Respiration Archives - Page 2 of 2 - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2024;36:e20240246en
DOI 10.62675/2965-2774.20240246-en
To discuss the strengths and limitations of ventilator-free days and to provide a comprehensive discussion of the different analytic methods for analyzing and interpreting this outcome.
Using simulations, the power of different analytical methods was assessed, namely: quantile (median) regression, cumulative logistic regression, generalized pairwise comparison, conditional approach and truncated approach. Overall, 3,000 simulations of a two-arm trial with n = 300 per arm were computed using a two-sided alternative hypothesis and a type I error rate of α = 0.05.
When considering power, median regression did not perform well in studies where the treatment effect was mainly driven by mortality. Median regression performed better in situations with a weak effect on mortality but a strong effect on duration, duration only, and moderate mortality and duration. Cumulative logistic regression was found to produce similar power to the Wilcoxon rank-sum test across all scenarios, being the best strategy for the scenarios of moderate mortality and duration, weak mortality and strong duration, and duration only.
In this study, we describe the relative power of new methods for analyzing ventilator-free days in critical care research. Our data provide validation and guidance for the use of the cumulative logistic model, median regression, generalized pairwise comparisons, and the conditional and truncated approach in specific scenarios.
Abstract
Crit Care Sci. 2024;36:e20240246en
DOI 10.62675/2965-2774.20240246-en
To discuss the strengths and limitations of ventilator-free days and to provide a comprehensive discussion of the different analytic methods for analyzing and interpreting this outcome.
Using simulations, the power of different analytical methods was assessed, namely: quantile (median) regression, cumulative logistic regression, generalized pairwise comparison, conditional approach and truncated approach. Overall, 3,000 simulations of a two-arm trial with n = 300 per arm were computed using a two-sided alternative hypothesis and a type I error rate of α = 0.05.
When considering power, median regression did not perform well in studies where the treatment effect was mainly driven by mortality. Median regression performed better in situations with a weak effect on mortality but a strong effect on duration, duration only, and moderate mortality and duration. Cumulative logistic regression was found to produce similar power to the Wilcoxon rank-sum test across all scenarios, being the best strategy for the scenarios of moderate mortality and duration, weak mortality and strong duration, and duration only.
In this study, we describe the relative power of new methods for analyzing ventilator-free days in critical care research. Our data provide validation and guidance for the use of the cumulative logistic model, median regression, generalized pairwise comparisons, and the conditional and truncated approach in specific scenarios.
Abstract
Crit Care Sci. 2024;36:e20240158en
DOI 10.62675/2965-2774.20240158-en
To evaluate the association of biomarkers with successful ventilatory weaning in COVID-19 patients.
An observational, retrospective, and single-center study was conducted between March 2020 and April 2021. C-reactive protein, total lymphocytes, and the neutrophil/lymphocyte ratio were evaluated during attrition and extubation, and the variation in these biomarker values was measured. The primary outcome was successful extubation. ROC curves were drawn to find the best cutoff points for the biomarkers based on sensitivity and specificity. Statistical analysis was performed using logistic regression.
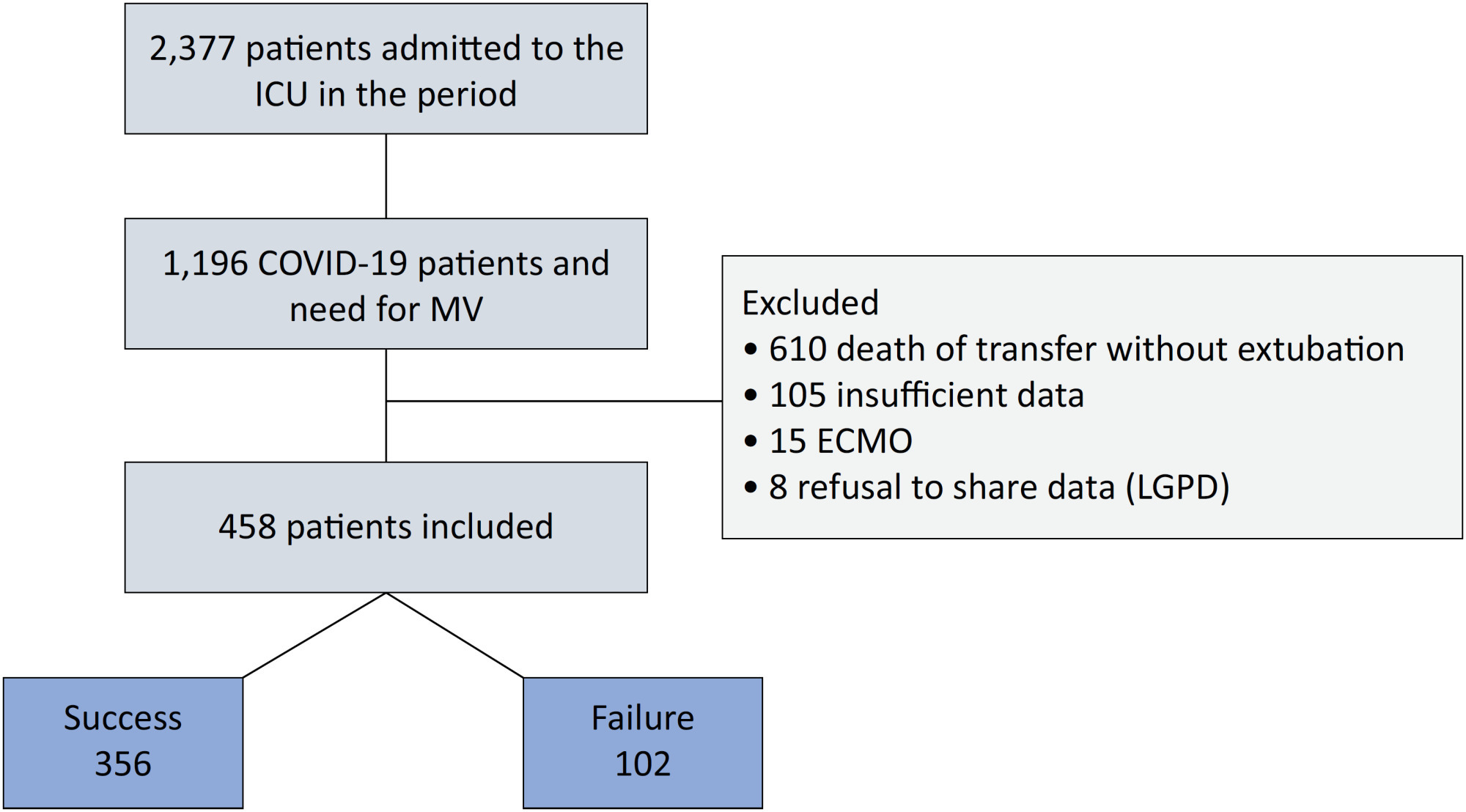
Of the 2,377 patients admitted to the intensive care unit, 458 were included in the analysis, 356 in the Successful Weaning Group and 102 in the Failure Group. The cutoff points found from the ROC curves were −62.4% for C-reactive protein, +45.7% for total lymphocytes, and −32.9% for neutrophil/lymphocyte ratio. These points were significantly associated with greater extubation success. In the multivariate analysis, only C-reactive protein variation remained statistically significant (OR 2.6; 95%CI 1.51 – 4.5; p < 0.001).
In this study, a decrease in C-reactive protein levels was associated with successful extubation in COVID-19 patients. Total lymphocytes and the neutrophil/lymphocyte ratio did not maintain the association after multivariate analysis. However, a decrease in C-reactive protein levels should not be used as a sole variable to identify COVID-19 patients suitable for weaning; as in our study, the area under the ROC curve demonstrated poor accuracy in discriminating extubation outcomes, with low sensitivity and specificity.
Abstract
Crit Care Sci. 2024;36:e20240158en
DOI 10.62675/2965-2774.20240158-en
To evaluate the association of biomarkers with successful ventilatory weaning in COVID-19 patients.
An observational, retrospective, and single-center study was conducted between March 2020 and April 2021. C-reactive protein, total lymphocytes, and the neutrophil/lymphocyte ratio were evaluated during attrition and extubation, and the variation in these biomarker values was measured. The primary outcome was successful extubation. ROC curves were drawn to find the best cutoff points for the biomarkers based on sensitivity and specificity. Statistical analysis was performed using logistic regression.
Of the 2,377 patients admitted to the intensive care unit, 458 were included in the analysis, 356 in the Successful Weaning Group and 102 in the Failure Group. The cutoff points found from the ROC curves were −62.4% for C-reactive protein, +45.7% for total lymphocytes, and −32.9% for neutrophil/lymphocyte ratio. These points were significantly associated with greater extubation success. In the multivariate analysis, only C-reactive protein variation remained statistically significant (OR 2.6; 95%CI 1.51 – 4.5; p < 0.001).
In this study, a decrease in C-reactive protein levels was associated with successful extubation in COVID-19 patients. Total lymphocytes and the neutrophil/lymphocyte ratio did not maintain the association after multivariate analysis. However, a decrease in C-reactive protein levels should not be used as a sole variable to identify COVID-19 patients suitable for weaning; as in our study, the area under the ROC curve demonstrated poor accuracy in discriminating extubation outcomes, with low sensitivity and specificity.
Abstract
Crit Care Sci. 2023;35(3):281-289
DOI 10.5935/2965-2774.20230041-pt
To evaluate if the reductions in systemic and renal oxygen consumption are associated with the development of evidence of anaerobic metabolism.
This is a subanalysis of a previously published study. In anesthetized and mechanically ventilated sheep, we measured the respiratory quotient by indirect calorimetry and its systemic, renal, and intestinal surrogates (the ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference. The Endotoxemic Shock Group (n = 12) was measured at baseline, after 60 minutes of endotoxemic shock, and after 60 and 120 minutes of fluid and norepinephrine resuscitation, and the values were compared with those of a Control Group (n = 12) without interventions.
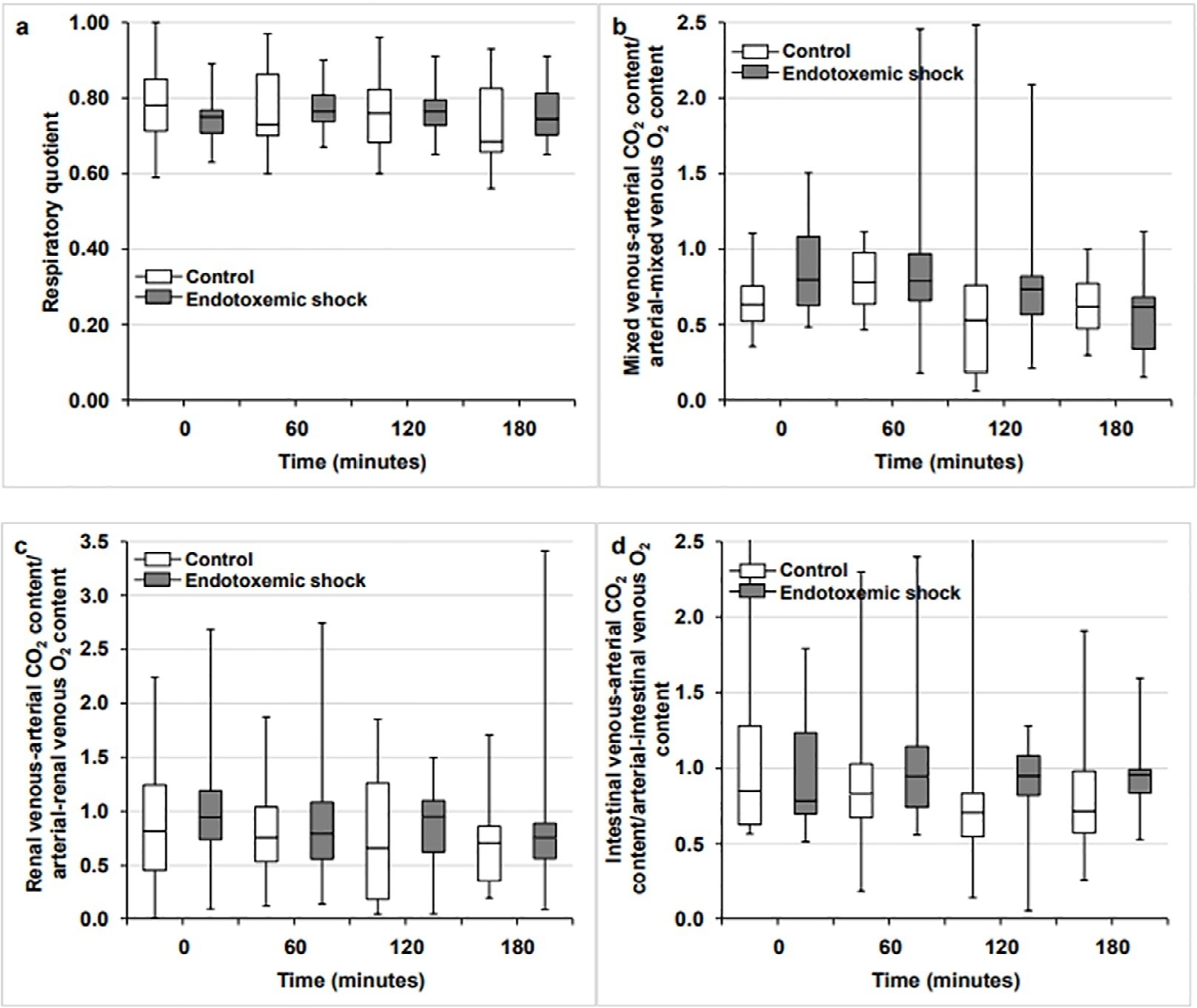
Endotoxemic shock decreased systemic and renal oxygen consumption (6.3 [5.6 - 6.6] versus 7.4 [6.3 - 8.5] mL/minute/kg and 3.7 [3.3 - 4.5] versus 5.4 [4.6 - 9.4] mL/minute/100g; p < 0.05 for both). After 120 minutes of resuscitation, systemic oxygen consumption was normalized, but renal oxygen consumption remained decreased (6.3 [5.9 - 8.2] versus 7.1 [6.1 - 8.6] mL/minute/100g; p = not significance and 3.8 [1.9 - 4.8] versus 5.7 [4.5 - 7.1]; p < 0.05). The respiratory quotient and the systemic, renal and intestinal ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference did not change throughout the experiments.
In this experimental model of septic shock, oxygen supply dependence was not associated with increases in the respiratory quotient or its surrogates. Putative explanations for these findings are the absence of anaerobic metabolism or the poor sensitivity of these variables in detecting this condition.
Abstract
Crit Care Sci. 2023;35(3):281-289
DOI 10.5935/2965-2774.20230041-pt
To evaluate if the reductions in systemic and renal oxygen consumption are associated with the development of evidence of anaerobic metabolism.
This is a subanalysis of a previously published study. In anesthetized and mechanically ventilated sheep, we measured the respiratory quotient by indirect calorimetry and its systemic, renal, and intestinal surrogates (the ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference. The Endotoxemic Shock Group (n = 12) was measured at baseline, after 60 minutes of endotoxemic shock, and after 60 and 120 minutes of fluid and norepinephrine resuscitation, and the values were compared with those of a Control Group (n = 12) without interventions.
Endotoxemic shock decreased systemic and renal oxygen consumption (6.3 [5.6 - 6.6] versus 7.4 [6.3 - 8.5] mL/minute/kg and 3.7 [3.3 - 4.5] versus 5.4 [4.6 - 9.4] mL/minute/100g; p < 0.05 for both). After 120 minutes of resuscitation, systemic oxygen consumption was normalized, but renal oxygen consumption remained decreased (6.3 [5.9 - 8.2] versus 7.1 [6.1 - 8.6] mL/minute/100g; p = not significance and 3.8 [1.9 - 4.8] versus 5.7 [4.5 - 7.1]; p < 0.05). The respiratory quotient and the systemic, renal and intestinal ratios of the venous-arterial carbon dioxide pressure and content difference to the arterial-venous oxygen content difference did not change throughout the experiments.
In this experimental model of septic shock, oxygen supply dependence was not associated with increases in the respiratory quotient or its surrogates. Putative explanations for these findings are the absence of anaerobic metabolism or the poor sensitivity of these variables in detecting this condition.
Abstract
Crit Care Sci. 2023;35(2):156-162
DOI 10.5935/2965-2774.20230343-pt
To identify risk factors for nonresponse to prone positioning in mechanically ventilated patients with COVID-19-associated severe acute respiratory distress syndrome and refractory hypoxemia in a tertiary care hospital in Colombia.
Observational study based on a retrospective cohort of mechanically ventilated patients with severe acute respiratory distress syndrome due to SARS-CoV-2 who underwent prone positioning due to refractory hypoxemia. The study considered an improvement ≥ 20% in the PaO2/FiO2 ratio after the first cycle of 16 hours in the prone position to be a ‘response’. Nonresponding patients were considered cases, and responding patients were controls. We controlled for clinical, laboratory, and radiological variables.
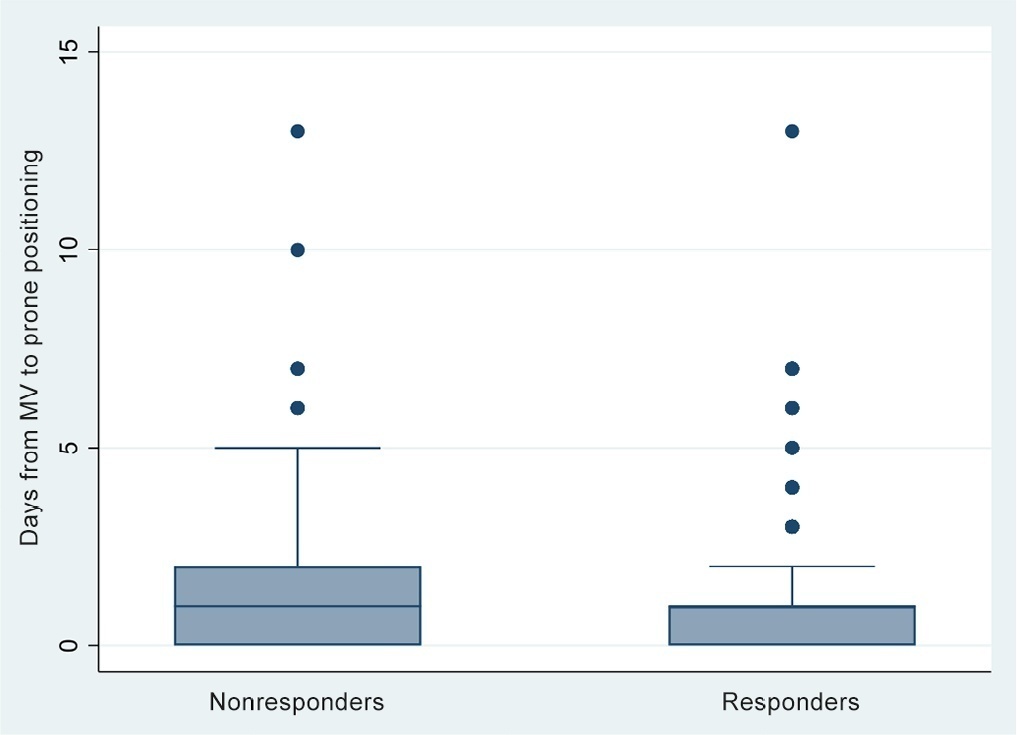
A total of 724 patients were included (58.67 ± 12.37 years, 67.7% males). Of those, 21.9% were nonresponders. Mortality was 54.1% for nonresponders and 31.3% for responders (p < 0.001). Variables associated with nonresponse were time from the start of mechanical ventilation to pronation (OR 1.23; 95%CI 1.10 - 1.41); preintubation PaO2/FiO2 ratio (OR 0.62; 95%CI 0.40 - 0.96); preprone PaO2/FiO2 ratio (OR 1.88. 95%CI 1.22 - 2.94); and radiologic multilobe consolidation (OR 2.12; 95%CI 1.33 - 3.33) or mixed pattern (OR 1.72; 95%CI 1.07 - 2.85) compared with a ground-glass pattern.
This study identified factors associated with nonresponse to prone positioning in patients with refractory hypoxemia and acute respiratory distress syndrome due to SARS-CoV-2 receiving mechanical ventilation. Recognizing such factors helps identify candidates for other rescue strategies, including more extensive prone positioning or extracorporeal membrane oxygenation. Further studies are needed to assess the consistency of these findings in populations with acute respiratory distress syndrome of other etiologies.
Abstract
Crit Care Sci. 2023;35(2):156-162
DOI 10.5935/2965-2774.20230343-pt
To identify risk factors for nonresponse to prone positioning in mechanically ventilated patients with COVID-19-associated severe acute respiratory distress syndrome and refractory hypoxemia in a tertiary care hospital in Colombia.
Observational study based on a retrospective cohort of mechanically ventilated patients with severe acute respiratory distress syndrome due to SARS-CoV-2 who underwent prone positioning due to refractory hypoxemia. The study considered an improvement ≥ 20% in the PaO2/FiO2 ratio after the first cycle of 16 hours in the prone position to be a ‘response’. Nonresponding patients were considered cases, and responding patients were controls. We controlled for clinical, laboratory, and radiological variables.
A total of 724 patients were included (58.67 ± 12.37 years, 67.7% males). Of those, 21.9% were nonresponders. Mortality was 54.1% for nonresponders and 31.3% for responders (p < 0.001). Variables associated with nonresponse were time from the start of mechanical ventilation to pronation (OR 1.23; 95%CI 1.10 - 1.41); preintubation PaO2/FiO2 ratio (OR 0.62; 95%CI 0.40 - 0.96); preprone PaO2/FiO2 ratio (OR 1.88. 95%CI 1.22 - 2.94); and radiologic multilobe consolidation (OR 2.12; 95%CI 1.33 - 3.33) or mixed pattern (OR 1.72; 95%CI 1.07 - 2.85) compared with a ground-glass pattern.
This study identified factors associated with nonresponse to prone positioning in patients with refractory hypoxemia and acute respiratory distress syndrome due to SARS-CoV-2 receiving mechanical ventilation. Recognizing such factors helps identify candidates for other rescue strategies, including more extensive prone positioning or extracorporeal membrane oxygenation. Further studies are needed to assess the consistency of these findings in populations with acute respiratory distress syndrome of other etiologies.
Abstract
Crit Care Sci. 2023;35(2):163-167
DOI 10.5935/2965-2774.20230009-pt
To assess the outcome of extubation in COVID-19 patients and the use of noninvasive ventilation in the weaning process.
This retrospective, observational, single-center study was conducted in COVID-19 patients aged 18 years or older who were admitted to an intensive care unit between April 2020 and December 2021, placed under mechanical ventilation for more than 48 hours and progressed to weaning. Early extubation was defined as extubation without a spontaneous breathing trial and immediate use of noninvasive ventilation after extubation. In patients who underwent a spontaneous breathing trial, noninvasive ventilation could be used as prophylactic ventilatory assistance when started immediately after extubation (prophylactic noninvasive ventilation) or as rescue therapy in cases of postextubation respiratory failure (therapeutic noninvasive ventilation). The primary outcome was extubation failure during the intensive care unit stay.
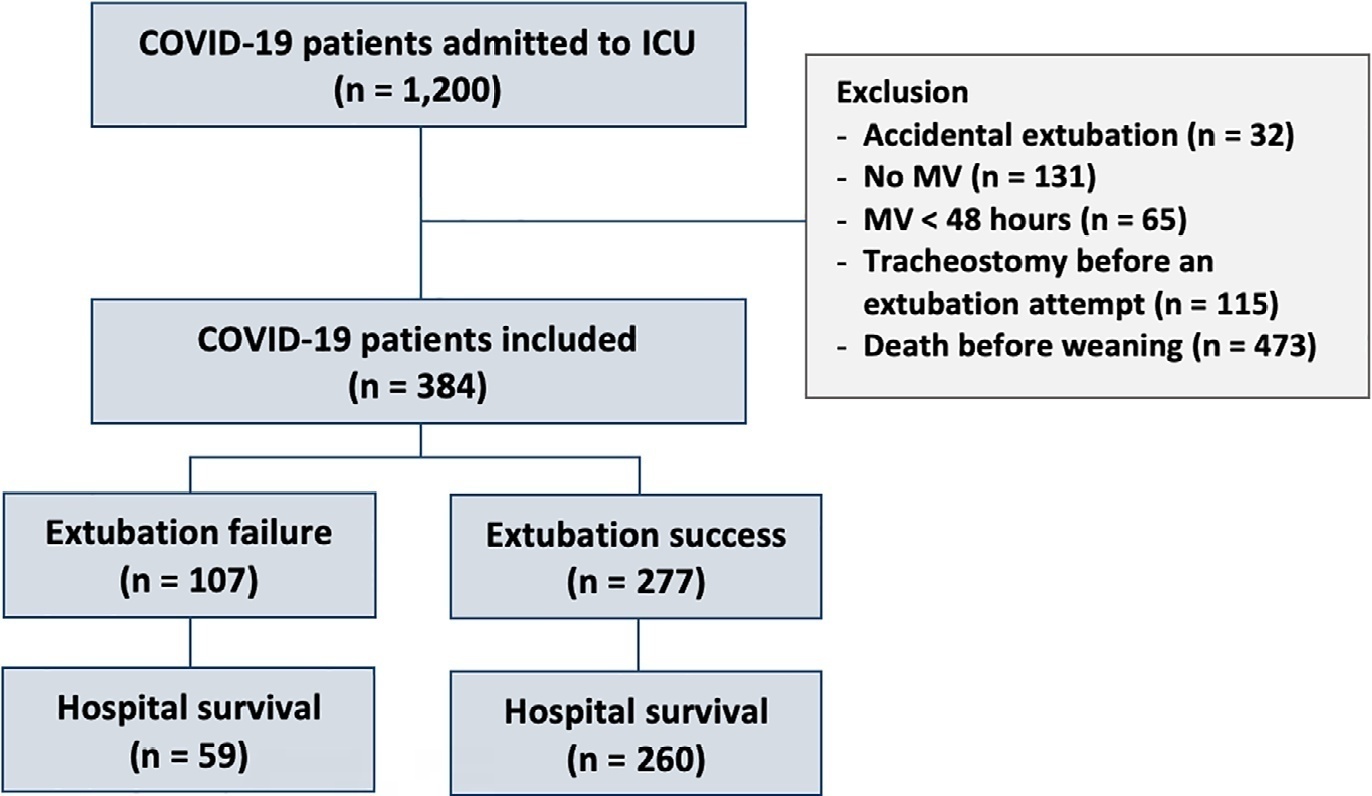
Three hundred eighty-four extubated patients were included. Extubation failure was observed in 107 (27.9%) patients. Forty-seven (12.2%) patients received prophylactic noninvasive ventilation. In 26 (6.8%) patients, early extubation was performed with immediate use of noninvasive ventilation. Noninvasive ventilation for the management of postextubation respiratory failure was administered to 64 (16.7%) patients.
We found that COVID-19 patients had a high rate of extubation failure. Despite the high risk of extubation failure, we observed low use of prophylactic noninvasive ventilation in these patients.
Abstract
Crit Care Sci. 2023;35(2):163-167
DOI 10.5935/2965-2774.20230009-pt
To assess the outcome of extubation in COVID-19 patients and the use of noninvasive ventilation in the weaning process.
This retrospective, observational, single-center study was conducted in COVID-19 patients aged 18 years or older who were admitted to an intensive care unit between April 2020 and December 2021, placed under mechanical ventilation for more than 48 hours and progressed to weaning. Early extubation was defined as extubation without a spontaneous breathing trial and immediate use of noninvasive ventilation after extubation. In patients who underwent a spontaneous breathing trial, noninvasive ventilation could be used as prophylactic ventilatory assistance when started immediately after extubation (prophylactic noninvasive ventilation) or as rescue therapy in cases of postextubation respiratory failure (therapeutic noninvasive ventilation). The primary outcome was extubation failure during the intensive care unit stay.
Three hundred eighty-four extubated patients were included. Extubation failure was observed in 107 (27.9%) patients. Forty-seven (12.2%) patients received prophylactic noninvasive ventilation. In 26 (6.8%) patients, early extubation was performed with immediate use of noninvasive ventilation. Noninvasive ventilation for the management of postextubation respiratory failure was administered to 64 (16.7%) patients.
We found that COVID-19 patients had a high rate of extubation failure. Despite the high risk of extubation failure, we observed low use of prophylactic noninvasive ventilation in these patients.
Abstract
Crit Care Sci. 2023;35(1):19-30
DOI 10.5935/2965-2774.20230203-pt
To evaluate the factors associated with mortality in mechanically ventilated patients with acute respiratory distress syndrome due to COVID-19.
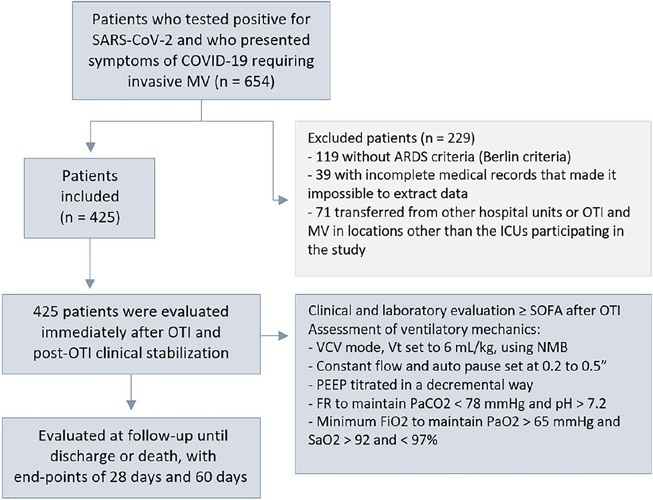
This was a retrospective, multicenter cohort study that included 425 mechanically ventilated adult patients with COVID-19 admitted to 4 intensive care units. Clinical data comprising the SOFA score, laboratory data and mechanical characteristics of the respiratory system were collected in a standardized way immediately after the start of invasive mechanical ventilation. The risk factors for death were analyzed using Cox regression to estimate the risk ratios and their respective 95%CIs.
Body mass index (RR 1.17; 95%CI 1.11 - 1.20; p < 0.001), SOFA score (RR 1.39; 95%CI 1.31 - 1.49; p < 0.001) and driving pressure (RR 1.24; 95%CI 1.21 - 1.29; p < 0.001) were considered independent factors associated with mortality in mechanically ventilated patients with acute respiratory distress syndrome due to COVID-19. Respiratory system compliance (RR 0.92; 95%CI 0.90 - 0.93; p < 0.001) was associated with lower mortality. The comparative analysis of the survival curves indicated that patients with respiratory system compliance (< 30mL/cmH2O), a higher SOFA score (> 5 points) and higher driving pressure (> 14cmH2O) were more significantly associated with the outcome of death at 28 days and 60 days.
Patients with a body mass index > 32kg/m2, respiratory system compliance < 30mL/cmH2O, driving pressure > 14cmH2O and SOFA score > 5.8 immediately after the initiation of invasive ventilatory support had worse outcomes, and independent risk factors were associated with higher mortality in this population.
Abstract
Crit Care Sci. 2023;35(1):19-30
DOI 10.5935/2965-2774.20230203-pt
To evaluate the factors associated with mortality in mechanically ventilated patients with acute respiratory distress syndrome due to COVID-19.
This was a retrospective, multicenter cohort study that included 425 mechanically ventilated adult patients with COVID-19 admitted to 4 intensive care units. Clinical data comprising the SOFA score, laboratory data and mechanical characteristics of the respiratory system were collected in a standardized way immediately after the start of invasive mechanical ventilation. The risk factors for death were analyzed using Cox regression to estimate the risk ratios and their respective 95%CIs.
Body mass index (RR 1.17; 95%CI 1.11 - 1.20; p < 0.001), SOFA score (RR 1.39; 95%CI 1.31 - 1.49; p < 0.001) and driving pressure (RR 1.24; 95%CI 1.21 - 1.29; p < 0.001) were considered independent factors associated with mortality in mechanically ventilated patients with acute respiratory distress syndrome due to COVID-19. Respiratory system compliance (RR 0.92; 95%CI 0.90 - 0.93; p < 0.001) was associated with lower mortality. The comparative analysis of the survival curves indicated that patients with respiratory system compliance (< 30mL/cmH2O), a higher SOFA score (> 5 points) and higher driving pressure (> 14cmH2O) were more significantly associated with the outcome of death at 28 days and 60 days.
Patients with a body mass index > 32kg/m2, respiratory system compliance < 30mL/cmH2O, driving pressure > 14cmH2O and SOFA score > 5.8 immediately after the initiation of invasive ventilatory support had worse outcomes, and independent risk factors were associated with higher mortality in this population.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):426-432
DOI 10.5935/0103-507X.20220278-en
To characterize the knowledge and perceived attitudes toward pharmacologic interventions for light sedation in mechanically ventilated patients and to understand the current gaps comparing current practice with the recommendations of the Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the Intensive Care Unit.
This was a cross-sectional cohort study based on the application of an electronic questionnaire focused on sedation practices.
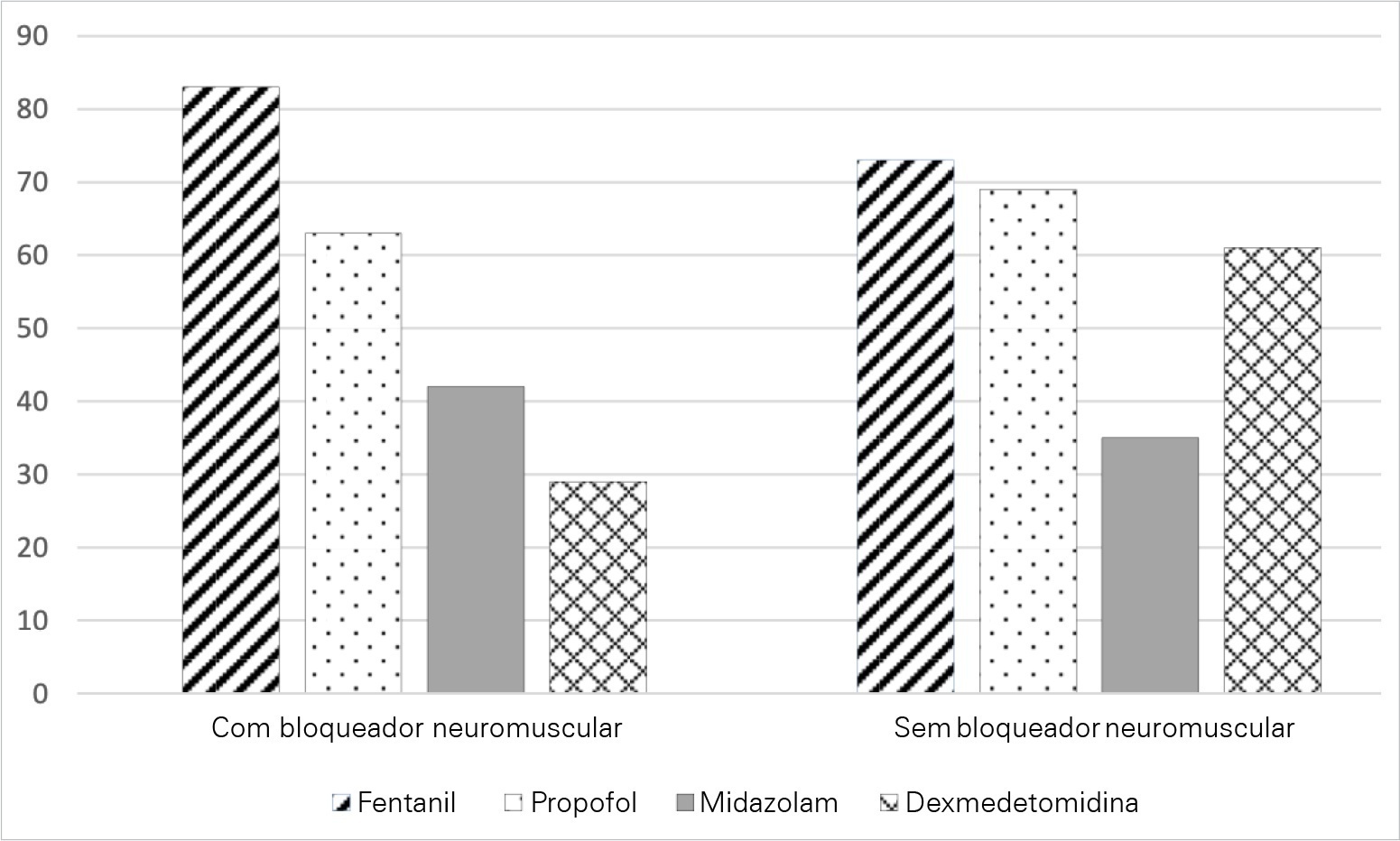
A total of 303 critical care physicians provided responses to the survey. Most respondents reported routine use of a structured sedation scale (281; 92.6%). Almost half of the respondents reported performing daily interruptions of sedation (147; 48.4%), and the same percentage of participants (48.0%) agreed that patients are often over sedated. During the COVID-19 pandemic, participants reported that patients had a higher chance of receiving midazolam compared to before the pandemic (178; 58.8% versus 106; 34.0%; p = 0.05), and heavy sedation was more common during the COVID-19 pandemic (241; 79.4% versus 148; 49.0%; p = 0.01).
This survey provides valuable data on the perceived attitudes of Brazilian intensive care physicians regarding sedation. Although daily interruption of sedation was a well-known concept and sedation scales were often used by the respondents, insufficient effort was put into frequent monitoring, use of protocols and systematic implementation of sedation strategies. Despite the perception of the benefits linked with light sedation, there is a need to identify improvement targets to propose educational strategies to improve current practices.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):426-432
DOI 10.5935/0103-507X.20220278-en
To characterize the knowledge and perceived attitudes toward pharmacologic interventions for light sedation in mechanically ventilated patients and to understand the current gaps comparing current practice with the recommendations of the Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the Intensive Care Unit.
This was a cross-sectional cohort study based on the application of an electronic questionnaire focused on sedation practices.
A total of 303 critical care physicians provided responses to the survey. Most respondents reported routine use of a structured sedation scale (281; 92.6%). Almost half of the respondents reported performing daily interruptions of sedation (147; 48.4%), and the same percentage of participants (48.0%) agreed that patients are often over sedated. During the COVID-19 pandemic, participants reported that patients had a higher chance of receiving midazolam compared to before the pandemic (178; 58.8% versus 106; 34.0%; p = 0.05), and heavy sedation was more common during the COVID-19 pandemic (241; 79.4% versus 148; 49.0%; p = 0.01).
This survey provides valuable data on the perceived attitudes of Brazilian intensive care physicians regarding sedation. Although daily interruption of sedation was a well-known concept and sedation scales were often used by the respondents, insufficient effort was put into frequent monitoring, use of protocols and systematic implementation of sedation strategies. Despite the perception of the benefits linked with light sedation, there is a need to identify improvement targets to propose educational strategies to improve current practices.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):212-219
DOI 10.5935/0103-507X.20220018-en
To analyze the influence of mechanical power and its components on mechanical ventilation for patients infected with SARS-CoV-2; identify the values of the mechanical ventilation components and verify their correlations with each other and with the mechanical power and effects on the result of the Gattinoni-S and Giosa formulas.
This was an observational, longitudinal, analytical and quantitative study of respirator and mechanical power parameters in patients with SARS-CoV-2.
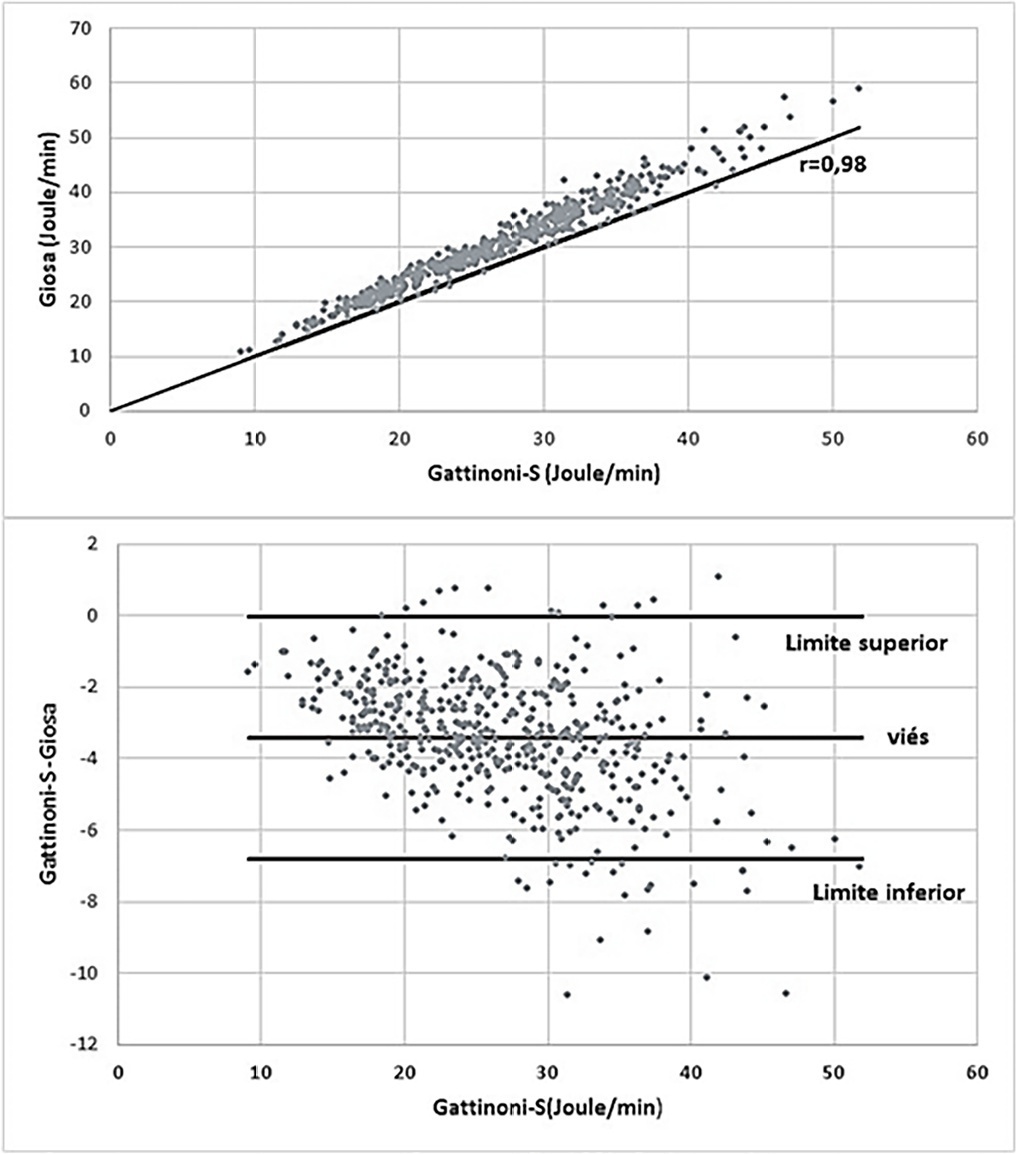
The mean mechanical power was 26.9J/minute (Gattinoni-S) and 30.3 J/minute (Giosa). The driving pressure was 14.4cmH2O, the plateau pressure was 26.5cmH2O, the positive end-expiratory pressure was 12.1cmH2O, the elastance was 40.6cmH2O/L, the tidal volume was 0.36L, and the respiratory rate was 32 breaths/minute. The correlation between the Gattinoni and Giosa formulas was 0.98, with a bias of -3.4J/minute and a difference in the correlation of the resistance pressure of 0.39 (Gattinoni) and 0.24 (Giosa). Among the components, the correlations between elastance and driving pressure (0.88), positive end-expiratory pressure (-0.54) and tidal volume (-0.44) stood out.
In the analysis of mechanical ventilation for patients with SARS-CoV-2, it was found that the correlations of its components with mechanical power influenced its high momentary values and and that the correlations of its components with each other influenced their behavior throughout the study period. Because they have specific effects on the Gatinnoni-S and Giosa formulas, the mechanical ventilation components influenced their calculations and caused divergence in the mechanical power values.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):212-219
DOI 10.5935/0103-507X.20220018-en
To analyze the influence of mechanical power and its components on mechanical ventilation for patients infected with SARS-CoV-2; identify the values of the mechanical ventilation components and verify their correlations with each other and with the mechanical power and effects on the result of the Gattinoni-S and Giosa formulas.
This was an observational, longitudinal, analytical and quantitative study of respirator and mechanical power parameters in patients with SARS-CoV-2.
The mean mechanical power was 26.9J/minute (Gattinoni-S) and 30.3 J/minute (Giosa). The driving pressure was 14.4cmH2O, the plateau pressure was 26.5cmH2O, the positive end-expiratory pressure was 12.1cmH2O, the elastance was 40.6cmH2O/L, the tidal volume was 0.36L, and the respiratory rate was 32 breaths/minute. The correlation between the Gattinoni and Giosa formulas was 0.98, with a bias of -3.4J/minute and a difference in the correlation of the resistance pressure of 0.39 (Gattinoni) and 0.24 (Giosa). Among the components, the correlations between elastance and driving pressure (0.88), positive end-expiratory pressure (-0.54) and tidal volume (-0.44) stood out.
In the analysis of mechanical ventilation for patients with SARS-CoV-2, it was found that the correlations of its components with mechanical power influenced its high momentary values and and that the correlations of its components with each other influenced their behavior throughout the study period. Because they have specific effects on the Gatinnoni-S and Giosa formulas, the mechanical ventilation components influenced their calculations and caused divergence in the mechanical power values.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)