-
Original Articles
Performance of six prognostic scores in critically ILL patients receiving renal replacement therapy
Rev Bras Ter Intensiva. 2008;20(2):115-123
Abstract
Original ArticlesPerformance of six prognostic scores in critically ILL patients receiving renal replacement therapy
Rev Bras Ter Intensiva. 2008;20(2):115-123
DOI 10.1590/S0103-507X2008000200001
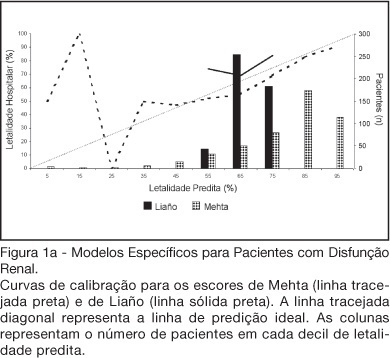
Views0See moreBACKGROUND AND OBJECTIVES: There is no consensus about prognostic scores for use in patients with acute kidney injury (AKI). The aim of this study was to evaluate the performance of six prognostic scores in predicting hospital mortality in patients with AKI and need for renal replacement therapy (RRT). METHODS: Prospective cohort of patients admitted to the intensive care units (ICU) of three tertiary care hospitals that required RRT for AKI over a 32-month period. Patients with end-stage renal disease and those with ICU stay < 24h were excluded. Data from the first 24h of ICU admission were used to calculate SAPS II and APACHE II scores, and data from the first 24h of RRT were used in the calculation of LOD, ODIN, Liaño and Mehta scores. Discrimination was evaluated using the area under ROC curve (AUROC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. The hospital mortality was the end-point of interest. RESULTS: 467 patients were evaluated. Hospital mortality rate was 75%. Mean SAPS II and APACHE II scores were 48.5 ±11.2 and 27.4 ± 6.3 points, and median LOD score was 7 (5-8) points. Except for Mehta score (p = 0.001), calibration was appropriate in all models. However, discrimination was uniformly unsatisfactory; AUROC ranged from 0.60 for ODIN to 0.72 for SAPS II and Mehta scores. In addition, except for Mehta, all models tended to underestimate hospital mortality. CONCLUSIONS: Organ dysfunction, general and renal-specific severity-of-illness scores were inaccurate in predicting outcome in ICU patients in need for RRT.
Views0

Abstract
Original ArticlesPerformance of six prognostic scores in critically ILL patients receiving renal replacement therapy
Rev Bras Ter Intensiva. 2008;20(2):115-123
DOI 10.1590/S0103-507X2008000200001
Views0See moreBACKGROUND AND OBJECTIVES: There is no consensus about prognostic scores for use in patients with acute kidney injury (AKI). The aim of this study was to evaluate the performance of six prognostic scores in predicting hospital mortality in patients with AKI and need for renal replacement therapy (RRT). METHODS: Prospective cohort of patients admitted to the intensive care units (ICU) of three tertiary care hospitals that required RRT for AKI over a 32-month period. Patients with end-stage renal disease and those with ICU stay < 24h were excluded. Data from the first 24h of ICU admission were used to calculate SAPS II and APACHE II scores, and data from the first 24h of RRT were used in the calculation of LOD, ODIN, Liaño and Mehta scores. Discrimination was evaluated using the area under ROC curve (AUROC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. The hospital mortality was the end-point of interest. RESULTS: 467 patients were evaluated. Hospital mortality rate was 75%. Mean SAPS II and APACHE II scores were 48.5 ±11.2 and 27.4 ± 6.3 points, and median LOD score was 7 (5-8) points. Except for Mehta score (p = 0.001), calibration was appropriate in all models. However, discrimination was uniformly unsatisfactory; AUROC ranged from 0.60 for ODIN to 0.72 for SAPS II and Mehta scores. In addition, except for Mehta, all models tended to underestimate hospital mortality. CONCLUSIONS: Organ dysfunction, general and renal-specific severity-of-illness scores were inaccurate in predicting outcome in ICU patients in need for RRT.
-
Original Articles
Validation of an early warning score in pre-intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):124-127
Abstract
Original ArticlesValidation of an early warning score in pre-intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):124-127
DOI 10.1590/S0103-507X2008000200002
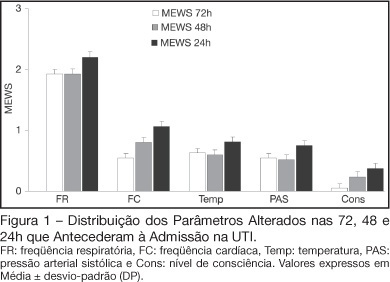
Views0See moreBACKGROUND AND OBJECTIVES: Prognosis of patients in the intensive care unit (ICU) has a relation with their severity just before admission. The Modified Early Warning Score (MEWS) was used to evaluate the severe condition of patients 12, 24 and 72 hours before admission in the ICU, assess the most prevalent parameters and correlate the MEWS before ICU with the outcome (survival versus death). METHODS: Retrospective analyses of 65 patients consecutively admitted to the ICU from July to October, 2006 evaluating the physiological parameters 72 hours prior to admission. RESULTS: APACHE II mean was 22.2 ± 7.9 points, mortality was 54.6% and standardized mortality ratio means was 1.24. MEWS means were 3.7 ± 0.2; 4.0 ± 0.2 and 5.1 ± 0.2 points, calculated 72, 48 and 24 hours previous to ICU admission, respectively. An increasing percentage of patients with MEWS > 3 points within 72, 48 and 24 hours before admission – 43.8%, 59.4% and 73.4%, respectively was recorded. Among the included physiological parameters respiratory rate contributed the most to the MEWS. Highest mortality was found in patients with MEWS > 3 points already found 72 hours before admission. Patients who died presented with a significant increase in the MEWS 24 hours prior to admission to the ICU (in relation to the MEWS recorded 72 hours before) but the situation was not identified in survivors. CONCLUSIONS: MEWS closely identified the severity of patients admitted to the ICU, suggesting that it can be a reliable score, useful in the situations preceding the ICU.
Views0Abstract
Original ArticlesValidation of an early warning score in pre-intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):124-127
DOI 10.1590/S0103-507X2008000200002
Views0See moreBACKGROUND AND OBJECTIVES: Prognosis of patients in the intensive care unit (ICU) has a relation with their severity just before admission. The Modified Early Warning Score (MEWS) was used to evaluate the severe condition of patients 12, 24 and 72 hours before admission in the ICU, assess the most prevalent parameters and correlate the MEWS before ICU with the outcome (survival versus death). METHODS: Retrospective analyses of 65 patients consecutively admitted to the ICU from July to October, 2006 evaluating the physiological parameters 72 hours prior to admission. RESULTS: APACHE II mean was 22.2 ± 7.9 points, mortality was 54.6% and standardized mortality ratio means was 1.24. MEWS means were 3.7 ± 0.2; 4.0 ± 0.2 and 5.1 ± 0.2 points, calculated 72, 48 and 24 hours previous to ICU admission, respectively. An increasing percentage of patients with MEWS > 3 points within 72, 48 and 24 hours before admission – 43.8%, 59.4% and 73.4%, respectively was recorded. Among the included physiological parameters respiratory rate contributed the most to the MEWS. Highest mortality was found in patients with MEWS > 3 points already found 72 hours before admission. Patients who died presented with a significant increase in the MEWS 24 hours prior to admission to the ICU (in relation to the MEWS recorded 72 hours before) but the situation was not identified in survivors. CONCLUSIONS: MEWS closely identified the severity of patients admitted to the ICU, suggesting that it can be a reliable score, useful in the situations preceding the ICU.
-
Original Articles
Sepsis in the intensive care unit: etiologies, prognostic factors and mortality
Rev Bras Ter Intensiva. 2008;20(2):128-134
Abstract
Original ArticlesSepsis in the intensive care unit: etiologies, prognostic factors and mortality
Rev Bras Ter Intensiva. 2008;20(2):128-134
DOI 10.1590/S0103-507X2008000200003
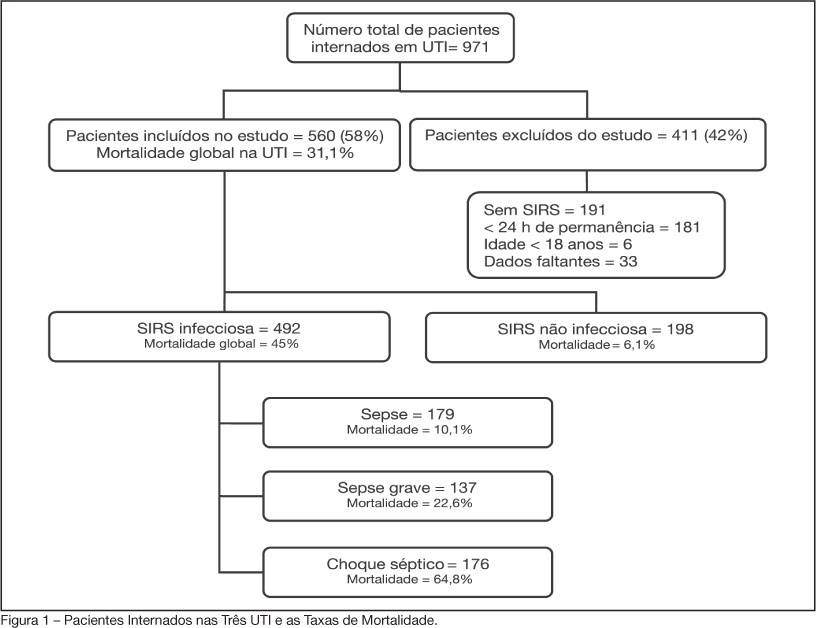
Views0See moreBACKGROUND AND OBJECTIVES: Sepsis is the main cause of death in patients treated in intensive care units (ICU). The aim of this study was to evaluate etiology, prognostic factors and mortality of septic patients treated in ICU of Passo Fundo, Brazil. METHODS: Out of 971 consecutive patients prospectively evaluated from August 2005 to February 2006, 560 were selected due to presence of systemic inflammatory response syndrome (SIRS) and followed for 28 days or until discharge or death. Patients were categorized according with the etiology of SIRS and further classified as having SIRS, sepsis, severe sepsis and septic shock. Prognosis was assessed by means of Apache II and SOFA. Mortality was compared in different etiologies of sepsis, APACHE II and SOFA scores, parameters. RESULTS: Of the 971 patients admitted to the ICU, 560 developed SIRS (58%). The most frequent cause of internation was neurological disease (28.9%), the most frequent site of infection was the respiratory tract (71.6%), and the most prevalent pathogens were gram-negative bacilli (53.2%). Mean APACHE II score was 18 ± 9, and mean SOFA score was 5 ± 4. Median ICU stay was 6 (3-11) days and overall mortality rate was 31.1%: 6.1% for non-infectious SIRS, 10.1% for sepsis, 22.6% for severe sepsis, and 64.8% for septic shock. CONCLUSIONS: Sepsis is an important health problem that leads to an extremely high mortality rate in the ICU of Passo Fundo, Brazil.
Views0Abstract
Original ArticlesSepsis in the intensive care unit: etiologies, prognostic factors and mortality
Rev Bras Ter Intensiva. 2008;20(2):128-134
DOI 10.1590/S0103-507X2008000200003
Views0See moreBACKGROUND AND OBJECTIVES: Sepsis is the main cause of death in patients treated in intensive care units (ICU). The aim of this study was to evaluate etiology, prognostic factors and mortality of septic patients treated in ICU of Passo Fundo, Brazil. METHODS: Out of 971 consecutive patients prospectively evaluated from August 2005 to February 2006, 560 were selected due to presence of systemic inflammatory response syndrome (SIRS) and followed for 28 days or until discharge or death. Patients were categorized according with the etiology of SIRS and further classified as having SIRS, sepsis, severe sepsis and septic shock. Prognosis was assessed by means of Apache II and SOFA. Mortality was compared in different etiologies of sepsis, APACHE II and SOFA scores, parameters. RESULTS: Of the 971 patients admitted to the ICU, 560 developed SIRS (58%). The most frequent cause of internation was neurological disease (28.9%), the most frequent site of infection was the respiratory tract (71.6%), and the most prevalent pathogens were gram-negative bacilli (53.2%). Mean APACHE II score was 18 ± 9, and mean SOFA score was 5 ± 4. Median ICU stay was 6 (3-11) days and overall mortality rate was 31.1%: 6.1% for non-infectious SIRS, 10.1% for sepsis, 22.6% for severe sepsis, and 64.8% for septic shock. CONCLUSIONS: Sepsis is an important health problem that leads to an extremely high mortality rate in the ICU of Passo Fundo, Brazil.
-
Original Articles
Characteristics and outcomes of patients treated with drotrecogin alpha and other interventions of the “Surviving Sepsis” campaign in clinical practice
Rev Bras Ter Intensiva. 2008;20(2):135-143
Abstract
Original ArticlesCharacteristics and outcomes of patients treated with drotrecogin alpha and other interventions of the “Surviving Sepsis” campaign in clinical practice
Rev Bras Ter Intensiva. 2008;20(2):135-143
DOI 10.1590/S0103-507X2008000200004
Views0See moreBACKGROUND AND OBJECTIVES: To face the high mortality of sepsis, interventions grouped as “Surviving Sepsis Campaign” have been suggested. The aim of the study was to describe the application of glycemic control, corticoid use in septic shock, inotropics and drotrecogin-alpha in sepsis. METHODS: We studied 110 patients with sepsis from Recife/Brazil, who received drotrecogin-alpha between 2003/2006. Data on management of sepsis considering Surviving Sepsis Campaign, drotrecogin-alpha, mortality at 28 days and severe bleeding were recorded. RESULTS: Mean APACHE II was 25.6 and mean SOFA was 9.2. Around 95% of the patients presented two or more organ dysfunctions and 98% presented septic shock. The majority (56%) were under 65 years. Abdominal (48%) and respiratory (28%) focus of infection were the most prevalent. Hydrocortisone was used in 61% of the patients, and 29 (48.3%) died. Of the 38 patients with prolonged shock that did not receive it, 28 (73.7%) died. Of the 97 patients who presented uncontrolled glycemia only 65% achieved strict glycemic control and the mortality was 51.6%. Fluid gain ranged from 600 ml to 9,400 ml in the first 24h. In only 30 patients was myocardial dysfunction detected. The infusion of drotrecogin alpha started within 24h in 45%, between 24 and 48h in 35% and after 48h in 20%. Death occurred in 57% and severe bleeding in 9%. CONCLUSIONS: Discrepancy between the recommendations of Surviving Sepsis Campaign and clinical practice was observed. Death rate was 57%, similar to that found in the literature for septic shock irrespective of the use of drotrecogin-alpha.
Views0Abstract
Original ArticlesCharacteristics and outcomes of patients treated with drotrecogin alpha and other interventions of the “Surviving Sepsis” campaign in clinical practice
Rev Bras Ter Intensiva. 2008;20(2):135-143
DOI 10.1590/S0103-507X2008000200004
Views0See moreBACKGROUND AND OBJECTIVES: To face the high mortality of sepsis, interventions grouped as “Surviving Sepsis Campaign” have been suggested. The aim of the study was to describe the application of glycemic control, corticoid use in septic shock, inotropics and drotrecogin-alpha in sepsis. METHODS: We studied 110 patients with sepsis from Recife/Brazil, who received drotrecogin-alpha between 2003/2006. Data on management of sepsis considering Surviving Sepsis Campaign, drotrecogin-alpha, mortality at 28 days and severe bleeding were recorded. RESULTS: Mean APACHE II was 25.6 and mean SOFA was 9.2. Around 95% of the patients presented two or more organ dysfunctions and 98% presented septic shock. The majority (56%) were under 65 years. Abdominal (48%) and respiratory (28%) focus of infection were the most prevalent. Hydrocortisone was used in 61% of the patients, and 29 (48.3%) died. Of the 38 patients with prolonged shock that did not receive it, 28 (73.7%) died. Of the 97 patients who presented uncontrolled glycemia only 65% achieved strict glycemic control and the mortality was 51.6%. Fluid gain ranged from 600 ml to 9,400 ml in the first 24h. In only 30 patients was myocardial dysfunction detected. The infusion of drotrecogin alpha started within 24h in 45%, between 24 and 48h in 35% and after 48h in 20%. Death occurred in 57% and severe bleeding in 9%. CONCLUSIONS: Discrepancy between the recommendations of Surviving Sepsis Campaign and clinical practice was observed. Death rate was 57%, similar to that found in the literature for septic shock irrespective of the use of drotrecogin-alpha.
-
Original Articles
Evaluation of intensivists’ knowledge on brain death
Rev Bras Ter Intensiva. 2008;20(2):144-148
Abstract
Original ArticlesEvaluation of intensivists’ knowledge on brain death
Rev Bras Ter Intensiva. 2008;20(2):144-148
DOI 10.1590/S0103-507X2008000200005
Views0See moreBACKGROUND AND OBJECTIVES: Failure or delay to diagnose brain death leads to needless occupation of a hospital bed, emotional and financial losses, and unavailability of organs for transplants. The intensive care physician plays an essential role in this diagnosis. This study intended to evaluate intensivists’ knowledge concerning brain death. METHODS: Cross-sectional study in 15 intensive care units (ICU) in eight hospitals in the city of Porto Alegre, Brazil. RESULTS: Two hundred forty-six intensivists were interviewed in a consecutive sample between April and December 2005. The prevalence of lack of knowledge regarding the concept was of 17%. Twenty per cent of the interviewees ignored the legal need for complementary confirmatory tests for their diagnosis. Forty-seven per cent considered themselves as having the highest level of assurance to explain the concept to a patient’s family members. Twenty-nine per cent erroneously determined the legal time of death for brain dead patients. Pediatric intensivists had less knowledge about the concept, when compared to intensivists for adults (p < 0.001). CONCLUSIONS: Current knowledge of brain death is insufficient in Brazil, among the health care professionals who most often find patients in this situation. Education on the subject is needed to avoid unnecessary expenses, reduce family suffering and increase the offer of organs for transplant.
Views0Abstract
Original ArticlesEvaluation of intensivists’ knowledge on brain death
Rev Bras Ter Intensiva. 2008;20(2):144-148
DOI 10.1590/S0103-507X2008000200005
Views0See moreBACKGROUND AND OBJECTIVES: Failure or delay to diagnose brain death leads to needless occupation of a hospital bed, emotional and financial losses, and unavailability of organs for transplants. The intensive care physician plays an essential role in this diagnosis. This study intended to evaluate intensivists’ knowledge concerning brain death. METHODS: Cross-sectional study in 15 intensive care units (ICU) in eight hospitals in the city of Porto Alegre, Brazil. RESULTS: Two hundred forty-six intensivists were interviewed in a consecutive sample between April and December 2005. The prevalence of lack of knowledge regarding the concept was of 17%. Twenty per cent of the interviewees ignored the legal need for complementary confirmatory tests for their diagnosis. Forty-seven per cent considered themselves as having the highest level of assurance to explain the concept to a patient’s family members. Twenty-nine per cent erroneously determined the legal time of death for brain dead patients. Pediatric intensivists had less knowledge about the concept, when compared to intensivists for adults (p < 0.001). CONCLUSIONS: Current knowledge of brain death is insufficient in Brazil, among the health care professionals who most often find patients in this situation. Education on the subject is needed to avoid unnecessary expenses, reduce family suffering and increase the offer of organs for transplant.
-
Original Articles
Variations in the measurement of weaning parameters of mechanical ventilation in Fortaleza hospitals
Rev Bras Ter Intensiva. 2008;20(2):149-153
Abstract
Original ArticlesVariations in the measurement of weaning parameters of mechanical ventilation in Fortaleza hospitals
Rev Bras Ter Intensiva. 2008;20(2):149-153
DOI 10.1590/S0103-507X2008000200006
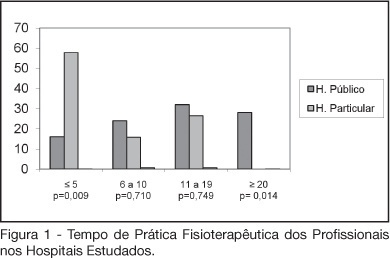
Views0See moreBACKGROUND AND OBJECTIVES: The number of patients requiring prolonged time on mechanical ventilation is increasing considerably in the intensive care unit (ICU). The objective of this study was to characterize the variability of methods and criteria used by physiotherapists to obtain weaning parameters in hospitals of Fortaleza. METHODS: After approval by the UNIFOR Ethics Committee, survey questionnaires were distributed among physiotherapists working in the ICU of three public and three private hospitals. Forty-four physiotherapists answered thirty-two multiple choice questions anonymously. RESULTS: The main results concerned parameters commonly evaluated by physiotherapists. A significant difference between hospitals was found regarding the rapid shallow breathing index and maximum inspiratory pressure, which are more often used in private hospitals, with a percentage of 100% and 89.5%, respectively. Concerning the ventilatory mode for obtaining the weaning parameters for mechanical ventilation; the T-tube was the most used, not only in the public (56%) but also in the private hospitals (57.9%). CONCLUSIONS: Variability in the methods and criteria used to obtain weaning parameters by the physiotherapists was found in public and private hospitals in Fortaleza. Results from this survey stress the need to develop new scientific studies to standardize the techniques used for weaning.
Views0Abstract
Original ArticlesVariations in the measurement of weaning parameters of mechanical ventilation in Fortaleza hospitals
Rev Bras Ter Intensiva. 2008;20(2):149-153
DOI 10.1590/S0103-507X2008000200006
Views0See moreBACKGROUND AND OBJECTIVES: The number of patients requiring prolonged time on mechanical ventilation is increasing considerably in the intensive care unit (ICU). The objective of this study was to characterize the variability of methods and criteria used by physiotherapists to obtain weaning parameters in hospitals of Fortaleza. METHODS: After approval by the UNIFOR Ethics Committee, survey questionnaires were distributed among physiotherapists working in the ICU of three public and three private hospitals. Forty-four physiotherapists answered thirty-two multiple choice questions anonymously. RESULTS: The main results concerned parameters commonly evaluated by physiotherapists. A significant difference between hospitals was found regarding the rapid shallow breathing index and maximum inspiratory pressure, which are more often used in private hospitals, with a percentage of 100% and 89.5%, respectively. Concerning the ventilatory mode for obtaining the weaning parameters for mechanical ventilation; the T-tube was the most used, not only in the public (56%) but also in the private hospitals (57.9%). CONCLUSIONS: Variability in the methods and criteria used to obtain weaning parameters by the physiotherapists was found in public and private hospitals in Fortaleza. Results from this survey stress the need to develop new scientific studies to standardize the techniques used for weaning.
-
Original Articles
Use of oral rinse with enzymatic system in patients totally dependent in the intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):154-159
Abstract
Original ArticlesUse of oral rinse with enzymatic system in patients totally dependent in the intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):154-159
DOI 10.1590/S0103-507X2008000200007
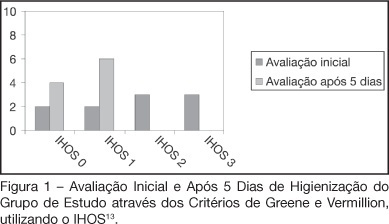
Views0See moreBACKGROUND AND OBJECTIVES: Patients admitted to an intensive care unit (ICU), in most cases do not have a proper oral hygiene. This deficient condition of oral hygiene in critical patients often triggers periodontitis, gingivitis and other systemic and oral complications. This research aimed to evaluate the efficiency of the antimicrobial action of a solution with bioactive enzymatic system for oral hygiene, in totally care-dependent patients admitted to ICU. METHODS: A prospective, double blind pilot study was conducted with 20 patients admitted to an ICU, divided into 2 groups with the same technique of oral hygiene, protocols but using different solutions: the study group (n = 10) using an oral solution with enzymatic system and the control group (n = 10) using an oral solution based on cetylpyridinium. RESULTS: Results of microbiological cultures collected in the study group and control group, before and after the use of enzymatic solution, showed no significant difference between groups (p = 0.41). In clinical evaluation of the Simplified Oral Hygiene Index (SOHI) statistical significance was found by the Fisher Exact test (p = 0.01) when comparing the study group and control group. The value of statistical significance was set at 5%, or p < 0.05. CONCLUSIONS: The use of oral rinse with the lactoperoxidase enzyme was effective in the clinical evaluation of the oral hygiene of patients totally care-dependent in the hospital. This study stresses the importance of developing more research on the oral care of these patients.
Views0Abstract
Original ArticlesUse of oral rinse with enzymatic system in patients totally dependent in the intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):154-159
DOI 10.1590/S0103-507X2008000200007
Views0See moreBACKGROUND AND OBJECTIVES: Patients admitted to an intensive care unit (ICU), in most cases do not have a proper oral hygiene. This deficient condition of oral hygiene in critical patients often triggers periodontitis, gingivitis and other systemic and oral complications. This research aimed to evaluate the efficiency of the antimicrobial action of a solution with bioactive enzymatic system for oral hygiene, in totally care-dependent patients admitted to ICU. METHODS: A prospective, double blind pilot study was conducted with 20 patients admitted to an ICU, divided into 2 groups with the same technique of oral hygiene, protocols but using different solutions: the study group (n = 10) using an oral solution with enzymatic system and the control group (n = 10) using an oral solution based on cetylpyridinium. RESULTS: Results of microbiological cultures collected in the study group and control group, before and after the use of enzymatic solution, showed no significant difference between groups (p = 0.41). In clinical evaluation of the Simplified Oral Hygiene Index (SOHI) statistical significance was found by the Fisher Exact test (p = 0.01) when comparing the study group and control group. The value of statistical significance was set at 5%, or p < 0.05. CONCLUSIONS: The use of oral rinse with the lactoperoxidase enzyme was effective in the clinical evaluation of the oral hygiene of patients totally care-dependent in the hospital. This study stresses the importance of developing more research on the oral care of these patients.
-
Original Articles
Antibiotic coated catheter to decrease infection: pilot study
Rev Bras Ter Intensiva. 2008;20(2):160-164
Abstract
Original ArticlesAntibiotic coated catheter to decrease infection: pilot study
Rev Bras Ter Intensiva. 2008;20(2):160-164
DOI 10.1590/S0103-507X2008000200008
Views0See moreBACKGROUND AND OBJECTIVES: Nosocomial catheter related bloodstream infections (CR-BSI) increase morbidity and mortality in critically ill patients. Central venous catheters (CVC) coated with rifampin and minocycline (RM) decrease rates of colonization and CR-BSI. However, recent trials challenged the clinical impact of such catheters. We designed this trial to compare rates of colonization and CR-BSI in RM catheters and controls in a cohort of critically ill patients in Brazil. METHODS: Prospective, controlled trial conducted in one medico-surgical ICU. Patients were assigned to receive a control or RM CVC. After removal, tips were cultured in association with blood cultures. Rates of colonization and CR-BSI were recorded. RESULTS: Among 120 catheters inserted, 100 could be evaluated, 49 in the uncoated and 51 in the coated group. Clinical characteristics of patients were similar in the two groups. Two cases of CR-BSI (3.9%) occurred in patients who received RM catheters compared with 5 (10.2%) in the uncoated group (p = 0.26). Six RM catheters (11.8%) were colonized compared with 14 (28.6%) control catheters (p = 0.036). Kaplan-Meier analysis showed no significant differences in the risk of colonization or CR-BSI. Rates of CR-BSI were 4.7 per 1000 catheter-days in the RM coated group compared to 11.4 per 1000 catheter days in the uncoated group (p = 0.45). CONCLUSIONS: In this pilot study, we showed lower rates of colonization in RM coated when compared with uncoated catheters. Incidence and rates of CR-BSI were similar in the two groups.
Views0Abstract
Original ArticlesAntibiotic coated catheter to decrease infection: pilot study
Rev Bras Ter Intensiva. 2008;20(2):160-164
DOI 10.1590/S0103-507X2008000200008
Views0See moreBACKGROUND AND OBJECTIVES: Nosocomial catheter related bloodstream infections (CR-BSI) increase morbidity and mortality in critically ill patients. Central venous catheters (CVC) coated with rifampin and minocycline (RM) decrease rates of colonization and CR-BSI. However, recent trials challenged the clinical impact of such catheters. We designed this trial to compare rates of colonization and CR-BSI in RM catheters and controls in a cohort of critically ill patients in Brazil. METHODS: Prospective, controlled trial conducted in one medico-surgical ICU. Patients were assigned to receive a control or RM CVC. After removal, tips were cultured in association with blood cultures. Rates of colonization and CR-BSI were recorded. RESULTS: Among 120 catheters inserted, 100 could be evaluated, 49 in the uncoated and 51 in the coated group. Clinical characteristics of patients were similar in the two groups. Two cases of CR-BSI (3.9%) occurred in patients who received RM catheters compared with 5 (10.2%) in the uncoated group (p = 0.26). Six RM catheters (11.8%) were colonized compared with 14 (28.6%) control catheters (p = 0.036). Kaplan-Meier analysis showed no significant differences in the risk of colonization or CR-BSI. Rates of CR-BSI were 4.7 per 1000 catheter-days in the RM coated group compared to 11.4 per 1000 catheter days in the uncoated group (p = 0.45). CONCLUSIONS: In this pilot study, we showed lower rates of colonization in RM coated when compared with uncoated catheters. Incidence and rates of CR-BSI were similar in the two groups.
-
Review Articles
Antithrombotics in acute coronary syndromes: actual guidelines and new evidences
Rev Bras Ter Intensiva. 2008;20(2):165-172
Abstract
Review ArticlesAntithrombotics in acute coronary syndromes: actual guidelines and new evidences
Rev Bras Ter Intensiva. 2008;20(2):165-172
DOI 10.1590/S0103-507X2008000200009
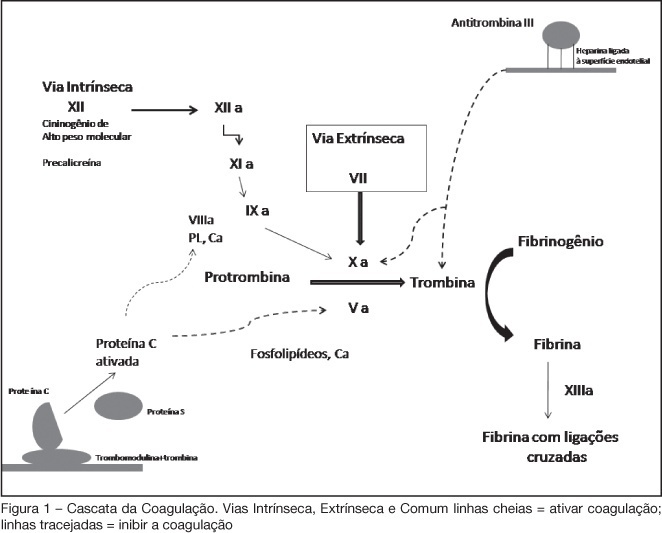
Views0See moreBACKGROUND AND OBJECTIVES: Acute coronary syndromes (ACS) are one of the most common causes of ICU admissions. New drugs have been developed for management of ACS. These drugs reduced morbidity and mortality; however their adverse effects or their incorrect use may cause excessive bleeding. The objective of this review is to present the principal peculiarities, doses, and indications of these drugs in ACS settings. METHODS: Original articles were retrieved crossing the terms acute coronary syndromes and antithrombotic therapy in the MedLine database as well as search for Brazilian and international guidelines in http://sumsearch.uthscsa.edu. RESULTS: In the treatment of acute coronary syndromes with non-ST-segment elevation enoxaparin was as efficient as UFH, but with a simpler management (SYNERGY and A to Z studies). In this same setting, fondaparinux was non inferior to enoxaparin and had lesser bleedings (OASIS 5), bivalirudin, combined or not with GPIIbIIIa blockers, was not inferior when compared with other heparins (ACUITY). In ST-segment elevation ACS, enoxaparin was superior to HNF in patients treated with fibrinolysis (EXTRACT TIMI 25); in OASIS 6 fondaparinux was superior to UFH in patients treated with thrombolytic therapy and not submitted to reperfusion. CONCLUSIONS: The correct management and individual combination of antithrombotic drugs are mandatory for decreased mortality and of major cardiovascular events, reducing the undesirable risk of additional bleeding.
Views0Abstract
Review ArticlesAntithrombotics in acute coronary syndromes: actual guidelines and new evidences
Rev Bras Ter Intensiva. 2008;20(2):165-172
DOI 10.1590/S0103-507X2008000200009
Views0See moreBACKGROUND AND OBJECTIVES: Acute coronary syndromes (ACS) are one of the most common causes of ICU admissions. New drugs have been developed for management of ACS. These drugs reduced morbidity and mortality; however their adverse effects or their incorrect use may cause excessive bleeding. The objective of this review is to present the principal peculiarities, doses, and indications of these drugs in ACS settings. METHODS: Original articles were retrieved crossing the terms acute coronary syndromes and antithrombotic therapy in the MedLine database as well as search for Brazilian and international guidelines in http://sumsearch.uthscsa.edu. RESULTS: In the treatment of acute coronary syndromes with non-ST-segment elevation enoxaparin was as efficient as UFH, but with a simpler management (SYNERGY and A to Z studies). In this same setting, fondaparinux was non inferior to enoxaparin and had lesser bleedings (OASIS 5), bivalirudin, combined or not with GPIIbIIIa blockers, was not inferior when compared with other heparins (ACUITY). In ST-segment elevation ACS, enoxaparin was superior to HNF in patients treated with fibrinolysis (EXTRACT TIMI 25); in OASIS 6 fondaparinux was superior to UFH in patients treated with thrombolytic therapy and not submitted to reperfusion. CONCLUSIONS: The correct management and individual combination of antithrombotic drugs are mandatory for decreased mortality and of major cardiovascular events, reducing the undesirable risk of additional bleeding.
-
Review Articles
Drotrecogin alfa activated in clinical practice and the current evidences
Rev Bras Ter Intensiva. 2008;20(2):173-177
Abstract
Review ArticlesDrotrecogin alfa activated in clinical practice and the current evidences
Rev Bras Ter Intensiva. 2008;20(2):173-177
DOI 10.1590/S0103-507X2008000200010
Views0See moreBACKGROUND AND OBJECTIVES: The debate on efficacy and patient safety related to the use of drotrecogin alfa (DrotAA) is timely, principally due to the negative results observed in clinical studies performed after the PROWESS study, and the economic cost-related impact of the drug on the healthcare system. The aim of this study was to review the main studies on the use of DrotAA in patients with severe sepsis. The focus was on drug efficacy-and patient safety-related issues. CONTENTS: Articles were selected by a MedLine search for studies on the use of DrotAA in patients with sepsis using the following key words: activated protein C; drotrecogin alfa; sepsis; septic shock; Xigris®. Additional references were retrieved from the studies initially selected. CONCLUSIONS: Mortality and bleeding complications associated with the use of DrotAA were more frequent in large observational studies than those reported in randomized trials. In the light of the current knowledge, routine use of DrotAA should be reevaluated until well-designed confirmatory clinical trials can clarify the true efficacy and safety of the drug and help identify the subgroup of patients that can benefit from use of DrotAA. Physicians should be cautious with the rapid transfer of evidences not well-documented, to the guidelines and recommendations practiced in the care and treatment of patients with severe sepsis.
Views0Abstract
Review ArticlesDrotrecogin alfa activated in clinical practice and the current evidences
Rev Bras Ter Intensiva. 2008;20(2):173-177
DOI 10.1590/S0103-507X2008000200010
Views0See moreBACKGROUND AND OBJECTIVES: The debate on efficacy and patient safety related to the use of drotrecogin alfa (DrotAA) is timely, principally due to the negative results observed in clinical studies performed after the PROWESS study, and the economic cost-related impact of the drug on the healthcare system. The aim of this study was to review the main studies on the use of DrotAA in patients with severe sepsis. The focus was on drug efficacy-and patient safety-related issues. CONTENTS: Articles were selected by a MedLine search for studies on the use of DrotAA in patients with sepsis using the following key words: activated protein C; drotrecogin alfa; sepsis; septic shock; Xigris®. Additional references were retrieved from the studies initially selected. CONCLUSIONS: Mortality and bleeding complications associated with the use of DrotAA were more frequent in large observational studies than those reported in randomized trials. In the light of the current knowledge, routine use of DrotAA should be reevaluated until well-designed confirmatory clinical trials can clarify the true efficacy and safety of the drug and help identify the subgroup of patients that can benefit from use of DrotAA. Physicians should be cautious with the rapid transfer of evidences not well-documented, to the guidelines and recommendations practiced in the care and treatment of patients with severe sepsis.
-
Review Articles
Pulmonary and extrapulmonary acute respiratory distress syndrome: are they different?
Rev Bras Ter Intensiva. 2008;20(2):178-183
Abstract
Review ArticlesPulmonary and extrapulmonary acute respiratory distress syndrome: are they different?
Rev Bras Ter Intensiva. 2008;20(2):178-183
DOI 10.1590/S0103-507X2008000200011
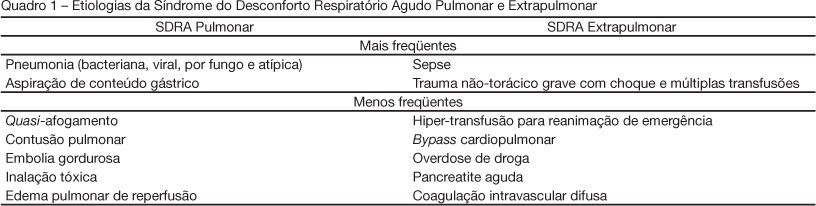
Views0See moreBACKGROUND AND OBJECTIVES: The pathogenesis of acute respiratory distress syndrome (ARDS) has been described by the presence of direct (pulmonary) and/or indirect (extrapulmonary) insult to the lung parenchyma. Evidence indicates that the pathophysiology of ARDS may differ according to the type of primary insult. This article presents a brief overview of differences between pulmonary and extrapulmonary ARDS, and discusses the interactions between morpho-functional aspects and response to differents therapies, both in experimental and clinical studies. CONTENTS: This systematic review included clinical and experimental ARDS studies found in MedLine and SciElo databases in the last 20 years. Many researchers acknowledge that experimental pulmonary and extrapulmonary ARDS are not identical with regard to morpho-functional aspects, the response to positive end-expiratory pressure (PEEP), recruitment manoeuvre, prone position and other adjunctive therapies. However, contradictory results have been reported in different clinical studies, which could be attributed to the difficulty of classifying ARDS in one or the other category, and to the assurance regarding the onset, phase and severity of ARDS in all patients. CONCLUSIONS: Heterogeneous ARDS patients are still considered as belonging to one syndrome, and are therefore treated in a similar manner. Thus, it is important to understand the pathophysiology of pulmonary and extrapulmonary ARDS in an attempt to better treat these patients.
Views0Abstract
Review ArticlesPulmonary and extrapulmonary acute respiratory distress syndrome: are they different?
Rev Bras Ter Intensiva. 2008;20(2):178-183
DOI 10.1590/S0103-507X2008000200011
Views0See moreBACKGROUND AND OBJECTIVES: The pathogenesis of acute respiratory distress syndrome (ARDS) has been described by the presence of direct (pulmonary) and/or indirect (extrapulmonary) insult to the lung parenchyma. Evidence indicates that the pathophysiology of ARDS may differ according to the type of primary insult. This article presents a brief overview of differences between pulmonary and extrapulmonary ARDS, and discusses the interactions between morpho-functional aspects and response to differents therapies, both in experimental and clinical studies. CONTENTS: This systematic review included clinical and experimental ARDS studies found in MedLine and SciElo databases in the last 20 years. Many researchers acknowledge that experimental pulmonary and extrapulmonary ARDS are not identical with regard to morpho-functional aspects, the response to positive end-expiratory pressure (PEEP), recruitment manoeuvre, prone position and other adjunctive therapies. However, contradictory results have been reported in different clinical studies, which could be attributed to the difficulty of classifying ARDS in one or the other category, and to the assurance regarding the onset, phase and severity of ARDS in all patients. CONCLUSIONS: Heterogeneous ARDS patients are still considered as belonging to one syndrome, and are therefore treated in a similar manner. Thus, it is important to understand the pathophysiology of pulmonary and extrapulmonary ARDS in an attempt to better treat these patients.
-
Review Articles
Benefits and complications of noninvasive mechanical ventilation for acute exacerbation of chronic obstructive pulmonary disease
Rev Bras Ter Intensiva. 2008;20(2):184-189
Abstract
Review ArticlesBenefits and complications of noninvasive mechanical ventilation for acute exacerbation of chronic obstructive pulmonary disease
Rev Bras Ter Intensiva. 2008;20(2):184-189
DOI 10.1590/S0103-507X2008000200012
Views0See moreBACKGROUND AND OBJECTIVES: Chronic obstructive pulmonary disease (COPD) is defined as a syndrome characterized by usually progressive chronic airflow limitation which is associated to a bronchial hyperresponsiveness and is partially reversible. Noninvasive mechanical ventilation is an alternative treatment for patients with COPD exacerbations. The objective of the literature reviews was to verify noninvasive mechanical ventilation benefits and complications in acute exacerbations of chronic obstructive pulmonary disease in patients. CONTENTS: This national and international’s scientific literature review was developed according to criteria established for documentary research in the MedLine, LILACS, SciElo, PubMed and Cochrane, databases using the key words: chronic obstructive pulmonary disease and noninvasive mechanical ventilation. Inclusion criteria were articles published from 1995 to 2007; in English, Spanish and Portuguese; studies in the human model and with no gender restriction. CONCLUSIONS: Noninvasive mechanical ventilation can reduce partial pressure of carbon dioxide, improve gas exchange, alleviate symptoms as dyspnea caused by fatigue of the respiratory muscles, reduce duration of hospitalization, decrease need for invasive mechanical ventilation, reduce number of complications and also lessen hospital mortality. The main complications found were: facial skin erythema, claustrophobia, nasal congestion, face pain, eye irritation, aspiration pneumonia, hypotension, pneumothorax, aerophagia, hypercapnia, gastric insufflation, vomit, bronchoaspiration, morning headaches, face injuries, air embolism and, last but not least, discomfort of the patient. Noninvasive mechanical ventilation can be more effective in patients with moderate-severe exacerbations of COPD and these complications can be minimized by an adequate interface also by the contribution of the physiotherapist experience.
Views0Abstract
Review ArticlesBenefits and complications of noninvasive mechanical ventilation for acute exacerbation of chronic obstructive pulmonary disease
Rev Bras Ter Intensiva. 2008;20(2):184-189
DOI 10.1590/S0103-507X2008000200012
Views0See moreBACKGROUND AND OBJECTIVES: Chronic obstructive pulmonary disease (COPD) is defined as a syndrome characterized by usually progressive chronic airflow limitation which is associated to a bronchial hyperresponsiveness and is partially reversible. Noninvasive mechanical ventilation is an alternative treatment for patients with COPD exacerbations. The objective of the literature reviews was to verify noninvasive mechanical ventilation benefits and complications in acute exacerbations of chronic obstructive pulmonary disease in patients. CONTENTS: This national and international’s scientific literature review was developed according to criteria established for documentary research in the MedLine, LILACS, SciElo, PubMed and Cochrane, databases using the key words: chronic obstructive pulmonary disease and noninvasive mechanical ventilation. Inclusion criteria were articles published from 1995 to 2007; in English, Spanish and Portuguese; studies in the human model and with no gender restriction. CONCLUSIONS: Noninvasive mechanical ventilation can reduce partial pressure of carbon dioxide, improve gas exchange, alleviate symptoms as dyspnea caused by fatigue of the respiratory muscles, reduce duration of hospitalization, decrease need for invasive mechanical ventilation, reduce number of complications and also lessen hospital mortality. The main complications found were: facial skin erythema, claustrophobia, nasal congestion, face pain, eye irritation, aspiration pneumonia, hypotension, pneumothorax, aerophagia, hypercapnia, gastric insufflation, vomit, bronchoaspiration, morning headaches, face injuries, air embolism and, last but not least, discomfort of the patient. Noninvasive mechanical ventilation can be more effective in patients with moderate-severe exacerbations of COPD and these complications can be minimized by an adequate interface also by the contribution of the physiotherapist experience.
-
Review Articles
Care of patient resuscitated from cardiac arrest
Rev Bras Ter Intensiva. 2008;20(2):190-196
Abstract
Review ArticlesCare of patient resuscitated from cardiac arrest
Rev Bras Ter Intensiva. 2008;20(2):190-196
DOI 10.1590/S0103-507X2008000200013
Views0See moreBACKGROUND AND OBJECTIVES: Out-of-hospital cardiac arrest is a major cause of death with survival rates as low as 5% to 35%. A large number of patients who survive resuscitation will face significant neurological damage, as a result of the ischemia that occurs both during cardiac arrest and reperfusion. However understanding of the mechanisms responsible for brain damage has not resulted in prognostic improvement. Therapeutic hypothermia after resuscitation may be a valid option associated to reduction of neurological damage. The purpose of this study was to review scientific evidence related to a therapy for patients resuscitated from cardiac arrest. CONTENTS: Description and analysis of the main risk factors associated with neurological damage after resuscitation from cardiac arrest as well as prognostic criteria was carried out. A non-systematic search was conducted in the PubMed data base for papers on a therapeutic approach for patients resuscitated from cardiac arrest. Bibliographic references of reviewed papers were also analyzed. Practical rules were drafted for such an approach. CONCLUSIONS: Patients resuscitated from cardiac arrest face a high level of risk of neurological damage. Therapeutic hypothermia and control of physiological parameters to optimise brain perfusion, may improve prognosis.
Views0Abstract
Review ArticlesCare of patient resuscitated from cardiac arrest
Rev Bras Ter Intensiva. 2008;20(2):190-196
DOI 10.1590/S0103-507X2008000200013
Views0See moreBACKGROUND AND OBJECTIVES: Out-of-hospital cardiac arrest is a major cause of death with survival rates as low as 5% to 35%. A large number of patients who survive resuscitation will face significant neurological damage, as a result of the ischemia that occurs both during cardiac arrest and reperfusion. However understanding of the mechanisms responsible for brain damage has not resulted in prognostic improvement. Therapeutic hypothermia after resuscitation may be a valid option associated to reduction of neurological damage. The purpose of this study was to review scientific evidence related to a therapy for patients resuscitated from cardiac arrest. CONTENTS: Description and analysis of the main risk factors associated with neurological damage after resuscitation from cardiac arrest as well as prognostic criteria was carried out. A non-systematic search was conducted in the PubMed data base for papers on a therapeutic approach for patients resuscitated from cardiac arrest. Bibliographic references of reviewed papers were also analyzed. Practical rules were drafted for such an approach. CONCLUSIONS: Patients resuscitated from cardiac arrest face a high level of risk of neurological damage. Therapeutic hypothermia and control of physiological parameters to optimise brain perfusion, may improve prognosis.
-
Review Articles
Acute coronary syndromes: treatment and risk stratification
Rev Bras Ter Intensiva. 2008;20(2):197-204
Abstract
Review ArticlesAcute coronary syndromes: treatment and risk stratification
Rev Bras Ter Intensiva. 2008;20(2):197-204
DOI 10.1590/S0103-507X2008000200014
Views0BACKGROUND AND OBJECTIVES: Acute coronary syndromes result from a disruption of a vulnerable coronary plaque complicated by intraluminal thrombus formation, embolisation, and variable degrees of coronary obstruction. Patients with total occlusion may present with acute ST Elevation Myocardial Infarction (STEMI). Partial vessel obstruction may result in Non-ST-Elevation Acute Myocardial Infarction (NSTEMI) or unstable angina (UA). Clinical symptoms and electrocardiographic changes are the main components of identification of ACS. The rapid and effective triage of such patients regarding presence or absence of ST-segment elevation is critical to dictate further therapeutic strategies. The objective of this chapter was to review current evidence and recommendations for the evaluation and early treatment of acute coronary syndromes. CONTENTS: We performed a clinical review using the electronic databases MedLine and LILACS from January 1990 to September 2007. CONCLUSIONS: Reperfusion of the infarct-related artery is the cornerstone of therapy for STEMI. Fibrinolysis and percutaneous coronary intervention are both well established as effective options. Management of UA/NSTEMI patients requires early risk stratification. High-risk patients should undergo an early invasive strategy that consists in performance of cardiac catheterization in the first 24 to 48 hours of presentation.
Keywords:acute coronary syndromesmyocardial infarctionNon-ST elevation acute coronary syndromepercutaneous coronary interventionreperfusion treatmentrisk stratificationST elevation acute coronary syndromeunstable anginaSee moreViews0Abstract
Review ArticlesAcute coronary syndromes: treatment and risk stratification
Rev Bras Ter Intensiva. 2008;20(2):197-204
DOI 10.1590/S0103-507X2008000200014
Views0BACKGROUND AND OBJECTIVES: Acute coronary syndromes result from a disruption of a vulnerable coronary plaque complicated by intraluminal thrombus formation, embolisation, and variable degrees of coronary obstruction. Patients with total occlusion may present with acute ST Elevation Myocardial Infarction (STEMI). Partial vessel obstruction may result in Non-ST-Elevation Acute Myocardial Infarction (NSTEMI) or unstable angina (UA). Clinical symptoms and electrocardiographic changes are the main components of identification of ACS. The rapid and effective triage of such patients regarding presence or absence of ST-segment elevation is critical to dictate further therapeutic strategies. The objective of this chapter was to review current evidence and recommendations for the evaluation and early treatment of acute coronary syndromes. CONTENTS: We performed a clinical review using the electronic databases MedLine and LILACS from January 1990 to September 2007. CONCLUSIONS: Reperfusion of the infarct-related artery is the cornerstone of therapy for STEMI. Fibrinolysis and percutaneous coronary intervention are both well established as effective options. Management of UA/NSTEMI patients requires early risk stratification. High-risk patients should undergo an early invasive strategy that consists in performance of cardiac catheterization in the first 24 to 48 hours of presentation.
Keywords:acute coronary syndromesmyocardial infarctionNon-ST elevation acute coronary syndromepercutaneous coronary interventionreperfusion treatmentrisk stratificationST elevation acute coronary syndromeunstable anginaSee more -
Case Reports
The use of noninvasive mechanical ventilation in the palliative care of a patient with metastatic thoracic sarcoma: case report
Rev Bras Ter Intensiva. 2008;20(2):205-209
Abstract
Case ReportsThe use of noninvasive mechanical ventilation in the palliative care of a patient with metastatic thoracic sarcoma: case report
Rev Bras Ter Intensiva. 2008;20(2):205-209
DOI 10.1590/S0103-507X2008000200015
Views0See moreBACKGROUND AND OBJECTIVES: Palliative care is based on prevention and relief of suffering, identifying, assessing and treating pain and other physical, psychological, social and spiritual problems. Sudden dyspnea is frequently observed in terminal oncologic patients. In these cases, noninvasive ventilation can be an adequate option to control dyspnea promoting comfort and allowing patient interaction with their relatives. The aim of this article was to present the benefits of noninvasive ventilation in the palliative care setting. CASE REPORT: The case of a 29 year old patient, admitted in intensive care unit (ICU), after cesarean section delivery, for clinical treatment of acute respiratory failure is reported. Chest X-ray showed pulmonary mass in the right lung. After clinical and image investigation, metastatic thoracic sarcoma was diagnosed and palliative cares were introduced. The ICU interdisciplinary team chose to use noninvasive ventilation (modality CPAP + PSV) to relieve dyspnea and discomfort, as well as to allow interaction with her baby and family. CONCLUSIONS: Palliative care with noninvasive ventilation contributed to increase comfort of the patient by controlling dyspnea.
Views0Abstract
Case ReportsThe use of noninvasive mechanical ventilation in the palliative care of a patient with metastatic thoracic sarcoma: case report
Rev Bras Ter Intensiva. 2008;20(2):205-209
DOI 10.1590/S0103-507X2008000200015
Views0See moreBACKGROUND AND OBJECTIVES: Palliative care is based on prevention and relief of suffering, identifying, assessing and treating pain and other physical, psychological, social and spiritual problems. Sudden dyspnea is frequently observed in terminal oncologic patients. In these cases, noninvasive ventilation can be an adequate option to control dyspnea promoting comfort and allowing patient interaction with their relatives. The aim of this article was to present the benefits of noninvasive ventilation in the palliative care setting. CASE REPORT: The case of a 29 year old patient, admitted in intensive care unit (ICU), after cesarean section delivery, for clinical treatment of acute respiratory failure is reported. Chest X-ray showed pulmonary mass in the right lung. After clinical and image investigation, metastatic thoracic sarcoma was diagnosed and palliative cares were introduced. The ICU interdisciplinary team chose to use noninvasive ventilation (modality CPAP + PSV) to relieve dyspnea and discomfort, as well as to allow interaction with her baby and family. CONCLUSIONS: Palliative care with noninvasive ventilation contributed to increase comfort of the patient by controlling dyspnea.

-
Case Reports
Noninvasive mechanical ventilation in patient with pneumocystis jirovecii pneumonia: case report
Rev Bras Ter Intensiva. 2008;20(2):210-212
Abstract
Case ReportsNoninvasive mechanical ventilation in patient with pneumocystis jirovecii pneumonia: case report
Rev Bras Ter Intensiva. 2008;20(2):210-212
DOI 10.1590/S0103-507X2008000200016
Views0See moreBACKGROUND AND OBJECTIVES: Pneumocystis jirovecii pneumonia has been one of the most common diseases and life-threatening infectious complications in acquired immunodeficiency syndrome patients. The objective of the case report was to present a patient with probable diagnosis of Pneumocystis jirovecii pneumonia who received noninvasive positive pressure ventilation. CASE REPORT: A female patient, 25 years old, with probable diagnosis of Pneumocystis jirovecii pneumonia received noninvasive positive pressure ventilation. CONCLUSIONS: All respiratory parameters progressively improved in the first five days. Results suggest the efficacy of this support to improve oxygenation, to revert hypoxemia and to prevent orotracheal intubation.
Views0Abstract
Case ReportsNoninvasive mechanical ventilation in patient with pneumocystis jirovecii pneumonia: case report
Rev Bras Ter Intensiva. 2008;20(2):210-212
DOI 10.1590/S0103-507X2008000200016
Views0See moreBACKGROUND AND OBJECTIVES: Pneumocystis jirovecii pneumonia has been one of the most common diseases and life-threatening infectious complications in acquired immunodeficiency syndrome patients. The objective of the case report was to present a patient with probable diagnosis of Pneumocystis jirovecii pneumonia who received noninvasive positive pressure ventilation. CASE REPORT: A female patient, 25 years old, with probable diagnosis of Pneumocystis jirovecii pneumonia received noninvasive positive pressure ventilation. CONCLUSIONS: All respiratory parameters progressively improved in the first five days. Results suggest the efficacy of this support to improve oxygenation, to revert hypoxemia and to prevent orotracheal intubation.
Volume Articles - Critical Care Science (CCS)
