Respiratory insufficiency Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2017;29(2):180-187
DOI 10.5935/0103-507X.20170028
To analyze patients after cardiac surgery that needed endotracheal reintubation and identify factors associated with death and its relation with the severity scores.
Retrospective analysis of information of 1,640 patients in the postoperative period of cardiac surgery between 2007 and 2015.
The reintubation rate was 7.26%. Of those who were reintubated, 36 (30.3%) underwent coronary artery bypass surgery, 27 (22.7%) underwent valve replacement, 25 (21.0%) underwent correction of an aneurysm, and 8 (6.7%) underwent a heart transplant. Among those with comorbidities, 54 (51.9%) were hypertensive, 22 (21.2%) were diabetic, and 10 (9.6%) had lung diseases. Among those who had complications, 61 (52.6%) had pneumonia, 50 (42.4%) developed renal failure, and 49 (51.0%) had a moderate form of the transient disturbance of gas exchange. Noninvasive ventilation was performed in 53 (44.5%) patients. The death rate was 40.3%, and mortality was higher in the group that did not receive noninvasive ventilation before reintubation (53.5%). Within the reintubated patients who died, the SOFA and APACHE II values were 7.9 ± 3.0 and 16.9 ± 4.5, respectively. Most of the reintubated patients (47.5%) belonged to the high-risk group, EuroSCORE (> 6 points).
The reintubation rate was high, and it was related to worse SOFA, APACHE II and EuroSCORE scores. Mortality was higher in the group that did not receive noninvasive ventilation before reintubation.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):180-187
DOI 10.5935/0103-507X.20170028
To analyze patients after cardiac surgery that needed endotracheal reintubation and identify factors associated with death and its relation with the severity scores.
Retrospective analysis of information of 1,640 patients in the postoperative period of cardiac surgery between 2007 and 2015.
The reintubation rate was 7.26%. Of those who were reintubated, 36 (30.3%) underwent coronary artery bypass surgery, 27 (22.7%) underwent valve replacement, 25 (21.0%) underwent correction of an aneurysm, and 8 (6.7%) underwent a heart transplant. Among those with comorbidities, 54 (51.9%) were hypertensive, 22 (21.2%) were diabetic, and 10 (9.6%) had lung diseases. Among those who had complications, 61 (52.6%) had pneumonia, 50 (42.4%) developed renal failure, and 49 (51.0%) had a moderate form of the transient disturbance of gas exchange. Noninvasive ventilation was performed in 53 (44.5%) patients. The death rate was 40.3%, and mortality was higher in the group that did not receive noninvasive ventilation before reintubation (53.5%). Within the reintubated patients who died, the SOFA and APACHE II values were 7.9 ± 3.0 and 16.9 ± 4.5, respectively. Most of the reintubated patients (47.5%) belonged to the high-risk group, EuroSCORE (> 6 points).
The reintubation rate was high, and it was related to worse SOFA, APACHE II and EuroSCORE scores. Mortality was higher in the group that did not receive noninvasive ventilation before reintubation.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):212-219
DOI 10.5935/0103-507X.20150034
To evaluate the clinical characteristics of patients with hematological disease admitted to the intensive care unit and the use of noninvasive mechanical ventilation in a subgroup with respiratory dysfunction.
A retrospective observational study from September 2011 to January 2014.
Overall, 157 patients were included. The mean age was 45.13 (± 17.2) years and 46.5% of the patients were female. Sixty-seven (48.4%) patients had sepsis, and 90 (57.3%) patients required vasoactive vasopressors. The main cause for admission to the intensive care unit was acute respiratory failure (94.3%). Among the 157 studied patients, 47 (29.9%) were intubated within the first 24 hours, and 38 (24.2%) underwent noninvasive mechanical ventilation. Among the 38 patients who initially received noninvasive mechanical ventilation, 26 (68.4%) were subsequently intubated, and 12 (31.6%) responded to this mode of ventilation. Patients who failed to respond to noninvasive mechanical ventilation had higher intensive care unit mortality (66.7% versus 16.7%; p = 0.004) and a longer stay in the intensive care unit (9.6 days versus 4.6 days, p = 0.02) compared with the successful cases. Baseline severity scores (SOFA and SAPS 3) and the total leukocyte count were not significantly different between these two subgroups. In a multivariate logistic regression model including the 157 patients, intubation at any time during the stay in the intensive care unit and SAPS 3 were independently associated with intensive care unit mortality, while using noninvasive mechanical ventilation was not.
In this retrospective study with severely ill hematologic patients, those who underwent noninvasive mechanical ventilation at admission and failed to respond to it presented elevated intensive care unit mortality. However, only intubation during the intensive care unit stay was independently associated with a poor outcome. Further studies are needed to define predictors of noninvasive mechanical ventilation failure.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):212-219
DOI 10.5935/0103-507X.20150034
To evaluate the clinical characteristics of patients with hematological disease admitted to the intensive care unit and the use of noninvasive mechanical ventilation in a subgroup with respiratory dysfunction.
A retrospective observational study from September 2011 to January 2014.
Overall, 157 patients were included. The mean age was 45.13 (± 17.2) years and 46.5% of the patients were female. Sixty-seven (48.4%) patients had sepsis, and 90 (57.3%) patients required vasoactive vasopressors. The main cause for admission to the intensive care unit was acute respiratory failure (94.3%). Among the 157 studied patients, 47 (29.9%) were intubated within the first 24 hours, and 38 (24.2%) underwent noninvasive mechanical ventilation. Among the 38 patients who initially received noninvasive mechanical ventilation, 26 (68.4%) were subsequently intubated, and 12 (31.6%) responded to this mode of ventilation. Patients who failed to respond to noninvasive mechanical ventilation had higher intensive care unit mortality (66.7% versus 16.7%; p = 0.004) and a longer stay in the intensive care unit (9.6 days versus 4.6 days, p = 0.02) compared with the successful cases. Baseline severity scores (SOFA and SAPS 3) and the total leukocyte count were not significantly different between these two subgroups. In a multivariate logistic regression model including the 157 patients, intubation at any time during the stay in the intensive care unit and SAPS 3 were independently associated with intensive care unit mortality, while using noninvasive mechanical ventilation was not.
In this retrospective study with severely ill hematologic patients, those who underwent noninvasive mechanical ventilation at admission and failed to respond to it presented elevated intensive care unit mortality. However, only intubation during the intensive care unit stay was independently associated with a poor outcome. Further studies are needed to define predictors of noninvasive mechanical ventilation failure.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):134-140
DOI 10.5935/0103-507X.20150024
The development of the extracorporeal membrane oxygenation in Latin America represents a challenge in this specialty field. The objective of this article was to describe the results of a new extracorporeal membrane oxygenation program in an intensive care unit.
This retrospective cohort study included 22 patients who required extracorporeal membrane oxygenation and were treated from January 2011 to June 2014. The baseline characteristics, indications, duration of the condition, days on mechanical ventilation, days in the intensive care unit, complications, and hospital mortality were evaluated.
Fifteen patients required extracorporeal membrane oxygenation after lung transplantation, and seven patients required oxygenation due to acute respiratory distress. All transplanted patients were weaned from extracorporeal membrane oxygenation with a median duration of 3 days (Interquartile range - IQR: 2 - 5), were on mechanical ventilation for a median of 15.5 days (IQR: 3 - 25), and had an intensive care unit stay of 31.5 days (IQR: 19 - 53) and a median hospital stay of 60 days (IQR: 36 - 89) with 20% mortality. Patients with acute respiratory distress had a median oxygenation membrane duration of 9 days (IQR: 3 - 14), median mechanical ventilation time of 25 days (IQR: 13 - 37), a 31 day stay in therapy (IQR: 11 - 38), a 32 day stay in the hospital (IQR: 11 - 41), and 57% mortality. The main complications were infections (80%), acute kidney failure (43%), bleeding at the surgical site and at the site of cannula placement (22%), plateletopenia (60%), and coagulopathy (30%).
In spite of the steep learning curve, we considered this experience to be satisfactory, with results and complications comparable to those reported in the literature.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):134-140
DOI 10.5935/0103-507X.20150024
The development of the extracorporeal membrane oxygenation in Latin America represents a challenge in this specialty field. The objective of this article was to describe the results of a new extracorporeal membrane oxygenation program in an intensive care unit.
This retrospective cohort study included 22 patients who required extracorporeal membrane oxygenation and were treated from January 2011 to June 2014. The baseline characteristics, indications, duration of the condition, days on mechanical ventilation, days in the intensive care unit, complications, and hospital mortality were evaluated.
Fifteen patients required extracorporeal membrane oxygenation after lung transplantation, and seven patients required oxygenation due to acute respiratory distress. All transplanted patients were weaned from extracorporeal membrane oxygenation with a median duration of 3 days (Interquartile range - IQR: 2 - 5), were on mechanical ventilation for a median of 15.5 days (IQR: 3 - 25), and had an intensive care unit stay of 31.5 days (IQR: 19 - 53) and a median hospital stay of 60 days (IQR: 36 - 89) with 20% mortality. Patients with acute respiratory distress had a median oxygenation membrane duration of 9 days (IQR: 3 - 14), median mechanical ventilation time of 25 days (IQR: 13 - 37), a 31 day stay in therapy (IQR: 11 - 38), a 32 day stay in the hospital (IQR: 11 - 41), and 57% mortality. The main complications were infections (80%), acute kidney failure (43%), bleeding at the surgical site and at the site of cannula placement (22%), plateletopenia (60%), and coagulopathy (30%).
In spite of the steep learning curve, we considered this experience to be satisfactory, with results and complications comparable to those reported in the literature.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):390-396
DOI 10.5935/0103-507X.20150065
To evaluate the quality of available evidence to establish guidelines for the use of noninvasive ventilation for the management of status asthmaticus in children unresponsive to standard treatment.
Search, selection and analysis of all original articles on asthma and noninvasive ventilation in children, published until September 1, 2014 in all languages in the electronic databases PubMed, Web of Science, Cochrane Library, Scopus and SciELO, located using the search terms: "asthma", "status asthmaticus", "noninvasive ventilation", "Bronchospasm", "continuous positive airway pressure", "child", "infant", "pediatrics", "hypercapnia", "respiratory failure" and the keywords "BIPAP", "CPAP", "Bilevel", "acute asthma" and "near fatal asthma". The articles were assessed based on the levels of evidence of the GRADE system.
Only nine original articles were located; two (22%) articles had level of evidence A, one (11%) had level of evidence B and six (67%) had level of evidence C.
The results suggest that noninvasive ventilation is applicable for the treatment of status asthmaticus in most pediatric patients unresponsive to standard treatment. However, the available evidence cannot be considered as conclusive, as further high-quality research is likely to have an impact on and change the estimate of the effect.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):390-396
DOI 10.5935/0103-507X.20150065
To evaluate the quality of available evidence to establish guidelines for the use of noninvasive ventilation for the management of status asthmaticus in children unresponsive to standard treatment.
Search, selection and analysis of all original articles on asthma and noninvasive ventilation in children, published until September 1, 2014 in all languages in the electronic databases PubMed, Web of Science, Cochrane Library, Scopus and SciELO, located using the search terms: "asthma", "status asthmaticus", "noninvasive ventilation", "Bronchospasm", "continuous positive airway pressure", "child", "infant", "pediatrics", "hypercapnia", "respiratory failure" and the keywords "BIPAP", "CPAP", "Bilevel", "acute asthma" and "near fatal asthma". The articles were assessed based on the levels of evidence of the GRADE system.
Only nine original articles were located; two (22%) articles had level of evidence A, one (11%) had level of evidence B and six (67%) had level of evidence C.
The results suggest that noninvasive ventilation is applicable for the treatment of status asthmaticus in most pediatric patients unresponsive to standard treatment. However, the available evidence cannot be considered as conclusive, as further high-quality research is likely to have an impact on and change the estimate of the effect.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
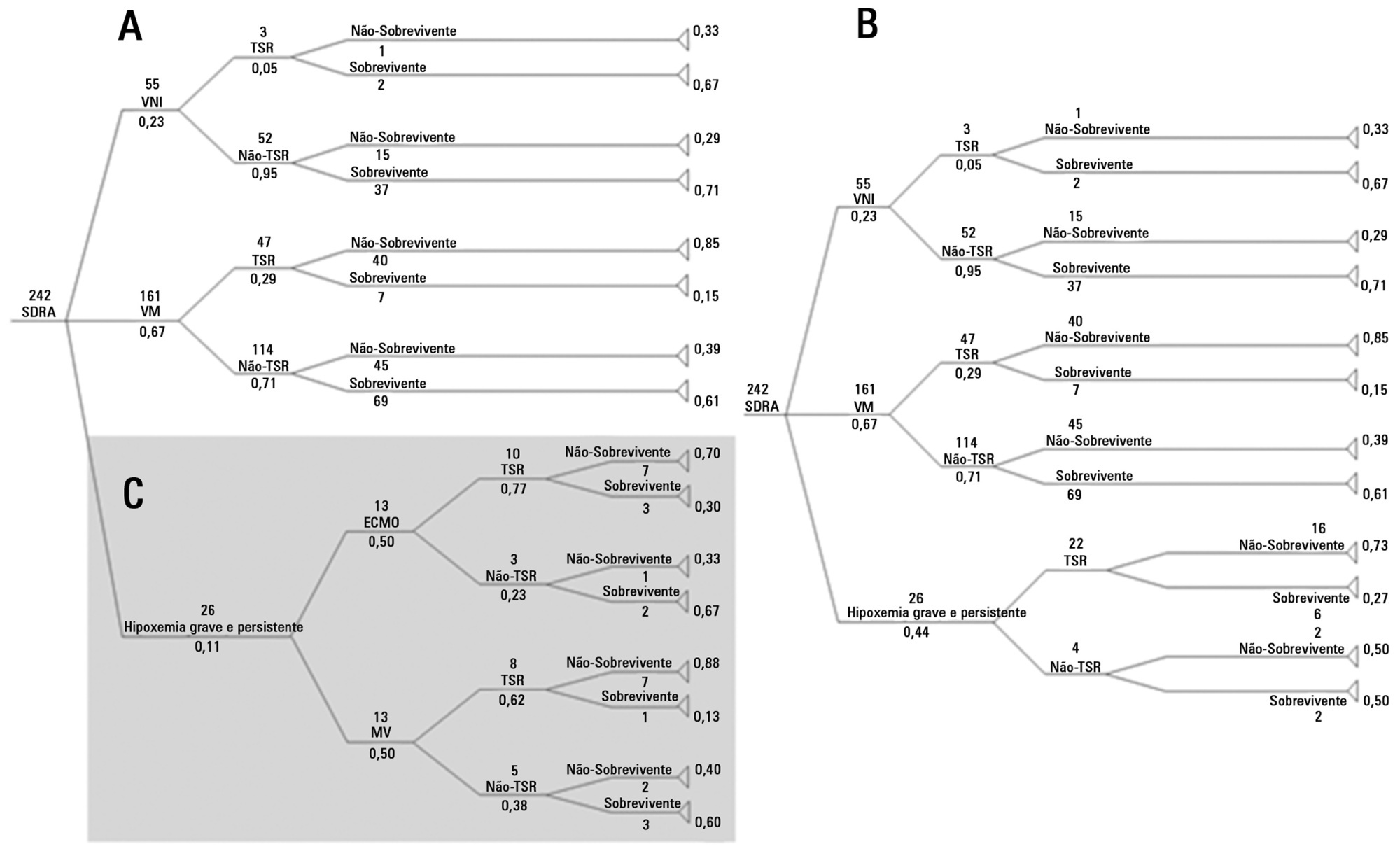
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):313-316
DOI 10.5935/0103-507X.20140044
We describe herein a case of a patient who, when in orthostatic positions, had severe hypoxemia and ventilatory dysfunction. Although the severity of symptoms required hospitalization in an intensive care setting, the initial tests only identified the presence of enlarged aortic root, which did not explain the condition. The association of these events with an unusual etiology, namely intracardiac shunt, characterized the diagnosis of platypnea-orthodeoxia syndrome. The literature review shows that, with advancing research methods, there was a progressive increase in the identification of this condition, and this association should be part of the differential diagnosis of dyspnea in patients with enlarged aortic root.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):313-316
DOI 10.5935/0103-507X.20140044
We describe herein a case of a patient who, when in orthostatic positions, had severe hypoxemia and ventilatory dysfunction. Although the severity of symptoms required hospitalization in an intensive care setting, the initial tests only identified the presence of enlarged aortic root, which did not explain the condition. The association of these events with an unusual etiology, namely intracardiac shunt, characterized the diagnosis of platypnea-orthodeoxia syndrome. The literature review shows that, with advancing research methods, there was a progressive increase in the identification of this condition, and this association should be part of the differential diagnosis of dyspnea in patients with enlarged aortic root.

Abstract
Rev Bras Ter Intensiva. 2013;25(2):130-136
DOI 10.5935/0103-507X.20130024
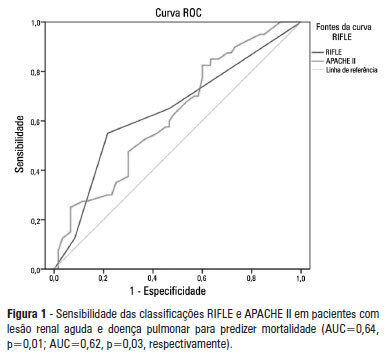
OBJECTIVE: To examine the factors associated with acute kidney injury and outcome in patients with lung disease. METHODS: A prospective study was conducted with 100 consecutive patients admitted to a respiratory intensive care unit in Fortaleza (CE), Brazil. The risk factors for acute kidney injury and mortality were investigated in a group of patients with lung diseases. RESULTS: The mean age of the study population was 57 years, and 50% were male. The incidence of acute kidney injury was higher in patients with PaO2/FiO2<200 mmHg (54% versus 23.7%; p=0.02). Death was observed in 40 cases and the rate of mortality of the acute kidney injury group was higher (62.8% versus 27.6%; p=0.01). The independent factor that was found to be associated with acute kidney injury was PaO2/FiO2<200 mmHg (p=0.01), and the independent risk factors for death were PEEP at admission (OR: 3.6; 95%CI: 1.3-9.6; p=0.009) and need for hemodialysis (OR: 7.9; 95%CI: 2.2-28.3; p=0.001). CONCLUSION: There was a higher mortality rate in the acute kidney injury group. Increased mortality was associated with mechanical ventilation, high PEEP, urea and need for dialysis. Further studies must be performed to better establish the relationship between kidney and lung injury and its impact on patient outcome.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):130-136
DOI 10.5935/0103-507X.20130024
OBJECTIVE: To examine the factors associated with acute kidney injury and outcome in patients with lung disease. METHODS: A prospective study was conducted with 100 consecutive patients admitted to a respiratory intensive care unit in Fortaleza (CE), Brazil. The risk factors for acute kidney injury and mortality were investigated in a group of patients with lung diseases. RESULTS: The mean age of the study population was 57 years, and 50% were male. The incidence of acute kidney injury was higher in patients with PaO2/FiO2<200 mmHg (54% versus 23.7%; p=0.02). Death was observed in 40 cases and the rate of mortality of the acute kidney injury group was higher (62.8% versus 27.6%; p=0.01). The independent factor that was found to be associated with acute kidney injury was PaO2/FiO2<200 mmHg (p=0.01), and the independent risk factors for death were PEEP at admission (OR: 3.6; 95%CI: 1.3-9.6; p=0.009) and need for hemodialysis (OR: 7.9; 95%CI: 2.2-28.3; p=0.001). CONCLUSION: There was a higher mortality rate in the acute kidney injury group. Increased mortality was associated with mechanical ventilation, high PEEP, urea and need for dialysis. Further studies must be performed to better establish the relationship between kidney and lung injury and its impact on patient outcome.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):415-419
DOI 10.1590/S0103-507X2012000400020
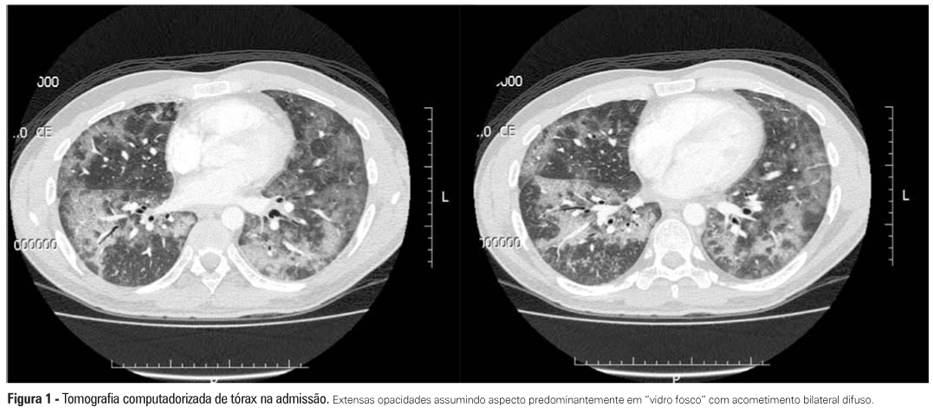
Interstitial lung diseases belong to a group of diseases that typically exhibit a subacute or chronic progression but that may cause acute respiratory failure. The male patient, who was 37 years of age and undergoing therapy for non-Hodgkin's lymphoma, was admitted with cough, fever, dyspnea and acute hypoxemic respiratory failure. Mechanical ventilation and antibiotic therapy were initiated but were associated with unfavorable progression. Thoracic computed tomography showed bilateral pulmonary "ground glass" opacities. Methylprednisolone pulse therapy was initiated with satisfactory response because the patient had used three drugs related to organizing pneumonia (cyclophosphamide, doxorubicin and rituximab), and the clinical and radiological symptoms were suggestive. Organizing pneumonia may be idiopathic or linked to collagen diseases, drugs and cancer and usually responds to corticosteroid therapy. The diagnosis was anatomopathological, but the patient's clinical condition precluded performing a lung biopsy. Organizing pneumonia should be a differential diagnosis in patients with apparent pneumonia and a progression that is unfavorable to antimicrobial treatment.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):415-419
DOI 10.1590/S0103-507X2012000400020
Interstitial lung diseases belong to a group of diseases that typically exhibit a subacute or chronic progression but that may cause acute respiratory failure. The male patient, who was 37 years of age and undergoing therapy for non-Hodgkin's lymphoma, was admitted with cough, fever, dyspnea and acute hypoxemic respiratory failure. Mechanical ventilation and antibiotic therapy were initiated but were associated with unfavorable progression. Thoracic computed tomography showed bilateral pulmonary "ground glass" opacities. Methylprednisolone pulse therapy was initiated with satisfactory response because the patient had used three drugs related to organizing pneumonia (cyclophosphamide, doxorubicin and rituximab), and the clinical and radiological symptoms were suggestive. Organizing pneumonia may be idiopathic or linked to collagen diseases, drugs and cancer and usually responds to corticosteroid therapy. The diagnosis was anatomopathological, but the patient's clinical condition precluded performing a lung biopsy. Organizing pneumonia should be a differential diagnosis in patients with apparent pneumonia and a progression that is unfavorable to antimicrobial treatment.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)