Critical care Archives - Critical Care Science (CCS)

Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(2):227-236
DOI 10.5935/0103-507X.20220020-en
To establish current Portuguese critical care practices regarding analgesia, sedation, and delirium based on a comparison between the activities reported and daily clinical practice.
A national survey was conducted among physicians invited to report their practice toward analgesia, sedation, and delirium in intensive care units. A point prevalence study was performed to analyze daily practices.
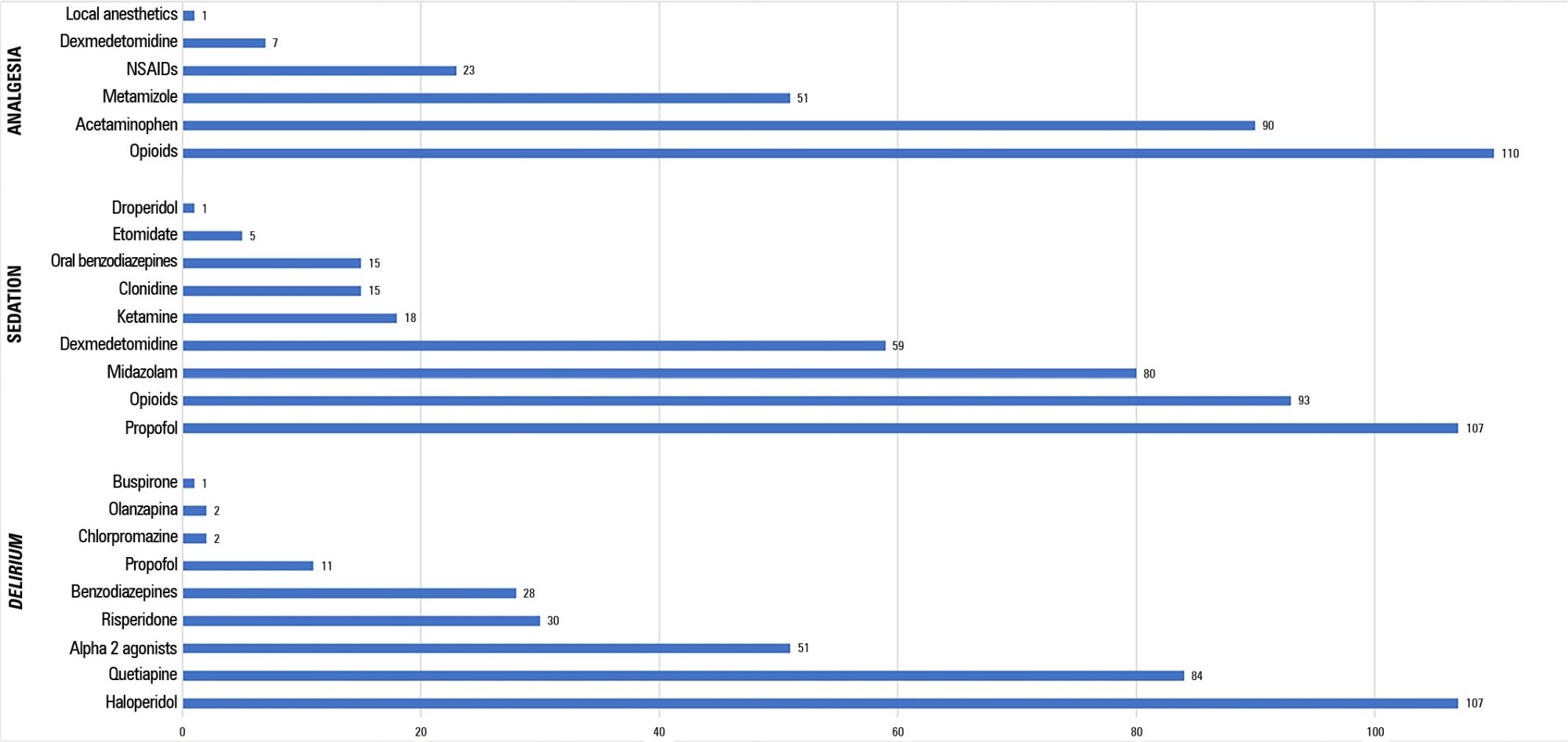
A total of 117 physicians answered the survey, and 192 patients were included in the point prevalence study. Survey and point prevalence studies reflect a high sedation assessment (92%; 88.5%), with the Richmond Agitated Sedation Scale being the most reported and used scale (41.7%; 58.2%) and propofol being the most reported and used medication (91.4%; 58.6%). Midazolam prescribing was reported by 68.4% of responders, but a point prevalence study revealed a use of 27.6%.
The results from the survey did not accurately reflect the common practices in Portuguese intensive care units, as reported in the point prevalence study. Efforts should be made specifically to avoid oversedation and to promote delirium assessment.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(2):227-236
DOI 10.5935/0103-507X.20220020-en
To establish current Portuguese critical care practices regarding analgesia, sedation, and delirium based on a comparison between the activities reported and daily clinical practice.
A national survey was conducted among physicians invited to report their practice toward analgesia, sedation, and delirium in intensive care units. A point prevalence study was performed to analyze daily practices.
A total of 117 physicians answered the survey, and 192 patients were included in the point prevalence study. Survey and point prevalence studies reflect a high sedation assessment (92%; 88.5%), with the Richmond Agitated Sedation Scale being the most reported and used scale (41.7%; 58.2%) and propofol being the most reported and used medication (91.4%; 58.6%). Midazolam prescribing was reported by 68.4% of responders, but a point prevalence study revealed a use of 27.6%.
The results from the survey did not accurately reflect the common practices in Portuguese intensive care units, as reported in the point prevalence study. Efforts should be made specifically to avoid oversedation and to promote delirium assessment.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):124-130
DOI 10.5935/0103-507X.20220006-en
The current study assessed the prevalence of troponin elevation and its capacity to predict 60day mortality in COVID-19 patients in intensive care.
A longitudinal prospective single-center study was performed on a cohort of patients in intensive care due to a COVID-19 diagnosis confirmed using real-time test polymerase chain reaction from May to December 2020. A Receiver Operating Characteristic curve was constructed to predict death according to troponin level by calculating the area under the curve and its confidence intervals. A Cox proportional hazards model was generated to report the hazard ratios with confidence intervals of 95% and the p value for its association with 60day mortality.
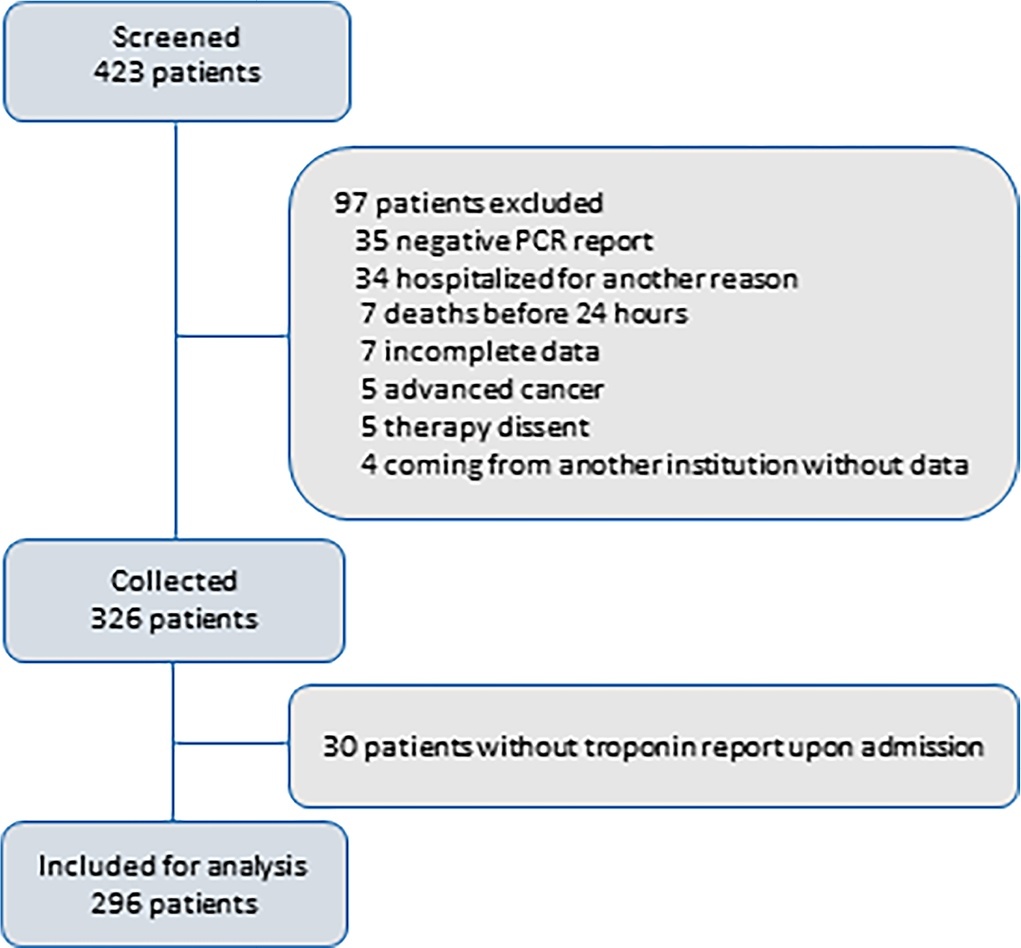
A total of 296 patients were included with a 51% 60-day mortality rate. Troponin was positive in 39.9% (29.6% versus 49.7% in survivors and non-survivors, respectively). An area under the curve of 0.65 was found (95%CI: 0.59 - 0.71) to predict mortality. The Cox univariate model demonstrated a hazard ratio of 1.94 (95%CI: 1.41 - 2.67) and p < 0.001, but this relationship did not remain in the multivariate model, in which the hazard ratio was 1.387 (95%CI: 0.21 - 1.56) and the p value was 0.12.
Troponin elevation is frequently found in patients in intensive care for COVID-19. Although its levels are higher in patients who die, no relationship was found in a multivariate model, which indicates that troponin should not be used as an only prognostic marker for mortality in this population.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):124-130
DOI 10.5935/0103-507X.20220006-en
The current study assessed the prevalence of troponin elevation and its capacity to predict 60day mortality in COVID-19 patients in intensive care.
A longitudinal prospective single-center study was performed on a cohort of patients in intensive care due to a COVID-19 diagnosis confirmed using real-time test polymerase chain reaction from May to December 2020. A Receiver Operating Characteristic curve was constructed to predict death according to troponin level by calculating the area under the curve and its confidence intervals. A Cox proportional hazards model was generated to report the hazard ratios with confidence intervals of 95% and the p value for its association with 60day mortality.
A total of 296 patients were included with a 51% 60-day mortality rate. Troponin was positive in 39.9% (29.6% versus 49.7% in survivors and non-survivors, respectively). An area under the curve of 0.65 was found (95%CI: 0.59 - 0.71) to predict mortality. The Cox univariate model demonstrated a hazard ratio of 1.94 (95%CI: 1.41 - 2.67) and p < 0.001, but this relationship did not remain in the multivariate model, in which the hazard ratio was 1.387 (95%CI: 0.21 - 1.56) and the p value was 0.12.
Troponin elevation is frequently found in patients in intensive care for COVID-19. Although its levels are higher in patients who die, no relationship was found in a multivariate model, which indicates that troponin should not be used as an only prognostic marker for mortality in this population.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):96-106
DOI 10.5935/0103-507X.20220004-en
Early reversion of sepsis-induced tissue hypoperfusion is essential for survival in septic shock. However, consensus regarding the best initial resuscitation strategy is lacking given that interventions designed for the entire population with septic shock might produce unnecessary fluid administration. This article reports the rationale, study design and analysis plan of the ANDROMEDA-2 study, which aims to determine whether a peripheral perfusion-guided strategy consisting of capillary refill time-targeted resuscitation based on clinical and hemodynamic phenotypes is associated with a decrease in a composite outcome of mortality, time to organ support cessation, and hospital length of stay compared to standard care in patients with early (< 4 hours of diagnosis) septic shock.
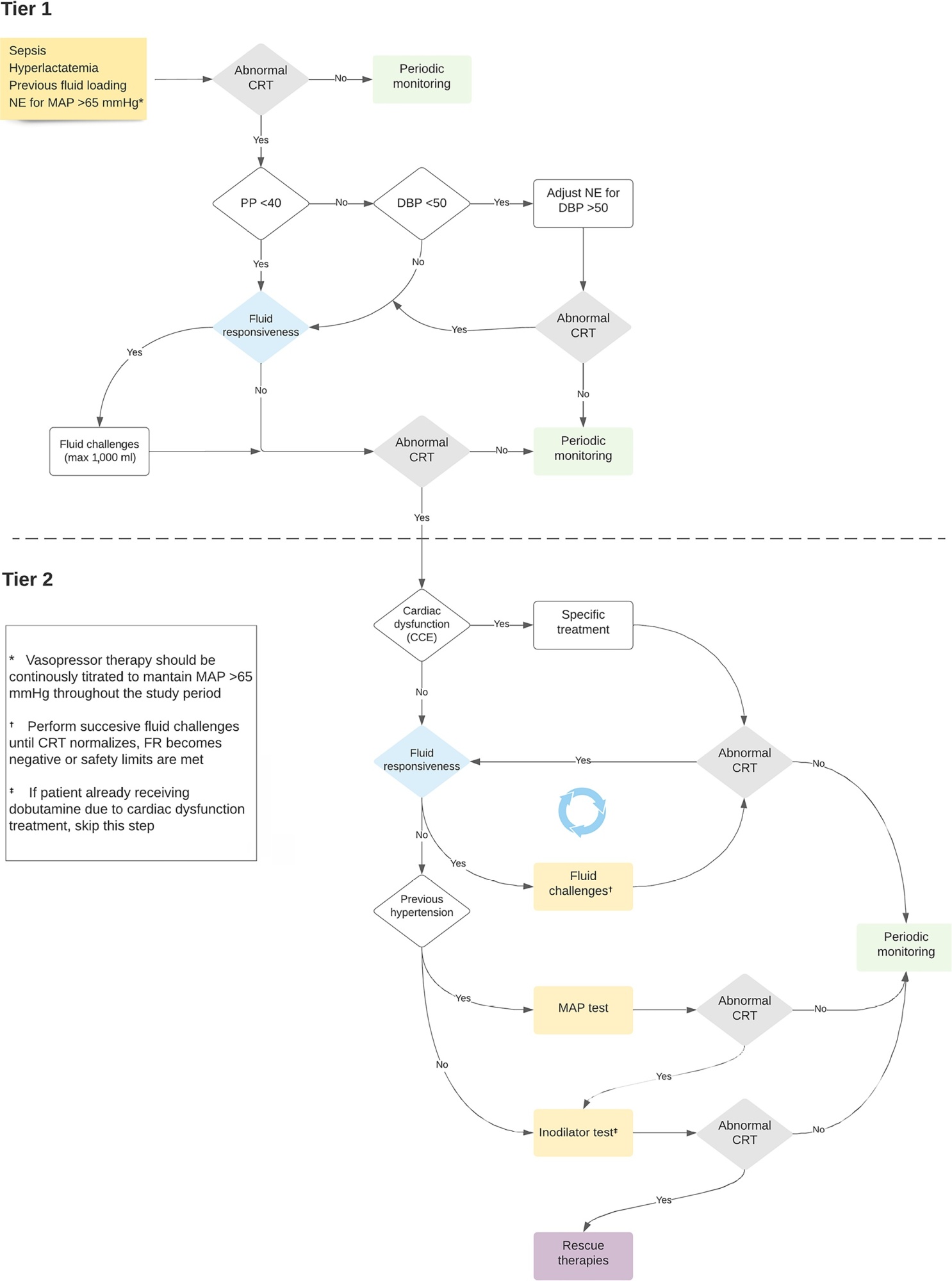
The ANDROMEDA-2 study is a multicenter, multinational randomized controlled trial. In the intervention group, capillary refill time will be measured hourly for 6 hours. If abnormal, patients will enter an algorithm starting with pulse pressure assessment. Patients with pulse pressure less than 40mmHg will be tested for fluid responsiveness and receive fluids accordingly. In patients with pulse pressure > 40mmHg, norepinephrine will be titrated to maintain diastolic arterial pressure > 50mmHg. Patients who fail to normalize capillary refill time after the previous steps will be subjected to critical care echocardiography for cardiac dysfunction evaluation and subsequent management. Finally, vasopressor and inodilator tests will be performed to further optimize perfusion. A sample size of 1,500 patients will provide 88% power to demonstrate superiority of the capillary refill time-targeted strategy.
If hemodynamic phenotype-based, capillary refill time-targeted resuscitation demonstrates to be a superior strategy, care processes in septic shock resuscitation can be optimized with bedside tools.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):96-106
DOI 10.5935/0103-507X.20220004-en
Early reversion of sepsis-induced tissue hypoperfusion is essential for survival in septic shock. However, consensus regarding the best initial resuscitation strategy is lacking given that interventions designed for the entire population with septic shock might produce unnecessary fluid administration. This article reports the rationale, study design and analysis plan of the ANDROMEDA-2 study, which aims to determine whether a peripheral perfusion-guided strategy consisting of capillary refill time-targeted resuscitation based on clinical and hemodynamic phenotypes is associated with a decrease in a composite outcome of mortality, time to organ support cessation, and hospital length of stay compared to standard care in patients with early (< 4 hours of diagnosis) septic shock.
The ANDROMEDA-2 study is a multicenter, multinational randomized controlled trial. In the intervention group, capillary refill time will be measured hourly for 6 hours. If abnormal, patients will enter an algorithm starting with pulse pressure assessment. Patients with pulse pressure less than 40mmHg will be tested for fluid responsiveness and receive fluids accordingly. In patients with pulse pressure > 40mmHg, norepinephrine will be titrated to maintain diastolic arterial pressure > 50mmHg. Patients who fail to normalize capillary refill time after the previous steps will be subjected to critical care echocardiography for cardiac dysfunction evaluation and subsequent management. Finally, vasopressor and inodilator tests will be performed to further optimize perfusion. A sample size of 1,500 patients will provide 88% power to demonstrate superiority of the capillary refill time-targeted strategy.
If hemodynamic phenotype-based, capillary refill time-targeted resuscitation demonstrates to be a superior strategy, care processes in septic shock resuscitation can be optimized with bedside tools.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
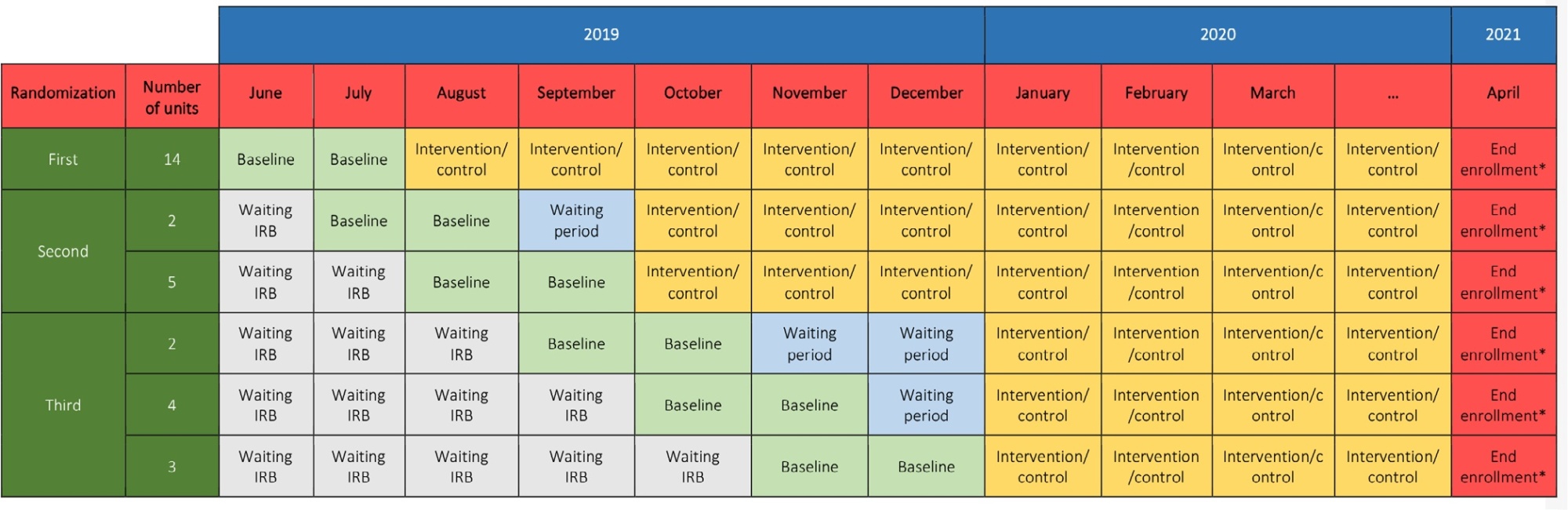
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):176-184
DOI 10.5935/0103-507X.20220012-en
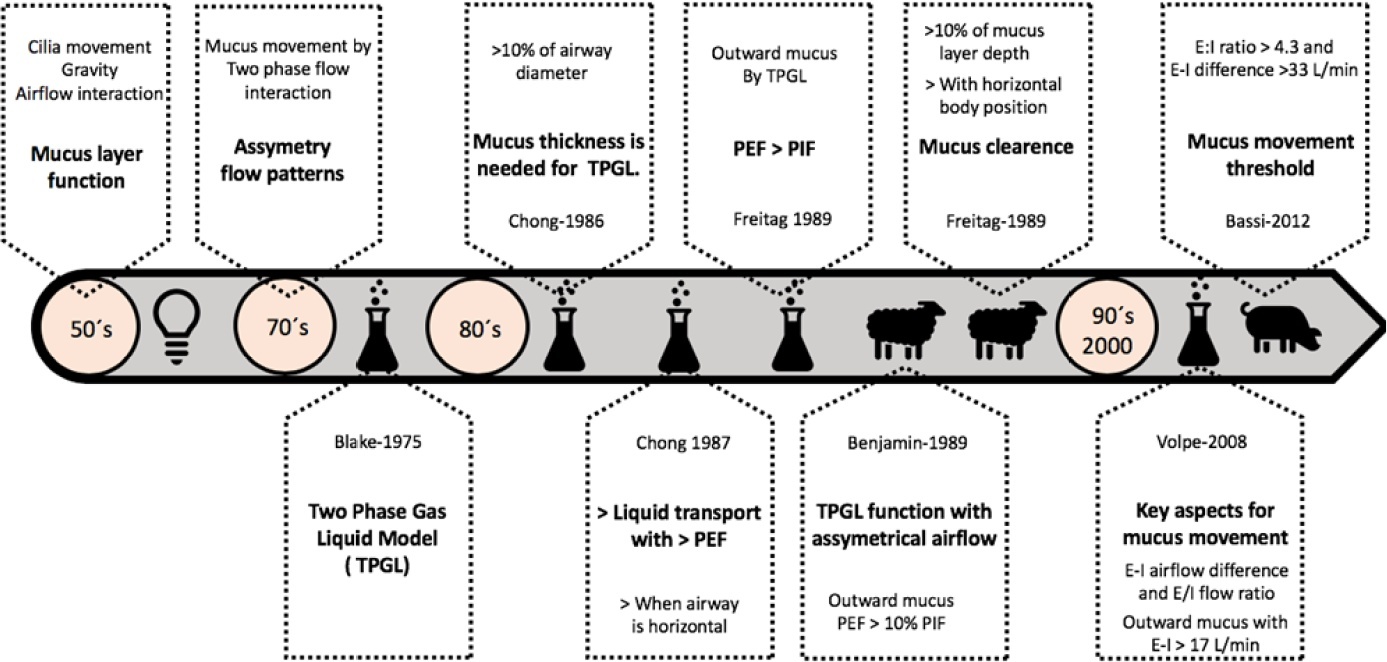
Defective management of secretions is one of the most frequent complications in invasive mechanically ventilated patients. Clearance of secretions through chest physiotherapy is a critical aspect of the treatment of these patients. Manual rib cage compression is one of the most practiced chest physiotherapy techniques in ventilated patients; however, its impact on clinical outcomes remains controversial due to methodological issues and poor understanding of its action. In this review, we present a detailed analysis of the physical principles involved in rib cage compression technique performance, as well as the physiological effects observed in experimental and clinical studies, which show that the use of brief and vigorous rib cage compression, based on increased expiratory flows (expiratory-inspiratory airflow difference of > 33L/minute), can improve mucus movement toward the glottis. On the other hand, the use of soft and gradual rib cage compression throughout the whole expiratory phase does not impact the expiratory flows, resulting in ineffective or undesired effects in some cases. More physiological studies are needed to understand the principles of the rib cage compression technique in ventilated humans. However, according to the evidence, rib cage compression has more potential benefits than risks, so its implementation should be promoted.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):176-184
DOI 10.5935/0103-507X.20220012-en
Defective management of secretions is one of the most frequent complications in invasive mechanically ventilated patients. Clearance of secretions through chest physiotherapy is a critical aspect of the treatment of these patients. Manual rib cage compression is one of the most practiced chest physiotherapy techniques in ventilated patients; however, its impact on clinical outcomes remains controversial due to methodological issues and poor understanding of its action. In this review, we present a detailed analysis of the physical principles involved in rib cage compression technique performance, as well as the physiological effects observed in experimental and clinical studies, which show that the use of brief and vigorous rib cage compression, based on increased expiratory flows (expiratory-inspiratory airflow difference of > 33L/minute), can improve mucus movement toward the glottis. On the other hand, the use of soft and gradual rib cage compression throughout the whole expiratory phase does not impact the expiratory flows, resulting in ineffective or undesired effects in some cases. More physiological studies are needed to understand the principles of the rib cage compression technique in ventilated humans. However, according to the evidence, rib cage compression has more potential benefits than risks, so its implementation should be promoted.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):141-146
DOI 10.5935/0103-507X.20220008-en
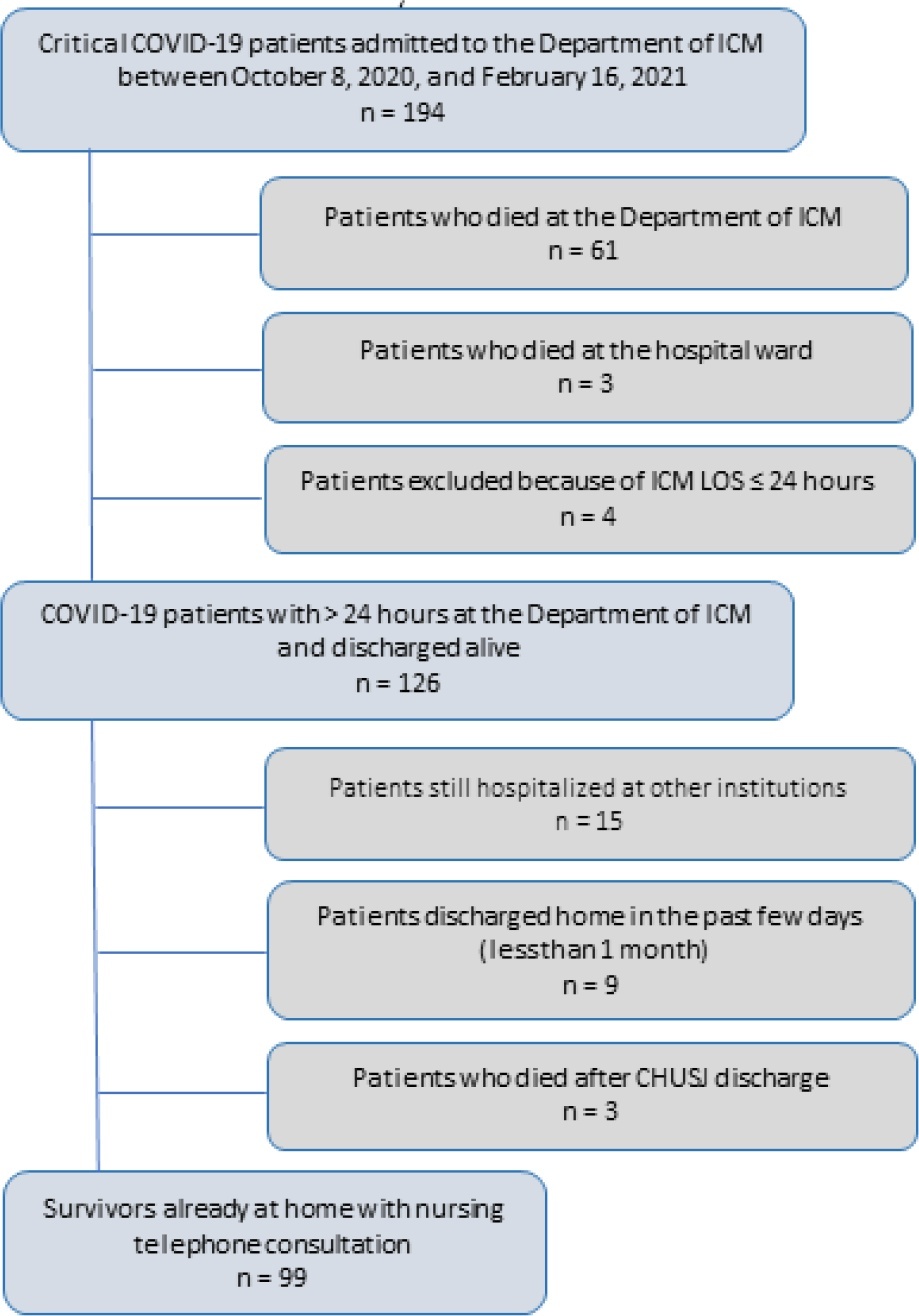
To assess early postdischarge health-related quality of life and disability of all survivors of critical COVID-19 admitted for more than 24 hours to na intensive care unit..
Study carried out at the Intensive Care Medicine Department of Centro Hospitalar Universitário São João from 8th October 2020 to 16th February 2021. Approximately 1 month after hospital discharge, an intensive care-trained nurse performed a telephone consultation with 99 survivors already at home applying the EuroQol Five-Dimensional Five-Level questionnaire and the 12-item World Health Organization Disability Assessment Schedule 2.0.
The mean age of the population studied was 63 ± 12 years, and 32.5% were submitted to invasive mechanical ventilation. Their mean Simplified Acute Physiologic Score was 35 ± 14, and the Charlson Comorbidity Index was 3 ± 2. Intensive care medicine and hospital lengths of stay were 13 ± 22 and 22 ± 25 days, respectively. The mean EuroQol Visual Analog Scale was 65% (± 21), and only 35.3% had no or slight problems performing their usual activities, most having some degree of pain/discomfort and anxiety/depression. The 12-item World Health Organization Disability Assessment Schedule 2.0 showed marked impairments in terms of reassuring usual work or community activities and mobility. The use of both tools suggested that their health status was worse than their perception of it.
This early identification of sequelae may help define flows and priorities for rehabilitation and reinsertion after critical COVID-19.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):141-146
DOI 10.5935/0103-507X.20220008-en
To assess early postdischarge health-related quality of life and disability of all survivors of critical COVID-19 admitted for more than 24 hours to na intensive care unit..
Study carried out at the Intensive Care Medicine Department of Centro Hospitalar Universitário São João from 8th October 2020 to 16th February 2021. Approximately 1 month after hospital discharge, an intensive care-trained nurse performed a telephone consultation with 99 survivors already at home applying the EuroQol Five-Dimensional Five-Level questionnaire and the 12-item World Health Organization Disability Assessment Schedule 2.0.
The mean age of the population studied was 63 ± 12 years, and 32.5% were submitted to invasive mechanical ventilation. Their mean Simplified Acute Physiologic Score was 35 ± 14, and the Charlson Comorbidity Index was 3 ± 2. Intensive care medicine and hospital lengths of stay were 13 ± 22 and 22 ± 25 days, respectively. The mean EuroQol Visual Analog Scale was 65% (± 21), and only 35.3% had no or slight problems performing their usual activities, most having some degree of pain/discomfort and anxiety/depression. The 12-item World Health Organization Disability Assessment Schedule 2.0 showed marked impairments in terms of reassuring usual work or community activities and mobility. The use of both tools suggested that their health status was worse than their perception of it.
This early identification of sequelae may help define flows and priorities for rehabilitation and reinsertion after critical COVID-19.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(4):635-639
DOI 10.5935/0103-507X.20210089
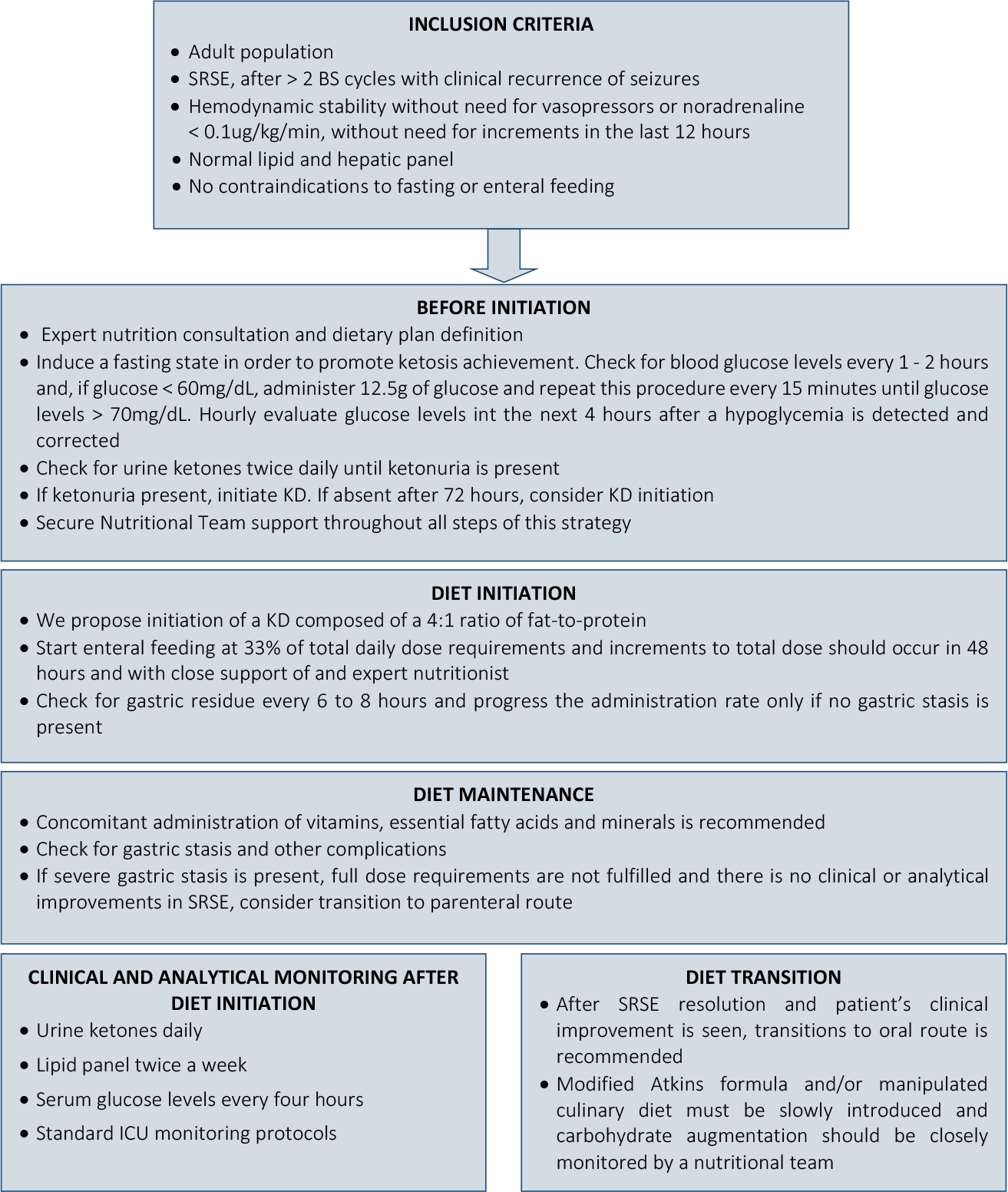
Super-refractory status epilepticus is defined as seizures that persist or reemerge in the setting of an intravenous anesthetic infusion for more than 24 hours. In recent years, attention has been driven to the potential benefits of a ketogenic diet in the management of these patients. However, the specific role of this strategy in the adult population, as well as its underlying mechanism of action and optimal time for the initiation and management of complications, remain widely debatable. We report a case series of three patients admitted to an intensive care unit due to super-refractory status epilepticus who were managed with a ketogenic diet and propose a clinical approach to its initiation, transition, and management of clinical intercurrences.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(4):635-639
DOI 10.5935/0103-507X.20210089
Super-refractory status epilepticus is defined as seizures that persist or reemerge in the setting of an intravenous anesthetic infusion for more than 24 hours. In recent years, attention has been driven to the potential benefits of a ketogenic diet in the management of these patients. However, the specific role of this strategy in the adult population, as well as its underlying mechanism of action and optimal time for the initiation and management of complications, remain widely debatable. We report a case series of three patients admitted to an intensive care unit due to super-refractory status epilepticus who were managed with a ketogenic diet and propose a clinical approach to its initiation, transition, and management of clinical intercurrences.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(4):600-615
DOI 10.5935/0103-507X.20210087
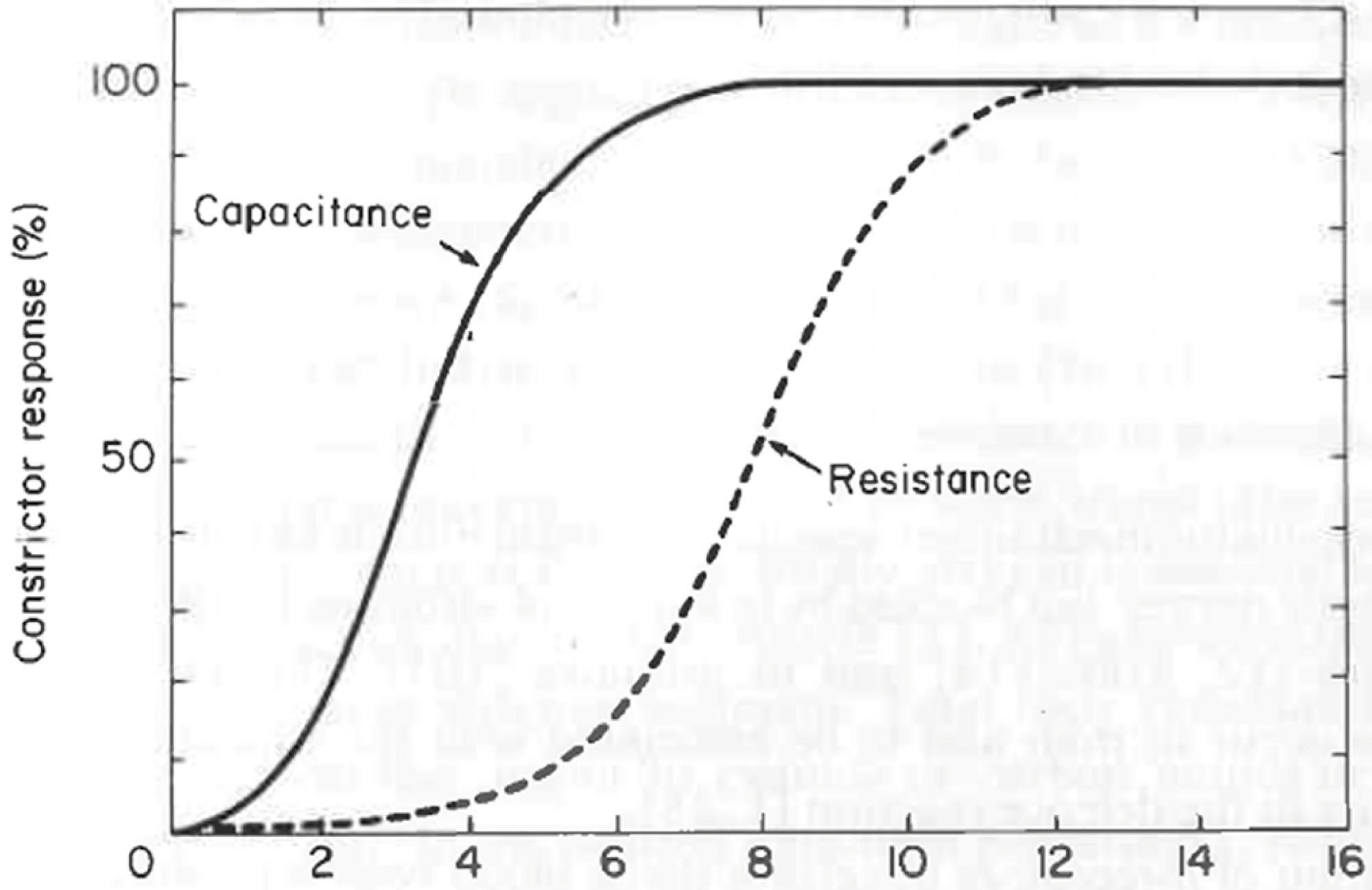
Cardiac, ventilatory and kidney management in the critical care setting has been optimized over the past decades. Cognition and sedation represent one of the last remaning challenges. As conventional sedation is suboptimal and as the sedation evoked by alpha-2 adrenergic agonists (“cooperative” sedation with dexmedetomidine, clonidine or guanfacine) represents a valuable alternative, this manuscript covers three practical topics for which evidence-based medicine is lacking: a) Switching from conventional to cooperative sedation (“switching”): the short answer is the abrupt withdrawal of conventional sedation, immediate implementation of alpha-2 agonist infusion and the use of “rescue sedation” (midazolam bolus[es]) or “breakthrough sedation” (haloperidol bolus[es]) to stabilize cooperative sedation. b) Switching from conventional to cooperative sedation in unstable patients (e.g., refractory delirium tremens, septic shock, acute respiratory distress syndrome, etc.): to avoid hypotension and bradycardia evoked by sympathetic deactivation, the short answer is to maintain the stroke volume through volume loading, vasopressors and inotropes. c) To avoid these switches and associated difficulties, alpha-2 agonists may be considered first-line sedatives. The short answer is to administer alpha-2 agonists slowly from admission or endotracheal intubation up to stabilized cooperative sedation. The “take home” message is as follows: a) alpha-2 agonists are jointly sympathetic deactivators and sedative agents; b) sympathetic deactivation implies maintaining the stroke volume and iterative assessment of volemia. Evidence-based medicine should document our propositions.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(4):600-615
DOI 10.5935/0103-507X.20210087
Cardiac, ventilatory and kidney management in the critical care setting has been optimized over the past decades. Cognition and sedation represent one of the last remaning challenges. As conventional sedation is suboptimal and as the sedation evoked by alpha-2 adrenergic agonists (“cooperative” sedation with dexmedetomidine, clonidine or guanfacine) represents a valuable alternative, this manuscript covers three practical topics for which evidence-based medicine is lacking: a) Switching from conventional to cooperative sedation (“switching”): the short answer is the abrupt withdrawal of conventional sedation, immediate implementation of alpha-2 agonist infusion and the use of “rescue sedation” (midazolam bolus[es]) or “breakthrough sedation” (haloperidol bolus[es]) to stabilize cooperative sedation. b) Switching from conventional to cooperative sedation in unstable patients (e.g., refractory delirium tremens, septic shock, acute respiratory distress syndrome, etc.): to avoid hypotension and bradycardia evoked by sympathetic deactivation, the short answer is to maintain the stroke volume through volume loading, vasopressors and inotropes. c) To avoid these switches and associated difficulties, alpha-2 agonists may be considered first-line sedatives. The short answer is to administer alpha-2 agonists slowly from admission or endotracheal intubation up to stabilized cooperative sedation. The “take home” message is as follows: a) alpha-2 agonists are jointly sympathetic deactivators and sedative agents; b) sympathetic deactivation implies maintaining the stroke volume and iterative assessment of volemia. Evidence-based medicine should document our propositions.