Rats, Wistar Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2014;26(3):277-286
DOI 10.5935/0103-507X.20140039
We investigated the effect of two different saline solutions on the mechanisms of injury after intestinal ischemia: oxidative stress and inflammatory responses.
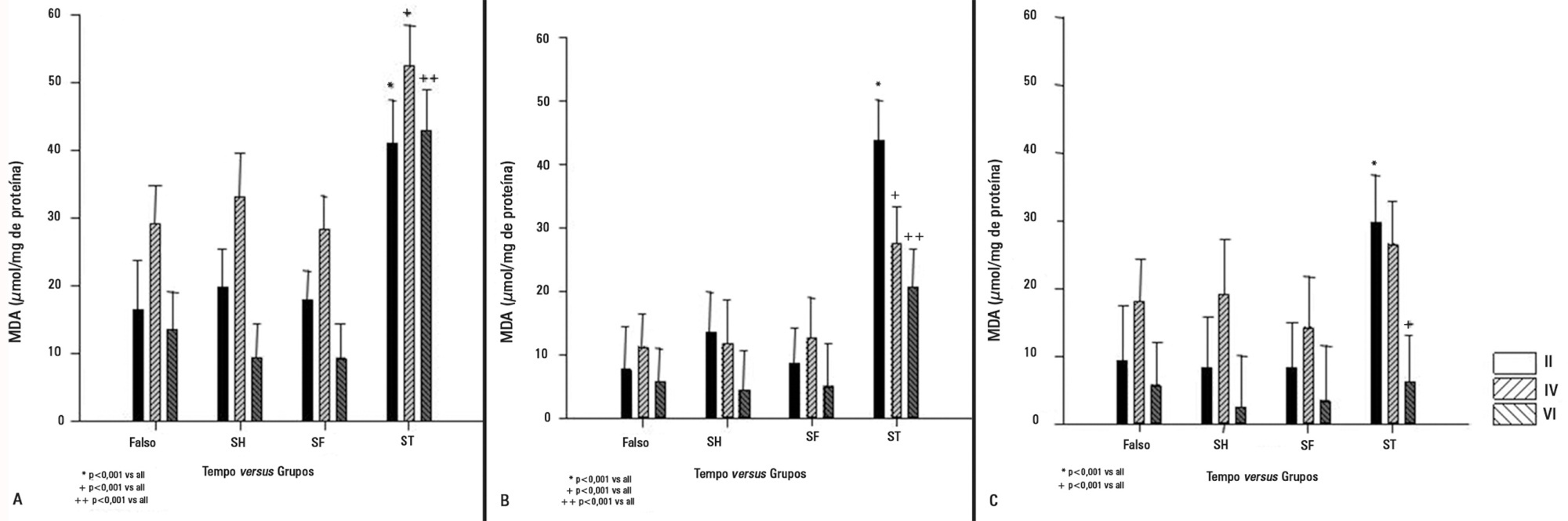
Wistar rats underwent transient superior mesenteric artery occlusion and were studied for 6 hours after reperfusion. After randomization, the animals were divided into four groups: Sham; Hypertonic Saline, in which they received infusion of 4mL/kg body weight of 7.5% hypertonic saline; Saline, in which they received infusion of 33mL/kg body weight of 0.9% saline; and Non Treatment. The infusion was performed immediately prior to the reperfusion. The plasma concentrations of interleukin 6 and interleukin 10 were measured. Tissue samples (lung, liver, and intestine) were collected for malondialdehyde, myeloperoxidase, and interleukin measurements.
The animals that received infusions (Hypertonic Saline and Saline) showed lower levels of tissue malondialdehyde, myeloperoxidase, interleukin 6, and interleukin 10 compared with the Non Treatment group. The plasma concentrations of interleukin 6 and interleukin 10 were higher in the animals treated with 7.5% hypertonic saline compared with Saline and Non Treatment groups.
In this model of transient intestinal ischemia, the adequate maintenance of intravascular volume decreased oxidative stress and the synthesis of inflammatory markers. Both 7.5% Hypertonic Saline and Saline attenuated the deleterious effects observed after intestinal ischemia.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):277-286
DOI 10.5935/0103-507X.20140039
We investigated the effect of two different saline solutions on the mechanisms of injury after intestinal ischemia: oxidative stress and inflammatory responses.
Wistar rats underwent transient superior mesenteric artery occlusion and were studied for 6 hours after reperfusion. After randomization, the animals were divided into four groups: Sham; Hypertonic Saline, in which they received infusion of 4mL/kg body weight of 7.5% hypertonic saline; Saline, in which they received infusion of 33mL/kg body weight of 0.9% saline; and Non Treatment. The infusion was performed immediately prior to the reperfusion. The plasma concentrations of interleukin 6 and interleukin 10 were measured. Tissue samples (lung, liver, and intestine) were collected for malondialdehyde, myeloperoxidase, and interleukin measurements.
The animals that received infusions (Hypertonic Saline and Saline) showed lower levels of tissue malondialdehyde, myeloperoxidase, interleukin 6, and interleukin 10 compared with the Non Treatment group. The plasma concentrations of interleukin 6 and interleukin 10 were higher in the animals treated with 7.5% hypertonic saline compared with Saline and Non Treatment groups.
In this model of transient intestinal ischemia, the adequate maintenance of intravascular volume decreased oxidative stress and the synthesis of inflammatory markers. Both 7.5% Hypertonic Saline and Saline attenuated the deleterious effects observed after intestinal ischemia.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):158-163
DOI 10.1590/S0103-507X2011000200007
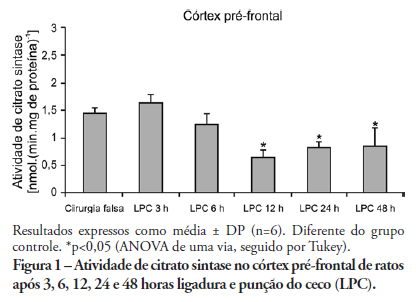
OBJECTIVE: An extensive body of evidence from experimental studies indicates that sepsis is associated with increased reactive oxygen species production, depletion of antioxidants, and accumulation of markers of oxidative stress. Moreover, mitochondrial dysfunction has been implicated in the pathogenesis of multiple organ dysfunction syndrome (MODS). Citrate synthase is an enzyme localized in the mitochondrial matrix and an important component of the Krebs cycle; consequently, citrate synthase has been used as a quantitative enzyme marker for the presence of intact mitochondria. Thus, we investigated citrate synthase activity in the brains of rats submitted to a cecal ligation puncture model of sepsis. METHODS: At several times points (3, 6, 12, 24 and 48 hours) after the cecal ligation puncture operation, six rats were killed by decapitation. Their brains were removed, and the hippocampus, striatum, cerebellum, cerebral cortex and prefrontal cortex were dissected and used to determine citrate synthase activity. RESULTS: We found that citrate synthase activity in the prefrontal cortex was inhibited 12, 24 and 48 hours after cecal ligation puncture. In the cerebral cortex, citrate synthase activity was inhibited 3, 12, 24 and 48 hours after cecal ligation puncture. Citrate synthase was not affected in the hippocampus, striatum or cerebellum up to 48 hours after cecal ligation puncture. CONCLUSION: Considering that energy impairment due to mitochondrial dysfunction in sepsis has been well described and that oxidative stress plays a crucial role in sepsis development, we believe that energy impairment may also be involved in these processes. If citrate synthase inhibition also occurs in a sepsis model, it is tempting to speculate that a reduction in brain metabolism may be related to the pathophysiology of this disease.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):158-163
DOI 10.1590/S0103-507X2011000200007
OBJECTIVE: An extensive body of evidence from experimental studies indicates that sepsis is associated with increased reactive oxygen species production, depletion of antioxidants, and accumulation of markers of oxidative stress. Moreover, mitochondrial dysfunction has been implicated in the pathogenesis of multiple organ dysfunction syndrome (MODS). Citrate synthase is an enzyme localized in the mitochondrial matrix and an important component of the Krebs cycle; consequently, citrate synthase has been used as a quantitative enzyme marker for the presence of intact mitochondria. Thus, we investigated citrate synthase activity in the brains of rats submitted to a cecal ligation puncture model of sepsis. METHODS: At several times points (3, 6, 12, 24 and 48 hours) after the cecal ligation puncture operation, six rats were killed by decapitation. Their brains were removed, and the hippocampus, striatum, cerebellum, cerebral cortex and prefrontal cortex were dissected and used to determine citrate synthase activity. RESULTS: We found that citrate synthase activity in the prefrontal cortex was inhibited 12, 24 and 48 hours after cecal ligation puncture. In the cerebral cortex, citrate synthase activity was inhibited 3, 12, 24 and 48 hours after cecal ligation puncture. Citrate synthase was not affected in the hippocampus, striatum or cerebellum up to 48 hours after cecal ligation puncture. CONCLUSION: Considering that energy impairment due to mitochondrial dysfunction in sepsis has been well described and that oxidative stress plays a crucial role in sepsis development, we believe that energy impairment may also be involved in these processes. If citrate synthase inhibition also occurs in a sepsis model, it is tempting to speculate that a reduction in brain metabolism may be related to the pathophysiology of this disease.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):321-326
DOI 10.1590/S0103-507X2010000400002
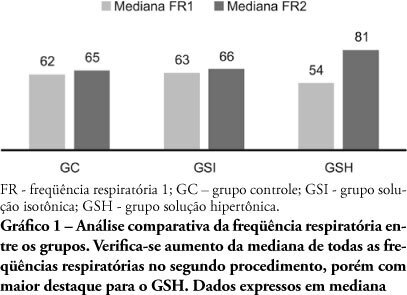
PURPOSE: Sepsis severity and mortality risk require aggressive therapy which includes hemodynamic support. The best fluid for volume replacement, however, is controversial. This study aimed to compare 0.9% isotonic saline solution versus 7.5% hypertonic saline solution as volume replacement fluid in sepsis induced by cecum ligation plus puncture rats. METHODS: This experimental trial included 30 rats divided into three groups: Control group (CG, n = 10), isotonic (ISG, n = 10) and hypertonic solution (HSG, n = 10). Fifteen hours after cecum ligation and puncture, all animals underwent respiratory rate, mean arterial pressure, renal and hepatic blood flow and weight evaluation, plus blood collection for TNF-α measurement. The ISG and HSG treatment groups received volume replacement 60 minutes before the procedure with either 0.9% or 7.5% saline solution, respectively. RESULTS: Two animals died. Significant differences were found for the animals' mean weight after 15 hours (p=0.018), particularly relevant when ISG and HSG are compared (p=0.003). Renal blood flow was also significantly different for the CG versus HSG (p=0.002) and CG versus ISG (p=0.008), but not significantly different for ISG versus HSG. No mean arterial pressure improvement was found for HSG (0.054). Other variables were not significant. CONCLUSIONS: Although no mean blood pressure, hepatic flow or TNF-α improvements were detected, the rats with sepsis 15 hours after cecum ligation and puncture showed significantly increased renal blood flow which was 0.9% isotonic saline solution or of 7.5% hypertonic solution use independent.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):321-326
DOI 10.1590/S0103-507X2010000400002
PURPOSE: Sepsis severity and mortality risk require aggressive therapy which includes hemodynamic support. The best fluid for volume replacement, however, is controversial. This study aimed to compare 0.9% isotonic saline solution versus 7.5% hypertonic saline solution as volume replacement fluid in sepsis induced by cecum ligation plus puncture rats. METHODS: This experimental trial included 30 rats divided into three groups: Control group (CG, n = 10), isotonic (ISG, n = 10) and hypertonic solution (HSG, n = 10). Fifteen hours after cecum ligation and puncture, all animals underwent respiratory rate, mean arterial pressure, renal and hepatic blood flow and weight evaluation, plus blood collection for TNF-α measurement. The ISG and HSG treatment groups received volume replacement 60 minutes before the procedure with either 0.9% or 7.5% saline solution, respectively. RESULTS: Two animals died. Significant differences were found for the animals' mean weight after 15 hours (p=0.018), particularly relevant when ISG and HSG are compared (p=0.003). Renal blood flow was also significantly different for the CG versus HSG (p=0.002) and CG versus ISG (p=0.008), but not significantly different for ISG versus HSG. No mean arterial pressure improvement was found for HSG (0.054). Other variables were not significant. CONCLUSIONS: Although no mean blood pressure, hepatic flow or TNF-α improvements were detected, the rats with sepsis 15 hours after cecum ligation and puncture showed significantly increased renal blood flow which was 0.9% isotonic saline solution or of 7.5% hypertonic solution use independent.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):245-249
DOI 10.1590/S0103-507X2010000300005
OBJECTIVE: Ischemic acute kidney injury (iLRA), with multifatorial cause, presents alarming morbidity and mortality. Statin, HMG-CoA inhibition reductase has shown a renoprotective effect, with antioxidant, antiinflamatory and vascular actions. The heme oxygenase-1 (HO-1) can be involved in these pleitropic effects of statin on the renal function. This study was performed in order to evaluate if the renoprotective effect of the statin is a heme mechanism of protection in rats. METHODS: The ischemic model was reproduced by through clamping the bilateral renal pedicles for 30 minutes followed by reperfusion. Adult Wistar rats, weighting from 250-300g, were divided into the following groups: SHAM (control); Ischemia (30 minutes renal ischemia); Ischemia+Statin (sinvastatin 0.5mg/kg,orally (v.o.) for 3 days); Ischemia+Hemin (Hemin, 1.0mg/100g, intraperitoneal (i.p.), 24 hours before surgery); Ischemia+SnPP (SnPP 2μmol/kg, i.p., 24 hours before surgery ); Ischemia+Statin+Hemin; Ischemia+Statin+SnPP. RF (clearance of creatinine, Jaffé method), urinary peroxides (UP), urinary osmolality (UO) and immunohistochemical for ED-1 were evaluated. RESULTS: Results showed that sinvastatin ameliorated RF, urinary osmolality, reduced the UP excrection and the macrophage infiltration in rats submitted to renal ischemia. The inducer of HO-1 and its association with sinvastatin induced a similar pattern of improvement of renal function. CONCLUSION: the study confirmed the renoprotective effect of the statins on renal function, with antioxidant and antiinflamatory actions, and it suggests that this effect can have an interface with the heme system of renal protection.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):245-249
DOI 10.1590/S0103-507X2010000300005
OBJECTIVE: Ischemic acute kidney injury (iLRA), with multifatorial cause, presents alarming morbidity and mortality. Statin, HMG-CoA inhibition reductase has shown a renoprotective effect, with antioxidant, antiinflamatory and vascular actions. The heme oxygenase-1 (HO-1) can be involved in these pleitropic effects of statin on the renal function. This study was performed in order to evaluate if the renoprotective effect of the statin is a heme mechanism of protection in rats. METHODS: The ischemic model was reproduced by through clamping the bilateral renal pedicles for 30 minutes followed by reperfusion. Adult Wistar rats, weighting from 250-300g, were divided into the following groups: SHAM (control); Ischemia (30 minutes renal ischemia); Ischemia+Statin (sinvastatin 0.5mg/kg,orally (v.o.) for 3 days); Ischemia+Hemin (Hemin, 1.0mg/100g, intraperitoneal (i.p.), 24 hours before surgery); Ischemia+SnPP (SnPP 2μmol/kg, i.p., 24 hours before surgery ); Ischemia+Statin+Hemin; Ischemia+Statin+SnPP. RF (clearance of creatinine, Jaffé method), urinary peroxides (UP), urinary osmolality (UO) and immunohistochemical for ED-1 were evaluated. RESULTS: Results showed that sinvastatin ameliorated RF, urinary osmolality, reduced the UP excrection and the macrophage infiltration in rats submitted to renal ischemia. The inducer of HO-1 and its association with sinvastatin induced a similar pattern of improvement of renal function. CONCLUSION: the study confirmed the renoprotective effect of the statins on renal function, with antioxidant and antiinflamatory actions, and it suggests that this effect can have an interface with the heme system of renal protection.