Diagnosis Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
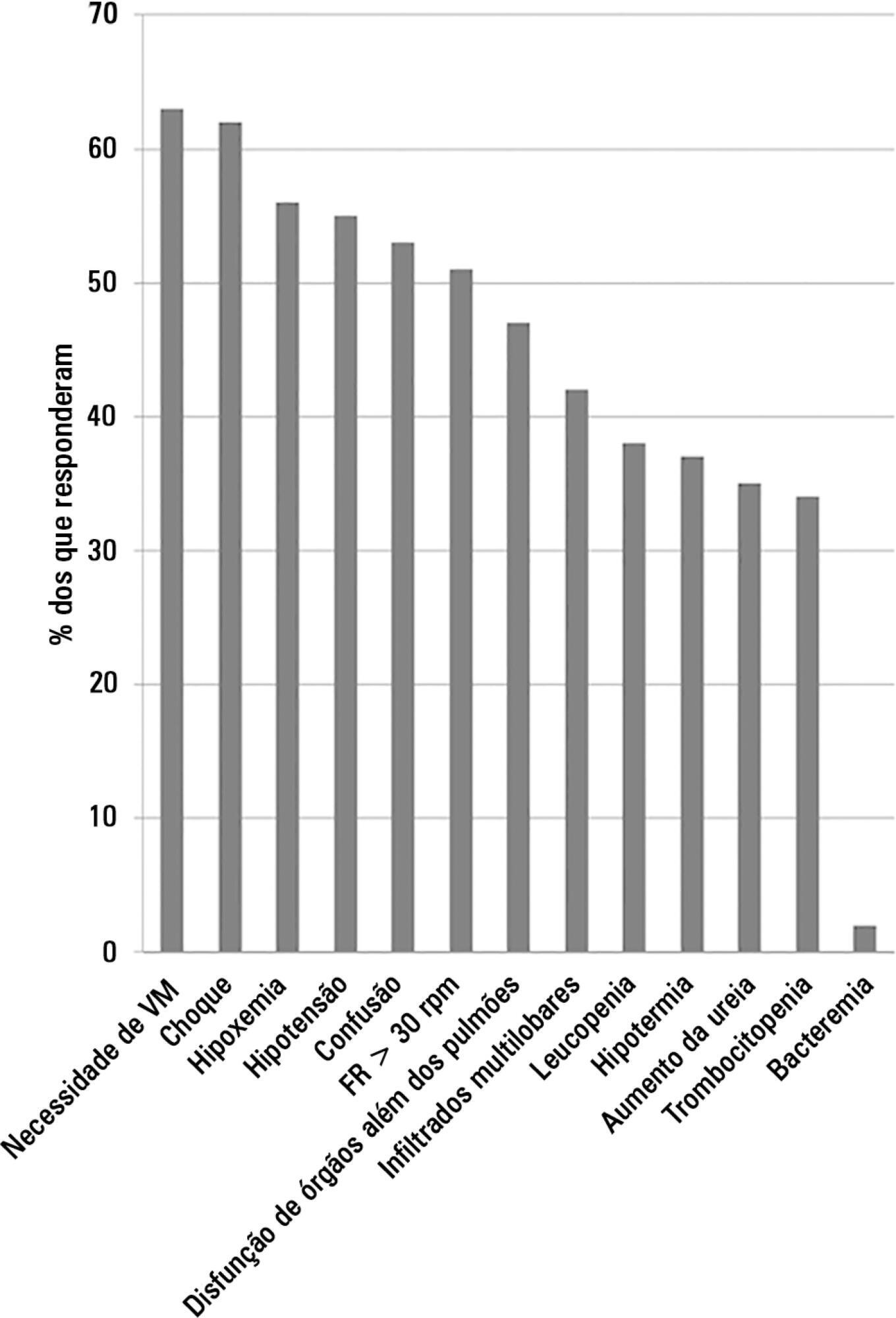
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):18-23
DOI 10.1590/S0103-507X2008000100003
BACKGROUND AND OBJECTIVES: The incidence of relative adrenal insufficiency (RAI) in patients with septic shock is high and has a significant impact on survival. The purpose of this study was to determine whether a random cortisol concentration < 25 mg/dL was as good as a low dose (1 mg) corticotrophin stimulation test in the diagnosis of RAI in patients with septic shock as assessed by the hemodynamic response to hydrocortisone. METHODS: Patients were randomized to a single cortisol determination or to a low dose corticotrophin stimulation test. After blood collection to cortisol determinations, hydrocortisone (100 mg every 8 hrs) was administered for all patients in the first 36 hours. RAI was defined by a random cortisol concentration < 25 mg/dL or a D cortisol concentration < 9 mg/dL in the corticotrophin test. RESULTS: Sixty patients (G1 = 30; G2 = 30) were included in the analysis and were comparable regarding to demographic data, nosologies and disease severity. The time to norepinephrin withdrawal in group 1 patients with RAI diagnostic criteria was not different from the patients with cortisol > 25 mg/dL. In group 2 patients with D cortisol < 9 mg/dL had a shorter time of norepinephrin infusion (3 days) compared to patients with D cortisol > 9 (6 days). CONCLUSIONS: This study suggests that 1 mg corticotrophin test is better than a random cortisol determination < 25 mg/dL to the diagnosis of relative adrenal insufficiency in septic shock patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):18-23
DOI 10.1590/S0103-507X2008000100003
BACKGROUND AND OBJECTIVES: The incidence of relative adrenal insufficiency (RAI) in patients with septic shock is high and has a significant impact on survival. The purpose of this study was to determine whether a random cortisol concentration < 25 mg/dL was as good as a low dose (1 mg) corticotrophin stimulation test in the diagnosis of RAI in patients with septic shock as assessed by the hemodynamic response to hydrocortisone. METHODS: Patients were randomized to a single cortisol determination or to a low dose corticotrophin stimulation test. After blood collection to cortisol determinations, hydrocortisone (100 mg every 8 hrs) was administered for all patients in the first 36 hours. RAI was defined by a random cortisol concentration < 25 mg/dL or a D cortisol concentration < 9 mg/dL in the corticotrophin test. RESULTS: Sixty patients (G1 = 30; G2 = 30) were included in the analysis and were comparable regarding to demographic data, nosologies and disease severity. The time to norepinephrin withdrawal in group 1 patients with RAI diagnostic criteria was not different from the patients with cortisol > 25 mg/dL. In group 2 patients with D cortisol < 9 mg/dL had a shorter time of norepinephrin infusion (3 days) compared to patients with D cortisol > 9 (6 days). CONCLUSIONS: This study suggests that 1 mg corticotrophin test is better than a random cortisol determination < 25 mg/dL to the diagnosis of relative adrenal insufficiency in septic shock patients.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)