-
Special Article
Use of bedside echocardiography in the care of critically ill patients – a joint consensus document of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Medicina de Emergência, and Sociedade Brasileira de Medicina Hospitalar. Part 1 – Competence in bedside echocardiography
- José Augusto Santos Pellegrini
 ,
, - Ciro Leite Mendes ,
- Paulo César Gottardo ,
- Khalil Feitosa,
- Josiane França John , [ … ],
- Ricardo Luiz Cordioli
Abstract
Special ArticleUse of bedside echocardiography in the care of critically ill patients – a joint consensus document of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Medicina de Emergência, and Sociedade Brasileira de Medicina Hospitalar. Part 1 – Competence in bedside echocardiography
Crit Care Sci. 2023;35(1):2-10
DOI 10.5935/2965-2774.20230307-pt
- José Augusto Santos Pellegrini ,
- Ciro Leite Mendes ,
- Paulo César Gottardo ,
- Khalil Feitosa,
- Josiane França John ,
- Ana Cláudia Tonelli de Oliveira ,
- Alexandre Jorge de Andrade Negri,
- Ana Burigo Grumann ,
- Dalton de Souza Barros,
- Fátima Elizabeth Fonseca de Oliveira Negri,
- Gérson Luiz de Macedo ,
- Júlio Leal Bandeira Neves,
- Márcio da Silveira Rodrigues,
- Marcio Fernando Spagnól ,
- Marcus Antonio Ferez,
- Ricardo Ávila Chalhub ,
- Ricardo Luiz Cordioli
Views42See moreABSTRACT
The use of echocardiography by physicians who are not echocardiographers has become common throughout the world across highly diverse settings where the care of acutely ill patients is provided. Echocardiographic evaluation performed in a point-of-care manner can provide relevant information regarding the mechanism of causes of shock, for example, increasing the rates of correct diagnosis and allowing for faster informed decision-making than through evaluation methods. Considering that the accurate diagnosis of life-threatening situations is essential for professionals working with acutely ill patients, several international associations recommend that physicians responsible for critically ill patients acquire and develop the ability to perform bedside ultrasound examinations, including echocardiographic examinations. However, there is no consensus in the literature regarding which specific applications should be included in the list of skills for nonechocardiographer physicians. Taking into account the multiplicity of applications of echocardiography in different scenarios related to acutely ill patients; the differences in the published protocols, with regard to both the teaching methodology and competence verification; and the heterogeneity of training among highly diverse specialties responsible for their care at different levels, this consensus document aimed to reflect the position of representatives of related Brazilian medical societies on the subject and may thus serve as a starting point both for standardization among different specialties and for the transmission of knowledge and verification of the corresponding competencies.
Views42

Abstract
Special ArticleUse of bedside echocardiography in the care of critically ill patients – a joint consensus document of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Medicina de Emergência, and Sociedade Brasileira de Medicina Hospitalar. Part 1 – Competence in bedside echocardiography
Crit Care Sci. 2023;35(1):2-10
DOI 10.5935/2965-2774.20230307-pt
- José Augusto Santos Pellegrini ,
- Ciro Leite Mendes ,
- Paulo César Gottardo ,
- Khalil Feitosa,
- Josiane França John ,
- Ana Cláudia Tonelli de Oliveira ,
- Alexandre Jorge de Andrade Negri,
- Ana Burigo Grumann ,
- Dalton de Souza Barros,
- Fátima Elizabeth Fonseca de Oliveira Negri,
- Gérson Luiz de Macedo ,
- Júlio Leal Bandeira Neves,
- Márcio da Silveira Rodrigues,
- Marcio Fernando Spagnól ,
- Marcus Antonio Ferez,
- Ricardo Ávila Chalhub ,
- Ricardo Luiz Cordioli
Views42See moreABSTRACT
The use of echocardiography by physicians who are not echocardiographers has become common throughout the world across highly diverse settings where the care of acutely ill patients is provided. Echocardiographic evaluation performed in a point-of-care manner can provide relevant information regarding the mechanism of causes of shock, for example, increasing the rates of correct diagnosis and allowing for faster informed decision-making than through evaluation methods. Considering that the accurate diagnosis of life-threatening situations is essential for professionals working with acutely ill patients, several international associations recommend that physicians responsible for critically ill patients acquire and develop the ability to perform bedside ultrasound examinations, including echocardiographic examinations. However, there is no consensus in the literature regarding which specific applications should be included in the list of skills for nonechocardiographer physicians. Taking into account the multiplicity of applications of echocardiography in different scenarios related to acutely ill patients; the differences in the published protocols, with regard to both the teaching methodology and competence verification; and the heterogeneity of training among highly diverse specialties responsible for their care at different levels, this consensus document aimed to reflect the position of representatives of related Brazilian medical societies on the subject and may thus serve as a starting point both for standardization among different specialties and for the transmission of knowledge and verification of the corresponding competencies.
- José Augusto Santos Pellegrini
-
Special Article
High versus low mean arterial pressure target in liver transplant patients. An open, controlled, single-center, randomized clinical trial – Protocol and methods (LIVER-PAM)
- Rodolpho Augusto de Moura Pedro ,
- Bruna Carla Scharranch,
- Lucas de Oliveira Araújo ,
- Luciana Severo Brandão,
- Lúcia da Conceição Andrade, [ … ],
- Luíz Marcelo Sá Malbouisson
Abstract
Special ArticleHigh versus low mean arterial pressure target in liver transplant patients. An open, controlled, single-center, randomized clinical trial – Protocol and methods (LIVER-PAM)
Crit Care Sci. 2023;35(1):11-18
DOI 10.5935/2965-2774.20230336-pt
- Rodolpho Augusto de Moura Pedro ,
- Bruna Carla Scharranch,
- Lucas de Oliveira Araújo ,
- Luciana Severo Brandão,
- Lúcia da Conceição Andrade,
- Wellington Andraus ,
- Luís Augusto Carneiro D’Albuquerque ,
- Luíz Marcelo Sá Malbouisson
Views13ABSTRACT
Objective:
To explain the rationale and protocol of the methods and analyses to be used in the LIVER-PAM randomized clinical trial, which seeks to understand whether a higher mean arterial pressure is capable of reducing the incidence of renal dysfunction postoperatively after liver transplantation.
Methods:
LIVER-PAM is an open-label, randomized, controlled, singlecenter clinical trial. Patients randomized to the intervention group will have a mean arterial pressure of 85 – 90mmHg in the initial 24 hours of postoperative management, while patients in the control group will have a mean arterial pressure of 65 – 70mmHg in the same period. A sample of 174 patients will be required to demonstrate a 20% reduction in the absolute incidence of renal dysfunction, with a power of 80% and an alpha of 0.05.
Conclusion:
If a 20% reduction in the absolute incidence of renal dysfunction in the postoperative period of liver transplantation is achieved with higher target mean arterial pressure in the first 24 hours, this would represent an inexpensive and simple therapy for improving current outcomes in the management of liver transplant patients.
Keywords:Arterial pressureHemodynamicsLiver transplantationPerioperative carePostoperative periodRenal insufficiencySee moreViews13Abstract
Special ArticleHigh versus low mean arterial pressure target in liver transplant patients. An open, controlled, single-center, randomized clinical trial – Protocol and methods (LIVER-PAM)
Crit Care Sci. 2023;35(1):11-18
DOI 10.5935/2965-2774.20230336-pt
- Rodolpho Augusto de Moura Pedro ,
- Bruna Carla Scharranch,
- Lucas de Oliveira Araújo ,
- Luciana Severo Brandão,
- Lúcia da Conceição Andrade,
- Wellington Andraus ,
- Luís Augusto Carneiro D’Albuquerque ,
- Luíz Marcelo Sá Malbouisson
Views13ABSTRACT
Objective:
To explain the rationale and protocol of the methods and analyses to be used in the LIVER-PAM randomized clinical trial, which seeks to understand whether a higher mean arterial pressure is capable of reducing the incidence of renal dysfunction postoperatively after liver transplantation.
Methods:
LIVER-PAM is an open-label, randomized, controlled, singlecenter clinical trial. Patients randomized to the intervention group will have a mean arterial pressure of 85 – 90mmHg in the initial 24 hours of postoperative management, while patients in the control group will have a mean arterial pressure of 65 – 70mmHg in the same period. A sample of 174 patients will be required to demonstrate a 20% reduction in the absolute incidence of renal dysfunction, with a power of 80% and an alpha of 0.05.
Conclusion:
If a 20% reduction in the absolute incidence of renal dysfunction in the postoperative period of liver transplantation is achieved with higher target mean arterial pressure in the first 24 hours, this would represent an inexpensive and simple therapy for improving current outcomes in the management of liver transplant patients.
Keywords:Arterial pressureHemodynamicsLiver transplantationPerioperative carePostoperative periodRenal insufficiencySee more - Rodolpho Augusto de Moura Pedro
-
Original Article
Factors associated with mortality in mechanically ventilated patients with severe acute respiratory syndrome due to COVID-19 evolution
- João Paulo Arruda de Oliveira ,
- Andreia Cristina Travassos Costa ,
- Agnaldo José Lopes ,
- Arthur de Sá Ferreira ,
- Luis Felipe da Fonseca Reis
Abstract
Original ArticleFactors associated with mortality in mechanically ventilated patients with severe acute respiratory syndrome due to COVID-19 evolution
Crit Care Sci. 2023;35(1):19-30
DOI 10.5935/2965-2774.20230203-pt
- João Paulo Arruda de Oliveira ,
- Andreia Cristina Travassos Costa ,
- Agnaldo José Lopes ,
- Arthur de Sá Ferreira ,
- Luis Felipe da Fonseca Reis
Views16ABSTRACT
Objectives:
To evaluate the factors associated with mortality in mechanically ventilated patients with acute respiratory distress syndrome due to COVID-19.
Methods:
This was a retrospective, multicenter cohort study that included 425 mechanically ventilated adult patients with COVID-19 admitted to 4 intensive care units. Clinical data comprising the SOFA score, laboratory data and mechanical characteristics of the respiratory system were collected in a standardized way immediately after the start of invasive mechanical ventilation. The risk factors for death were analyzed using Cox regression to estimate the risk ratios and their respective 95%CIs.
Results:
Body mass index (RR 1.17; 95%CI 1.11 – 1.20; p < 0.001), SOFA score (RR 1.39; 95%CI 1.31 - 1.49; p < 0.001) and driving pressure (RR 1.24; 95%CI 1.21 - 1.29; p < 0.001) were considered independent factors associated with mortality in mechanically ventilated patients with acute respiratory distress syndrome due to COVID-19. Respiratory system compliance (RR 0.92; 95%CI 0.90 - 0.93; p < 0.001) was associated with lower mortality. The comparative analysis of the survival curves indicated that patients with respiratory system compliance (< 30mL/cmH2O), a higher SOFA score (> 5 points) and higher driving pressure (> 14cmH2O) were more significantly associated with the outcome of death at 28 days and 60 days.
Conclusion:
Patients with a body mass index > 32kg/m2, respiratory system compliance < 30mL/cmH2O, driving pressure > 14cmH2O and SOFA score > 5.8 immediately after the initiation of invasive ventilatory support had worse outcomes, and independent risk factors were associated with higher mortality in this population.
Keywords:artificialCoronavirus infectionsCOVID-19MortalityRespirationRespiratory distress syndromeRespiratory mechanicsSARS-CoV-2See moreViews16Abstract
Original ArticleFactors associated with mortality in mechanically ventilated patients with severe acute respiratory syndrome due to COVID-19 evolution
Crit Care Sci. 2023;35(1):19-30
DOI 10.5935/2965-2774.20230203-pt
- João Paulo Arruda de Oliveira ,
- Andreia Cristina Travassos Costa ,
- Agnaldo José Lopes ,
- Arthur de Sá Ferreira ,
- Luis Felipe da Fonseca Reis
Views16ABSTRACT
Objectives:
To evaluate the factors associated with mortality in mechanically ventilated patients with acute respiratory distress syndrome due to COVID-19.
Methods:
This was a retrospective, multicenter cohort study that included 425 mechanically ventilated adult patients with COVID-19 admitted to 4 intensive care units. Clinical data comprising the SOFA score, laboratory data and mechanical characteristics of the respiratory system were collected in a standardized way immediately after the start of invasive mechanical ventilation. The risk factors for death were analyzed using Cox regression to estimate the risk ratios and their respective 95%CIs.
Results:
Body mass index (RR 1.17; 95%CI 1.11 – 1.20; p < 0.001), SOFA score (RR 1.39; 95%CI 1.31 - 1.49; p < 0.001) and driving pressure (RR 1.24; 95%CI 1.21 - 1.29; p < 0.001) were considered independent factors associated with mortality in mechanically ventilated patients with acute respiratory distress syndrome due to COVID-19. Respiratory system compliance (RR 0.92; 95%CI 0.90 - 0.93; p < 0.001) was associated with lower mortality. The comparative analysis of the survival curves indicated that patients with respiratory system compliance (< 30mL/cmH2O), a higher SOFA score (> 5 points) and higher driving pressure (> 14cmH2O) were more significantly associated with the outcome of death at 28 days and 60 days.
Conclusion:
Patients with a body mass index > 32kg/m2, respiratory system compliance < 30mL/cmH2O, driving pressure > 14cmH2O and SOFA score > 5.8 immediately after the initiation of invasive ventilatory support had worse outcomes, and independent risk factors were associated with higher mortality in this population.
Keywords:artificialCoronavirus infectionsCOVID-19MortalityRespirationRespiratory distress syndromeRespiratory mechanicsSARS-CoV-2See more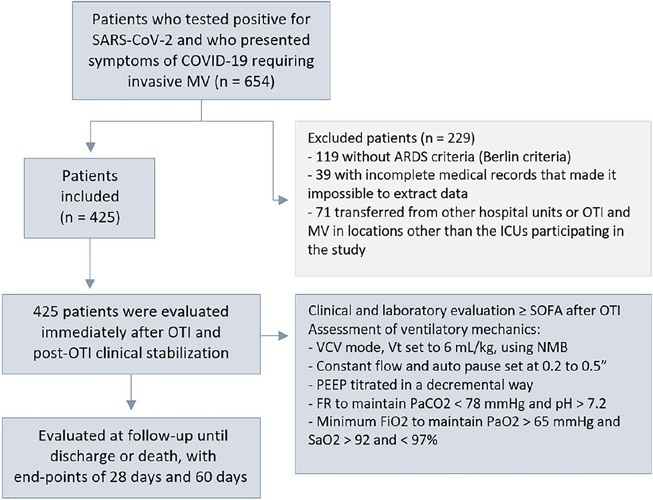
- João Paulo Arruda de Oliveira
-
Original Article
Does an educational website improve psychological outcomes and satisfaction among family members of intensive care unit patients?
- Tarissa da Silva Ribeiro Haack ,
- Regis Goulart Rosa ,
- Cassiano Teixeira ,
- Daniel Sganzerla ,
- Caroline Cabral Robinson, [ … ],
- Cleidilene Ramos Magalhães
Abstract
Original ArticleDoes an educational website improve psychological outcomes and satisfaction among family members of intensive care unit patients?
Crit Care Sci. 2023;35(1):31-36
DOI 10.5935/2965-2774.20230113-pt
- Tarissa da Silva Ribeiro Haack ,
- Regis Goulart Rosa ,
- Cassiano Teixeira ,
- Daniel Sganzerla ,
- Caroline Cabral Robinson,
- Cláudia Severgnini Eugênio ,
- Cleidilene Ramos Magalhães
Views10ABSTRACT
Objective:
To evaluate the impact of an educational website on satisfaction and symptoms of anxiety and depression among family members of critically ill adult patients.
Methods:
We embedded an analysis of website access in a cohort study conducted in intensive care units with flexible visiting hours in Brazil. Family members were guided to access an educational website designed to help them understand the processes and emotions associated with an intensive care unit stay. Subjects were evaluated for baseline data within the first 48 hours following enrollment and outcome assessment at up to 7 days after patient discharge from the intensive care unit, death, or until the 30th day of the study. The main outcomes were satisfaction using the Critical Care Family Needs Inventory and the presence of anxiety and depression symptoms using the Hospital Anxiety and Depression Scale.
Results:
A total of 532 family members were evaluated during the study period. Of these, 61 (11.5%) accessed the website. After adjustments, family members who accessed the website had significantly better mean Critical Care Family Needs Inventory scores (152.8 versus 145.2, p = 0.01) and a lower prevalence of probable clinical anxiety (prevalence ratio 0.35; 95%CI 0.14 – 0.89) than family members who did not access the website. There were no differences regarding symptoms of depression.
Conclusion:
Access to an educational website was associated with higher family satisfaction with care and a lower prevalence of clinical anxiety.
Keywords:AnxietyDepressionFamilyHealth information systemsIntensive care unitsInternetOutcome assessment, health carePersonal satisfactionSee moreViews10Abstract
Original ArticleDoes an educational website improve psychological outcomes and satisfaction among family members of intensive care unit patients?
Crit Care Sci. 2023;35(1):31-36
DOI 10.5935/2965-2774.20230113-pt
- Tarissa da Silva Ribeiro Haack ,
- Regis Goulart Rosa ,
- Cassiano Teixeira ,
- Daniel Sganzerla ,
- Caroline Cabral Robinson,
- Cláudia Severgnini Eugênio ,
- Cleidilene Ramos Magalhães
Views10ABSTRACT
Objective:
To evaluate the impact of an educational website on satisfaction and symptoms of anxiety and depression among family members of critically ill adult patients.
Methods:
We embedded an analysis of website access in a cohort study conducted in intensive care units with flexible visiting hours in Brazil. Family members were guided to access an educational website designed to help them understand the processes and emotions associated with an intensive care unit stay. Subjects were evaluated for baseline data within the first 48 hours following enrollment and outcome assessment at up to 7 days after patient discharge from the intensive care unit, death, or until the 30th day of the study. The main outcomes were satisfaction using the Critical Care Family Needs Inventory and the presence of anxiety and depression symptoms using the Hospital Anxiety and Depression Scale.
Results:
A total of 532 family members were evaluated during the study period. Of these, 61 (11.5%) accessed the website. After adjustments, family members who accessed the website had significantly better mean Critical Care Family Needs Inventory scores (152.8 versus 145.2, p = 0.01) and a lower prevalence of probable clinical anxiety (prevalence ratio 0.35; 95%CI 0.14 – 0.89) than family members who did not access the website. There were no differences regarding symptoms of depression.
Conclusion:
Access to an educational website was associated with higher family satisfaction with care and a lower prevalence of clinical anxiety.
Keywords:AnxietyDepressionFamilyHealth information systemsIntensive care unitsInternetOutcome assessment, health carePersonal satisfactionSee more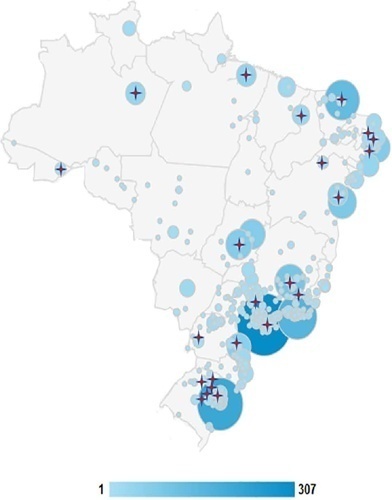
- Tarissa da Silva Ribeiro Haack
-
Original Article
Maximal expiratory pressure compared with maximal expiratory pressure during induced cough as a predictor of extubation failure
- Melina Carrera ,
- Jose García Urrutia ,
- Cesar Bueno Ardariz ,
- Maria Luz Porra ,
- Claudio Gamarra , [ … ],
- Ladislao Pablo Diaz Ballve
Abstract
Original ArticleMaximal expiratory pressure compared with maximal expiratory pressure during induced cough as a predictor of extubation failure
Crit Care Sci. 2023;35(1):37-43
DOI 10.5935/2965-2774.20230275-pt
- Melina Carrera ,
- Jose García Urrutia ,
- Cesar Bueno Ardariz ,
- Maria Luz Porra ,
- Claudio Gamarra ,
- Ladislao Pablo Diaz Ballve
Views5See moreABSTRACT
Objective:
To compare the diagnostic performance of maximal expiratory pressure with maximal expiratory pressure during induced cough for predicting extubation failure within 72 hours in patients who completed a spontaneous breathing trial (SBT).
Methods:
The study was conducted between October 2018 and September 2019. All patients aged over 18 years admitted to the intensive care unit who required invasive mechanical ventilation for over 48 hours and successfully completed a spontaneous breathing trial were included. The maximal expiratory pressure was assessed with a unidirectional valve for 40 seconds, and verbal encouragement was given. The maximal expiratory pressure during induced cough was measured with slow instillation of 2mL of a 0.9% saline solution. The primary outcome variable was extubation failure.
Results:
Eighty patients were included, of which 43 (54%) were male. Twenty-two patients [27.5% (95%CI 18.9 – 38.1)] failed extubation within 72 hours. Differences were observed in the maximal expiratory pressure during induced cough between the group who failed extubation, with a median of 0cmH2O (P25-75: 0 – 90), and the group without extubation failure, with a median of 120cmH2O (P25-75: 73 – 120); p < 0.001.
Conclusion:
In patients who completed a spontaneous breathing trial, the maximal expiratory pressure during induced cough had a higher diagnostic performance for predicting extubation failure within 72 hours.
Views5Abstract
Original ArticleMaximal expiratory pressure compared with maximal expiratory pressure during induced cough as a predictor of extubation failure
Crit Care Sci. 2023;35(1):37-43
DOI 10.5935/2965-2774.20230275-pt
- Melina Carrera ,
- Jose García Urrutia ,
- Cesar Bueno Ardariz ,
- Maria Luz Porra ,
- Claudio Gamarra ,
- Ladislao Pablo Diaz Ballve
Views5See moreABSTRACT
Objective:
To compare the diagnostic performance of maximal expiratory pressure with maximal expiratory pressure during induced cough for predicting extubation failure within 72 hours in patients who completed a spontaneous breathing trial (SBT).
Methods:
The study was conducted between October 2018 and September 2019. All patients aged over 18 years admitted to the intensive care unit who required invasive mechanical ventilation for over 48 hours and successfully completed a spontaneous breathing trial were included. The maximal expiratory pressure was assessed with a unidirectional valve for 40 seconds, and verbal encouragement was given. The maximal expiratory pressure during induced cough was measured with slow instillation of 2mL of a 0.9% saline solution. The primary outcome variable was extubation failure.
Results:
Eighty patients were included, of which 43 (54%) were male. Twenty-two patients [27.5% (95%CI 18.9 – 38.1)] failed extubation within 72 hours. Differences were observed in the maximal expiratory pressure during induced cough between the group who failed extubation, with a median of 0cmH2O (P25-75: 0 – 90), and the group without extubation failure, with a median of 120cmH2O (P25-75: 73 – 120); p < 0.001.
Conclusion:
In patients who completed a spontaneous breathing trial, the maximal expiratory pressure during induced cough had a higher diagnostic performance for predicting extubation failure within 72 hours.

- Melina Carrera
-
Original Article
Protocol-directed weaning versus conventional weaning from mechanical ventilation for neurocritical patients in an intensive care unit: a nonrandomized quasi-experimental study
- Alberto Belenguer-Muncharaz ,
- Carmen Díaz-Tormo ,
- Estefania Granero-Gasamans ,
- Maria-Lidón Mateu-Campos
Abstract
Original ArticleProtocol-directed weaning versus conventional weaning from mechanical ventilation for neurocritical patients in an intensive care unit: a nonrandomized quasi-experimental study
Crit Care Sci. 2023;35(1):44-56
DOI 10.5935/2965-2774.20230340-pt
- Alberto Belenguer-Muncharaz ,
- Carmen Díaz-Tormo ,
- Estefania Granero-Gasamans ,
- Maria-Lidón Mateu-Campos
Views8ABSTRACT
Objective:
To investigate whether protocol-directed weaning in neurocritical patients would reduce the rate of extubation failure (as a primary outcome) and the associated complications (as a secondary outcome) compared with conventional weaning.
Methods:
A quasi-experimental study was conducted in a medical-surgical intensive care unit from January 2016 to December 2018. Patients aged 18 years or older with an acute neurological disease who were on mechanical ventilation > 24 hours were included. All patients included in the study were ready to wean, with no or minimal sedation, Glasgow coma score ≥ 9, spontaneous ventilatory stimulus, noradrenaline ≤ 0.2μgr/kg/ minute, fraction of inspired oxygen ≤ 0.5, positive end-expiratory pressure ≤ 5cmH2O, maximal inspiratory pressure < -20cmH2O, and occlusion pressure < 6cmH2O.
Results:
Ninety-four of 314 patients admitted to the intensive care unit were included (50 in the Intervention Group and 44 in the Control Group). There was no significant difference in spontaneous breathing trial failure (18% in the Intervention Group versus 34% in the Control Group, p = 0.12). More patients in the Intervention Group were extubated than in the Control Group (100% versus 79%, p = 0.01). The rate of extubation failure was not signifiantly diffrent between the groups (18% in the Intervention Group versus 17% in the Control Group; relative risk 1.02; 95%CI 0.64 – 1.61; p = 1.00). The reintubation rate was lower in the Control Group (16% in the Intervention Group versus 11% in the Control Group; relative risk 1.15; 95%CI 0.74 – 1.82; p = 0.75). The need for tracheotomy was lower in the Intervention Group [4 (8%) versus 11 (25%) in the Control Group; relative risk 0.32; 95%CI 0.11 – 0.93; p = 0.04]. At Day 28, the patients in the Intervention Group had more ventilator-free days than those in the Control Group [28 (26 – 28) days versus 26 (19 – 28) days; p = 0.01]. The total duration of mechanical ventilation was shorter in the Intervention Group than in the Control Group [5 (2 – 13) days versus 9 (3 – 22) days; p = 0.01]. There were no diffrences in the length of intensive care unit stay, 28-day free from mechanical ventilation, hospital stay or 90-day mortality.
Conclusion:
Considering the limitations of our study, the application of a weaning protocol for neurocritical patients led to a high percentage of extubation, a reduced need for tracheotomy and a shortened duration of mechanical ventilation. However, there was no reduction in extubation failure or the 28-day free of from mechanical ventilation compared with the Control Group.
Keywords:Airway extubation, WeaningCritical illnessRespiration, artificialTracheotomyVentilator weaningSee moreViews8Abstract
Original ArticleProtocol-directed weaning versus conventional weaning from mechanical ventilation for neurocritical patients in an intensive care unit: a nonrandomized quasi-experimental study
Crit Care Sci. 2023;35(1):44-56
DOI 10.5935/2965-2774.20230340-pt
- Alberto Belenguer-Muncharaz ,
- Carmen Díaz-Tormo ,
- Estefania Granero-Gasamans ,
- Maria-Lidón Mateu-Campos
Views8ABSTRACT
Objective:
To investigate whether protocol-directed weaning in neurocritical patients would reduce the rate of extubation failure (as a primary outcome) and the associated complications (as a secondary outcome) compared with conventional weaning.
Methods:
A quasi-experimental study was conducted in a medical-surgical intensive care unit from January 2016 to December 2018. Patients aged 18 years or older with an acute neurological disease who were on mechanical ventilation > 24 hours were included. All patients included in the study were ready to wean, with no or minimal sedation, Glasgow coma score ≥ 9, spontaneous ventilatory stimulus, noradrenaline ≤ 0.2μgr/kg/ minute, fraction of inspired oxygen ≤ 0.5, positive end-expiratory pressure ≤ 5cmH2O, maximal inspiratory pressure < -20cmH2O, and occlusion pressure < 6cmH2O.
Results:
Ninety-four of 314 patients admitted to the intensive care unit were included (50 in the Intervention Group and 44 in the Control Group). There was no significant difference in spontaneous breathing trial failure (18% in the Intervention Group versus 34% in the Control Group, p = 0.12). More patients in the Intervention Group were extubated than in the Control Group (100% versus 79%, p = 0.01). The rate of extubation failure was not signifiantly diffrent between the groups (18% in the Intervention Group versus 17% in the Control Group; relative risk 1.02; 95%CI 0.64 – 1.61; p = 1.00). The reintubation rate was lower in the Control Group (16% in the Intervention Group versus 11% in the Control Group; relative risk 1.15; 95%CI 0.74 – 1.82; p = 0.75). The need for tracheotomy was lower in the Intervention Group [4 (8%) versus 11 (25%) in the Control Group; relative risk 0.32; 95%CI 0.11 – 0.93; p = 0.04]. At Day 28, the patients in the Intervention Group had more ventilator-free days than those in the Control Group [28 (26 – 28) days versus 26 (19 – 28) days; p = 0.01]. The total duration of mechanical ventilation was shorter in the Intervention Group than in the Control Group [5 (2 – 13) days versus 9 (3 – 22) days; p = 0.01]. There were no diffrences in the length of intensive care unit stay, 28-day free from mechanical ventilation, hospital stay or 90-day mortality.
Conclusion:
Considering the limitations of our study, the application of a weaning protocol for neurocritical patients led to a high percentage of extubation, a reduced need for tracheotomy and a shortened duration of mechanical ventilation. However, there was no reduction in extubation failure or the 28-day free of from mechanical ventilation compared with the Control Group.
Keywords:Airway extubation, WeaningCritical illnessRespiration, artificialTracheotomyVentilator weaningSee more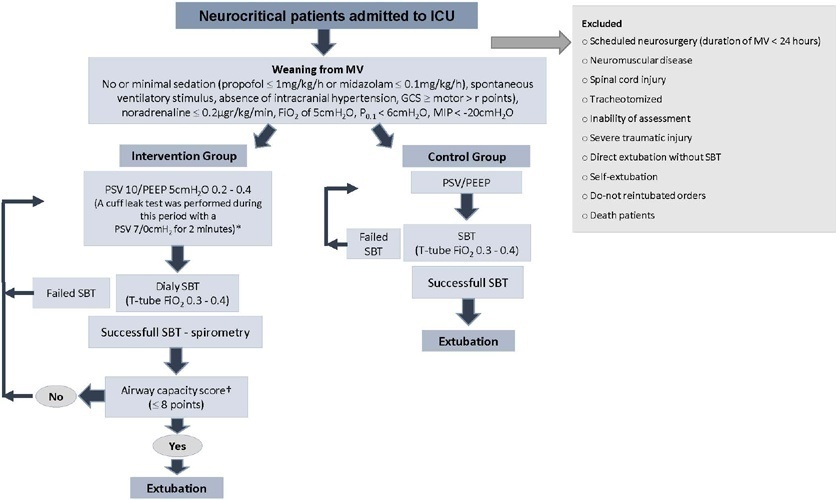
- Alberto Belenguer-Muncharaz
-
Original Article
Knowledge regarding extracorporeal membrane oxygenation management among Brazilian pediatric intensivists: a cross-sectional survey
- José Colleti Júnior ,
- Arnaldo Prata-Barbosa ,
- Orlei Ribeiro Araujo ,
- Cristian Tedesco Tonial ,
- Felipe Rezende Caino de Oliveira , [ … ],
- Daniel Garros
Abstract
Original ArticleKnowledge regarding extracorporeal membrane oxygenation management among Brazilian pediatric intensivists: a cross-sectional survey
Crit Care Sci. 2023;35(1):57-65
DOI 10.5935/2965-2774.20230350-pt
- José Colleti Júnior ,
- Arnaldo Prata-Barbosa ,
- Orlei Ribeiro Araujo ,
- Cristian Tedesco Tonial ,
- Felipe Rezende Caino de Oliveira ,
- Daniela Carla de Souza ,
- Fernanda Lima-Setta ,
- Thiago Silveira Jannuzzi de Oliveira ,
- Mary Lucy Ferraz Maia Fiuza de Mello ,
- Carolina Amoretti ,
- Paulo Ramos David João ,
- Cinara Carneiro Neves ,
- Norma Suely Oliveira ,
- Cira Ferreira Antunes Costa ,
- Daniel Garros
Views4ABSTRACT
Objective:
To assess Brazilian pediatric intensivists’ general knowledge of extracorporeal membrane oxygenation, including evidence for its use, the national funding model, indications, and complications.
Methods:
This was a multicenter cross-sectional survey including 45 Brazilian pediatric intensive care units. A convenience sample of 654 intensivists was surveyed regarding their knowledge on managing patients on extracorporeal membrane oxygenation, its indications, complications, funding, and literature evidence.
Results:
The survey addressed questions regarding the knowledge and experience of pediatric intensivists with extracorporeal membrane oxygenation, including two clinical cases and 6 optional questions about the management of patients on extracorporeal membrane oxygenation. Of the 45 invited centers, 42 (91%) participated in the study, and 412 of 654 (63%) pediatric intensivists responded to the survey. Most pediatric intensive care units were from the Southeast region of Brazil (59.5%), and private/for-profit hospitals represented 28.6% of the participating centers. The average age of respondents was 41.4 (standard deviation 9.1) years, and the majority (77%) were women. Only 12.4% of respondents had taken an extracorporeal membrane oxygenation course. Only 19% of surveyed hospitals have an extracorporeal membrane oxygenation program, and only 27% of intensivists reported having already managed patients on extracorporeal membrane oxygenation. Specific extracorporeal membrane oxygenation management questions were responded to by only 64 physicians (15.5%), who had a fair/good correct response rate (median 63.4%; range 32.8% to 91.9%).
Conclusion:
Most Brazilian pediatric intensivists demonstrated limited knowledge regarding extracorporeal membrane oxygenation, including its indications and complications. Extracorporeal membrane oxygenation is not yet widely available in Brazil, with few intensivists prepared to manage patients on extracorporeal membrane oxygenation and even fewer intensivists recognizing when to refer patients to extracorporeal membrane oxygenation centers.
Keywords:ChildExtracorporeal membrane oxygenationHealth knowledge, attitudes, practicePediatric intensive care unitsSurvey and questionnairesSee moreViews4Abstract
Original ArticleKnowledge regarding extracorporeal membrane oxygenation management among Brazilian pediatric intensivists: a cross-sectional survey
Crit Care Sci. 2023;35(1):57-65
DOI 10.5935/2965-2774.20230350-pt
- José Colleti Júnior ,
- Arnaldo Prata-Barbosa ,
- Orlei Ribeiro Araujo ,
- Cristian Tedesco Tonial ,
- Felipe Rezende Caino de Oliveira ,
- Daniela Carla de Souza ,
- Fernanda Lima-Setta ,
- Thiago Silveira Jannuzzi de Oliveira ,
- Mary Lucy Ferraz Maia Fiuza de Mello ,
- Carolina Amoretti ,
- Paulo Ramos David João ,
- Cinara Carneiro Neves ,
- Norma Suely Oliveira ,
- Cira Ferreira Antunes Costa ,
- Daniel Garros
Views4ABSTRACT
Objective:
To assess Brazilian pediatric intensivists’ general knowledge of extracorporeal membrane oxygenation, including evidence for its use, the national funding model, indications, and complications.
Methods:
This was a multicenter cross-sectional survey including 45 Brazilian pediatric intensive care units. A convenience sample of 654 intensivists was surveyed regarding their knowledge on managing patients on extracorporeal membrane oxygenation, its indications, complications, funding, and literature evidence.
Results:
The survey addressed questions regarding the knowledge and experience of pediatric intensivists with extracorporeal membrane oxygenation, including two clinical cases and 6 optional questions about the management of patients on extracorporeal membrane oxygenation. Of the 45 invited centers, 42 (91%) participated in the study, and 412 of 654 (63%) pediatric intensivists responded to the survey. Most pediatric intensive care units were from the Southeast region of Brazil (59.5%), and private/for-profit hospitals represented 28.6% of the participating centers. The average age of respondents was 41.4 (standard deviation 9.1) years, and the majority (77%) were women. Only 12.4% of respondents had taken an extracorporeal membrane oxygenation course. Only 19% of surveyed hospitals have an extracorporeal membrane oxygenation program, and only 27% of intensivists reported having already managed patients on extracorporeal membrane oxygenation. Specific extracorporeal membrane oxygenation management questions were responded to by only 64 physicians (15.5%), who had a fair/good correct response rate (median 63.4%; range 32.8% to 91.9%).
Conclusion:
Most Brazilian pediatric intensivists demonstrated limited knowledge regarding extracorporeal membrane oxygenation, including its indications and complications. Extracorporeal membrane oxygenation is not yet widely available in Brazil, with few intensivists prepared to manage patients on extracorporeal membrane oxygenation and even fewer intensivists recognizing when to refer patients to extracorporeal membrane oxygenation centers.
Keywords:ChildExtracorporeal membrane oxygenationHealth knowledge, attitudes, practicePediatric intensive care unitsSurvey and questionnairesSee more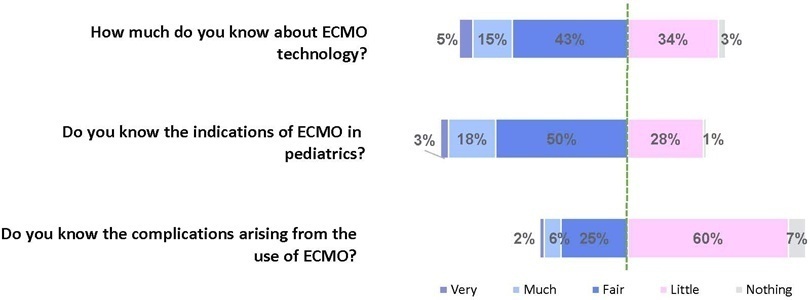
- José Colleti Júnior
-
Original Article
Fitness checklist model for spontaneous breathing tests in pediatrics
- Bruno Silva Miranda ,
- Valéria Cabral Neves ,
- Yessa do Prado Albuquerque ,
- Emilly Freitas de Souza ,
- Adriana Koliski , [ … ],
- José Eduardo Carreiro
Abstract
Original ArticleFitness checklist model for spontaneous breathing tests in pediatrics
Crit Care Sci. 2023;35(1):66-72
DOI 10.5935/2965-2774.20230312-pt
- Bruno Silva Miranda ,
- Valéria Cabral Neves ,
- Yessa do Prado Albuquerque ,
- Emilly Freitas de Souza ,
- Adriana Koliski ,
- Mônica Nunes Lima Cat ,
- José Eduardo Carreiro
Views4ABSTRACT
Objective:
To evaluate whether a model of a daily fitness checklist for spontaneous breathing tests is able to identify predictive variables of extubation failure in pediatric patients admitted to a Brazilian intensive care unit.
Methods:
This was a single-center, cross-sectional study with prospective data collection. The checklist model comprised 20 items and was applied to assess the ability to perform spontaneous breathing tests.
Results:
The sample consisted of 126 pediatric patients (85 males (67.5%)) on invasive mechanical ventilation, for whom 1,217 daily assessments were applied at the bedside. The weighted total score of the prediction model showed the highest discriminatory power for the spontaneous breathing test, with sensitivity and specificity indices for fitness failure of 89.7% or success of 84.6%. The cutoff point suggested by the checklist was 8, with a probability of extubation failure less than 5%. Failure increased progressively with increasing score, with a maximum probability of predicting extubation failure of 85%.
Conclusion:
The extubation failure rate with the use of this model was within what is acceptable in the literature. The daily checklist model for the spontaneous breathing test was able to identify predictive variables of failure in the extubation process in pediatric patients.
Keywords:Airway extubationChecklistChildIntensive care units, pediatricRespiration, artificialRespiratory function testSee moreViews4Abstract
Original ArticleFitness checklist model for spontaneous breathing tests in pediatrics
Crit Care Sci. 2023;35(1):66-72
DOI 10.5935/2965-2774.20230312-pt
- Bruno Silva Miranda ,
- Valéria Cabral Neves ,
- Yessa do Prado Albuquerque ,
- Emilly Freitas de Souza ,
- Adriana Koliski ,
- Mônica Nunes Lima Cat ,
- José Eduardo Carreiro
Views4ABSTRACT
Objective:
To evaluate whether a model of a daily fitness checklist for spontaneous breathing tests is able to identify predictive variables of extubation failure in pediatric patients admitted to a Brazilian intensive care unit.
Methods:
This was a single-center, cross-sectional study with prospective data collection. The checklist model comprised 20 items and was applied to assess the ability to perform spontaneous breathing tests.
Results:
The sample consisted of 126 pediatric patients (85 males (67.5%)) on invasive mechanical ventilation, for whom 1,217 daily assessments were applied at the bedside. The weighted total score of the prediction model showed the highest discriminatory power for the spontaneous breathing test, with sensitivity and specificity indices for fitness failure of 89.7% or success of 84.6%. The cutoff point suggested by the checklist was 8, with a probability of extubation failure less than 5%. Failure increased progressively with increasing score, with a maximum probability of predicting extubation failure of 85%.
Conclusion:
The extubation failure rate with the use of this model was within what is acceptable in the literature. The daily checklist model for the spontaneous breathing test was able to identify predictive variables of failure in the extubation process in pediatric patients.
Keywords:Airway extubationChecklistChildIntensive care units, pediatricRespiration, artificialRespiratory function testSee more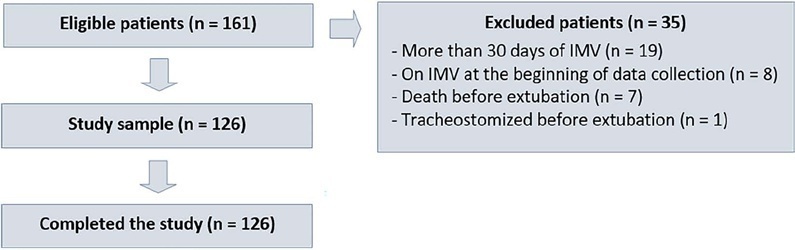
- Bruno Silva Miranda
-
Original Article
Needs of family members of patients in intensive care and their perception of medical communication
Crit Care Sci. 2023;35(1):73-83
Abstract
Original ArticleNeeds of family members of patients in intensive care and their perception of medical communication
Crit Care Sci. 2023;35(1):73-83
DOI 10.5935/2965-2774.20230374-pt
Views6ABSTRACT
Objective:
To understand the perception of medical communication and needs of family members with loved ones in intensive care.
Methods:
The study was mainly qualitative and exploratory, with thematic analysis of comments made by 92 family members with loved ones in intensive care units when answering in-person interviews comprising the Quality of Communication Questionnaire (QoC) and open-ended questions about their need for additional help, the appropriateness of the place where they received information, and additional comments.
Results:
The participants’ mean age was 46.8 years (SD = 11.8), and most of them were female, married and had incomplete or completed elementary education. The following themes were found: perception of characteristics of medical communication; feelings generated by communication; considerations about specific questions in the QoC; family members’ needs; and strategies to overcome needs regarding communication. Characteristics that facilitated communication included attention and listening. Characteristics that made communication difficult included aspects of information sharing, such as inaccessible language; lack of clarity, objectivity, sincerity, and agreement among the team; limited time; and inadequate location. Feelings such as shame, helplessness, and sadness were cited when communication was inadequate. Family members’ needs related to communication included more details about the loved one’s diagnosis, prognosis, and health condition; participation in decisionmaking; and being asked about feelings, spirituality, dying and death. Others were related to longer visitation time, psychological support, social assistance, and better infrastructure.
Conclusion:
It is necessary to enhance medical communication and improve hospital infrastructure to improve the quality of care for family members.
Keywords:CommunicationCritical illnessFamilyIntensive care unitsProfessional-family relationsSurveys and questionnairesSee moreViews6Abstract
Original ArticleNeeds of family members of patients in intensive care and their perception of medical communication
Crit Care Sci. 2023;35(1):73-83
DOI 10.5935/2965-2774.20230374-pt
Views6ABSTRACT
Objective:
To understand the perception of medical communication and needs of family members with loved ones in intensive care.
Methods:
The study was mainly qualitative and exploratory, with thematic analysis of comments made by 92 family members with loved ones in intensive care units when answering in-person interviews comprising the Quality of Communication Questionnaire (QoC) and open-ended questions about their need for additional help, the appropriateness of the place where they received information, and additional comments.
Results:
The participants’ mean age was 46.8 years (SD = 11.8), and most of them were female, married and had incomplete or completed elementary education. The following themes were found: perception of characteristics of medical communication; feelings generated by communication; considerations about specific questions in the QoC; family members’ needs; and strategies to overcome needs regarding communication. Characteristics that facilitated communication included attention and listening. Characteristics that made communication difficult included aspects of information sharing, such as inaccessible language; lack of clarity, objectivity, sincerity, and agreement among the team; limited time; and inadequate location. Feelings such as shame, helplessness, and sadness were cited when communication was inadequate. Family members’ needs related to communication included more details about the loved one’s diagnosis, prognosis, and health condition; participation in decisionmaking; and being asked about feelings, spirituality, dying and death. Others were related to longer visitation time, psychological support, social assistance, and better infrastructure.
Conclusion:
It is necessary to enhance medical communication and improve hospital infrastructure to improve the quality of care for family members.
Keywords:CommunicationCritical illnessFamilyIntensive care unitsProfessional-family relationsSurveys and questionnairesSee more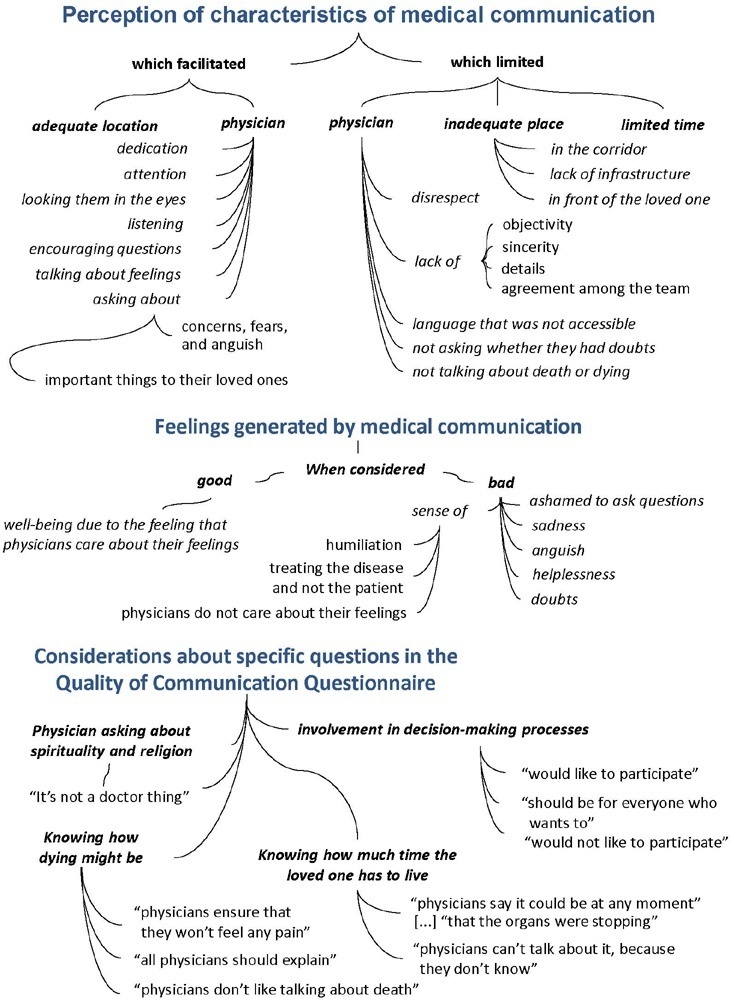
-
Review
High-value care for critically ill oncohematological patients: what do we know thus far?
- Fernanda Chohfi Atallah ,
- Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola , [ … ],
- Thiago Gomes Romano
Abstract
ReviewHigh-value care for critically ill oncohematological patients: what do we know thus far?
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
- Fernanda Chohfi Atallah ,
- Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola ,
- Jorge Ibrain Figueira Salluh ,
- Thiago Gomes Romano
Views7ABSTRACT
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Keywords:Cost of illnessCritical illnessHospital costsIntensive care unitsLow-value careNeoplasmsPatient care managementSee moreViews7Abstract
ReviewHigh-value care for critically ill oncohematological patients: what do we know thus far?
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
- Fernanda Chohfi Atallah ,
- Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola ,
- Jorge Ibrain Figueira Salluh ,
- Thiago Gomes Romano
Views7ABSTRACT
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Keywords:Cost of illnessCritical illnessHospital costsIntensive care unitsLow-value careNeoplasmsPatient care managementSee more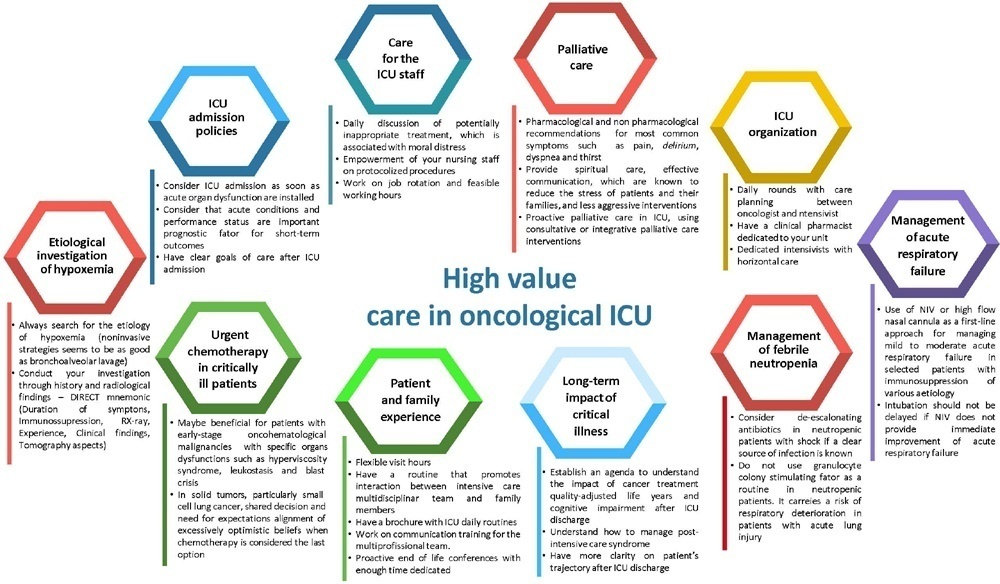
- Fernanda Chohfi Atallah
-
Letter to the Editor
Impact of the COVID-19 pandemic on predictions of death from stroke in a poor region of Brazil: a retrospective cohort study
- João Ricardo Bispo de Jesus ,
- Paulo Ricardo Martins Filho ,
- Aline Ferreira de Brito Mota ,
- Crislaine Souza Santos ,
- Joyce Menezes Santos , [ … ],
- Kelly da Silva
Abstract
Letter to the EditorImpact of the COVID-19 pandemic on predictions of death from stroke in a poor region of Brazil: a retrospective cohort study
Crit Care Sci. 2023;35(1):97-99
DOI 10.5935/2965-2774.20230357-pt
- João Ricardo Bispo de Jesus ,
- Paulo Ricardo Martins Filho ,
- Aline Ferreira de Brito Mota ,
- Crislaine Souza Santos ,
- Joyce Menezes Santos ,
- Franklim Oliveira Souza ,
- Raphaela Barroso Guedes-Granzotti ,
- Miburge Bolivar Gois Junior ,
- Kelly da Silva
Views5Stroke and cardiovascular disease are the leading causes of morbidity and mortality worldwide. However, epidemiological indicators show a decrease in the number of stroke deaths in recent decades, which can be attributed to advances in clinical interventions. The coronavirus disease 2019 (COVID-19) pandemic and the redirection of health services raised concerns about the diagnosis and […]See moreViews5Abstract
Letter to the EditorImpact of the COVID-19 pandemic on predictions of death from stroke in a poor region of Brazil: a retrospective cohort study
Crit Care Sci. 2023;35(1):97-99
DOI 10.5935/2965-2774.20230357-pt
- João Ricardo Bispo de Jesus ,
- Paulo Ricardo Martins Filho ,
- Aline Ferreira de Brito Mota ,
- Crislaine Souza Santos ,
- Joyce Menezes Santos ,
- Franklim Oliveira Souza ,
- Raphaela Barroso Guedes-Granzotti ,
- Miburge Bolivar Gois Junior ,
- Kelly da Silva
Views5Stroke and cardiovascular disease are the leading causes of morbidity and mortality worldwide. However, epidemiological indicators show a decrease in the number of stroke deaths in recent decades, which can be attributed to advances in clinical interventions. The coronavirus disease 2019 (COVID-19) pandemic and the redirection of health services raised concerns about the diagnosis and […]See more - João Ricardo Bispo de Jesus
-
Letter to the Editor
Sedation with volatile anesthetics in the intensive care unit: a new option with old agents
Crit Care Sci. 2023;35(1):100-101
Abstract
Letter to the EditorSedation with volatile anesthetics in the intensive care unit: a new option with old agents
Crit Care Sci. 2023;35(1):100-101
DOI 10.5935/2965-2774.20230394-pt
Views8INTRODUCTIONSince December 2019, when the first cases were described in China, the coronavirus disease 2019 (COVID-19) pandemic has impacted health systems around the world. A significant number of patients have the severe form of the disease, requiring admission to the intensive care unit (ICU).() The shortage of beds, equipment and drugs represented an even greater […]See moreViews8Abstract
Letter to the EditorSedation with volatile anesthetics in the intensive care unit: a new option with old agents
Crit Care Sci. 2023;35(1):100-101
DOI 10.5935/2965-2774.20230394-pt
Views8INTRODUCTIONSince December 2019, when the first cases were described in China, the coronavirus disease 2019 (COVID-19) pandemic has impacted health systems around the world. A significant number of patients have the severe form of the disease, requiring admission to the intensive care unit (ICU).() The shortage of beds, equipment and drugs represented an even greater […]See more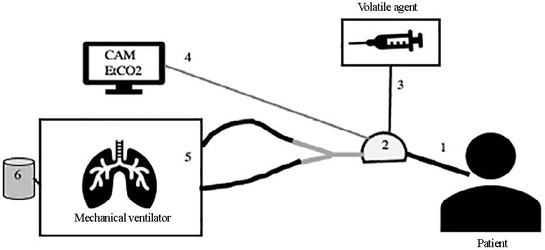
-
Letter to the Editor
Intensive care and the different meanings of vulnerability
Crit Care Sci. 2023;35(1):102-106
Abstract
Letter to the EditorIntensive care and the different meanings of vulnerability
Crit Care Sci. 2023;35(1):102-106
DOI 10.5935/2965-2774.20230317-pt
Views8INTRODUCTIONIn the eyes of laypeople, intensive care may seem like a precise and objective field of study. Even to health professionals, believing that medical practice within intensive care units (ICUs) should be predominantly guided by technical decisions seems sensible and reasonable, even though there are nuances and some space for subjectivity. However, a careful look […]See moreViews8Abstract
Letter to the EditorIntensive care and the different meanings of vulnerability
Crit Care Sci. 2023;35(1):102-106
DOI 10.5935/2965-2774.20230317-pt
Views8INTRODUCTIONIn the eyes of laypeople, intensive care may seem like a precise and objective field of study. Even to health professionals, believing that medical practice within intensive care units (ICUs) should be predominantly guided by technical decisions seems sensible and reasonable, even though there are nuances and some space for subjectivity. However, a careful look […]See more -
Letter to the Editor
Estimated continuous cardiac output based on pulse wave transit time in critically ill children: a report of two cases
- Humberto Magalhães Silva ,
- Raisa Sanches Uzun ,
- Isabel de Siqueira Ferraz ,
- Marcelo Barciela Brandão ,
- Tiago Henrique de Souza
Abstract
Letter to the EditorEstimated continuous cardiac output based on pulse wave transit time in critically ill children: a report of two cases
Crit Care Sci. 2023;35(1):107-111
DOI 10.5935/2965-2774.20230305-pt
- Humberto Magalhães Silva ,
- Raisa Sanches Uzun ,
- Isabel de Siqueira Ferraz ,
- Marcelo Barciela Brandão ,
- Tiago Henrique de Souza
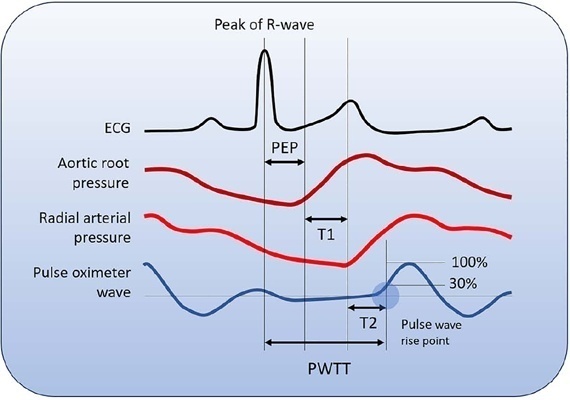
Views6See moreABSTRACT
Cardiac output is an essential determinant of oxygen delivery, although unreliably measured on clinical examination and routine monitoring. Unfortunately, cardiac output monitoring is rarely performed in pediatric critical care medicine, with a limited availability of accurate methods for children. Herein, we report two pediatric cases in which noninvasive pulse-wave transit time-based cardiac output monitoring (esCCO, Nihon Kohden, Tokyo, Japan) was used. The esCCO system calculates cardiac output continuously by using the negative correlation between stroke volume and pulse wave transit time and requires only electrocardiogram monitoring, noninvasive blood pressure, and pulse oximetry signals. Before starting its use, esCCO should be calibrated, which can be done using patient information (gender, age, height, and body weight) or entering cardiac output values obtained by other methods. In both cases, when calibrations were performed using patient information, the agreement between esCCO and echocardiographic measurements was poor. However, after calibration with transthoracic echocardiography, the cardiac output values obtained by both methods remained similar after 2 hours and 18 hours. The results indicate that the esCCO system is suitable for use in children; however, further studies are needed to optimize its algorithm and determine its accuracy, precision, and trend in children.
Views6Abstract
Letter to the EditorEstimated continuous cardiac output based on pulse wave transit time in critically ill children: a report of two cases
Crit Care Sci. 2023;35(1):107-111
DOI 10.5935/2965-2774.20230305-pt
- Humberto Magalhães Silva ,
- Raisa Sanches Uzun ,
- Isabel de Siqueira Ferraz ,
- Marcelo Barciela Brandão ,
- Tiago Henrique de Souza
Views6See moreABSTRACT
Cardiac output is an essential determinant of oxygen delivery, although unreliably measured on clinical examination and routine monitoring. Unfortunately, cardiac output monitoring is rarely performed in pediatric critical care medicine, with a limited availability of accurate methods for children. Herein, we report two pediatric cases in which noninvasive pulse-wave transit time-based cardiac output monitoring (esCCO, Nihon Kohden, Tokyo, Japan) was used. The esCCO system calculates cardiac output continuously by using the negative correlation between stroke volume and pulse wave transit time and requires only electrocardiogram monitoring, noninvasive blood pressure, and pulse oximetry signals. Before starting its use, esCCO should be calibrated, which can be done using patient information (gender, age, height, and body weight) or entering cardiac output values obtained by other methods. In both cases, when calibrations were performed using patient information, the agreement between esCCO and echocardiographic measurements was poor. However, after calibration with transthoracic echocardiography, the cardiac output values obtained by both methods remained similar after 2 hours and 18 hours. The results indicate that the esCCO system is suitable for use in children; however, further studies are needed to optimize its algorithm and determine its accuracy, precision, and trend in children.
- Humberto Magalhães Silva
Volume Articles - Critical Care Science (CCS)
