-
Editorial
RBTI and history
Rev Bras Ter Intensiva. 2008;20(4):7-7
-
Original Articles
Validation of sedation scores in mechanically ventilated children admitted to a tertiary pediatric intensive care unit
Rev Bras Ter Intensiva. 2008;20(4):325-330
Abstract
Original ArticlesValidation of sedation scores in mechanically ventilated children admitted to a tertiary pediatric intensive care unit
Rev Bras Ter Intensiva. 2008;20(4):325-330
DOI 10.1590/S0103-507X2008000400002
Views0OBJECTIVES: Sedation scores are important tools for use in pediatric intensive care units. The Comfort-Behavior scale is a valid method for the assessment of children although it is considered an extensive scale. The motor activity assessment scale is validated for an adult population. We considered it simpler then the one above and suitable for application in children. None of these scores had been translated into Portuguese. Our objective was to apply both scales in Portuguese to a pediatric population under mechanical ventilation. Secondary objectives were to evaluate the sedation level of children on mechanical ventilation in tertiary pediatric intensive care units and to compare the Comfort- Behavior and motor activity assessment scales in this population. METHODS: After translating the scales into Portuguese, both were simultaneously applied to 26 patients by 2 pediatricians. Each scale was applied 116 times in total. RESULTS: The intraclass correlation coefficient was 0.90 (0.85 – 0.93 CI 95%) for the Comfort-Behavior and 0.94 (0.92 – 0.96 CI 95%) for the motor activity assessment scale. When applying the Comfort-Behavior scale, the Crombach’s alpha was 0.81 for observer A and 0.92 for observer B. The Spearman coefficient was 0.86 for observer A and 0.91 for observer B. These patients were found to be deeply sedated, showing low values in both scales. CONCLUSIONS: The scales were successfully translated into Portuguese and both were adequate to assess pain and sedation in the pediatric population under mechanical ventilation. Sedation level was high in this sample of applications.
Keywords:AnalgesicsChildChild behaviorIntensive care units, pediatricMonitoring, physiologicPain measurementRespiration, artificialSee moreViews0

Abstract
Original ArticlesValidation of sedation scores in mechanically ventilated children admitted to a tertiary pediatric intensive care unit
Rev Bras Ter Intensiva. 2008;20(4):325-330
DOI 10.1590/S0103-507X2008000400002
Views0OBJECTIVES: Sedation scores are important tools for use in pediatric intensive care units. The Comfort-Behavior scale is a valid method for the assessment of children although it is considered an extensive scale. The motor activity assessment scale is validated for an adult population. We considered it simpler then the one above and suitable for application in children. None of these scores had been translated into Portuguese. Our objective was to apply both scales in Portuguese to a pediatric population under mechanical ventilation. Secondary objectives were to evaluate the sedation level of children on mechanical ventilation in tertiary pediatric intensive care units and to compare the Comfort- Behavior and motor activity assessment scales in this population. METHODS: After translating the scales into Portuguese, both were simultaneously applied to 26 patients by 2 pediatricians. Each scale was applied 116 times in total. RESULTS: The intraclass correlation coefficient was 0.90 (0.85 – 0.93 CI 95%) for the Comfort-Behavior and 0.94 (0.92 – 0.96 CI 95%) for the motor activity assessment scale. When applying the Comfort-Behavior scale, the Crombach’s alpha was 0.81 for observer A and 0.92 for observer B. The Spearman coefficient was 0.86 for observer A and 0.91 for observer B. These patients were found to be deeply sedated, showing low values in both scales. CONCLUSIONS: The scales were successfully translated into Portuguese and both were adequate to assess pain and sedation in the pediatric population under mechanical ventilation. Sedation level was high in this sample of applications.
Keywords:AnalgesicsChildChild behaviorIntensive care units, pediatricMonitoring, physiologicPain measurementRespiration, artificialSee more -
Original Articles
Comparison between open and closed suction systems: a systematic review
Rev Bras Ter Intensiva. 2008;20(4):331-338
Abstract
Original ArticlesComparison between open and closed suction systems: a systematic review
Rev Bras Ter Intensiva. 2008;20(4):331-338
DOI 10.1590/S0103-507X2008000400003
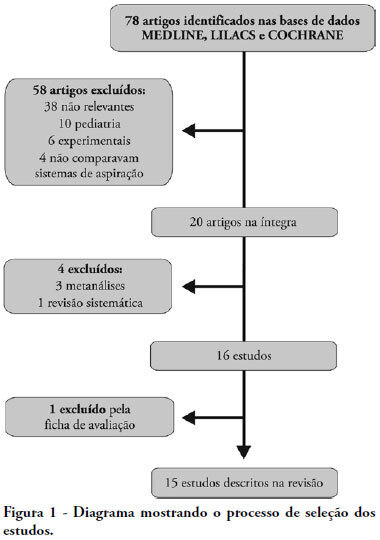
Views0See moreOBJECTIVES: This study attempted to identify which is the more effective suction system. The objective was to compare open versus closed suction systems according to a systematic review. METHODS: A search of scientific literature was conducted in MedLine, LILACS and Cochrane between 1997 and August 2007 using the key words: endotracheal suction and closed suction. Included were articles that compared the open and closed suction systems used in adult humans and that were randomized and controlled trials. RESULTS: From the 78 articles identified, only 15 were accepted and described in this review. Nine compared incidence of ventilator-associated pneumonia, six compared oxygen saturation, four compared blood pressure and heart rate, three compared pulmonary volumes, two compared secretion removal and four compared costs. No difference was found in these variables compared: incidence of ventilator associated pneumonia, mortality, intensive care unit length of stay, duration of mechanical ventilation, PaCO2, PaO2, mean blood pressure, heart rate and secretion removal. However, there were always SpO2 and pulmonary volume decreases when using the open suction system; and costs were lower in most of the studies that used the closed suction system. CONCLUSIONS: Closed suction system seems to increase the risk of colonization, but has the advantage of not reducing the pulmonary volumes and not entailing a drop of saturation, especially in patients with severe respiratory failure and in the use of higher levels of positive end expiratory pressure.
Views0Abstract
Original ArticlesComparison between open and closed suction systems: a systematic review
Rev Bras Ter Intensiva. 2008;20(4):331-338
DOI 10.1590/S0103-507X2008000400003
Views0See moreOBJECTIVES: This study attempted to identify which is the more effective suction system. The objective was to compare open versus closed suction systems according to a systematic review. METHODS: A search of scientific literature was conducted in MedLine, LILACS and Cochrane between 1997 and August 2007 using the key words: endotracheal suction and closed suction. Included were articles that compared the open and closed suction systems used in adult humans and that were randomized and controlled trials. RESULTS: From the 78 articles identified, only 15 were accepted and described in this review. Nine compared incidence of ventilator-associated pneumonia, six compared oxygen saturation, four compared blood pressure and heart rate, three compared pulmonary volumes, two compared secretion removal and four compared costs. No difference was found in these variables compared: incidence of ventilator associated pneumonia, mortality, intensive care unit length of stay, duration of mechanical ventilation, PaCO2, PaO2, mean blood pressure, heart rate and secretion removal. However, there were always SpO2 and pulmonary volume decreases when using the open suction system; and costs were lower in most of the studies that used the closed suction system. CONCLUSIONS: Closed suction system seems to increase the risk of colonization, but has the advantage of not reducing the pulmonary volumes and not entailing a drop of saturation, especially in patients with severe respiratory failure and in the use of higher levels of positive end expiratory pressure.
-
Original Articles
Effects of respiratory physiotherapy on intracranial pressure and cerebral perfusion pressure in severe traumatic brain injury patients
Rev Bras Ter Intensiva. 2008;20(4):339-343
Abstract
Original ArticlesEffects of respiratory physiotherapy on intracranial pressure and cerebral perfusion pressure in severe traumatic brain injury patients
Rev Bras Ter Intensiva. 2008;20(4):339-343
DOI 10.1590/S0103-507X2008000400004
Views0OBJECTIVE: After brain injury intracranial hypertension is the major cause of mortality, in addition to the possibility of functional, behavioral and cognitive sequels. Scarcity of studies on the effects of respiratory physiotherapy on these patients may lead to contradictory performances. This study aimed to assess the effects of customary respiratory physiotherapy maneuvers on intracranial and cerebral perfusion pressures in patients with severe brain injury. METHODS: Clinical, prospective trial with patients with severe traumatic brain injury, mechanically ventilated and with a continued measurement of intracranial pressure. The effects of manual vibrocompression maneuvers and intratracheal aspiration with or without saline infusion on the measurements of intracranial and cerebral perfusion pressures, between the first and third day after cerebral injury were evaluated. RESULTS: Data were collected from 11 patients, 41 years of age (median) and APACHE II of 19.5 ± 5. The manual vibrocompression maneuver did not cause an increase of intracranial pressure on any of the days assessed. Intracranial pressure significantly increased after intratracheal aspiration maneuvers in relation to the basal measurement (day1, 9.5 ± 0.9 mm Hg vs 18.0 ± 3.2 mm Hg; day 2, 10.6 ± 1.7 mm Hg vs 21.4 ± 3.8 mm Hg; day 3, 14.4 ± 1.0 vs 24.9 ± 2.7 mm Hg; p<0.05 for all). However, these elevations were transient (about 27 seconds) and accompanied by compensatory increases of the cerebral perfusion pressure. CONCLUSION: The manual vibrocompression maneuver did not increase intracranial pressure or cerebral perfusion pressure in patients with severe brain injury. Intratracheal aspiration induced a significant and transient increase of the intracranial and cerebral perfusion pressures.
Keywords:Brain injuriesIntracranial hypertensionIntracranial pressureIntubation, intratrachealPhysical therapy modalitiesRespiratory therapySee moreViews0Abstract
Original ArticlesEffects of respiratory physiotherapy on intracranial pressure and cerebral perfusion pressure in severe traumatic brain injury patients
Rev Bras Ter Intensiva. 2008;20(4):339-343
DOI 10.1590/S0103-507X2008000400004
Views0OBJECTIVE: After brain injury intracranial hypertension is the major cause of mortality, in addition to the possibility of functional, behavioral and cognitive sequels. Scarcity of studies on the effects of respiratory physiotherapy on these patients may lead to contradictory performances. This study aimed to assess the effects of customary respiratory physiotherapy maneuvers on intracranial and cerebral perfusion pressures in patients with severe brain injury. METHODS: Clinical, prospective trial with patients with severe traumatic brain injury, mechanically ventilated and with a continued measurement of intracranial pressure. The effects of manual vibrocompression maneuvers and intratracheal aspiration with or without saline infusion on the measurements of intracranial and cerebral perfusion pressures, between the first and third day after cerebral injury were evaluated. RESULTS: Data were collected from 11 patients, 41 years of age (median) and APACHE II of 19.5 ± 5. The manual vibrocompression maneuver did not cause an increase of intracranial pressure on any of the days assessed. Intracranial pressure significantly increased after intratracheal aspiration maneuvers in relation to the basal measurement (day1, 9.5 ± 0.9 mm Hg vs 18.0 ± 3.2 mm Hg; day 2, 10.6 ± 1.7 mm Hg vs 21.4 ± 3.8 mm Hg; day 3, 14.4 ± 1.0 vs 24.9 ± 2.7 mm Hg; p<0.05 for all). However, these elevations were transient (about 27 seconds) and accompanied by compensatory increases of the cerebral perfusion pressure. CONCLUSION: The manual vibrocompression maneuver did not increase intracranial pressure or cerebral perfusion pressure in patients with severe brain injury. Intratracheal aspiration induced a significant and transient increase of the intracranial and cerebral perfusion pressures.
Keywords:Brain injuriesIntracranial hypertensionIntracranial pressureIntubation, intratrachealPhysical therapy modalitiesRespiratory therapySee more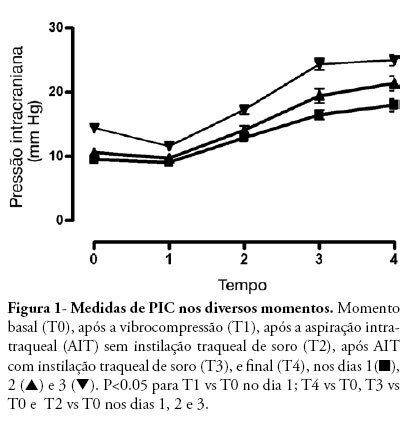
-
Original Articles
Ramsay and Richmond’s scores are equivalent to assessment sedation level on critical patients
Rev Bras Ter Intensiva. 2008;20(4):344-348
Abstract
Original ArticlesRamsay and Richmond’s scores are equivalent to assessment sedation level on critical patients
Rev Bras Ter Intensiva. 2008;20(4):344-348
DOI 10.1590/S0103-507X2008000400005
Views0OBJECTIVE: The main purpose of this study was to compare performance of the Ramsay and Richmond sedation scores on mechanically ventilated critically ill patients, in a university-affiliated hospital. METHODS: This was a 4-month prospective study, which included a total of 45 patients mechanically ventilated, with at least 48 hours stay in the intensive care unit. Each patient was assessed daily for sedation mode, sedative and analgesic doses and sedation level using the Ramsay and Richmond scores. Statistical analysis was made using Student’s t-test, Pearson’s and Spearman’s correlation, and constructing ROC-curves. RESULTS: A high general mortality of 60% was observed. The length of sedation and daily dose of medication did not correlate with mortality. Deep sedation (Ramsay > 4 or Richmond < -3) was positively correlated with probability of death with an AUC > 0.78. An adequate level of sedation (Ramsay 2 to 4 or Richmond 0 to -3) was sensitively correlated with probability of survival with an AUC > 0.80. A low level of sedation was observed in 63 days evaluated (8.64%), and no correlation was found between occurrence of agitation and unfavorable outcomes. Correlation between Ramsay and Richmond scores (Pearson’s > 0.810 – p<0.0001) was good. CONCLUSION: In this study, Ramsay and Richmond sedation scores were similar for the assessment of deep, insufficient and adequate sedation. Both have good correlation with mortality in over sedated patients.
Keywords:Deep sedationHypnotics and sedativesIntensive careIntensive care unitsMonitoring, physiologicRespiration, artificialSee moreViews0Abstract
Original ArticlesRamsay and Richmond’s scores are equivalent to assessment sedation level on critical patients
Rev Bras Ter Intensiva. 2008;20(4):344-348
DOI 10.1590/S0103-507X2008000400005
Views0OBJECTIVE: The main purpose of this study was to compare performance of the Ramsay and Richmond sedation scores on mechanically ventilated critically ill patients, in a university-affiliated hospital. METHODS: This was a 4-month prospective study, which included a total of 45 patients mechanically ventilated, with at least 48 hours stay in the intensive care unit. Each patient was assessed daily for sedation mode, sedative and analgesic doses and sedation level using the Ramsay and Richmond scores. Statistical analysis was made using Student’s t-test, Pearson’s and Spearman’s correlation, and constructing ROC-curves. RESULTS: A high general mortality of 60% was observed. The length of sedation and daily dose of medication did not correlate with mortality. Deep sedation (Ramsay > 4 or Richmond < -3) was positively correlated with probability of death with an AUC > 0.78. An adequate level of sedation (Ramsay 2 to 4 or Richmond 0 to -3) was sensitively correlated with probability of survival with an AUC > 0.80. A low level of sedation was observed in 63 days evaluated (8.64%), and no correlation was found between occurrence of agitation and unfavorable outcomes. Correlation between Ramsay and Richmond scores (Pearson’s > 0.810 – p<0.0001) was good. CONCLUSION: In this study, Ramsay and Richmond sedation scores were similar for the assessment of deep, insufficient and adequate sedation. Both have good correlation with mortality in over sedated patients.
Keywords:Deep sedationHypnotics and sedativesIntensive careIntensive care unitsMonitoring, physiologicRespiration, artificialSee more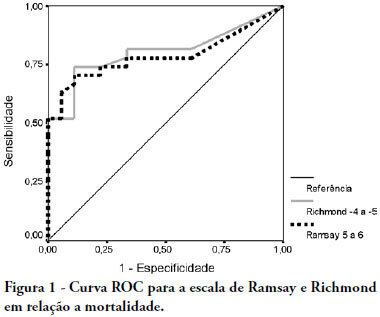
-
Original Articles
Potential drug interactions prevalence in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):349-354
Abstract
Original ArticlesPotential drug interactions prevalence in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):349-354
DOI 10.1590/S0103-507X2008000400006
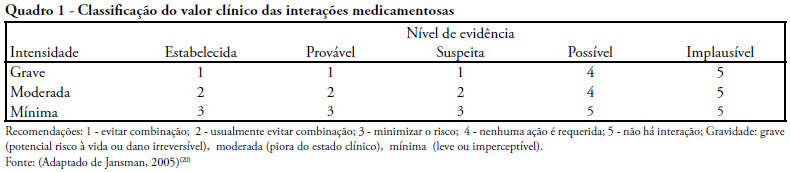
Views0See moreOBJECTIVES: Drug interactions occur when effects and/or toxicity of a drug are affected by presence of another drug. They are usually unpredictable and undesirable. A study was conducted to verify the prevalence and clinical value of potential drug interactions in intensive care units METHODS: All patients, of three intensive care units were included in a cross-sectional study, over a period of two months. Patients with less than a 2 days length of stay were excluded. Data were collected from twenty-four hour prescriptions and all possible paired combinations drug-drug were recorded. Prevalence and clinical value (significance) were checked at the end of follow-up. RESULTS: One hundred and forty patients were analyzed, 67.1% presented with some significant potential drug interactions and of the 1069 prescriptions, 39.2% disclosed the same potential. Of 188 different potential drug interactions, 29 were considered highly significant. Univariate analysis showed that in the group with significant potential drug interactions a higher number of different drugs, drugs/day had been used, there were more prescribing physicians and extended stay in intensive care units. Adjusted to the multivariate logistic regression model, only the number of drugs/day correlated with increased risk of significant potential drug interaction (p = 0.0011) and, furthermore that use of more than 6 drugs/day increased relative risk by 9.8 times. CONCLUSIONS: Critically ill patients are submitted to high risk of potential drug interactions and the number of drugs/day has a high positive predictive value for these interactions. Therefore, it is imperative that critical care physicians be constantly alert to recognize this problem and provide appropriate mechanisms for management, thereby reducing adverse outcomes.
Views0Abstract
Original ArticlesPotential drug interactions prevalence in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):349-354
DOI 10.1590/S0103-507X2008000400006
Views0See moreOBJECTIVES: Drug interactions occur when effects and/or toxicity of a drug are affected by presence of another drug. They are usually unpredictable and undesirable. A study was conducted to verify the prevalence and clinical value of potential drug interactions in intensive care units METHODS: All patients, of three intensive care units were included in a cross-sectional study, over a period of two months. Patients with less than a 2 days length of stay were excluded. Data were collected from twenty-four hour prescriptions and all possible paired combinations drug-drug were recorded. Prevalence and clinical value (significance) were checked at the end of follow-up. RESULTS: One hundred and forty patients were analyzed, 67.1% presented with some significant potential drug interactions and of the 1069 prescriptions, 39.2% disclosed the same potential. Of 188 different potential drug interactions, 29 were considered highly significant. Univariate analysis showed that in the group with significant potential drug interactions a higher number of different drugs, drugs/day had been used, there were more prescribing physicians and extended stay in intensive care units. Adjusted to the multivariate logistic regression model, only the number of drugs/day correlated with increased risk of significant potential drug interaction (p = 0.0011) and, furthermore that use of more than 6 drugs/day increased relative risk by 9.8 times. CONCLUSIONS: Critically ill patients are submitted to high risk of potential drug interactions and the number of drugs/day has a high positive predictive value for these interactions. Therefore, it is imperative that critical care physicians be constantly alert to recognize this problem and provide appropriate mechanisms for management, thereby reducing adverse outcomes.
-
Original Articles
Evaluation of extracurricular internships in the adult’s intensive care units
Rev Bras Ter Intensiva. 2008;20(4):355-361
Abstract
Original ArticlesEvaluation of extracurricular internships in the adult’s intensive care units
Rev Bras Ter Intensiva. 2008;20(4):355-361
DOI 10.1590/S0103-507X2008000400007
Views0OBJECTIVES: Students of Salvador – BA, Brazil were trained in critical care medicine by accomplishing extracurricular internships. This study aims to detect changes in attitude and interest of students who concluded these internships as well as the most frequent activities developed. METHODS: Descriptive cross-sectional survey conducted with students who did extracurricular internships in adult intensive care units during the second semester of 2006. A self-administered questionnaire was given using objective questions. RESULTS: We evaluated 49 students. Interest in becoming an intensivist was classified as high/very high by 32.7% before internship, after which 61.2% reported increased interest. Before internship, students on a 1 to 5 scale rated the importance of critical care medicine as 4.55 ± 0.70. After internship, 98% felt more confident to refer a patient to the intensive care unit, 95.9% to evaluate with supervision, patients admitted to intensive care units and 89.8% to attend patients in the emergency room. The most common procedures observed were: central venous access (100%), peripheral venous access (91.8%) and orotracheal intubation (91.8%). Topics ranked in terms of interest from 1 to 5 were: systemic inflammatory response syndrome/sepsis (4.82 ± 0.48), shock (4.81 ± 0.44) and cardiopulmonary resuscitation (4.77 ± 0.55). CONCLUSIONS: This study showed that internships in adult intensive care units of Salvador (BA), Brazil provided students with greater assurance to evaluate critical patients, increased their interest to follow an intensivist physician career and allowed contact with the main procedures and topics related to critical care medicine.
Keywords:Clinical clerkshipEducation, medicalFellowships and internshipsIntensive care unitsQuestionnairesStudents, medicalSee moreViews0Abstract
Original ArticlesEvaluation of extracurricular internships in the adult’s intensive care units
Rev Bras Ter Intensiva. 2008;20(4):355-361
DOI 10.1590/S0103-507X2008000400007
Views0OBJECTIVES: Students of Salvador – BA, Brazil were trained in critical care medicine by accomplishing extracurricular internships. This study aims to detect changes in attitude and interest of students who concluded these internships as well as the most frequent activities developed. METHODS: Descriptive cross-sectional survey conducted with students who did extracurricular internships in adult intensive care units during the second semester of 2006. A self-administered questionnaire was given using objective questions. RESULTS: We evaluated 49 students. Interest in becoming an intensivist was classified as high/very high by 32.7% before internship, after which 61.2% reported increased interest. Before internship, students on a 1 to 5 scale rated the importance of critical care medicine as 4.55 ± 0.70. After internship, 98% felt more confident to refer a patient to the intensive care unit, 95.9% to evaluate with supervision, patients admitted to intensive care units and 89.8% to attend patients in the emergency room. The most common procedures observed were: central venous access (100%), peripheral venous access (91.8%) and orotracheal intubation (91.8%). Topics ranked in terms of interest from 1 to 5 were: systemic inflammatory response syndrome/sepsis (4.82 ± 0.48), shock (4.81 ± 0.44) and cardiopulmonary resuscitation (4.77 ± 0.55). CONCLUSIONS: This study showed that internships in adult intensive care units of Salvador (BA), Brazil provided students with greater assurance to evaluate critical patients, increased their interest to follow an intensivist physician career and allowed contact with the main procedures and topics related to critical care medicine.
Keywords:Clinical clerkshipEducation, medicalFellowships and internshipsIntensive care unitsQuestionnairesStudents, medicalSee more -
Original Articles
Increased lipase and amilase levels in critically ill patients: retrospective study
Rev Bras Ter Intensiva. 2008;20(4):362-369
Abstract
Original ArticlesIncreased lipase and amilase levels in critically ill patients: retrospective study
Rev Bras Ter Intensiva. 2008;20(4):362-369
DOI 10.1590/S0103-507X2008000400008
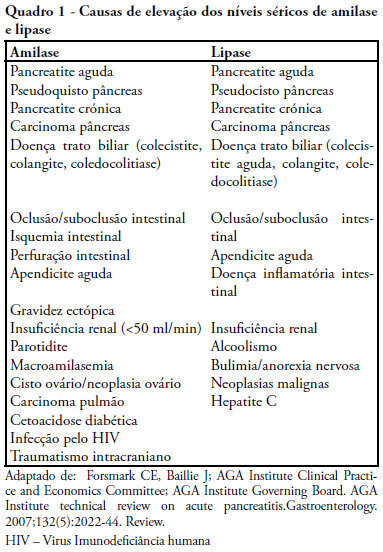
Views0See moreOBJECTIVES: Elevated lipase and amylase are commonly found in patients in intensive care unit without a previously recognized pancreatic illness, constituting a diagnostic and therapeutic challenge. The authors therefore proposed to determine the frequency of asymptomatic high serum lipase in critically ill patients, involved risk factors and outcome. METHODS: Retrospective study of patients admitted in an intensive care unit from January 1 to December 31, 2006, excluding admissions for acute pancreatitis, history of pancreatic disease, renal insufficiency or lacking of data. Patients were divided in two groups (with and without high serum lipase) that were compared for clinical, laboratory and radiological variables. Statistical analysis: SPSS 13; Student’s t test and Chi-square test (CI 95%) with statistical significance if p< 0.05). RESULTS: 102 patients were included with high serum lipase was present in 39.2% of patients, mean lipase of 797U/L. Patients with high serum lipase had longer hospital stay (p< 0.001), parenteral nutrition (p< 0.001), ventilator support (p=0.04), fever (p< 0.001), hyperamylasemia (p<0.05), hyperbilirrubinemia (p=0.003) and rise of transaminases (p=0.001), with no significant differences in diagnosis, gender, age, APACHE II, SOFA, SAPS, mortality, hypotension, alkaline phosphatase, hemoglobin, lactate, tolerance to enteral nutrition and use of propofol. Imaging study revealed pancreatic alterations in two patients with high serum lipase. CONCLUSIONS: Elevated lipase was commonly found in critical patients, it related with longer length of stay but was not accompanied by increased clinical severity or mortality. It was more frequent with parenteral nutrition. A minority of patients met the criteria of acute pancreatitis.
Views0Abstract
Original ArticlesIncreased lipase and amilase levels in critically ill patients: retrospective study
Rev Bras Ter Intensiva. 2008;20(4):362-369
DOI 10.1590/S0103-507X2008000400008
Views0See moreOBJECTIVES: Elevated lipase and amylase are commonly found in patients in intensive care unit without a previously recognized pancreatic illness, constituting a diagnostic and therapeutic challenge. The authors therefore proposed to determine the frequency of asymptomatic high serum lipase in critically ill patients, involved risk factors and outcome. METHODS: Retrospective study of patients admitted in an intensive care unit from January 1 to December 31, 2006, excluding admissions for acute pancreatitis, history of pancreatic disease, renal insufficiency or lacking of data. Patients were divided in two groups (with and without high serum lipase) that were compared for clinical, laboratory and radiological variables. Statistical analysis: SPSS 13; Student’s t test and Chi-square test (CI 95%) with statistical significance if p< 0.05). RESULTS: 102 patients were included with high serum lipase was present in 39.2% of patients, mean lipase of 797U/L. Patients with high serum lipase had longer hospital stay (p< 0.001), parenteral nutrition (p< 0.001), ventilator support (p=0.04), fever (p< 0.001), hyperamylasemia (p<0.05), hyperbilirrubinemia (p=0.003) and rise of transaminases (p=0.001), with no significant differences in diagnosis, gender, age, APACHE II, SOFA, SAPS, mortality, hypotension, alkaline phosphatase, hemoglobin, lactate, tolerance to enteral nutrition and use of propofol. Imaging study revealed pancreatic alterations in two patients with high serum lipase. CONCLUSIONS: Elevated lipase was commonly found in critical patients, it related with longer length of stay but was not accompanied by increased clinical severity or mortality. It was more frequent with parenteral nutrition. A minority of patients met the criteria of acute pancreatitis.
-
Original Articles
The experience of family members of patients staying in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):370-375
Abstract
Original ArticlesThe experience of family members of patients staying in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):370-375
DOI 10.1590/S0103-507X2008000400009
Views0OBJECTIVE: The aim of this study was to understand the experience of family members, during a patient’s stay in the intensive care unit of public and private hospitals using an approximation to the phenomenology referential. METHODS: We interviewed 27 relatives of adult patients, 10 from a public institution and 17 from a private one. RESULTS: From analyses of interviews in a public institution, four thematic categories emerged. In a private institution six categories were identified. Searching for differences and similarities, four similar thematic categories were perceived in both institutions and two categories were absent in the public hospital. CONCLUSION: There are no significant differences between categories in private and public hospitals. This indicates that family behavior and reactions to patient’s admission to the ICU are not associated with social or financial aspects. However, a greater knowledge of government policies and programs is necessary, because they favor humanization by allowing family members to accompany the patient in tertiary services.
Keywords:Family relationsIn-patientsIntensive care unitsProfessional-family relationsQualitative researchSee moreViews0Abstract
Original ArticlesThe experience of family members of patients staying in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):370-375
DOI 10.1590/S0103-507X2008000400009
Views0OBJECTIVE: The aim of this study was to understand the experience of family members, during a patient’s stay in the intensive care unit of public and private hospitals using an approximation to the phenomenology referential. METHODS: We interviewed 27 relatives of adult patients, 10 from a public institution and 17 from a private one. RESULTS: From analyses of interviews in a public institution, four thematic categories emerged. In a private institution six categories were identified. Searching for differences and similarities, four similar thematic categories were perceived in both institutions and two categories were absent in the public hospital. CONCLUSION: There are no significant differences between categories in private and public hospitals. This indicates that family behavior and reactions to patient’s admission to the ICU are not associated with social or financial aspects. However, a greater knowledge of government policies and programs is necessary, because they favor humanization by allowing family members to accompany the patient in tertiary services.
Keywords:Family relationsIn-patientsIntensive care unitsProfessional-family relationsQualitative researchSee more -
Original Articles
Epidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
Abstract
Original ArticlesEpidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
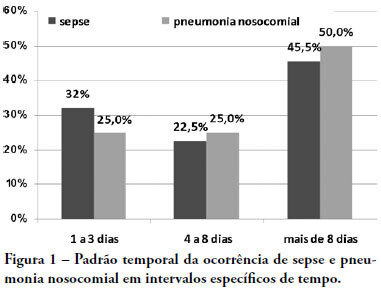
Views0See moreOBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Views0Abstract
Original ArticlesEpidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
Views0See moreOBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
-
Original Articles
Renal function of intensive care unit patients: plasma creatinine and urinary retinol-binding protein
Rev Bras Ter Intensiva. 2008;20(4):385-393
Abstract
Original ArticlesRenal function of intensive care unit patients: plasma creatinine and urinary retinol-binding protein
Rev Bras Ter Intensiva. 2008;20(4):385-393
DOI 10.1590/S0103-507X2008000400011
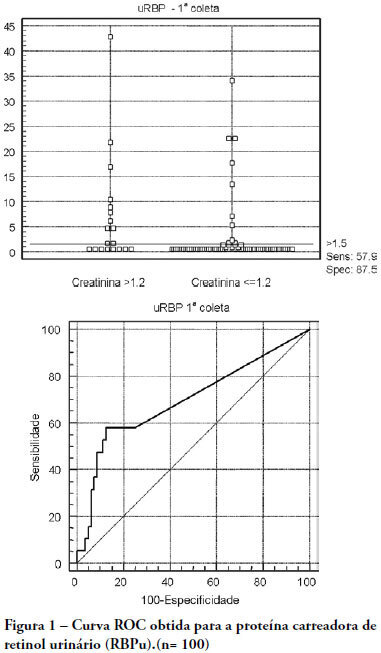
Views0See moreOBJECTIVES: The early assessment of renal dysfunction using common markers does not provide either a sensitive or specific indication of renal dysfunction in critically ill patients. More specific and sensitive markers are desirable for the early detection of an initial renal pathophysiological process. Urinary retinol-binding protein could be an alternative method to early evaluation of renal function in these patients. METHODS: This study followed-up 100 critical care patients and assessed their clinical and laboratory variables, including plasma creatinine and urinary retinol-binding ratio, and demographic variables. RESULTS: The sample was characterized by geriatric (63.4±15.6 years), male (68%), being 53% surgical patients. Statistical analysis showed association between plasma creatinine and the following variables: gender (p-0.026), age (p-0.038), use of vasoactive drugs (p-0.003), proteinuria (p-0.025), Acute Physiological Chronic Health Evaluation (APACHE) II score (p-0.000), urea (p-0.000), potassium (p-0.003) and estimated creatinine clearance (p-0.000). Urinary retinol-binding protein was correlated with more variables: weight, use of invasive ventilation (p-0.000), use of nonsteroidal antiinflammatory drugs (p-0.018), use of vasoactive drugs (p-0.021), high temperature (>37.5ºC) (p-0.005), proteinuria (p-0.000), bilirubinuria (p-0.004), urinary flow (p-0.019), minimal diastolic pressure (p-0.032), minimal systolic pressure (p-0.029), APACHE II (p-0.000), creatinine (p-0.001), urea (p-0.001), estimated creatinine clearance (p-0.000). Urinary retinol-binding protein also tended to associate with previous renal disease, vasculopathy and neoplasm. Sodium excretion fraction correlated with plasma creatinine and urinary retinol-binding protein in univariate analysis. CONCLUSIONS: Urinary retinol-binding protein might be considered in clinical practice as a better marker regarding diagnostic performance in patients at risk of developing acute kidney injury, when compared with other markers routinely used. Moreover, urinary retinol-binding protein has other features of a good diagnostic test – it is a practical and non-invasive method.
Views0Abstract
Original ArticlesRenal function of intensive care unit patients: plasma creatinine and urinary retinol-binding protein
Rev Bras Ter Intensiva. 2008;20(4):385-393
DOI 10.1590/S0103-507X2008000400011
Views0See moreOBJECTIVES: The early assessment of renal dysfunction using common markers does not provide either a sensitive or specific indication of renal dysfunction in critically ill patients. More specific and sensitive markers are desirable for the early detection of an initial renal pathophysiological process. Urinary retinol-binding protein could be an alternative method to early evaluation of renal function in these patients. METHODS: This study followed-up 100 critical care patients and assessed their clinical and laboratory variables, including plasma creatinine and urinary retinol-binding ratio, and demographic variables. RESULTS: The sample was characterized by geriatric (63.4±15.6 years), male (68%), being 53% surgical patients. Statistical analysis showed association between plasma creatinine and the following variables: gender (p-0.026), age (p-0.038), use of vasoactive drugs (p-0.003), proteinuria (p-0.025), Acute Physiological Chronic Health Evaluation (APACHE) II score (p-0.000), urea (p-0.000), potassium (p-0.003) and estimated creatinine clearance (p-0.000). Urinary retinol-binding protein was correlated with more variables: weight, use of invasive ventilation (p-0.000), use of nonsteroidal antiinflammatory drugs (p-0.018), use of vasoactive drugs (p-0.021), high temperature (>37.5ºC) (p-0.005), proteinuria (p-0.000), bilirubinuria (p-0.004), urinary flow (p-0.019), minimal diastolic pressure (p-0.032), minimal systolic pressure (p-0.029), APACHE II (p-0.000), creatinine (p-0.001), urea (p-0.001), estimated creatinine clearance (p-0.000). Urinary retinol-binding protein also tended to associate with previous renal disease, vasculopathy and neoplasm. Sodium excretion fraction correlated with plasma creatinine and urinary retinol-binding protein in univariate analysis. CONCLUSIONS: Urinary retinol-binding protein might be considered in clinical practice as a better marker regarding diagnostic performance in patients at risk of developing acute kidney injury, when compared with other markers routinely used. Moreover, urinary retinol-binding protein has other features of a good diagnostic test – it is a practical and non-invasive method.
-
Original Articles
Cesarean deliveries and other risks for persistent pulmonary hypertension of the newborn
Rev Bras Ter Intensiva. 2008;20(4):394-397
Abstract
Original ArticlesCesarean deliveries and other risks for persistent pulmonary hypertension of the newborn
Rev Bras Ter Intensiva. 2008;20(4):394-397
DOI 10.1590/S0103-507X2008000400012
Views0See moreOBJECTIVES: To evaluate risks for persistent pulmonary hypertension in the newborn, confirmed by echocardiography, associated with cesarean deliveries and other factors. METHODS: Cohort of all deliveries >36 weeks within a period of 23 months. A nested case-control study was performed in a subset of the cohort, involving newborns admitted into neonatal intensive care unit with diagnosis of persistent pulmonary hypertension matched with normal controls, with application of questionnaires to mothers to identify risks. Logistic regression was used to calculate odds ratios. RESULTS: From 9452 newborns, 8388 (88.7%) were delivered by cesarean and 1064 (11.3%) by vaginal delivery. Questionnaires were applied to 173 mothers. Infants from cesareans had a fivefold increased risk of persistent pulmonary hypertension of the newborn: 42 (0.5%) versus 1 case (0.09%) in the vaginal group (OR 5.32, p=0.027). No interactions were found between smoking, parity, arterial hypertension and labor before cesarean section and persistent pulmonary hypertension of the newborn. First minute Apgar score <7 and maternal diabetes were related to increased risk. CONCLUSION: Reducing cesarean deliveries could prevent many cases of serious persistent pulmonary hypertension of the newborn.
Views0Abstract
Original ArticlesCesarean deliveries and other risks for persistent pulmonary hypertension of the newborn
Rev Bras Ter Intensiva. 2008;20(4):394-397
DOI 10.1590/S0103-507X2008000400012
Views0See moreOBJECTIVES: To evaluate risks for persistent pulmonary hypertension in the newborn, confirmed by echocardiography, associated with cesarean deliveries and other factors. METHODS: Cohort of all deliveries >36 weeks within a period of 23 months. A nested case-control study was performed in a subset of the cohort, involving newborns admitted into neonatal intensive care unit with diagnosis of persistent pulmonary hypertension matched with normal controls, with application of questionnaires to mothers to identify risks. Logistic regression was used to calculate odds ratios. RESULTS: From 9452 newborns, 8388 (88.7%) were delivered by cesarean and 1064 (11.3%) by vaginal delivery. Questionnaires were applied to 173 mothers. Infants from cesareans had a fivefold increased risk of persistent pulmonary hypertension of the newborn: 42 (0.5%) versus 1 case (0.09%) in the vaginal group (OR 5.32, p=0.027). No interactions were found between smoking, parity, arterial hypertension and labor before cesarean section and persistent pulmonary hypertension of the newborn. First minute Apgar score <7 and maternal diabetes were related to increased risk. CONCLUSION: Reducing cesarean deliveries could prevent many cases of serious persistent pulmonary hypertension of the newborn.
-
Original Articles
Central and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
Abstract
Original ArticlesCentral and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
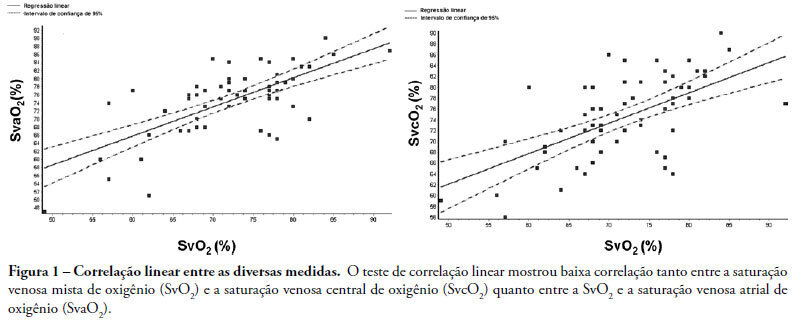
Views0See moreINTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Views0Abstract
Original ArticlesCentral and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
Views0See moreINTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
-
Review Articles
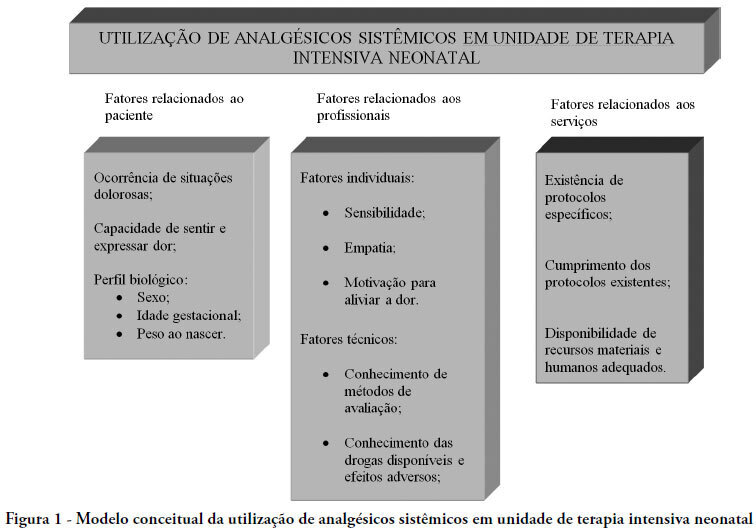
Factors related to use of systemic analgesia in neonatology
Rev Bras Ter Intensiva. 2008;20(4):405-410
Abstract
Review ArticlesFactors related to use of systemic analgesia in neonatology
Rev Bras Ter Intensiva. 2008;20(4):405-410
DOI 10.1590/S0103-507X2008000400014
Views0See moreThe purpose of this paper was to carry out a review of literature on the history and current stage of the knowledge of systemic analgesia in neonatology and the factors influencing its use. A search for scientific articles was made in the MEDLINE, SciELO and LILACS databases using the keywords: analgesia, systemic analgesics, pain, neonatology, newborn, intensive care units and neonatal intensive care units. Additional research was made on dissertations and thesis databanks as well as text books. Literature consulted disclosed that, in general, analgesia is not a routine practice in neonatal intensive care units, despite the numerous studies demonstrating its importance. Although pain relief is a basic principle of medicine, involving ethic and humanitarian issues and despite the current availability of a number of practical guidelines and consensus regarding pain management in newborns at risk, findings of the present study fall far short of current recommendations. Urgent intervention is required to redress this situation.
Views0Abstract
Review ArticlesFactors related to use of systemic analgesia in neonatology
Rev Bras Ter Intensiva. 2008;20(4):405-410
DOI 10.1590/S0103-507X2008000400014
Views0See moreThe purpose of this paper was to carry out a review of literature on the history and current stage of the knowledge of systemic analgesia in neonatology and the factors influencing its use. A search for scientific articles was made in the MEDLINE, SciELO and LILACS databases using the keywords: analgesia, systemic analgesics, pain, neonatology, newborn, intensive care units and neonatal intensive care units. Additional research was made on dissertations and thesis databanks as well as text books. Literature consulted disclosed that, in general, analgesia is not a routine practice in neonatal intensive care units, despite the numerous studies demonstrating its importance. Although pain relief is a basic principle of medicine, involving ethic and humanitarian issues and despite the current availability of a number of practical guidelines and consensus regarding pain management in newborns at risk, findings of the present study fall far short of current recommendations. Urgent intervention is required to redress this situation.
-
Review Articles
Outcome biomarkers following severe traumatic brain injury
Rev Bras Ter Intensiva. 2008;20(4):411-421
Abstract
Review ArticlesOutcome biomarkers following severe traumatic brain injury
Rev Bras Ter Intensiva. 2008;20(4):411-421
DOI 10.1590/S0103-507X2008000400015
Views0See moreTrauma is the leading cause of death of people from 1 to 44 years of age. Traumatic brain injury is the main determinant for mortality and morbidity caused by trauma. Outcome prediction is one of the major problems related to severe traumatic brain injury because clinical evaluation has an unreliable predictive value and complicates identification of patients with higher risk of developing secondary lesions and fatal outcome. That is why, there is considerable interest in development of biomarkers that reflect the severity of brain injury and correlate with mortality and functional outcome. Proteins S100B and neuron specific enolases are among the markers most studied for this purpose, however some studies are investigating glial fibrillary acidic protein, creatinine phospokinase, isoenzime B, myelin basic protein, plasma desoxiribonucleic acid, heat shock protein 70, von Willebrand factor, metalloproteinases and brain-derived neurotrophic factor, among others. Evidence suggests that inflammation, oxidative stress, excitotoxicity, neuroendocrine responses and apoptosis play an important role in the development of secondary lesions. Markers involved in these processes are being studied in traumatic brain injury. We reviewed these biomarkers, some of which present promising results for future clinical application.
Views0Abstract
Review ArticlesOutcome biomarkers following severe traumatic brain injury
Rev Bras Ter Intensiva. 2008;20(4):411-421
DOI 10.1590/S0103-507X2008000400015
Views0See moreTrauma is the leading cause of death of people from 1 to 44 years of age. Traumatic brain injury is the main determinant for mortality and morbidity caused by trauma. Outcome prediction is one of the major problems related to severe traumatic brain injury because clinical evaluation has an unreliable predictive value and complicates identification of patients with higher risk of developing secondary lesions and fatal outcome. That is why, there is considerable interest in development of biomarkers that reflect the severity of brain injury and correlate with mortality and functional outcome. Proteins S100B and neuron specific enolases are among the markers most studied for this purpose, however some studies are investigating glial fibrillary acidic protein, creatinine phospokinase, isoenzime B, myelin basic protein, plasma desoxiribonucleic acid, heat shock protein 70, von Willebrand factor, metalloproteinases and brain-derived neurotrophic factor, among others. Evidence suggests that inflammation, oxidative stress, excitotoxicity, neuroendocrine responses and apoptosis play an important role in the development of secondary lesions. Markers involved in these processes are being studied in traumatic brain injury. We reviewed these biomarkers, some of which present promising results for future clinical application.
-
Review Articles
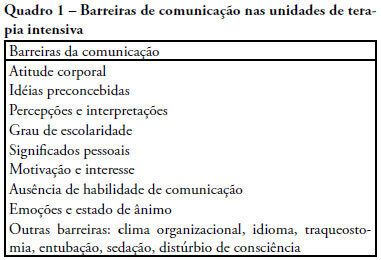
End of life and palliative care in intensive care unit
Rev Bras Ter Intensiva. 2008;20(4):422-428
Abstract
Review ArticlesEnd of life and palliative care in intensive care unit
Rev Bras Ter Intensiva. 2008;20(4):422-428
DOI 10.1590/S0103-507X2008000400016
Views0See moreThe objective of this review was to evaluate current knowledge regarding terminal illness and palliative care in the intensive care unit, to identify the major challenges involved and propose a research agenda on these issues The Brazilian Critical Care Association organized a specific forum on terminally ill patients, to which were invited experienced and skilled professionals on critical care. These professionals were divided in three groups: communication in the intensive care unit, the decision making process when faced with a terminally ill patient and palliative actions and care in the intensive care unit. Data and bibliographic references were stored in a restricted website. During a twelve hour meeting and following a modified Delphi methodology, the groups prepared the final document. Consensual definition regarding terminality was reached. Good communication was considered the cornerstone to define the best treatment for a terminally ill patient. Accordingly some communication barriers were described that should be avoided as well as some approaches that should be pursued. Criteria for palliative care and palliative action in the intensive care unit were defined. Acceptance of death as a natural event as well as respect for the patient’s autonomy and the nonmaleficence principles were stressed. A recommendation was made to withdraw the futile treatment that prolongs the dying process and to elected analgesia and measures that alleviate suffering in terminally ill patients. To deliver palliative care to terminally ill patients and their relatives some principles and guides should be followed, respecting individual necessities and beliefs. The intensive care unit staff involved with the treatment of terminally ill patients is subject to stress and tension. Availability of a continuous education program on palliative care is desirable.
Views0Abstract
Review ArticlesEnd of life and palliative care in intensive care unit
Rev Bras Ter Intensiva. 2008;20(4):422-428
DOI 10.1590/S0103-507X2008000400016
Views0See moreThe objective of this review was to evaluate current knowledge regarding terminal illness and palliative care in the intensive care unit, to identify the major challenges involved and propose a research agenda on these issues The Brazilian Critical Care Association organized a specific forum on terminally ill patients, to which were invited experienced and skilled professionals on critical care. These professionals were divided in three groups: communication in the intensive care unit, the decision making process when faced with a terminally ill patient and palliative actions and care in the intensive care unit. Data and bibliographic references were stored in a restricted website. During a twelve hour meeting and following a modified Delphi methodology, the groups prepared the final document. Consensual definition regarding terminality was reached. Good communication was considered the cornerstone to define the best treatment for a terminally ill patient. Accordingly some communication barriers were described that should be avoided as well as some approaches that should be pursued. Criteria for palliative care and palliative action in the intensive care unit were defined. Acceptance of death as a natural event as well as respect for the patient’s autonomy and the nonmaleficence principles were stressed. A recommendation was made to withdraw the futile treatment that prolongs the dying process and to elected analgesia and measures that alleviate suffering in terminally ill patients. To deliver palliative care to terminally ill patients and their relatives some principles and guides should be followed, respecting individual necessities and beliefs. The intensive care unit staff involved with the treatment of terminally ill patients is subject to stress and tension. Availability of a continuous education program on palliative care is desirable.
-
Case Reports
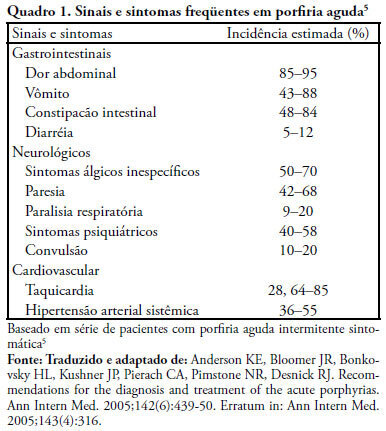
Acute intermittent porphyria: case report and review of the literature
Rev Bras Ter Intensiva. 2008;20(4):429-434
Abstract
Case ReportsAcute intermittent porphyria: case report and review of the literature
Rev Bras Ter Intensiva. 2008;20(4):429-434
DOI 10.1590/S0103-507X2008000400017
Views0See moreAcute intermittent porphyria is an unusual pathology with potentially severe consequences when not early detected. Among the possible causes of porphyric crises decrease of caloric intake has been described. A case of acute intermittent porphyria in the late postoperative period of a bariatric surgery performed for treatment of obesity is reported. A review of the diagnostic aspects and management of this pathology in the intensive care unit follows. A 31 year old woman was admitted in the intensive care unit three weeks after a bariatric surgery, with decreased level of consciousness and respiratory distress. The patient evolved with psychomotor agitation, mental confusion, abdominal pain and proximal tetraparesis. Diagnosis investigation disclosed severe hyponatremia (92mEq/L), hypomagnesemia, hypophosfatemia and hypocalcemia and cloudy urine without hematuria. Acute porphyria was suspected and the urine test detected high delta amino-levulinic acid and porphobilinogen. Treatment consisted of a correction of electrolyte disturbances and high carbohydrate intake. Hematin and heme arginate were not used, due to the difficulty to acquire the medication. After 8 months the patient progressed with full recovery of muscle strength and a clinical improvement. Acute intermittent porphyria has signs and symptoms common to several clinical, neurological, psychiatric and gastroenterological pathologies, which complicate diagnosis. Therefore, acute intermittent porphyria should be included in the differential diagnosis of neurological, psychiatric and gastroenterological alterations when results of all other exams are normal. Attention must be given to patients undergoing surgery mainly bariatric that, in addition to procedure stress, substantially limit the total caloric intake, potentially triggering crises. Review of literature did not disclose any report of acute intermittent porphyria crisis induced by bariatric surgery.
Views0Abstract
Case ReportsAcute intermittent porphyria: case report and review of the literature
Rev Bras Ter Intensiva. 2008;20(4):429-434
DOI 10.1590/S0103-507X2008000400017
Views0See moreAcute intermittent porphyria is an unusual pathology with potentially severe consequences when not early detected. Among the possible causes of porphyric crises decrease of caloric intake has been described. A case of acute intermittent porphyria in the late postoperative period of a bariatric surgery performed for treatment of obesity is reported. A review of the diagnostic aspects and management of this pathology in the intensive care unit follows. A 31 year old woman was admitted in the intensive care unit three weeks after a bariatric surgery, with decreased level of consciousness and respiratory distress. The patient evolved with psychomotor agitation, mental confusion, abdominal pain and proximal tetraparesis. Diagnosis investigation disclosed severe hyponatremia (92mEq/L), hypomagnesemia, hypophosfatemia and hypocalcemia and cloudy urine without hematuria. Acute porphyria was suspected and the urine test detected high delta amino-levulinic acid and porphobilinogen. Treatment consisted of a correction of electrolyte disturbances and high carbohydrate intake. Hematin and heme arginate were not used, due to the difficulty to acquire the medication. After 8 months the patient progressed with full recovery of muscle strength and a clinical improvement. Acute intermittent porphyria has signs and symptoms common to several clinical, neurological, psychiatric and gastroenterological pathologies, which complicate diagnosis. Therefore, acute intermittent porphyria should be included in the differential diagnosis of neurological, psychiatric and gastroenterological alterations when results of all other exams are normal. Attention must be given to patients undergoing surgery mainly bariatric that, in addition to procedure stress, substantially limit the total caloric intake, potentially triggering crises. Review of literature did not disclose any report of acute intermittent porphyria crisis induced by bariatric surgery.
Volume Articles - Critical Care Science (CCS)
