Myocarditis Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):443-451
DOI 10.5935/0103-507X.20220440-en
To characterize myocardial injury and cardiovascular complications and their predictors in severe and critical COVID-19 patients admitted to the intensive care unit.
This was an observational cohort study of severe and critical COVID-19 patients admitted to the intensive care unit. Myocardial injury was defined as blood levels of cardiac troponin above the 99th percentile upper reference limit. Cardiovascular events considered were the composite of deep vein thrombosis, pulmonary embolism, stroke, myocardial infarction, acute limb ischemia, mesenteric ischemia, heart failure and arrhythmia. Univariate and multivariate logistic regression or Cox proportional hazard models were used to determine predictors of myocardial injury.
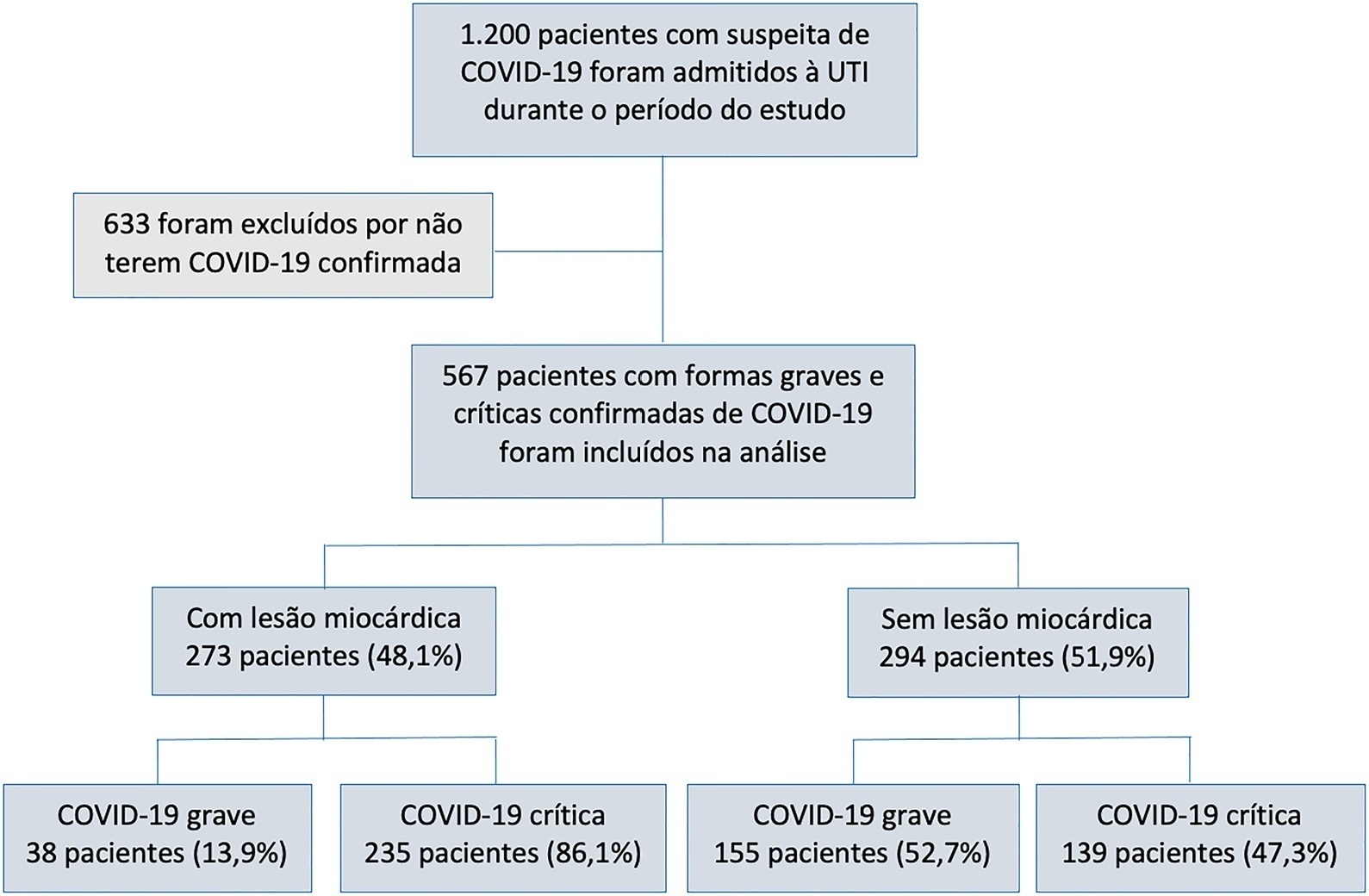
Of 567 patients with severe and critical COVID-19 admitted to the intensive care unit, 273 (48.1%) had myocardial injury. Of the 374 patients with critical COVID-19, 86.1% had myocardial injury, and also showed more organ dysfunction and higher 28-day mortality (56.6% versus 27.1%, p < 0.001). Advanced age, arterial hypertension and immune modulator use were predictors of myocardial injury. Cardiovascular complications occurred in 19.9% of patients with severe and critical COVID-19 admitted to the intensive care unit, with most events occurring in patients with myocardial injury (28.2% versus 12.2%, p < 0.001). The occurrence of an early cardiovascular event during intensive care unit stay was associated with higher 28-day mortality compared with late or no events (57.1% versus 34% versus 41.8%, p = 0.01).
Myocardial injury and cardiovascular complications were commonly found in patients with severe and critical forms of COVID-19 admitted to the intensive care unit, and both were associated with increased mortality in these patients.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):443-451
DOI 10.5935/0103-507X.20220440-en
To characterize myocardial injury and cardiovascular complications and their predictors in severe and critical COVID-19 patients admitted to the intensive care unit.
This was an observational cohort study of severe and critical COVID-19 patients admitted to the intensive care unit. Myocardial injury was defined as blood levels of cardiac troponin above the 99th percentile upper reference limit. Cardiovascular events considered were the composite of deep vein thrombosis, pulmonary embolism, stroke, myocardial infarction, acute limb ischemia, mesenteric ischemia, heart failure and arrhythmia. Univariate and multivariate logistic regression or Cox proportional hazard models were used to determine predictors of myocardial injury.
Of 567 patients with severe and critical COVID-19 admitted to the intensive care unit, 273 (48.1%) had myocardial injury. Of the 374 patients with critical COVID-19, 86.1% had myocardial injury, and also showed more organ dysfunction and higher 28-day mortality (56.6% versus 27.1%, p < 0.001). Advanced age, arterial hypertension and immune modulator use were predictors of myocardial injury. Cardiovascular complications occurred in 19.9% of patients with severe and critical COVID-19 admitted to the intensive care unit, with most events occurring in patients with myocardial injury (28.2% versus 12.2%, p < 0.001). The occurrence of an early cardiovascular event during intensive care unit stay was associated with higher 28-day mortality compared with late or no events (57.1% versus 34% versus 41.8%, p = 0.01).
Myocardial injury and cardiovascular complications were commonly found in patients with severe and critical forms of COVID-19 admitted to the intensive care unit, and both were associated with increased mortality in these patients.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):321-326
DOI 10.5935/0103-507X.20140046
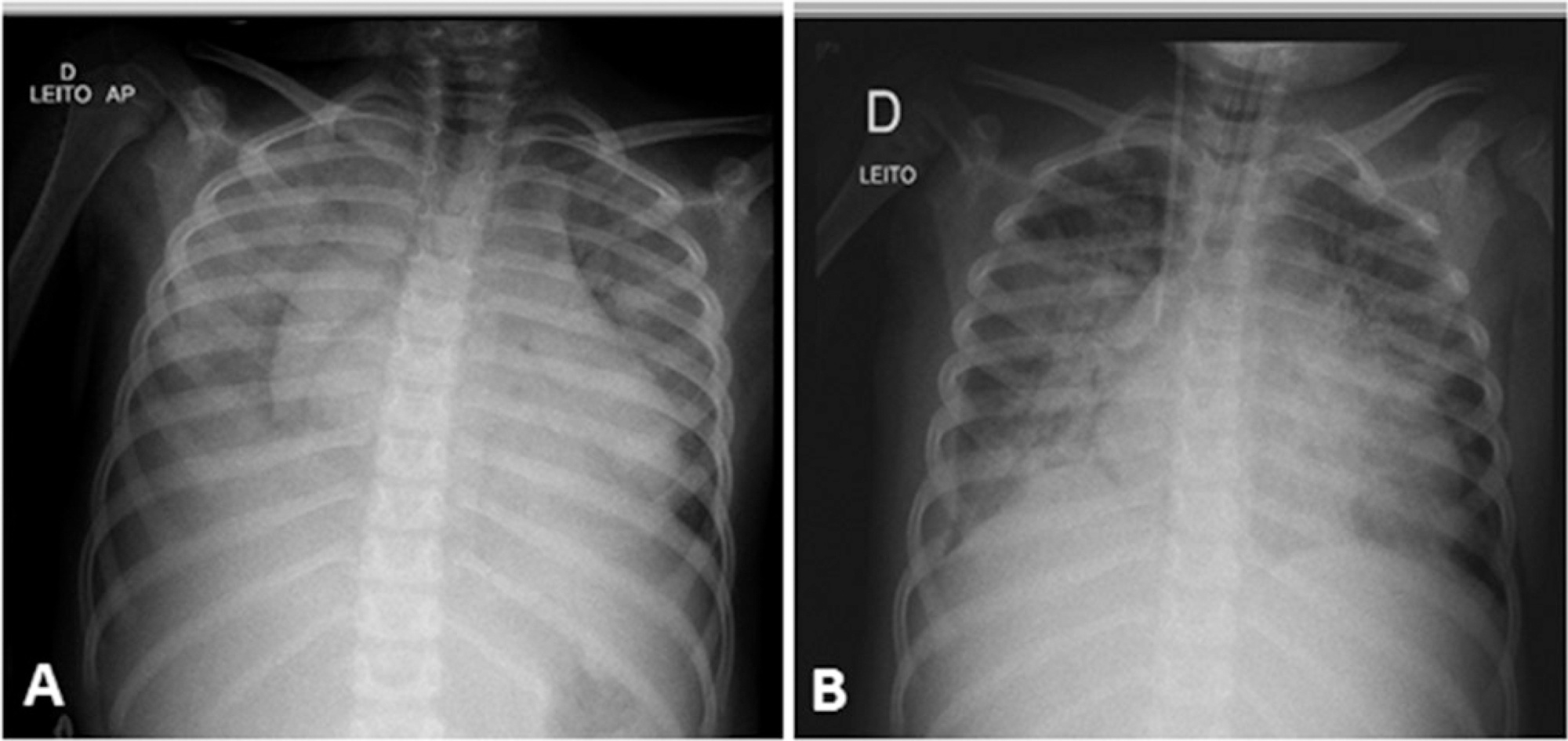
A case of fulminant myocarditis associated with the H1N1 influenza virus. This case report describes the patient's clinical course and emphasizes the importance of bedside echocardiography as an aid in the early diagnosis and management of children with severe myocardial dysfunction. It also discusses aspects relevant to the treatment and prognosis of fulminant myocarditis. The patient was a female, 4 years and 8 months old, previously healthy and with a history of flu symptoms in the past two weeks. The patient was admitted to the emergency room with signs of hemodynamic instability, requiring ventilatory support and vasoactive drugs. The laboratory tests, chest X-ray and echocardiogram suggested the presence of myocarditis. The test for H1N1 in nasopharyngeal secretions was positive. The patient evolved to refractory cardiogenic shock despite the clinical measures applied and died 48 hours after admission to the intensive care unit. The H1N1 influenza virus is an etiological agent associated with acute myocarditis, but there are few reported cases of fulminant myocarditis caused by the H1N1 virus. The identification of signs and symptoms suggestive of fulminant progression should be immediate, and bedside echocardiography is a useful tool for the early detection of myocardial dysfunction and for therapeutic guidance. The use of immunosuppressive therapy and antiviral therapy in acute myocarditis of viral etiology is controversial; hence, the treatment is based on hemodynamic and ventilatory support. The use of hemodynamic support by extracorporeal membrane oxygenation emerges as a promising treatment.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):321-326
DOI 10.5935/0103-507X.20140046
A case of fulminant myocarditis associated with the H1N1 influenza virus. This case report describes the patient's clinical course and emphasizes the importance of bedside echocardiography as an aid in the early diagnosis and management of children with severe myocardial dysfunction. It also discusses aspects relevant to the treatment and prognosis of fulminant myocarditis. The patient was a female, 4 years and 8 months old, previously healthy and with a history of flu symptoms in the past two weeks. The patient was admitted to the emergency room with signs of hemodynamic instability, requiring ventilatory support and vasoactive drugs. The laboratory tests, chest X-ray and echocardiogram suggested the presence of myocarditis. The test for H1N1 in nasopharyngeal secretions was positive. The patient evolved to refractory cardiogenic shock despite the clinical measures applied and died 48 hours after admission to the intensive care unit. The H1N1 influenza virus is an etiological agent associated with acute myocarditis, but there are few reported cases of fulminant myocarditis caused by the H1N1 virus. The identification of signs and symptoms suggestive of fulminant progression should be immediate, and bedside echocardiography is a useful tool for the early detection of myocardial dysfunction and for therapeutic guidance. The use of immunosuppressive therapy and antiviral therapy in acute myocarditis of viral etiology is controversial; hence, the treatment is based on hemodynamic and ventilatory support. The use of hemodynamic support by extracorporeal membrane oxygenation emerges as a promising treatment.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)