Critical care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):443-451
DOI 10.5935/0103-507X.20220440-en
To characterize myocardial injury and cardiovascular complications and their predictors in severe and critical COVID-19 patients admitted to the intensive care unit.
This was an observational cohort study of severe and critical COVID-19 patients admitted to the intensive care unit. Myocardial injury was defined as blood levels of cardiac troponin above the 99th percentile upper reference limit. Cardiovascular events considered were the composite of deep vein thrombosis, pulmonary embolism, stroke, myocardial infarction, acute limb ischemia, mesenteric ischemia, heart failure and arrhythmia. Univariate and multivariate logistic regression or Cox proportional hazard models were used to determine predictors of myocardial injury.
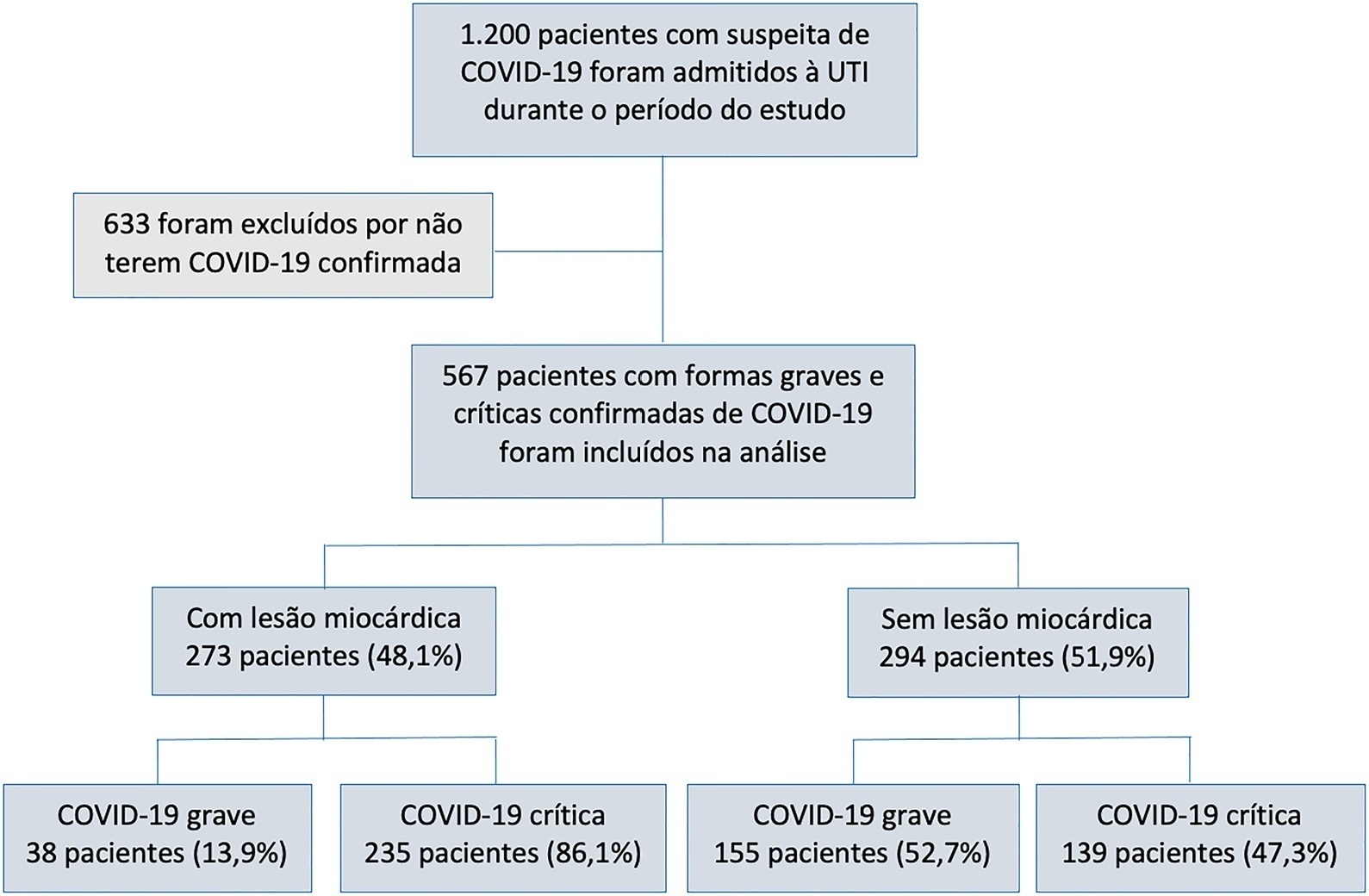
Of 567 patients with severe and critical COVID-19 admitted to the intensive care unit, 273 (48.1%) had myocardial injury. Of the 374 patients with critical COVID-19, 86.1% had myocardial injury, and also showed more organ dysfunction and higher 28-day mortality (56.6% versus 27.1%, p < 0.001). Advanced age, arterial hypertension and immune modulator use were predictors of myocardial injury. Cardiovascular complications occurred in 19.9% of patients with severe and critical COVID-19 admitted to the intensive care unit, with most events occurring in patients with myocardial injury (28.2% versus 12.2%, p < 0.001). The occurrence of an early cardiovascular event during intensive care unit stay was associated with higher 28-day mortality compared with late or no events (57.1% versus 34% versus 41.8%, p = 0.01).
Myocardial injury and cardiovascular complications were commonly found in patients with severe and critical forms of COVID-19 admitted to the intensive care unit, and both were associated with increased mortality in these patients.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):443-451
DOI 10.5935/0103-507X.20220440-en
To characterize myocardial injury and cardiovascular complications and their predictors in severe and critical COVID-19 patients admitted to the intensive care unit.
This was an observational cohort study of severe and critical COVID-19 patients admitted to the intensive care unit. Myocardial injury was defined as blood levels of cardiac troponin above the 99th percentile upper reference limit. Cardiovascular events considered were the composite of deep vein thrombosis, pulmonary embolism, stroke, myocardial infarction, acute limb ischemia, mesenteric ischemia, heart failure and arrhythmia. Univariate and multivariate logistic regression or Cox proportional hazard models were used to determine predictors of myocardial injury.
Of 567 patients with severe and critical COVID-19 admitted to the intensive care unit, 273 (48.1%) had myocardial injury. Of the 374 patients with critical COVID-19, 86.1% had myocardial injury, and also showed more organ dysfunction and higher 28-day mortality (56.6% versus 27.1%, p < 0.001). Advanced age, arterial hypertension and immune modulator use were predictors of myocardial injury. Cardiovascular complications occurred in 19.9% of patients with severe and critical COVID-19 admitted to the intensive care unit, with most events occurring in patients with myocardial injury (28.2% versus 12.2%, p < 0.001). The occurrence of an early cardiovascular event during intensive care unit stay was associated with higher 28-day mortality compared with late or no events (57.1% versus 34% versus 41.8%, p = 0.01).
Myocardial injury and cardiovascular complications were commonly found in patients with severe and critical forms of COVID-19 admitted to the intensive care unit, and both were associated with increased mortality in these patients.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):477-483
DOI 10.5935/0103-507X.20220280-en
To create and validate a model for predicting septic or hypovolemic shock from easily obtainable variables collected from patients at admission to an intensive care unit.
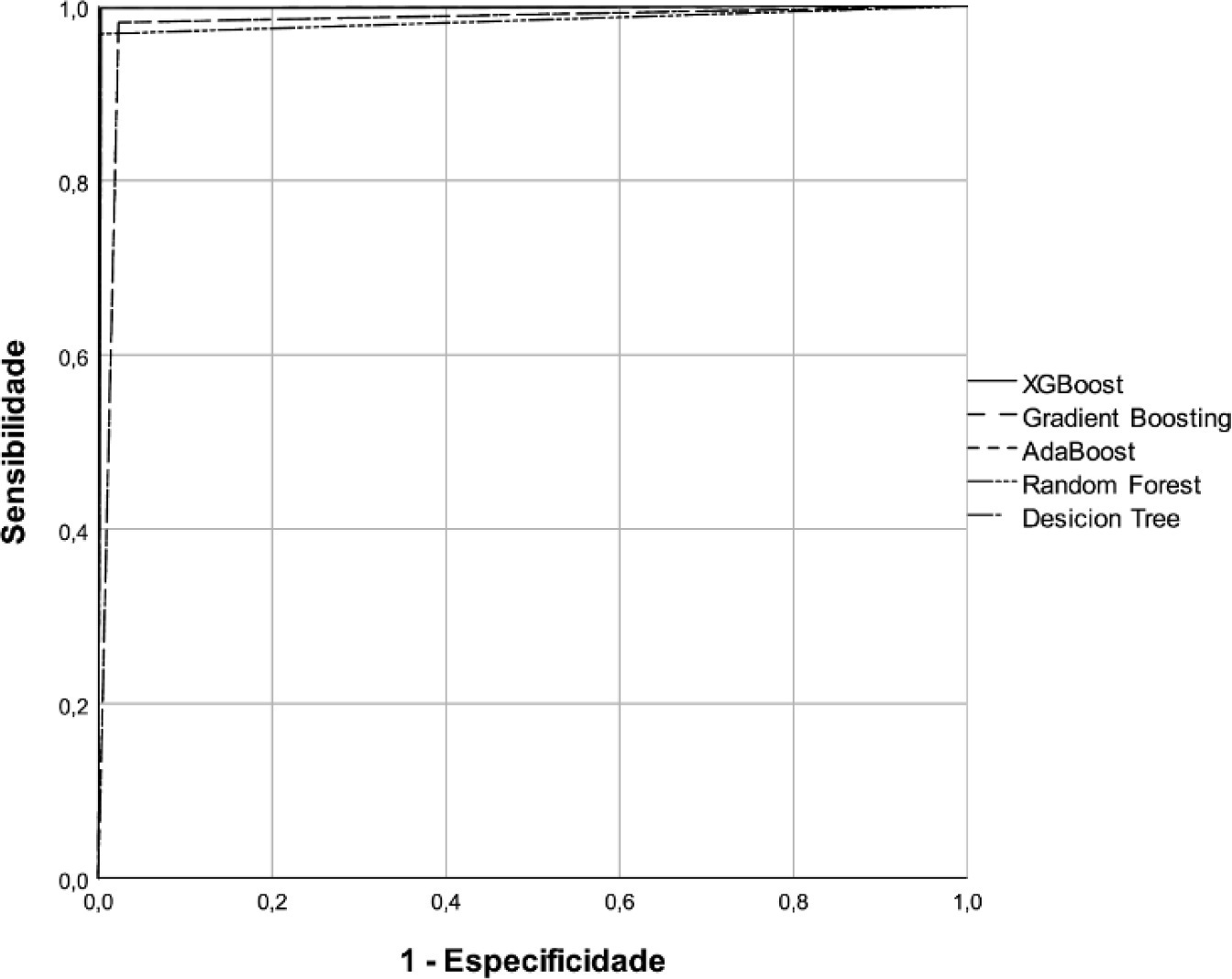
A predictive modeling study with concurrent cohort data was conducted in a hospital in the interior of northeastern Brazil. Patients aged 18 years or older who were not using vasoactive drugs on the day of admission and were hospitalized from November 2020 to July 2021 were included. The Decision Tree, Random Forest, AdaBoost, Gradient Boosting and XGBoost classification algorithms were tested for use in building the model. The validation method used was k-fold cross validation. The evaluation metrics used were recall, precision and area under the Receiver Operating Characteristic curve.
A total of 720 patients were used to create and validate the model. The models showed high predictive capacity with areas under the Receiver Operating Characteristic curve of 0.979; 0.999; 0.980; 0.998 and 1.00 for the Decision Tree, Random Forest, AdaBoost, Gradient Boosting and XGBoost algorithms, respectively.
The predictive model created and validated showed a high ability to predict septic and hypovolemic shock from the time of admission of patients to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):477-483
DOI 10.5935/0103-507X.20220280-en
To create and validate a model for predicting septic or hypovolemic shock from easily obtainable variables collected from patients at admission to an intensive care unit.
A predictive modeling study with concurrent cohort data was conducted in a hospital in the interior of northeastern Brazil. Patients aged 18 years or older who were not using vasoactive drugs on the day of admission and were hospitalized from November 2020 to July 2021 were included. The Decision Tree, Random Forest, AdaBoost, Gradient Boosting and XGBoost classification algorithms were tested for use in building the model. The validation method used was k-fold cross validation. The evaluation metrics used were recall, precision and area under the Receiver Operating Characteristic curve.
A total of 720 patients were used to create and validate the model. The models showed high predictive capacity with areas under the Receiver Operating Characteristic curve of 0.979; 0.999; 0.980; 0.998 and 1.00 for the Decision Tree, Random Forest, AdaBoost, Gradient Boosting and XGBoost algorithms, respectively.
The predictive model created and validated showed a high ability to predict septic and hypovolemic shock from the time of admission of patients to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):484-491
DOI 10.5935/0103-507X.20220264-en
To obtain data on bed refusal in intensive care units in Brazil and to evaluate the use of triage systems by professionals.
A cross-sectional survey. Using the Delphi methodology, a questionnaire was created contemplating the objectives of the study. Physicians and nurses enrolled in the research network of the Associação de Medicina Intensiva Brasileira (AMIBnet) were invited to participate. A web platform (SurveyMonkey®) was used to distribute the questionnaire. The variables in this study were measured in categories and expressed as proportions. The chi-square test or Fisher’s exact test was used to verify associations. The significance level was set at 5%.
In total, 231 professionals answered the questionnaire, representing all regions of the country. The national intensive care units had an occupancy rate of more than 90% always or frequently for 90.8% of the participants. Among the participants, 84.4% had already refused admitting patients to the intensive care unit due to the capacity of the unit. Half of the Brazilian institutions (49.7%) did not have triage protocols for admission to intensive beds.
Bed refusal due to high occupancy rates is common in Brazilian intensive care units. Even so, half of the services in Brazil do not adopt protocols for triage of beds.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):484-491
DOI 10.5935/0103-507X.20220264-en
To obtain data on bed refusal in intensive care units in Brazil and to evaluate the use of triage systems by professionals.
A cross-sectional survey. Using the Delphi methodology, a questionnaire was created contemplating the objectives of the study. Physicians and nurses enrolled in the research network of the Associação de Medicina Intensiva Brasileira (AMIBnet) were invited to participate. A web platform (SurveyMonkey®) was used to distribute the questionnaire. The variables in this study were measured in categories and expressed as proportions. The chi-square test or Fisher’s exact test was used to verify associations. The significance level was set at 5%.
In total, 231 professionals answered the questionnaire, representing all regions of the country. The national intensive care units had an occupancy rate of more than 90% always or frequently for 90.8% of the participants. Among the participants, 84.4% had already refused admitting patients to the intensive care unit due to the capacity of the unit. Half of the Brazilian institutions (49.7%) did not have triage protocols for admission to intensive beds.
Bed refusal due to high occupancy rates is common in Brazilian intensive care units. Even so, half of the services in Brazil do not adopt protocols for triage of beds.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):335-341
DOI 10.5935/0103-507X.20220040-en
To compare the lung mechanics and outcomes between COVID-19-associated acute respiratory distress syndrome and non-COVID-19-associated acute respiratory distress syndrome.
We combined data from two randomized trials in acute respiratory distress syndrome, one including only COVID-19 patients and the other including only patients without COVID-19, to determine whether COVID-19-associated acute respiratory distress syndrome is associated with higher 28-day mortality than non-COVID-19 acute respiratory distress syndrome and to examine the differences in lung mechanics between these two types of acute respiratory distress syndrome.
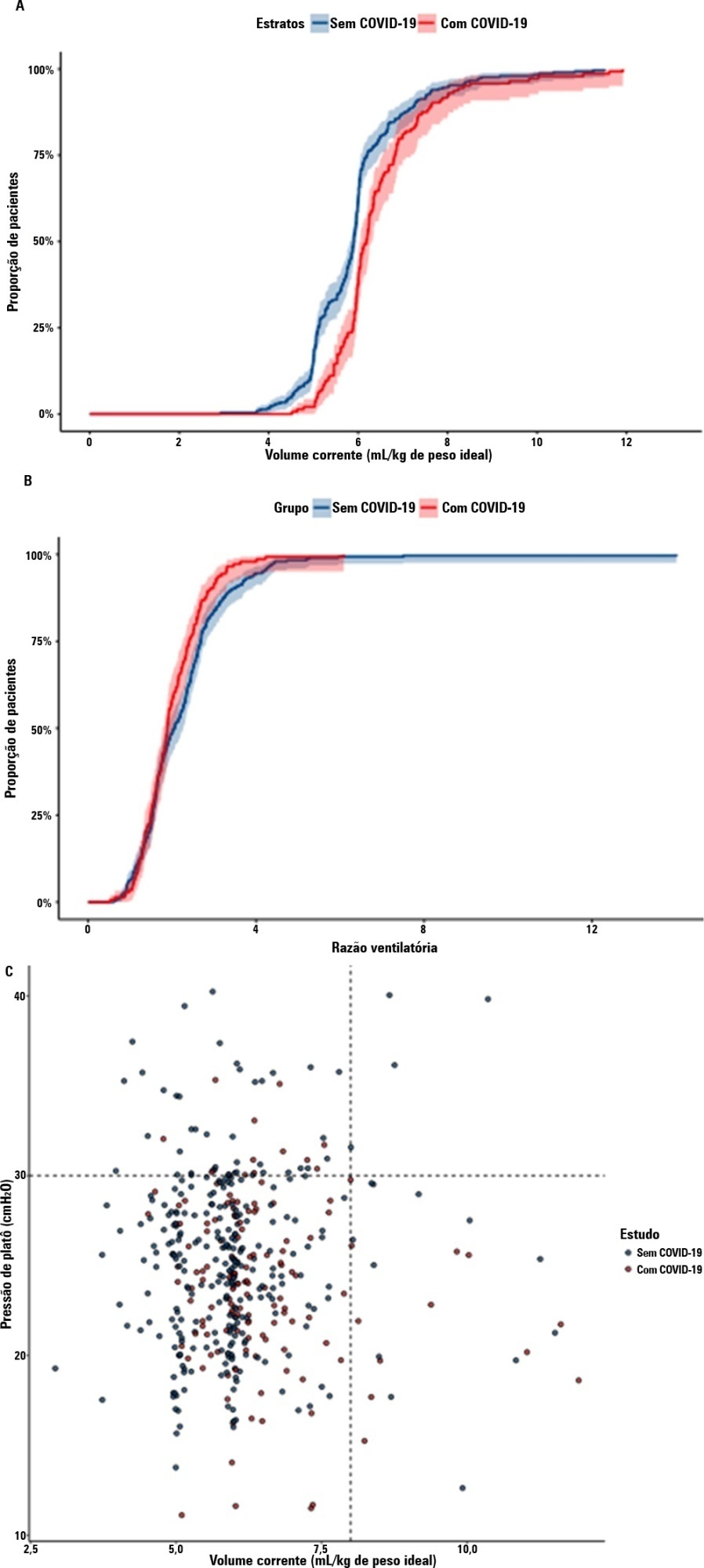
A total of 299 patients with COVID-19-associated acute respiratory distress syndrome and 1,010 patients with non-COVID-19-associated acute respiratory distress syndrome were included in the main analysis. The results showed that non-COVID-19 patients used higher positive end-expiratory pressure (12.5cmH2O; SD 3.2 versus 11.7cmH2O SD 2.8; p < 0.001), were ventilated with lower tidal volumes (5.8mL/kg; SD 1.0 versus 6.5mL/kg; SD 1.2; p < 0.001) and had lower static respiratory compliance adjusted for ideal body weight (0.5mL/cmH2O/kg; SD 0.3 versus 0.6mL/cmH2O/kg; SD 0.3; p = 0.01). There was no difference between groups in 28-day mortality (52.3% versus 58.9%; p = 0.52) or mechanical ventilation duration in the first 28 days among survivors (13 [IQR 5 - 22] versus 12 [IQR 6 - 26], p = 0.46).
This analysis showed that patients with non-COVID-19-associated acute respiratory distress syndrome have different lung mechanics but similar outcomes to COVID-19-associated acute respiratory distress syndrome patients. After propensity score matching, there was no difference in lung mechanics or outcomes between groups.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):335-341
DOI 10.5935/0103-507X.20220040-en
To compare the lung mechanics and outcomes between COVID-19-associated acute respiratory distress syndrome and non-COVID-19-associated acute respiratory distress syndrome.
We combined data from two randomized trials in acute respiratory distress syndrome, one including only COVID-19 patients and the other including only patients without COVID-19, to determine whether COVID-19-associated acute respiratory distress syndrome is associated with higher 28-day mortality than non-COVID-19 acute respiratory distress syndrome and to examine the differences in lung mechanics between these two types of acute respiratory distress syndrome.
A total of 299 patients with COVID-19-associated acute respiratory distress syndrome and 1,010 patients with non-COVID-19-associated acute respiratory distress syndrome were included in the main analysis. The results showed that non-COVID-19 patients used higher positive end-expiratory pressure (12.5cmH2O; SD 3.2 versus 11.7cmH2O SD 2.8; p < 0.001), were ventilated with lower tidal volumes (5.8mL/kg; SD 1.0 versus 6.5mL/kg; SD 1.2; p < 0.001) and had lower static respiratory compliance adjusted for ideal body weight (0.5mL/cmH2O/kg; SD 0.3 versus 0.6mL/cmH2O/kg; SD 0.3; p = 0.01). There was no difference between groups in 28-day mortality (52.3% versus 58.9%; p = 0.52) or mechanical ventilation duration in the first 28 days among survivors (13 [IQR 5 - 22] versus 12 [IQR 6 - 26], p = 0.46).
This analysis showed that patients with non-COVID-19-associated acute respiratory distress syndrome have different lung mechanics but similar outcomes to COVID-19-associated acute respiratory distress syndrome patients. After propensity score matching, there was no difference in lung mechanics or outcomes between groups.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):360-366
DOI 10.5935/0103-507X.20220477-en
To investigate the applicability of the Respiratory Rate-Oxygenation Index to identify the risk of high-flow nasal cannula failure in post-extubation pneumonia patients.
This was a 2-year retrospective observational study conducted in a reference hospital in Bogotá, Colombia. All patients in whom post-extubation high-flow nasal cannula therapy was used as a bridge to extubation were included in the study. The Respiratory Rate-Oxygenation Index was calculated to assess the risk of post-extubation high-flow nasal cannula failure.
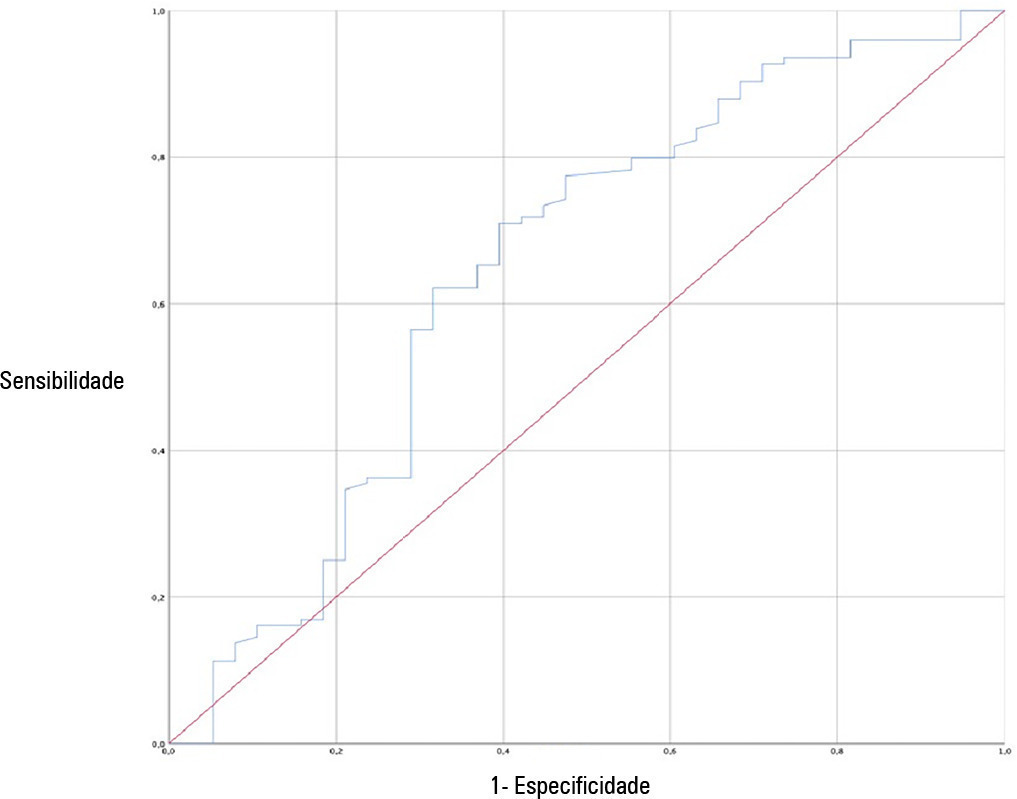
A total of 162 patients were included in the study. Of these, 23.5% developed high-flow nasal cannula failure. The Respiratory Rate-Oxygenation Index was significantly lower in patients who had high-flow nasal cannula failure [median (IQR): 10.0 (7.7 - 14.4) versus 12.6 (10.1 - 15.6); p = 0.006]. Respiratory Rate-Oxygenation Index > 4.88 showed a crude OR of 0.23 (95%CI 0.17 - 0.30) and an adjusted OR of 0.89 (95%CI 0.81 - 0.98) stratified by severity and comorbidity. After logistic regression analysis, the Respiratory Rate-Oxygenation Index had an adjusted OR of 0.90 (95%CI 0.82 - 0.98; p = 0.026). The area under the Receiver Operating Characteristic curve for extubation failure was 0.64 (95%CI 0.53 - 0.75; p = 0.06). The Respiratory Rate-Oxygenation Index did not show differences between patients who survived and those who died during the intensive care unit stay.
The Respiratory Rate-Oxygenation Index is an accessible tool to identify patients at risk of failing high-flow nasal cannula post-extubation treatment. Prospective studies are needed to broaden the utility in this scenario.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):360-366
DOI 10.5935/0103-507X.20220477-en
To investigate the applicability of the Respiratory Rate-Oxygenation Index to identify the risk of high-flow nasal cannula failure in post-extubation pneumonia patients.
This was a 2-year retrospective observational study conducted in a reference hospital in Bogotá, Colombia. All patients in whom post-extubation high-flow nasal cannula therapy was used as a bridge to extubation were included in the study. The Respiratory Rate-Oxygenation Index was calculated to assess the risk of post-extubation high-flow nasal cannula failure.
A total of 162 patients were included in the study. Of these, 23.5% developed high-flow nasal cannula failure. The Respiratory Rate-Oxygenation Index was significantly lower in patients who had high-flow nasal cannula failure [median (IQR): 10.0 (7.7 - 14.4) versus 12.6 (10.1 - 15.6); p = 0.006]. Respiratory Rate-Oxygenation Index > 4.88 showed a crude OR of 0.23 (95%CI 0.17 - 0.30) and an adjusted OR of 0.89 (95%CI 0.81 - 0.98) stratified by severity and comorbidity. After logistic regression analysis, the Respiratory Rate-Oxygenation Index had an adjusted OR of 0.90 (95%CI 0.82 - 0.98; p = 0.026). The area under the Receiver Operating Characteristic curve for extubation failure was 0.64 (95%CI 0.53 - 0.75; p = 0.06). The Respiratory Rate-Oxygenation Index did not show differences between patients who survived and those who died during the intensive care unit stay.
The Respiratory Rate-Oxygenation Index is an accessible tool to identify patients at risk of failing high-flow nasal cannula post-extubation treatment. Prospective studies are needed to broaden the utility in this scenario.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):374-379
DOI 10.5935/0103-507X.20220114-en
To compare the perceptions of patients’ relatives with the perceptions of health professionals regarding a flexible visitation model in intensive care units.
Cross-sectional study. This study was carried out with patients’ relatives and members of the care team of a clinical-surgical intensive care unit with a flexible visitation model (12 hours/day) from September to December 2018. The evaluation of the flexible visitation policy was carried out through an open visitation instrument composed of 22 questions divided into three domains (evaluation of family stress, provision of information, and interference in the work of the team).
Ninety-five accompanying relatives and 95 members of the care team were analyzed. The perceptions of relatives regarding the decrease in anxiety and stress with flexible visitation was higher than the perceptions of the team (91.6% versus 58.9%, p < 0.001), and the family also had a more positive perception regarding the provision of information (86.3% versus 64.2%, p < 0.001). The care team believed that the presence of the relative made it difficult to provide care to the patient and caused work interruptions (46.3% versus 6.3%, p < 0.001).
Family members and staff-intensive care unit teams have different perceptions about flexible visits in the intensive care unit. However, a positive view regarding the perception of decreased anxiety and stress among the family members and greater information and contributions to patient recovery predominates.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):374-379
DOI 10.5935/0103-507X.20220114-en
To compare the perceptions of patients’ relatives with the perceptions of health professionals regarding a flexible visitation model in intensive care units.
Cross-sectional study. This study was carried out with patients’ relatives and members of the care team of a clinical-surgical intensive care unit with a flexible visitation model (12 hours/day) from September to December 2018. The evaluation of the flexible visitation policy was carried out through an open visitation instrument composed of 22 questions divided into three domains (evaluation of family stress, provision of information, and interference in the work of the team).
Ninety-five accompanying relatives and 95 members of the care team were analyzed. The perceptions of relatives regarding the decrease in anxiety and stress with flexible visitation was higher than the perceptions of the team (91.6% versus 58.9%, p < 0.001), and the family also had a more positive perception regarding the provision of information (86.3% versus 64.2%, p < 0.001). The care team believed that the presence of the relative made it difficult to provide care to the patient and caused work interruptions (46.3% versus 6.3%, p < 0.001).
Family members and staff-intensive care unit teams have different perceptions about flexible visits in the intensive care unit. However, a positive view regarding the perception of decreased anxiety and stress among the family members and greater information and contributions to patient recovery predominates.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):227-236
DOI 10.5935/0103-507X.20220020-en
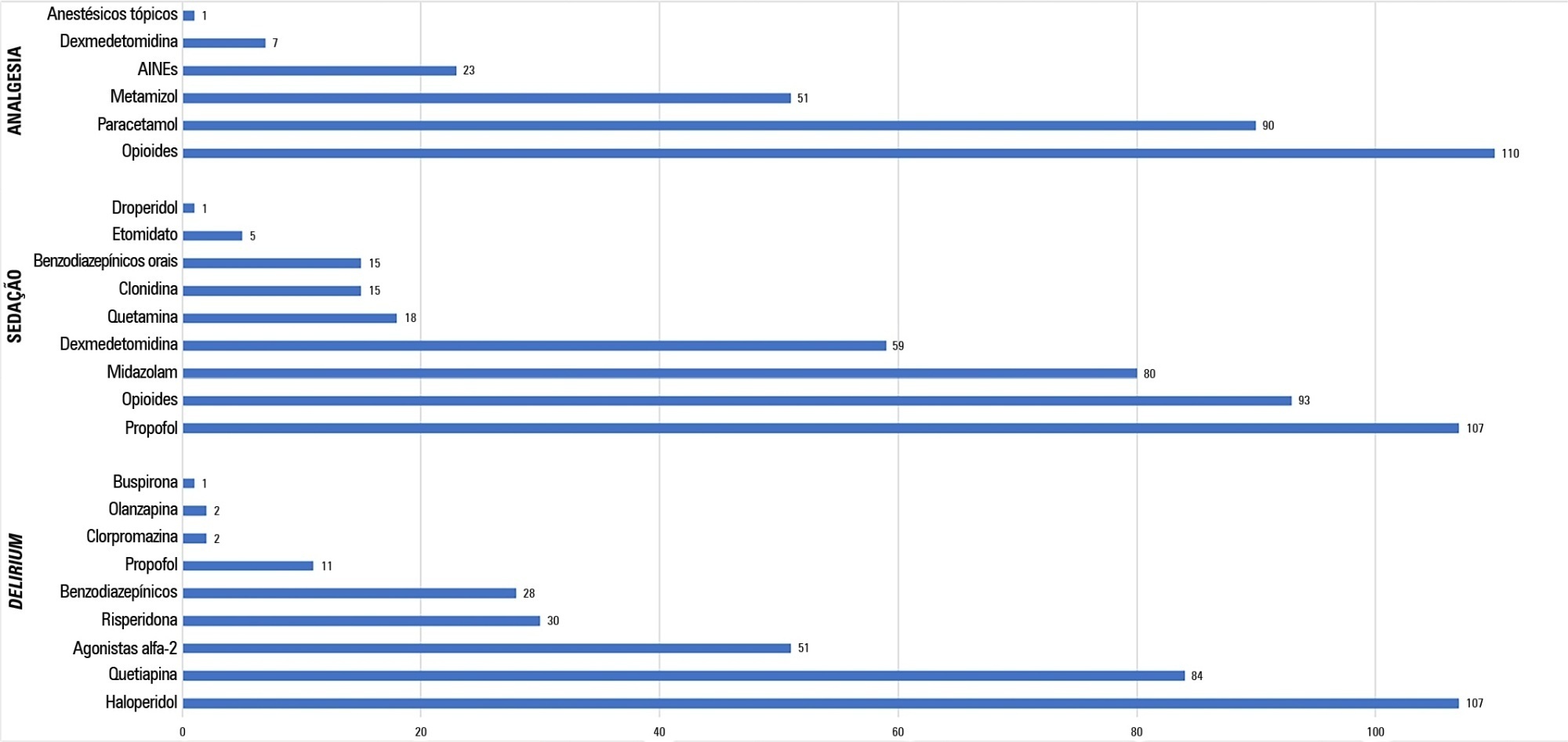
To establish current Portuguese critical care practices regarding analgesia, sedation, and delirium based on a comparison between the activities reported and daily clinical practice.
A national survey was conducted among physicians invited to report their practice toward analgesia, sedation, and delirium in intensive care units. A point prevalence study was performed to analyze daily practices.
A total of 117 physicians answered the survey, and 192 patients were included in the point prevalence study. Survey and point prevalence studies reflect a high sedation assessment (92%; 88.5%), with the Richmond Agitated Sedation Scale being the most reported and used scale (41.7%; 58.2%) and propofol being the most reported and used medication (91.4%; 58.6%). Midazolam prescribing was reported by 68.4% of responders, but a point prevalence study revealed a use of 27.6%.
The results from the survey did not accurately reflect the common practices in Portuguese intensive care units, as reported in the point prevalence study. Efforts should be made specifically to avoid oversedation and to promote delirium assessment.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):227-236
DOI 10.5935/0103-507X.20220020-en
To establish current Portuguese critical care practices regarding analgesia, sedation, and delirium based on a comparison between the activities reported and daily clinical practice.
A national survey was conducted among physicians invited to report their practice toward analgesia, sedation, and delirium in intensive care units. A point prevalence study was performed to analyze daily practices.
A total of 117 physicians answered the survey, and 192 patients were included in the point prevalence study. Survey and point prevalence studies reflect a high sedation assessment (92%; 88.5%), with the Richmond Agitated Sedation Scale being the most reported and used scale (41.7%; 58.2%) and propofol being the most reported and used medication (91.4%; 58.6%). Midazolam prescribing was reported by 68.4% of responders, but a point prevalence study revealed a use of 27.6%.
The results from the survey did not accurately reflect the common practices in Portuguese intensive care units, as reported in the point prevalence study. Efforts should be made specifically to avoid oversedation and to promote delirium assessment.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):262-271
DOI 10.5935/0103-507X.20220024-en
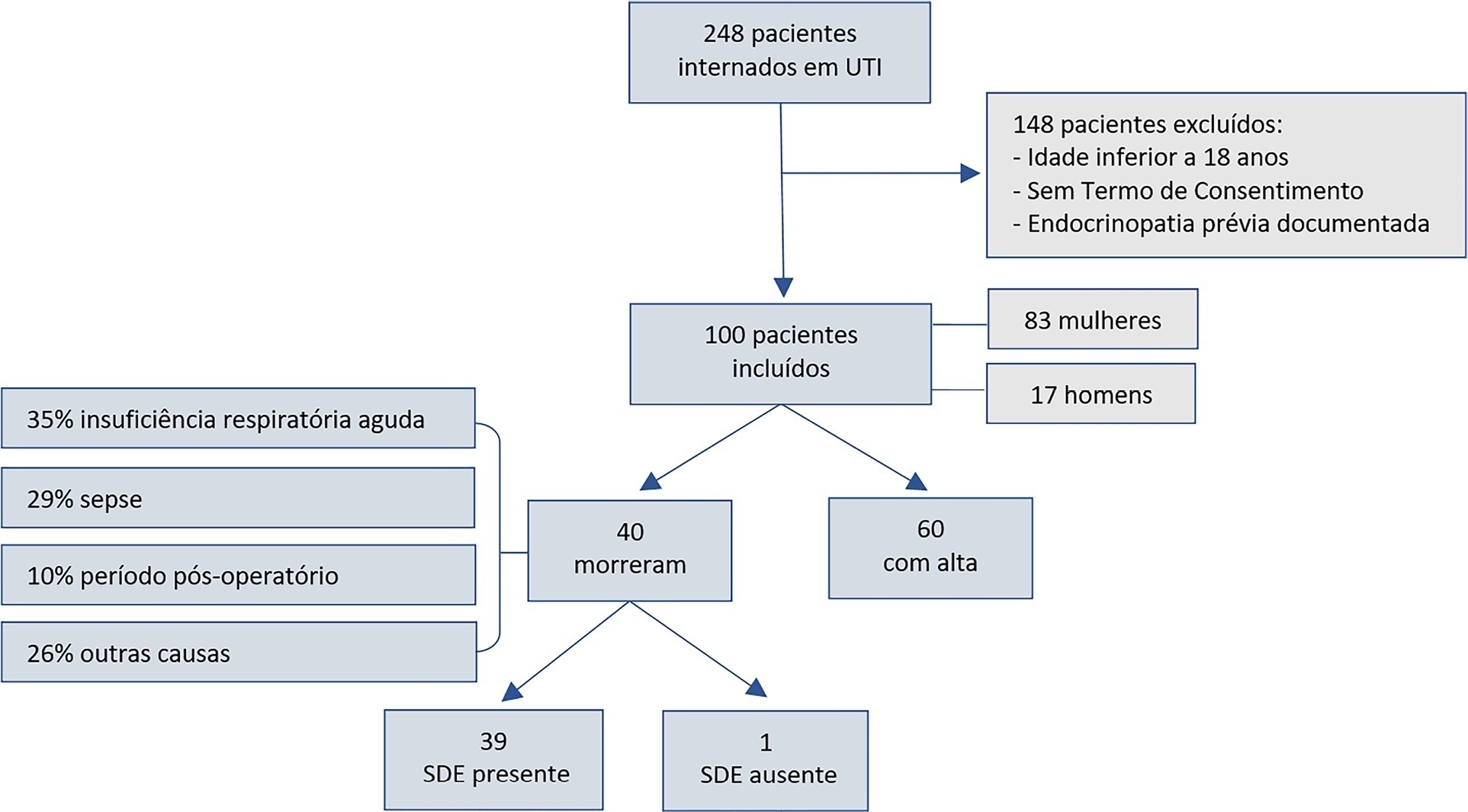
To assess euthyroid sick syndrome as a prognostic factor in patients in the intensive care unit; to detect factors that may affect mortality; and to develop an equation to calculate death probability.
This was a longitudinal, observational, nonconcurrent cohort study developed in the intensive care unit of Fundação Santa Casa de Misericórdia do Pará. One hundred adults with no prior documented endocrinopathy were submitted to a 20mL blood sample collection for the measurement of thyroid stimulating hormone, free tetraiodothyronine, free triiodothyronine and reverse triiodothyronine.
Most patients were female, aged 20 to 29 years. Most patients who died were older (median age of 48 years), and euthyroid sick syndrome was present in 97.5% of them. Euthyroid sick syndrome was related to death, comorbidities, age and length of stay in the intensive care unit (median of 7.5 days).
The main limitation of this study is the fact that it was conducted in a reference hospital for maternal and child care; therefore, there was a greater number of female patients and, consequently, a sampling bias existed. However, opportune measurement of free and reverse triiodothyronine levels in critical patients and application of the proposed equation are suggested.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):262-271
DOI 10.5935/0103-507X.20220024-en
To assess euthyroid sick syndrome as a prognostic factor in patients in the intensive care unit; to detect factors that may affect mortality; and to develop an equation to calculate death probability.
This was a longitudinal, observational, nonconcurrent cohort study developed in the intensive care unit of Fundação Santa Casa de Misericórdia do Pará. One hundred adults with no prior documented endocrinopathy were submitted to a 20mL blood sample collection for the measurement of thyroid stimulating hormone, free tetraiodothyronine, free triiodothyronine and reverse triiodothyronine.
Most patients were female, aged 20 to 29 years. Most patients who died were older (median age of 48 years), and euthyroid sick syndrome was present in 97.5% of them. Euthyroid sick syndrome was related to death, comorbidities, age and length of stay in the intensive care unit (median of 7.5 days).
The main limitation of this study is the fact that it was conducted in a reference hospital for maternal and child care; therefore, there was a greater number of female patients and, consequently, a sampling bias existed. However, opportune measurement of free and reverse triiodothyronine levels in critical patients and application of the proposed equation are suggested.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)