-
Microcirculation in the intensive care unit
Rev Bras Ter Intensiva. 2011;23(3):249-251
-
From “infection in intensive care” to “intensive care in infection”: intensive care specialists’ perspective of tropical medicine
Rev Bras Ter Intensiva. 2011;23(3):252-254
-
Special Articles
Guidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
DOI 10.1590/S0103-507X2011000300003
Views0See moreThere is a relative shortage of appropriate organs available for transplantation. The appropriate diagnosis of brain death, a suitable family approach and the maintenance of the deceased donor are fundamental in addressing this issue. The intensive care physician plays a key role in the maintenance of the deceased donor, thereby reducing losses and increasing the number of successful transplants
Views0

Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
DOI 10.1590/S0103-507X2011000300003
Views0See moreThere is a relative shortage of appropriate organs available for transplantation. The appropriate diagnosis of brain death, a suitable family approach and the maintenance of the deceased donor are fundamental in addressing this issue. The intensive care physician plays a key role in the maintenance of the deceased donor, thereby reducing losses and increasing the number of successful transplants
-
Special Articles
Guidelines for potential multiple organ donors (adult): part II. Mechanical ventilation, endocrine metabolic management, hematological and infectious aspects
Rev Bras Ter Intensiva. 2011;23(3):269-282
Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part II. Mechanical ventilation, endocrine metabolic management, hematological and infectious aspects
Rev Bras Ter Intensiva. 2011;23(3):269-282
DOI 10.1590/S0103-507X2011000300004
Views0See moreThe role of intensive care specialists in the maintenance of deceased potential donors is not restricted to hemodynamics. Appropriate endocrine-metabolic management is fundamental to maintaining energy support and hydroelectrolytic control, which cooperate for hemodynamic stability. Hematological changes are also important, especially considering the issues caused by inappropriate transfusions. In addition, this article discusses the role of appropriate protective ventilation to prevent inflammatory responses and to provide more transplantable lungs. Finally, judicious assessment of infections and antibiotic therapy is discussed
Views0Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part II. Mechanical ventilation, endocrine metabolic management, hematological and infectious aspects
Rev Bras Ter Intensiva. 2011;23(3):269-282
DOI 10.1590/S0103-507X2011000300004
Views0See moreThe role of intensive care specialists in the maintenance of deceased potential donors is not restricted to hemodynamics. Appropriate endocrine-metabolic management is fundamental to maintaining energy support and hydroelectrolytic control, which cooperate for hemodynamic stability. Hematological changes are also important, especially considering the issues caused by inappropriate transfusions. In addition, this article discusses the role of appropriate protective ventilation to prevent inflammatory responses and to provide more transplantable lungs. Finally, judicious assessment of infections and antibiotic therapy is discussed
-
Original Article – Basic Research
Hemodynamic and perfusion variables during experimental septic shock treated with goal-directed fluid resuscitation
Rev Bras Ter Intensiva. 2011;23(3):283-290
Abstract
Original Article – Basic ResearchHemodynamic and perfusion variables during experimental septic shock treated with goal-directed fluid resuscitation
Rev Bras Ter Intensiva. 2011;23(3):283-290
DOI 10.1590/S0103-507X2011000300005
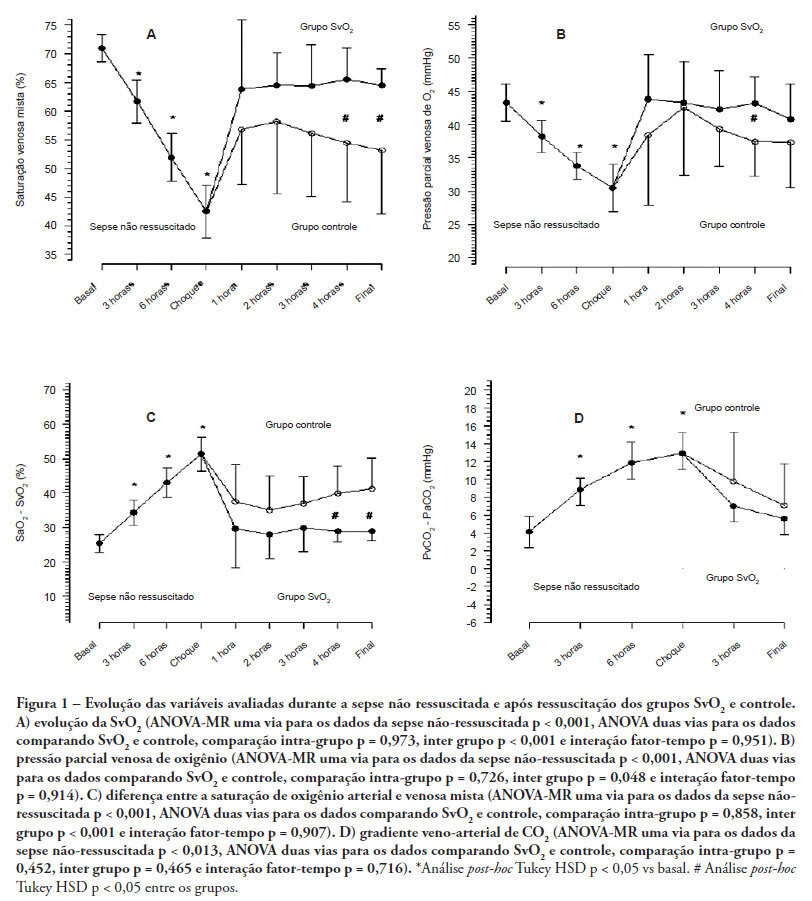
Views0See moreOBJECTIVES: Although fluid resuscitation guided by central venous oxygen saturation (SvcO2) is currently considered the gold standard in sepsis therapy, few studies have described hemodynamic and perfusion parameters during this procedure. This study aims to describe these parameters during septic shock without resuscitation and after 12 hours of goal-directed resuscitation. METHODS: Thirteen anesthetized pigs (35-45 kg) had peritonitis caused by fecal inoculation (0.75 g/kg). After developing persistent hypotension, both groups were given antibiotics and randomized either to the control group (n=7) or the experimental group (n=6). In the control group, hemodynamic control was optimized to maintain a central venous pressure of 8-12 mmHg, a urinary output above 0.5 mL/kg/hour and a mean arterial blood pressure above 65 mmHg. The experimental group received the above target therapy in addition to maintaining a SvO2 above 65%. The interventions included lactated Ringer’s solution and norepinephrine for both groups and dobutamine in the SvO2 group. The animals were treated for 12 hours or until death. RESULTS: Untreated sepsis was associated with significant reductions in SvO2, PvO2, cardiac output and central venous pressure in addition to increased arteriovenous oxygen saturation and veno-arterial CO2 differences. Following resuscitation, these parameters were corrected in both groups. Goal-directed resuscitation was associated with a better hemodynamic profile, characterized by higher SvO2, cardiac output and central venous pressure. CONCLUSIONS: Non-resuscitated sepsis showed a hemodynamic profile suggesting hypovolemia, with worsened perfusion and hemodynamics, which is reversed upon fluid resuscitation. Goal-directed resuscitation is associated with significantly improved hemodynamic and perfusion parameters
Views0Abstract
Original Article – Basic ResearchHemodynamic and perfusion variables during experimental septic shock treated with goal-directed fluid resuscitation
Rev Bras Ter Intensiva. 2011;23(3):283-290
DOI 10.1590/S0103-507X2011000300005
Views0See moreOBJECTIVES: Although fluid resuscitation guided by central venous oxygen saturation (SvcO2) is currently considered the gold standard in sepsis therapy, few studies have described hemodynamic and perfusion parameters during this procedure. This study aims to describe these parameters during septic shock without resuscitation and after 12 hours of goal-directed resuscitation. METHODS: Thirteen anesthetized pigs (35-45 kg) had peritonitis caused by fecal inoculation (0.75 g/kg). After developing persistent hypotension, both groups were given antibiotics and randomized either to the control group (n=7) or the experimental group (n=6). In the control group, hemodynamic control was optimized to maintain a central venous pressure of 8-12 mmHg, a urinary output above 0.5 mL/kg/hour and a mean arterial blood pressure above 65 mmHg. The experimental group received the above target therapy in addition to maintaining a SvO2 above 65%. The interventions included lactated Ringer’s solution and norepinephrine for both groups and dobutamine in the SvO2 group. The animals were treated for 12 hours or until death. RESULTS: Untreated sepsis was associated with significant reductions in SvO2, PvO2, cardiac output and central venous pressure in addition to increased arteriovenous oxygen saturation and veno-arterial CO2 differences. Following resuscitation, these parameters were corrected in both groups. Goal-directed resuscitation was associated with a better hemodynamic profile, characterized by higher SvO2, cardiac output and central venous pressure. CONCLUSIONS: Non-resuscitated sepsis showed a hemodynamic profile suggesting hypovolemia, with worsened perfusion and hemodynamics, which is reversed upon fluid resuscitation. Goal-directed resuscitation is associated with significantly improved hemodynamic and perfusion parameters
-
Original Articles – Clinical Research
The impact of positive end-expiratory pressure on cerebral perfusion pressure in adult patients with hemorrhagic stroke
Rev Bras Ter Intensiva. 2011;23(3):291-296
Abstract
Original Articles – Clinical ResearchThe impact of positive end-expiratory pressure on cerebral perfusion pressure in adult patients with hemorrhagic stroke
Rev Bras Ter Intensiva. 2011;23(3):291-296
DOI 10.1590/S0103-507X2011000300006
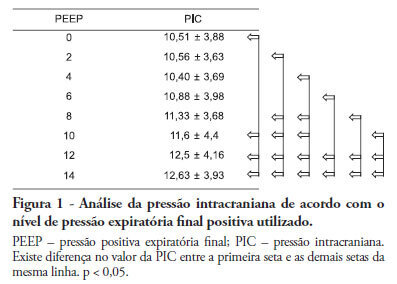
Views0See morePositive intrathoracic pressure may cause hemodynamic changes, which can be transmitted to the cranial compartment, changing intracranial pressure and cerebral perfusion pressure. This can be increased when high positive end-expiratory pressure values are used. OBJECTIVE: To measure the impact of different positive end-expiratory pressure levels on intracranial pressure, cerebral perfusion pressure and mean blood pressure. METHOD: This study was conducted in a neurological intensive care unit and included 25 adult hemorrhagic stroke patients who were mechanically ventilated on airway pressure control mode. Patients were subjected to various positive end-expiratory values ranging between 0 and 14 cmH2O. The order of these values were randomized, and the variables were assessed five minutes after each new positive end-expiratory pressure level was initiated. RESULTS: Incremental positive end-expiratory pressures led to increased intracranial pressure (p < 0.001), however, no statistically significant changes were observed in mean blood pressure or cerebral perfusion pressure. CONCLUSION: In this population of patients with hemorrhagic stroke, positive end-expiratory pressure values up to 14 cmH2O did not alter cerebral perfusion pressure or mean blood pressure. Increased intracranial pressures were noted, although these elevations were not clinically significant
Views0Abstract
Original Articles – Clinical ResearchThe impact of positive end-expiratory pressure on cerebral perfusion pressure in adult patients with hemorrhagic stroke
Rev Bras Ter Intensiva. 2011;23(3):291-296
DOI 10.1590/S0103-507X2011000300006
Views0See morePositive intrathoracic pressure may cause hemodynamic changes, which can be transmitted to the cranial compartment, changing intracranial pressure and cerebral perfusion pressure. This can be increased when high positive end-expiratory pressure values are used. OBJECTIVE: To measure the impact of different positive end-expiratory pressure levels on intracranial pressure, cerebral perfusion pressure and mean blood pressure. METHOD: This study was conducted in a neurological intensive care unit and included 25 adult hemorrhagic stroke patients who were mechanically ventilated on airway pressure control mode. Patients were subjected to various positive end-expiratory values ranging between 0 and 14 cmH2O. The order of these values were randomized, and the variables were assessed five minutes after each new positive end-expiratory pressure level was initiated. RESULTS: Incremental positive end-expiratory pressures led to increased intracranial pressure (p < 0.001), however, no statistically significant changes were observed in mean blood pressure or cerebral perfusion pressure. CONCLUSION: In this population of patients with hemorrhagic stroke, positive end-expiratory pressure values up to 14 cmH2O did not alter cerebral perfusion pressure or mean blood pressure. Increased intracranial pressures were noted, although these elevations were not clinically significant
-
Original Articles – Clinical Research
Gender and mortality in sepsis: do sex hormones impact the outcome?
Rev Bras Ter Intensiva. 2011;23(3):297-303
Abstract
Original Articles – Clinical ResearchGender and mortality in sepsis: do sex hormones impact the outcome?
Rev Bras Ter Intensiva. 2011;23(3):297-303
DOI 10.1590/S0103-507X2011000300007
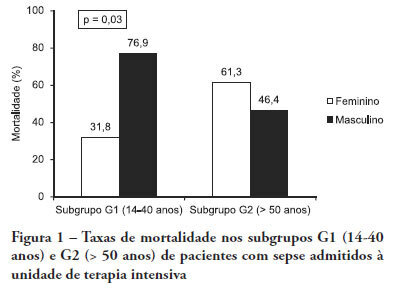
Views0See moreOBJECTIVE: Comparative assessment of the mortality rates of two septic patients’ ages and/or gender subgroups, admitted to the intensive care unit of a university hospital. METHODS: From December 2005 to April 2008, from a total of 628 patients, 133 were admitted to the intensive care unit with sepsis and included into two age subgroups: (G1) 14 – 40 years old and (G2) more than 50 years old. Patients aged between 41 and 50 years old (n = 8) were excluded. Demographic data, prognostic indicators (APACHE II score, organ dysfunction and circulatory shock) and outcome (mortality) were analyzed. RESULTS: Of the G1 patients (n = 44), 27 were female (61.4%), and in G2 (n = 81), 40 were female (49.4%). For both groups, mean APACHE II scores, multi-organ dysfunction and progression to circulatory shock rates were not significantly different between female and male patients. For G1, overall mortality rate was lower in female than in male patients (P = 0.04), while for G2, the opposite trend was observed. CONCLUSIONS: In this sample, reproductive age female patients younger than 40 years old showed lower mortality rates compared with age-matched male patients; for patients older than 50 years old, male patients had lower mortality rates than female patients.
Views0Abstract
Original Articles – Clinical ResearchGender and mortality in sepsis: do sex hormones impact the outcome?
Rev Bras Ter Intensiva. 2011;23(3):297-303
DOI 10.1590/S0103-507X2011000300007
Views0See moreOBJECTIVE: Comparative assessment of the mortality rates of two septic patients’ ages and/or gender subgroups, admitted to the intensive care unit of a university hospital. METHODS: From December 2005 to April 2008, from a total of 628 patients, 133 were admitted to the intensive care unit with sepsis and included into two age subgroups: (G1) 14 – 40 years old and (G2) more than 50 years old. Patients aged between 41 and 50 years old (n = 8) were excluded. Demographic data, prognostic indicators (APACHE II score, organ dysfunction and circulatory shock) and outcome (mortality) were analyzed. RESULTS: Of the G1 patients (n = 44), 27 were female (61.4%), and in G2 (n = 81), 40 were female (49.4%). For both groups, mean APACHE II scores, multi-organ dysfunction and progression to circulatory shock rates were not significantly different between female and male patients. For G1, overall mortality rate was lower in female than in male patients (P = 0.04), while for G2, the opposite trend was observed. CONCLUSIONS: In this sample, reproductive age female patients younger than 40 years old showed lower mortality rates compared with age-matched male patients; for patients older than 50 years old, male patients had lower mortality rates than female patients.
-
Original Articles – Clinical Research
Postoperative complications of surgically treated ascending aortic dissection
Rev Bras Ter Intensiva. 2011;23(3):304-311
Abstract
Original Articles – Clinical ResearchPostoperative complications of surgically treated ascending aortic dissection
Rev Bras Ter Intensiva. 2011;23(3):304-311
DOI 10.1590/S0103-507X2011000300008
Views0See moreOBJECTIVES: Ascending aortic dissection has a poor prognosis if it is not promptly corrected surgically. Even with surgical correction, postoperative management is feared because of its complicated course. Our aim was to describe the incidence of postoperative complications and identify the 1 and 6-month mortality rate of our ascending aortic dissection surgical cohort. Secondarily, a comparison was made between ascending aortic dissection patients and paired-matched patients who received urgent coronary artery bypass graft surgery. METHODS: A retrospective analysis of a prospectively-collected database from February 2005 through June 2008 revealed 12 ascending aortic dissection and 10 elective ascending aortic aneurysm repair patients. These patients were analyzed for demographic and perioperative characteristics. Ascending aortic dissection patients were compared to paired-matched coronary artery bypass graft surgery patients according to age (± 3 years), gender, elective/urgent procedure and surgical team. The main outcome was in-hospital morbidity, defined by postoperative complications, intensive care unit admission and hospital length of stay. RESULTS: Twenty-two patients received operations to correct ascending aortic dissections and ascending aortic aneurysms, while 246 patients received coronary artery bypass graft surgeries. Ascending aortic dissection patients were notably similar to ascending aortic aneurysm brackets, except for longer mechanical ventilation times and lengths of stay in the hospital. After matching coronary artery bypass graft surgery patients to an ascending aortic dissection group, the following significantly worse results were found for the Aorta group: higher incidence of postoperative complications (91% vs. 45%, p=0.03), and longer hospital length of stay (19 [11-41] vs. 12.5 [8.5-13] days, p=0.05). No difference in mortality was found at the 1-month (8.3%) or 6-month (16.6%) postoperative care date. CONCLUSION: Ascending aortic dissection correction is associated with an increased incidence of postoperative complications and an increased hospital length of stay, but 1 and 6-month mortality is similar to that of paired-matched coronary artery bypass graft surgery patients.
Views0Abstract
Original Articles – Clinical ResearchPostoperative complications of surgically treated ascending aortic dissection
Rev Bras Ter Intensiva. 2011;23(3):304-311
DOI 10.1590/S0103-507X2011000300008
Views0See moreOBJECTIVES: Ascending aortic dissection has a poor prognosis if it is not promptly corrected surgically. Even with surgical correction, postoperative management is feared because of its complicated course. Our aim was to describe the incidence of postoperative complications and identify the 1 and 6-month mortality rate of our ascending aortic dissection surgical cohort. Secondarily, a comparison was made between ascending aortic dissection patients and paired-matched patients who received urgent coronary artery bypass graft surgery. METHODS: A retrospective analysis of a prospectively-collected database from February 2005 through June 2008 revealed 12 ascending aortic dissection and 10 elective ascending aortic aneurysm repair patients. These patients were analyzed for demographic and perioperative characteristics. Ascending aortic dissection patients were compared to paired-matched coronary artery bypass graft surgery patients according to age (± 3 years), gender, elective/urgent procedure and surgical team. The main outcome was in-hospital morbidity, defined by postoperative complications, intensive care unit admission and hospital length of stay. RESULTS: Twenty-two patients received operations to correct ascending aortic dissections and ascending aortic aneurysms, while 246 patients received coronary artery bypass graft surgeries. Ascending aortic dissection patients were notably similar to ascending aortic aneurysm brackets, except for longer mechanical ventilation times and lengths of stay in the hospital. After matching coronary artery bypass graft surgery patients to an ascending aortic dissection group, the following significantly worse results were found for the Aorta group: higher incidence of postoperative complications (91% vs. 45%, p=0.03), and longer hospital length of stay (19 [11-41] vs. 12.5 [8.5-13] days, p=0.05). No difference in mortality was found at the 1-month (8.3%) or 6-month (16.6%) postoperative care date. CONCLUSION: Ascending aortic dissection correction is associated with an increased incidence of postoperative complications and an increased hospital length of stay, but 1 and 6-month mortality is similar to that of paired-matched coronary artery bypass graft surgery patients.
-
Original Articles – Clinical Research
Complications and hospital length of stay in coronary artery bypass graft surgery in public hospitals in Rio de Janeiro
Rev Bras Ter Intensiva. 2011;23(3):312-320
Abstract
Original Articles – Clinical ResearchComplications and hospital length of stay in coronary artery bypass graft surgery in public hospitals in Rio de Janeiro
Rev Bras Ter Intensiva. 2011;23(3):312-320
DOI 10.1590/S0103-507X2011000300009
Views0OBJECTIVE: To evaluate associations between post-operative complications in patients who survive surgery and in-hospital deaths and lengths of hospital stays of patients who undergo coronary artery bypass graft surgery METHODS: Patients who underwent coronary artery bypass graft surgery and survived the operating theater were randomly selected. Information on complications and hospital lengths of stay until hospital discharge or death were retrospectively collected based on medical records and declarations of death. These aspects were estimated according to the presence of complications, frequency of complications, mortality, relative risk and attributable population risk. Mean hospital lengths of stay were compared using Wald’s statistics. RESULTS: Medical records indicating deaths in the operating theater were excluded, and 86.9% of the included records reported complications; the greatest loss of information (43.9%) was related to kidney failure. Hyperglycemia was estimated as the most frequent complication (74.6%), with an attributable risk of 31.6%. The population’s attributable risks were greater than 60% for low cardiac output (77.0%), kidney failure (64.3%) and cardiorespiratory failure (60.4%). Twelve different situations were identified for paired combinations of significant differences between average post-operative hospitalization times and complications, according to the outcome of discharge or death. CONCLUSION: Several complications were identified during the postoperative period of coronary artery bypass graft surgery, with different frequencies and impacts on mortality. Control of the myocardium at the risk of ischemia, hemodynamic stabilization and volume replacement strategies may be effective for controlling mortality rates and shortening hospital lengths of stay.
Keywords:Cardiac surgical proceduresLength of stayMortalityMyocardial revascularizationPostoperative complicationsSee moreViews0Abstract
Original Articles – Clinical ResearchComplications and hospital length of stay in coronary artery bypass graft surgery in public hospitals in Rio de Janeiro
Rev Bras Ter Intensiva. 2011;23(3):312-320
DOI 10.1590/S0103-507X2011000300009
Views0OBJECTIVE: To evaluate associations between post-operative complications in patients who survive surgery and in-hospital deaths and lengths of hospital stays of patients who undergo coronary artery bypass graft surgery METHODS: Patients who underwent coronary artery bypass graft surgery and survived the operating theater were randomly selected. Information on complications and hospital lengths of stay until hospital discharge or death were retrospectively collected based on medical records and declarations of death. These aspects were estimated according to the presence of complications, frequency of complications, mortality, relative risk and attributable population risk. Mean hospital lengths of stay were compared using Wald’s statistics. RESULTS: Medical records indicating deaths in the operating theater were excluded, and 86.9% of the included records reported complications; the greatest loss of information (43.9%) was related to kidney failure. Hyperglycemia was estimated as the most frequent complication (74.6%), with an attributable risk of 31.6%. The population’s attributable risks were greater than 60% for low cardiac output (77.0%), kidney failure (64.3%) and cardiorespiratory failure (60.4%). Twelve different situations were identified for paired combinations of significant differences between average post-operative hospitalization times and complications, according to the outcome of discharge or death. CONCLUSION: Several complications were identified during the postoperative period of coronary artery bypass graft surgery, with different frequencies and impacts on mortality. Control of the myocardium at the risk of ischemia, hemodynamic stabilization and volume replacement strategies may be effective for controlling mortality rates and shortening hospital lengths of stay.
Keywords:Cardiac surgical proceduresLength of stayMortalityMyocardial revascularizationPostoperative complicationsSee more -
Original Articles – Clinical Research
Acute kidney injury in intensive care unit patients: a prospective study on incidence, risk factors and
Rev Bras Ter Intensiva. 2011;23(3):321-326
Abstract
Original Articles – Clinical ResearchAcute kidney injury in intensive care unit patients: a prospective study on incidence, risk factors and
Rev Bras Ter Intensiva. 2011;23(3):321-326
DOI 10.1590/S0103-507X2011000300010
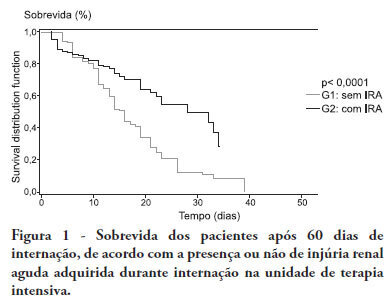
Views0See moreOBJECTIVE:To compare the clinical features and outcomes of patients with and without acute kidney injury in an intensive care unit of a tertiary university hospital and to identify acute kidney injury and mortality risk factors. METHODS: This was a prospective observational study of a cohort including 564 patients followed during their stay in the intensive care unit of Hospital das Clinicas da Faculdade de Medicina de Botucatu (Botucatu, São Paulo, Brazil) between May 2008 and May 2010. Patients were allocated to two different groups: with (G1) and without (G2) acute kidney injury. RESULTS: The incidence of acute kidney injury was 25.5%. The groups were different with respect to the reason for admission to the intensive care unit (sepsis, G1: 41.6% versus G2: 24.1%; P < 0.0001; neurosurgery, postoperative G1: 13.8% versus G2: 38.1%; P < 0.0001); age (G1: 56.8 ± 15.9 vs. G2: 49.8 ± 17.8 years; P < 0.0001); Acute Physiological Chronic Health Evaluation (APACHE) II score (G1: 21.9 ± 6.9 versus G2: 14.1 ± 4.6; P < 0.0001); use of mechanical ventilation (G1: 89.2% vs. G2: 69.1%; P < 0.0001) and use of vasoactive drugs (G1: 78.3% vs. G2: 56.1%; P < 0.0001). Higher rates of diabetes mellitus, congestive heart failure, chronic renal disease and use of non-steroidal anti-inflammatory drugs were more frequent in acute kidney injury patients (28.2% vs. 19.7%, P = 0.03; 23.6 vs. 11.6%, P = 0.0002; 21.5% vs. 11.5%, P < 0.0001 and 23.5% vs. 71.%, P < 0.0001, for G1 versus G2, respectively). Length of hospital stay and mortality were also higher for acute kidney injury patients (G1: 6.6 ± 2.7 days versus G2: 12.9 ±5.6 days, P < 0.0001 and G1: 62.5% versus G2: 16.4%, P < 0.0001). Multivariate analysis identified the following as risk factors for acute kidney injury: age above 55 years, APACHE II score above 16, baseline creatinine above 1.2 and use of non-steroidal anti-inflammatory drugs (odds ratio (OR) = 1.36, 95% confidence interval (95%CI): 1.22 - 1.85; OR = 1.2, 95%CI: 1.11 - 1.33; OR = 5.2, 95%CI: 2.3 - 11.6 and OR = 2.15, 95%CI: 1.1 - 4.2, respectively). Acute kidney injury was independently associated with longer hospital stay and increased mortality (OR = 1.18, 95%CI: 1.05 - 1.26 and OR = 1.24, 95%CI: 1.09 - 1.99, respectively). Analysis of the survival curve 30 days after admission showed 83.3% mortality for acute kidney injury patients and 45.2% for non-acute kidney injury patients (P < 0.0001). CONCLUSION: The incidence of acute kidney injury was high in this intensive care unit; the independent risk factors associated with acute kidney injury were age > 55 years, APACHE II > 16, baseline serum creatinine > 1.2 and use of non-steroidal anti-inflammatory drugs. Acute kidney injury is an independent risk factor for longer intensive care unit stay and mortality.
Views0Abstract
Original Articles – Clinical ResearchAcute kidney injury in intensive care unit patients: a prospective study on incidence, risk factors and
Rev Bras Ter Intensiva. 2011;23(3):321-326
DOI 10.1590/S0103-507X2011000300010
Views0See moreOBJECTIVE:To compare the clinical features and outcomes of patients with and without acute kidney injury in an intensive care unit of a tertiary university hospital and to identify acute kidney injury and mortality risk factors. METHODS: This was a prospective observational study of a cohort including 564 patients followed during their stay in the intensive care unit of Hospital das Clinicas da Faculdade de Medicina de Botucatu (Botucatu, São Paulo, Brazil) between May 2008 and May 2010. Patients were allocated to two different groups: with (G1) and without (G2) acute kidney injury. RESULTS: The incidence of acute kidney injury was 25.5%. The groups were different with respect to the reason for admission to the intensive care unit (sepsis, G1: 41.6% versus G2: 24.1%; P < 0.0001; neurosurgery, postoperative G1: 13.8% versus G2: 38.1%; P < 0.0001); age (G1: 56.8 ± 15.9 vs. G2: 49.8 ± 17.8 years; P < 0.0001); Acute Physiological Chronic Health Evaluation (APACHE) II score (G1: 21.9 ± 6.9 versus G2: 14.1 ± 4.6; P < 0.0001); use of mechanical ventilation (G1: 89.2% vs. G2: 69.1%; P < 0.0001) and use of vasoactive drugs (G1: 78.3% vs. G2: 56.1%; P < 0.0001). Higher rates of diabetes mellitus, congestive heart failure, chronic renal disease and use of non-steroidal anti-inflammatory drugs were more frequent in acute kidney injury patients (28.2% vs. 19.7%, P = 0.03; 23.6 vs. 11.6%, P = 0.0002; 21.5% vs. 11.5%, P < 0.0001 and 23.5% vs. 71.%, P < 0.0001, for G1 versus G2, respectively). Length of hospital stay and mortality were also higher for acute kidney injury patients (G1: 6.6 ± 2.7 days versus G2: 12.9 ±5.6 days, P < 0.0001 and G1: 62.5% versus G2: 16.4%, P < 0.0001). Multivariate analysis identified the following as risk factors for acute kidney injury: age above 55 years, APACHE II score above 16, baseline creatinine above 1.2 and use of non-steroidal anti-inflammatory drugs (odds ratio (OR) = 1.36, 95% confidence interval (95%CI): 1.22 - 1.85; OR = 1.2, 95%CI: 1.11 - 1.33; OR = 5.2, 95%CI: 2.3 - 11.6 and OR = 2.15, 95%CI: 1.1 - 4.2, respectively). Acute kidney injury was independently associated with longer hospital stay and increased mortality (OR = 1.18, 95%CI: 1.05 - 1.26 and OR = 1.24, 95%CI: 1.09 - 1.99, respectively). Analysis of the survival curve 30 days after admission showed 83.3% mortality for acute kidney injury patients and 45.2% for non-acute kidney injury patients (P < 0.0001). CONCLUSION: The incidence of acute kidney injury was high in this intensive care unit; the independent risk factors associated with acute kidney injury were age > 55 years, APACHE II > 16, baseline serum creatinine > 1.2 and use of non-steroidal anti-inflammatory drugs. Acute kidney injury is an independent risk factor for longer intensive care unit stay and mortality.
-
Original Articles – Clinical Research
Effectiveness of a noise control program in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2011;23(3):327-334
Abstract
Original Articles – Clinical ResearchEffectiveness of a noise control program in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2011;23(3):327-334
DOI 10.1590/S0103-507X2011000300011
Views0See morePURPOSE: To evaluate the effectiveness of a noise control program in the Neonatal Intensive Care Unit of the Hospital Universitário Santa Maria (NICU-HUSM) in Santa Maria, Rio Grande do Sul, Brazil. METHODS: NICU-HUSM professionals were initially contacted through informal interviews during the morning, afternoon and night shifts. Leaflets were delivered and posters were installed to raise awareness of the harmful effects of noise on neonates and professionals and to suggest behavioral changes to reduce noise levels. The suggestions included avoiding loud talking, careful handling of the incubator doors and keeping mobile phones on silent mode. One month later, questionnaires were used to assess behavioral changes since the first contact. RESULTS: Most of the professionals rated the NICU-HUSM noise level as moderate. Overall, 71.4% of the respondents acknowledged that their behaviors were noisy. The entire sample reported believing that the unit noise levels could be reduced by speaking lower, reacting more quickly to alarms and handling furniture more carefully. The NICU professionals reported adopting these behaviors. CONCLUSION: This noise control program was considered successful because the professionals became aware of the level of noise and adopted behavioral changes to avoid generating unnecessary noise.
Views0Abstract
Original Articles – Clinical ResearchEffectiveness of a noise control program in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2011;23(3):327-334
DOI 10.1590/S0103-507X2011000300011
Views0See morePURPOSE: To evaluate the effectiveness of a noise control program in the Neonatal Intensive Care Unit of the Hospital Universitário Santa Maria (NICU-HUSM) in Santa Maria, Rio Grande do Sul, Brazil. METHODS: NICU-HUSM professionals were initially contacted through informal interviews during the morning, afternoon and night shifts. Leaflets were delivered and posters were installed to raise awareness of the harmful effects of noise on neonates and professionals and to suggest behavioral changes to reduce noise levels. The suggestions included avoiding loud talking, careful handling of the incubator doors and keeping mobile phones on silent mode. One month later, questionnaires were used to assess behavioral changes since the first contact. RESULTS: Most of the professionals rated the NICU-HUSM noise level as moderate. Overall, 71.4% of the respondents acknowledged that their behaviors were noisy. The entire sample reported believing that the unit noise levels could be reduced by speaking lower, reacting more quickly to alarms and handling furniture more carefully. The NICU professionals reported adopting these behaviors. CONCLUSION: This noise control program was considered successful because the professionals became aware of the level of noise and adopted behavioral changes to avoid generating unnecessary noise.
-
Original Articles – Clinical Research
Intermittent heparin is not effective at preventing the occlusion of peripherally inserted central venous catheters in preterm and term neonates
Rev Bras Ter Intensiva. 2011;23(3):335-340
Abstract
Original Articles – Clinical ResearchIntermittent heparin is not effective at preventing the occlusion of peripherally inserted central venous catheters in preterm and term neonates
Rev Bras Ter Intensiva. 2011;23(3):335-340
DOI 10.1590/S0103-507X2011000300012
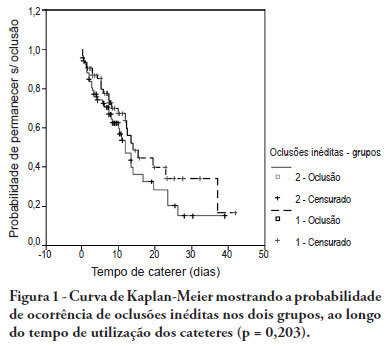
Views0See moreOBJECTIVE: To evaluate the effectiveness of intermittent 10 U/mL heparin flushes in reducing the occlusion of peripherally inserted central catheters in neonates. METHODS: In this randomized, open-label, prospective, controlled study, neonates were allocated either to receive 0.5 mL flushes of heparin (Group 1: n = 64) or saline (Group 2: n = 69) every 4 hours. Actions were taken to restore patency by using negative pressure (3-way stopcock method) in cases of occlusion. RESULTS: A total of 133 neonates were included. No significant intergroup difference was observed in the number of new occlusions (26 in Group 1, or 31/1,000 catheter-days; 36 in Group 2, or 36/1,000 catheter-days; P = 0.19). In Group 1, 5 catheters had 9 recurrent obstructions after successful clearance maneuvers. In Group 2, 19 catheters had 40 relapses (P < 0.0001), showing heparin's protective role against recurrence of obstruction (Relative Risk = 0.36). However, heparin failed to prevent catheter withdrawal due to permanent occlusion (3 catheters in Group 1 and 8 in Group 2; P = 0.24). CONCLUSION: Intermittent heparin is not effective for preventing the occlusion of peripherally inserted central catheters in neonates but reduces relapses when clearance maneuvers were successful
Views0Abstract
Original Articles – Clinical ResearchIntermittent heparin is not effective at preventing the occlusion of peripherally inserted central venous catheters in preterm and term neonates
Rev Bras Ter Intensiva. 2011;23(3):335-340
DOI 10.1590/S0103-507X2011000300012
Views0See moreOBJECTIVE: To evaluate the effectiveness of intermittent 10 U/mL heparin flushes in reducing the occlusion of peripherally inserted central catheters in neonates. METHODS: In this randomized, open-label, prospective, controlled study, neonates were allocated either to receive 0.5 mL flushes of heparin (Group 1: n = 64) or saline (Group 2: n = 69) every 4 hours. Actions were taken to restore patency by using negative pressure (3-way stopcock method) in cases of occlusion. RESULTS: A total of 133 neonates were included. No significant intergroup difference was observed in the number of new occlusions (26 in Group 1, or 31/1,000 catheter-days; 36 in Group 2, or 36/1,000 catheter-days; P = 0.19). In Group 1, 5 catheters had 9 recurrent obstructions after successful clearance maneuvers. In Group 2, 19 catheters had 40 relapses (P < 0.0001), showing heparin's protective role against recurrence of obstruction (Relative Risk = 0.36). However, heparin failed to prevent catheter withdrawal due to permanent occlusion (3 catheters in Group 1 and 8 in Group 2; P = 0.24). CONCLUSION: Intermittent heparin is not effective for preventing the occlusion of peripherally inserted central catheters in neonates but reduces relapses when clearance maneuvers were successful
-
Review Articles
Near-infrared spectroscopy for monitoring peripheral tissue perfusion in critically ill patients
Rev Bras Ter Intensiva. 2011;23(3):341-351
Abstract
Review ArticlesNear-infrared spectroscopy for monitoring peripheral tissue perfusion in critically ill patients
Rev Bras Ter Intensiva. 2011;23(3):341-351
DOI 10.1590/S0103-507X2011000300013
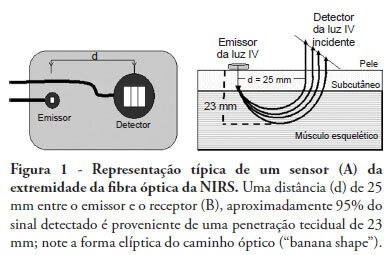
Views0See moreNear infrared spectroscopy (NIRS) is a non-invasive technique that allows determination of tissue oxygenation based on spectro-photometric quantitation of oxy- and deoxyhemoglobin within a tissue. This technique has gained acceptance as a tool to monitor peripheral tissue perfusion in critically ill patient. NIRS principle is based on the use of near-infrared electromagnetic waves for qualitative and quantitative assessments of molecular factors related to tissue oxygenation. Although this technique can be apllied in any tissue, it is primarily used for monitoring peripheral oxygenation in the muscle. Parameters that are determined using NIRS can be either directly calculated or can be derived from physiological interventions, such as arterial and venous occlusions methods. Information regarding muscle oxygen saturation, muscle oxygen consumption and regional blood flow can therefore be obtained. Clinical applications of NIRS include peripheral oxygenation monitoring during resuscitation of trauma and septic shock as well as the assessment of regional microcirculatory disorders. This review provides a brief discussion of NIRS basic principles and main clinical uses of this technique, with a specific focus on studies that assess the usefulness of NIRS in intensive care and emergency patients.
Views0Abstract
Review ArticlesNear-infrared spectroscopy for monitoring peripheral tissue perfusion in critically ill patients
Rev Bras Ter Intensiva. 2011;23(3):341-351
DOI 10.1590/S0103-507X2011000300013
Views0See moreNear infrared spectroscopy (NIRS) is a non-invasive technique that allows determination of tissue oxygenation based on spectro-photometric quantitation of oxy- and deoxyhemoglobin within a tissue. This technique has gained acceptance as a tool to monitor peripheral tissue perfusion in critically ill patient. NIRS principle is based on the use of near-infrared electromagnetic waves for qualitative and quantitative assessments of molecular factors related to tissue oxygenation. Although this technique can be apllied in any tissue, it is primarily used for monitoring peripheral oxygenation in the muscle. Parameters that are determined using NIRS can be either directly calculated or can be derived from physiological interventions, such as arterial and venous occlusions methods. Information regarding muscle oxygen saturation, muscle oxygen consumption and regional blood flow can therefore be obtained. Clinical applications of NIRS include peripheral oxygenation monitoring during resuscitation of trauma and septic shock as well as the assessment of regional microcirculatory disorders. This review provides a brief discussion of NIRS basic principles and main clinical uses of this technique, with a specific focus on studies that assess the usefulness of NIRS in intensive care and emergency patients.
-
Review Articles
Microcirculatory assessment: a new weapon in the treatment of sepsis?
Rev Bras Ter Intensiva. 2011;23(3):352-357
Abstract
Review ArticlesMicrocirculatory assessment: a new weapon in the treatment of sepsis?
Rev Bras Ter Intensiva. 2011;23(3):352-357
DOI 10.1590/S0103-507X2011000300014
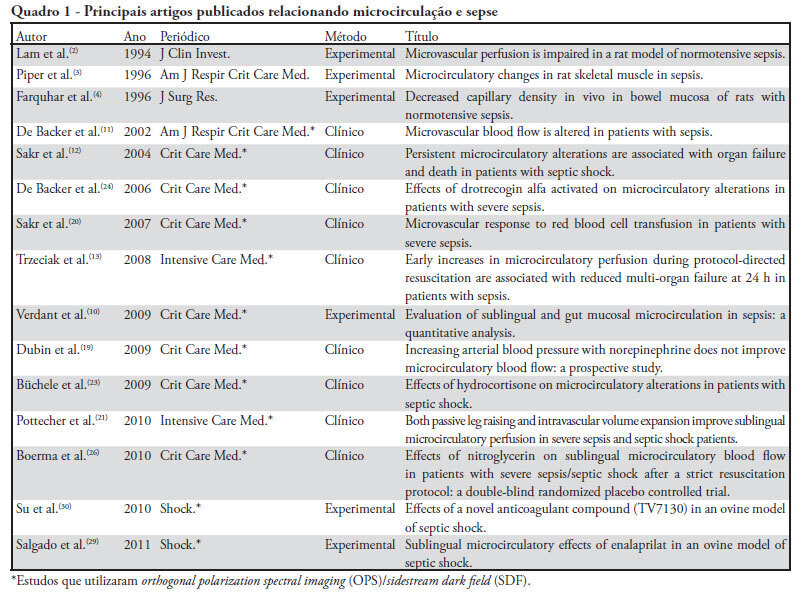
Views0See moreThe progression into multi-organ failure continues to be a common feature of sepsis and is directly related to microcirculatory dysfunction. Based on a PubMed database search using the key words microcirculation and sepsis, twenty-six articles were selected for this review. The relevant references from these articles were also selected and included in this analysis. Orthogonal polarization spectral imaging allows for the bedside assessment of the microcirculation of critically ill patients. Such imaging has established a correlation between microvascular dysfunction and patient outcomes, which allows practitioners to directly assess the effects of therapeutic interventions. However, the causal relationships between microcirculatory dysfunction, adverse outcomes, and the effects of therapies aimed at these microcirculatory changes in sepsis, are not clear.
Views0Abstract
Review ArticlesMicrocirculatory assessment: a new weapon in the treatment of sepsis?
Rev Bras Ter Intensiva. 2011;23(3):352-357
DOI 10.1590/S0103-507X2011000300014
Views0See moreThe progression into multi-organ failure continues to be a common feature of sepsis and is directly related to microcirculatory dysfunction. Based on a PubMed database search using the key words microcirculation and sepsis, twenty-six articles were selected for this review. The relevant references from these articles were also selected and included in this analysis. Orthogonal polarization spectral imaging allows for the bedside assessment of the microcirculation of critically ill patients. Such imaging has established a correlation between microvascular dysfunction and patient outcomes, which allows practitioners to directly assess the effects of therapeutic interventions. However, the causal relationships between microcirculatory dysfunction, adverse outcomes, and the effects of therapies aimed at these microcirculatory changes in sepsis, are not clear.
-
Review Articles
Severe Plasmodium falciparum malaria
Rev Bras Ter Intensiva. 2011;23(3):358-369
Abstract
Review ArticlesSevere Plasmodium falciparum malaria
Rev Bras Ter Intensiva. 2011;23(3):358-369
DOI 10.1590/S0103-507X2011000300015
Views0Malaria is one of the world’s leading parasitic diseases and affects a considerably large number of people. Considering the epidemiological reach of Plasmodium falciparum, which is almost always responsible for the most severe cases of malaria, a discussion of the clinical features and therapeutic interventions is important. In the cases of patients with severe malaria, admission to an intensive care unit is mandatory to reduce complications. To have an impact on survival rates, treatment with antimalarial drugs and supportive measures should be initiated as quickly as possible. The aim of this article is to discuss the components of severe malaria, with an emphasis on its clinical features and treatment
Keywords:MalariaPlasmodium falciparumSee moreViews0Abstract
Review ArticlesSevere Plasmodium falciparum malaria
Rev Bras Ter Intensiva. 2011;23(3):358-369
DOI 10.1590/S0103-507X2011000300015
Views0Malaria is one of the world’s leading parasitic diseases and affects a considerably large number of people. Considering the epidemiological reach of Plasmodium falciparum, which is almost always responsible for the most severe cases of malaria, a discussion of the clinical features and therapeutic interventions is important. In the cases of patients with severe malaria, admission to an intensive care unit is mandatory to reduce complications. To have an impact on survival rates, treatment with antimalarial drugs and supportive measures should be initiated as quickly as possible. The aim of this article is to discuss the components of severe malaria, with an emphasis on its clinical features and treatment
Keywords:MalariaPlasmodium falciparumSee more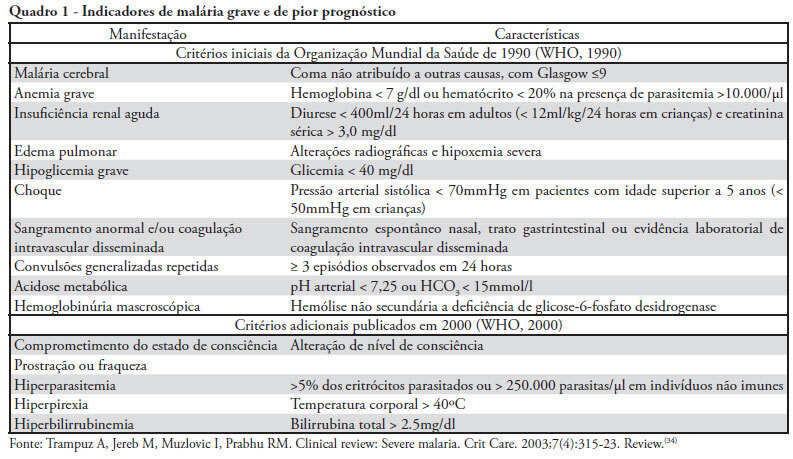
-
Review Articles
Effects of kangaroo care during painful procedures in preterm infants: a review
Rev Bras Ter Intensiva. 2011;23(3):370-373
Abstract
Review ArticlesEffects of kangaroo care during painful procedures in preterm infants: a review
Rev Bras Ter Intensiva. 2011;23(3):370-373
DOI 10.1590/S0103-507X2011000300016
Views0See moreAlthough low-birth neonates are acknowledged to experience pain, many routine procedures continue to be conducted without proper pharmacological or non-pharmacological analgesia. Kangaroo care is a low-cost strategy that can be used in the preterm newborn. Mothers should be encouraged to use this easy-to-perform method, which is feasible both before and during neonatal units’ invasive procedures, therefore contributing to pain reduction
Views0Abstract
Review ArticlesEffects of kangaroo care during painful procedures in preterm infants: a review
Rev Bras Ter Intensiva. 2011;23(3):370-373
DOI 10.1590/S0103-507X2011000300016
Views0See moreAlthough low-birth neonates are acknowledged to experience pain, many routine procedures continue to be conducted without proper pharmacological or non-pharmacological analgesia. Kangaroo care is a low-cost strategy that can be used in the preterm newborn. Mothers should be encouraged to use this easy-to-perform method, which is feasible both before and during neonatal units’ invasive procedures, therefore contributing to pain reduction
-
Case Reports
Hemodynamic and respiratory support using venoarterial extracorporeal membrane oxygenation (ECMO) in a polytrauma patient
Rev Bras Ter Intensiva. 2011;23(3):374-379
Abstract
Case ReportsHemodynamic and respiratory support using venoarterial extracorporeal membrane oxygenation (ECMO) in a polytrauma patient
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
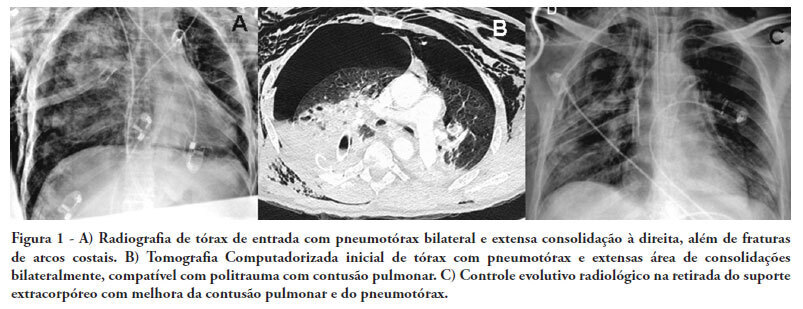
Views0See moreThere are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Views0Abstract
Case ReportsHemodynamic and respiratory support using venoarterial extracorporeal membrane oxygenation (ECMO) in a polytrauma patient
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
Views0See moreThere are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
-
Letters to the Editor
Influence of peripheral muscle strength on the decannulation success rate
Rev Bras Ter Intensiva. 2011;23(3):380-381
Abstract
Letters to the EditorInfluence of peripheral muscle strength on the decannulation success rate
Rev Bras Ter Intensiva. 2011;23(3):380-381
Views0Abstract
Letters to the EditorInfluence of peripheral muscle strength on the decannulation success rate
Rev Bras Ter Intensiva. 2011;23(3):380-381
-
Letters to the Editor
Influence of peripheral muscle strength on the decannulation success rate
Rev Bras Ter Intensiva. 2011;23(3):381-382
Abstract
Letters to the EditorInfluence of peripheral muscle strength on the decannulation success rate
Rev Bras Ter Intensiva. 2011;23(3):381-382
Views0Abstract
Letters to the EditorInfluence of peripheral muscle strength on the decannulation success rate
Rev Bras Ter Intensiva. 2011;23(3):381-382
Volume Articles - Critical Care Science (CCS)
