
You searched for:"Anderson José"
We found (6) results for your search.-
Standardization of weaning of the mechanical ventilation in a Intensive Care Unit: results afterwards one year
Rev Bras Ter Intensiva. 2006;18(2):131-136
Abstract
Standardization of weaning of the mechanical ventilation in a Intensive Care Unit: results afterwards one year
Rev Bras Ter Intensiva. 2006;18(2):131-136
DOI 10.1590/S0103-507X2006000200005
Views0See moreBACKGROUND AND OBJECTIVES: The weaning of mechanical ventilation is the process of transition from mechanical ventilation to spontaneous. The actual practice weaning reveals that the empirism is insufficient and inadequate. On the other side, the standardization of the weaning provides best conductions in the process. The objective of this study was to evaluate the effects of the application of a weaning protocol in an intensive care unit. METHODS: Method: It was included in this study all the patients in program of liberation from the mechanical ventilation, in which the evolution of the weaning was followed by the utilization of a pre-establish protocol and publicated by the service. RESULTS: It was studied 127 patients. In 91% (115) of the patients we had success in the weaning and unsuccess in 9% (12). The non-invasive ventilation after the extubation was utilized in 19% (24) of them. None obit was observed. Comparing the group of the patients that had success with the failed group, there were no statistically significant variations observed in sex (p = 0.96), APACHE II (19.5 versus 18.6 p = 0.75), risk of obit (29% versus 22% p = 0.54), MIP (38 versus 32 cmH2O p = 0.17), duration of mechanical ventilation (6 versus 7 days p = 0.70), PaO2/FiO2 relation (324 versus 312 p = 0.83), weaning modality (PSV or T Tube p = 0.29). There were statistically significant variations observed in rapid shallow respiratory index (59 versus 77 p = 0.02) and duration of the weaning (1 versus 30 hours p < 0.001). CONCLUSIONS: The weaning of the ventilation realized following the standardization brought improvement in its conduction, maintaining the high success index with low mortality.
Views0

Abstract
Standardization of weaning of the mechanical ventilation in a Intensive Care Unit: results afterwards one year
Rev Bras Ter Intensiva. 2006;18(2):131-136
DOI 10.1590/S0103-507X2006000200005
Views0See moreBACKGROUND AND OBJECTIVES: The weaning of mechanical ventilation is the process of transition from mechanical ventilation to spontaneous. The actual practice weaning reveals that the empirism is insufficient and inadequate. On the other side, the standardization of the weaning provides best conductions in the process. The objective of this study was to evaluate the effects of the application of a weaning protocol in an intensive care unit. METHODS: Method: It was included in this study all the patients in program of liberation from the mechanical ventilation, in which the evolution of the weaning was followed by the utilization of a pre-establish protocol and publicated by the service. RESULTS: It was studied 127 patients. In 91% (115) of the patients we had success in the weaning and unsuccess in 9% (12). The non-invasive ventilation after the extubation was utilized in 19% (24) of them. None obit was observed. Comparing the group of the patients that had success with the failed group, there were no statistically significant variations observed in sex (p = 0.96), APACHE II (19.5 versus 18.6 p = 0.75), risk of obit (29% versus 22% p = 0.54), MIP (38 versus 32 cmH2O p = 0.17), duration of mechanical ventilation (6 versus 7 days p = 0.70), PaO2/FiO2 relation (324 versus 312 p = 0.83), weaning modality (PSV or T Tube p = 0.29). There were statistically significant variations observed in rapid shallow respiratory index (59 versus 77 p = 0.02) and duration of the weaning (1 versus 30 hours p < 0.001). CONCLUSIONS: The weaning of the ventilation realized following the standardization brought improvement in its conduction, maintaining the high success index with low mortality.
-
Best positive end expiratory pressure settlement in acute respiratory discomfort syndrome and prone position
Rev Bras Ter Intensiva. 2008;20(1):37-42
Abstract
Best positive end expiratory pressure settlement in acute respiratory discomfort syndrome and prone position
Rev Bras Ter Intensiva. 2008;20(1):37-42
DOI 10.1590/S0103-507X2008000100006
Views0See moreBACKGROUND AND OBJECTIVES: In acute respiratory discomfort syndrome (ARDS) patients, prone position improves oxygenation in more than 70% of the cases. It is well known that prone position promotes a lot of pulmonary changes, including pulmonary mechanics, so we hypothesized that there is the necessity to optimize the ventilatory parameters after the patient is placed in prone position, especially the positive end expiratory pressure (PEEP) values. The objective of this study valued the influence of the prone position at the calculation of the ideal PEEP, given a title by the best pulmonary complaisance and he compared the pulmonary alterations of mechanics, of oxygenation and of ventilation in the positions supine and prone. METHODS: Prospective study, taken place in the Irmandade Santa Casa de Misericórdia de São Paulo Intensive Care Service. Three fases have been compared. Fase 1: in supine position, after the best PEEP calculation. Fase 2: two hours after the patient was placed in prone position and the best PEEP was calculated. The patient was kept for 6 hours in this position. Fase 3: after this time, patient was placed in supine again and after two hours, a new best PEEP calculation and arterial gas analysis was done. And then fase1 versus fase 2, fase 2 versus fase 3, fase 3 versus fase1 were compared. RESULTS: There were no differences in the PEEP values found in all study fases: fase 1 = 14 ± 4.43; fase 2 = 14.73 ± 4.77 and fase 3 = 13.65 ± 4.92. CONCLUSIONS: There were no differences in best PEEP values between prone and supine position. Therefore, there is no need to recalculate the PEEP value after each position change.
Views0Abstract
Best positive end expiratory pressure settlement in acute respiratory discomfort syndrome and prone position
Rev Bras Ter Intensiva. 2008;20(1):37-42
DOI 10.1590/S0103-507X2008000100006
Views0See moreBACKGROUND AND OBJECTIVES: In acute respiratory discomfort syndrome (ARDS) patients, prone position improves oxygenation in more than 70% of the cases. It is well known that prone position promotes a lot of pulmonary changes, including pulmonary mechanics, so we hypothesized that there is the necessity to optimize the ventilatory parameters after the patient is placed in prone position, especially the positive end expiratory pressure (PEEP) values. The objective of this study valued the influence of the prone position at the calculation of the ideal PEEP, given a title by the best pulmonary complaisance and he compared the pulmonary alterations of mechanics, of oxygenation and of ventilation in the positions supine and prone. METHODS: Prospective study, taken place in the Irmandade Santa Casa de Misericórdia de São Paulo Intensive Care Service. Three fases have been compared. Fase 1: in supine position, after the best PEEP calculation. Fase 2: two hours after the patient was placed in prone position and the best PEEP was calculated. The patient was kept for 6 hours in this position. Fase 3: after this time, patient was placed in supine again and after two hours, a new best PEEP calculation and arterial gas analysis was done. And then fase1 versus fase 2, fase 2 versus fase 3, fase 3 versus fase1 were compared. RESULTS: There were no differences in the PEEP values found in all study fases: fase 1 = 14 ± 4.43; fase 2 = 14.73 ± 4.77 and fase 3 = 13.65 ± 4.92. CONCLUSIONS: There were no differences in best PEEP values between prone and supine position. Therefore, there is no need to recalculate the PEEP value after each position change.
-
Artigos originais
Noninvasive positive pressure ventilation in patients with acute respiratory failure after tracheal extubation
Rev Bras Ter Intensiva. 2006;18(4):338-343
Abstract
Artigos originaisNoninvasive positive pressure ventilation in patients with acute respiratory failure after tracheal extubation
Rev Bras Ter Intensiva. 2006;18(4):338-343
DOI 10.1590/S0103-507X2006000400004
Views0See moreBACKGROUND AND OBJECTIVES: Noninvasive positive pressure ventilation (NPPV) has been routinely used to assist the weaning of the mechanical ventilation. One of the applications most common is in patients who had acute respiratory failure after extubation, even the scientific evidences for this indication still controversy. The aims of this study were to evaluate the index of patients that evolve for respiratory failure after extubation and evaluated the effectiveness of NPPV to avoid the need for reintubation and to promote increase in success index of weaning. METHODS: We conducted a transversal and prospective study. It was applied to NPPV in the patients who presented respiratory failure after extubation, independent of its etiology. NPPV was applied in to pressure support ventilation, with Vte for 6 to 8 mL/kg, PEEP and FiO2 adjusted to reach SaO2 > 95%. The NPPV was accomplished of a continuous mould even interrupt the signs of respiratory failure presented initially. The success of weaning and the NPPV was defined when the clinical events were reverted by a period greater than 48 hours in spontaneous breathing, avoid thus reintubation. RESULTS: We included 103 patients. Noted that 32% (33) evolved with signals of respiratory failure after extubation and were submitted to NPPV. The time of NPPV was on mean 8 ± 5 hours, PSV of 12 ± 2 cmH2O, PEEP of 7 ± 2 cmH2O, FiO2 of 40% ± 20%, Vte of 462 ± 100 mL, RR of 26 ± 5 rpm. Among patients who accomplished NPPV (33), 76% (25) attended with success and them afterwards let the ICU. Of the patients assigned to NPPV, 24% (8) did not tolerate the procedure and were reintubated. CONCLUSIONS: We conclude that NPPV is safe and effective in averting the need for reintubation in patients with respiratory failure after extubation.
Views0Abstract
Artigos originaisNoninvasive positive pressure ventilation in patients with acute respiratory failure after tracheal extubation
Rev Bras Ter Intensiva. 2006;18(4):338-343
DOI 10.1590/S0103-507X2006000400004
Views0See moreBACKGROUND AND OBJECTIVES: Noninvasive positive pressure ventilation (NPPV) has been routinely used to assist the weaning of the mechanical ventilation. One of the applications most common is in patients who had acute respiratory failure after extubation, even the scientific evidences for this indication still controversy. The aims of this study were to evaluate the index of patients that evolve for respiratory failure after extubation and evaluated the effectiveness of NPPV to avoid the need for reintubation and to promote increase in success index of weaning. METHODS: We conducted a transversal and prospective study. It was applied to NPPV in the patients who presented respiratory failure after extubation, independent of its etiology. NPPV was applied in to pressure support ventilation, with Vte for 6 to 8 mL/kg, PEEP and FiO2 adjusted to reach SaO2 > 95%. The NPPV was accomplished of a continuous mould even interrupt the signs of respiratory failure presented initially. The success of weaning and the NPPV was defined when the clinical events were reverted by a period greater than 48 hours in spontaneous breathing, avoid thus reintubation. RESULTS: We included 103 patients. Noted that 32% (33) evolved with signals of respiratory failure after extubation and were submitted to NPPV. The time of NPPV was on mean 8 ± 5 hours, PSV of 12 ± 2 cmH2O, PEEP of 7 ± 2 cmH2O, FiO2 of 40% ± 20%, Vte of 462 ± 100 mL, RR of 26 ± 5 rpm. Among patients who accomplished NPPV (33), 76% (25) attended with success and them afterwards let the ICU. Of the patients assigned to NPPV, 24% (8) did not tolerate the procedure and were reintubated. CONCLUSIONS: We conclude that NPPV is safe and effective in averting the need for reintubation in patients with respiratory failure after extubation.
-
Mechanical ventilation in the acute lung injury/acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2007;19(3):374-383
Abstract
Mechanical ventilation in the acute lung injury/acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2007;19(3):374-383
DOI 10.1590/S0103-507X2007000300020
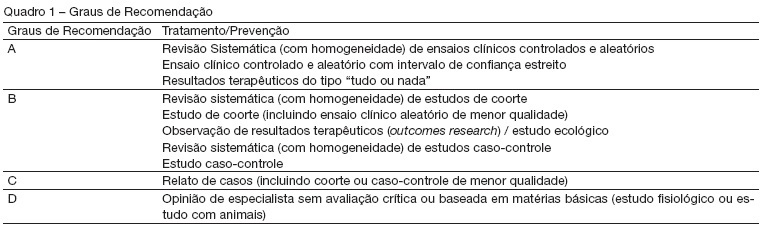
Views0See moreBACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence – based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB – Associação de Medicina Intensiva Brasileira and SBPT – Sociedade Brasileira de Pneumologia e Tisiologia – decided to update the recommendations of the II Brazilian Consensus. Acute Respiratory Distress Syndrome (ARDS) has been one of the updated topics. This objective was described the most important topics related to mechanical ventilation in patients with acute respiratory distress syndrome. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words mechanical ventilation and acute respiratory distress syndrome. RESULTS: Recommendations on the use of lung protective strategies during mechanical ventilation based on reduced tidal volumes and limitation of plateau pressure. The state of the art of recruitment maneuvers and PEEP titration is also discussed. CONCLUSIONS: The mechanical ventilation of patients with ADRS changed in the last few years. We presented the role of lung protective strategies that could be applied to these patients.
Views0Abstract
Mechanical ventilation in the acute lung injury/acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2007;19(3):374-383
DOI 10.1590/S0103-507X2007000300020
Views0See moreBACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence – based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB – Associação de Medicina Intensiva Brasileira and SBPT – Sociedade Brasileira de Pneumologia e Tisiologia – decided to update the recommendations of the II Brazilian Consensus. Acute Respiratory Distress Syndrome (ARDS) has been one of the updated topics. This objective was described the most important topics related to mechanical ventilation in patients with acute respiratory distress syndrome. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words mechanical ventilation and acute respiratory distress syndrome. RESULTS: Recommendations on the use of lung protective strategies during mechanical ventilation based on reduced tidal volumes and limitation of plateau pressure. The state of the art of recruitment maneuvers and PEEP titration is also discussed. CONCLUSIONS: The mechanical ventilation of patients with ADRS changed in the last few years. We presented the role of lung protective strategies that could be applied to these patients.
-
Mechanical ventilation in chronic obstructive pulmonary disease
Rev Bras Ter Intensiva. 2007;19(2):264-272
Abstract
Mechanical ventilation in chronic obstructive pulmonary disease
Rev Bras Ter Intensiva. 2007;19(2):264-272
DOI 10.1590/S0103-507X2007000200021
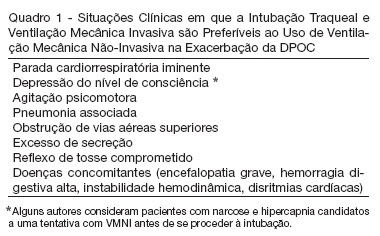
Views0See moreBACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence – based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB – Associação de Medicina Intensiva Brasileira and SBPT – Sociedade Brasileira de Pneumologia e Tisiologia – decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in COPD exacerbation has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the COPD exacerbation and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the keywords “mechanical ventilation” and “COPD”. RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a.
Views0Abstract
Mechanical ventilation in chronic obstructive pulmonary disease
Rev Bras Ter Intensiva. 2007;19(2):264-272
DOI 10.1590/S0103-507X2007000200021
Views0See moreBACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence – based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB – Associação de Medicina Intensiva Brasileira and SBPT – Sociedade Brasileira de Pneumologia e Tisiologia – decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in COPD exacerbation has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the COPD exacerbation and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the keywords “mechanical ventilation” and “COPD”. RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a.
-
Mechanical ventilation in acute asthma crisis
Rev Bras Ter Intensiva. 2007;19(2):258-263
Abstract
Mechanical ventilation in acute asthma crisis
Rev Bras Ter Intensiva. 2007;19(2):258-263
DOI 10.1590/S0103-507X2007000200020
Views1See moreBACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence – based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB – Associação de Medicina Intensiva Brasileira and SBPT – Sociedade Brasileira de Pneumologia e Tisiologia – decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in the asthma attack has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the asthma attack and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words “mechanical ventilation” and “asthma”. RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a severe asthma attack.
Views1Abstract
Mechanical ventilation in acute asthma crisis
Rev Bras Ter Intensiva. 2007;19(2):258-263
DOI 10.1590/S0103-507X2007000200020
Views1See moreBACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence – based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB – Associação de Medicina Intensiva Brasileira and SBPT – Sociedade Brasileira de Pneumologia e Tisiologia – decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in the asthma attack has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the asthma attack and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words “mechanical ventilation” and “asthma”. RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a severe asthma attack.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis