-
Sepsis: a problem for everyone
Rev Bras Ter Intensiva. 2011;23(2):115-116
-
Intra-abdominal hypertension associated with acute lung injury: effects on intracranial pressure
Rev Bras Ter Intensiva. 2011;23(2):117-119
Abstract
Intra-abdominal hypertension associated with acute lung injury: effects on intracranial pressure
Rev Bras Ter Intensiva. 2011;23(2):117-119
DOI 10.1590/S0103-507X2011000200002
Views0EDITORIAL Intra-abdominal hypertension associated with acute lung injury: effects on intracranial pressure […]See moreViews0

Abstract
Intra-abdominal hypertension associated with acute lung injury: effects on intracranial pressure
Rev Bras Ter Intensiva. 2011;23(2):117-119
DOI 10.1590/S0103-507X2011000200002
Views0EDITORIAL Intra-abdominal hypertension associated with acute lung injury: effects on intracranial pressure […]See more -
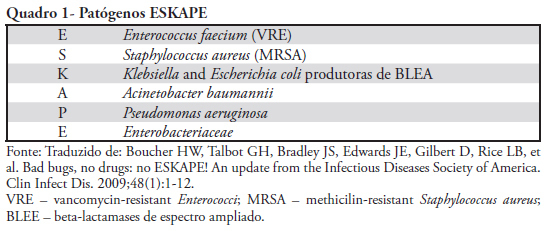
Infection with multi-resistant agents in the ICU: how to escape?
Rev Bras Ter Intensiva. 2011;23(2):120-124
-
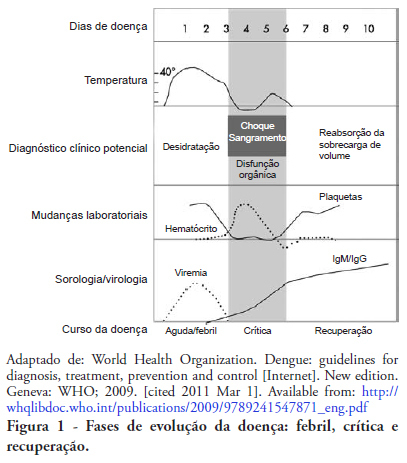
Guidelines for the management of patients with severe forms of dengue
Rev Bras Ter Intensiva. 2011;23(2):125-133
Abstract
Guidelines for the management of patients with severe forms of dengue
Rev Bras Ter Intensiva. 2011;23(2):125-133
DOI 10.1590/S0103-507X2011000200004
Views0See moreDengue is the most common vector-borne viral infection worldwide. In Brazil, the incidence has increased with successive epidemics, and an increasing proportion of patients present with severe forms of the disease. The prognosis for these patients is directly influenced by the quality of medical care. These guidelines present the management of the severe forms of dengue, including the recognition of warning signs, the treatment for prompt re-establishment of euvolemia and the evaluation and appropriate care of potential complications, thus reducing morbidity and mortality of infected children and adults
Views0Abstract
Guidelines for the management of patients with severe forms of dengue
Rev Bras Ter Intensiva. 2011;23(2):125-133
DOI 10.1590/S0103-507X2011000200004
Views0See moreDengue is the most common vector-borne viral infection worldwide. In Brazil, the incidence has increased with successive epidemics, and an increasing proportion of patients present with severe forms of the disease. The prognosis for these patients is directly influenced by the quality of medical care. These guidelines present the management of the severe forms of dengue, including the recognition of warning signs, the treatment for prompt re-establishment of euvolemia and the evaluation and appropriate care of potential complications, thus reducing morbidity and mortality of infected children and adults
-
Guidelines for the treatment of severe sepsis and septic shock: management of the infectious agent – diagnosis
Rev Bras Ter Intensiva. 2011;23(2):134-144
Abstract
Guidelines for the treatment of severe sepsis and septic shock: management of the infectious agent – diagnosis
Rev Bras Ter Intensiva. 2011;23(2):134-144
DOI 10.1590/S0103-507X2011000200005
Views1See moreSepsis is a common and lethal condition that carries a substantial financial burden and is the primary cause of death in intensive care units. Early diagnosis and treatment of patients has been clearly shown to improve prognosis. Therefore, early diagnosis of infections and control of the primary infection site are fundamental to improving patients’ prognosis. This guideline reviews the available evidence concerning the primary strategies for the diagnosis of infection
Views1Abstract
Guidelines for the treatment of severe sepsis and septic shock: management of the infectious agent – diagnosis
Rev Bras Ter Intensiva. 2011;23(2):134-144
DOI 10.1590/S0103-507X2011000200005
Views1See moreSepsis is a common and lethal condition that carries a substantial financial burden and is the primary cause of death in intensive care units. Early diagnosis and treatment of patients has been clearly shown to improve prognosis. Therefore, early diagnosis of infections and control of the primary infection site are fundamental to improving patients’ prognosis. This guideline reviews the available evidence concerning the primary strategies for the diagnosis of infection
-
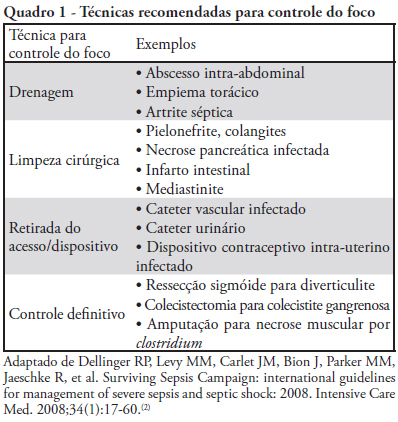
Guidelines for the treatment of severe sepsis and septic shock – management of the infectious agent – source control and antimicrobial treatment
Rev Bras Ter Intensiva. 2011;23(2):145-157
Abstract
Guidelines for the treatment of severe sepsis and septic shock – management of the infectious agent – source control and antimicrobial treatment
Rev Bras Ter Intensiva. 2011;23(2):145-157
DOI 10.1590/S0103-507X2011000200006
Views0See moreSepsis is a common and lethal condition that carries a substantial financial burden. In addition, it is the main cause of death in intensive care units. Early diagnosis and treatment of patients has been clearly shown to improve prognosis. Therefore, early diagnosis of the infecting agent, control of the primary infection site and the use of appropriate antibiotic therapy are fundamental to improving outcomes. This guideline reviews the available evidence in the literature concerning infection control and therapy strategies
Views0Abstract
Guidelines for the treatment of severe sepsis and septic shock – management of the infectious agent – source control and antimicrobial treatment
Rev Bras Ter Intensiva. 2011;23(2):145-157
DOI 10.1590/S0103-507X2011000200006
Views0See moreSepsis is a common and lethal condition that carries a substantial financial burden. In addition, it is the main cause of death in intensive care units. Early diagnosis and treatment of patients has been clearly shown to improve prognosis. Therefore, early diagnosis of the infecting agent, control of the primary infection site and the use of appropriate antibiotic therapy are fundamental to improving outcomes. This guideline reviews the available evidence in the literature concerning infection control and therapy strategies
-
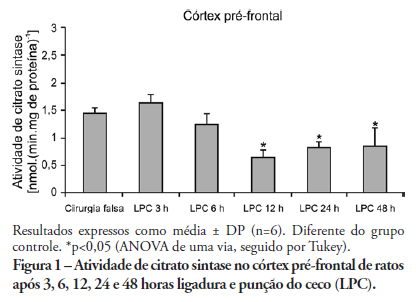
Inhibition of brain citrate synthase activity in an animal model of sepsis
Rev Bras Ter Intensiva. 2011;23(2):158-163
Abstract
Inhibition of brain citrate synthase activity in an animal model of sepsis
Rev Bras Ter Intensiva. 2011;23(2):158-163
DOI 10.1590/S0103-507X2011000200007
Views0See moreOBJECTIVE: An extensive body of evidence from experimental studies indicates that sepsis is associated with increased reactive oxygen species production, depletion of antioxidants, and accumulation of markers of oxidative stress. Moreover, mitochondrial dysfunction has been implicated in the pathogenesis of multiple organ dysfunction syndrome (MODS). Citrate synthase is an enzyme localized in the mitochondrial matrix and an important component of the Krebs cycle; consequently, citrate synthase has been used as a quantitative enzyme marker for the presence of intact mitochondria. Thus, we investigated citrate synthase activity in the brains of rats submitted to a cecal ligation puncture model of sepsis. METHODS: At several times points (3, 6, 12, 24 and 48 hours) after the cecal ligation puncture operation, six rats were killed by decapitation. Their brains were removed, and the hippocampus, striatum, cerebellum, cerebral cortex and prefrontal cortex were dissected and used to determine citrate synthase activity. RESULTS: We found that citrate synthase activity in the prefrontal cortex was inhibited 12, 24 and 48 hours after cecal ligation puncture. In the cerebral cortex, citrate synthase activity was inhibited 3, 12, 24 and 48 hours after cecal ligation puncture. Citrate synthase was not affected in the hippocampus, striatum or cerebellum up to 48 hours after cecal ligation puncture. CONCLUSION: Considering that energy impairment due to mitochondrial dysfunction in sepsis has been well described and that oxidative stress plays a crucial role in sepsis development, we believe that energy impairment may also be involved in these processes. If citrate synthase inhibition also occurs in a sepsis model, it is tempting to speculate that a reduction in brain metabolism may be related to the pathophysiology of this disease.
Views0Abstract
Inhibition of brain citrate synthase activity in an animal model of sepsis
Rev Bras Ter Intensiva. 2011;23(2):158-163
DOI 10.1590/S0103-507X2011000200007
Views0See moreOBJECTIVE: An extensive body of evidence from experimental studies indicates that sepsis is associated with increased reactive oxygen species production, depletion of antioxidants, and accumulation of markers of oxidative stress. Moreover, mitochondrial dysfunction has been implicated in the pathogenesis of multiple organ dysfunction syndrome (MODS). Citrate synthase is an enzyme localized in the mitochondrial matrix and an important component of the Krebs cycle; consequently, citrate synthase has been used as a quantitative enzyme marker for the presence of intact mitochondria. Thus, we investigated citrate synthase activity in the brains of rats submitted to a cecal ligation puncture model of sepsis. METHODS: At several times points (3, 6, 12, 24 and 48 hours) after the cecal ligation puncture operation, six rats were killed by decapitation. Their brains were removed, and the hippocampus, striatum, cerebellum, cerebral cortex and prefrontal cortex were dissected and used to determine citrate synthase activity. RESULTS: We found that citrate synthase activity in the prefrontal cortex was inhibited 12, 24 and 48 hours after cecal ligation puncture. In the cerebral cortex, citrate synthase activity was inhibited 3, 12, 24 and 48 hours after cecal ligation puncture. Citrate synthase was not affected in the hippocampus, striatum or cerebellum up to 48 hours after cecal ligation puncture. CONCLUSION: Considering that energy impairment due to mitochondrial dysfunction in sepsis has been well described and that oxidative stress plays a crucial role in sepsis development, we believe that energy impairment may also be involved in these processes. If citrate synthase inhibition also occurs in a sepsis model, it is tempting to speculate that a reduction in brain metabolism may be related to the pathophysiology of this disease.
-
Factors associated with variation in intracranial pressure in a model of intra-abdominal hypertension with acute lung injury
Rev Bras Ter Intensiva. 2011;23(2):164-169
Abstract
Factors associated with variation in intracranial pressure in a model of intra-abdominal hypertension with acute lung injury
Rev Bras Ter Intensiva. 2011;23(2):164-169
DOI 10.1590/S0103-507X2011000200008
Views0OBJECTIVE: To evaluate the effects of hemodynamic, respiratory and metabolic changes on intracranial pressure in a model of acute lung injury and abdominal compartment syndrome. METHODS: Eight Agroceres pigs were submitted to five different clinical scenarios after instrumentation: 1) a baseline condition with low intra-abdominal pressure and healthy lungs; 2) pneumoperitoneum with 20 mmHg intra-abdominal pressure; 3) acute lung injury induced by pulmonary lavage with surfactant deactivation; 4) pneumoperitoneum with 20 mmHg intra-abdominal pressure with lung pulmonary injury and low positive end-expiratory pressure; and 5) 27 cmH2O positive end-expiratory pressure with pneumoperitoneum and acute lung injury. Respiratory and hemodynamic variables were collected. A multivariate analysis was conducted to search for variables associated with increased intracranial pressure in the five scenarios. RESULTS: Only plateau airway pressure showed a positive correlation with intracranial pressure in the multivariate analysis. In the models with acute lung injury, plateau airway pressure, CO2 arterial pressure, end tidal CO2 and central venous pressure were positively correlated with increased intracranial pressure. CONCLUSION: In a model of multiple organ dysfunction with associated clinical conditions causing increased intra-thoracic and abdominal pressure, increased intracranial pressure triggered by elevated intra-abdominal pressure is apparently caused by worsened respiratory system compliance and a reduced brain venous drainage gradient due to increased central venous pressure.
Keywords:Acute Lung InjuryCompartment syndromesDiseases models, animalIntensive care unitsIntracranial pressureRespiration, artificialSwineSee moreViews0Abstract
Factors associated with variation in intracranial pressure in a model of intra-abdominal hypertension with acute lung injury
Rev Bras Ter Intensiva. 2011;23(2):164-169
DOI 10.1590/S0103-507X2011000200008
Views0OBJECTIVE: To evaluate the effects of hemodynamic, respiratory and metabolic changes on intracranial pressure in a model of acute lung injury and abdominal compartment syndrome. METHODS: Eight Agroceres pigs were submitted to five different clinical scenarios after instrumentation: 1) a baseline condition with low intra-abdominal pressure and healthy lungs; 2) pneumoperitoneum with 20 mmHg intra-abdominal pressure; 3) acute lung injury induced by pulmonary lavage with surfactant deactivation; 4) pneumoperitoneum with 20 mmHg intra-abdominal pressure with lung pulmonary injury and low positive end-expiratory pressure; and 5) 27 cmH2O positive end-expiratory pressure with pneumoperitoneum and acute lung injury. Respiratory and hemodynamic variables were collected. A multivariate analysis was conducted to search for variables associated with increased intracranial pressure in the five scenarios. RESULTS: Only plateau airway pressure showed a positive correlation with intracranial pressure in the multivariate analysis. In the models with acute lung injury, plateau airway pressure, CO2 arterial pressure, end tidal CO2 and central venous pressure were positively correlated with increased intracranial pressure. CONCLUSION: In a model of multiple organ dysfunction with associated clinical conditions causing increased intra-thoracic and abdominal pressure, increased intracranial pressure triggered by elevated intra-abdominal pressure is apparently caused by worsened respiratory system compliance and a reduced brain venous drainage gradient due to increased central venous pressure.
Keywords:Acute Lung InjuryCompartment syndromesDiseases models, animalIntensive care unitsIntracranial pressureRespiration, artificialSwineSee more -
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
Abstract
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
DOI 10.1590/S0103-507X2011000200009
Views0See moreOBJECTIVE: To compare the differences in fluid and electrolyte balance in patients with low and high weight in the first postoperative day. METHODS: Over a period of 18 months, we prospectively evaluated 150 patients in the first 24 hours after surgery, in a university-affiliated hospital intensive care unit. Patients with low weight (< 60 kg) and high body weight (> 90 Kg) were compared in terms of fluid intake and output. RESULTS: No significant differences were observed in the volume (4334 ± 1097 vs. 4644 ± 1957 ml/24 h) and composition of the fluids administered (481 ± 187 vs. 586 ± 288 mEq [Na+]administered/24 h). The 24 h urine output was similar (2474 ± 1597 vs.2208 ± 678 ml/24 h) but low weight group showed higher electrolyte elimination (296 ± 195 vs.192 ± 117 mEq [Na+]urine /24 h, p = 0.0246). When the administered fluids were adjusted for body weight, the volume and amount of electrolytes of fluids administered were higher in the low weight group (79 ± 21 vs. 47 ± 22 ml/kg/24 h, p < 0.0001 and 8.8 ± 3.4 vs. 5.8 ± 3.3 mEq [Na+]administered/kg/24 h, p = 0.017, respectively). This group also showed higher urine output and electrolyte elimination (45 ± 28 vs. 22 ± 7 ml/kg/24 h, p = 0.0002 and 5.3 ± 3.5 vs. 1.8 ± 1.2 mEq [Na+]urine/kg/24 h, p < 0.0001, respectively). CONCLUSIONS: The lack of adjustment of the fluid therapy to body weight determined that low weight patients received more fluid than high weight patients according to their body weight. This fluid overload could be compensated by increased urine output and electrolyte elimination.
Views0Abstract
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
DOI 10.1590/S0103-507X2011000200009
Views0See moreOBJECTIVE: To compare the differences in fluid and electrolyte balance in patients with low and high weight in the first postoperative day. METHODS: Over a period of 18 months, we prospectively evaluated 150 patients in the first 24 hours after surgery, in a university-affiliated hospital intensive care unit. Patients with low weight (< 60 kg) and high body weight (> 90 Kg) were compared in terms of fluid intake and output. RESULTS: No significant differences were observed in the volume (4334 ± 1097 vs. 4644 ± 1957 ml/24 h) and composition of the fluids administered (481 ± 187 vs. 586 ± 288 mEq [Na+]administered/24 h). The 24 h urine output was similar (2474 ± 1597 vs.2208 ± 678 ml/24 h) but low weight group showed higher electrolyte elimination (296 ± 195 vs.192 ± 117 mEq [Na+]urine /24 h, p = 0.0246). When the administered fluids were adjusted for body weight, the volume and amount of electrolytes of fluids administered were higher in the low weight group (79 ± 21 vs. 47 ± 22 ml/kg/24 h, p < 0.0001 and 8.8 ± 3.4 vs. 5.8 ± 3.3 mEq [Na+]administered/kg/24 h, p = 0.017, respectively). This group also showed higher urine output and electrolyte elimination (45 ± 28 vs. 22 ± 7 ml/kg/24 h, p = 0.0002 and 5.3 ± 3.5 vs. 1.8 ± 1.2 mEq [Na+]urine/kg/24 h, p < 0.0001, respectively). CONCLUSIONS: The lack of adjustment of the fluid therapy to body weight determined that low weight patients received more fluid than high weight patients according to their body weight. This fluid overload could be compensated by increased urine output and electrolyte elimination.
-
Physicochemical characterization of metabolic acidosis induced by normal saline resuscitation of patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2011;23(2):176-182
Abstract
Physicochemical characterization of metabolic acidosis induced by normal saline resuscitation of patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2011;23(2):176-182
DOI 10.1590/S0103-507X2011000200010
Views0OBJECTIVE: The aim of this study was to characterize and quantify metabolic acidosis that was caused by initial volume expansion during the reanimation of patients with severe sepsis and septic shock. METHODS: A blood sample was drawn for physicochemical characterization of the patient’s acid-base equilibrium both before and after volume expansion using 30 mL/kg 0.9% saline solution. The diagnosis and quantification of metabolic acidosis were based on the standard base excess (SBE). RESULTS: Eight patients with a mean age of 58 ± 13 years and mean APACHE II scores of 20 ± 4 were expanded using 2,000 ± 370 mL of 0.9% saline solution. Blood pH dropped from 7.404 ± 0.080 to 7.367 ± 0.086 (p=0.018), and PC O2 increased from 30 ± 5 to 32 ± 2 mmHg (p=0.215); SBE dropped from -4.4 ± 5.6 to -6.0 ± 5.7 mEq/L (p=0.039). The drop in SBE was associated with the acidifying power of two factors, namely, a significant increase in the strong ion gap (SIG) from 6.1 ± 3.4 to 7.7 ± 4.0 mEq/L (p = 0.134) and a non-significant drop in the apparent inorganic strong ion differences (SIDai) from 40 ± 5 to 38 ± 4 mEq/L (p = 0.318). Conversely, the serum albumin levels decreased from 3.1 ± 1.0 to 2.6 ± 0.8 mEq/L (p = 0.003) with an alkalinizing effect on SBE. Increased serum chloride levels from 103 ± 10 to 106 ± 7 mEq/L (p < 0.001) led to a drop in SIDai. CONCLUSION: Initial resuscitation using 30 mL/kg of 0.9% saline solution for patients with severe sepsis and septic shock is associated with worsened metabolic acidosis, as measured by SBE. This worsened SBE can be ascribed to a serum increase in the levels of unmeasurable anions and chloride.
Keywords:Acid-base equilibriumIntensive care unitsKetosisSaline solution, hypertonic/therapeutic useSepsisShock, septic/therapySee moreViews0Abstract
Physicochemical characterization of metabolic acidosis induced by normal saline resuscitation of patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2011;23(2):176-182
DOI 10.1590/S0103-507X2011000200010
Views0OBJECTIVE: The aim of this study was to characterize and quantify metabolic acidosis that was caused by initial volume expansion during the reanimation of patients with severe sepsis and septic shock. METHODS: A blood sample was drawn for physicochemical characterization of the patient’s acid-base equilibrium both before and after volume expansion using 30 mL/kg 0.9% saline solution. The diagnosis and quantification of metabolic acidosis were based on the standard base excess (SBE). RESULTS: Eight patients with a mean age of 58 ± 13 years and mean APACHE II scores of 20 ± 4 were expanded using 2,000 ± 370 mL of 0.9% saline solution. Blood pH dropped from 7.404 ± 0.080 to 7.367 ± 0.086 (p=0.018), and PC O2 increased from 30 ± 5 to 32 ± 2 mmHg (p=0.215); SBE dropped from -4.4 ± 5.6 to -6.0 ± 5.7 mEq/L (p=0.039). The drop in SBE was associated with the acidifying power of two factors, namely, a significant increase in the strong ion gap (SIG) from 6.1 ± 3.4 to 7.7 ± 4.0 mEq/L (p = 0.134) and a non-significant drop in the apparent inorganic strong ion differences (SIDai) from 40 ± 5 to 38 ± 4 mEq/L (p = 0.318). Conversely, the serum albumin levels decreased from 3.1 ± 1.0 to 2.6 ± 0.8 mEq/L (p = 0.003) with an alkalinizing effect on SBE. Increased serum chloride levels from 103 ± 10 to 106 ± 7 mEq/L (p < 0.001) led to a drop in SIDai. CONCLUSION: Initial resuscitation using 30 mL/kg of 0.9% saline solution for patients with severe sepsis and septic shock is associated with worsened metabolic acidosis, as measured by SBE. This worsened SBE can be ascribed to a serum increase in the levels of unmeasurable anions and chloride.
Keywords:Acid-base equilibriumIntensive care unitsKetosisSaline solution, hypertonic/therapeutic useSepsisShock, septic/therapySee more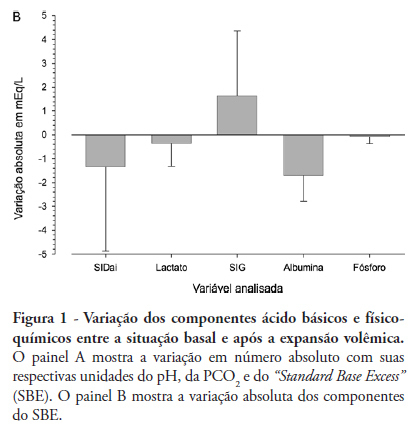
-
Impact of the adequacy of energy intake on intensive care unit mortality in patients receiving enteral nutrition
Rev Bras Ter Intensiva. 2011;23(2):183-189
Abstract
Impact of the adequacy of energy intake on intensive care unit mortality in patients receiving enteral nutrition
Rev Bras Ter Intensiva. 2011;23(2):183-189
DOI 10.1590/S0103-507X2011000200011
Views0OBJECTIVE: To investigate the relationship between adequacy of energy intake and intensive care unit mortality in patients receiving exclusive enteral nutrition therapy. METHODS: Observational and prospective study conducted during 2008 and 2009. Patients above 18 years with exclusive enteral nutrition therapy for at least 72 hours were included. The adequacy of energy intake was estimated by the administered/prescribed ratio. Non-conditional logistic regression was used to assess the relationship between predictive variables (adequacy of energy intake, APACHE II, gender, age, and intensive care unit length of stay) and intensive care unit mortality. RESULTS: Sixty-three patients (mean 58 years, 27% mortality) were included, 47.6% of whom received more than 90% of the energy prescribed (mean adequacy 88.2%). Mean energy balance was -190 kcal/day. Significant associations between death in the intensive care unit and the variables age and intensive care unit length of stay were observed, after removing the variables adequacy of energy intake, APACHE II, gender and age during the modeling process. CONCLUSION: In our study, adequacy of energy intake did not affect intensive care unit mortality. Carefully followed enteral nutrition protocols, resulting in an administered/prescribed ratio above 70%, are apparently not sufficient to impact the mortality rates in the intensive care unit. Therefore, it may not be necessary to achieve 100% of the targeted energy, considering the high frequency of enteral feeding interruptions due to gastrointestinal intolerance and fasting for tests and procedures. Additional research is needed to identify the optimal energy intake for improved outcomes and reduced costs.
Keywords:Energy requirementsenteral nutritionIntensive care unitsMeasures of association, exposure, risk or outcomeMortalitySee moreViews0Abstract
Impact of the adequacy of energy intake on intensive care unit mortality in patients receiving enteral nutrition
Rev Bras Ter Intensiva. 2011;23(2):183-189
DOI 10.1590/S0103-507X2011000200011
Views0OBJECTIVE: To investigate the relationship between adequacy of energy intake and intensive care unit mortality in patients receiving exclusive enteral nutrition therapy. METHODS: Observational and prospective study conducted during 2008 and 2009. Patients above 18 years with exclusive enteral nutrition therapy for at least 72 hours were included. The adequacy of energy intake was estimated by the administered/prescribed ratio. Non-conditional logistic regression was used to assess the relationship between predictive variables (adequacy of energy intake, APACHE II, gender, age, and intensive care unit length of stay) and intensive care unit mortality. RESULTS: Sixty-three patients (mean 58 years, 27% mortality) were included, 47.6% of whom received more than 90% of the energy prescribed (mean adequacy 88.2%). Mean energy balance was -190 kcal/day. Significant associations between death in the intensive care unit and the variables age and intensive care unit length of stay were observed, after removing the variables adequacy of energy intake, APACHE II, gender and age during the modeling process. CONCLUSION: In our study, adequacy of energy intake did not affect intensive care unit mortality. Carefully followed enteral nutrition protocols, resulting in an administered/prescribed ratio above 70%, are apparently not sufficient to impact the mortality rates in the intensive care unit. Therefore, it may not be necessary to achieve 100% of the targeted energy, considering the high frequency of enteral feeding interruptions due to gastrointestinal intolerance and fasting for tests and procedures. Additional research is needed to identify the optimal energy intake for improved outcomes and reduced costs.
Keywords:Energy requirementsenteral nutritionIntensive care unitsMeasures of association, exposure, risk or outcomeMortalitySee more -
Bronchial hygiene technique with manual hyperinflation and thoracic compression: effectiveness and safety
Rev Bras Ter Intensiva. 2011;23(2):190-198
Abstract
Bronchial hygiene technique with manual hyperinflation and thoracic compression: effectiveness and safety
Rev Bras Ter Intensiva. 2011;23(2):190-198
DOI 10.1590/S0103-507X2011000200012
Views0OBJECTIVES: To evaluate the effects of the manual hyperinflation with thoracic compression (MHTC) maneuver on the clearance of secretions, pulmonary mechanics, hemodynamics and oxygenation in mechanically ventilated patients. METHODS: This was a controlled, crossover study that included twenty patients who were under invasive ventilation for more than 48 hours. Four hours after the last airway suctioning procedure, the patients underwent the study interventions, Suction alone or MHTC plus Suction, in sequence at four hour intervals. The sequence order for the procedures was established by randomization. Data were collected before, during and 5, 15, 30 and 60 minutes after each intervention. The suctioned secretions were collected and weighed. RESULTS: No significant differences between the procedures were found regarding tidal volume, plateau pressure and pulmonary compliance (p>0.05). The hemodynamic variables showed increased pressures and heart rate during the procedures and returned to baseline values five minutes after the end of the procedure (p≤0.001). No significant hemodynamic differences were seen between the interventions (p>0.05). For the duration of the study, oxygen saturation was 99% with only two exceptions during the MHTC + Suction procedure, where saturation was 98% (p<0.05). No significant differences were observed between the techniques regarding the weight of the suctioned secretion. CONCLUSION: The results suggest that MHTC, as performed in this study, adds no benefit with respect to oxygenation optimization, pulmonary mechanics and clearance of secretions. However, the MHTC maneuver did not result in hemodynamic changes when compared to the suctioning procedure alone.
Keywords:Bronchi/secretionPhysical therapy modalitiesRespiration, artificialRespiratory therapy/methodsSuctionSee moreViews0Abstract
Bronchial hygiene technique with manual hyperinflation and thoracic compression: effectiveness and safety
Rev Bras Ter Intensiva. 2011;23(2):190-198
DOI 10.1590/S0103-507X2011000200012
Views0OBJECTIVES: To evaluate the effects of the manual hyperinflation with thoracic compression (MHTC) maneuver on the clearance of secretions, pulmonary mechanics, hemodynamics and oxygenation in mechanically ventilated patients. METHODS: This was a controlled, crossover study that included twenty patients who were under invasive ventilation for more than 48 hours. Four hours after the last airway suctioning procedure, the patients underwent the study interventions, Suction alone or MHTC plus Suction, in sequence at four hour intervals. The sequence order for the procedures was established by randomization. Data were collected before, during and 5, 15, 30 and 60 minutes after each intervention. The suctioned secretions were collected and weighed. RESULTS: No significant differences between the procedures were found regarding tidal volume, plateau pressure and pulmonary compliance (p>0.05). The hemodynamic variables showed increased pressures and heart rate during the procedures and returned to baseline values five minutes after the end of the procedure (p≤0.001). No significant hemodynamic differences were seen between the interventions (p>0.05). For the duration of the study, oxygen saturation was 99% with only two exceptions during the MHTC + Suction procedure, where saturation was 98% (p<0.05). No significant differences were observed between the techniques regarding the weight of the suctioned secretion. CONCLUSION: The results suggest that MHTC, as performed in this study, adds no benefit with respect to oxygenation optimization, pulmonary mechanics and clearance of secretions. However, the MHTC maneuver did not result in hemodynamic changes when compared to the suctioning procedure alone.
Keywords:Bronchi/secretionPhysical therapy modalitiesRespiration, artificialRespiratory therapy/methodsSuctionSee more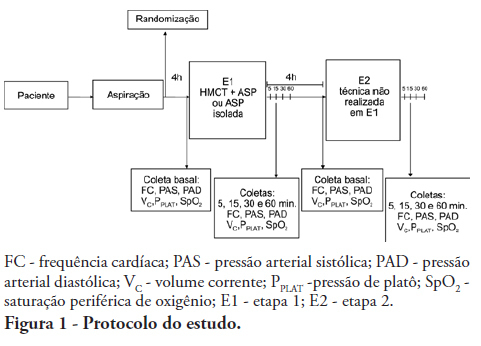
-
Lack of accuracy of ventilatory indexes in predicting extubation success in children submitted to mechanical ventilation
Rev Bras Ter Intensiva. 2011;23(2):199-206
Abstract
Lack of accuracy of ventilatory indexes in predicting extubation success in children submitted to mechanical ventilation
Rev Bras Ter Intensiva. 2011;23(2):199-206
DOI 10.1590/S0103-507X2011000200013
Views0OBJECTIVES: Between 10% and 20% of children submitted to mechanical ventilation in the pediatric intensive care unit present extubation failure. Several ventilatory indexes have been proposed to predict extubation failure. The aim of this study was to analyze the accuracy of these indices in predicting successful extubation in children and to evaluate these variables according to the age of the patient and the specific disease. METHODS: A prospective observational study including all children submitted to mechanical ventilation in a Brazilian referral pediatric intensive care unit was conducted between August 2007 and August 2008. The tidal volume, maximal negative inspiratory pressure, rapid shallow breathing index and other ventilatory indexes were measured before extubation. These variables were analyzed according to the extubation outcome (success or failure) as well as age and specific disease (post cardiac surgery and acute viral bronchiolitis). RESULTS: A total of 100 patients were included (median age of 2.1 years old). Extubation failure was observed in 13% and was associated with lower weight (10.3+8.1 Kg vs. 5.5+2.4 Kg; p=0.01). We also evaluated the relationship between extubation failure and the main cause indicating mechanical ventilation: children who had received cardiac surgery (n=17) presented an extubation failure rate of 29.4% with a relative risk of 4.6 (1.2-17.2) when compared to children with acute viral bronchiolitis (n=47, extubation failure rate of 6.4%). The maximal inspiratory pressure was the only physiologic variable independently associated with the outcome. However, this variable showed a wide dispersion and lack of accuracy for predicting extubation success (sensitivity of 82% and specificity of 55% for a cut point of -37.5 cmH2O predicting successful extubation). The same wide dispersion was observed with other ventilatory indexes. CONCLUSION: The indexes for predicting extubation success in children submitted to mechanical ventilation are not accurate; they vary widely depending on age, main disease and other clinical aspects. New formulas including clinical variables should be developed for better prediction of extubation success in children submitted to mechanical ventilation
Keywords:Intubation/adverse effectspediatric intensive careRespiration, artificialRespiratory insufficiencyVentilator weaningSee moreViews0Abstract
Lack of accuracy of ventilatory indexes in predicting extubation success in children submitted to mechanical ventilation
Rev Bras Ter Intensiva. 2011;23(2):199-206
DOI 10.1590/S0103-507X2011000200013
Views0OBJECTIVES: Between 10% and 20% of children submitted to mechanical ventilation in the pediatric intensive care unit present extubation failure. Several ventilatory indexes have been proposed to predict extubation failure. The aim of this study was to analyze the accuracy of these indices in predicting successful extubation in children and to evaluate these variables according to the age of the patient and the specific disease. METHODS: A prospective observational study including all children submitted to mechanical ventilation in a Brazilian referral pediatric intensive care unit was conducted between August 2007 and August 2008. The tidal volume, maximal negative inspiratory pressure, rapid shallow breathing index and other ventilatory indexes were measured before extubation. These variables were analyzed according to the extubation outcome (success or failure) as well as age and specific disease (post cardiac surgery and acute viral bronchiolitis). RESULTS: A total of 100 patients were included (median age of 2.1 years old). Extubation failure was observed in 13% and was associated with lower weight (10.3+8.1 Kg vs. 5.5+2.4 Kg; p=0.01). We also evaluated the relationship between extubation failure and the main cause indicating mechanical ventilation: children who had received cardiac surgery (n=17) presented an extubation failure rate of 29.4% with a relative risk of 4.6 (1.2-17.2) when compared to children with acute viral bronchiolitis (n=47, extubation failure rate of 6.4%). The maximal inspiratory pressure was the only physiologic variable independently associated with the outcome. However, this variable showed a wide dispersion and lack of accuracy for predicting extubation success (sensitivity of 82% and specificity of 55% for a cut point of -37.5 cmH2O predicting successful extubation). The same wide dispersion was observed with other ventilatory indexes. CONCLUSION: The indexes for predicting extubation success in children submitted to mechanical ventilation are not accurate; they vary widely depending on age, main disease and other clinical aspects. New formulas including clinical variables should be developed for better prediction of extubation success in children submitted to mechanical ventilation
Keywords:Intubation/adverse effectspediatric intensive careRespiration, artificialRespiratory insufficiencyVentilator weaningSee more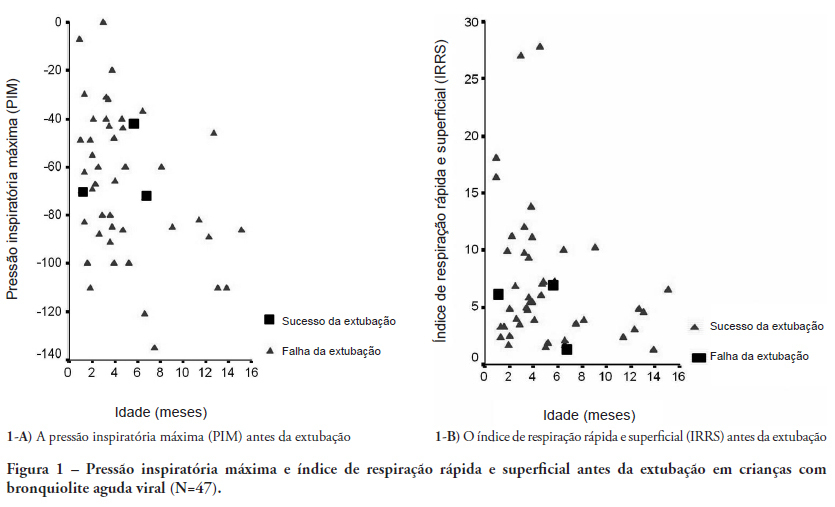
-
Sepsis: an update
Rev Bras Ter Intensiva. 2011;23(2):207-216
Abstract
Sepsis: an update
Rev Bras Ter Intensiva. 2011;23(2):207-216
DOI 10.1590/S0103-507X2011000200014
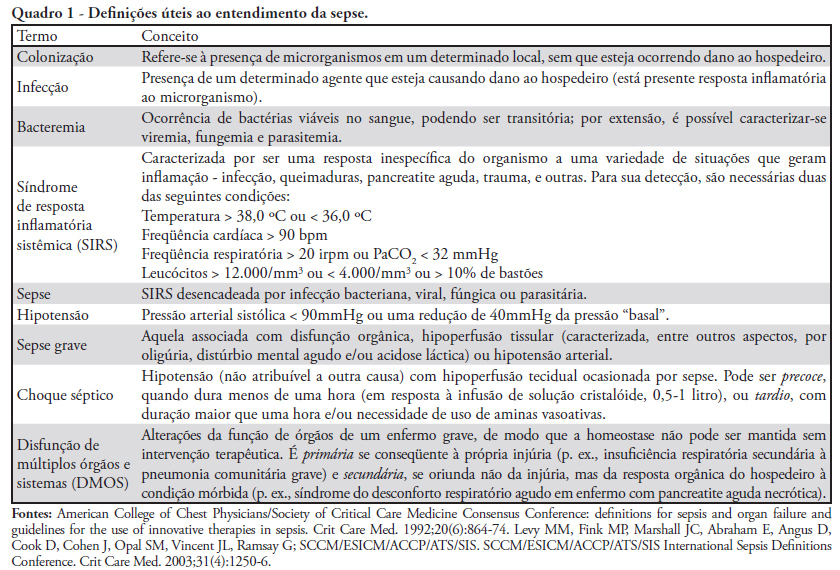
Views0See moreThis paper aims to provide an update on the main aspects of sepsis, a very relevant health care issue. A number of hypotheses have been proposed to explain its origin, involving interactions between microorganisms and the innate immune system, inflammation/immune mediation and the coagulation system. The clinical features of sepsis are variable and depend on the primary site of infection. The identification of early signs and symptoms is crucial for starting therapeutic measures fundamentally based on volume resuscitation, antibiotic therapy, use of steroids, anticoagulant therapy, biologic viability maintenance interventions and nutritional support.
Views0Abstract
Sepsis: an update
Rev Bras Ter Intensiva. 2011;23(2):207-216
DOI 10.1590/S0103-507X2011000200014
Views0See moreThis paper aims to provide an update on the main aspects of sepsis, a very relevant health care issue. A number of hypotheses have been proposed to explain its origin, involving interactions between microorganisms and the innate immune system, inflammation/immune mediation and the coagulation system. The clinical features of sepsis are variable and depend on the primary site of infection. The identification of early signs and symptoms is crucial for starting therapeutic measures fundamentally based on volume resuscitation, antibiotic therapy, use of steroids, anticoagulant therapy, biologic viability maintenance interventions and nutritional support.
-
Ultrasound-guided central venous catheterization: what is the evidence?
Rev Bras Ter Intensiva. 2011;23(2):217-221
Abstract
Ultrasound-guided central venous catheterization: what is the evidence?
Rev Bras Ter Intensiva. 2011;23(2):217-221
DOI 10.1590/S0103-507X2011000200015
Views0See moreIn recent years, international health quality assurance organizations have been recommending ultrasound guidance for central venous punctures. This article reviews the evidence behind these recommendations. The MEDLINE, PubMed and SCIELO databases were searched for the following MeSH terms: central venous access, ultrasonography, and adults. The search was conducted on September 24, 2010, and selected meta-analyses, randomized clinical trials and reviews, retrieving 291 papers. The 21 most important papers were analyzed in this review. The internal jugular vein is the most studied ultrasound-guided puncture site, with meta-analysis showing lower relative risks of failure and complications. In addition, the largest available randomized clinical trial demonstrated a reduced central venous catheter-associated blood stream infection rate. There are few studies involving subclavian vein puncture; however, ultrasound was shown to be beneficial in two meta-analyses (however, with small numbers of patients). Regarding the femoral venous site, only one randomized clinical trial (20 patients) was identified, showing positive findings. In a British cost-effectiveness study, ultrasound use lead to resource savings for different sites of venous puncture. There is strong evidence for ultrasound benefit for internal jugular vein puncture. Although the method appears attractive for the other sites, the data are not sufficient to support any recommendation.
Views0Abstract
Ultrasound-guided central venous catheterization: what is the evidence?
Rev Bras Ter Intensiva. 2011;23(2):217-221
DOI 10.1590/S0103-507X2011000200015
Views0See moreIn recent years, international health quality assurance organizations have been recommending ultrasound guidance for central venous punctures. This article reviews the evidence behind these recommendations. The MEDLINE, PubMed and SCIELO databases were searched for the following MeSH terms: central venous access, ultrasonography, and adults. The search was conducted on September 24, 2010, and selected meta-analyses, randomized clinical trials and reviews, retrieving 291 papers. The 21 most important papers were analyzed in this review. The internal jugular vein is the most studied ultrasound-guided puncture site, with meta-analysis showing lower relative risks of failure and complications. In addition, the largest available randomized clinical trial demonstrated a reduced central venous catheter-associated blood stream infection rate. There are few studies involving subclavian vein puncture; however, ultrasound was shown to be beneficial in two meta-analyses (however, with small numbers of patients). Regarding the femoral venous site, only one randomized clinical trial (20 patients) was identified, showing positive findings. In a British cost-effectiveness study, ultrasound use lead to resource savings for different sites of venous puncture. There is strong evidence for ultrasound benefit for internal jugular vein puncture. Although the method appears attractive for the other sites, the data are not sufficient to support any recommendation.
-
Mechanisms of dysfunction of the blood-brain barrier in critically ill patients: emphasis on the role of matrix metalloproteinases
Rev Bras Ter Intensiva. 2011;23(2):222-227
Abstract
Mechanisms of dysfunction of the blood-brain barrier in critically ill patients: emphasis on the role of matrix metalloproteinases
Rev Bras Ter Intensiva. 2011;23(2):222-227
DOI 10.1590/S0103-507X2011000200016
Views0See moreThis paper aims to describe the physiological basis of the blood-brain barrier components and its properties. Additionally, the particular effects of metalloproteinases and their control over the extracellular matrix and its relationship with blood-brain barrier dysfunction are discussed. Finally, the role of metalloproteinases on changes in the central nervous system in critically ill patients is discussed.
Views0Abstract
Mechanisms of dysfunction of the blood-brain barrier in critically ill patients: emphasis on the role of matrix metalloproteinases
Rev Bras Ter Intensiva. 2011;23(2):222-227
DOI 10.1590/S0103-507X2011000200016
Views0See moreThis paper aims to describe the physiological basis of the blood-brain barrier components and its properties. Additionally, the particular effects of metalloproteinases and their control over the extracellular matrix and its relationship with blood-brain barrier dysfunction are discussed. Finally, the role of metalloproteinases on changes in the central nervous system in critically ill patients is discussed.
-
Benefits and limitations of the use of glucose for the treatment of pain in neonates: a literature review
Rev Bras Ter Intensiva. 2011;23(2):228-237
Abstract
Benefits and limitations of the use of glucose for the treatment of pain in neonates: a literature review
Rev Bras Ter Intensiva. 2011;23(2):228-237
DOI 10.1590/S0103-507X2011000200017
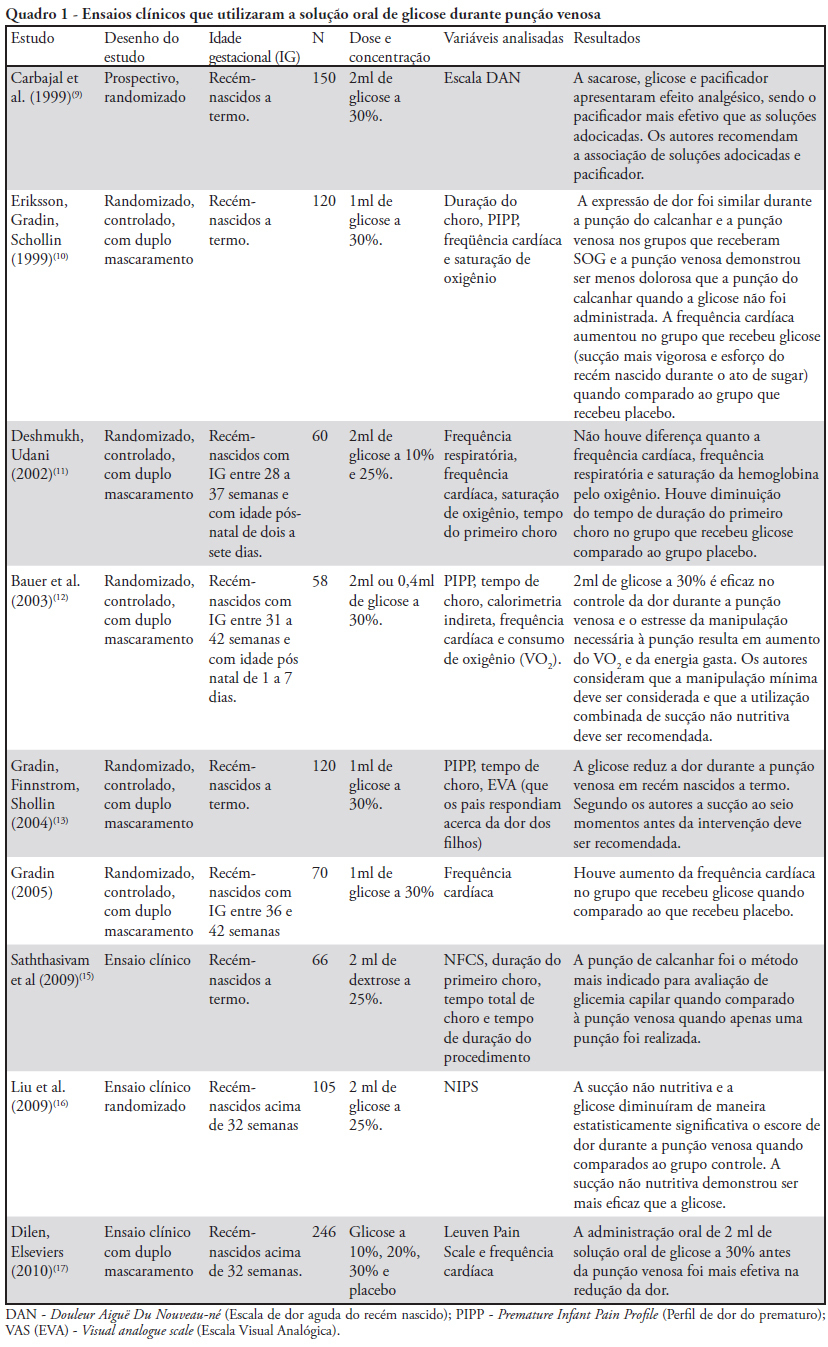
Views0See moreThis article aims to review the main studies evaluating glucose as a therapeutic alternative during mildly to moderately painful procedures in neonatology, highlighting its benefits and limitations. During their stay in neonatal intensive care units, neonates are constantly subjected to a number of painful procedures without proper therapeutic management, although the medical literature emphatically recommends this type of management, highlighting the deleterious neurological consequences of pain. Most of these interventions are frequently necessary in neonatal intensive care units to maintain clinical stability in these children; the use of systemic analgesia, however, is not considered to be a good option. The administration of oral glucose solution is apparently effective and safe for pain control during procedures causing mild-to-moderate pain in neonate intensive care units, with rare adverse effects; however, its mode of action has not yet been described clearly in the literature. The administration of oral glucose solution is well described for use in venous punctures; it is apparently effective also for heel punctures, especially when associated with nonnutritive sucking, with most studies showing favorable results.
Views0Abstract
Benefits and limitations of the use of glucose for the treatment of pain in neonates: a literature review
Rev Bras Ter Intensiva. 2011;23(2):228-237
DOI 10.1590/S0103-507X2011000200017
Views0See moreThis article aims to review the main studies evaluating glucose as a therapeutic alternative during mildly to moderately painful procedures in neonatology, highlighting its benefits and limitations. During their stay in neonatal intensive care units, neonates are constantly subjected to a number of painful procedures without proper therapeutic management, although the medical literature emphatically recommends this type of management, highlighting the deleterious neurological consequences of pain. Most of these interventions are frequently necessary in neonatal intensive care units to maintain clinical stability in these children; the use of systemic analgesia, however, is not considered to be a good option. The administration of oral glucose solution is apparently effective and safe for pain control during procedures causing mild-to-moderate pain in neonate intensive care units, with rare adverse effects; however, its mode of action has not yet been described clearly in the literature. The administration of oral glucose solution is well described for use in venous punctures; it is apparently effective also for heel punctures, especially when associated with nonnutritive sucking, with most studies showing favorable results.
-
ABDOPRE: an external device for the reduction of intra-abdominal pressure
Rev Bras Ter Intensiva. 2011;23(2):238-241
Abstract
ABDOPRE: an external device for the reduction of intra-abdominal pressure
Rev Bras Ter Intensiva. 2011;23(2):238-241
DOI 10.1590/S0103-507X2011000200018
Views0This article describes a device for the reduction of intra-abdominal pressure. The device (ABDOPRE) includes a unique external servo-control mechanism, based on urinary bladder pressure measurement. The results of ABDOPRE use in the first four intra-abdominal hypertension patients are reported; the device resulted in a reduction of intra-abdominal pressure between 16% and 35% in 3 cases and in a paradoxical increase of the intra-abdominal pressure in an obese woman, likely due to inappropriate chamber size for the patient’s anatomy. These results are promising and ABDOPRE may be useful in clinical practice.
Keywords:Abdominal cavity/physiopathologyCase reportsCompartment syndromesMonitoring, physiologic/instrumentationMonitoring, physiologic/methodsSee moreViews0Abstract
ABDOPRE: an external device for the reduction of intra-abdominal pressure
Rev Bras Ter Intensiva. 2011;23(2):238-241
DOI 10.1590/S0103-507X2011000200018
Views0This article describes a device for the reduction of intra-abdominal pressure. The device (ABDOPRE) includes a unique external servo-control mechanism, based on urinary bladder pressure measurement. The results of ABDOPRE use in the first four intra-abdominal hypertension patients are reported; the device resulted in a reduction of intra-abdominal pressure between 16% and 35% in 3 cases and in a paradoxical increase of the intra-abdominal pressure in an obese woman, likely due to inappropriate chamber size for the patient’s anatomy. These results are promising and ABDOPRE may be useful in clinical practice.
Keywords:Abdominal cavity/physiopathologyCase reportsCompartment syndromesMonitoring, physiologic/instrumentationMonitoring, physiologic/methodsSee more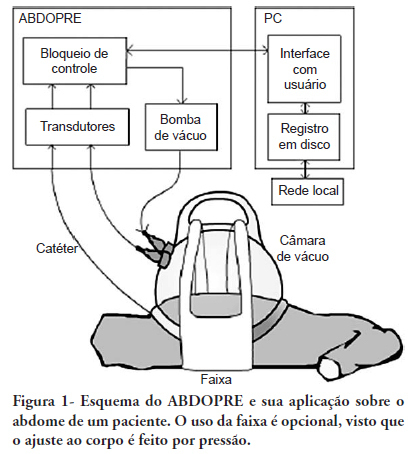
-
Levothyroxine absorption and difficult management of hypothyroid patients in the intensive care unit: two case reports and a literature review
Rev Bras Ter Intensiva. 2011;23(2):242-248
Abstract
Levothyroxine absorption and difficult management of hypothyroid patients in the intensive care unit: two case reports and a literature review
Rev Bras Ter Intensiva. 2011;23(2):242-248
DOI 10.1590/S0103-507X2011000200019
Views0See moreLevothyroxine absorption in hypothyroid patients can be influenced by several factors, particularly medications and concomitant food administration. This is especially evident in intensive care unit patients, where a continual enteral diet and the administration of multiple medications changes its absorption. Changes or adaptations in the hypothalamic-pituitary-thyroid axis, in conjunction with clinical abnormalities possibly related to under-treatment of hypothyroidism, render levothyroxine replacement therapy very challenging. Here, we report two intensive care hypothyroidism patients and their respective levothyroxine replacement management issues, focusing on a number of controversial issues, such as the optimal replacement dose, how fast the levothyroxine doses should be increased, triiodothyronine requirements, the interference of an enteral diet with absorption, and finally, the possible consequences of undertreated hypothyroidism and levothyroxine replacement monitoring useful clinical/laboratory parameters.
Views0Abstract
Levothyroxine absorption and difficult management of hypothyroid patients in the intensive care unit: two case reports and a literature review
Rev Bras Ter Intensiva. 2011;23(2):242-248
DOI 10.1590/S0103-507X2011000200019
Views0See moreLevothyroxine absorption in hypothyroid patients can be influenced by several factors, particularly medications and concomitant food administration. This is especially evident in intensive care unit patients, where a continual enteral diet and the administration of multiple medications changes its absorption. Changes or adaptations in the hypothalamic-pituitary-thyroid axis, in conjunction with clinical abnormalities possibly related to under-treatment of hypothyroidism, render levothyroxine replacement therapy very challenging. Here, we report two intensive care hypothyroidism patients and their respective levothyroxine replacement management issues, focusing on a number of controversial issues, such as the optimal replacement dose, how fast the levothyroxine doses should be increased, triiodothyronine requirements, the interference of an enteral diet with absorption, and finally, the possible consequences of undertreated hypothyroidism and levothyroxine replacement monitoring useful clinical/laboratory parameters.
Volume Articles - Critical Care Science (CCS)
