-
Editorial
RBTI is ambitious!
Rev Bras Ter Intensiva. 2008;20(3):vii-vii
-
Original Articles
Comparative analysis of respiratory systems compliance in three different positioning (lateral, dorsal and sitting) in patients in prolonged invasive mechanical ventilation
Rev Bras Ter Intensiva. 2008;20(3):213-219
Abstract
Original ArticlesComparative analysis of respiratory systems compliance in three different positioning (lateral, dorsal and sitting) in patients in prolonged invasive mechanical ventilation
Rev Bras Ter Intensiva. 2008;20(3):213-219
DOI 10.1590/S0103-507X2008000300002
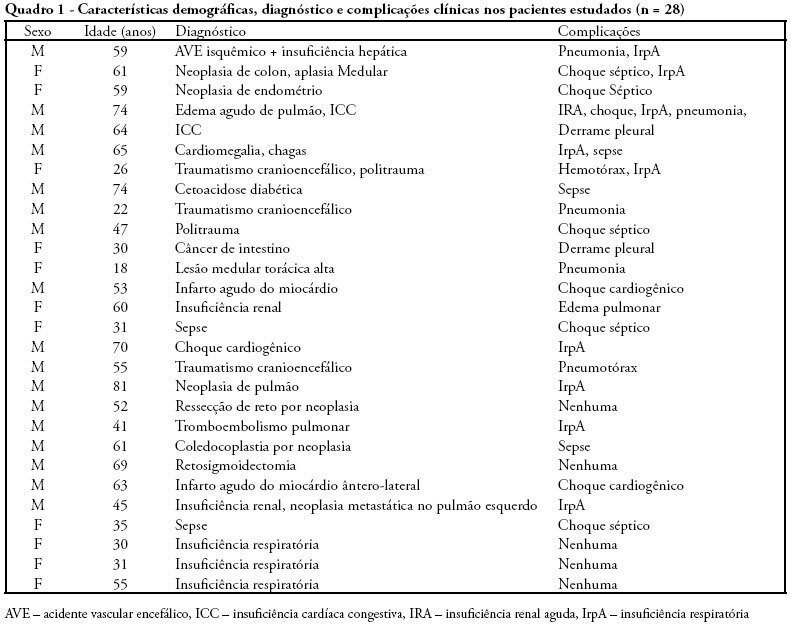
Views0See moreOBJECTIVES: This study is justified by the fact that in clinical practice, changes occur in patient’s positioning in the bed during hospitalization in intensive care unity, it’s necessary better understanding about possible adverse effects that such changes might cause mainly on the respiratory system condition. The objective this study was to evaluate if the patients positioning in bed can to alter the pulmonary complacency. METHODS: All included patients were submitted to mechanical ventilation and were sedated and curarized respiratory system compliance was assessed in three different positioning: lateral, dorsal and sitting. After an alveolar recruitment maneuver, patients were placed to a position throughout two hours, and in the last five minutes the data was collected from the mechanical ventilator display. RESULTS: twenty eight patients were prospectively assessed. Values of respiratory system compliance in the lateral position were 37,07 ± 12,9 in the dorsal were 39,2 ± 10,5 and in the sitting 43,4 ± 9,6 mL/cmH2O. There were a statistical difference when we compared to the sitting and dorsal with lateral positioning for respiratory system compliance (p = 0.0052) and tidal volume (p < 0.001). There was a negative correlation between mean values of positive end expiratory pressure a respiratory system compliance (r = 0.59, p = 0.002). The FIO2 administered was 0.6 for the lateral positioning and 0.5 for the dorsal and sitting positioning (p = 0.049). CONCLUSIONS: That body positioning in patients restrained to a bed and submitted to invasive mechanical ventilation leads to pulmonary compliance, tidal volume and SpO2 oscillations. In the sitting position the pulmonary compliance is higher than in others positions.
Views0

Abstract
Original ArticlesComparative analysis of respiratory systems compliance in three different positioning (lateral, dorsal and sitting) in patients in prolonged invasive mechanical ventilation
Rev Bras Ter Intensiva. 2008;20(3):213-219
DOI 10.1590/S0103-507X2008000300002
Views0See moreOBJECTIVES: This study is justified by the fact that in clinical practice, changes occur in patient’s positioning in the bed during hospitalization in intensive care unity, it’s necessary better understanding about possible adverse effects that such changes might cause mainly on the respiratory system condition. The objective this study was to evaluate if the patients positioning in bed can to alter the pulmonary complacency. METHODS: All included patients were submitted to mechanical ventilation and were sedated and curarized respiratory system compliance was assessed in three different positioning: lateral, dorsal and sitting. After an alveolar recruitment maneuver, patients were placed to a position throughout two hours, and in the last five minutes the data was collected from the mechanical ventilator display. RESULTS: twenty eight patients were prospectively assessed. Values of respiratory system compliance in the lateral position were 37,07 ± 12,9 in the dorsal were 39,2 ± 10,5 and in the sitting 43,4 ± 9,6 mL/cmH2O. There were a statistical difference when we compared to the sitting and dorsal with lateral positioning for respiratory system compliance (p = 0.0052) and tidal volume (p < 0.001). There was a negative correlation between mean values of positive end expiratory pressure a respiratory system compliance (r = 0.59, p = 0.002). The FIO2 administered was 0.6 for the lateral positioning and 0.5 for the dorsal and sitting positioning (p = 0.049). CONCLUSIONS: That body positioning in patients restrained to a bed and submitted to invasive mechanical ventilation leads to pulmonary compliance, tidal volume and SpO2 oscillations. In the sitting position the pulmonary compliance is higher than in others positions.
-
Original Articles
Cuff pressure analysis of intensive care unit patients with different inclinations of the head section of the bed
Rev Bras Ter Intensiva. 2008;20(3):220-225
Abstract
Original ArticlesCuff pressure analysis of intensive care unit patients with different inclinations of the head section of the bed
Rev Bras Ter Intensiva. 2008;20(3):220-225
DOI 10.1590/S0103-507X2008000300003
Views0See moreOBJECTIVES: Correct cuff inflation allows appropriate ventilation, and prevents aspiration pneumonia as well as several tracheal complications. The objective of this study was to evaluate endotracheal cuff pressure and/or tracheotomy tubes at zero, 30 and 60 degrees inclination of the patient’s bed head section in adult intensive care units. METHODS: A cross sectional study was carried out evaluating the cuff pressure, the expiratory tidal volume (VT) and the peak airway pressure (PP) at inclinations zero, 30 and 60 degree of the head section of the patients’ bed. The 30 degree inclination was considered the standard position used as control to analyze values in the zero and 60 degree positions, which were randomly ordered. The Student’s t test was used and was considered significant when p < 0.05. RESULTS: A sample of 12 women and 12 men with a mean age of 51.29 ± 19.55 years was surveyed. When inclination of the bed head section was changed from 30 to zero degrees, there was a 16.9% mean reduction of the cuff pressure and 11.8% mean increase of the PP. On the other hand, changing the position from 30 to 60 degrees caused a mean reduction of 18.8% in the cuff pressure and a mean increase of 13.3% in the PP. Findings were significant when p < 0.05. CONCLUSIONS: To prevent air leak and risk of aspiration pneumonia, adequate adjustments and monitoring of the patients cuff pressure are necessary when inclination of the bed head section is changed.
Views0Abstract
Original ArticlesCuff pressure analysis of intensive care unit patients with different inclinations of the head section of the bed
Rev Bras Ter Intensiva. 2008;20(3):220-225
DOI 10.1590/S0103-507X2008000300003
Views0See moreOBJECTIVES: Correct cuff inflation allows appropriate ventilation, and prevents aspiration pneumonia as well as several tracheal complications. The objective of this study was to evaluate endotracheal cuff pressure and/or tracheotomy tubes at zero, 30 and 60 degrees inclination of the patient’s bed head section in adult intensive care units. METHODS: A cross sectional study was carried out evaluating the cuff pressure, the expiratory tidal volume (VT) and the peak airway pressure (PP) at inclinations zero, 30 and 60 degree of the head section of the patients’ bed. The 30 degree inclination was considered the standard position used as control to analyze values in the zero and 60 degree positions, which were randomly ordered. The Student’s t test was used and was considered significant when p < 0.05. RESULTS: A sample of 12 women and 12 men with a mean age of 51.29 ± 19.55 years was surveyed. When inclination of the bed head section was changed from 30 to zero degrees, there was a 16.9% mean reduction of the cuff pressure and 11.8% mean increase of the PP. On the other hand, changing the position from 30 to 60 degrees caused a mean reduction of 18.8% in the cuff pressure and a mean increase of 13.3% in the PP. Findings were significant when p < 0.05. CONCLUSIONS: To prevent air leak and risk of aspiration pneumonia, adequate adjustments and monitoring of the patients cuff pressure are necessary when inclination of the bed head section is changed.
-
Original Articles
Postoperative cardiac artery bypass graft complications in elderly patients
Rev Bras Ter Intensiva. 2008;20(3):226-234
Abstract
Original ArticlesPostoperative cardiac artery bypass graft complications in elderly patients
Rev Bras Ter Intensiva. 2008;20(3):226-234
DOI 10.1590/S0103-507X2008000300004
Views0PURPOSE: Due to the increasing longevity of the and high prevalence of coronary heart disease in the aged , coronary artery bypass graft surgery has become frequent in older patients. The purpose of this study is to describe operative features, length of stay, complications and short term outcomes after coronary artery bypass graft in such patients. METHODS: From February 2005 to October 2007, 269 patients underwent coronary artery bypass graft. Demographic data, comorbidities, prognostic scores, coronary artery bypass graft elective versus urgent indication, intensive care unit length of stay, postoperative complications and intensive care unit mortality were recorded. Intra-operative characteristics, such as total surgery time, use of bypass device, on-pump time, urine output, fluid balance, use of blood products and number of grafts, were analyzed. Patients were divided in four age groups: group I (< 60 n = 68), II (60 to 69 n = 86), III (70 to 79 n = 93) IV and older than 80 years (n = 22). RESULTS: Group IV patients were more frequently submitted to coronary artery bypass graft combined with valve replacement, emergency surgery, and had longer stay in the intensive care unit (p < 0.01). The incidence of at least one postoperative complication was also higher among patients older than 80 (p < 0.001). Multivariate analysis identified age and on-pump time as independent risk factors for development of complications. Mortality increased in patients older than 70 years (p = 0.03). CONCLUSIONS: Octogenarian patients undergoing coronary artery bypass graft have longer intensive care unit length of stay, incidence of complications and mortality. Age and on-pump time were independent risk factors associated with the incidence of postoperative complications.
Keywords:AgedCoronary artery bypassCoronary artery diseaseGraft occlusion, vascularPostoperative complicationsPrognosisSee moreViews0Abstract
Original ArticlesPostoperative cardiac artery bypass graft complications in elderly patients
Rev Bras Ter Intensiva. 2008;20(3):226-234
DOI 10.1590/S0103-507X2008000300004
Views0PURPOSE: Due to the increasing longevity of the and high prevalence of coronary heart disease in the aged , coronary artery bypass graft surgery has become frequent in older patients. The purpose of this study is to describe operative features, length of stay, complications and short term outcomes after coronary artery bypass graft in such patients. METHODS: From February 2005 to October 2007, 269 patients underwent coronary artery bypass graft. Demographic data, comorbidities, prognostic scores, coronary artery bypass graft elective versus urgent indication, intensive care unit length of stay, postoperative complications and intensive care unit mortality were recorded. Intra-operative characteristics, such as total surgery time, use of bypass device, on-pump time, urine output, fluid balance, use of blood products and number of grafts, were analyzed. Patients were divided in four age groups: group I (< 60 n = 68), II (60 to 69 n = 86), III (70 to 79 n = 93) IV and older than 80 years (n = 22). RESULTS: Group IV patients were more frequently submitted to coronary artery bypass graft combined with valve replacement, emergency surgery, and had longer stay in the intensive care unit (p < 0.01). The incidence of at least one postoperative complication was also higher among patients older than 80 (p < 0.001). Multivariate analysis identified age and on-pump time as independent risk factors for development of complications. Mortality increased in patients older than 70 years (p = 0.03). CONCLUSIONS: Octogenarian patients undergoing coronary artery bypass graft have longer intensive care unit length of stay, incidence of complications and mortality. Age and on-pump time were independent risk factors associated with the incidence of postoperative complications.
Keywords:AgedCoronary artery bypassCoronary artery diseaseGraft occlusion, vascularPostoperative complicationsPrognosisSee more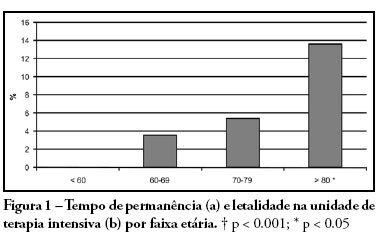
-
Original Articles
Intensive care unit physicians: socio-demographic profile, working conditions and factors associated with burnout syndrome
Rev Bras Ter Intensiva. 2008;20(3):235-240
Abstract
Original ArticlesIntensive care unit physicians: socio-demographic profile, working conditions and factors associated with burnout syndrome
Rev Bras Ter Intensiva. 2008;20(3):235-240
DOI 10.1590/S0103-507X2008000300005
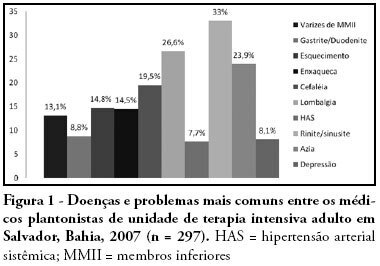
Views0See moreOBJECTIVES: Burnout syndrome is a response to prolonged occupational stress that involves three main dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. The aim of this study was to describe socio-demographic characteristics of intensive care unit physicians and evaluate factors associated to the presence of Burnout syndrome in this population. METHODS: A cross-sectional study was performed to evaluate physicians who have worked in intensive care units from the city of Salvador (Bahia – Brazil) with a minimum weekly workload of 12-hour. An anonymous self-reported questionnaire was used and it was divided into two parts: socio-demographic characteristics and evaluation of Burnout syndrome through Maslach Burnout Inventory. RESULTS: We studied 297 physicians and most of them were male (70%). The mean age and time of graduation were, respectively, 34.2 and 9 years. High levels of emotional exhaustion, depersonalization, and reduced personal accomplishment were found in respectively, 47.5%, 24.6% and 28.3%. The prevalence of Burnout syndrome, considered as high level in at least one dimension, was of 63.3%. This prevalence was statistically lower in physicians specialized on intensive care, those with more than nine years of graduation and those who intend to continue working in intensive care units for more than 10 years. The prevalence was higher in the doctors with more than 24-hours of uninterrupted intensive care work per week. CONCLUSIONS: Burnout syndrome was common among intensive care physicians and it was more frequent in the youngest doctors, with higher workload and without specialization on intensive care.
Views0Abstract
Original ArticlesIntensive care unit physicians: socio-demographic profile, working conditions and factors associated with burnout syndrome
Rev Bras Ter Intensiva. 2008;20(3):235-240
DOI 10.1590/S0103-507X2008000300005
Views0See moreOBJECTIVES: Burnout syndrome is a response to prolonged occupational stress that involves three main dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. The aim of this study was to describe socio-demographic characteristics of intensive care unit physicians and evaluate factors associated to the presence of Burnout syndrome in this population. METHODS: A cross-sectional study was performed to evaluate physicians who have worked in intensive care units from the city of Salvador (Bahia – Brazil) with a minimum weekly workload of 12-hour. An anonymous self-reported questionnaire was used and it was divided into two parts: socio-demographic characteristics and evaluation of Burnout syndrome through Maslach Burnout Inventory. RESULTS: We studied 297 physicians and most of them were male (70%). The mean age and time of graduation were, respectively, 34.2 and 9 years. High levels of emotional exhaustion, depersonalization, and reduced personal accomplishment were found in respectively, 47.5%, 24.6% and 28.3%. The prevalence of Burnout syndrome, considered as high level in at least one dimension, was of 63.3%. This prevalence was statistically lower in physicians specialized on intensive care, those with more than nine years of graduation and those who intend to continue working in intensive care units for more than 10 years. The prevalence was higher in the doctors with more than 24-hours of uninterrupted intensive care work per week. CONCLUSIONS: Burnout syndrome was common among intensive care physicians and it was more frequent in the youngest doctors, with higher workload and without specialization on intensive care.
-
Original Articles
Enteral nutritional therapy with pre, pro and symbiotic and gastrointestinal tract and inferior airway colonization in mechanically ventilated patients
Rev Bras Ter Intensiva. 2008;20(3):241-248
Abstract
Original ArticlesEnteral nutritional therapy with pre, pro and symbiotic and gastrointestinal tract and inferior airway colonization in mechanically ventilated patients
Rev Bras Ter Intensiva. 2008;20(3):241-248
DOI 10.1590/S0103-507X2008000300006
Views2OBJECTIVES: Sepsis is the main cause of death in the intensive care unit. New preventive measures for nosocomial infections have been researched, such as pre, pro and symbiotic usage, due to its immunoregulatory properties. The objective was to evaluate the effect of administration of pre, pro and symbiotic on gastrointestinal and inferior airway colonization and on nosocomial infections, particularly ventilator-associated pneumonia. METHODS: Patients who were admitted to the intensive care unit at Hospital Universitário Clementino Fraga Filho between November 2004 and September 2006 and mechanically ventilated were randomized in one of four groups: control (n = 16), prebiotic (n = 10), probiotic (n = 12) or symbiotic (n = 11). Treatment was administered for fourteen days. Outcomes measured were: a) Colonization of the gastrointestinal tract and trachea; b) incidence of nosocomial infections, particularly ventilator associated pneumonia; c) duration of mechanical ventilation, length of stay in the intensive care unit, duration of hospitalization, mortality rates, and d) development of organ dysfunction. RESULTS: Forty-nine patients were evaluated. intensive care unit’s mortality was 34% and in-hospital mortality was 53%, APACHE II median was 20 (13 -25). The groups were matched at admission. There was no difference between the groups in relation to the incidence of ventilator associated pneumonia or nosocomial infection. There was a non-significant increase in the proportion of enterobacteria in the trachea at the seventh day in the pre and probiotic groups compared to control. There was a non-significant decrease in the number of bacteria found in the stomach in the pre, pro and symbiotic group at day 7. No significant difference, in regards to the remaining measured parameters, could be found. CONCLUSIONS: Probiotic therapy was not efficient in the prevention of nosocomial infection but there was a tendency to reduction in tracheal colonization by non-fermenting bacteria.
Keywords:enteral nutritionGastrointestinal tractnutritional therapyPneumonia, ventilator-associatedProbioticsSee moreViews2Abstract
Original ArticlesEnteral nutritional therapy with pre, pro and symbiotic and gastrointestinal tract and inferior airway colonization in mechanically ventilated patients
Rev Bras Ter Intensiva. 2008;20(3):241-248
DOI 10.1590/S0103-507X2008000300006
Views2OBJECTIVES: Sepsis is the main cause of death in the intensive care unit. New preventive measures for nosocomial infections have been researched, such as pre, pro and symbiotic usage, due to its immunoregulatory properties. The objective was to evaluate the effect of administration of pre, pro and symbiotic on gastrointestinal and inferior airway colonization and on nosocomial infections, particularly ventilator-associated pneumonia. METHODS: Patients who were admitted to the intensive care unit at Hospital Universitário Clementino Fraga Filho between November 2004 and September 2006 and mechanically ventilated were randomized in one of four groups: control (n = 16), prebiotic (n = 10), probiotic (n = 12) or symbiotic (n = 11). Treatment was administered for fourteen days. Outcomes measured were: a) Colonization of the gastrointestinal tract and trachea; b) incidence of nosocomial infections, particularly ventilator associated pneumonia; c) duration of mechanical ventilation, length of stay in the intensive care unit, duration of hospitalization, mortality rates, and d) development of organ dysfunction. RESULTS: Forty-nine patients were evaluated. intensive care unit’s mortality was 34% and in-hospital mortality was 53%, APACHE II median was 20 (13 -25). The groups were matched at admission. There was no difference between the groups in relation to the incidence of ventilator associated pneumonia or nosocomial infection. There was a non-significant increase in the proportion of enterobacteria in the trachea at the seventh day in the pre and probiotic groups compared to control. There was a non-significant decrease in the number of bacteria found in the stomach in the pre, pro and symbiotic group at day 7. No significant difference, in regards to the remaining measured parameters, could be found. CONCLUSIONS: Probiotic therapy was not efficient in the prevention of nosocomial infection but there was a tendency to reduction in tracheal colonization by non-fermenting bacteria.
Keywords:enteral nutritionGastrointestinal tractnutritional therapyPneumonia, ventilator-associatedProbioticsSee more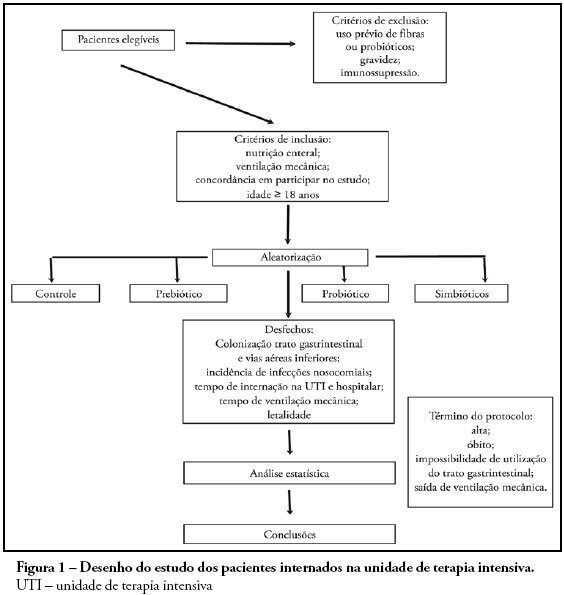
-
Original Articles
Characteristics of patients with systemic lupus erythematosus admitted to the intensive care unit in a brazilian teaching hospital
Rev Bras Ter Intensiva. 2008;20(3):249-253
Abstract
Original ArticlesCharacteristics of patients with systemic lupus erythematosus admitted to the intensive care unit in a brazilian teaching hospital
Rev Bras Ter Intensiva. 2008;20(3):249-253
DOI 10.1590/S0103-507X2008000300007
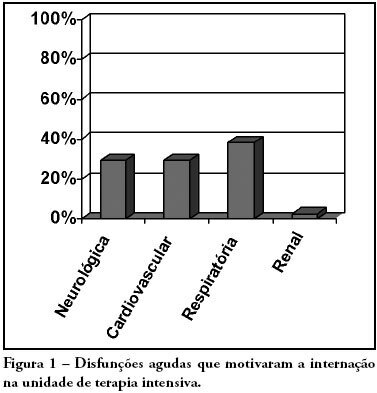
Views0See moreOBJECTIVES: Due to the high incidence in our service, we did object on this study describe the features and outcome of patients with systemic lupus erythematosus (SLE) admitted to the intensive care unit of Walter Cantídio University Hospital METHODS: Patients were restrospectively characterized according to demography parameters, time of diagnosis of SLE, organ dysfunction and laboratorial parameters at admission, supportive therapies during their stay, length of stay in the hospital before admission, length of stay in the unit, readmission to the unit and outcome. We also evaluated Systemic Lupus Erythematosus Disease Activity (SLEDAI) score, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, expected mortality and standardized mortality ratio. RESULTS: From November 2003 to October 2006, 1,052 patients were admitted to the intensive care unit. Fifty patients had SLE and were included in this retrospective study. Of the 50 patients with SLE admitted to the ICU, 88.2% were female. The mean age was 30.3 ± 12.8 years. The median time of diagnosis of SLE was 67 months. The most common organ dysfunctions were renal (70.6%), cardiovascular (61.8%), respiratory (55.9%) and neurological (55.9%). The main reasons for admission to the ICU were respiratory (38.2%), cardiologic (29.4%) and neurological (29.4%) dysfunctions. Among the intensive care therapies, 44.1% of the patients needed blood products, 41.2% vasopressor agents and 35.3% mechanical ventilation, 23.5% dialysis. The mean SLEDAI score was 15.0 ± 12.2. The mean APACHE II score was 19.3 ± 6.8, with a predicted mortality rate of 37.6%. The actual mortality rate in ICU was 29.4%, with 8.8% before 48 hours. The standardized mortality ratio was 0.78. Patients with APACHE II > 18, with more than 3 acute organ involvements, leukopenia (< 4000 cells/mm3) and gastrointestinal or metabolic involvement had higher mortality in the intensive care unit. CONCLUSION: Although the severity of patients at admission to the ICU, demonstrated by APACHE II and the acute dysfunctions, the outcomes of analysed patients sugest susceptibility to the therapy.
Views0Abstract
Original ArticlesCharacteristics of patients with systemic lupus erythematosus admitted to the intensive care unit in a brazilian teaching hospital
Rev Bras Ter Intensiva. 2008;20(3):249-253
DOI 10.1590/S0103-507X2008000300007
Views0See moreOBJECTIVES: Due to the high incidence in our service, we did object on this study describe the features and outcome of patients with systemic lupus erythematosus (SLE) admitted to the intensive care unit of Walter Cantídio University Hospital METHODS: Patients were restrospectively characterized according to demography parameters, time of diagnosis of SLE, organ dysfunction and laboratorial parameters at admission, supportive therapies during their stay, length of stay in the hospital before admission, length of stay in the unit, readmission to the unit and outcome. We also evaluated Systemic Lupus Erythematosus Disease Activity (SLEDAI) score, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, expected mortality and standardized mortality ratio. RESULTS: From November 2003 to October 2006, 1,052 patients were admitted to the intensive care unit. Fifty patients had SLE and were included in this retrospective study. Of the 50 patients with SLE admitted to the ICU, 88.2% were female. The mean age was 30.3 ± 12.8 years. The median time of diagnosis of SLE was 67 months. The most common organ dysfunctions were renal (70.6%), cardiovascular (61.8%), respiratory (55.9%) and neurological (55.9%). The main reasons for admission to the ICU were respiratory (38.2%), cardiologic (29.4%) and neurological (29.4%) dysfunctions. Among the intensive care therapies, 44.1% of the patients needed blood products, 41.2% vasopressor agents and 35.3% mechanical ventilation, 23.5% dialysis. The mean SLEDAI score was 15.0 ± 12.2. The mean APACHE II score was 19.3 ± 6.8, with a predicted mortality rate of 37.6%. The actual mortality rate in ICU was 29.4%, with 8.8% before 48 hours. The standardized mortality ratio was 0.78. Patients with APACHE II > 18, with more than 3 acute organ involvements, leukopenia (< 4000 cells/mm3) and gastrointestinal or metabolic involvement had higher mortality in the intensive care unit. CONCLUSION: Although the severity of patients at admission to the ICU, demonstrated by APACHE II and the acute dysfunctions, the outcomes of analysed patients sugest susceptibility to the therapy.
-
Original Articles
Effects of different tidal volumes and positive end expiratory pressure on gas exchange in experimental bronchopleural fistula
Rev Bras Ter Intensiva. 2008;20(3):254-260
Abstract
Original ArticlesEffects of different tidal volumes and positive end expiratory pressure on gas exchange in experimental bronchopleural fistula
Rev Bras Ter Intensiva. 2008;20(3):254-260
DOI 10.1590/S0103-507X2008000300008
Views0OBJECTIVES: The present study was designed to identify the effect of positive end expiratory pressure (PEEP) and the ideal pulmonary tidal volume to ventilate animals with a surgically produced bronchopleural fistula, aiming to reduce fistula output without affecting gas exchange. METHODS: Hemodynamic and respiratory assessment of gas exchange was obtained in five, healthy, young, mechanically ventilated Large White pigs under volume controlled ventilation with FiO2 of 0.4 and an inspiration:expiration ratio of 1:2, keeping respiratory rate at 22 cpm. A bronchopleural fistula was produced by resection of the lingula. Underwater seal drainage was installed and the thorax was hermetically closed. Gas exchange and fistula output were measured with the animals ventilated sequentially with tidal volumes of 4 ml/kg, 7 ml/kg and 10 ml/Kg alternating zero of positive end expiratory pressure (ZEEP) and PEEP of 10 cmH2O, always in the same order. RESULTS: These findings are attributed to reduced alveolar ventilation and ventilation/perfusion abnormalities and were attenuated with larger tidal volumes. PEEP increases air leak, even with low volume (of 2.0 ± 2.8mL to 31 ± 20.7mL; p= 0.006) and decreases alveolar ventilation in all tidal volumes. Alveolar ventilation improved with larger tidal volumes, but increased fistula output (10 mL/kg – 25.8 ± 18.3mL to 80.2 ± 43.9mL; p=0.0010). Low tidal volumes result in hypercapnia (ZEEP – Toneloto MGC, Terzi RGG, Silva WA, Moraes AC, Moreira MM 83.7± 6.9 mmHg and with PEEP 10 – 93 ± 10.1mmHg) and severely decreased arterial oxygen saturation, about of 84%. CONCLUSIONS: The tidal volume of 7 ml/Kg with ZEEP was considered the best tidal volume because, despite moderate hypercapnia, arterial oxygen saturation is sustained around 90%, alveolar ventilation improves and the fistula output is reduced when compared with a tidal volume of 10ml/Kg. A low tidal volume results in hypercapnia and severe desaturation. Finally, at any tidal volume, PEEP increases the fistula leak and decreases alveolar ventilation.
Keywords:Bronchial fistulaHypercapniaPositive pressure respirationRespiration, artificialRespiratory tract fistulaSwineTidal VolumeSee moreViews0Abstract
Original ArticlesEffects of different tidal volumes and positive end expiratory pressure on gas exchange in experimental bronchopleural fistula
Rev Bras Ter Intensiva. 2008;20(3):254-260
DOI 10.1590/S0103-507X2008000300008
Views0OBJECTIVES: The present study was designed to identify the effect of positive end expiratory pressure (PEEP) and the ideal pulmonary tidal volume to ventilate animals with a surgically produced bronchopleural fistula, aiming to reduce fistula output without affecting gas exchange. METHODS: Hemodynamic and respiratory assessment of gas exchange was obtained in five, healthy, young, mechanically ventilated Large White pigs under volume controlled ventilation with FiO2 of 0.4 and an inspiration:expiration ratio of 1:2, keeping respiratory rate at 22 cpm. A bronchopleural fistula was produced by resection of the lingula. Underwater seal drainage was installed and the thorax was hermetically closed. Gas exchange and fistula output were measured with the animals ventilated sequentially with tidal volumes of 4 ml/kg, 7 ml/kg and 10 ml/Kg alternating zero of positive end expiratory pressure (ZEEP) and PEEP of 10 cmH2O, always in the same order. RESULTS: These findings are attributed to reduced alveolar ventilation and ventilation/perfusion abnormalities and were attenuated with larger tidal volumes. PEEP increases air leak, even with low volume (of 2.0 ± 2.8mL to 31 ± 20.7mL; p= 0.006) and decreases alveolar ventilation in all tidal volumes. Alveolar ventilation improved with larger tidal volumes, but increased fistula output (10 mL/kg – 25.8 ± 18.3mL to 80.2 ± 43.9mL; p=0.0010). Low tidal volumes result in hypercapnia (ZEEP – Toneloto MGC, Terzi RGG, Silva WA, Moraes AC, Moreira MM 83.7± 6.9 mmHg and with PEEP 10 – 93 ± 10.1mmHg) and severely decreased arterial oxygen saturation, about of 84%. CONCLUSIONS: The tidal volume of 7 ml/Kg with ZEEP was considered the best tidal volume because, despite moderate hypercapnia, arterial oxygen saturation is sustained around 90%, alveolar ventilation improves and the fistula output is reduced when compared with a tidal volume of 10ml/Kg. A low tidal volume results in hypercapnia and severe desaturation. Finally, at any tidal volume, PEEP increases the fistula leak and decreases alveolar ventilation.
Keywords:Bronchial fistulaHypercapniaPositive pressure respirationRespiration, artificialRespiratory tract fistulaSwineTidal VolumeSee more
-
Original Articles
Factors that cause stress in physicians and nurses working in a pediatric and neonatal intensive care unit: bibliographic review
Rev Bras Ter Intensiva. 2008;20(3):261-266
Abstract
Original ArticlesFactors that cause stress in physicians and nurses working in a pediatric and neonatal intensive care unit: bibliographic review
Rev Bras Ter Intensiva. 2008;20(3):261-266
DOI 10.1590/S0103-507X2008000300009
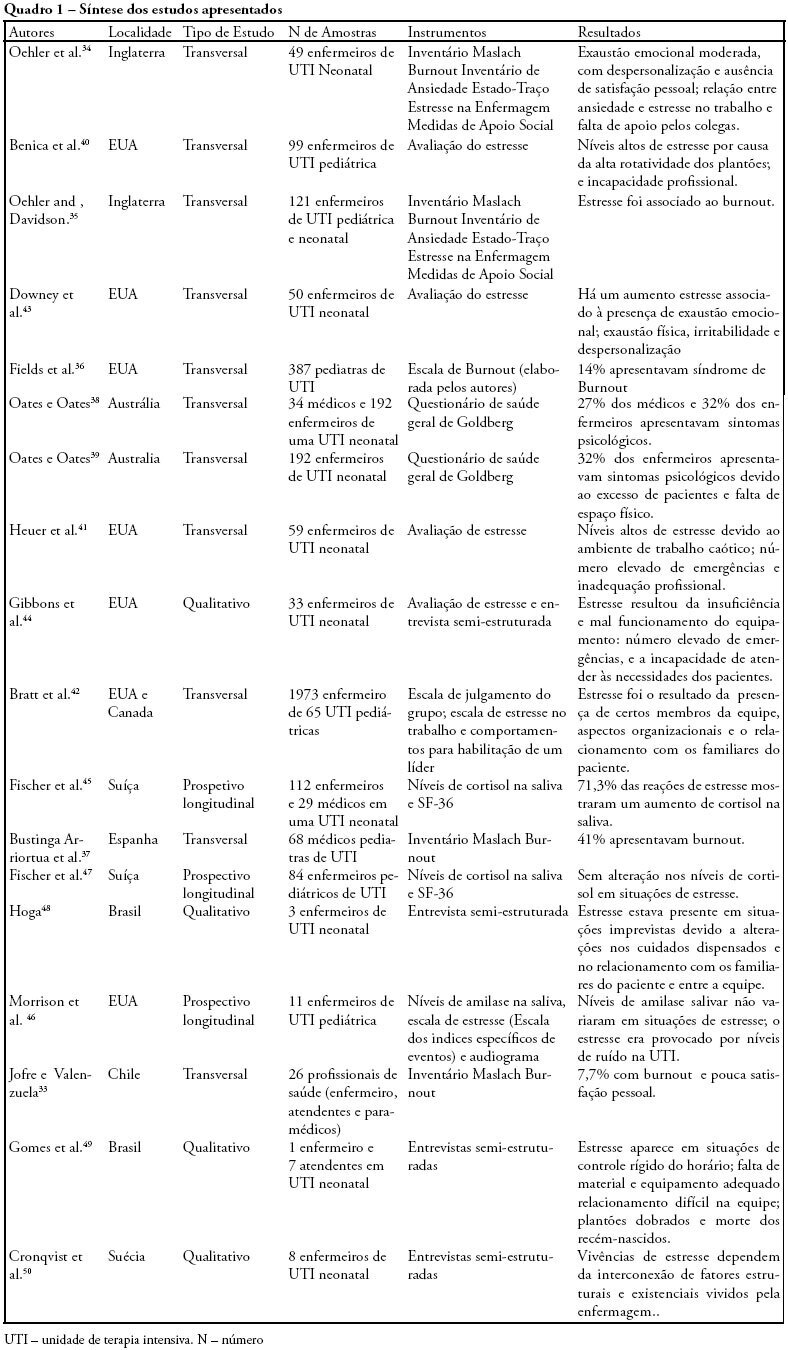
Views0See moreOBJECTIVES: Bibliographic review on occupational stress and burnout presence in physicians and nurses that work in pediatric and neonatal intensive care units. METHODS: The articles were selected from the MedLine, LILACS and SciElo data base using the key words: stress, burnout, physicians, nursing, intensive care unit, pediatric intensive care unit and neonatal intensive care unit. The studied period ranged from 1990 to 2007. RESULTS: Health professionals who work in pediatric and neonatal intensive care units are strong candidates for developing stress, psychological alterations and burnout syndrome. Researches on this subject identified important alterations suffered by these physicians and nurses, such as: work overload, burnout, desires of giving up their jobs, high levels of cortisol, among other alterations. CONCLUSIONS: Professionals, who work in pediatric and neonatal intensive care units, due to the specificity of their job, are liable to develop occupational stress, and consequently burnout. These results suggest the need for further research with the objective of developing preventive measures and intervention models.
Views0Abstract
Original ArticlesFactors that cause stress in physicians and nurses working in a pediatric and neonatal intensive care unit: bibliographic review
Rev Bras Ter Intensiva. 2008;20(3):261-266
DOI 10.1590/S0103-507X2008000300009
Views0See moreOBJECTIVES: Bibliographic review on occupational stress and burnout presence in physicians and nurses that work in pediatric and neonatal intensive care units. METHODS: The articles were selected from the MedLine, LILACS and SciElo data base using the key words: stress, burnout, physicians, nursing, intensive care unit, pediatric intensive care unit and neonatal intensive care unit. The studied period ranged from 1990 to 2007. RESULTS: Health professionals who work in pediatric and neonatal intensive care units are strong candidates for developing stress, psychological alterations and burnout syndrome. Researches on this subject identified important alterations suffered by these physicians and nurses, such as: work overload, burnout, desires of giving up their jobs, high levels of cortisol, among other alterations. CONCLUSIONS: Professionals, who work in pediatric and neonatal intensive care units, due to the specificity of their job, are liable to develop occupational stress, and consequently burnout. These results suggest the need for further research with the objective of developing preventive measures and intervention models.
-
Original Articles
Sepsis volume reposition with hypertonic saline solution
Rev Bras Ter Intensiva. 2008;20(3):267-277
Abstract
Original ArticlesSepsis volume reposition with hypertonic saline solution
Rev Bras Ter Intensiva. 2008;20(3):267-277
DOI 10.1590/S0103-507X2008000300010
Views0See moreThe present review discusses the hemodynamic and immune-modulatory effects of hypertonic saline in experimental shock and in patients with sepsis. We comment on the mechanisms of action of hypertonic saline, calling upon data in hemorrhagic and septic shock. Specific actions of hypertonic saline applicable to severe sepsis and septic shock are highlighted. Data available support potential benefits of hypertonic saline infusion in various aspects of the pathophysiology of sepsis, including tissue hypoperfusion, decreased oxygen consumption, endothelial dysfunction, cardiac depression, and the presence of a broad array of pro-inflammatory cytokines and various oxidant species. A therapy that simultaneously blocks the damaging components of sepsis will have an impact on the management of sepsis. Proper designed prospective studies may prove a beneficial role for hypertonic saline solution in the future.
Views0Abstract
Original ArticlesSepsis volume reposition with hypertonic saline solution
Rev Bras Ter Intensiva. 2008;20(3):267-277
DOI 10.1590/S0103-507X2008000300010
Views0See moreThe present review discusses the hemodynamic and immune-modulatory effects of hypertonic saline in experimental shock and in patients with sepsis. We comment on the mechanisms of action of hypertonic saline, calling upon data in hemorrhagic and septic shock. Specific actions of hypertonic saline applicable to severe sepsis and septic shock are highlighted. Data available support potential benefits of hypertonic saline infusion in various aspects of the pathophysiology of sepsis, including tissue hypoperfusion, decreased oxygen consumption, endothelial dysfunction, cardiac depression, and the presence of a broad array of pro-inflammatory cytokines and various oxidant species. A therapy that simultaneously blocks the damaging components of sepsis will have an impact on the management of sepsis. Proper designed prospective studies may prove a beneficial role for hypertonic saline solution in the future.
-
Review Articles
Acute tumor lysis syndrome: a comprehensive review
Rev Bras Ter Intensiva. 2008;20(3):278-285
Abstract
Review ArticlesAcute tumor lysis syndrome: a comprehensive review
Rev Bras Ter Intensiva. 2008;20(3):278-285
DOI 10.1590/S0103-507X2008000300011
Views1Tumor lysis syndrome is characterized by the massive destruction of malignant cells and the release in the extra-cellular space of their content. While Tumor lysis syndrome may occur spontaneously before treatment, it usually develops shortly after the initiation of cytotoxic chemotherapy. These metabolites can overwhelm the homeostatic mechanisms with development of hyperuricaemia, hyperkalaemia, hyperphosphataemia, and hypocalcaemia. These biological manifestations may lead to clinical manifestations including, acute kidney injury, seizure, or sudden death that require intensive care. Since clinical tumor lysis syndrome is associated with a poor prognosis both prevention of tumor lysis syndrome and prevention of clinical consequences of tumor lysis syndrome are mandatory. The objective of this review is to describe pathophysiological mechanisms, biological and clinical manifestations of tumor Lysis syndrome, and to provide upto-date guidelines to ensure prevention of tumor lysis syndrome. Review of selected studies on tumor lysis syndrome published at the PubMed database www.pubmed.gov during the last 20 years. Additional references were retrieved from the studies initially selected. Tumor lysis syndrome is a frequent and life-threatening complication of the newly diagnosed malignancies. Preventive measures, including hydration, uricolytic agents, eviction of factors predisposing to acute kidney injury and, in the more severe patients, on prophylactic renal replacement therapy, are required to prevent or limit clinical consequences of Tumor lysis syndrome. However optimal timing and modalities of prevention remains unknown and may be modified by the changing spectrum of patients at risk of tumor lysis syndrome. Development and validation of risk based strategies is required to limit the high morbidity and mortality of this complication.
Keywords:Antineoplastic agentsHypercalcemiaHyperuricemiaIntensive care unitsKidney diseasesleukemiaLymphoma, non-HodgkinRenal insufficiency, acuteTumor Lysis syndromeUric acidSee moreViews1Abstract
Review ArticlesAcute tumor lysis syndrome: a comprehensive review
Rev Bras Ter Intensiva. 2008;20(3):278-285
DOI 10.1590/S0103-507X2008000300011
Views1Tumor lysis syndrome is characterized by the massive destruction of malignant cells and the release in the extra-cellular space of their content. While Tumor lysis syndrome may occur spontaneously before treatment, it usually develops shortly after the initiation of cytotoxic chemotherapy. These metabolites can overwhelm the homeostatic mechanisms with development of hyperuricaemia, hyperkalaemia, hyperphosphataemia, and hypocalcaemia. These biological manifestations may lead to clinical manifestations including, acute kidney injury, seizure, or sudden death that require intensive care. Since clinical tumor lysis syndrome is associated with a poor prognosis both prevention of tumor lysis syndrome and prevention of clinical consequences of tumor lysis syndrome are mandatory. The objective of this review is to describe pathophysiological mechanisms, biological and clinical manifestations of tumor Lysis syndrome, and to provide upto-date guidelines to ensure prevention of tumor lysis syndrome. Review of selected studies on tumor lysis syndrome published at the PubMed database www.pubmed.gov during the last 20 years. Additional references were retrieved from the studies initially selected. Tumor lysis syndrome is a frequent and life-threatening complication of the newly diagnosed malignancies. Preventive measures, including hydration, uricolytic agents, eviction of factors predisposing to acute kidney injury and, in the more severe patients, on prophylactic renal replacement therapy, are required to prevent or limit clinical consequences of Tumor lysis syndrome. However optimal timing and modalities of prevention remains unknown and may be modified by the changing spectrum of patients at risk of tumor lysis syndrome. Development and validation of risk based strategies is required to limit the high morbidity and mortality of this complication.
Keywords:Antineoplastic agentsHypercalcemiaHyperuricemiaIntensive care unitsKidney diseasesleukemiaLymphoma, non-HodgkinRenal insufficiency, acuteTumor Lysis syndromeUric acidSee more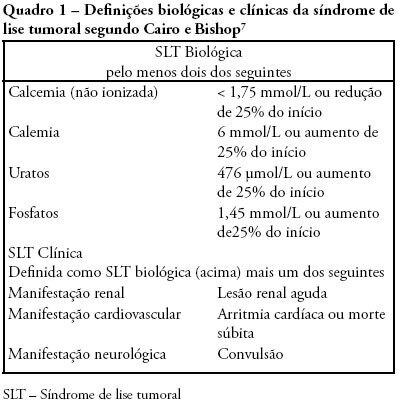
-
Review Articles
Nutritional assessment of the severely ill patient
Rev Bras Ter Intensiva. 2008;20(3):286-295
Abstract
Review ArticlesNutritional assessment of the severely ill patient
Rev Bras Ter Intensiva. 2008;20(3):286-295
DOI 10.1590/S0103-507X2008000300012
Views0Considering the importance and the difficulties inherent to nutritional state assessment, as well as the results interpretation and the inexistence of specific and validated guidelines related to applied methods to the severely ill patient, the present revision aims to contribute to the analysis and recommendation of efficient methods, which are suitable to use and reliable in terms of interpretation in the context of the severely ill patient. The presence of edema and unspecific alterations in the plasmatic concentrations of proteins; altered anthropometrics variables reflecting more the rearrangement of the total body water than the nutritional state changes; inconclusive studies with electric bioimpedance; absence of data related to the application of the global subjective assessment to severely ill patients; altered biochemical markers as a consequence of the metabolic changes that, among others, indicate several method limitations to these patients. Notwithstanding the lack of studies to validate the various methods, recommendations based on clinical evidences, observation and physiopathology alterations are available. Independent from the methods, clinical observation by the health staff at all stages is mandatory. It is crucial to dedicate more efforts to identify methods and their specificity to detection, risk assessment or monitoring.
Keywords:Critical careIntensive carenutrition assessmentNutritional statusNutritional supportPatient careSee moreViews0Abstract
Review ArticlesNutritional assessment of the severely ill patient
Rev Bras Ter Intensiva. 2008;20(3):286-295
DOI 10.1590/S0103-507X2008000300012
Views0Considering the importance and the difficulties inherent to nutritional state assessment, as well as the results interpretation and the inexistence of specific and validated guidelines related to applied methods to the severely ill patient, the present revision aims to contribute to the analysis and recommendation of efficient methods, which are suitable to use and reliable in terms of interpretation in the context of the severely ill patient. The presence of edema and unspecific alterations in the plasmatic concentrations of proteins; altered anthropometrics variables reflecting more the rearrangement of the total body water than the nutritional state changes; inconclusive studies with electric bioimpedance; absence of data related to the application of the global subjective assessment to severely ill patients; altered biochemical markers as a consequence of the metabolic changes that, among others, indicate several method limitations to these patients. Notwithstanding the lack of studies to validate the various methods, recommendations based on clinical evidences, observation and physiopathology alterations are available. Independent from the methods, clinical observation by the health staff at all stages is mandatory. It is crucial to dedicate more efforts to identify methods and their specificity to detection, risk assessment or monitoring.
Keywords:Critical careIntensive carenutrition assessmentNutritional statusNutritional supportPatient careSee more -
Review Articles
How to conduct clinical research studies using high quality-clinical databases in the critical care
Rev Bras Ter Intensiva. 2008;20(3):296-304
Abstract
Review ArticlesHow to conduct clinical research studies using high quality-clinical databases in the critical care
Rev Bras Ter Intensiva. 2008;20(3):296-304
DOI 10.1590/S0103-507X2008000300013
Views0The sources of intensive care-related information and the means of communication increase rapidly. We presented here an overview of what should be done to collect high quality database. In a second part, the principle of the choice of the research question, the outcome, the explanatory variables and the statistical methods to address the question are overviewed, emphasizing major and frequent pitfalls which should be avoided.
Keywords:Biomedical researchData collectionDatabase, factualEvaluation studiesInformation systemsQuality controlSee moreViews0Abstract
Review ArticlesHow to conduct clinical research studies using high quality-clinical databases in the critical care
Rev Bras Ter Intensiva. 2008;20(3):296-304
DOI 10.1590/S0103-507X2008000300013
Views0The sources of intensive care-related information and the means of communication increase rapidly. We presented here an overview of what should be done to collect high quality database. In a second part, the principle of the choice of the research question, the outcome, the explanatory variables and the statistical methods to address the question are overviewed, emphasizing major and frequent pitfalls which should be avoided.
Keywords:Biomedical researchData collectionDatabase, factualEvaluation studiesInformation systemsQuality controlSee more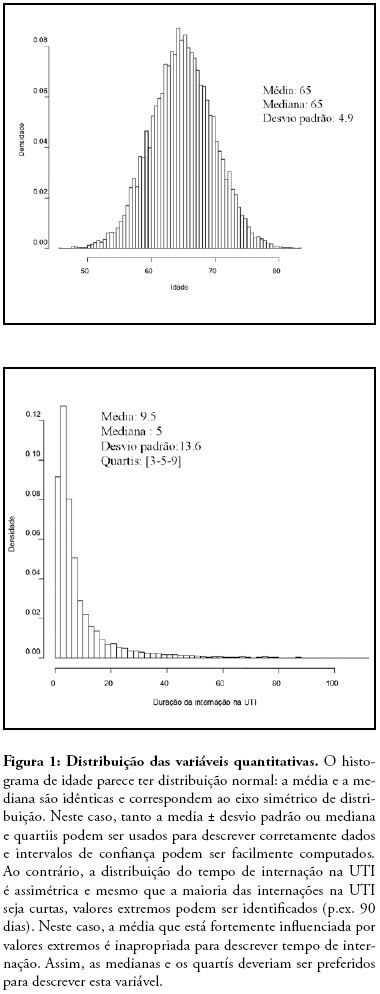
-
Review Articles
Hypertensive emergencies
Rev Bras Ter Intensiva. 2008;20(3):305-312
Abstract
Review ArticlesHypertensive emergencies
Rev Bras Ter Intensiva. 2008;20(3):305-312
DOI 10.1590/S0103-507X2008000300014
Views0Emergencies and hypertensive crises are clinical situations which may represent more than 25% of all medical emergency care. Considering such high prevalence, physicians should be prepared to correctly identify these crises and differentiate between urgent and emergent hypertension. Approximately 3% of all visits to emergency rooms are due to significant elevation of blood pressure. Across the spectrum of blood systemic arterial pressure, hypertensive emergency is the most critical clinical situation, thus requiring special attention and care. Such patients present with high blood pressure and signs of acute specific target organ damage (such as acute myocardial infarction, unstable angina, acute pulmonary edema, eclampsia, and stroke). Key elements of diagnosis and specific treatment for the different presentations of hypertensive emergency will be reviewed in this article. The MedLine and PubMed databases were searched for pertinent abstracts, using the key words “hypertensive crises” and “hypertensive emergencies”. Additional references were obtained from review articles. Available English language clinical trials, retrospective studies and review articles were identified, reviewed and summarized in a simple and practical way. The hypertensive crisis is a clinical situation characterized by acute elevation of blood pressure followed by clinical signs and symptoms. These signs and symptoms may be mild (headache, dizziness, tinnitus) or severe (dyspnea, chest pain, coma or death). If the patient presents with mild symptoms, but without acute specific target organ damage, diagnosis is hypertensive urgency. However, if severe signs and symptoms and acute specific target organ damage are present, then the patient is experiencing a hypertensive emergency. Some patients arrive at the emergency rooms with high blood pressure, but without any other sign or symptom. In these cases, they usually are not taking their medications correctly. Therefore, this is not a hypertensive crisis, but rather non-controlled chronic hypertension. This type of distinction is important for those working in emergency rooms and intensive care unit. Correct diagnosis must be made to assure the most appropriate treatment.
Keywords:EmergenciesHipertensionSee moreViews0Abstract
Review ArticlesHypertensive emergencies
Rev Bras Ter Intensiva. 2008;20(3):305-312
DOI 10.1590/S0103-507X2008000300014
Views0Emergencies and hypertensive crises are clinical situations which may represent more than 25% of all medical emergency care. Considering such high prevalence, physicians should be prepared to correctly identify these crises and differentiate between urgent and emergent hypertension. Approximately 3% of all visits to emergency rooms are due to significant elevation of blood pressure. Across the spectrum of blood systemic arterial pressure, hypertensive emergency is the most critical clinical situation, thus requiring special attention and care. Such patients present with high blood pressure and signs of acute specific target organ damage (such as acute myocardial infarction, unstable angina, acute pulmonary edema, eclampsia, and stroke). Key elements of diagnosis and specific treatment for the different presentations of hypertensive emergency will be reviewed in this article. The MedLine and PubMed databases were searched for pertinent abstracts, using the key words “hypertensive crises” and “hypertensive emergencies”. Additional references were obtained from review articles. Available English language clinical trials, retrospective studies and review articles were identified, reviewed and summarized in a simple and practical way. The hypertensive crisis is a clinical situation characterized by acute elevation of blood pressure followed by clinical signs and symptoms. These signs and symptoms may be mild (headache, dizziness, tinnitus) or severe (dyspnea, chest pain, coma or death). If the patient presents with mild symptoms, but without acute specific target organ damage, diagnosis is hypertensive urgency. However, if severe signs and symptoms and acute specific target organ damage are present, then the patient is experiencing a hypertensive emergency. Some patients arrive at the emergency rooms with high blood pressure, but without any other sign or symptom. In these cases, they usually are not taking their medications correctly. Therefore, this is not a hypertensive crisis, but rather non-controlled chronic hypertension. This type of distinction is important for those working in emergency rooms and intensive care unit. Correct diagnosis must be made to assure the most appropriate treatment.
Keywords:EmergenciesHipertensionSee more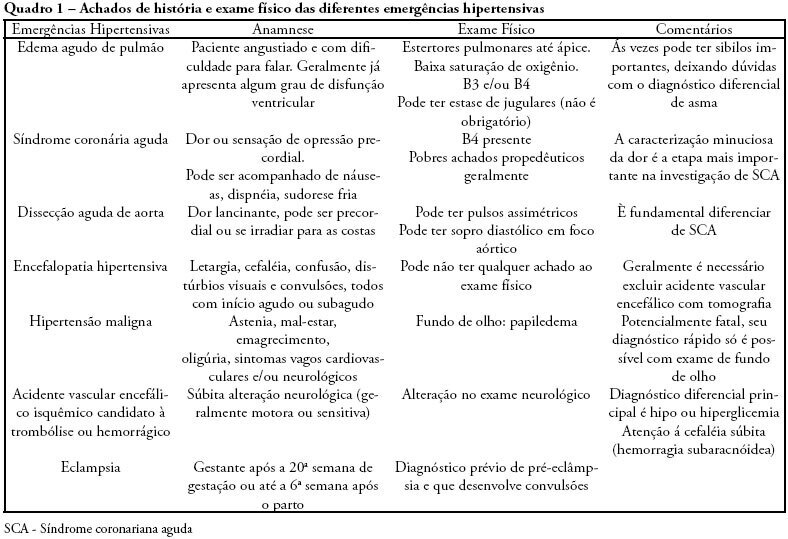
-
Case Reports
Use of noninvasive positive pressure ventilation and spinal anesthesia during hip replacement arthroplasty in a patient with severe chronic obstructive pulmonary disease: case report
Rev Bras Ter Intensiva. 2008;20(3):313-317
Abstract
Case ReportsUse of noninvasive positive pressure ventilation and spinal anesthesia during hip replacement arthroplasty in a patient with severe chronic obstructive pulmonary disease: case report
Rev Bras Ter Intensiva. 2008;20(3):313-317
DOI 10.1590/S0103-507X2008000300015
Views0Anesthetic management of patients with severe chronic obstructive pulmonary disease is extensively discussed, due to the high rates of complications in this subtype of patients submitted to medium and high complexity surgical procedures. The objective of this study is to report use of noninvasive positive pressure mechanical ventilation – bilevel positive airway pressure – and spinal anesthesia in a patient with severe chronic obstructive pulmonary disease during total hip arthroplasty. An 81 year old, male patient with severe chronic obstructive pulmonary disease (GOLD 4) was submitted to total hip arthroplasty due to a femoral bone fracture under spinal anestesia and noninvasive positive pressure mechanical ventilation-bilevel positive airway pressure with expiratory pressure of 7 cmH2O, inspiratory pressure of 15 cmH2O and O2 flow of 3 L/min. During the procedure, the patient had one episode of bronchospasm that was promptly reverted pharmacologically with no complications in the postoperative period. The combination of less invasive anesthetic and ventilation techniques is easy to apply and may be useful in the perioperative management of patients with high anesthetic morbidity. Interaction between clinical, surgical and anesthetic teams for these cases is very important to reduce the mortality associated with extensive procedures in severe patients.
Keywords:AgedoAnesthesia, epiduralArthroplastyCase Reportchronic obstructiveHumanMalePositive pressure respirationpulmonary diseaseReplacement, hipRespiration, artificialSee moreViews0Abstract
Case ReportsUse of noninvasive positive pressure ventilation and spinal anesthesia during hip replacement arthroplasty in a patient with severe chronic obstructive pulmonary disease: case report
Rev Bras Ter Intensiva. 2008;20(3):313-317
DOI 10.1590/S0103-507X2008000300015
Views0Anesthetic management of patients with severe chronic obstructive pulmonary disease is extensively discussed, due to the high rates of complications in this subtype of patients submitted to medium and high complexity surgical procedures. The objective of this study is to report use of noninvasive positive pressure mechanical ventilation – bilevel positive airway pressure – and spinal anesthesia in a patient with severe chronic obstructive pulmonary disease during total hip arthroplasty. An 81 year old, male patient with severe chronic obstructive pulmonary disease (GOLD 4) was submitted to total hip arthroplasty due to a femoral bone fracture under spinal anestesia and noninvasive positive pressure mechanical ventilation-bilevel positive airway pressure with expiratory pressure of 7 cmH2O, inspiratory pressure of 15 cmH2O and O2 flow of 3 L/min. During the procedure, the patient had one episode of bronchospasm that was promptly reverted pharmacologically with no complications in the postoperative period. The combination of less invasive anesthetic and ventilation techniques is easy to apply and may be useful in the perioperative management of patients with high anesthetic morbidity. Interaction between clinical, surgical and anesthetic teams for these cases is very important to reduce the mortality associated with extensive procedures in severe patients.
Keywords:AgedoAnesthesia, epiduralArthroplastyCase Reportchronic obstructiveHumanMalePositive pressure respirationpulmonary diseaseReplacement, hipRespiration, artificialSee more
-
Case Reports
Intra-arterial pulmonary thrombolysis at the postoperative period of brain aneurysm clamping: case report
Rev Bras Ter Intensiva. 2008;20(3):318-320
Abstract
Case ReportsIntra-arterial pulmonary thrombolysis at the postoperative period of brain aneurysm clamping: case report
Rev Bras Ter Intensiva. 2008;20(3):318-320
DOI 10.1590/S0103-507X2008000300016
Views0Pulmonary thromboembolism is a major cause of morbidity and mortality of patients undergoing neurosurgical procedures. The purpose of this study was to present a case of intra-arterial pulmonary thrombolysis in recent neurosurgery postoperative period. Male patient, undergoing neurosurgery, presented as a complication on the seventh day of postoperative massive pulmonary embolism with hemodynamic instability and intraarterial pulmonary thrombolysis with alteplase was indicated. Evolution was satisfactory without bleeding complications and patient was discharged. Pulmonary thromboembolism is a high morbidity and mortality condition at neurosurgical postoperative period and thrombolysis should be an alternative therapy in cases refractory to clinical treatment.
Keywords:Case reportsIntracranial aneurysmPostoperative periodpulmonary embolismThrombolytic therapySee moreViews0Abstract
Case ReportsIntra-arterial pulmonary thrombolysis at the postoperative period of brain aneurysm clamping: case report
Rev Bras Ter Intensiva. 2008;20(3):318-320
DOI 10.1590/S0103-507X2008000300016
Views0Pulmonary thromboembolism is a major cause of morbidity and mortality of patients undergoing neurosurgical procedures. The purpose of this study was to present a case of intra-arterial pulmonary thrombolysis in recent neurosurgery postoperative period. Male patient, undergoing neurosurgery, presented as a complication on the seventh day of postoperative massive pulmonary embolism with hemodynamic instability and intraarterial pulmonary thrombolysis with alteplase was indicated. Evolution was satisfactory without bleeding complications and patient was discharged. Pulmonary thromboembolism is a high morbidity and mortality condition at neurosurgical postoperative period and thrombolysis should be an alternative therapy in cases refractory to clinical treatment.
Keywords:Case reportsIntracranial aneurysmPostoperative periodpulmonary embolismThrombolytic therapySee more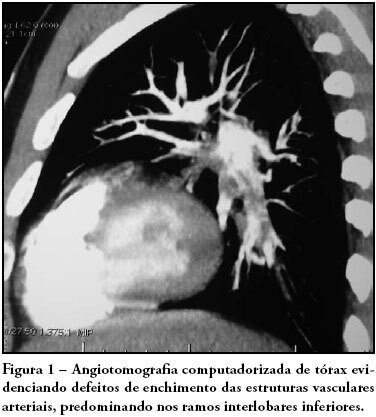
-
Letters to the Editor
Drotrecogin alfa (activated) in clinical practice and current evidences
Rev Bras Ter Intensiva. 2008;20(3):321-322
Abstract
Letters to the EditorDrotrecogin alfa (activated) in clinical practice and current evidences
Rev Bras Ter Intensiva. 2008;20(3):321-322
DOI 10.1590/S0103-507X2008000300017
Views0LETTER TO THE EDITOR Drotrecogin alfa (activated) in clinical practice and current evidences[…]See moreViews0Abstract
Letters to the EditorDrotrecogin alfa (activated) in clinical practice and current evidences
Rev Bras Ter Intensiva. 2008;20(3):321-322
DOI 10.1590/S0103-507X2008000300017
Views0LETTER TO THE EDITOR Drotrecogin alfa (activated) in clinical practice and current evidences[…]See more -
Letters to the Editor
Drotrecogin alfa (activated) in clinical practice and current evidences: reply
Rev Bras Ter Intensiva. 2008;20(3):323-324
Abstract
Letters to the EditorDrotrecogin alfa (activated) in clinical practice and current evidences: reply
Rev Bras Ter Intensiva. 2008;20(3):323-324
DOI 10.1590/S0103-507X2008000300018
Views0LETTER TO THE EDITOR Drotrecogin alfa (activated) in clinical practice and current evidences[…]See moreViews0Abstract
Letters to the EditorDrotrecogin alfa (activated) in clinical practice and current evidences: reply
Rev Bras Ter Intensiva. 2008;20(3):323-324
DOI 10.1590/S0103-507X2008000300018
Views0LETTER TO THE EDITOR Drotrecogin alfa (activated) in clinical practice and current evidences[…]See more
Volume Articles - Critical Care Science (CCS)
