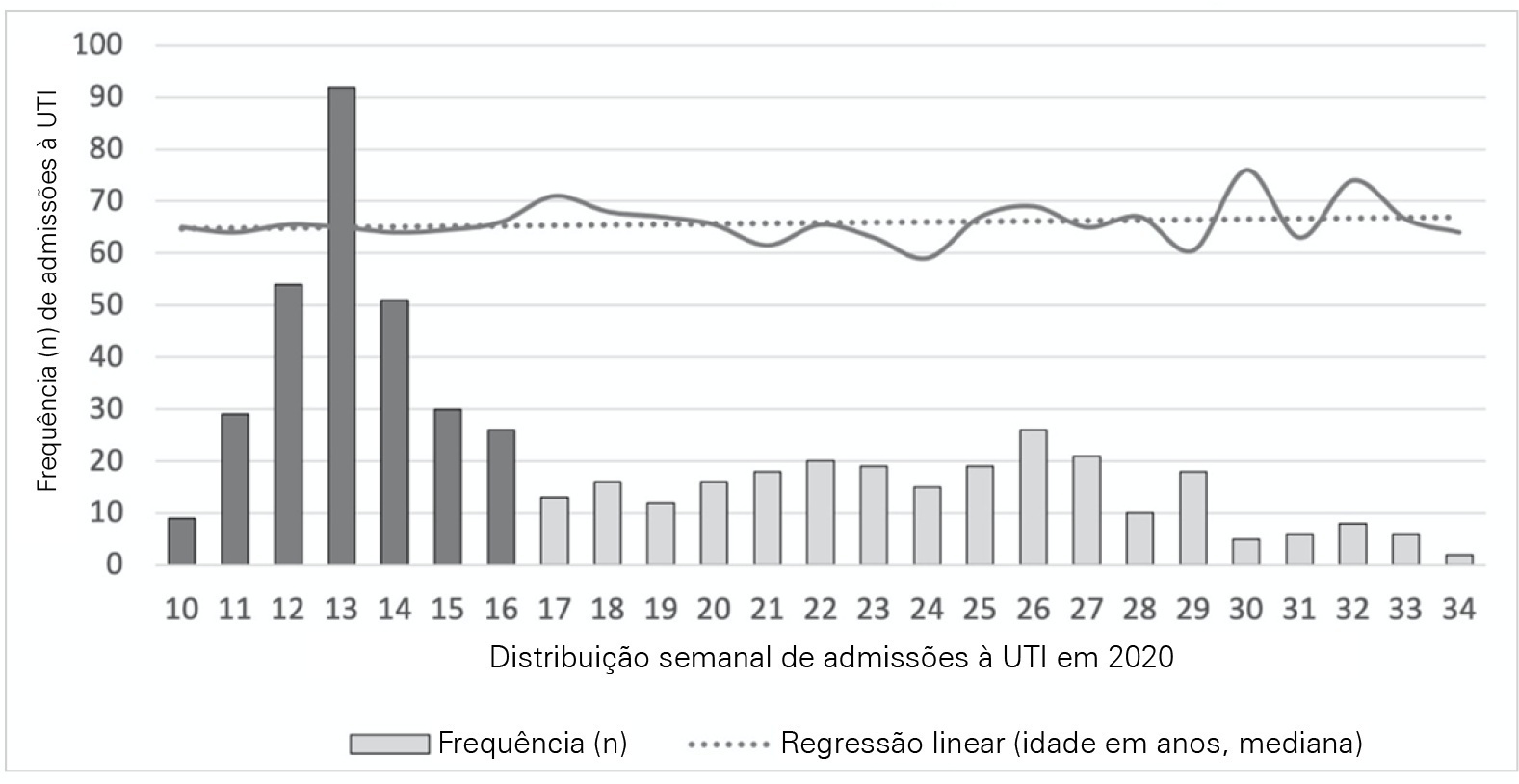
- Rui Antunes Pereira
-
Original Article
suPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
Abstract
Original ArticlesuPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
Views0See moreABSTRACT
Objective:
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
Methods:
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Results:
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 – 0.86); 0.70 (95%CI 0.61 – 0.79); 0.54 (95%CI 0.42 – 0.65); 0.48 (95%CI 0.36 – 0.58); and 0.68 (95%CI 0.58 – 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 – 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 – 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 – 2.022).
Conclusion:
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
Views0Abstract
Original ArticlesuPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
Views0See moreABSTRACT
Objective:
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
Methods:
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Results:
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 – 0.86); 0.70 (95%CI 0.61 – 0.79); 0.54 (95%CI 0.42 – 0.65); 0.48 (95%CI 0.36 – 0.58); and 0.68 (95%CI 0.58 – 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 – 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 – 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 – 2.022).
Conclusion:
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
-
Original Articles – Clinical Research
The neuroprotective role of therapeutic hypothermia after cardiac arrest
Rev Bras Ter Intensiva. 2011;23(4):455-461
Abstract
Original Articles – Clinical ResearchThe neuroprotective role of therapeutic hypothermia after cardiac arrest
Rev Bras Ter Intensiva. 2011;23(4):455-461
DOI 10.1590/S0103-507X2011000400010
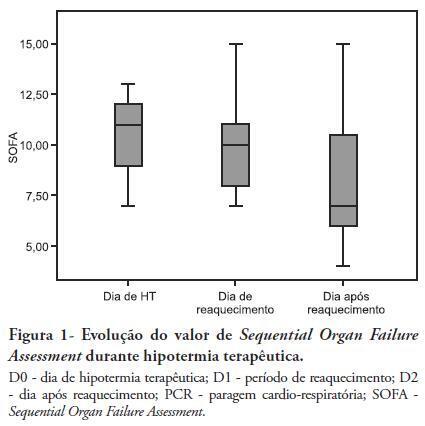
Views0See moreOBJECTIVES: Therapeutic hypothermia following cardiorespiratory arrest has been demonstrated to have cardio- and neuroprotective effects, resulting in improved survival and better neurological outcomes. The objective of this study was to assess the outcomes of patients undergoing therapeutic hypothermia following cardiorespiratory arrest. METHODS: A prospective, 10-month observational study of patients admitted to an intensive care unit and undergoing therapeutic hypothermia after cardiorespiratory arrest was undertaken. Therapeutic hypothermia was induced by cold fluid administration and body surface cooling in patients admitted no more than 12 hours after resuscitation from cardiorespiratory arrest. A target temperature of 33ºC was maintained for 24 hours. RESULTS: Overall, 12 patients were included (median age 64 years, 58% male). Half of the cardiorespiratory arrests were in-hospital. The median first-day Charlson Index, Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation II scores were of 2.9, 11 and 24.5, respectively. The intensive care unit mortality rate was 42% (N=5). Five of the 7 surviving patients recovered their pre-cardiorespiratory arrest neurological status. Hypothermia was initiated 120 min (median) after recovery of spontaneous circulation. Most patients (75%) required vasopressor support. During the first 3 days after cardiorespiratory arrest and therapeutic hypothermia, a progressive SOFA score decrease (median 11 on day 0, 10 on day 1 and 7 on day 2) was observed. DISCUSSION: In this study, therapeutic hypothermia was applied to all post-cardiorespiratory arrest patients and demonstrated good neurological outcome in surviving patients.
Views0Abstract
Original Articles – Clinical ResearchThe neuroprotective role of therapeutic hypothermia after cardiac arrest
Rev Bras Ter Intensiva. 2011;23(4):455-461
DOI 10.1590/S0103-507X2011000400010
Views0See moreOBJECTIVES: Therapeutic hypothermia following cardiorespiratory arrest has been demonstrated to have cardio- and neuroprotective effects, resulting in improved survival and better neurological outcomes. The objective of this study was to assess the outcomes of patients undergoing therapeutic hypothermia following cardiorespiratory arrest. METHODS: A prospective, 10-month observational study of patients admitted to an intensive care unit and undergoing therapeutic hypothermia after cardiorespiratory arrest was undertaken. Therapeutic hypothermia was induced by cold fluid administration and body surface cooling in patients admitted no more than 12 hours after resuscitation from cardiorespiratory arrest. A target temperature of 33ºC was maintained for 24 hours. RESULTS: Overall, 12 patients were included (median age 64 years, 58% male). Half of the cardiorespiratory arrests were in-hospital. The median first-day Charlson Index, Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation II scores were of 2.9, 11 and 24.5, respectively. The intensive care unit mortality rate was 42% (N=5). Five of the 7 surviving patients recovered their pre-cardiorespiratory arrest neurological status. Hypothermia was initiated 120 min (median) after recovery of spontaneous circulation. Most patients (75%) required vasopressor support. During the first 3 days after cardiorespiratory arrest and therapeutic hypothermia, a progressive SOFA score decrease (median 11 on day 0, 10 on day 1 and 7 on day 2) was observed. DISCUSSION: In this study, therapeutic hypothermia was applied to all post-cardiorespiratory arrest patients and demonstrated good neurological outcome in surviving patients.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis