-
Editorial
Prone position failure in moderate-severe acute respiratory distress syndrome: and now?
Crit Care Sci. 2023;35(2):112-114
Abstract
EditorialProne position failure in moderate-severe acute respiratory distress syndrome: and now?
Crit Care Sci. 2023;35(2):112-114
DOI 10.5935/2965-2774.2023.Edit-1.v35n2-pt
Views11In 2013, a randomized, control, prospective, multicenter PROSEVA study was published() and compared 16 hours early prone to supine position in 474 acute respiratory distress syndrome (ARDS) patients with a partial pressure of oxygen/fraction of inspired oxygen (PaO2/FiO2) < 150 and with a positive end-expiratory pressure (PEEP) > 5cmH2O, and the study revealed that the […]See moreViews11

Abstract
EditorialProne position failure in moderate-severe acute respiratory distress syndrome: and now?
Crit Care Sci. 2023;35(2):112-114
DOI 10.5935/2965-2774.2023.Edit-1.v35n2-pt
Views11In 2013, a randomized, control, prospective, multicenter PROSEVA study was published() and compared 16 hours early prone to supine position in 474 acute respiratory distress syndrome (ARDS) patients with a partial pressure of oxygen/fraction of inspired oxygen (PaO2/FiO2) < 150 and with a positive end-expiratory pressure (PEEP) > 5cmH2O, and the study revealed that the […]See more -
Editorial
The relationship of postocclusive reactive hyperemia assessed by the plethysmographic perfusion index to lactate clearance: a new piece in the unsolved puzzle of tissue perfusion and oxygenation in septic shock
Crit Care Sci. 2023;35(2):115-116
Abstract
EditorialThe relationship of postocclusive reactive hyperemia assessed by the plethysmographic perfusion index to lactate clearance: a new piece in the unsolved puzzle of tissue perfusion and oxygenation in septic shock
Crit Care Sci. 2023;35(2):115-116
DOI 10.5935/2965-2774.2023.Edit-2.v35n2-pt
Views6Septic shock is commonly characterized by the lack of coherence between systemic hemodynamics and microcirculation.() The optimization of systemic cardiovascular variables frequently fails to improve the outcome of septic patients. Since the final goal of resuscitation should be the normalization of tissue perfusion and oxygenation, there is a growing interest in the monitoring of microvascular […]See moreViews6Abstract
EditorialThe relationship of postocclusive reactive hyperemia assessed by the plethysmographic perfusion index to lactate clearance: a new piece in the unsolved puzzle of tissue perfusion and oxygenation in septic shock
Crit Care Sci. 2023;35(2):115-116
DOI 10.5935/2965-2774.2023.Edit-2.v35n2-pt
Views6Septic shock is commonly characterized by the lack of coherence between systemic hemodynamics and microcirculation.() The optimization of systemic cardiovascular variables frequently fails to improve the outcome of septic patients. Since the final goal of resuscitation should be the normalization of tissue perfusion and oxygenation, there is a growing interest in the monitoring of microvascular […]See more -
Special Article
The use of bedside echocardiography in the care of critically ill patients – a joint consensus document of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Medicina de Emergência and Sociedade Brasileira de Medicina Hospitalar. Part 2 – Technical aspects
- José Augusto Santos Pellegrini
 ,
, - Ciro Leite Mendes ,
- Paulo César Gottardo ,
- Khalil Feitosa,
- Josiane França John , [ … ],
- Ricardo Luiz Cordioli
Abstract
Special ArticleThe use of bedside echocardiography in the care of critically ill patients – a joint consensus document of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Medicina de Emergência and Sociedade Brasileira de Medicina Hospitalar. Part 2 – Technical aspects
Crit Care Sci. 2023;35(2):117-146
DOI 10.5935/2965-2774.20230310-pt
- José Augusto Santos Pellegrini ,
- Ciro Leite Mendes ,
- Paulo César Gottardo ,
- Khalil Feitosa,
- Josiane França John ,
- Ana Cláudia Tonelli de Oliveira ,
- Alexandre Jorge de Andrade Negri,
- Ana Burigo Grumann ,
- Dalton de Souza Barros,
- Fátima Elizabeth Fonseca de Oliveira Negri,
- Gérson Luiz de Macedo ,
- Júlio Leal Bandeira Neves,
- Márcio da Silveira Rodrigues,
- Marcio Fernando Spagnól ,
- Marcus Antonio Ferez,
- Ricardo Ávila Chalhub ,
- Ricardo Luiz Cordioli
Views4ABSTRACT
Echocardiography in critically ill patients has become essential in the evaluation of patients in different settings, such as the hospital. However, unlike for other matters related to the care of these patients, there are still no recommendations from national medical societies on the subject. The objective of this document was to organize and make available expert consensus opinions that may help to better incorporate echocardiography in the evaluation of critically ill patients. Thus, the Associação de Medicina Intensiva Brasileira, the Associação Brasileira de Medicina de Emergência, and the Sociedade Brasileira de Medicina Hospitalar formed a group of 17 physicians to formulate questions relevant to the topic and discuss the possibility of consensus for each of them. All questions were prepared using a five-point Likert scale. Consensus was defined a priori as at least 80% of the responses between one and two or between four and five. The consideration of the issues involved two rounds of voting and debate among all participants. The 27 questions prepared make up the present document and are divided into 4 major assessment areas: left ventricular function, right ventricular function, diagnosis of shock, and hemodynamics. At the end of the process, there were 17 positive (agreement) and 3 negative (disagreement) consensuses; another 7 questions remained without consensus. Although areas of uncertainty persist, this document brings together consensus opinions on several issues related to echocardiography in critically ill patients and may enhance its development in the national scenario.
Keywords:Critical illnessEchocardiographyHemodynamicsShockSurveys and questionnairesVentricular function, leftVentricular function, rightSee moreViews4Abstract
Special ArticleThe use of bedside echocardiography in the care of critically ill patients – a joint consensus document of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Medicina de Emergência and Sociedade Brasileira de Medicina Hospitalar. Part 2 – Technical aspects
Crit Care Sci. 2023;35(2):117-146
DOI 10.5935/2965-2774.20230310-pt
- José Augusto Santos Pellegrini ,
- Ciro Leite Mendes ,
- Paulo César Gottardo ,
- Khalil Feitosa,
- Josiane França John ,
- Ana Cláudia Tonelli de Oliveira ,
- Alexandre Jorge de Andrade Negri,
- Ana Burigo Grumann ,
- Dalton de Souza Barros,
- Fátima Elizabeth Fonseca de Oliveira Negri,
- Gérson Luiz de Macedo ,
- Júlio Leal Bandeira Neves,
- Márcio da Silveira Rodrigues,
- Marcio Fernando Spagnól ,
- Marcus Antonio Ferez,
- Ricardo Ávila Chalhub ,
- Ricardo Luiz Cordioli
Views4ABSTRACT
Echocardiography in critically ill patients has become essential in the evaluation of patients in different settings, such as the hospital. However, unlike for other matters related to the care of these patients, there are still no recommendations from national medical societies on the subject. The objective of this document was to organize and make available expert consensus opinions that may help to better incorporate echocardiography in the evaluation of critically ill patients. Thus, the Associação de Medicina Intensiva Brasileira, the Associação Brasileira de Medicina de Emergência, and the Sociedade Brasileira de Medicina Hospitalar formed a group of 17 physicians to formulate questions relevant to the topic and discuss the possibility of consensus for each of them. All questions were prepared using a five-point Likert scale. Consensus was defined a priori as at least 80% of the responses between one and two or between four and five. The consideration of the issues involved two rounds of voting and debate among all participants. The 27 questions prepared make up the present document and are divided into 4 major assessment areas: left ventricular function, right ventricular function, diagnosis of shock, and hemodynamics. At the end of the process, there were 17 positive (agreement) and 3 negative (disagreement) consensuses; another 7 questions remained without consensus. Although areas of uncertainty persist, this document brings together consensus opinions on several issues related to echocardiography in critically ill patients and may enhance its development in the national scenario.
Keywords:Critical illnessEchocardiographyHemodynamicsShockSurveys and questionnairesVentricular function, leftVentricular function, rightSee more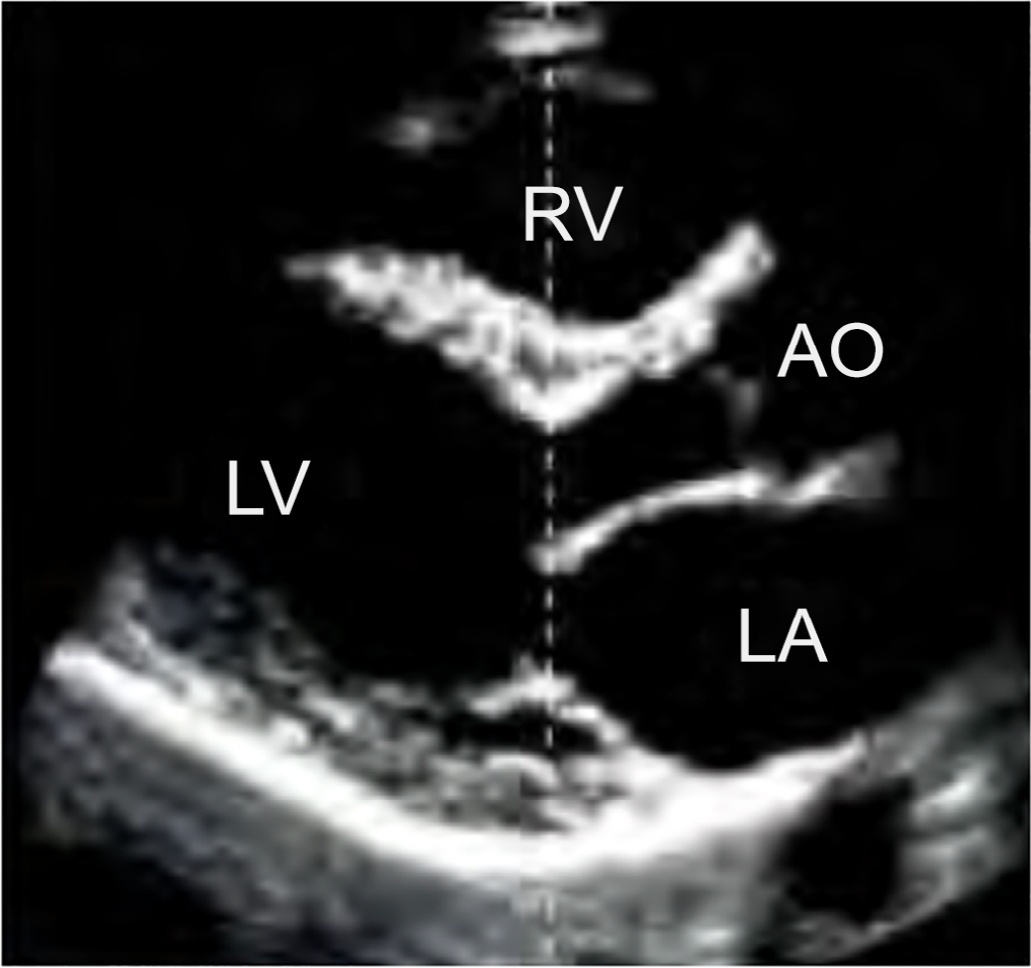
- José Augusto Santos Pellegrini
-
Original Article
Biomarkers of neuropsychiatric dysfunction in intensive care unit survivors: a prospective cohort study
- Franciani Rodrigues da Rocha ,
- Renata Casagrande Gonçalves ,
- Gabriele da Silveira Prestes ,
- Danusa Damásio ,
- Amanda Indalécio Goulart, [ … ],
- Felipe Dal-Pizzol
Abstract
Original ArticleBiomarkers of neuropsychiatric dysfunction in intensive care unit survivors: a prospective cohort study
Crit Care Sci. 2023;35(2):147-155
DOI 10.5935/2965-2774.20230422-pt
- Franciani Rodrigues da Rocha ,
- Renata Casagrande Gonçalves ,
- Gabriele da Silveira Prestes ,
- Danusa Damásio ,
- Amanda Indalécio Goulart,
- Andriele Aparecida da Silva Vieira ,
- Monique Michels ,
- Maria Inês da Rosa ,
- Cristiane Ritter ,
- Felipe Dal-Pizzol
Views8ABSTRACT
Objective:
To assess factors associated with long-term neuropsychiatric outcomes, including biomarkers measured after discharge from the intensive care unit.
Methods:
A prospective cohort study was performed with 65 intensive care unit survivors. The cognitive evaluation was performed through the Mini-Mental State Examination, the symptoms of anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale, and posttraumatic stress disorder was evaluated using the Impact of Event Scale-6. Plasma levels of amyloid-beta (1-42) [Aβ (1-42)], Aβ (1-40), interleukin (IL)-10, IL-6, IL-33, IL-4, IL-5, tumor necrosis factor alpha, C-reactive protein, and brain-derived neurotrophic factor were measured at intensive care unit discharge.
Results:
Of the variables associated with intensive care, only delirium was independently related to the occurrence of long-term cognitive impairment. In addition, higher levels of IL-10 and IL-6 were associated with cognitive dysfunction. Only IL-6 was independently associated with depression. Mechanical ventilation, IL-33 levels, and C-reactive protein levels were independently associated with anxiety. No variables were independently associated with posttraumatic stress disorder.
Conclusion:
Cognitive dysfunction, as well as symptoms of depression, anxiety, and posttraumatic stress disorder, are present in patients who survive a critical illness, and some of these outcomes are associated with the levels of inflammatory biomarkers measured at discharge from the intensive care unit.
Keywords:AnxietyBiomarkersCognitive dysfunctionCritical care outcomesCritical illnessDeliriumDepressionIntensive care unitsPatient dischargeSee moreViews8Abstract
Original ArticleBiomarkers of neuropsychiatric dysfunction in intensive care unit survivors: a prospective cohort study
Crit Care Sci. 2023;35(2):147-155
DOI 10.5935/2965-2774.20230422-pt
- Franciani Rodrigues da Rocha ,
- Renata Casagrande Gonçalves ,
- Gabriele da Silveira Prestes ,
- Danusa Damásio ,
- Amanda Indalécio Goulart,
- Andriele Aparecida da Silva Vieira ,
- Monique Michels ,
- Maria Inês da Rosa ,
- Cristiane Ritter ,
- Felipe Dal-Pizzol
Views8ABSTRACT
Objective:
To assess factors associated with long-term neuropsychiatric outcomes, including biomarkers measured after discharge from the intensive care unit.
Methods:
A prospective cohort study was performed with 65 intensive care unit survivors. The cognitive evaluation was performed through the Mini-Mental State Examination, the symptoms of anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale, and posttraumatic stress disorder was evaluated using the Impact of Event Scale-6. Plasma levels of amyloid-beta (1-42) [Aβ (1-42)], Aβ (1-40), interleukin (IL)-10, IL-6, IL-33, IL-4, IL-5, tumor necrosis factor alpha, C-reactive protein, and brain-derived neurotrophic factor were measured at intensive care unit discharge.
Results:
Of the variables associated with intensive care, only delirium was independently related to the occurrence of long-term cognitive impairment. In addition, higher levels of IL-10 and IL-6 were associated with cognitive dysfunction. Only IL-6 was independently associated with depression. Mechanical ventilation, IL-33 levels, and C-reactive protein levels were independently associated with anxiety. No variables were independently associated with posttraumatic stress disorder.
Conclusion:
Cognitive dysfunction, as well as symptoms of depression, anxiety, and posttraumatic stress disorder, are present in patients who survive a critical illness, and some of these outcomes are associated with the levels of inflammatory biomarkers measured at discharge from the intensive care unit.
Keywords:AnxietyBiomarkersCognitive dysfunctionCritical care outcomesCritical illnessDeliriumDepressionIntensive care unitsPatient dischargeSee more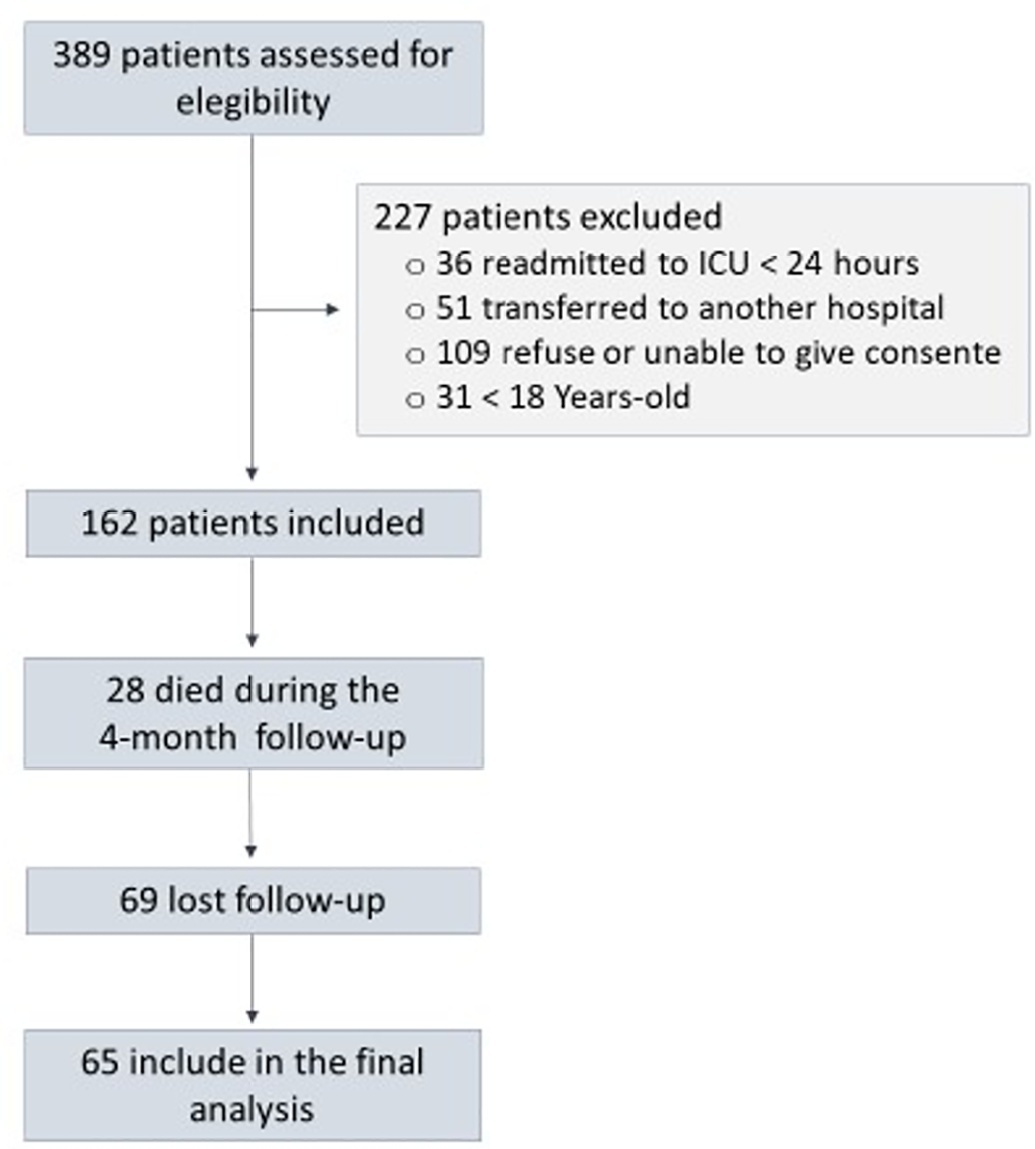
- Franciani Rodrigues da Rocha
-
Original Article
Factors associated with a nonresponse to prone positioning in patients with severe acute respiratory distress syndrome due to SARS-CoV-2
Crit Care Sci. 2023;35(2):156-162
Abstract
Original ArticleFactors associated with a nonresponse to prone positioning in patients with severe acute respiratory distress syndrome due to SARS-CoV-2
Crit Care Sci. 2023;35(2):156-162
DOI 10.5935/2965-2774.20230343-pt
Views7ABSTRACT
Objective:
To identify risk factors for nonresponse to prone positioning in mechanically ventilated patients with COVID-19-associated severe acute respiratory distress syndrome and refractory hypoxemia in a tertiary care hospital in Colombia.
Methods:
Observational study based on a retrospective cohort of mechanically ventilated patients with severe acute respiratory distress syndrome due to SARS-CoV-2 who underwent prone positioning due to refractory hypoxemia. The study considered an improvement ≥ 20% in the PaO2/FiO2 ratio after the first cycle of 16 hours in the prone position to be a ‘response’. Nonresponding patients were considered cases, and responding patients were controls. We controlled for clinical, laboratory, and radiological variables.
Results:
A total of 724 patients were included (58.67 ± 12.37 years, 67.7% males). Of those, 21.9% were nonresponders. Mortality was 54.1% for nonresponders and 31.3% for responders (p < 0.001). Variables associated with nonresponse were time from the start of mechanical ventilation to pronation (OR 1.23; 95%CI 1.10 - 1.41); preintubation PaO2/FiO2 ratio (OR 0.62; 95%CI 0.40 – 0.96); preprone PaO2/FiO2 ratio (OR 1.88. 95%CI 1.22 – 2.94); and radiologic multilobe consolidation (OR 2.12; 95%CI 1.33 – 3.33) or mixed pattern (OR 1.72; 95%CI 1.07 – 2.85) compared with a ground-glass pattern.
Conclusion:
This study identified factors associated with nonresponse to prone positioning in patients with refractory hypoxemia and acute respiratory distress syndrome due to SARS-CoV-2 receiving mechanical ventilation. Recognizing such factors helps identify candidates for other rescue strategies, including more extensive prone positioning or extracorporeal membrane oxygenation. Further studies are needed to assess the consistency of these findings in populations with acute respiratory distress syndrome of other etiologies.
Keywords:artificialCoronavirus infectionsCOVID-19HypoxiaintratrachealIntubationProne positionRespirationRespiratory distress syndromeSARS-CoV-2See moreViews7Abstract
Original ArticleFactors associated with a nonresponse to prone positioning in patients with severe acute respiratory distress syndrome due to SARS-CoV-2
Crit Care Sci. 2023;35(2):156-162
DOI 10.5935/2965-2774.20230343-pt
Views7ABSTRACT
Objective:
To identify risk factors for nonresponse to prone positioning in mechanically ventilated patients with COVID-19-associated severe acute respiratory distress syndrome and refractory hypoxemia in a tertiary care hospital in Colombia.
Methods:
Observational study based on a retrospective cohort of mechanically ventilated patients with severe acute respiratory distress syndrome due to SARS-CoV-2 who underwent prone positioning due to refractory hypoxemia. The study considered an improvement ≥ 20% in the PaO2/FiO2 ratio after the first cycle of 16 hours in the prone position to be a ‘response’. Nonresponding patients were considered cases, and responding patients were controls. We controlled for clinical, laboratory, and radiological variables.
Results:
A total of 724 patients were included (58.67 ± 12.37 years, 67.7% males). Of those, 21.9% were nonresponders. Mortality was 54.1% for nonresponders and 31.3% for responders (p < 0.001). Variables associated with nonresponse were time from the start of mechanical ventilation to pronation (OR 1.23; 95%CI 1.10 - 1.41); preintubation PaO2/FiO2 ratio (OR 0.62; 95%CI 0.40 – 0.96); preprone PaO2/FiO2 ratio (OR 1.88. 95%CI 1.22 – 2.94); and radiologic multilobe consolidation (OR 2.12; 95%CI 1.33 – 3.33) or mixed pattern (OR 1.72; 95%CI 1.07 – 2.85) compared with a ground-glass pattern.
Conclusion:
This study identified factors associated with nonresponse to prone positioning in patients with refractory hypoxemia and acute respiratory distress syndrome due to SARS-CoV-2 receiving mechanical ventilation. Recognizing such factors helps identify candidates for other rescue strategies, including more extensive prone positioning or extracorporeal membrane oxygenation. Further studies are needed to assess the consistency of these findings in populations with acute respiratory distress syndrome of other etiologies.
Keywords:artificialCoronavirus infectionsCOVID-19HypoxiaintratrachealIntubationProne positionRespirationRespiratory distress syndromeSARS-CoV-2See more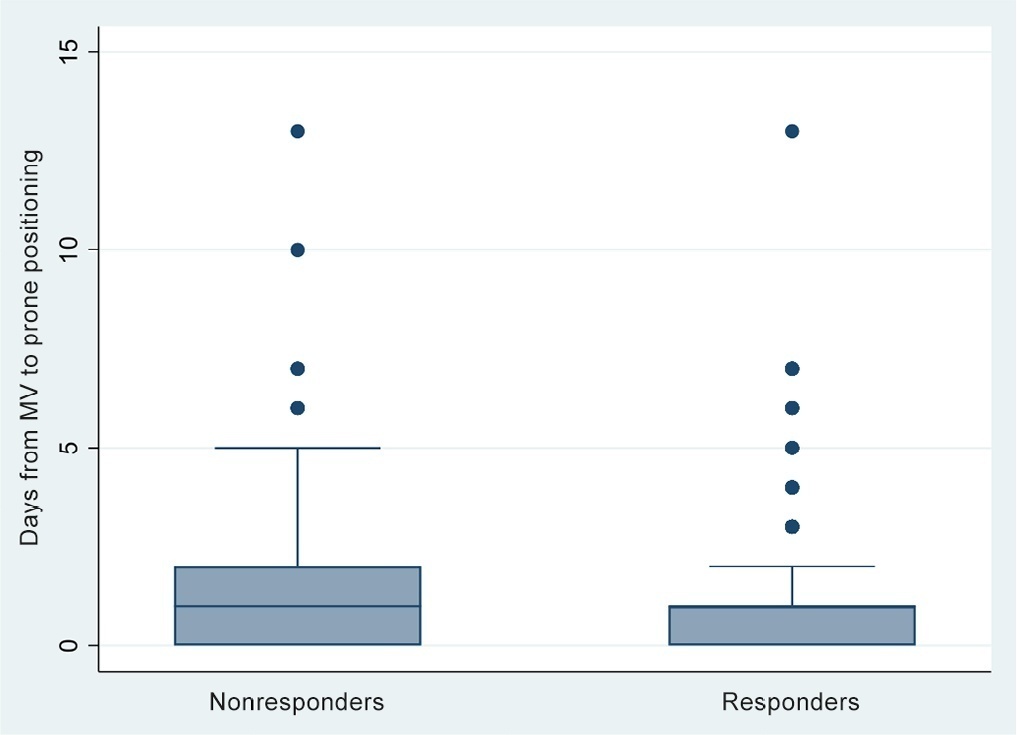
-
Original Article
Extubation failure and the use of noninvasive ventilation during the weaning process in critically ill COVID-19 patients
- Viviane Martins Corrêa Boniatti ,
- Chaiane Ribeiro Pereira ,
- Gabriela Machado Costa ,
- Michelle Carneiro Teixeira ,
- Alessandra Preisig Werlang , [ … ],
- Márcio Manozzo Boniatti
Abstract
Original ArticleExtubation failure and the use of noninvasive ventilation during the weaning process in critically ill COVID-19 patients
Crit Care Sci. 2023;35(2):163-167
DOI 10.5935/2965-2774.20230009-pt
- Viviane Martins Corrêa Boniatti ,
- Chaiane Ribeiro Pereira ,
- Gabriela Machado Costa ,
- Michelle Carneiro Teixeira ,
- Alessandra Preisig Werlang ,
- Francielle Thaisa Morais Martins ,
- Leonardo da Silva Marques ,
- Wagner Luís Nedel ,
- Márcio Manozzo Boniatti
Views7ABSTRACT
Objective:
To assess the outcome of extubation in COVID-19 patients and the use of noninvasive ventilation in the weaning process.
Methods:
This retrospective, observational, single-center study was conducted in COVID-19 patients aged 18 years or older who were admitted to an intensive care unit between April 2020 and December 2021, placed under mechanical ventilation for more than 48 hours and progressed to weaning. Early extubation was defined as extubation without a spontaneous breathing trial and immediate use of noninvasive ventilation after extubation. In patients who underwent a spontaneous breathing trial, noninvasive ventilation could be used as prophylactic ventilatory assistance when started immediately after extubation (prophylactic noninvasive ventilation) or as rescue therapy in cases of postextubation respiratory failure (therapeutic noninvasive ventilation). The primary outcome was extubation failure during the intensive care unit stay.
Results:
Three hundred eighty-four extubated patients were included. Extubation failure was observed in 107 (27.9%) patients. Forty-seven (12.2%) patients received prophylactic noninvasive ventilation. In 26 (6.8%) patients, early extubation was performed with immediate use of noninvasive ventilation. Noninvasive ventilation for the management of postextubation respiratory failure was administered to 64 (16.7%) patients.
Conclusion:
We found that COVID-19 patients had a high rate of extubation failure. Despite the high risk of extubation failure, we observed low use of prophylactic noninvasive ventilation in these patients.
Keywords:Airway extubationartificialCoronavirus infectionsCOVID-19Noninvasive ventilationRespirationSARS-CoV-2Ventilator weaningSee moreViews7Abstract
Original ArticleExtubation failure and the use of noninvasive ventilation during the weaning process in critically ill COVID-19 patients
Crit Care Sci. 2023;35(2):163-167
DOI 10.5935/2965-2774.20230009-pt
- Viviane Martins Corrêa Boniatti ,
- Chaiane Ribeiro Pereira ,
- Gabriela Machado Costa ,
- Michelle Carneiro Teixeira ,
- Alessandra Preisig Werlang ,
- Francielle Thaisa Morais Martins ,
- Leonardo da Silva Marques ,
- Wagner Luís Nedel ,
- Márcio Manozzo Boniatti
Views7ABSTRACT
Objective:
To assess the outcome of extubation in COVID-19 patients and the use of noninvasive ventilation in the weaning process.
Methods:
This retrospective, observational, single-center study was conducted in COVID-19 patients aged 18 years or older who were admitted to an intensive care unit between April 2020 and December 2021, placed under mechanical ventilation for more than 48 hours and progressed to weaning. Early extubation was defined as extubation without a spontaneous breathing trial and immediate use of noninvasive ventilation after extubation. In patients who underwent a spontaneous breathing trial, noninvasive ventilation could be used as prophylactic ventilatory assistance when started immediately after extubation (prophylactic noninvasive ventilation) or as rescue therapy in cases of postextubation respiratory failure (therapeutic noninvasive ventilation). The primary outcome was extubation failure during the intensive care unit stay.
Results:
Three hundred eighty-four extubated patients were included. Extubation failure was observed in 107 (27.9%) patients. Forty-seven (12.2%) patients received prophylactic noninvasive ventilation. In 26 (6.8%) patients, early extubation was performed with immediate use of noninvasive ventilation. Noninvasive ventilation for the management of postextubation respiratory failure was administered to 64 (16.7%) patients.
Conclusion:
We found that COVID-19 patients had a high rate of extubation failure. Despite the high risk of extubation failure, we observed low use of prophylactic noninvasive ventilation in these patients.
Keywords:Airway extubationartificialCoronavirus infectionsCOVID-19Noninvasive ventilationRespirationSARS-CoV-2Ventilator weaningSee more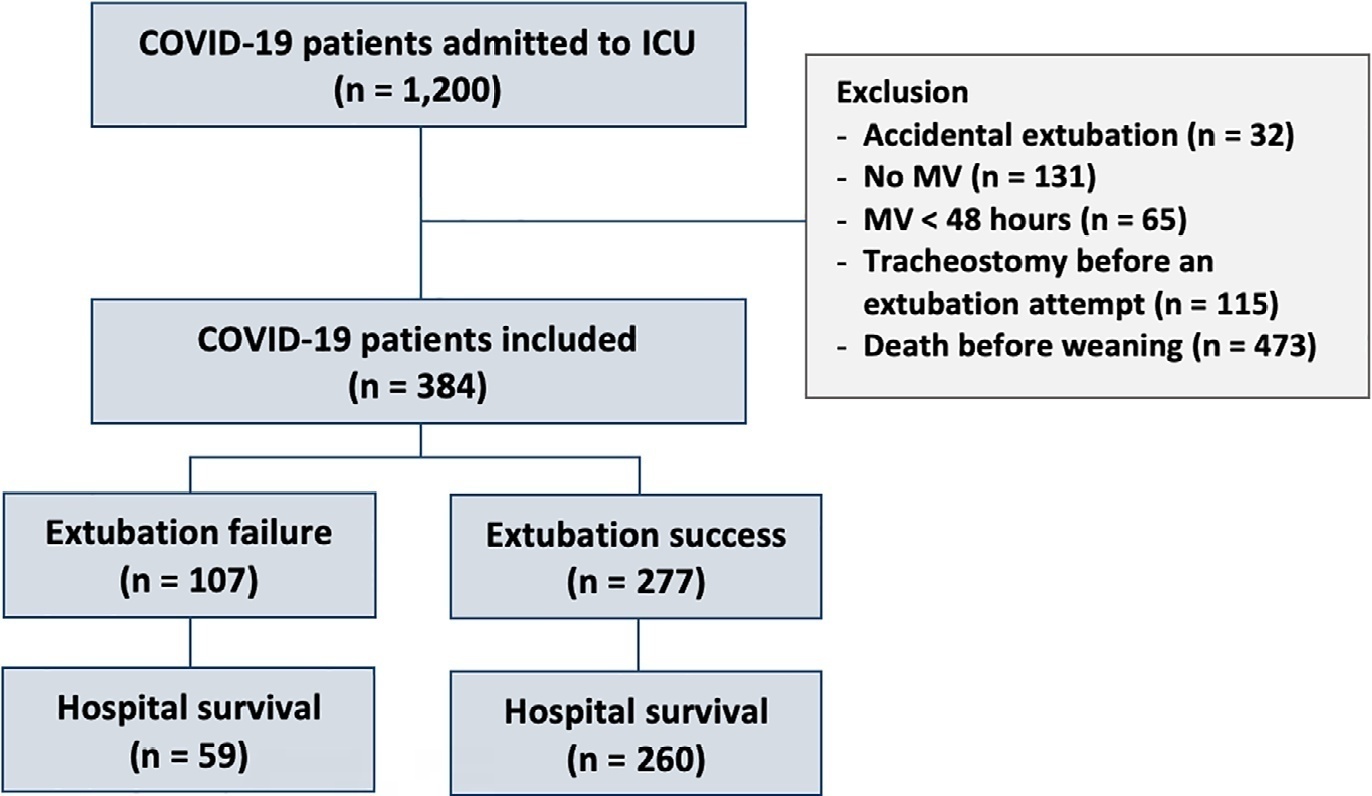
- Viviane Martins Corrêa Boniatti
-
Original Article
Effects of mechanical in-exsufflation in preventing postextubation acute respiratory failure in intensive care acquired weakness patients: a randomized controlled trial
- Philippe Wibart,
- Thomas Réginault ,
- Margarita Garcia-Fontan,
- Bérangère Barbrel,
- Clement Bader , [ … ],
- Frédéric Vargas
Abstract
Original ArticleEffects of mechanical in-exsufflation in preventing postextubation acute respiratory failure in intensive care acquired weakness patients: a randomized controlled trial
Crit Care Sci. 2023;35(2):168-176
DOI 10.5935/2965-2774.20230410-pt
- Philippe Wibart,
- Thomas Réginault ,
- Margarita Garcia-Fontan,
- Bérangère Barbrel,
- Clement Bader ,
- Antoine Benard,
- Verônica Franco Parreira ,
- Daniel Gonzalez-Antón,
- Nam H. Bui,
- Didier Gruson,
- Gilles Hilbert ,
- Roberto Martinez-Alejos ,
- Frédéric Vargas
Views5ABSTRACT
Objective:
We hypothesized that the use of mechanical insufflation-exsufflation can reduce the incidence of acute respiratory failure within the 48-hour post-extubation period in intensive care unit-acquired weakness patients.
Methods:
This was a prospective randomized controlled open-label trial. Patients diagnosed with intensive care unit-acquired weakness were consecutively enrolled based on a Medical Research Council score ≤ 48/60. The patients randomly received two daily sessions; in the control group, conventional chest physiotherapy was performed, while in the intervention group, chest physiotherapy was associated with mechanical insufflation-exsufflation. The incidence of acute respiratory failure within 48 hours of extubation was evaluated. Similarly, the reintubation rate, intensive care unit length of stay, mortality at 28 days, and survival probability at 90 days were assessed. The study was stopped after futility results in the interim analysis.
Results:
We included 122 consecutive patients (n = 61 per group). There was no significant difference in the incidence of acute respiratory failure between treatments (11.5% control group versus 16.4%, intervention group; p = 0.60), the need for reintubation (3.6% versus 10.7%; p = 0.27), mean length of stay (3 versus 4 days; p = 0.33), mortality at Day 28 (9.8% versus 15.0%; p = 0.42), or survival probability at Day 90 (21.3% versus 28.3%; p = 0.41).
Conclusion:
Mechanical insufflation-exsufflation combined with chest physiotherapy seems to have no impact in preventing postextubation acute respiratory failure in intensive care unit-acquired weakness patients. Similarly, mortality and survival probability were similar in both groups. Nevertheless, given the early termination of the trial, further clinical investigation is strongly recommended.
Clinical Trials Register:
Keywords:InsufflationIntensive care unitsMuscle weaknessRespiratory insufficiencyVentilator weaningWeaningSee moreViews5Abstract
Original ArticleEffects of mechanical in-exsufflation in preventing postextubation acute respiratory failure in intensive care acquired weakness patients: a randomized controlled trial
Crit Care Sci. 2023;35(2):168-176
DOI 10.5935/2965-2774.20230410-pt
- Philippe Wibart,
- Thomas Réginault ,
- Margarita Garcia-Fontan,
- Bérangère Barbrel,
- Clement Bader ,
- Antoine Benard,
- Verônica Franco Parreira ,
- Daniel Gonzalez-Antón,
- Nam H. Bui,
- Didier Gruson,
- Gilles Hilbert ,
- Roberto Martinez-Alejos ,
- Frédéric Vargas
Views5ABSTRACT
Objective:
We hypothesized that the use of mechanical insufflation-exsufflation can reduce the incidence of acute respiratory failure within the 48-hour post-extubation period in intensive care unit-acquired weakness patients.
Methods:
This was a prospective randomized controlled open-label trial. Patients diagnosed with intensive care unit-acquired weakness were consecutively enrolled based on a Medical Research Council score ≤ 48/60. The patients randomly received two daily sessions; in the control group, conventional chest physiotherapy was performed, while in the intervention group, chest physiotherapy was associated with mechanical insufflation-exsufflation. The incidence of acute respiratory failure within 48 hours of extubation was evaluated. Similarly, the reintubation rate, intensive care unit length of stay, mortality at 28 days, and survival probability at 90 days were assessed. The study was stopped after futility results in the interim analysis.
Results:
We included 122 consecutive patients (n = 61 per group). There was no significant difference in the incidence of acute respiratory failure between treatments (11.5% control group versus 16.4%, intervention group; p = 0.60), the need for reintubation (3.6% versus 10.7%; p = 0.27), mean length of stay (3 versus 4 days; p = 0.33), mortality at Day 28 (9.8% versus 15.0%; p = 0.42), or survival probability at Day 90 (21.3% versus 28.3%; p = 0.41).
Conclusion:
Mechanical insufflation-exsufflation combined with chest physiotherapy seems to have no impact in preventing postextubation acute respiratory failure in intensive care unit-acquired weakness patients. Similarly, mortality and survival probability were similar in both groups. Nevertheless, given the early termination of the trial, further clinical investigation is strongly recommended.
Clinical Trials Register:
Keywords:InsufflationIntensive care unitsMuscle weaknessRespiratory insufficiencyVentilator weaningWeaningSee more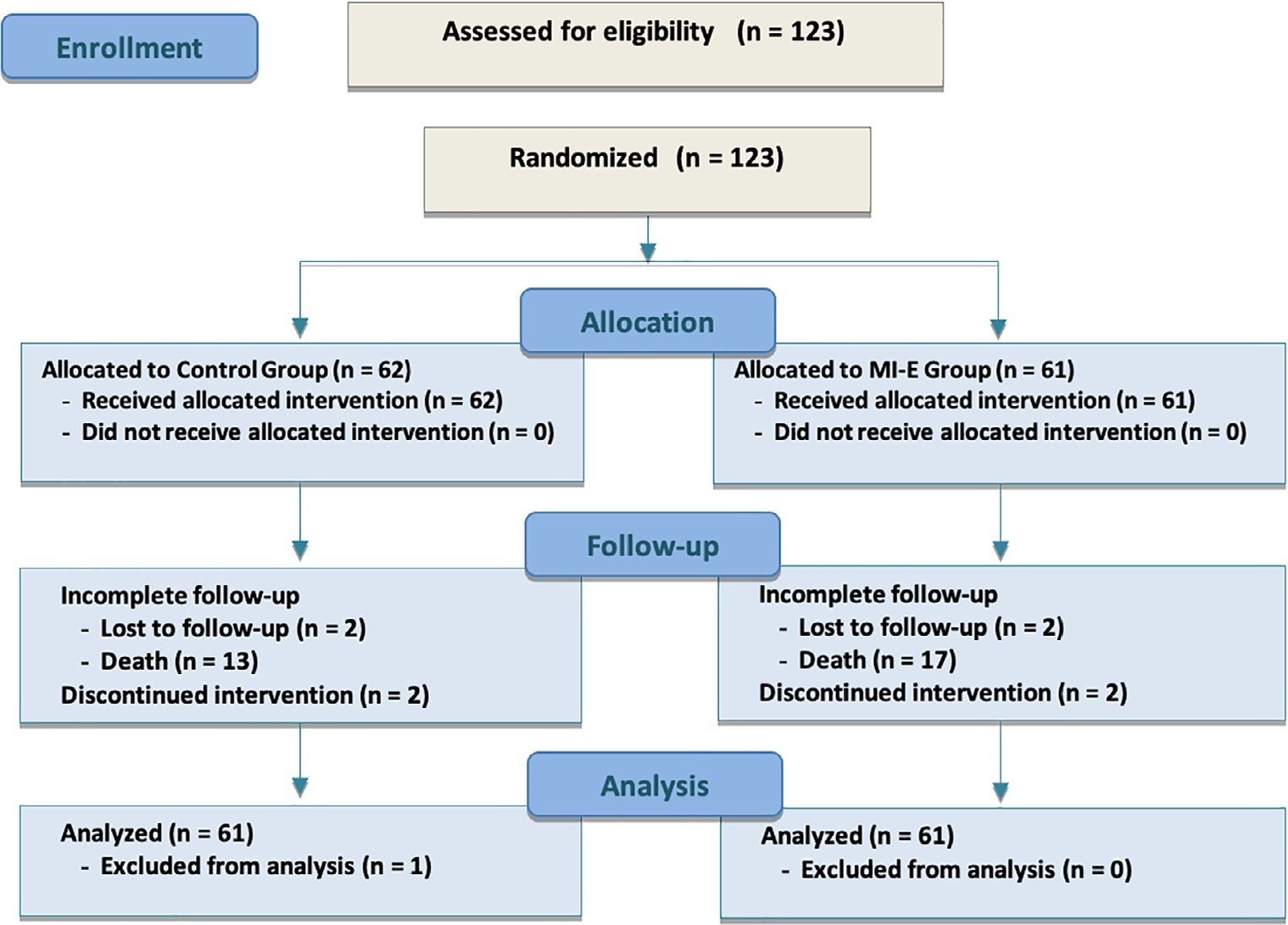
-
Original Article
Relationship between peripheral ischemic microvascular reserve, persistent hyperlactatemia, and its temporal dynamics in sepsis: a post hoc study
- Ana Carolina de Miranda ,
- Fernanda do Carmo De Stefani ,
- Bruna Cassia Dal Vesco ,
- Hipólito Carraro Júnior ,
- Jamil Assreuy , [ … ],
- Igor Alexandre Cortês de Menezes
Abstract
Original ArticleRelationship between peripheral ischemic microvascular reserve, persistent hyperlactatemia, and its temporal dynamics in sepsis: a post hoc study
Crit Care Sci. 2023;35(2):177-186
DOI 10.5935/2965-2774.20230348-pt
- Ana Carolina de Miranda ,
- Fernanda do Carmo De Stefani ,
- Bruna Cassia Dal Vesco ,
- Hipólito Carraro Júnior ,
- Jamil Assreuy ,
- Luis Gustavo Morello ,
- Igor Alexandre Cortês de Menezes
Views5See moreABSTRACT
Objective:
To measure the prognostic value of peripheral ischemic microvascular reserve in the context of persistent sepsis-induced hyperlactatemia and measure its influence on the temporal dynamics of lactate and the strength of association between these variables.
Methods:
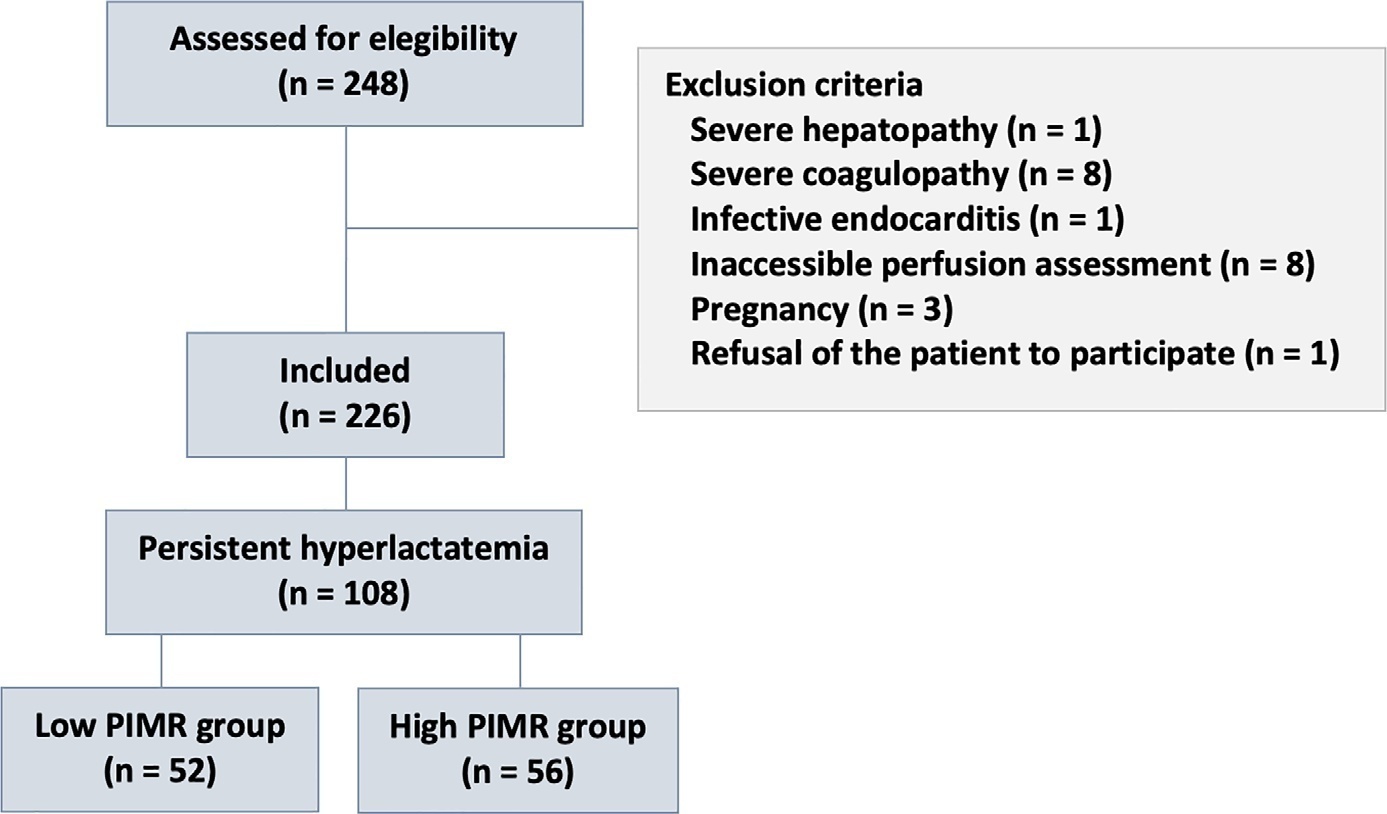
This post hoc analysis of the peripheral perfusion index/postocclusive reactive hyperemia trial, an observational cohort study that enrolled patients with sepsis who persisted with lactate levels ≥ 2mmol/L after fluid resuscitation (with or without shock). Peripheral ischemic microvascular reserve was evaluated using the association of the peripheral perfusion index and postocclusive reactive hyperemia techniques. The cutoff point of ∆ peripheral perfusion index peak values (%) defined the groups with low (≤ 62%) and high peripheral ischemic microvascular reserve (> 62%).
Results:
A total of 108 consecutive patients with persistent sepsis-induced hyperlactatemia were studied. The high peripheral ischemic microvascular reserve group showed higher 28-day mortality than the low peripheral ischemic microvascular reserve group (p < 0.01). The temporal dynamics of lactate within the first 48 hours showed a rapid decrease in lactate levels in the low peripheral ischemic microvascular reserve group (p < 0.01). However, this result was not reproduced in the linear mixed effects model. A weak correlation between peripheral ischemic microvascular reserve (%) and lactate level (mmol/L) was observed within the first 24 hours (r = 0.23; p < 0.05).
Conclusion:
The prognostic value of high peripheral ischemic microvascular reserve was confirmed in the context of persistent sepsis-induced hyperlactatemia. Although there was a weak positive correlation between peripheral ischemic microvascular reserve value and lactate level within the first 24 hours of sepsis diagnosis, the low peripheral ischemic microvascular reserve group appeared to have a faster decrease in lactate over the 48 hours of follow-up.
Views5Abstract
Original ArticleRelationship between peripheral ischemic microvascular reserve, persistent hyperlactatemia, and its temporal dynamics in sepsis: a post hoc study
Crit Care Sci. 2023;35(2):177-186
DOI 10.5935/2965-2774.20230348-pt
- Ana Carolina de Miranda ,
- Fernanda do Carmo De Stefani ,
- Bruna Cassia Dal Vesco ,
- Hipólito Carraro Júnior ,
- Jamil Assreuy ,
- Luis Gustavo Morello ,
- Igor Alexandre Cortês de Menezes
Views5See moreABSTRACT
Objective:
To measure the prognostic value of peripheral ischemic microvascular reserve in the context of persistent sepsis-induced hyperlactatemia and measure its influence on the temporal dynamics of lactate and the strength of association between these variables.
Methods:
This post hoc analysis of the peripheral perfusion index/postocclusive reactive hyperemia trial, an observational cohort study that enrolled patients with sepsis who persisted with lactate levels ≥ 2mmol/L after fluid resuscitation (with or without shock). Peripheral ischemic microvascular reserve was evaluated using the association of the peripheral perfusion index and postocclusive reactive hyperemia techniques. The cutoff point of ∆ peripheral perfusion index peak values (%) defined the groups with low (≤ 62%) and high peripheral ischemic microvascular reserve (> 62%).
Results:
A total of 108 consecutive patients with persistent sepsis-induced hyperlactatemia were studied. The high peripheral ischemic microvascular reserve group showed higher 28-day mortality than the low peripheral ischemic microvascular reserve group (p < 0.01). The temporal dynamics of lactate within the first 48 hours showed a rapid decrease in lactate levels in the low peripheral ischemic microvascular reserve group (p < 0.01). However, this result was not reproduced in the linear mixed effects model. A weak correlation between peripheral ischemic microvascular reserve (%) and lactate level (mmol/L) was observed within the first 24 hours (r = 0.23; p < 0.05).
Conclusion:
The prognostic value of high peripheral ischemic microvascular reserve was confirmed in the context of persistent sepsis-induced hyperlactatemia. Although there was a weak positive correlation between peripheral ischemic microvascular reserve value and lactate level within the first 24 hours of sepsis diagnosis, the low peripheral ischemic microvascular reserve group appeared to have a faster decrease in lactate over the 48 hours of follow-up.
- Ana Carolina de Miranda
-
Original Article
The predictive value of left ventricular global longitudinal strain in normotensive critically ill septic patients
- Timor Omar ,
- Kamil İnci ,
- Yusuf Oflu ,
- Mustafa Dilek ,
- Zeynep Binici Çelik , [ … ],
- Halil Murat Bucak
Abstract
Original ArticleThe predictive value of left ventricular global longitudinal strain in normotensive critically ill septic patients
Crit Care Sci. 2023;35(2):187-195
DOI 10.5935/2965-2774.20230378-pt
- Timor Omar ,
- Kamil İnci ,
- Yusuf Oflu ,
- Mustafa Dilek ,
- Zeynep Binici Çelik ,
- Soner Kına ,
- Doğan İliş ,
- Halil Murat Bucak
Views6ABSTRACT
Objective:
Evaluation of left ventricular systolic function using speckle tracking echocardiography is more sensitive than conventional echocardiographic measurement in detecting subtle left ventricular dysfunction in septic patients. Our purpose was to investigate the predictive significance of left ventricular global longitudinal strain in normotensive septic intensive care patients.
Methods:
This observational, prospective cohort study included septic normotensive adults admitted to the intensive care unit between June 1, 2021, and August 31, 2021. Left ventricular systolic function was measured using speckle-tracking echocardiography within 24 hours of admission.
Results:
One hundred fifty-two patients were enrolled. The intensive care unit mortality rate was 27%. Left ventricular global longitudinal strain was less negative, which indicated worse left ventricular function in non-survivors than survivors (median [interquartile range], -15.2 [-17.2 – -12.5] versus -17.3 [-18.8 – -15.5]; p < 0.001). The optimal cutoff value for left ventricular global longitudinal strain was -17% in predicting intensive care unit mortality (area under the curve, 0.728). Patients with left ventricular global longitudinal strain > -17% (less negative than -17%, which indicated worse left ventricular function) showed a significantly higher mortality rate (39.2% versus 13.7%; p < 0.001). According to multivariate analysis, left ventricular global longitudinal strain was an independent predictor of intensive care unit mortality [OR (95%CI), 1.326 (1.038 - 1.693); p = 0.024], along with invasive mechanical ventilation and Glasgow coma scale, APACHE II, and SOFA risk scores.
Conclusion:
Impaired left ventricular global longitudinal strain is associated with mortality and provided predictive data in normotensive septic intensive care patients.
Keywords:Critical careEchocardiographyGlobal longitudinal strainMortalitySepsisVentricular dysfunctionSee moreViews6Abstract
Original ArticleThe predictive value of left ventricular global longitudinal strain in normotensive critically ill septic patients
Crit Care Sci. 2023;35(2):187-195
DOI 10.5935/2965-2774.20230378-pt
- Timor Omar ,
- Kamil İnci ,
- Yusuf Oflu ,
- Mustafa Dilek ,
- Zeynep Binici Çelik ,
- Soner Kına ,
- Doğan İliş ,
- Halil Murat Bucak
Views6ABSTRACT
Objective:
Evaluation of left ventricular systolic function using speckle tracking echocardiography is more sensitive than conventional echocardiographic measurement in detecting subtle left ventricular dysfunction in septic patients. Our purpose was to investigate the predictive significance of left ventricular global longitudinal strain in normotensive septic intensive care patients.
Methods:
This observational, prospective cohort study included septic normotensive adults admitted to the intensive care unit between June 1, 2021, and August 31, 2021. Left ventricular systolic function was measured using speckle-tracking echocardiography within 24 hours of admission.
Results:
One hundred fifty-two patients were enrolled. The intensive care unit mortality rate was 27%. Left ventricular global longitudinal strain was less negative, which indicated worse left ventricular function in non-survivors than survivors (median [interquartile range], -15.2 [-17.2 – -12.5] versus -17.3 [-18.8 – -15.5]; p < 0.001). The optimal cutoff value for left ventricular global longitudinal strain was -17% in predicting intensive care unit mortality (area under the curve, 0.728). Patients with left ventricular global longitudinal strain > -17% (less negative than -17%, which indicated worse left ventricular function) showed a significantly higher mortality rate (39.2% versus 13.7%; p < 0.001). According to multivariate analysis, left ventricular global longitudinal strain was an independent predictor of intensive care unit mortality [OR (95%CI), 1.326 (1.038 - 1.693); p = 0.024], along with invasive mechanical ventilation and Glasgow coma scale, APACHE II, and SOFA risk scores.
Conclusion:
Impaired left ventricular global longitudinal strain is associated with mortality and provided predictive data in normotensive septic intensive care patients.
Keywords:Critical careEchocardiographyGlobal longitudinal strainMortalitySepsisVentricular dysfunctionSee more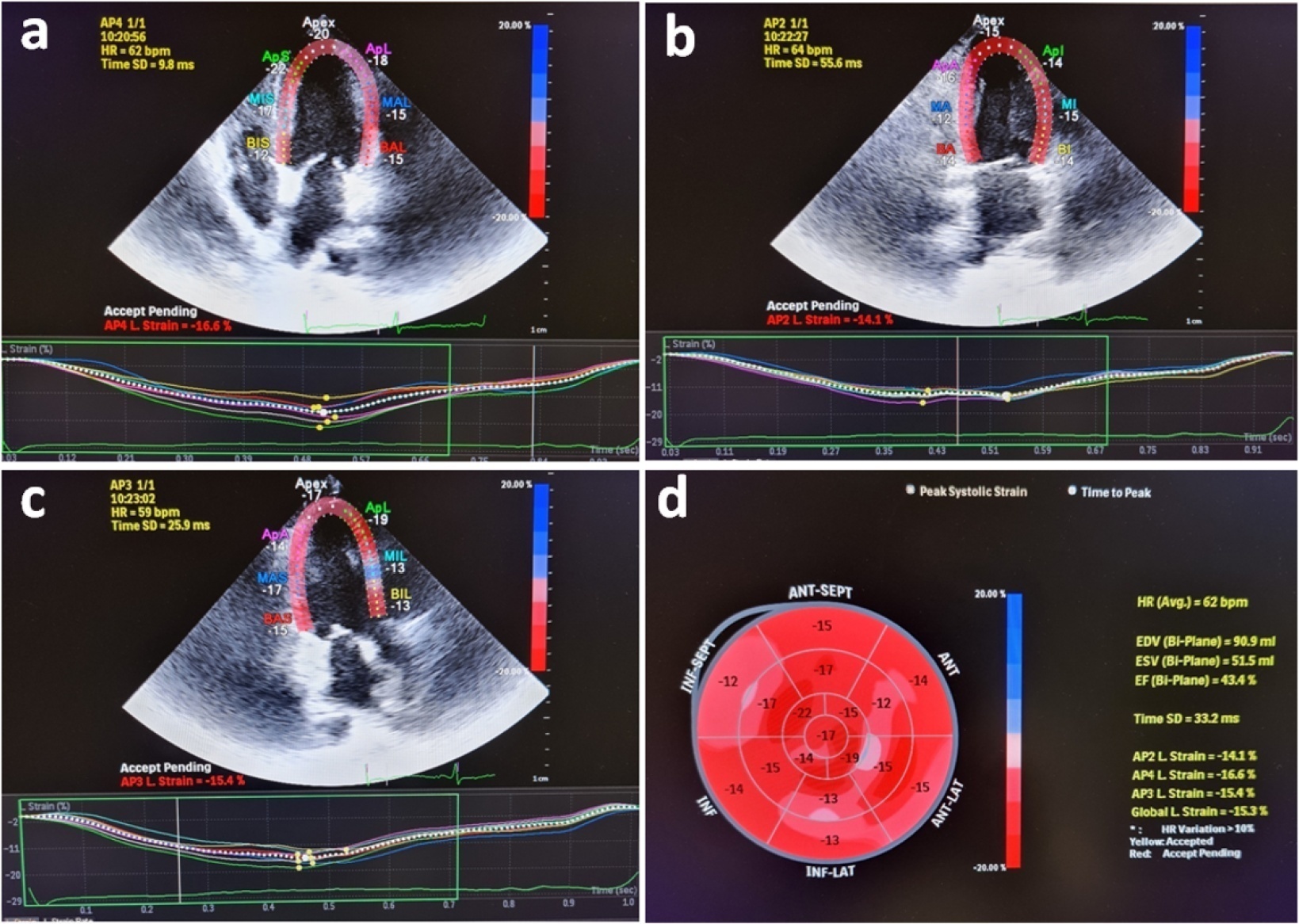
- Timor Omar
-
Original Article
Neurocritical care management supported by multimodal brain monitoring after acute brain injury
- Elisabete Monteiro ,
- António Ferreira ,
- Edite Raquel Mendes,
- Sofia Rocha e Silva,
- Isabel Maia, [ … ],
- Celeste Dias
Abstract
Original ArticleNeurocritical care management supported by multimodal brain monitoring after acute brain injury
Crit Care Sci. 2023;35(2):196-202
DOI 10.5935/2965-2774.20230036-pt
- Elisabete Monteiro ,
- António Ferreira ,
- Edite Raquel Mendes,
- Sofia Rocha e Silva,
- Isabel Maia,
- Cláudia Camila Dias ,
- Marek Czosnyka ,
- José Artur Paiva ,
- Celeste Dias
Views11ABSTRACT
Objective:
To evaluate the association between different intensive care units and levels of brain monitoring with outcomes in acute brain injury.
Methods:
Patients with traumatic brain injury and subarachnoid hemorrhage admitted to intensive care units were included. Neurocritical care unit management was compared to general intensive care unit management. Patients managed with multimodal brain monitoring and optimal cerebral perfusion pressure were compared with general management patients. A good outcome was defined as a Glasgow outcome scale score of 4 or 5.
Results:
Among 389 patients, 237 were admitted to the neurocritical care unit, and 152 were admitted to the general intensive care unit. Neurocritical care unit management patients had a lower risk of poor outcome (OR = 0.228). A subgroup of 69 patients with multimodal brain monitoring (G1) was compared with the remaining patients (G2). In the G1 and G2 groups, 59% versus 23% of patients, respectively, had a good outcome at intensive care unit discharge; 64% versus 31% had a good outcome at 28 days; 76% versus 50% had a good outcome at 3 months (p < 0.001); and 77% versus 58% had a good outcome at 6 months (p = 0.005). When outcomes were adjusted by SAPS II severity score, using good outcome as the dependent variable, the results were as follows: for G1 compared to G2, the OR was 4.607 at intensive care unit discharge (p < 0.001), 4.22 at 28 days (p = 0.001), 3.250 at 3 months (p = 0.001) and 2.529 at 6 months (p = 0.006). Patients with optimal cerebral perfusion pressure management (n = 127) had a better outcome at all points of evaluation. Mortality for those patients was significantly lower at 28 days (p = 0.001), 3 months (p < 0.001) and 6 months (p = 0.001).
Conclusion:
Multimodal brain monitoring with autoregulation and neurocritical care unit management were associated with better outcomes and should be considered after severe acute brain injury.
Keywords:Acute brain injuryAutoregulationCritical care outcomeIntensive care unitsMultimodal brain monitoringOptimal cerebral perfusion pressurePrognosisSee moreViews11Abstract
Original ArticleNeurocritical care management supported by multimodal brain monitoring after acute brain injury
Crit Care Sci. 2023;35(2):196-202
DOI 10.5935/2965-2774.20230036-pt
- Elisabete Monteiro ,
- António Ferreira ,
- Edite Raquel Mendes,
- Sofia Rocha e Silva,
- Isabel Maia,
- Cláudia Camila Dias ,
- Marek Czosnyka ,
- José Artur Paiva ,
- Celeste Dias
Views11ABSTRACT
Objective:
To evaluate the association between different intensive care units and levels of brain monitoring with outcomes in acute brain injury.
Methods:
Patients with traumatic brain injury and subarachnoid hemorrhage admitted to intensive care units were included. Neurocritical care unit management was compared to general intensive care unit management. Patients managed with multimodal brain monitoring and optimal cerebral perfusion pressure were compared with general management patients. A good outcome was defined as a Glasgow outcome scale score of 4 or 5.
Results:
Among 389 patients, 237 were admitted to the neurocritical care unit, and 152 were admitted to the general intensive care unit. Neurocritical care unit management patients had a lower risk of poor outcome (OR = 0.228). A subgroup of 69 patients with multimodal brain monitoring (G1) was compared with the remaining patients (G2). In the G1 and G2 groups, 59% versus 23% of patients, respectively, had a good outcome at intensive care unit discharge; 64% versus 31% had a good outcome at 28 days; 76% versus 50% had a good outcome at 3 months (p < 0.001); and 77% versus 58% had a good outcome at 6 months (p = 0.005). When outcomes were adjusted by SAPS II severity score, using good outcome as the dependent variable, the results were as follows: for G1 compared to G2, the OR was 4.607 at intensive care unit discharge (p < 0.001), 4.22 at 28 days (p = 0.001), 3.250 at 3 months (p = 0.001) and 2.529 at 6 months (p = 0.006). Patients with optimal cerebral perfusion pressure management (n = 127) had a better outcome at all points of evaluation. Mortality for those patients was significantly lower at 28 days (p = 0.001), 3 months (p < 0.001) and 6 months (p = 0.001).
Conclusion:
Multimodal brain monitoring with autoregulation and neurocritical care unit management were associated with better outcomes and should be considered after severe acute brain injury.
Keywords:Acute brain injuryAutoregulationCritical care outcomeIntensive care unitsMultimodal brain monitoringOptimal cerebral perfusion pressurePrognosisSee more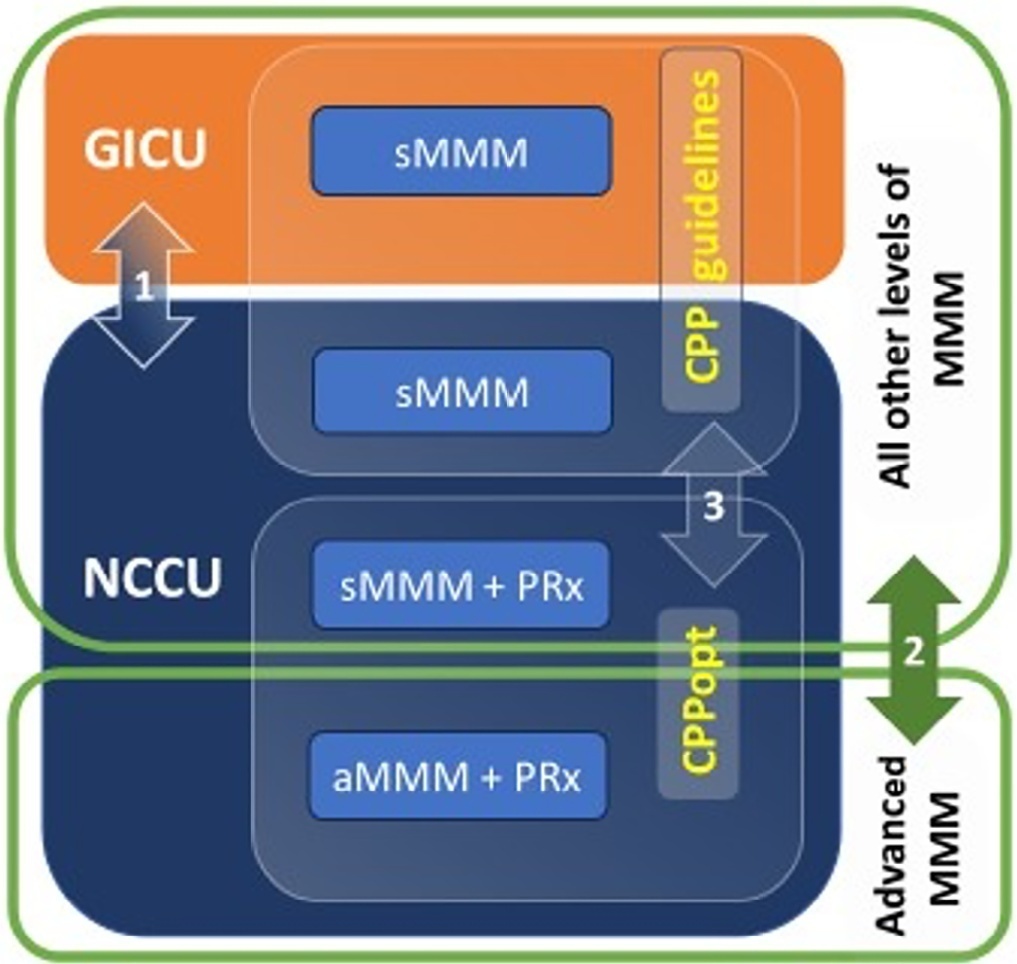
- Elisabete Monteiro
-
Original Article
Effects of participation in interdisciplinary rounds in the intensive care unit on family satisfaction: A cross-sectional study
- Daniel Schneider ,
- Regis Goulart Rosa ,
- Rosa da Rosa Minho dos Santos ,
- Débora Vaccaro Fogazzi ,
- Gabriela Soares Rech , [ … ],
- Mellina da Silva Terres
Abstract
Original ArticleEffects of participation in interdisciplinary rounds in the intensive care unit on family satisfaction: A cross-sectional study
Crit Care Sci. 2023;35(2):203-208
DOI 10.5935/2965-2774.20230274-pt
- Daniel Schneider ,
- Regis Goulart Rosa ,
- Rosa da Rosa Minho dos Santos ,
- Débora Vaccaro Fogazzi ,
- Gabriela Soares Rech ,
- Daiana Barbosa da Silva ,
- Mellina da Silva Terres
Views4See moreABSTRACT
Objective:
To investigate whether family participation in intensive care unit interdisciplinary bedside rounds affects family satisfaction.
Methods:
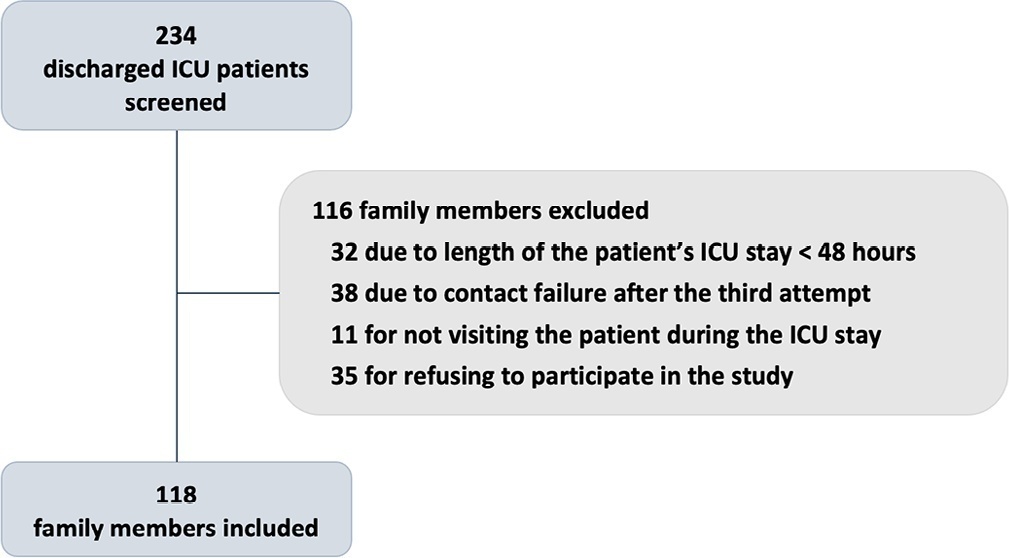
A cross-sectional study was conducted at a 56-bed, adult, mixed intensive care unit of a tertiary hospital in Southern Brazil. From May to June 2019, family members of patients who stayed in the intensive care unit for at least 48 hours were invited to participate in the study at the time of patient discharge. The main exposure variable was participation in intensive care unit bedside rounds during the intensive care unit stay. Family satisfaction was assessed by using the Brazilian version of the Family Satisfaction in the Intensive Care Unit questionnaire.
Results:
Of the 234 screened individuals, 118 were included. Eleven participants withdrew consent. A total of 107 individuals were assessed; 58 (54%) reported being present during bedside rounds, and 49 (46%) reported never being present. General satisfaction and satisfaction with the decision-making process were higher among families who were present during rounds than among families who were not (p = 0.01 and p = 0.007, respectively).
Conclusion:
The presence during interdisciplinary rounds was associated with improved general satisfaction and satisfaction with the decision-making aspect. This outcome indicates that efforts must be directed to conduct studies with more robust methodologies to confirm this association.
Views4Abstract
Original ArticleEffects of participation in interdisciplinary rounds in the intensive care unit on family satisfaction: A cross-sectional study
Crit Care Sci. 2023;35(2):203-208
DOI 10.5935/2965-2774.20230274-pt
- Daniel Schneider ,
- Regis Goulart Rosa ,
- Rosa da Rosa Minho dos Santos ,
- Débora Vaccaro Fogazzi ,
- Gabriela Soares Rech ,
- Daiana Barbosa da Silva ,
- Mellina da Silva Terres
Views4See moreABSTRACT
Objective:
To investigate whether family participation in intensive care unit interdisciplinary bedside rounds affects family satisfaction.
Methods:
A cross-sectional study was conducted at a 56-bed, adult, mixed intensive care unit of a tertiary hospital in Southern Brazil. From May to June 2019, family members of patients who stayed in the intensive care unit for at least 48 hours were invited to participate in the study at the time of patient discharge. The main exposure variable was participation in intensive care unit bedside rounds during the intensive care unit stay. Family satisfaction was assessed by using the Brazilian version of the Family Satisfaction in the Intensive Care Unit questionnaire.
Results:
Of the 234 screened individuals, 118 were included. Eleven participants withdrew consent. A total of 107 individuals were assessed; 58 (54%) reported being present during bedside rounds, and 49 (46%) reported never being present. General satisfaction and satisfaction with the decision-making process were higher among families who were present during rounds than among families who were not (p = 0.01 and p = 0.007, respectively).
Conclusion:
The presence during interdisciplinary rounds was associated with improved general satisfaction and satisfaction with the decision-making aspect. This outcome indicates that efforts must be directed to conduct studies with more robust methodologies to confirm this association.
- Daniel Schneider
-
Original Article
Oropharyngeal colostrum administration in neonates with gastroschisis: a randomized clinical trial
- Hellen Porto Pimenta ,
- Adriana Duarte Rocha ,
- Aline Carnevale Lia Dias Guimarães ,
- Ana Carolina Carioca da Costa ,
- Maria Elisabeth Lopes Moreira
Abstract
Original ArticleOropharyngeal colostrum administration in neonates with gastroschisis: a randomized clinical trial
Crit Care Sci. 2023;35(2):209-216
DOI 10.5935/2965-2774.20230010-pt
- Hellen Porto Pimenta ,
- Adriana Duarte Rocha ,
- Aline Carnevale Lia Dias Guimarães ,
- Ana Carolina Carioca da Costa ,
- Maria Elisabeth Lopes Moreira
Views3See moreABSTRACT
Objective:
To evaluate the effect of colostrum therapy on days to start a suckling diet in newborns diagnosed with simple gastroschisis.
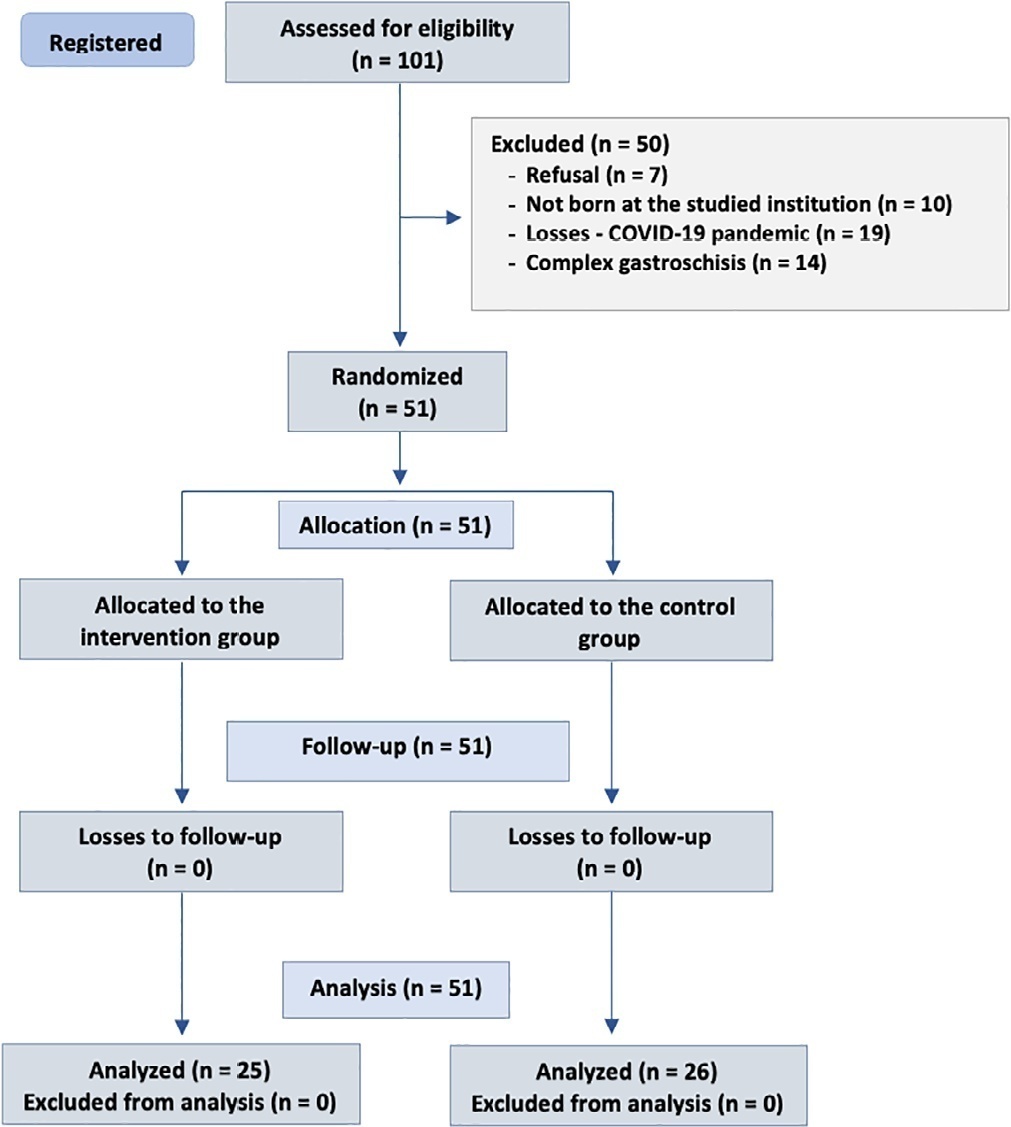
Methods:
Randomized clinical trial with newborns diagnosed with simple gastroschisis at a federal hospital in Rio de Janeiro who were randomized to receive oropharyngeal administration of 0.2mL of colostrum or a “sham procedure” during the first 3 days of life. The analysis included clinical outcomes such as days without food, days with parenteral feeding, days until the start of enteral feeding, days to reach complete enteral feeding, sepsis and length of hospital stay.
Results:
The onset of oral feeding (suction) in patients with simple gastroschisis in both groups occurred at a median of 15 days.
Conclusion:
The present study showed that there were no significant differences in the use of colostrum therapy and the number of days to the start of enteral feeding and suction diet between groups of newborns with simple gastroschisis.
Views3Abstract
Original ArticleOropharyngeal colostrum administration in neonates with gastroschisis: a randomized clinical trial
Crit Care Sci. 2023;35(2):209-216
DOI 10.5935/2965-2774.20230010-pt
- Hellen Porto Pimenta ,
- Adriana Duarte Rocha ,
- Aline Carnevale Lia Dias Guimarães ,
- Ana Carolina Carioca da Costa ,
- Maria Elisabeth Lopes Moreira
Views3See moreABSTRACT
Objective:
To evaluate the effect of colostrum therapy on days to start a suckling diet in newborns diagnosed with simple gastroschisis.
Methods:
Randomized clinical trial with newborns diagnosed with simple gastroschisis at a federal hospital in Rio de Janeiro who were randomized to receive oropharyngeal administration of 0.2mL of colostrum or a “sham procedure” during the first 3 days of life. The analysis included clinical outcomes such as days without food, days with parenteral feeding, days until the start of enteral feeding, days to reach complete enteral feeding, sepsis and length of hospital stay.
Results:
The onset of oral feeding (suction) in patients with simple gastroschisis in both groups occurred at a median of 15 days.
Conclusion:
The present study showed that there were no significant differences in the use of colostrum therapy and the number of days to the start of enteral feeding and suction diet between groups of newborns with simple gastroschisis.
- Hellen Porto Pimenta
-
Review
Cytokine hemoadsorption with CytoSorb® in patients with sepsis: a systematic review and meta-analysis
- Jiovany Jhan Carlos Saldaña-Gastulo ,
- María del Rosario Llamas-Barbarán ,
- Lelis G. Coronel-Chucos ,
- Yamilée Hurtado-Roca
Abstract
ReviewCytokine hemoadsorption with CytoSorb® in patients with sepsis: a systematic review and meta-analysis
Crit Care Sci. 2023;35(2):217-225
DOI 10.5935/2965-2774.20230289-pt
- Jiovany Jhan Carlos Saldaña-Gastulo ,
- María del Rosario Llamas-Barbarán ,
- Lelis G. Coronel-Chucos ,
- Yamilée Hurtado-Roca
Views4See moreABSTRACT
Objective:
To analyze the effect of CytoSorb® on mortality, interleukin levels, vasopressor use and adverse events in patients with sepsis.
Methods:
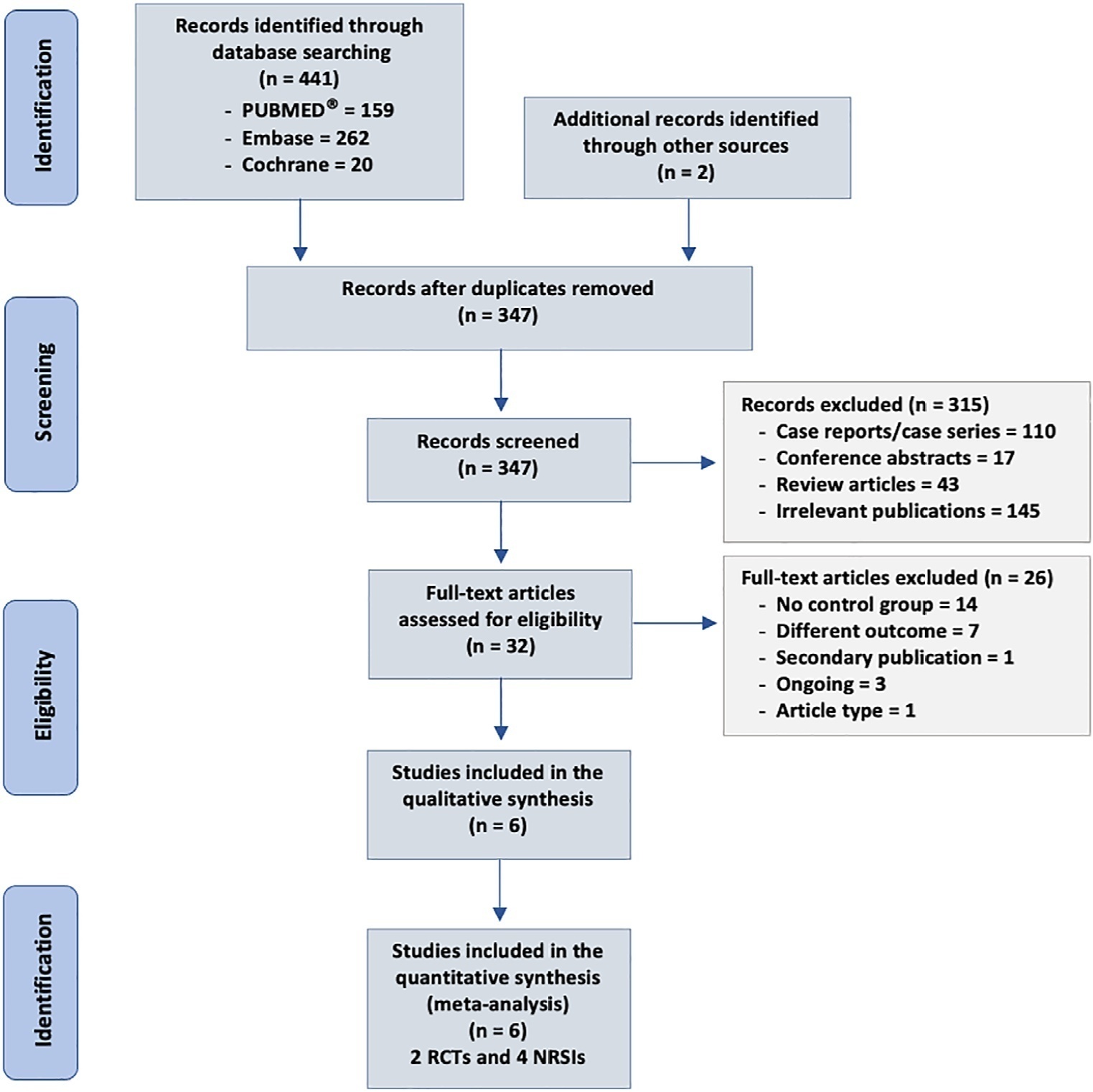
We searched MEDLINE®, Embase and the Cochrane Library for randomized controlled trials and cohort studies that reported the use of CytoSorb® among septic patients. The primary outcome was mortality, and secondary outcomes included the use of vasopressors, levels of inflammatory markers, predicted versus observed mortality, length of stay in the intensive care unit, and adverse events.
Results:
We included 6 studies enrolling 413 patients, and assessment for risk of bias indicated variations in study quality from high to moderate. The overall mortality rate was 45%, and no significant effect on mortality was found at 28 – 30 days (RR 0.98 [0.12 – 8.25] for the randomized clinical trial and RR 0.74 [0.49 – 1.13] for cohort studies). We did not perform a metanalysis for other outcomes due to the small number of studies found or the lack of data.
Conclusion:
Our study found very low certainty evidence, due to imprecision, risk of bias, and heterogeneity, thereby showing no benefit of CytoSorb® use in terms of mortality at 28 – 30 days. We cannot recommend the use of CytoSorb® in septic or septic shock patients outside clinical trials. Further high-quality randomized trials with a common intervention arm are needed to evaluate the influence of CytoSorb® in this population.
PROSPERO register:
Views4Abstract
ReviewCytokine hemoadsorption with CytoSorb® in patients with sepsis: a systematic review and meta-analysis
Crit Care Sci. 2023;35(2):217-225
DOI 10.5935/2965-2774.20230289-pt
- Jiovany Jhan Carlos Saldaña-Gastulo ,
- María del Rosario Llamas-Barbarán ,
- Lelis G. Coronel-Chucos ,
- Yamilée Hurtado-Roca
Views4See moreABSTRACT
Objective:
To analyze the effect of CytoSorb® on mortality, interleukin levels, vasopressor use and adverse events in patients with sepsis.
Methods:
We searched MEDLINE®, Embase and the Cochrane Library for randomized controlled trials and cohort studies that reported the use of CytoSorb® among septic patients. The primary outcome was mortality, and secondary outcomes included the use of vasopressors, levels of inflammatory markers, predicted versus observed mortality, length of stay in the intensive care unit, and adverse events.
Results:
We included 6 studies enrolling 413 patients, and assessment for risk of bias indicated variations in study quality from high to moderate. The overall mortality rate was 45%, and no significant effect on mortality was found at 28 – 30 days (RR 0.98 [0.12 – 8.25] for the randomized clinical trial and RR 0.74 [0.49 – 1.13] for cohort studies). We did not perform a metanalysis for other outcomes due to the small number of studies found or the lack of data.
Conclusion:
Our study found very low certainty evidence, due to imprecision, risk of bias, and heterogeneity, thereby showing no benefit of CytoSorb® use in terms of mortality at 28 – 30 days. We cannot recommend the use of CytoSorb® in septic or septic shock patients outside clinical trials. Further high-quality randomized trials with a common intervention arm are needed to evaluate the influence of CytoSorb® in this population.
PROSPERO register:
- Jiovany Jhan Carlos Saldaña-Gastulo
-
Letter to the Editor
Beyond fluid responsiveness: the concept of fluid tolerance and its potential implication in hemodynamic management
Crit Care Sci. 2023;35(2):226-229
Abstract
Letter to the EditorBeyond fluid responsiveness: the concept of fluid tolerance and its potential implication in hemodynamic management
Crit Care Sci. 2023;35(2):226-229
DOI 10.5935/2965-2774.20230012-pt
Views4INTRODUCTIONDespite the different methodologies and definitions in the literature, the most accepted concept of fluid responsiveness (FR) is an increase in cardiac output greater than 10-15% induced by an increased preload. Thus, volume expansion is the initial measure most frequently used to optimize tissue perfusion in a hemodynamically unstable patient. However, the prevalence of FR […]See moreViews4Abstract
Letter to the EditorBeyond fluid responsiveness: the concept of fluid tolerance and its potential implication in hemodynamic management
Crit Care Sci. 2023;35(2):226-229
DOI 10.5935/2965-2774.20230012-pt
Views4INTRODUCTIONDespite the different methodologies and definitions in the literature, the most accepted concept of fluid responsiveness (FR) is an increase in cardiac output greater than 10-15% induced by an increased preload. Thus, volume expansion is the initial measure most frequently used to optimize tissue perfusion in a hemodynamically unstable patient. However, the prevalence of FR […]See more
-
Letter to the Editor
High mortality in Brazilian intensive care units can be a problem of laws rather than a technical one: focus on sedation practices
Crit Care Sci. 2023;35(2):230-232
Abstract
Letter to the EditorHigh mortality in Brazilian intensive care units can be a problem of laws rather than a technical one: focus on sedation practices
Crit Care Sci. 2023;35(2):230-232
DOI 10.5935/2965-2774.20230337-pt
Views6TO THE EDITORIn the care of ventilated critically ill patients, there is a consistent relationship between deeper sedation and worse intensive care unit (ICU) outcomes.(,) Deep sedation in the first 48 hours of an ICU stay has been associated with delayed time to extubation, higher need for tracheostomy, longer ICU stays, and increased risk of […]See moreViews6Abstract
Letter to the EditorHigh mortality in Brazilian intensive care units can be a problem of laws rather than a technical one: focus on sedation practices
Crit Care Sci. 2023;35(2):230-232
DOI 10.5935/2965-2774.20230337-pt
Views6TO THE EDITORIn the care of ventilated critically ill patients, there is a consistent relationship between deeper sedation and worse intensive care unit (ICU) outcomes.(,) Deep sedation in the first 48 hours of an ICU stay has been associated with delayed time to extubation, higher need for tracheostomy, longer ICU stays, and increased risk of […]See more -
Letter to the Editor
Methemoglobinemia induced by dapsone in a pediatric patient: case report
Crit Care Sci. 2023;35(2):233-235
Abstract
Letter to the EditorMethemoglobinemia induced by dapsone in a pediatric patient: case report
Crit Care Sci. 2023;35(2):233-235
DOI 10.5935/2965-2774.20230018-pt
Views5INTRODUCTIONMethemoglobinemia is a rare condition and one of the differential diagnoses of cyanosis in the pediatric age group.() Clinical symptoms vary according to the levels of methemoglobin (MetHb) in the blood and may be nonspecific. The most common symptoms are central cyanosis, headache, fatigue, and respiratory depression.() Therefore, it is essential to recognize and treat […]See moreViews5Abstract
Letter to the EditorMethemoglobinemia induced by dapsone in a pediatric patient: case report
Crit Care Sci. 2023;35(2):233-235
DOI 10.5935/2965-2774.20230018-pt
Views5INTRODUCTIONMethemoglobinemia is a rare condition and one of the differential diagnoses of cyanosis in the pediatric age group.() Clinical symptoms vary according to the levels of methemoglobin (MetHb) in the blood and may be nonspecific. The most common symptoms are central cyanosis, headache, fatigue, and respiratory depression.() Therefore, it is essential to recognize and treat […]See more -
Letter to the Editor
Acute kidney injury in hospitalized patients with COVID-19: a retrospective cohort
- Fernando Godinho Zampieri ,
- Henrique Palomba ,
- Fernando Augusto Bozza ,
- Daniel C. Cubos ,
- Thiago G Romano
Abstract
Letter to the EditorAcute kidney injury in hospitalized patients with COVID-19: a retrospective cohort
Crit Care Sci. 2023;35(2):236-238
DOI 10.5935/2965-2774.20230428-pt
- Fernando Godinho Zampieri ,
- Henrique Palomba ,
- Fernando Augusto Bozza ,
- Daniel C. Cubos ,
- Thiago G Romano
Views4TO THE EDITORCoronavirus disease 2019 (COVID-19) has been reported to cause acute kidney injury (AKI).(-) Although severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may directly harm the kidneys through endothelial and coagulation dysfunction,() AKI in COVID-19 may also be related to additional organ dysfunctions and other host factors, including mechanical ventilation. The incidence of AKI […]See moreViews4Abstract
Letter to the EditorAcute kidney injury in hospitalized patients with COVID-19: a retrospective cohort
Crit Care Sci. 2023;35(2):236-238
DOI 10.5935/2965-2774.20230428-pt
- Fernando Godinho Zampieri ,
- Henrique Palomba ,
- Fernando Augusto Bozza ,
- Daniel C. Cubos ,
- Thiago G Romano
Views4TO THE EDITORCoronavirus disease 2019 (COVID-19) has been reported to cause acute kidney injury (AKI).(-) Although severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may directly harm the kidneys through endothelial and coagulation dysfunction,() AKI in COVID-19 may also be related to additional organ dysfunctions and other host factors, including mechanical ventilation. The incidence of AKI […]See more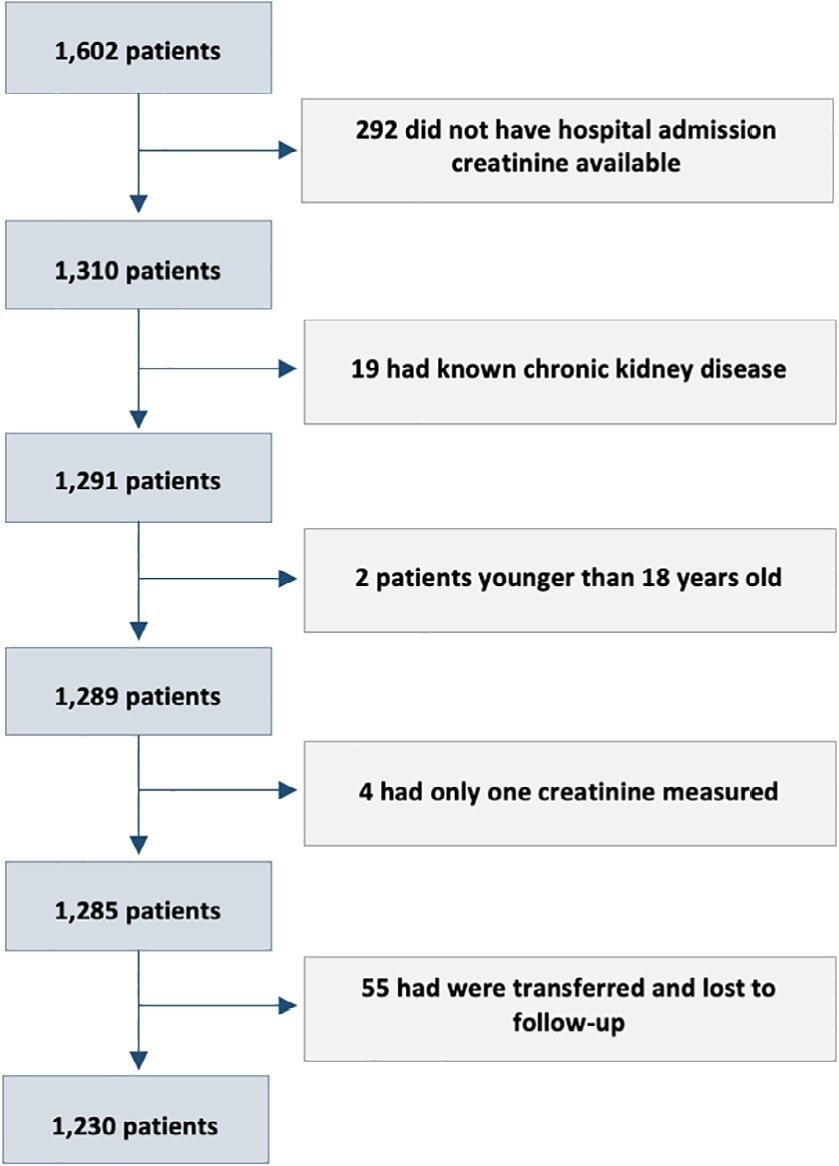
- Fernando Godinho Zampieri
-
Letter to the Editor
Sulfonamide-induced acute eosinophilic pneumonia requiring extracorporeal membrane oxygenation support: a case report
- Ana Flávia Garcia Silva ,
- Lívia Maria Garcia Melro ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Pedro Vitale Mendes ,
- Marcelo Park
Abstract
Letter to the EditorSulfonamide-induced acute eosinophilic pneumonia requiring extracorporeal membrane oxygenation support: a case report
Crit Care Sci. 2023;35(2):239-242
DOI 10.5935/2965-2774.20230404-pt
- Ana Flávia Garcia Silva ,
- Lívia Maria Garcia Melro ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Pedro Vitale Mendes ,
- Marcelo Park
Views3INTRODUCTIONAcute eosinophilic pneumonia (AEP) is a rare cause of acute respiratory failure that affects people aged 20-40 years old.() Patients with AEP present with rapid onset of cough, dyspnea, tachypnea and fever of usually less than 7 days of duration. Hypoxemia is present in all cases, and most patients do not have peripheral blood eosinophilia. […]See moreViews3Abstract
Letter to the EditorSulfonamide-induced acute eosinophilic pneumonia requiring extracorporeal membrane oxygenation support: a case report
Crit Care Sci. 2023;35(2):239-242
DOI 10.5935/2965-2774.20230404-pt
- Ana Flávia Garcia Silva ,
- Lívia Maria Garcia Melro ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Pedro Vitale Mendes ,
- Marcelo Park
Views3INTRODUCTIONAcute eosinophilic pneumonia (AEP) is a rare cause of acute respiratory failure that affects people aged 20-40 years old.() Patients with AEP present with rapid onset of cough, dyspnea, tachypnea and fever of usually less than 7 days of duration. Hypoxemia is present in all cases, and most patients do not have peripheral blood eosinophilia. […]See more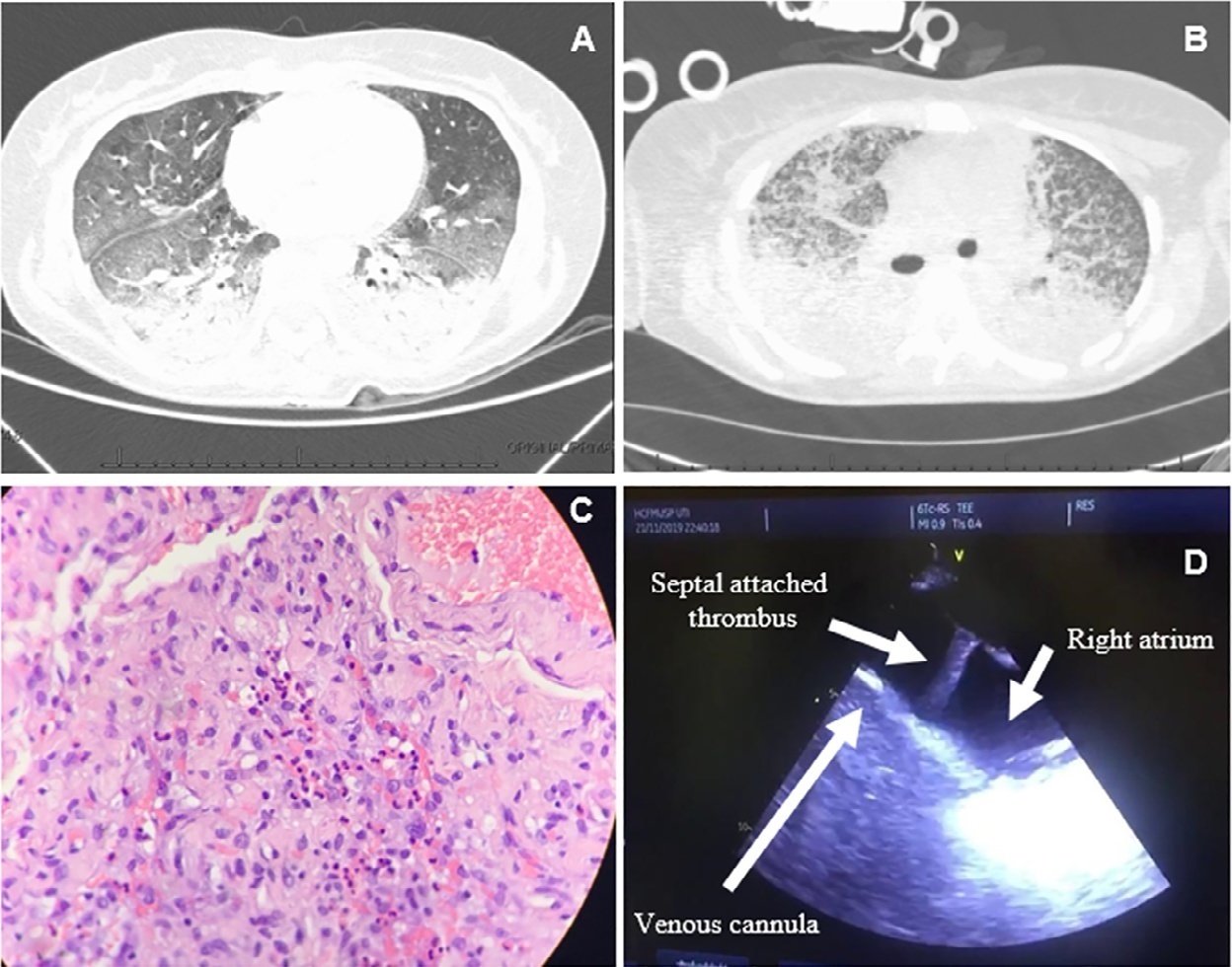
- Ana Flávia Garcia Silva
Volume Articles - Critical Care Science (CCS)
