mechanical ventilation Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2009;21(1):96-103
DOI 10.1590/S0103-507X2009000100014
This article intends to review literature on high frequency oscillatory ventilation and describe its main clinical applications for children and neonates. Articles from the last 15 years were selected using MedLine and SciElo databases. The following key words were used: high frequency oscillatory ventilation, mechanical ventilation, acute respiratory distress syndrome, children, and new-born. The review describes high frequency oscillatory ventilation in children with acute respiratory distress syndrome, air leak syndrome, and obstructive lung disease. Respiratory distress syndrome, bronchopulmonary dysplasia, intracranial hemorrhage, periventricular leukomalacia, and air leak syndrome were reviewed in neonates. Transition from conventional mechanical ventilation to high frequency ventilation and its adjustments relating to oxygenation, CO2 elimination, chest radiography, suctioning, sedatives and use of neuromuscular blocking agents were described. Weaning and complications were also reported. For children, high frequency oscillatory ventilation is a therapeutic option, particularly in acute respiratory distress syndrome, and should be used as early as possible. It may be also useful in the air leak syndrome and obstructive pulmonary disease. Evidence that, in neonates, high frequency oscillatory ventilation is superior to conventional mechanical ventilation is lacking. However there is evidence that better results are only achieved with this ventilatory mode to manage the air leak syndrome.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):96-103
DOI 10.1590/S0103-507X2009000100014
This article intends to review literature on high frequency oscillatory ventilation and describe its main clinical applications for children and neonates. Articles from the last 15 years were selected using MedLine and SciElo databases. The following key words were used: high frequency oscillatory ventilation, mechanical ventilation, acute respiratory distress syndrome, children, and new-born. The review describes high frequency oscillatory ventilation in children with acute respiratory distress syndrome, air leak syndrome, and obstructive lung disease. Respiratory distress syndrome, bronchopulmonary dysplasia, intracranial hemorrhage, periventricular leukomalacia, and air leak syndrome were reviewed in neonates. Transition from conventional mechanical ventilation to high frequency ventilation and its adjustments relating to oxygenation, CO2 elimination, chest radiography, suctioning, sedatives and use of neuromuscular blocking agents were described. Weaning and complications were also reported. For children, high frequency oscillatory ventilation is a therapeutic option, particularly in acute respiratory distress syndrome, and should be used as early as possible. It may be also useful in the air leak syndrome and obstructive pulmonary disease. Evidence that, in neonates, high frequency oscillatory ventilation is superior to conventional mechanical ventilation is lacking. However there is evidence that better results are only achieved with this ventilatory mode to manage the air leak syndrome.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):149-153
DOI 10.1590/S0103-507X2008000200006
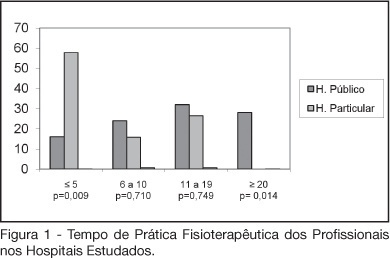
BACKGROUND AND OBJECTIVES: The number of patients requiring prolonged time on mechanical ventilation is increasing considerably in the intensive care unit (ICU). The objective of this study was to characterize the variability of methods and criteria used by physiotherapists to obtain weaning parameters in hospitals of Fortaleza. METHODS: After approval by the UNIFOR Ethics Committee, survey questionnaires were distributed among physiotherapists working in the ICU of three public and three private hospitals. Forty-four physiotherapists answered thirty-two multiple choice questions anonymously. RESULTS: The main results concerned parameters commonly evaluated by physiotherapists. A significant difference between hospitals was found regarding the rapid shallow breathing index and maximum inspiratory pressure, which are more often used in private hospitals, with a percentage of 100% and 89.5%, respectively. Concerning the ventilatory mode for obtaining the weaning parameters for mechanical ventilation; the T-tube was the most used, not only in the public (56%) but also in the private hospitals (57.9%). CONCLUSIONS: Variability in the methods and criteria used to obtain weaning parameters by the physiotherapists was found in public and private hospitals in Fortaleza. Results from this survey stress the need to develop new scientific studies to standardize the techniques used for weaning.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):149-153
DOI 10.1590/S0103-507X2008000200006
BACKGROUND AND OBJECTIVES: The number of patients requiring prolonged time on mechanical ventilation is increasing considerably in the intensive care unit (ICU). The objective of this study was to characterize the variability of methods and criteria used by physiotherapists to obtain weaning parameters in hospitals of Fortaleza. METHODS: After approval by the UNIFOR Ethics Committee, survey questionnaires were distributed among physiotherapists working in the ICU of three public and three private hospitals. Forty-four physiotherapists answered thirty-two multiple choice questions anonymously. RESULTS: The main results concerned parameters commonly evaluated by physiotherapists. A significant difference between hospitals was found regarding the rapid shallow breathing index and maximum inspiratory pressure, which are more often used in private hospitals, with a percentage of 100% and 89.5%, respectively. Concerning the ventilatory mode for obtaining the weaning parameters for mechanical ventilation; the T-tube was the most used, not only in the public (56%) but also in the private hospitals (57.9%). CONCLUSIONS: Variability in the methods and criteria used to obtain weaning parameters by the physiotherapists was found in public and private hospitals in Fortaleza. Results from this survey stress the need to develop new scientific studies to standardize the techniques used for weaning.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):256-262
DOI 10.1590/S0103-507X2006000300007
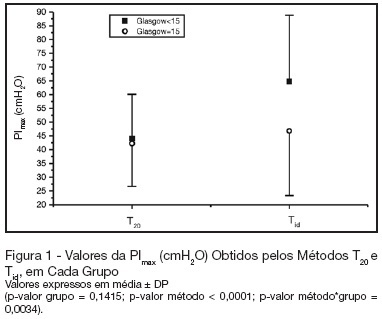
BACKGROUND AND OBJECTIVES: There is no literature consensus about the time of airway occlusion sufficient enough to get a true PImax during weaning from mechanical ventilation (MV). So, the main objectives of the present study were to compare two methods PImax measurement and to evaluate the influence of patients' level of conscience on them. METHODS: The population was composed by 28 general ICU patients, with MV > 48h, in a weaning process, divided into two groups according to Glasgow coma scale score: with (GCS < 15) and without (GCS = 15) alterations of conscience level. The airway was occluded by using an unidirectional valve for 20s (PImaxT20), or for a maximum time of one minute if a plateau of inspiratory pressure was not observed during three consecutive inspirations (PImaxTid). RESULTS: PImaxT20 (mean ± SD, cmH2O) values were similar in both groups (44 ± 16 vs42 ± 15, p = 0.52). However, PImaxTid values, as long as the time needed to their attainment, were greater in GCS < 15 group (65 ± 24 vs 47 ± 23cmH2O and 37 ± 10 vs24 ± 8s, p = 0.04 and 0.0019, respectively). CONCLUSIONS: The method commonly used of 20s airway occlusion seems to be inadequate to get the true PImax in patients with alterations of the level of conscience. Additional studies, now in a more homogeneous group (e. g.: patients with structural brain lesion), are needed to clarify these findings.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):256-262
DOI 10.1590/S0103-507X2006000300007
BACKGROUND AND OBJECTIVES: There is no literature consensus about the time of airway occlusion sufficient enough to get a true PImax during weaning from mechanical ventilation (MV). So, the main objectives of the present study were to compare two methods PImax measurement and to evaluate the influence of patients' level of conscience on them. METHODS: The population was composed by 28 general ICU patients, with MV > 48h, in a weaning process, divided into two groups according to Glasgow coma scale score: with (GCS < 15) and without (GCS = 15) alterations of conscience level. The airway was occluded by using an unidirectional valve for 20s (PImaxT20), or for a maximum time of one minute if a plateau of inspiratory pressure was not observed during three consecutive inspirations (PImaxTid). RESULTS: PImaxT20 (mean ± SD, cmH2O) values were similar in both groups (44 ± 16 vs42 ± 15, p = 0.52). However, PImaxTid values, as long as the time needed to their attainment, were greater in GCS < 15 group (65 ± 24 vs 47 ± 23cmH2O and 37 ± 10 vs24 ± 8s, p = 0.04 and 0.0019, respectively). CONCLUSIONS: The method commonly used of 20s airway occlusion seems to be inadequate to get the true PImax in patients with alterations of the level of conscience. Additional studies, now in a more homogeneous group (e. g.: patients with structural brain lesion), are needed to clarify these findings.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):219-228
DOI 10.1590/S0103-507X2006000300002
BACKGROUND AND OBJECTIVES: There are few epidemiological studies in mechanical ventilation, and the aim of the study is to show how this procedure is being used in Brazil. METHODS: A 1-day point prevalence study was performed in 40 ICUs, with 390 patients; 217 of these patients were in mechanical ventilation. The results evaluated were the characteristics of ventilated patients, their distribution in Brazil, the mechanical ventilation's causes, the main ventilatory modes, the more important ventilators settings, and the weaning stage of mechanical ventilation. RESULTS: The median age of the ventilated patients was 66 years old. The median APACHE II was 20, while the median time of mechanical ventilation was 11 days. Acute respiratory failure occurred in 71% of the patients, coma in 21.2%, acute exacerbation of chronic respiratory failure in 5.5%, and the neuromuscular disease in 2.3%. The volume-controlled ventilation (VCV) (30%), the pressure support ventilation (PSV) (29.5%), and the pressure-controlled ventilation (PCV) (18%) were the ventilatory modes most used; the PSV had been the main mode in weaning (63.5%). The median of tidal volume (8 mL/kg) was higher in VCV. The median of maximal inspiratory pression (30 cmH2O) and the median of positive end-expiration pressure (PEEP) (8 cmH2O) were higher in PCV. CONCLUSIONS: The predominance of ventilated patients in ICUs was marked by clinical severity of them, and a longer hospital stay time; acute respiratory failure was the principal mechanical ventilation cause; VCV and PSV ventilated more patients, with PSV being more used in weaning patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):219-228
DOI 10.1590/S0103-507X2006000300002
BACKGROUND AND OBJECTIVES: There are few epidemiological studies in mechanical ventilation, and the aim of the study is to show how this procedure is being used in Brazil. METHODS: A 1-day point prevalence study was performed in 40 ICUs, with 390 patients; 217 of these patients were in mechanical ventilation. The results evaluated were the characteristics of ventilated patients, their distribution in Brazil, the mechanical ventilation's causes, the main ventilatory modes, the more important ventilators settings, and the weaning stage of mechanical ventilation. RESULTS: The median age of the ventilated patients was 66 years old. The median APACHE II was 20, while the median time of mechanical ventilation was 11 days. Acute respiratory failure occurred in 71% of the patients, coma in 21.2%, acute exacerbation of chronic respiratory failure in 5.5%, and the neuromuscular disease in 2.3%. The volume-controlled ventilation (VCV) (30%), the pressure support ventilation (PSV) (29.5%), and the pressure-controlled ventilation (PCV) (18%) were the ventilatory modes most used; the PSV had been the main mode in weaning (63.5%). The median of tidal volume (8 mL/kg) was higher in VCV. The median of maximal inspiratory pression (30 cmH2O) and the median of positive end-expiration pressure (PEEP) (8 cmH2O) were higher in PCV. CONCLUSIONS: The predominance of ventilated patients in ICUs was marked by clinical severity of them, and a longer hospital stay time; acute respiratory failure was the principal mechanical ventilation cause; VCV and PSV ventilated more patients, with PSV being more used in weaning patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):121-125
DOI 10.1590/S0103-507X2006000200003
BACKGROUND AND OBJECTIVES: Weaning from mechanical ventilation (MV) is an important strategy to reduce morbidity and mortality in critical care patients. In this setting, this study aimed at evaluation of T-tube trial (TT) in weaning from MV. METHODS: Patient admitted in the ICU were included if they present the following inclusion criteria: MV > 24 hours, no neuromuscular disorders, PaO2/FiO2 ratio >200, hemodynamic stability, reversion of the cause of respiratory failure, adequate respiratory drive. All were submitted to TT. Failure was defined by the presence of one of these symptoms: RR > 30 ipm, hypoxemia, tachycardia, arrhythmia, hypertension or hypotension. After two hours of TT, patients without failure criteria were extubated. After 48 hours of adequate spontaneous respiration the patient was considered successful weaned. Results were considered significant if p < 0.05. RESULTS: Forty-nine patients were included with a mean age 51.8 ± 21.7 years. The incidence of ARDS and septic shock were 26.5% and 32.7% and mean duration of MV was 11.9 ± 13 days. Discontinuation of MV occurred in 79.2%, reintubation in 31.6%, in a mean time of 13 ± 8.7 hours and in 75% of the cases it was due to respiratory failure. There was no correlation between success in TT and hemoglobin levels, PaO2/FiO2 ratio, age, gender, prior ARDS or septic shock. Weaning success was not correlated with none of the above variables. CONCLUSIONS: TT was adequated for weaning from mechanical ventilation in the majority of the cases. However, reintubation rate was high. Possible causes are the long period of TT, prior mechanical ventilation or the failure in the criteria used to indicate extubation.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):121-125
DOI 10.1590/S0103-507X2006000200003
BACKGROUND AND OBJECTIVES: Weaning from mechanical ventilation (MV) is an important strategy to reduce morbidity and mortality in critical care patients. In this setting, this study aimed at evaluation of T-tube trial (TT) in weaning from MV. METHODS: Patient admitted in the ICU were included if they present the following inclusion criteria: MV > 24 hours, no neuromuscular disorders, PaO2/FiO2 ratio >200, hemodynamic stability, reversion of the cause of respiratory failure, adequate respiratory drive. All were submitted to TT. Failure was defined by the presence of one of these symptoms: RR > 30 ipm, hypoxemia, tachycardia, arrhythmia, hypertension or hypotension. After two hours of TT, patients without failure criteria were extubated. After 48 hours of adequate spontaneous respiration the patient was considered successful weaned. Results were considered significant if p < 0.05. RESULTS: Forty-nine patients were included with a mean age 51.8 ± 21.7 years. The incidence of ARDS and septic shock were 26.5% and 32.7% and mean duration of MV was 11.9 ± 13 days. Discontinuation of MV occurred in 79.2%, reintubation in 31.6%, in a mean time of 13 ± 8.7 hours and in 75% of the cases it was due to respiratory failure. There was no correlation between success in TT and hemoglobin levels, PaO2/FiO2 ratio, age, gender, prior ARDS or septic shock. Weaning success was not correlated with none of the above variables. CONCLUSIONS: TT was adequated for weaning from mechanical ventilation in the majority of the cases. However, reintubation rate was high. Possible causes are the long period of TT, prior mechanical ventilation or the failure in the criteria used to indicate extubation.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):126-130
DOI 10.1590/S0103-507X2006000200004
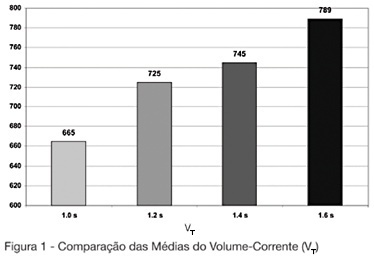
BACKGROUND AND OBJECTIVES: The mechanical ventilator support is one of the main used modalities of support in intensive therapy. In the modality of predetermined pressure, the maximum pressure is regulated, but the current volume (V T) is a complex function of the applied pressure and its speed to reach the pressure-target, of the available breathing time and the resistance to the breath. This paper has as objective to evaluate the influences of the increment of the breathing time in the pulmonary ventilation. METHODS: The study was carried through in the Adult ICU of the Regional Hospital of Mato Grosso do Sul, located in Campo Grande. They had been enclosed individuals adult, both genders, between 16 and 84 years, submitted to the mechanical ventilation in controlled pressure mode or in controlled-watched mode. The breathing time was adjusted in 1 sec, developing in 0.2 sec until the boundary-value of 1.6 sec. The tidal volume (V T) and the volume minute (V E) had been evaluated of 13 patients in the breathing times of 1s; 1.2s; 1.4s and 1.6s. RESULTS: In the mean of V T and V E an increasing increase was observed after-increment of the breathing time. We did not find in consulted literature, data which correlated the breathing time with alterations in the current volume. CONCLUSIONS: The increment of the breathing time in the ventilation for pressure control can have influence in the determination of the current volume offered to the patient.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):126-130
DOI 10.1590/S0103-507X2006000200004
BACKGROUND AND OBJECTIVES: The mechanical ventilator support is one of the main used modalities of support in intensive therapy. In the modality of predetermined pressure, the maximum pressure is regulated, but the current volume (V T) is a complex function of the applied pressure and its speed to reach the pressure-target, of the available breathing time and the resistance to the breath. This paper has as objective to evaluate the influences of the increment of the breathing time in the pulmonary ventilation. METHODS: The study was carried through in the Adult ICU of the Regional Hospital of Mato Grosso do Sul, located in Campo Grande. They had been enclosed individuals adult, both genders, between 16 and 84 years, submitted to the mechanical ventilation in controlled pressure mode or in controlled-watched mode. The breathing time was adjusted in 1 sec, developing in 0.2 sec until the boundary-value of 1.6 sec. The tidal volume (V T) and the volume minute (V E) had been evaluated of 13 patients in the breathing times of 1s; 1.2s; 1.4s and 1.6s. RESULTS: In the mean of V T and V E an increasing increase was observed after-increment of the breathing time. We did not find in consulted literature, data which correlated the breathing time with alterations in the current volume. CONCLUSIONS: The increment of the breathing time in the ventilation for pressure control can have influence in the determination of the current volume offered to the patient.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):131-136
DOI 10.1590/S0103-507X2006000200005
BACKGROUND AND OBJECTIVES: The weaning of mechanical ventilation is the process of transition from mechanical ventilation to spontaneous. The actual practice weaning reveals that the empirism is insufficient and inadequate. On the other side, the standardization of the weaning provides best conductions in the process. The objective of this study was to evaluate the effects of the application of a weaning protocol in an intensive care unit. METHODS: Method: It was included in this study all the patients in program of liberation from the mechanical ventilation, in which the evolution of the weaning was followed by the utilization of a pre-establish protocol and publicated by the service. RESULTS: It was studied 127 patients. In 91% (115) of the patients we had success in the weaning and unsuccess in 9% (12). The non-invasive ventilation after the extubation was utilized in 19% (24) of them. None obit was observed. Comparing the group of the patients that had success with the failed group, there were no statistically significant variations observed in sex (p = 0.96), APACHE II (19.5 versus 18.6 p = 0.75), risk of obit (29% versus 22% p = 0.54), MIP (38 versus 32 cmH2O p = 0.17), duration of mechanical ventilation (6 versus 7 days p = 0.70), PaO2/FiO2 relation (324 versus 312 p = 0.83), weaning modality (PSV or T Tube p = 0.29). There were statistically significant variations observed in rapid shallow respiratory index (59 versus 77 p = 0.02) and duration of the weaning (1 versus 30 hours p < 0.001). CONCLUSIONS: The weaning of the ventilation realized following the standardization brought improvement in its conduction, maintaining the high success index with low mortality.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):131-136
DOI 10.1590/S0103-507X2006000200005
BACKGROUND AND OBJECTIVES: The weaning of mechanical ventilation is the process of transition from mechanical ventilation to spontaneous. The actual practice weaning reveals that the empirism is insufficient and inadequate. On the other side, the standardization of the weaning provides best conductions in the process. The objective of this study was to evaluate the effects of the application of a weaning protocol in an intensive care unit. METHODS: Method: It was included in this study all the patients in program of liberation from the mechanical ventilation, in which the evolution of the weaning was followed by the utilization of a pre-establish protocol and publicated by the service. RESULTS: It was studied 127 patients. In 91% (115) of the patients we had success in the weaning and unsuccess in 9% (12). The non-invasive ventilation after the extubation was utilized in 19% (24) of them. None obit was observed. Comparing the group of the patients that had success with the failed group, there were no statistically significant variations observed in sex (p = 0.96), APACHE II (19.5 versus 18.6 p = 0.75), risk of obit (29% versus 22% p = 0.54), MIP (38 versus 32 cmH2O p = 0.17), duration of mechanical ventilation (6 versus 7 days p = 0.70), PaO2/FiO2 relation (324 versus 312 p = 0.83), weaning modality (PSV or T Tube p = 0.29). There were statistically significant variations observed in rapid shallow respiratory index (59 versus 77 p = 0.02) and duration of the weaning (1 versus 30 hours p < 0.001). CONCLUSIONS: The weaning of the ventilation realized following the standardization brought improvement in its conduction, maintaining the high success index with low mortality.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):24-30
DOI 10.1590/S0103-507X2008000100004
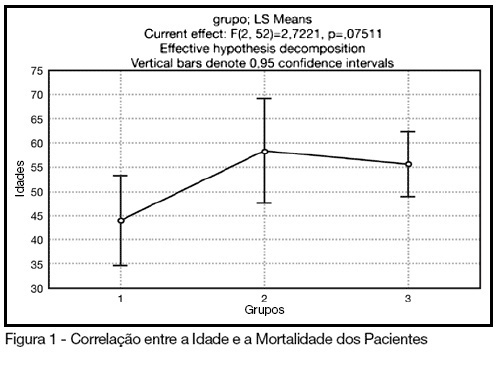
BACKGROUND AND OBJECTIVES: The control of patient discomfort in the intensive care unit (ICU) has become an integral part of critical care practice. The sedoanalgesic drugs could influence critically ill patient's morbimortality. Alpha²-adrenoceptor agonists might have an interesting future in ICU. The objective of this study is to evaluate the clonidine use for sedoanalgesia in ICU patients under prolonged mechanical ventilation. METHODS: Historical cohort study. Admitted patient files, January-December 2006, which stayed under mechanical ventilation, analgesia and sedation > 7days were analyzed. Demographic, clinical features and therapeutic data concerning analgesia and sedation were remarked. The data allowed classify the patients in three different groups: G1 = patients that used clonidine and other drugs; G2 = patients that used three or more drugs, without clonidine and G3 = patients that used fentanyl and midazolam. The mean daily doses of infused clonidine were registered, and the values of heat rate (HR), blood arterial pressure (BAP) before starting use of clonidine, after six hours and 24 hours were also registered. Statistical analyzes were performed using Variance Analysis (ANOVA), t tests and x² (significance p < 0.05). RESULTS: Were selected 55 patients. Fifteen (27.2%) belonged to G1, 11 (20%) belonged to G2 and 29 (52.7%) belonged to G3. The mean age of patients was 44 (G1), 50 (G2) and 56 (G3) (p = NS). The mean score APACHE II was 18 (G1), 20.4 (G2) and 20.7 (G3) (p = NS). G1 and G2 patients presented higher ICU length-of-stay (p < 0.05). The mean dose of clonidine used was 1.21 ± 0.54 mg/kg/min. G1 patients had HR and BAP decreased, however these effects were not considered clinically relevant. The mortality was lower in the patients from G1 (20%) when compared to G2 (54.5%) and G3 (62%) (p < 0.05). CONCLUSIONS: The clonidine use to analyzed patients did not result in clinical relevant side effects. The lower mortality index in patients that used clonidine was statistical significant.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):24-30
DOI 10.1590/S0103-507X2008000100004
BACKGROUND AND OBJECTIVES: The control of patient discomfort in the intensive care unit (ICU) has become an integral part of critical care practice. The sedoanalgesic drugs could influence critically ill patient's morbimortality. Alpha²-adrenoceptor agonists might have an interesting future in ICU. The objective of this study is to evaluate the clonidine use for sedoanalgesia in ICU patients under prolonged mechanical ventilation. METHODS: Historical cohort study. Admitted patient files, January-December 2006, which stayed under mechanical ventilation, analgesia and sedation > 7days were analyzed. Demographic, clinical features and therapeutic data concerning analgesia and sedation were remarked. The data allowed classify the patients in three different groups: G1 = patients that used clonidine and other drugs; G2 = patients that used three or more drugs, without clonidine and G3 = patients that used fentanyl and midazolam. The mean daily doses of infused clonidine were registered, and the values of heat rate (HR), blood arterial pressure (BAP) before starting use of clonidine, after six hours and 24 hours were also registered. Statistical analyzes were performed using Variance Analysis (ANOVA), t tests and x² (significance p < 0.05). RESULTS: Were selected 55 patients. Fifteen (27.2%) belonged to G1, 11 (20%) belonged to G2 and 29 (52.7%) belonged to G3. The mean age of patients was 44 (G1), 50 (G2) and 56 (G3) (p = NS). The mean score APACHE II was 18 (G1), 20.4 (G2) and 20.7 (G3) (p = NS). G1 and G2 patients presented higher ICU length-of-stay (p < 0.05). The mean dose of clonidine used was 1.21 ± 0.54 mg/kg/min. G1 patients had HR and BAP decreased, however these effects were not considered clinically relevant. The mortality was lower in the patients from G1 (20%) when compared to G2 (54.5%) and G3 (62%) (p < 0.05). CONCLUSIONS: The clonidine use to analyzed patients did not result in clinical relevant side effects. The lower mortality index in patients that used clonidine was statistical significant.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)