-
Daily interruption of sedatives: a panacea?
Rev Bras Ter Intensiva. 2008;20(1):5-5
-
Assessment of a risk scale in patients submitted to coronary artery bypass surgery: analysis of 400 cases
Rev Bras Ter Intensiva. 2008;20(1):6-17
Abstract
Assessment of a risk scale in patients submitted to coronary artery bypass surgery: analysis of 400 cases
Rev Bras Ter Intensiva. 2008;20(1):6-17
DOI 10.1590/S0103-507X2008000100002
Views0See moreBACKGROUND AND OBJECTIVES: The objective of this paper was to assess a risk scale based on a protocol developed at The Cleveland Clinic Foundation for the coronary artery bypass surgery using preoperative and perioperative parameters and the patient’s physiological profile at the admission in the intensive care unit (ICU). METHODS: In the period between May,1999 and January,2002 part of the patients who underwent coronary artery bypass surgery in the cardiac service of the Hospital Universitário Cajuru of Pontifícia Universidade Católica do Paraná were included in the assessment of the operative risk scale, prospectively and consecutive. During the postoperative assessment a parameter < 6 was associated to less severe cases and parameters above 7 corresponding to more severe cases. For the evaluation of ICU admission, this classification was associated with parameter values < and > 14. Morbidity was classified in major complications as well as less important complications. There were including all patients that it was possible to include all variables of the protocol. RESULTS: Four hundred patients who underwent surgery, with cardiopulmonary bypass or off-pump coronary bypass, were assessed. There was 22 deaths (5.5%) and 124 patients with major complications (31%). The most common preoperative risk factors were the age between 65 and 74 in 111 cases (27.75%), weight below 65 kg in 106 (26.5%). Diabetes mellitus being treated in 89 cases (22.5%). The cardiopulmonary bypass time was above 160 minutes in 13 cases (6.95%) and intra-aortic balloon pump was used in 11 (2.75%). During the analysis of the ICU admission physiology, the alveolar arterial gradient equal or above 250 mmHg was the parameter found in 334 patients (83.5%), arterial sodium bicarbonate at ICU below 21 mmol/L was identified in 265 patients (66.25%), and the marginal or inadequate cardiovascular performance was observed in 263 patients (65.75%). The major complications occurred in 124 patients (31%) and the low output syndrome was more frequently seen in 64 (51.61%) of the cases. Twenty-two deaths were recorded (5.5%) and the ones with cardiovascular etiology were the most frequent (40.9%). In 370 patients (92.5%) the preoperative assessment showed as a result a parameter equal or below 6 and the ICU admission, the parameter was equal or below 14 in 345 cases (86.25%). Patients with parameters above that, at the preoperative and at the ICU admission, have shown more complications and more deaths. CONCLUSIONS: It was possible to conclude that the parameters recorded at the preoperative and at the ICU admission were correlated with the probability of death and complications and the ICU admission parameter, associated with the preoperative parameters and intraoperative factors bring more information for the prognostic of death and complications. The adjusted models adequately express the death and complications probabilities estimate, due to the preoperative, intraoperative and ICU admission parameters.
Views0

Abstract
Assessment of a risk scale in patients submitted to coronary artery bypass surgery: analysis of 400 cases
Rev Bras Ter Intensiva. 2008;20(1):6-17
DOI 10.1590/S0103-507X2008000100002
Views0See moreBACKGROUND AND OBJECTIVES: The objective of this paper was to assess a risk scale based on a protocol developed at The Cleveland Clinic Foundation for the coronary artery bypass surgery using preoperative and perioperative parameters and the patient’s physiological profile at the admission in the intensive care unit (ICU). METHODS: In the period between May,1999 and January,2002 part of the patients who underwent coronary artery bypass surgery in the cardiac service of the Hospital Universitário Cajuru of Pontifícia Universidade Católica do Paraná were included in the assessment of the operative risk scale, prospectively and consecutive. During the postoperative assessment a parameter < 6 was associated to less severe cases and parameters above 7 corresponding to more severe cases. For the evaluation of ICU admission, this classification was associated with parameter values < and > 14. Morbidity was classified in major complications as well as less important complications. There were including all patients that it was possible to include all variables of the protocol. RESULTS: Four hundred patients who underwent surgery, with cardiopulmonary bypass or off-pump coronary bypass, were assessed. There was 22 deaths (5.5%) and 124 patients with major complications (31%). The most common preoperative risk factors were the age between 65 and 74 in 111 cases (27.75%), weight below 65 kg in 106 (26.5%). Diabetes mellitus being treated in 89 cases (22.5%). The cardiopulmonary bypass time was above 160 minutes in 13 cases (6.95%) and intra-aortic balloon pump was used in 11 (2.75%). During the analysis of the ICU admission physiology, the alveolar arterial gradient equal or above 250 mmHg was the parameter found in 334 patients (83.5%), arterial sodium bicarbonate at ICU below 21 mmol/L was identified in 265 patients (66.25%), and the marginal or inadequate cardiovascular performance was observed in 263 patients (65.75%). The major complications occurred in 124 patients (31%) and the low output syndrome was more frequently seen in 64 (51.61%) of the cases. Twenty-two deaths were recorded (5.5%) and the ones with cardiovascular etiology were the most frequent (40.9%). In 370 patients (92.5%) the preoperative assessment showed as a result a parameter equal or below 6 and the ICU admission, the parameter was equal or below 14 in 345 cases (86.25%). Patients with parameters above that, at the preoperative and at the ICU admission, have shown more complications and more deaths. CONCLUSIONS: It was possible to conclude that the parameters recorded at the preoperative and at the ICU admission were correlated with the probability of death and complications and the ICU admission parameter, associated with the preoperative parameters and intraoperative factors bring more information for the prognostic of death and complications. The adjusted models adequately express the death and complications probabilities estimate, due to the preoperative, intraoperative and ICU admission parameters.
-
Relative adrenal insufficiency in septic shock: comparison of the response to hydrocortisone in patients diagnosed through random cortisol measurement versus corticotropin test
Rev Bras Ter Intensiva. 2008;20(1):18-23
Abstract
Relative adrenal insufficiency in septic shock: comparison of the response to hydrocortisone in patients diagnosed through random cortisol measurement versus corticotropin test
Rev Bras Ter Intensiva. 2008;20(1):18-23
DOI 10.1590/S0103-507X2008000100003
Views0See moreBACKGROUND AND OBJECTIVES: The incidence of relative adrenal insufficiency (RAI) in patients with septic shock is high and has a significant impact on survival. The purpose of this study was to determine whether a random cortisol concentration < 25 mg/dL was as good as a low dose (1 mg) corticotrophin stimulation test in the diagnosis of RAI in patients with septic shock as assessed by the hemodynamic response to hydrocortisone. METHODS: Patients were randomized to a single cortisol determination or to a low dose corticotrophin stimulation test. After blood collection to cortisol determinations, hydrocortisone (100 mg every 8 hrs) was administered for all patients in the first 36 hours. RAI was defined by a random cortisol concentration < 25 mg/dL or a D cortisol concentration < 9 mg/dL in the corticotrophin test. RESULTS: Sixty patients (G1 = 30; G2 = 30) were included in the analysis and were comparable regarding to demographic data, nosologies and disease severity. The time to norepinephrin withdrawal in group 1 patients with RAI diagnostic criteria was not different from the patients with cortisol > 25 mg/dL. In group 2 patients with D cortisol < 9 mg/dL had a shorter time of norepinephrin infusion (3 days) compared to patients with D cortisol > 9 (6 days). CONCLUSIONS: This study suggests that 1 mg corticotrophin test is better than a random cortisol determination < 25 mg/dL to the diagnosis of relative adrenal insufficiency in septic shock patients.
Views0Abstract
Relative adrenal insufficiency in septic shock: comparison of the response to hydrocortisone in patients diagnosed through random cortisol measurement versus corticotropin test
Rev Bras Ter Intensiva. 2008;20(1):18-23
DOI 10.1590/S0103-507X2008000100003
Views0See moreBACKGROUND AND OBJECTIVES: The incidence of relative adrenal insufficiency (RAI) in patients with septic shock is high and has a significant impact on survival. The purpose of this study was to determine whether a random cortisol concentration < 25 mg/dL was as good as a low dose (1 mg) corticotrophin stimulation test in the diagnosis of RAI in patients with septic shock as assessed by the hemodynamic response to hydrocortisone. METHODS: Patients were randomized to a single cortisol determination or to a low dose corticotrophin stimulation test. After blood collection to cortisol determinations, hydrocortisone (100 mg every 8 hrs) was administered for all patients in the first 36 hours. RAI was defined by a random cortisol concentration < 25 mg/dL or a D cortisol concentration < 9 mg/dL in the corticotrophin test. RESULTS: Sixty patients (G1 = 30; G2 = 30) were included in the analysis and were comparable regarding to demographic data, nosologies and disease severity. The time to norepinephrin withdrawal in group 1 patients with RAI diagnostic criteria was not different from the patients with cortisol > 25 mg/dL. In group 2 patients with D cortisol < 9 mg/dL had a shorter time of norepinephrin infusion (3 days) compared to patients with D cortisol > 9 (6 days). CONCLUSIONS: This study suggests that 1 mg corticotrophin test is better than a random cortisol determination < 25 mg/dL to the diagnosis of relative adrenal insufficiency in septic shock patients.
-
Evaluate the clonidine use for sedoanalgesia in intensive care unit patients under prolonged mechanical ventilation
Rev Bras Ter Intensiva. 2008;20(1):24-30
Abstract
Evaluate the clonidine use for sedoanalgesia in intensive care unit patients under prolonged mechanical ventilation
Rev Bras Ter Intensiva. 2008;20(1):24-30
DOI 10.1590/S0103-507X2008000100004
Views0See moreBACKGROUND AND OBJECTIVES: The control of patient discomfort in the intensive care unit (ICU) has become an integral part of critical care practice. The sedoanalgesic drugs could influence critically ill patient’s morbimortality. Alpha²-adrenoceptor agonists might have an interesting future in ICU. The objective of this study is to evaluate the clonidine use for sedoanalgesia in ICU patients under prolonged mechanical ventilation. METHODS: Historical cohort study. Admitted patient files, January-December 2006, which stayed under mechanical ventilation, analgesia and sedation > 7days were analyzed. Demographic, clinical features and therapeutic data concerning analgesia and sedation were remarked. The data allowed classify the patients in three different groups: G1 = patients that used clonidine and other drugs; G2 = patients that used three or more drugs, without clonidine and G3 = patients that used fentanyl and midazolam. The mean daily doses of infused clonidine were registered, and the values of heat rate (HR), blood arterial pressure (BAP) before starting use of clonidine, after six hours and 24 hours were also registered. Statistical analyzes were performed using Variance Analysis (ANOVA), t tests and x² (significance p < 0.05). RESULTS: Were selected 55 patients. Fifteen (27.2%) belonged to G1, 11 (20%) belonged to G2 and 29 (52.7%) belonged to G3. The mean age of patients was 44 (G1), 50 (G2) and 56 (G3) (p = NS). The mean score APACHE II was 18 (G1), 20.4 (G2) and 20.7 (G3) (p = NS). G1 and G2 patients presented higher ICU length-of-stay (p < 0.05). The mean dose of clonidine used was 1.21 ± 0.54 mg/kg/min. G1 patients had HR and BAP decreased, however these effects were not considered clinically relevant. The mortality was lower in the patients from G1 (20%) when compared to G2 (54.5%) and G3 (62%) (p < 0.05). CONCLUSIONS: The clonidine use to analyzed patients did not result in clinical relevant side effects. The lower mortality index in patients that used clonidine was statistical significant.
Views0Abstract
Evaluate the clonidine use for sedoanalgesia in intensive care unit patients under prolonged mechanical ventilation
Rev Bras Ter Intensiva. 2008;20(1):24-30
DOI 10.1590/S0103-507X2008000100004
Views0See moreBACKGROUND AND OBJECTIVES: The control of patient discomfort in the intensive care unit (ICU) has become an integral part of critical care practice. The sedoanalgesic drugs could influence critically ill patient’s morbimortality. Alpha²-adrenoceptor agonists might have an interesting future in ICU. The objective of this study is to evaluate the clonidine use for sedoanalgesia in ICU patients under prolonged mechanical ventilation. METHODS: Historical cohort study. Admitted patient files, January-December 2006, which stayed under mechanical ventilation, analgesia and sedation > 7days were analyzed. Demographic, clinical features and therapeutic data concerning analgesia and sedation were remarked. The data allowed classify the patients in three different groups: G1 = patients that used clonidine and other drugs; G2 = patients that used three or more drugs, without clonidine and G3 = patients that used fentanyl and midazolam. The mean daily doses of infused clonidine were registered, and the values of heat rate (HR), blood arterial pressure (BAP) before starting use of clonidine, after six hours and 24 hours were also registered. Statistical analyzes were performed using Variance Analysis (ANOVA), t tests and x² (significance p < 0.05). RESULTS: Were selected 55 patients. Fifteen (27.2%) belonged to G1, 11 (20%) belonged to G2 and 29 (52.7%) belonged to G3. The mean age of patients was 44 (G1), 50 (G2) and 56 (G3) (p = NS). The mean score APACHE II was 18 (G1), 20.4 (G2) and 20.7 (G3) (p = NS). G1 and G2 patients presented higher ICU length-of-stay (p < 0.05). The mean dose of clonidine used was 1.21 ± 0.54 mg/kg/min. G1 patients had HR and BAP decreased, however these effects were not considered clinically relevant. The mortality was lower in the patients from G1 (20%) when compared to G2 (54.5%) and G3 (62%) (p < 0.05). CONCLUSIONS: The clonidine use to analyzed patients did not result in clinical relevant side effects. The lower mortality index in patients that used clonidine was statistical significant.
-
Cardiorespiratory repercussions of the peritoneal dialysis in critically ill children
Rev Bras Ter Intensiva. 2008;20(1):31-36
Abstract
Cardiorespiratory repercussions of the peritoneal dialysis in critically ill children
Rev Bras Ter Intensiva. 2008;20(1):31-36
DOI 10.1590/S0103-507X2008000100005
Views0See moreBACKGROUND AND OBJECTIVES: Peritoneal dialysis (PD) is frequently used to replace glomerular filtration and to control acid-base, electrolyte and fluid disturbances in critically ill children with acute renal failure. However, cardiorespiratory changes can happen during this procedure. The objective of this review is to describe the PD cardio-respiratory repercutions in the pediatric patient and the evidence level of the studies that approach these repercutions. METHODS: Bibliographic revision about PD cardio-respiratory repercutions in the pediatric patient. Medline, Ovid e Lilacs databases were searched for articles from 1990 to 2007 with the following key words in Portuguese, English and Spanish: diálise peritoneal, efeitos hemodinâmicos, complicações respiratórias, complicações cardíacas, Pediatria; peritoneal dialysis, hemodynamic effects, respiratory complications, cardiac complications, Pediatric; peritoneal diálisis, efecto hemodinámico, complicaciones respiratorias, complicaciones cardiacas, Pediatria. The retrieved articles were classified according to Cook et al. 1992. RESULTS: Thirteen articles were retrieved, 8 of them were about cardiorespiratory repercussions and five approached respiratory repercussions of PD. These studies evaluated 178 critically ill patients, from newborns to adolescents. Among the respiratory repercutions during PD the most frequent ones were decrease of the pulmonary compliance and arterial oxygen partial pressure and increase of airway resistance and carbon dioxide partial pressure; after the infusion of PD fluid the studies pointed out an increased arterial oxygen partial pressure/ inspired oxygen fraction relation and diminution of the alveolar-arterial difference and oxygenation index. Increase of the mean arterial pressure, pulmonary artery pressure, right and left atrial pressure and systemic vascular resistance and, reduction of the central venous pressure were the described cardio-circulatory repercutions during PD. CONCLUSIONS: Pulmonary volumes, gas exchange and cardio-circulatory alterations are the most frequent complications during and after PD in the pediatric patient. Therefore critically ill pediatric patients with acute renal failure needing PD should be monitored during and after this procedure to avoid clinical deterioration and to educate the multi-professional team.
Views0Abstract
Cardiorespiratory repercussions of the peritoneal dialysis in critically ill children
Rev Bras Ter Intensiva. 2008;20(1):31-36
DOI 10.1590/S0103-507X2008000100005
Views0See moreBACKGROUND AND OBJECTIVES: Peritoneal dialysis (PD) is frequently used to replace glomerular filtration and to control acid-base, electrolyte and fluid disturbances in critically ill children with acute renal failure. However, cardiorespiratory changes can happen during this procedure. The objective of this review is to describe the PD cardio-respiratory repercutions in the pediatric patient and the evidence level of the studies that approach these repercutions. METHODS: Bibliographic revision about PD cardio-respiratory repercutions in the pediatric patient. Medline, Ovid e Lilacs databases were searched for articles from 1990 to 2007 with the following key words in Portuguese, English and Spanish: diálise peritoneal, efeitos hemodinâmicos, complicações respiratórias, complicações cardíacas, Pediatria; peritoneal dialysis, hemodynamic effects, respiratory complications, cardiac complications, Pediatric; peritoneal diálisis, efecto hemodinámico, complicaciones respiratorias, complicaciones cardiacas, Pediatria. The retrieved articles were classified according to Cook et al. 1992. RESULTS: Thirteen articles were retrieved, 8 of them were about cardiorespiratory repercussions and five approached respiratory repercussions of PD. These studies evaluated 178 critically ill patients, from newborns to adolescents. Among the respiratory repercutions during PD the most frequent ones were decrease of the pulmonary compliance and arterial oxygen partial pressure and increase of airway resistance and carbon dioxide partial pressure; after the infusion of PD fluid the studies pointed out an increased arterial oxygen partial pressure/ inspired oxygen fraction relation and diminution of the alveolar-arterial difference and oxygenation index. Increase of the mean arterial pressure, pulmonary artery pressure, right and left atrial pressure and systemic vascular resistance and, reduction of the central venous pressure were the described cardio-circulatory repercutions during PD. CONCLUSIONS: Pulmonary volumes, gas exchange and cardio-circulatory alterations are the most frequent complications during and after PD in the pediatric patient. Therefore critically ill pediatric patients with acute renal failure needing PD should be monitored during and after this procedure to avoid clinical deterioration and to educate the multi-professional team.
-
Best positive end expiratory pressure settlement in acute respiratory discomfort syndrome and prone position
Rev Bras Ter Intensiva. 2008;20(1):37-42
Abstract
Best positive end expiratory pressure settlement in acute respiratory discomfort syndrome and prone position
Rev Bras Ter Intensiva. 2008;20(1):37-42
DOI 10.1590/S0103-507X2008000100006
Views0See moreBACKGROUND AND OBJECTIVES: In acute respiratory discomfort syndrome (ARDS) patients, prone position improves oxygenation in more than 70% of the cases. It is well known that prone position promotes a lot of pulmonary changes, including pulmonary mechanics, so we hypothesized that there is the necessity to optimize the ventilatory parameters after the patient is placed in prone position, especially the positive end expiratory pressure (PEEP) values. The objective of this study valued the influence of the prone position at the calculation of the ideal PEEP, given a title by the best pulmonary complaisance and he compared the pulmonary alterations of mechanics, of oxygenation and of ventilation in the positions supine and prone. METHODS: Prospective study, taken place in the Irmandade Santa Casa de Misericórdia de São Paulo Intensive Care Service. Three fases have been compared. Fase 1: in supine position, after the best PEEP calculation. Fase 2: two hours after the patient was placed in prone position and the best PEEP was calculated. The patient was kept for 6 hours in this position. Fase 3: after this time, patient was placed in supine again and after two hours, a new best PEEP calculation and arterial gas analysis was done. And then fase1 versus fase 2, fase 2 versus fase 3, fase 3 versus fase1 were compared. RESULTS: There were no differences in the PEEP values found in all study fases: fase 1 = 14 ± 4.43; fase 2 = 14.73 ± 4.77 and fase 3 = 13.65 ± 4.92. CONCLUSIONS: There were no differences in best PEEP values between prone and supine position. Therefore, there is no need to recalculate the PEEP value after each position change.
Views0Abstract
Best positive end expiratory pressure settlement in acute respiratory discomfort syndrome and prone position
Rev Bras Ter Intensiva. 2008;20(1):37-42
DOI 10.1590/S0103-507X2008000100006
Views0See moreBACKGROUND AND OBJECTIVES: In acute respiratory discomfort syndrome (ARDS) patients, prone position improves oxygenation in more than 70% of the cases. It is well known that prone position promotes a lot of pulmonary changes, including pulmonary mechanics, so we hypothesized that there is the necessity to optimize the ventilatory parameters after the patient is placed in prone position, especially the positive end expiratory pressure (PEEP) values. The objective of this study valued the influence of the prone position at the calculation of the ideal PEEP, given a title by the best pulmonary complaisance and he compared the pulmonary alterations of mechanics, of oxygenation and of ventilation in the positions supine and prone. METHODS: Prospective study, taken place in the Irmandade Santa Casa de Misericórdia de São Paulo Intensive Care Service. Three fases have been compared. Fase 1: in supine position, after the best PEEP calculation. Fase 2: two hours after the patient was placed in prone position and the best PEEP was calculated. The patient was kept for 6 hours in this position. Fase 3: after this time, patient was placed in supine again and after two hours, a new best PEEP calculation and arterial gas analysis was done. And then fase1 versus fase 2, fase 2 versus fase 3, fase 3 versus fase1 were compared. RESULTS: There were no differences in the PEEP values found in all study fases: fase 1 = 14 ± 4.43; fase 2 = 14.73 ± 4.77 and fase 3 = 13.65 ± 4.92. CONCLUSIONS: There were no differences in best PEEP values between prone and supine position. Therefore, there is no need to recalculate the PEEP value after each position change.
-
Survey on Brazilian Critical Care Medicine undergraduate study groups
Rev Bras Ter Intensiva. 2008;20(1):43-48
Abstract
Survey on Brazilian Critical Care Medicine undergraduate study groups
Rev Bras Ter Intensiva. 2008;20(1):43-48
DOI 10.1590/S0103-507X2008000100007
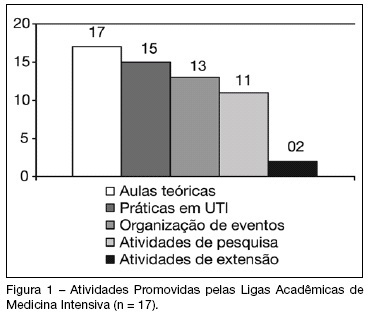
Views0See moreBACKGROUND AND OBJECTIVES: The Brazilian Intensive Care Medicine Association (AMIB) has been stimulating the creation of undergraduate associations/study groups on Critical Care Medicine (CCM), considering them a useful instrument to fill gaps in professional formation. The aim of this study was to evaluate the activities developed by CCM undergraduate study groups in Brazil. METHODS: The analyzed information was obtained on answers to a standard questionnaire. Contact by e-mail and/or telephone was made with representatives of all study groups registered on AMIB Committee of Undergraduate Study Groups on CCM (LIGAMI-AMIB) in September of 2007. In that period, there were 33 groups associated to LIGAMI, which 4 doesn’t exist anymore, 17 answered to the sent questionnaire and the remaining 12 didn’t answer the questionnaire or it was not obtained contact. RESULTS: Most study groups were founded after 2005, coinciding with the LIGAMI-AMIB Committee creation, and they are linked to one or more medical schools. Among the group’s activities, the most frequent was theoretical classes (100%), usually supplied by teachers or invited physicians (69%). Other activities include practices on Intensive Care Units (88%), organization of scientific events (77%) and research projects (65%). Most study groups (65%) had already organized some scientific event such as courses and symposia; however, only three had already accomplished the AMIB CCM Introductory Course. CONCLUSIONS: The growing number of CCM undergraduate study groups in Brazil demonstrates students’ interest for this specialty. Besides, there is a necessity of larger integration between existing groups to change experiences, cooperate in the accomplishment of research projects and participation on national and international events.
Views0Abstract
Survey on Brazilian Critical Care Medicine undergraduate study groups
Rev Bras Ter Intensiva. 2008;20(1):43-48
DOI 10.1590/S0103-507X2008000100007
Views0See moreBACKGROUND AND OBJECTIVES: The Brazilian Intensive Care Medicine Association (AMIB) has been stimulating the creation of undergraduate associations/study groups on Critical Care Medicine (CCM), considering them a useful instrument to fill gaps in professional formation. The aim of this study was to evaluate the activities developed by CCM undergraduate study groups in Brazil. METHODS: The analyzed information was obtained on answers to a standard questionnaire. Contact by e-mail and/or telephone was made with representatives of all study groups registered on AMIB Committee of Undergraduate Study Groups on CCM (LIGAMI-AMIB) in September of 2007. In that period, there were 33 groups associated to LIGAMI, which 4 doesn’t exist anymore, 17 answered to the sent questionnaire and the remaining 12 didn’t answer the questionnaire or it was not obtained contact. RESULTS: Most study groups were founded after 2005, coinciding with the LIGAMI-AMIB Committee creation, and they are linked to one or more medical schools. Among the group’s activities, the most frequent was theoretical classes (100%), usually supplied by teachers or invited physicians (69%). Other activities include practices on Intensive Care Units (88%), organization of scientific events (77%) and research projects (65%). Most study groups (65%) had already organized some scientific event such as courses and symposia; however, only three had already accomplished the AMIB CCM Introductory Course. CONCLUSIONS: The growing number of CCM undergraduate study groups in Brazil demonstrates students’ interest for this specialty. Besides, there is a necessity of larger integration between existing groups to change experiences, cooperate in the accomplishment of research projects and participation on national and international events.
-
Dopamine and noradrenaline effects in the blood flux regional on therapeutic in the septic shock
Rev Bras Ter Intensiva. 2008;20(1):49-56
Abstract
Dopamine and noradrenaline effects in the blood flux regional on therapeutic in the septic shock
Rev Bras Ter Intensiva. 2008;20(1):49-56
DOI 10.1590/S0103-507X2008000100008
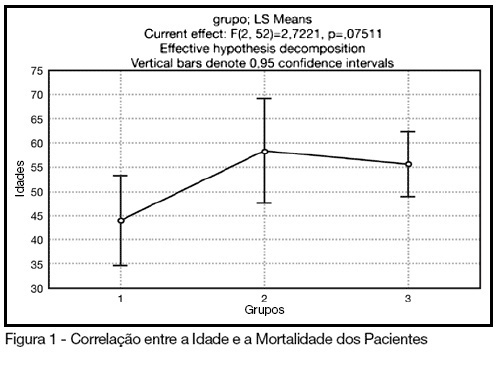
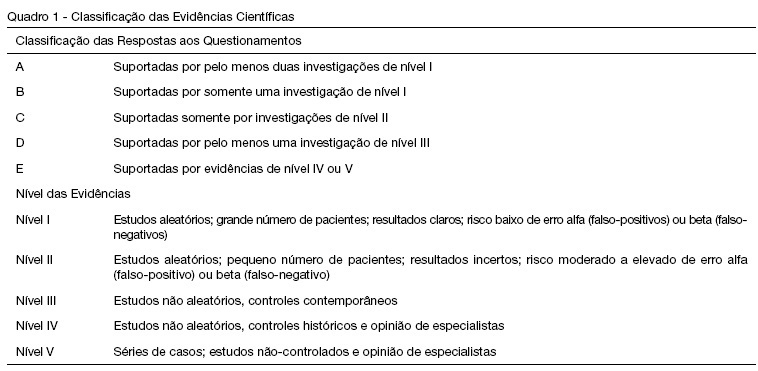
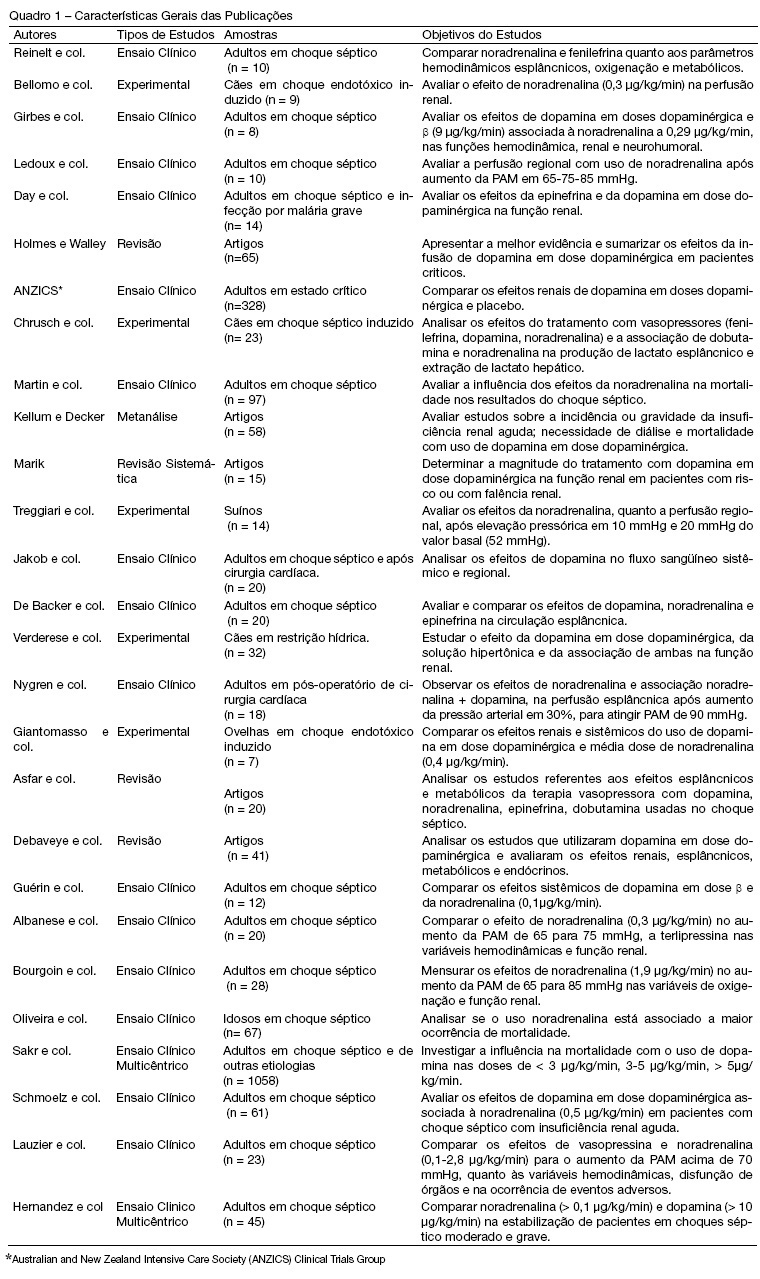
Views0See moreBACKGROUND AND OBJECTIVES: Norepinephrine and dopamine are used, in the state of shock, with the intention of offering hemodynamic support and to reestablish tissue perfusion. The pharmacological effects of these vasopressors can be diverse, for this reason, their use requires, through the clinician, an interpretation of the hemodynamic effects with observation of the systemic variations and region. With this in mind, the objective of this study was to analyze the publications regarding the effects of norepinephrine and low-dose dopamine in hepatosplenic perfusion and renal in treatment of septic shock. METHODS: Articles were selected (n = 27) concerning the use of norepinephrine and dopamine in septic shock, published during the period of 1997 to September 2007, revised in PubMed, data base of the National Library of Medicine (NLM). The MESH method was utilized with the descriptors norepinephrine, dopamine and sepsis. RESULTS: The effects of dopamine and norepinephrine in kidney perfusion are similar; there is an increase in diuresis and no change in creatinine clearance. Norepinephrine did not affect kidney tissue perfusion in spite of the increase of vascular tone. Regarding the splancnic effects, these drugs showed an increase in blood flow, though redistributing the blood in this compartment. CONCLUSIONS: The best agent for the hemodynamic reestablishment that keeps the adequate regional perfusion remains inconclusive.
Views0Abstract
Dopamine and noradrenaline effects in the blood flux regional on therapeutic in the septic shock
Rev Bras Ter Intensiva. 2008;20(1):49-56
DOI 10.1590/S0103-507X2008000100008
Views0See moreBACKGROUND AND OBJECTIVES: Norepinephrine and dopamine are used, in the state of shock, with the intention of offering hemodynamic support and to reestablish tissue perfusion. The pharmacological effects of these vasopressors can be diverse, for this reason, their use requires, through the clinician, an interpretation of the hemodynamic effects with observation of the systemic variations and region. With this in mind, the objective of this study was to analyze the publications regarding the effects of norepinephrine and low-dose dopamine in hepatosplenic perfusion and renal in treatment of septic shock. METHODS: Articles were selected (n = 27) concerning the use of norepinephrine and dopamine in septic shock, published during the period of 1997 to September 2007, revised in PubMed, data base of the National Library of Medicine (NLM). The MESH method was utilized with the descriptors norepinephrine, dopamine and sepsis. RESULTS: The effects of dopamine and norepinephrine in kidney perfusion are similar; there is an increase in diuresis and no change in creatinine clearance. Norepinephrine did not affect kidney tissue perfusion in spite of the increase of vascular tone. Regarding the splancnic effects, these drugs showed an increase in blood flow, though redistributing the blood in this compartment. CONCLUSIONS: The best agent for the hemodynamic reestablishment that keeps the adequate regional perfusion remains inconclusive.
-
Post cardiac surgery In children: extubation failure predictor’s
Rev Bras Ter Intensiva. 2008;20(1):57-62
Abstract
Post cardiac surgery In children: extubation failure predictor’s
Rev Bras Ter Intensiva. 2008;20(1):57-62
DOI 10.1590/S0103-507X2008000100009
Views0See moreBACKGROUND AND OBJECTIVES: It is important to know the risk factors for extubation failure (EF) in children submitted to cardiac surgery in order to avoid inherent events due to reintubation (airways injury, usage of medications, cardiovascular changes) and because of prolonged ventilatory support (pneumonias, reduction of the ventilatory muscles strength). The objective of this study is to evaluate mechanical ventilation (MV) parameters, ventilatory mechanics [rapid shallow breathing index (RSBI), ventilatory muscles force [the maximum inspiratory pressure (MIP), the maximum expiratory pressure (MEP) and the load/force balance (LFB)] and blood gases before and after extubation in pediatric patients undergoing cardiac surgery. METHODS: Prospective (March 2004 to March 2006) observational cross sectional study, enrolling children submitted to cardiac surgery admitted to an university PICU hospital and considered able to be extubated. With the tracheal tube in situ and maintaining the children spontaneously breathing we evaluate: expiratory minute volume (V E), MIP and MEP. We calculated the RSBI [(RR/VT)/Weight)], LFB [15x [(3xMAP)/MIP] + 0.03 x RSBI-5], the mean airway pressure (MAP) [MAP={(PIP-PEEP)x[Ti/(Te+Ti)]}+PEEP] and the oxygenation index (OI) [OI=(FiO2 x MAP/PaO2)x100]. Arterial blood gas was collected one hour before extubation. If after 48 hours there was no need to reintubate the patient the extubation was considered successful (SE). RESULTS: 59 children were included. EF was observed in 19% (11/59). Median (QI25%-75%) for age, weight, MAP, OI, duration of MV after cardiac surgery (DMV) were respectively, 36 (12-82) months, 12 (8-20) kg, 8 (6-9), 2 (2-5), 1 (1-3) days. Median (QI25-75%) of EF in relation to SE for OI, LFB and DMV were respectively 5(3-8) versus 2(2-4), p = 0.005; [8(6-11) versus 5(4-6), p =0.002 and 3(2-5) versus 1(1-2) days, p = 0.026. Mean ± SD of EF in relation to SE for V E, PaO2 and MIP were respectively 1.7 ± 0.82 versus 3 ± 2.7 mL/kg/min, p = 0.003); 64 ± 34 versus 111 ± 50 mmHg, p = 0.002 and 53 ± 18 versus 78 ± 28 cmH2O; p=0.002. Concerning the risk factors for EF: OI > 2 (area under the ROC 0.74, p = 0.017) and LFB > 4 (area under the ROC 0.80, p = 0.002), achieved a sensibility of 100% and specificity of 80%; MIP < -35 cmH2O (area under the ROC 0.23; p= 0.004) achieved a sensibility of 80% and specificity of 60%. CONCLUSIONS: EF in children submitted to cardiac surgery is related to OI > 2, LFB > 4, DMV > 3 days; V E < 1.7 mL/kg/min, PaO2 < 64 mmHg and MIP < - 53 cmH2O. The kind of cardiac defect, MAP, RSBI and arterial blood gas were not related to EF.
Views0Abstract
Post cardiac surgery In children: extubation failure predictor’s
Rev Bras Ter Intensiva. 2008;20(1):57-62
DOI 10.1590/S0103-507X2008000100009
Views0See moreBACKGROUND AND OBJECTIVES: It is important to know the risk factors for extubation failure (EF) in children submitted to cardiac surgery in order to avoid inherent events due to reintubation (airways injury, usage of medications, cardiovascular changes) and because of prolonged ventilatory support (pneumonias, reduction of the ventilatory muscles strength). The objective of this study is to evaluate mechanical ventilation (MV) parameters, ventilatory mechanics [rapid shallow breathing index (RSBI), ventilatory muscles force [the maximum inspiratory pressure (MIP), the maximum expiratory pressure (MEP) and the load/force balance (LFB)] and blood gases before and after extubation in pediatric patients undergoing cardiac surgery. METHODS: Prospective (March 2004 to March 2006) observational cross sectional study, enrolling children submitted to cardiac surgery admitted to an university PICU hospital and considered able to be extubated. With the tracheal tube in situ and maintaining the children spontaneously breathing we evaluate: expiratory minute volume (V E), MIP and MEP. We calculated the RSBI [(RR/VT)/Weight)], LFB [15x [(3xMAP)/MIP] + 0.03 x RSBI-5], the mean airway pressure (MAP) [MAP={(PIP-PEEP)x[Ti/(Te+Ti)]}+PEEP] and the oxygenation index (OI) [OI=(FiO2 x MAP/PaO2)x100]. Arterial blood gas was collected one hour before extubation. If after 48 hours there was no need to reintubate the patient the extubation was considered successful (SE). RESULTS: 59 children were included. EF was observed in 19% (11/59). Median (QI25%-75%) for age, weight, MAP, OI, duration of MV after cardiac surgery (DMV) were respectively, 36 (12-82) months, 12 (8-20) kg, 8 (6-9), 2 (2-5), 1 (1-3) days. Median (QI25-75%) of EF in relation to SE for OI, LFB and DMV were respectively 5(3-8) versus 2(2-4), p = 0.005; [8(6-11) versus 5(4-6), p =0.002 and 3(2-5) versus 1(1-2) days, p = 0.026. Mean ± SD of EF in relation to SE for V E, PaO2 and MIP were respectively 1.7 ± 0.82 versus 3 ± 2.7 mL/kg/min, p = 0.003); 64 ± 34 versus 111 ± 50 mmHg, p = 0.002 and 53 ± 18 versus 78 ± 28 cmH2O; p=0.002. Concerning the risk factors for EF: OI > 2 (area under the ROC 0.74, p = 0.017) and LFB > 4 (area under the ROC 0.80, p = 0.002), achieved a sensibility of 100% and specificity of 80%; MIP < -35 cmH2O (area under the ROC 0.23; p= 0.004) achieved a sensibility of 80% and specificity of 60%. CONCLUSIONS: EF in children submitted to cardiac surgery is related to OI > 2, LFB > 4, DMV > 3 days; V E < 1.7 mL/kg/min, PaO2 < 64 mmHg and MIP < - 53 cmH2O. The kind of cardiac defect, MAP, RSBI and arterial blood gas were not related to EF.
-
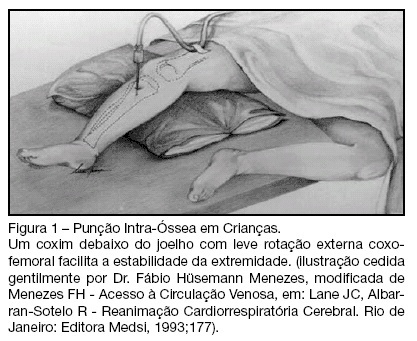
Venous access by intraosseous access in medical urgencies
Rev Bras Ter Intensiva. 2008;20(1):63-67
Abstract
Venous access by intraosseous access in medical urgencies
Rev Bras Ter Intensiva. 2008;20(1):63-67
DOI 10.1590/S0103-507X2008000100010
Views0See moreBACKGROUND AND OBJECTIVES: First introduced in 1922, the intraosseous access technique was extensively used in the 1940’s and revised in the 1980’s. Since this technique is recommended in actual cardiopulmonary resuscitation guidelines, the authors present an historical and clinical review of intraosseous access to the venous system. CONTENTS: The MedLine (1950 to January 2008) database was searched for pertinent abstracts, using the key term intraosseous access. Additional references and historical papers were obtained from the bibliographies of the articles reviewed. Manufacturer Web sites were used to obtain information about intraosseous venous (IO) insertion devices. Were identified and reviewed 231 articles, and this present article condensed the mainly the principal findings described. All available English-language clinical trials, retrospective studies and review articles describing IO drug administration were reviewed. CONCLUSIONS: The intraosseous access is used mainly to gain rapid access to the intravenous system when there is delay in obtaining the latter one. The technique is simple to learn. The complications rate is less than 1%. Most emergency drugs can be administered in the same doses used by intravenous routes. Bone access can be used in children and adults of any age in several sites. This access can be used satisfactorily to draw blood for cross-matching, blood gases and blood chemistries and emergency infusion of blood and its derivatives, saline solutions for volume replacement in shock, cardiac arrest and emergencies when an intravenous access cannot be made readily available.
Views0Abstract
Venous access by intraosseous access in medical urgencies
Rev Bras Ter Intensiva. 2008;20(1):63-67
DOI 10.1590/S0103-507X2008000100010
Views0See moreBACKGROUND AND OBJECTIVES: First introduced in 1922, the intraosseous access technique was extensively used in the 1940’s and revised in the 1980’s. Since this technique is recommended in actual cardiopulmonary resuscitation guidelines, the authors present an historical and clinical review of intraosseous access to the venous system. CONTENTS: The MedLine (1950 to January 2008) database was searched for pertinent abstracts, using the key term intraosseous access. Additional references and historical papers were obtained from the bibliographies of the articles reviewed. Manufacturer Web sites were used to obtain information about intraosseous venous (IO) insertion devices. Were identified and reviewed 231 articles, and this present article condensed the mainly the principal findings described. All available English-language clinical trials, retrospective studies and review articles describing IO drug administration were reviewed. CONCLUSIONS: The intraosseous access is used mainly to gain rapid access to the intravenous system when there is delay in obtaining the latter one. The technique is simple to learn. The complications rate is less than 1%. Most emergency drugs can be administered in the same doses used by intravenous routes. Bone access can be used in children and adults of any age in several sites. This access can be used satisfactorily to draw blood for cross-matching, blood gases and blood chemistries and emergency infusion of blood and its derivatives, saline solutions for volume replacement in shock, cardiac arrest and emergencies when an intravenous access cannot be made readily available.
-
Risks to health of intensive care unity nursing staff: proposal of integral approach of health
Rev Bras Ter Intensiva. 2008;20(1):68-76
Abstract
Risks to health of intensive care unity nursing staff: proposal of integral approach of health
Rev Bras Ter Intensiva. 2008;20(1):68-76
DOI 10.1590/S0103-507X2008000100011
Views0See moreBACKGROUND AND OBJECTIVES: In this study we discuss about risks to health of intensive care unity staff and suggest a proposal of integral approach of health. CONTENTS: Literature review, from 1997 to 2007, at Bireme database about “health education”, “intensive care unity”, “nursing” and “occupational health”, regardless of design of study. CONCLUSIONS: All studies show that the environment of intensive care unity is unhealthy, which is also due to habits and attitudes of ICU health professionals. An approach to health education would be beneficial to minimize the problem. Strategies for continuing education are appropriate both in the prevention of occupational and environmental risks in intensive care units.
Views0Abstract
Risks to health of intensive care unity nursing staff: proposal of integral approach of health
Rev Bras Ter Intensiva. 2008;20(1):68-76
DOI 10.1590/S0103-507X2008000100011
Views0See moreBACKGROUND AND OBJECTIVES: In this study we discuss about risks to health of intensive care unity staff and suggest a proposal of integral approach of health. CONTENTS: Literature review, from 1997 to 2007, at Bireme database about “health education”, “intensive care unity”, “nursing” and “occupational health”, regardless of design of study. CONCLUSIONS: All studies show that the environment of intensive care unity is unhealthy, which is also due to habits and attitudes of ICU health professionals. An approach to health education would be beneficial to minimize the problem. Strategies for continuing education are appropriate both in the prevention of occupational and environmental risks in intensive care units.
-
The use of the cuff leak test as a factor to predict laryngospasm
Rev Bras Ter Intensiva. 2008;20(1):77-81
Abstract
The use of the cuff leak test as a factor to predict laryngospasm
Rev Bras Ter Intensiva. 2008;20(1):77-81
DOI 10.1590/S0103-507X2008000100012
Views0BACKGROUND AND OBJECTIVES: Weaning patients from mechanical ventilation is a challenge in the intensive care unit (ICU) practice and is related to some complications. One of these is the pos-extubation laryngospasm, an event that can be anticipated for the cuff leak test (CLT). The objective was demonstrate that the CLT is a simple, reliable and low costs method to available the presence of obstruction in high airway in patients under weaning ventilator. CONTENTS: It was made a systematic review in databases MedLine, SciElo and LILACS with articles from 1995 to 2007. The selected studies focused the use of the CLT to predict laryngospasm and extubation failure. It was excluded studies with animals and others literature reviews. It was looked correlates the CLT with mechanical ventilation’s days, age and specific groups that could beneficiates with the application of this technique. CONCLUSIONS: The CLT can be considerate a good index to predict laryngospasm pos-extubation, when considerate the studied population characteristics.
Keywords:cuff leak testextubation failurelaryngeal edematracheal intubationweaning from mechanical ventilationSee moreViews0Abstract
The use of the cuff leak test as a factor to predict laryngospasm
Rev Bras Ter Intensiva. 2008;20(1):77-81
DOI 10.1590/S0103-507X2008000100012
Views0BACKGROUND AND OBJECTIVES: Weaning patients from mechanical ventilation is a challenge in the intensive care unit (ICU) practice and is related to some complications. One of these is the pos-extubation laryngospasm, an event that can be anticipated for the cuff leak test (CLT). The objective was demonstrate that the CLT is a simple, reliable and low costs method to available the presence of obstruction in high airway in patients under weaning ventilator. CONTENTS: It was made a systematic review in databases MedLine, SciElo and LILACS with articles from 1995 to 2007. The selected studies focused the use of the CLT to predict laryngospasm and extubation failure. It was excluded studies with animals and others literature reviews. It was looked correlates the CLT with mechanical ventilation’s days, age and specific groups that could beneficiates with the application of this technique. CONCLUSIONS: The CLT can be considerate a good index to predict laryngospasm pos-extubation, when considerate the studied population characteristics.
Keywords:cuff leak testextubation failurelaryngeal edematracheal intubationweaning from mechanical ventilationSee more -
Outcome in critically ill cancer patients: past and present
Rev Bras Ter Intensiva. 2008;20(1):82-87
Abstract
Outcome in critically ill cancer patients: past and present
Rev Bras Ter Intensiva. 2008;20(1):82-87
DOI 10.1590/S0103-507X2008000100013
Views0See moreBACKGROUND AND OBJECTIVES: Until the end of the previous century it remained controversial to admit cancer patients to the ICU for advanced-life-supporting therapy. However, over the past few years several centres over the world have shown that it is possible to achieve a meaningful survival in these patients. The aim of this review is to focus on the improvement in outcome that has been achieved over the past two decades in critically ill cancer patients. CONTENTS: We performed a MEDLINE search (period of 1980 to November 2007) to identify full-text English language publications on critically ill patients with solid tumors or hematological malignancies with particular interest for the outcome and treatment. Major MESH search terms included; cancer, solid tumor, hematologic or hematological malignancies, immunosupression, ICU, ventilation, organ failure, sepsis and infection. Additional studies were identified through a manual search of citations from retrieved articles. CONCLUSIONS: In this review, we first focus on the grim prognosis in the past, subsequently we discuss the improvements in outcome over the past few years across subgroups of cancer patients with increasing degree of severity of illness, and finally, we focus on the value of non-invasive ventilation since it is considered the initial ventilatory strategy in these patients.
Views0Abstract
Outcome in critically ill cancer patients: past and present
Rev Bras Ter Intensiva. 2008;20(1):82-87
DOI 10.1590/S0103-507X2008000100013
Views0See moreBACKGROUND AND OBJECTIVES: Until the end of the previous century it remained controversial to admit cancer patients to the ICU for advanced-life-supporting therapy. However, over the past few years several centres over the world have shown that it is possible to achieve a meaningful survival in these patients. The aim of this review is to focus on the improvement in outcome that has been achieved over the past two decades in critically ill cancer patients. CONTENTS: We performed a MEDLINE search (period of 1980 to November 2007) to identify full-text English language publications on critically ill patients with solid tumors or hematological malignancies with particular interest for the outcome and treatment. Major MESH search terms included; cancer, solid tumor, hematologic or hematological malignancies, immunosupression, ICU, ventilation, organ failure, sepsis and infection. Additional studies were identified through a manual search of citations from retrieved articles. CONCLUSIONS: In this review, we first focus on the grim prognosis in the past, subsequently we discuss the improvements in outcome over the past few years across subgroups of cancer patients with increasing degree of severity of illness, and finally, we focus on the value of non-invasive ventilation since it is considered the initial ventilatory strategy in these patients.
-
How to implement quality in palliative care at intensive care unit
Rev Bras Ter Intensiva. 2008;20(1):88-92
Abstract
How to implement quality in palliative care at intensive care unit
Rev Bras Ter Intensiva. 2008;20(1):88-92
DOI 10.1590/S0103-507X2008000100014
Views0BACKGROUND AND OBJECTIVES: Palliative care has the objective of preventing and relieving suffering by improving communication and synergism with curative therapy. This philosophy of treatment combines the patients’ values and their families and facilitates the movement in various hospital departments, which might occur with critically ill patients. CONTENTS: Though still little developed in the world, palliative care is gradually integrating curative care in intensive care units. However, various pieces of evidence have been showing that there is still a necessity to improve, especially for patients with symptoms of discomfort and pain, in intensive care environments. The patients’ families still have a poor understanding of the basic recommendations: diagnostic, prognostic and therapeutic interventions. CONCLUSIONS: Development of research in this area can promote performance indicators trying to ensure efficiency, operational quality, and constant improvement of care. This article highlights the importance of palliative medicine and proposes alternatives to promoting an appropriate time approach, bringing general medicine closer to human values.
Keywords:End-of-Life and qualityPalliative Carepatients valuePhilosophy of treatmentrelieving sufferingSee moreViews0Abstract
How to implement quality in palliative care at intensive care unit
Rev Bras Ter Intensiva. 2008;20(1):88-92
DOI 10.1590/S0103-507X2008000100014
Views0BACKGROUND AND OBJECTIVES: Palliative care has the objective of preventing and relieving suffering by improving communication and synergism with curative therapy. This philosophy of treatment combines the patients’ values and their families and facilitates the movement in various hospital departments, which might occur with critically ill patients. CONTENTS: Though still little developed in the world, palliative care is gradually integrating curative care in intensive care units. However, various pieces of evidence have been showing that there is still a necessity to improve, especially for patients with symptoms of discomfort and pain, in intensive care environments. The patients’ families still have a poor understanding of the basic recommendations: diagnostic, prognostic and therapeutic interventions. CONCLUSIONS: Development of research in this area can promote performance indicators trying to ensure efficiency, operational quality, and constant improvement of care. This article highlights the importance of palliative medicine and proposes alternatives to promoting an appropriate time approach, bringing general medicine closer to human values.
Keywords:End-of-Life and qualityPalliative Carepatients valuePhilosophy of treatmentrelieving sufferingSee more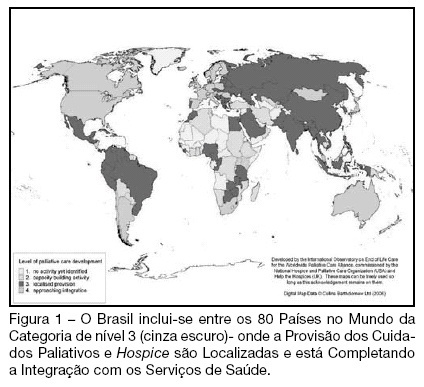
-
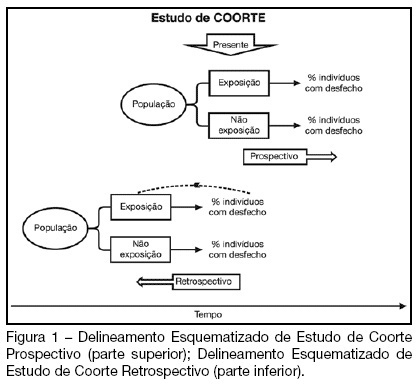
How to critically assess intensive care cohort studies?
Rev Bras Ter Intensiva. 2008;20(1):93-98
Abstract
How to critically assess intensive care cohort studies?
Rev Bras Ter Intensiva. 2008;20(1):93-98
DOI 10.1590/S0103-507X2008000100015
Views0See moreBACKGROUND AND OBJECTIVES: Cohort studies are useful to identify risk and prognostic factors, assess disease natural history and verify the impact of diagnostic or therapeutic interventions. This article aims to guide readers on how to critically assess papers using a cohort research design. CONTENTS: For a critical appraisal of cohort studies, one must observe: the existence of selection and information bias, the continuity of the follow-up, the control of confounding variables, the significance of the results and its applicability in clinical practice. CONCLUSIONS: Knowledge of factors which affect the quality of cohort studies allows intensive care professionals to select the best available evidence to guide the decision making process.
Views0Abstract
How to critically assess intensive care cohort studies?
Rev Bras Ter Intensiva. 2008;20(1):93-98
DOI 10.1590/S0103-507X2008000100015
Views0See moreBACKGROUND AND OBJECTIVES: Cohort studies are useful to identify risk and prognostic factors, assess disease natural history and verify the impact of diagnostic or therapeutic interventions. This article aims to guide readers on how to critically assess papers using a cohort research design. CONTENTS: For a critical appraisal of cohort studies, one must observe: the existence of selection and information bias, the continuity of the follow-up, the control of confounding variables, the significance of the results and its applicability in clinical practice. CONCLUSIONS: Knowledge of factors which affect the quality of cohort studies allows intensive care professionals to select the best available evidence to guide the decision making process.
-
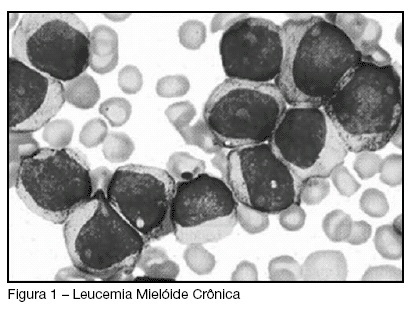
Chronicle myeloid leukemia and hiperviscosity syndrome: case report
Rev Bras Ter Intensiva. 2008;20(1):99-102
Abstract
Chronicle myeloid leukemia and hiperviscosity syndrome: case report
Rev Bras Ter Intensiva. 2008;20(1):99-102
DOI 10.1590/S0103-507X2008000100016
Views0See moreBACKGROUND AND OBJECTIVES: Hyperleukocytosis (> 100 x 10(9)/L) is an uncommon presentation of chronic leukemias and it can present clinical symptoms of hyperviscosity syndrome. Hearing loss and blindness rarely occurs in patients with leukemia; however, it can be strong association with hyper-viscosity syndrome. The purpose of this paper is to report a case of acute hearing loss as the initial manifestation of acute leukemia and hyper-viscosity syndrome and also mainly aspects of the intensive care treatment. CASE REPORT: A 41 year-old, male patient, who has been complaining about dizziness for six months with no response to symptomatic medications, was admitted to the emergency department with acute hearing loss. The physical examination was normal except for a bilateral hearing loss without an apparent cause. Laboratory exams showed total leukocyte: 645.000 with 66.4% blasts, hemoglobin: 7.0, hematocrit: 20.5, urea: 94, creatinine: 1.59, K: 5.6, Na: 138, INR: 1.38, TTPa: 0.89, troponin lower than 0.2, CK: 218, CKMB: 50, uric acid: 11.1. After a first hypothesis of leukemia with a high risk of hyper-viscosity complications, the patient was admitted to the Intensive Care Unit for monitoring and treatment. A bone marrow biopsy was performed and than started hidratation, hydroxyurea, allopurinol, dexamethasone. According to hematologists the patient had a chronic myeloid leukemia. Leukopheresis was performed one week after admission when total blood leukocytes were around 488.000. Ten days after the procedure the patient had no improvement of the hearing loss but total leukocytes were 10.100. He was discharge to the ward and 2 weeks later went home to continue ambulatory treatment. CONCLUSIONS: The frequency of sensitive manifestations in patients with leukemia include not only visual and hearing loss but also many others manifestations such as conductive vertigo, facial palsy and infections. Hyperviscosity syndrome due to hyperleukocytosis is also a possible cause of sensorial loss, but the syndrome is often dependent on leukocyte counts greater than (>100 x 10(9)/L).This case is a representative of rare cases in which acute sensorineural hearing loss occurred as the initial manifestation of hyper-viscosity syndrome due to leukemia.
Views0Abstract
Chronicle myeloid leukemia and hiperviscosity syndrome: case report
Rev Bras Ter Intensiva. 2008;20(1):99-102
DOI 10.1590/S0103-507X2008000100016
Views0See moreBACKGROUND AND OBJECTIVES: Hyperleukocytosis (> 100 x 10(9)/L) is an uncommon presentation of chronic leukemias and it can present clinical symptoms of hyperviscosity syndrome. Hearing loss and blindness rarely occurs in patients with leukemia; however, it can be strong association with hyper-viscosity syndrome. The purpose of this paper is to report a case of acute hearing loss as the initial manifestation of acute leukemia and hyper-viscosity syndrome and also mainly aspects of the intensive care treatment. CASE REPORT: A 41 year-old, male patient, who has been complaining about dizziness for six months with no response to symptomatic medications, was admitted to the emergency department with acute hearing loss. The physical examination was normal except for a bilateral hearing loss without an apparent cause. Laboratory exams showed total leukocyte: 645.000 with 66.4% blasts, hemoglobin: 7.0, hematocrit: 20.5, urea: 94, creatinine: 1.59, K: 5.6, Na: 138, INR: 1.38, TTPa: 0.89, troponin lower than 0.2, CK: 218, CKMB: 50, uric acid: 11.1. After a first hypothesis of leukemia with a high risk of hyper-viscosity complications, the patient was admitted to the Intensive Care Unit for monitoring and treatment. A bone marrow biopsy was performed and than started hidratation, hydroxyurea, allopurinol, dexamethasone. According to hematologists the patient had a chronic myeloid leukemia. Leukopheresis was performed one week after admission when total blood leukocytes were around 488.000. Ten days after the procedure the patient had no improvement of the hearing loss but total leukocytes were 10.100. He was discharge to the ward and 2 weeks later went home to continue ambulatory treatment. CONCLUSIONS: The frequency of sensitive manifestations in patients with leukemia include not only visual and hearing loss but also many others manifestations such as conductive vertigo, facial palsy and infections. Hyperviscosity syndrome due to hyperleukocytosis is also a possible cause of sensorial loss, but the syndrome is often dependent on leukocyte counts greater than (>100 x 10(9)/L).This case is a representative of rare cases in which acute sensorineural hearing loss occurred as the initial manifestation of hyper-viscosity syndrome due to leukemia.
-
Transfusion-related acute lung injury after following neurosurgery: case report
Rev Bras Ter Intensiva. 2008;20(1):103-105
Abstract
Transfusion-related acute lung injury after following neurosurgery: case report
Rev Bras Ter Intensiva. 2008;20(1):103-105
DOI 10.1590/S0103-507X2008000100017
Views0See moreBACKGROUND AND OBJECTIVES: The Transfusion-Related Acute Lung Injury (TRALI), is defined as noncardiogenic pulmonary edema temporally related to transfusion therapy, evolving with ventilation necessity mechanics in the great majority of the cases. This objective of this study was to present case of TRALI in the immediate postoperative of neurosurgery. CASE REPORT: We describe the case of a patient who presented broncoespasm and decreased oxygen saturation after to have received fresh-frozen plasma in the neurosurgery, who presented TRALI. The patient was submitted a invasive hemodynamic monitoring, sedation and supplemental oxygen with mechanical ventilation, with gradual improvement, leaving the intensive care unit in the eight day of postoperative. CONCLUSIONS: The TRALI must be investigated in the patients who receive transfusion therapy and present lung injury.
Views0Abstract
Transfusion-related acute lung injury after following neurosurgery: case report
Rev Bras Ter Intensiva. 2008;20(1):103-105
DOI 10.1590/S0103-507X2008000100017
Views0See moreBACKGROUND AND OBJECTIVES: The Transfusion-Related Acute Lung Injury (TRALI), is defined as noncardiogenic pulmonary edema temporally related to transfusion therapy, evolving with ventilation necessity mechanics in the great majority of the cases. This objective of this study was to present case of TRALI in the immediate postoperative of neurosurgery. CASE REPORT: We describe the case of a patient who presented broncoespasm and decreased oxygen saturation after to have received fresh-frozen plasma in the neurosurgery, who presented TRALI. The patient was submitted a invasive hemodynamic monitoring, sedation and supplemental oxygen with mechanical ventilation, with gradual improvement, leaving the intensive care unit in the eight day of postoperative. CONCLUSIONS: The TRALI must be investigated in the patients who receive transfusion therapy and present lung injury.
-
Trichosporon asahii an emerging etiologic agent of fungal infection and colonization in heart failure patients in intensive care unit: case report and literature review
Rev Bras Ter Intensiva. 2008;20(1):106-109
Abstract
Trichosporon asahii an emerging etiologic agent of fungal infection and colonization in heart failure patients in intensive care unit: case report and literature review
Rev Bras Ter Intensiva. 2008;20(1):106-109
DOI 10.1590/S0103-507X2008000100018
Views0See moreBACKGROUND AND OBJECTIVES: Infection with the non-Candida yeast species Trichosporon have been recognized with increasing frequency over the last two decades. Invasive disease due to trichosporonosis has been reported from neutropenic patients with cancer and the mortality is high. Recently, others groups of patients have become susceptible to this rare fungi. We report the emerging of infection with pathogenic Trichosporon asahii in severely ill heart failure patients in a tertiary cardiological intensive care unit (CICU). We describe our data, and report a fatal case of disseminated trichosporonosis in a patient with heart failure. We also review literature pertaining to T. asahii infections. CASE REPORT: An 85 year-old woman with a history of hypertension, heart failure (ejection fraction (EJ): 30%) and pulmonary embolism was admitted to a medical cardiological ICU after cardiac arrest (ventricular fibrillation) resuscitated during a routine consultation. There were no neurological sequelae and the echocardiogram revels no changes, neither the cardiac biomarkers. Ventricular fibrillation was considered secondary to heart failure. The patient had extubation failure and difficult weaning needing long term mechanical ventilation even after tracheostomy. Her hospital course was complicated by acute renal failure and recurrent respiratory, urinary and systemic bacterial infections, which responded to broad-spectrum antibiotics. After a temporary improvement she developed urinary infection and subsequent septic shock. Cultures of urine and blood specimens grew T. asahii. Treatment with liposome amphotericin B (5 mg/kg/day) was started. Despite receiving vancomycin and imipenem, the clinical condition of the patient deteriorates. Blood taken for culture on the seventh day of amphotericin B therapy were negative but urine specimen still grew T. asahii. On the eighteenth day of antifungal therapy, the patient died with multiorgan failure. CONCLUSIONS: The increasing of severely ill patients, and the use of broad spectrum antibiotics, has predisposed the emerging of invasive infections by rare and new opportunistic fungal pathogens. Severe infection related to T. asahii, until recently restricted to neutropenic patients with cancer, has been frequently identified in heart failure patients with advanced age. The mortality is high. These data highlights the importance of considering this group of patients as a risk group for T. asahii infection.
Views0Abstract
Trichosporon asahii an emerging etiologic agent of fungal infection and colonization in heart failure patients in intensive care unit: case report and literature review
Rev Bras Ter Intensiva. 2008;20(1):106-109
DOI 10.1590/S0103-507X2008000100018
Views0See moreBACKGROUND AND OBJECTIVES: Infection with the non-Candida yeast species Trichosporon have been recognized with increasing frequency over the last two decades. Invasive disease due to trichosporonosis has been reported from neutropenic patients with cancer and the mortality is high. Recently, others groups of patients have become susceptible to this rare fungi. We report the emerging of infection with pathogenic Trichosporon asahii in severely ill heart failure patients in a tertiary cardiological intensive care unit (CICU). We describe our data, and report a fatal case of disseminated trichosporonosis in a patient with heart failure. We also review literature pertaining to T. asahii infections. CASE REPORT: An 85 year-old woman with a history of hypertension, heart failure (ejection fraction (EJ): 30%) and pulmonary embolism was admitted to a medical cardiological ICU after cardiac arrest (ventricular fibrillation) resuscitated during a routine consultation. There were no neurological sequelae and the echocardiogram revels no changes, neither the cardiac biomarkers. Ventricular fibrillation was considered secondary to heart failure. The patient had extubation failure and difficult weaning needing long term mechanical ventilation even after tracheostomy. Her hospital course was complicated by acute renal failure and recurrent respiratory, urinary and systemic bacterial infections, which responded to broad-spectrum antibiotics. After a temporary improvement she developed urinary infection and subsequent septic shock. Cultures of urine and blood specimens grew T. asahii. Treatment with liposome amphotericin B (5 mg/kg/day) was started. Despite receiving vancomycin and imipenem, the clinical condition of the patient deteriorates. Blood taken for culture on the seventh day of amphotericin B therapy were negative but urine specimen still grew T. asahii. On the eighteenth day of antifungal therapy, the patient died with multiorgan failure. CONCLUSIONS: The increasing of severely ill patients, and the use of broad spectrum antibiotics, has predisposed the emerging of invasive infections by rare and new opportunistic fungal pathogens. Severe infection related to T. asahii, until recently restricted to neutropenic patients with cancer, has been frequently identified in heart failure patients with advanced age. The mortality is high. These data highlights the importance of considering this group of patients as a risk group for T. asahii infection.
Volume Articles - Critical Care Science (CCS)
