
You searched for:"Wagner Luís Nedel"
We found (8) results for your search.-
Correspondence
Reply to: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
- Fernando Nataniel Vieira
 ,
, - Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho , [ … ],
- Bruna Ziegler
Abstract
CorrespondenceReply to: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
Crit Care Sci. 2024;36:e20240012en
DOI 10.62675/2965-2774.20240012-en
- Fernando Nataniel Vieira ,
- Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho ,
- Fabiana de Oliveira Chaise,
- Jaqueline da Silva Fink ,
- Wagner Luis Nedel ,
- Bruna Ziegler
Views24Dear editor, We appreciate the interesting and thoughtful critique provided by Finsterer et al. in the letter to the editor regarding our article titled “Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit”.() We would like to address the raised concerns and provide additional clarification […]See moreViews24

Abstract
CorrespondenceReply to: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
Crit Care Sci. 2024;36:e20240012en
DOI 10.62675/2965-2774.20240012-en
- Fernando Nataniel Vieira ,
- Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho ,
- Fabiana de Oliveira Chaise,
- Jaqueline da Silva Fink ,
- Wagner Luis Nedel ,
- Bruna Ziegler
Views24Dear editor, We appreciate the interesting and thoughtful critique provided by Finsterer et al. in the letter to the editor regarding our article titled “Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit”.() We would like to address the raised concerns and provide additional clarification […]See more - Fernando Nataniel Vieira
-
Letter to the Editor
Outcomes of critically ill pregnant COVID-19 patients: a cohort study
- Pedro Henrique Rigotti Soares ,
- Cesar Antônio Sebben Filho,
- Rafaela Doebber Escobar ,
- Leonardo Bianchet Botega,
- Laura Rodolpho Petry , [ … ],
- Wagner Luís Nedel
Abstract
Letter to the EditorOutcomes of critically ill pregnant COVID-19 patients: a cohort study
Crit Care Sci. 2023;35(4):411-412
DOI 10.5935/2965-2774.20230222-pt
- Pedro Henrique Rigotti Soares ,
- Cesar Antônio Sebben Filho,
- Rafaela Doebber Escobar ,
- Leonardo Bianchet Botega,
- Laura Rodolpho Petry ,
- Wagner Luís Nedel
Views8To the editor,Information related to coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), in pregnant women is scarce and limited. Increased oxygen consumption, a reduction in chest wall compliance, and decreased functional residual capacity can exacerbate respiratory distress and may lead to the development of acute respiratory distress syndrome (ARDS).() […]See moreViews8Abstract
Letter to the EditorOutcomes of critically ill pregnant COVID-19 patients: a cohort study
Crit Care Sci. 2023;35(4):411-412
DOI 10.5935/2965-2774.20230222-pt
- Pedro Henrique Rigotti Soares ,
- Cesar Antônio Sebben Filho,
- Rafaela Doebber Escobar ,
- Leonardo Bianchet Botega,
- Laura Rodolpho Petry ,
- Wagner Luís Nedel
Views8To the editor,Information related to coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), in pregnant women is scarce and limited. Increased oxygen consumption, a reduction in chest wall compliance, and decreased functional residual capacity can exacerbate respiratory distress and may lead to the development of acute respiratory distress syndrome (ARDS).() […]See more - Pedro Henrique Rigotti Soares
-
Original Article
Extubation failure and the use of noninvasive ventilation during the weaning process in critically ill COVID-19 patients
- Viviane Martins Corrêa Boniatti ,
- Chaiane Ribeiro Pereira ,
- Gabriela Machado Costa ,
- Michelle Carneiro Teixeira ,
- Alessandra Preisig Werlang , [ … ],
- Márcio Manozzo Boniatti
Abstract
Original ArticleExtubation failure and the use of noninvasive ventilation during the weaning process in critically ill COVID-19 patients
Crit Care Sci. 2023;35(2):163-167
DOI 10.5935/2965-2774.20230009-pt
- Viviane Martins Corrêa Boniatti ,
- Chaiane Ribeiro Pereira ,
- Gabriela Machado Costa ,
- Michelle Carneiro Teixeira ,
- Alessandra Preisig Werlang ,
- Francielle Thaisa Morais Martins ,
- Leonardo da Silva Marques ,
- Wagner Luís Nedel ,
- Márcio Manozzo Boniatti
Views7ABSTRACT
Objective:
To assess the outcome of extubation in COVID-19 patients and the use of noninvasive ventilation in the weaning process.
Methods:
This retrospective, observational, single-center study was conducted in COVID-19 patients aged 18 years or older who were admitted to an intensive care unit between April 2020 and December 2021, placed under mechanical ventilation for more than 48 hours and progressed to weaning. Early extubation was defined as extubation without a spontaneous breathing trial and immediate use of noninvasive ventilation after extubation. In patients who underwent a spontaneous breathing trial, noninvasive ventilation could be used as prophylactic ventilatory assistance when started immediately after extubation (prophylactic noninvasive ventilation) or as rescue therapy in cases of postextubation respiratory failure (therapeutic noninvasive ventilation). The primary outcome was extubation failure during the intensive care unit stay.
Results:
Three hundred eighty-four extubated patients were included. Extubation failure was observed in 107 (27.9%) patients. Forty-seven (12.2%) patients received prophylactic noninvasive ventilation. In 26 (6.8%) patients, early extubation was performed with immediate use of noninvasive ventilation. Noninvasive ventilation for the management of postextubation respiratory failure was administered to 64 (16.7%) patients.
Conclusion:
We found that COVID-19 patients had a high rate of extubation failure. Despite the high risk of extubation failure, we observed low use of prophylactic noninvasive ventilation in these patients.
Keywords:Airway extubationartificialCoronavirus infectionsCOVID-19Noninvasive ventilationRespirationSARS-CoV-2Ventilator weaningSee moreViews7Abstract
Original ArticleExtubation failure and the use of noninvasive ventilation during the weaning process in critically ill COVID-19 patients
Crit Care Sci. 2023;35(2):163-167
DOI 10.5935/2965-2774.20230009-pt
- Viviane Martins Corrêa Boniatti ,
- Chaiane Ribeiro Pereira ,
- Gabriela Machado Costa ,
- Michelle Carneiro Teixeira ,
- Alessandra Preisig Werlang ,
- Francielle Thaisa Morais Martins ,
- Leonardo da Silva Marques ,
- Wagner Luís Nedel ,
- Márcio Manozzo Boniatti
Views7ABSTRACT
Objective:
To assess the outcome of extubation in COVID-19 patients and the use of noninvasive ventilation in the weaning process.
Methods:
This retrospective, observational, single-center study was conducted in COVID-19 patients aged 18 years or older who were admitted to an intensive care unit between April 2020 and December 2021, placed under mechanical ventilation for more than 48 hours and progressed to weaning. Early extubation was defined as extubation without a spontaneous breathing trial and immediate use of noninvasive ventilation after extubation. In patients who underwent a spontaneous breathing trial, noninvasive ventilation could be used as prophylactic ventilatory assistance when started immediately after extubation (prophylactic noninvasive ventilation) or as rescue therapy in cases of postextubation respiratory failure (therapeutic noninvasive ventilation). The primary outcome was extubation failure during the intensive care unit stay.
Results:
Three hundred eighty-four extubated patients were included. Extubation failure was observed in 107 (27.9%) patients. Forty-seven (12.2%) patients received prophylactic noninvasive ventilation. In 26 (6.8%) patients, early extubation was performed with immediate use of noninvasive ventilation. Noninvasive ventilation for the management of postextubation respiratory failure was administered to 64 (16.7%) patients.
Conclusion:
We found that COVID-19 patients had a high rate of extubation failure. Despite the high risk of extubation failure, we observed low use of prophylactic noninvasive ventilation in these patients.
Keywords:Airway extubationartificialCoronavirus infectionsCOVID-19Noninvasive ventilationRespirationSARS-CoV-2Ventilator weaningSee more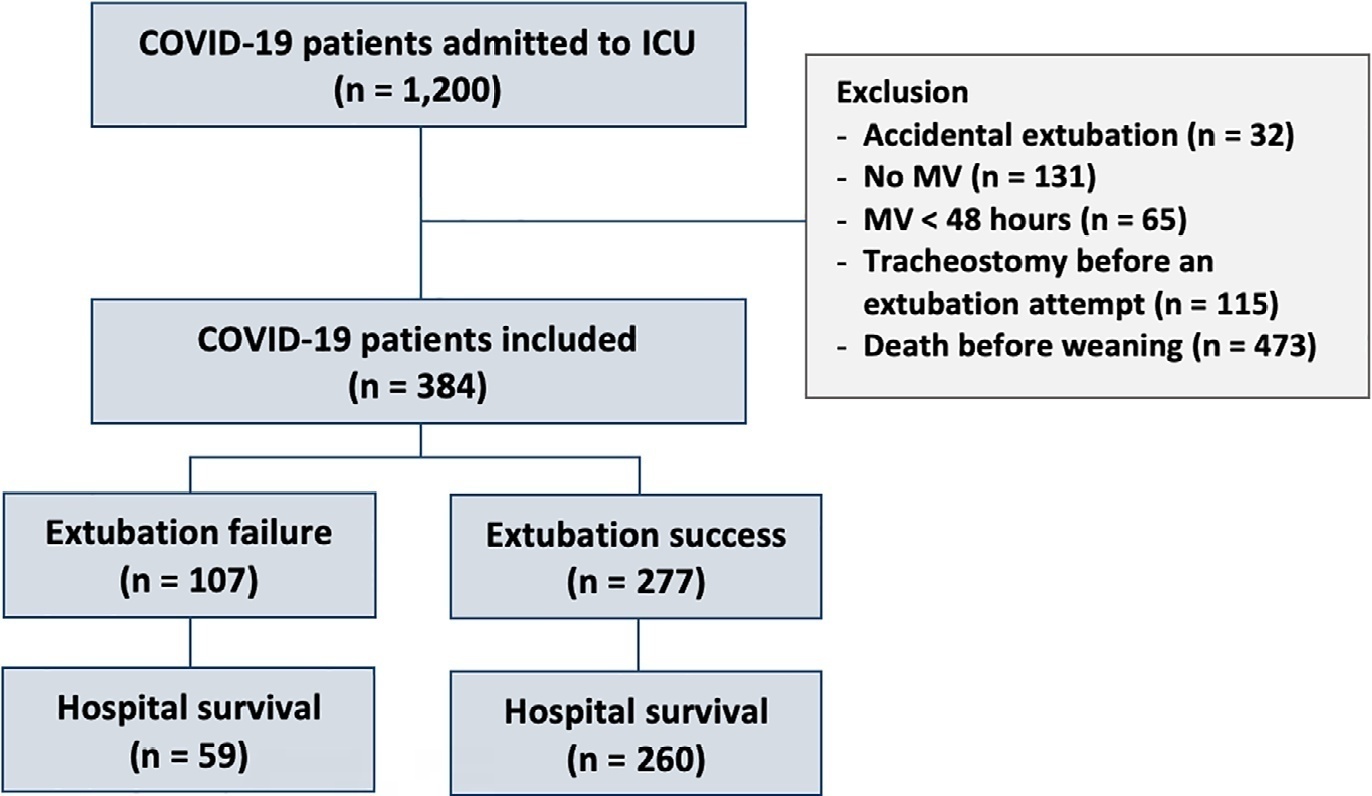
- Viviane Martins Corrêa Boniatti
-
Original Article
Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
- Fernando Nataniel Vieira ,
- Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho , [ … ],
- Bruna Ziegler
Abstract
Original ArticleAssociation between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
Rev Bras Ter Intensiva. 2022;34(4):452-460
DOI 10.5935/0103-507X.20220087-en
- Fernando Nataniel Vieira ,
- Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho ,
- Fabiana de Oliveira Chaise,
- Jaqueline da Silva Fink ,
- Wagner Luis Nedel ,
- Bruna Ziegler
Views4See moreABSTRACT
Objective:
To verify the relationship between the rectus femoris cross-sectional area and diaphragmatic excursion with successful weaning from mechanical ventilation in chronic critically tracheostomized patients.
Methods:
This was a prospective observational cohort study. We included chronic critically ill patients (those who underwent tracheostomy placement after 10 days under mechanical ventilation). The rectus femoris cross-sectional area and diaphragmatic excursion were obtained by ultrasonography performed within the first 48 hours after tracheostomy. We measured rectus femoris cross-sectional area and diaphragmatic excursion to assess their association with weaning from mechanical ventilation, including their potential to predict successful weaning and survival throughout the intensive care unit stay.
Results:
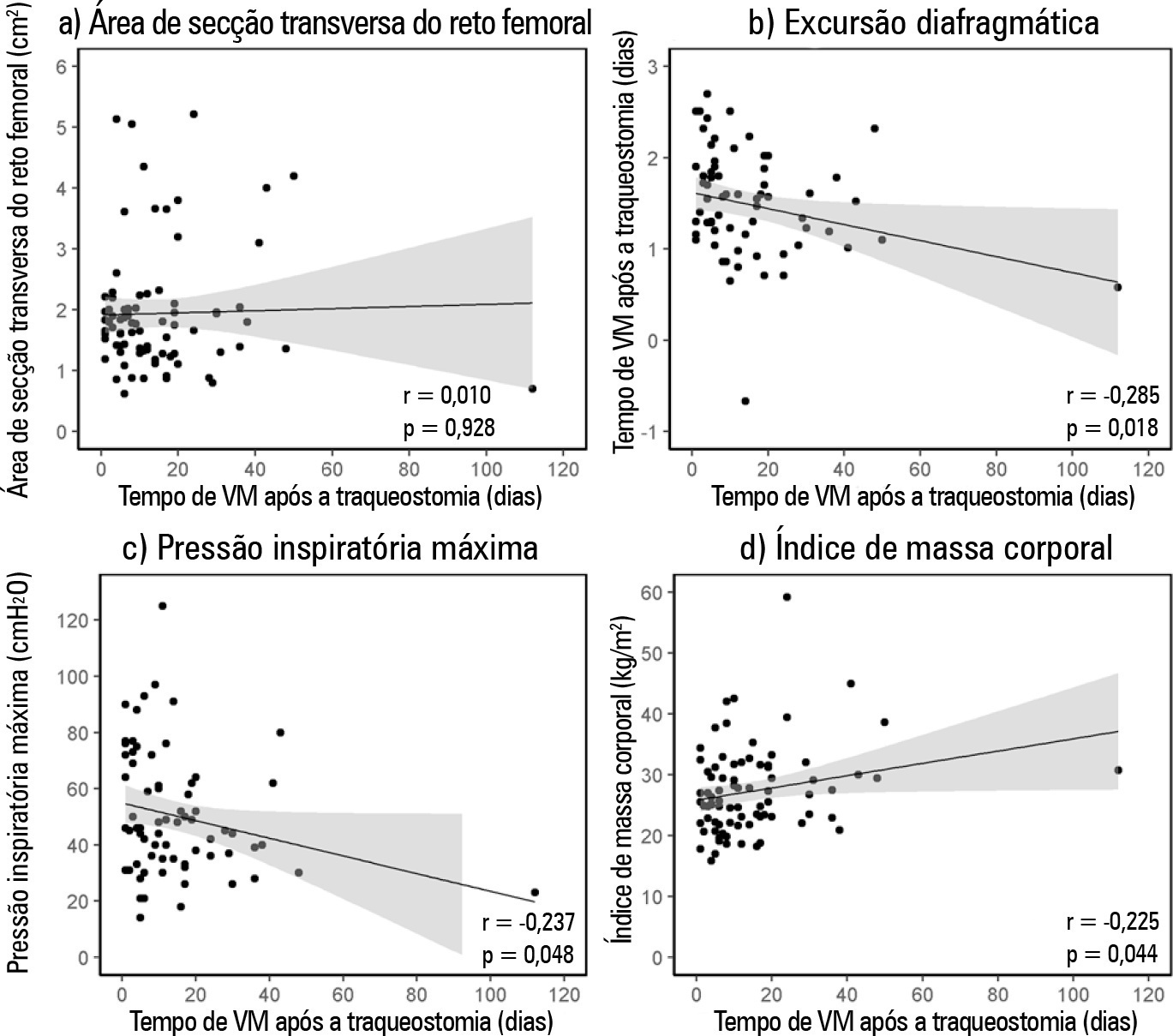
Eighty-one patients were included. Forty-five patients (55%) were weaned from mechanical ventilation. The mortality rates were 42% and 61.7% in the intensive care unit and hospital, respectively. The fail group in relation to the success group at weaning presented a lower rectus femoris cross-sectional area (1.4 [0.8] versus 1.84 [0.76]cm2, p = 0.014) and lower diaphragmatic excursion (1.29 ± 0.62 versus 1.62 ± 0.51cm, p = 0.019). When rectus femoris cross-sectional area ≥ 1.80cm2 and diaphragmatic excursion ≥ 1.25cm was a combined condition, it had a strong association with successful weaning (adjusted OR = 20.81, 95%CI 2.38 – 182.28; p = 0.006) but not with intensive care unit survival (adjusted OR = 0.19, 95%CI 0.03 – 1.08; p = 0.061).
Conclusion:
Successful weaning from mechanical ventilation in chronic critically ill patients was associated with higher measurements of rectus femoris cross-sectional area and diaphragmatic excursion.
Views4Abstract
Original ArticleAssociation between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
Rev Bras Ter Intensiva. 2022;34(4):452-460
DOI 10.5935/0103-507X.20220087-en
- Fernando Nataniel Vieira ,
- Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho ,
- Fabiana de Oliveira Chaise,
- Jaqueline da Silva Fink ,
- Wagner Luis Nedel ,
- Bruna Ziegler
Views4See moreABSTRACT
Objective:
To verify the relationship between the rectus femoris cross-sectional area and diaphragmatic excursion with successful weaning from mechanical ventilation in chronic critically tracheostomized patients.
Methods:
This was a prospective observational cohort study. We included chronic critically ill patients (those who underwent tracheostomy placement after 10 days under mechanical ventilation). The rectus femoris cross-sectional area and diaphragmatic excursion were obtained by ultrasonography performed within the first 48 hours after tracheostomy. We measured rectus femoris cross-sectional area and diaphragmatic excursion to assess their association with weaning from mechanical ventilation, including their potential to predict successful weaning and survival throughout the intensive care unit stay.
Results:
Eighty-one patients were included. Forty-five patients (55%) were weaned from mechanical ventilation. The mortality rates were 42% and 61.7% in the intensive care unit and hospital, respectively. The fail group in relation to the success group at weaning presented a lower rectus femoris cross-sectional area (1.4 [0.8] versus 1.84 [0.76]cm2, p = 0.014) and lower diaphragmatic excursion (1.29 ± 0.62 versus 1.62 ± 0.51cm, p = 0.019). When rectus femoris cross-sectional area ≥ 1.80cm2 and diaphragmatic excursion ≥ 1.25cm was a combined condition, it had a strong association with successful weaning (adjusted OR = 20.81, 95%CI 2.38 – 182.28; p = 0.006) but not with intensive care unit survival (adjusted OR = 0.19, 95%CI 0.03 – 1.08; p = 0.061).
Conclusion:
Successful weaning from mechanical ventilation in chronic critically ill patients was associated with higher measurements of rectus femoris cross-sectional area and diaphragmatic excursion.
- Fernando Nataniel Vieira
-
Original Article
Epidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama, [ … ],
- Suzana Margareth Ajeje Lobo
Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee moreViews1Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee more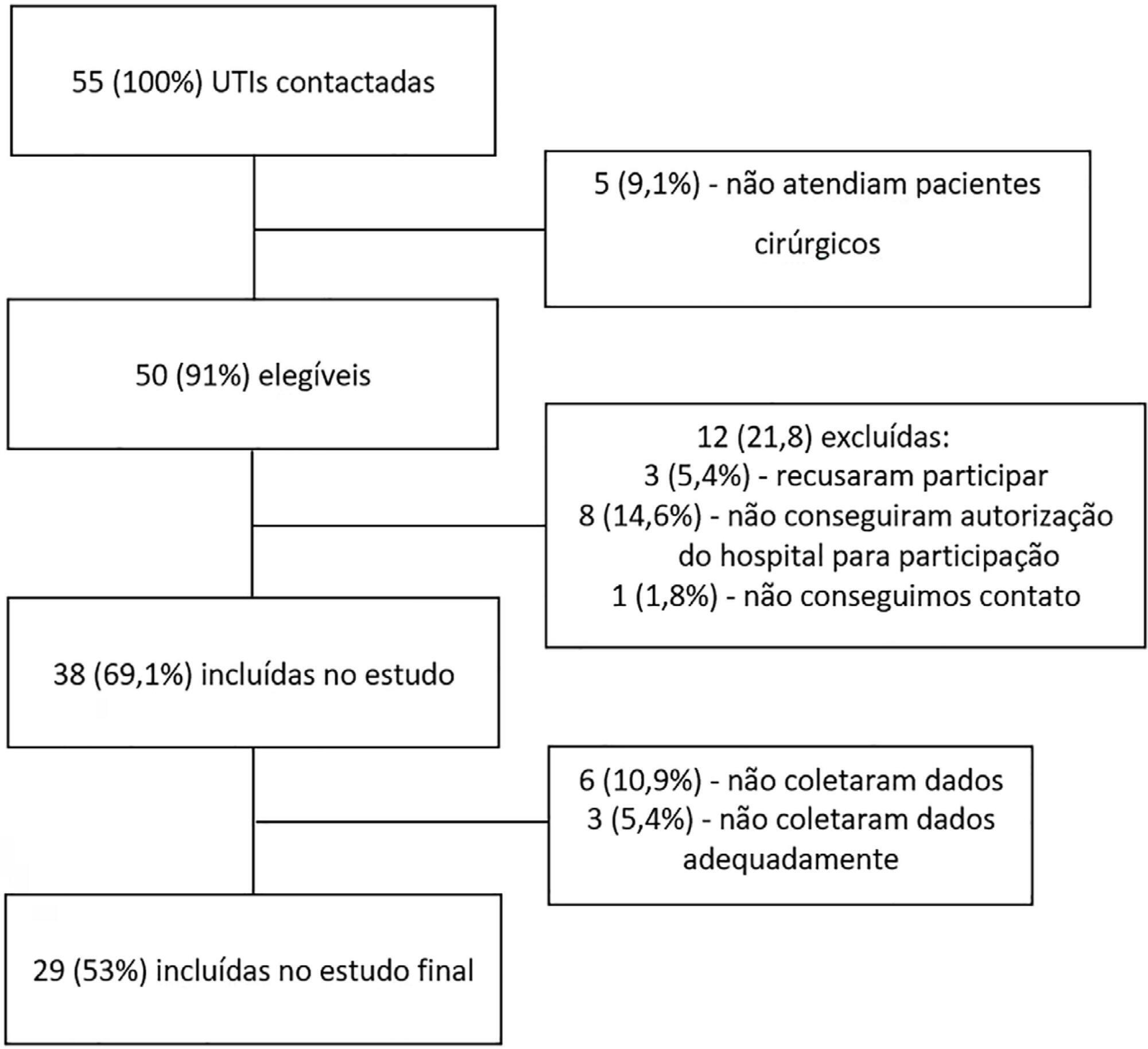
- João Manoel Silva Júnior
-
Letter to the Editor
Variability in the rectus femoris muscle area and its association with clinical outcomes in critically ill patients: a prospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):156-158
Abstract
Letter to the EditorVariability in the rectus femoris muscle area and its association with clinical outcomes in critically ill patients: a prospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):156-158
DOI 10.5935/0103-507X.20200023
Views0To the Editor, Muscle weakness is a common complication in critically ill patients, with loss of muscle mass during hospitalization in the intensive care unit (ICU), which is enhanced by the magnitude of organ failure and is associated with long-term morbidity.(,) Rectus femoris muscle (RFM) ultrasound has emerged as a practical, easily performed and applied […]See moreViews0Abstract
Letter to the EditorVariability in the rectus femoris muscle area and its association with clinical outcomes in critically ill patients: a prospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):156-158
DOI 10.5935/0103-507X.20200023
Views0To the Editor, Muscle weakness is a common complication in critically ill patients, with loss of muscle mass during hospitalization in the intensive care unit (ICU), which is enhanced by the magnitude of organ failure and is associated with long-term morbidity.(,) Rectus femoris muscle (RFM) ultrasound has emerged as a practical, easily performed and applied […]See more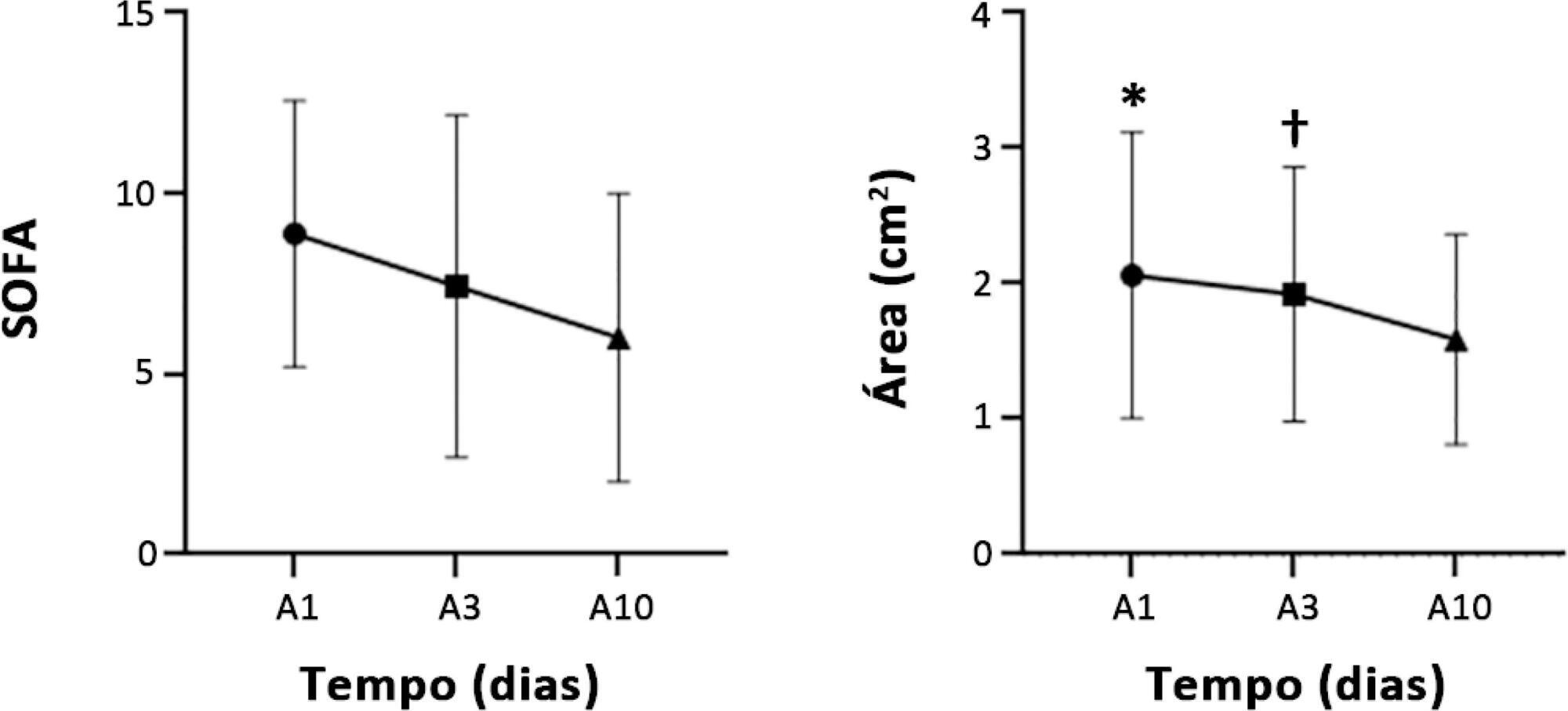
-
Special Articles
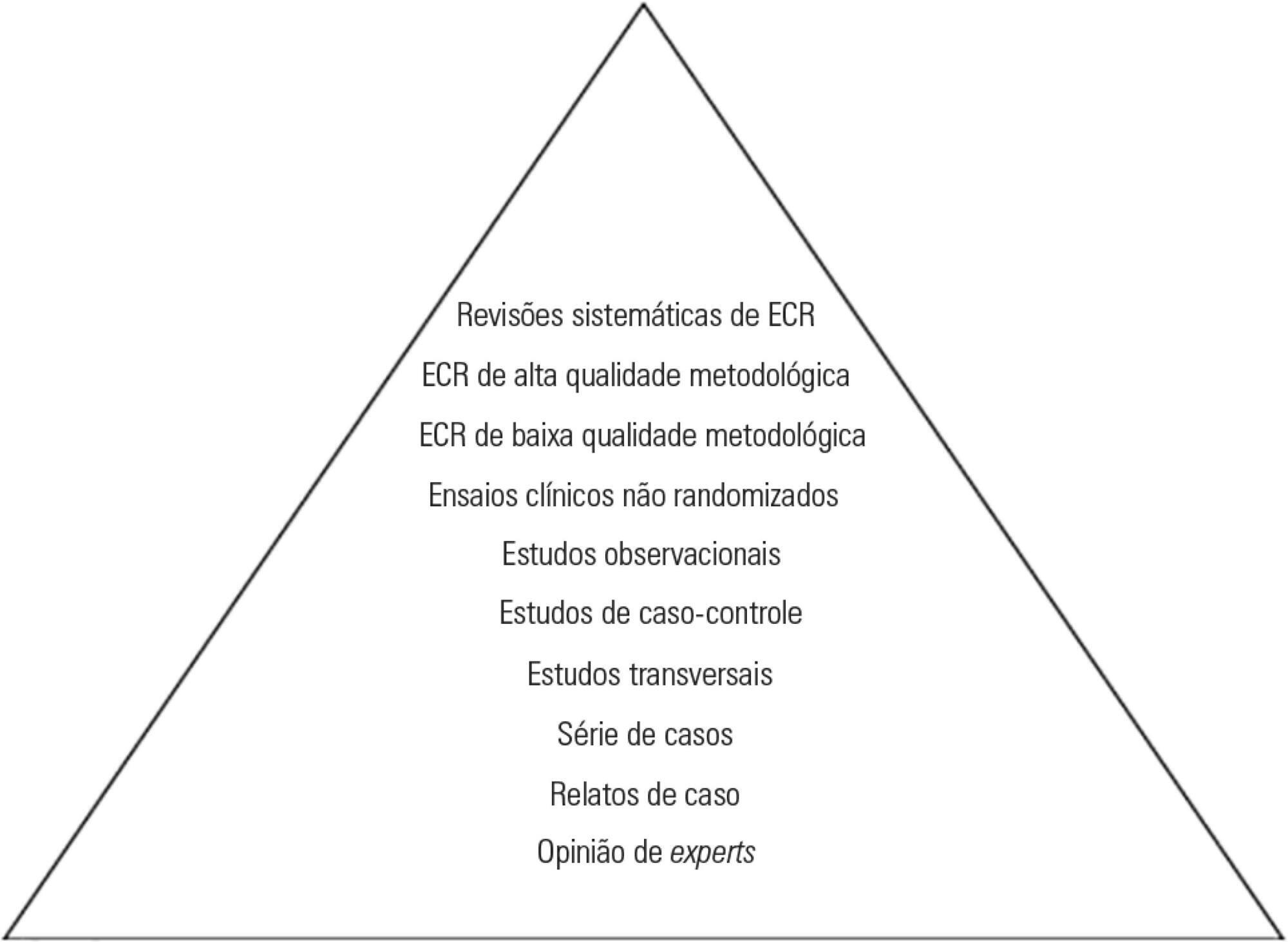
Different research designs and their characteristics in intensive care
Rev Bras Ter Intensiva. 2016;28(3):256-260
Abstract
Special ArticlesDifferent research designs and their characteristics in intensive care
Rev Bras Ter Intensiva. 2016;28(3):256-260
DOI 10.5935/0103-507X.20160050
Views0See moreABSTRACT
Different research designs have various advantages and limitations inherent to their main characteristics. Knowledge of the proper use of each design is of great importance to understanding the applicability of research findings to clinical epidemiology.
In intensive care, a hierarchical classification of designs can often be misleading if the characteristics of the design in this context are not understood. One must therefore be alert to common problems in randomized clinical trials and systematic reviews/meta-analyses that address clinical issues related to the care of the critically ill patient.
Views0Abstract
Special ArticlesDifferent research designs and their characteristics in intensive care
Rev Bras Ter Intensiva. 2016;28(3):256-260
DOI 10.5935/0103-507X.20160050
Views0See moreABSTRACT
Different research designs have various advantages and limitations inherent to their main characteristics. Knowledge of the proper use of each design is of great importance to understanding the applicability of research findings to clinical epidemiology.
In intensive care, a hierarchical classification of designs can often be misleading if the characteristics of the design in this context are not understood. One must therefore be alert to common problems in randomized clinical trials and systematic reviews/meta-analyses that address clinical issues related to the care of the critically ill patient.
-
Original Article
Thrombin activatable fibrinolysis inhibitor as a bleeding predictor in liver transplantation: a pilot observational study
Rev Bras Ter Intensiva. 2016;28(2):161-166
Abstract
Original ArticleThrombin activatable fibrinolysis inhibitor as a bleeding predictor in liver transplantation: a pilot observational study
Rev Bras Ter Intensiva. 2016;28(2):161-166
DOI 10.5935/0103-507X.20160031
Views0See moreABSTRACT
Objective:
To correlate the levels of thrombin activatable fibrinolysis inhibitor in the immediate postoperative period and at 24 hours postoperatively with the volume of intraoperative bleeding.
Methods:
Twenty-one patients allocated immediately before (elective or emergency) liver transplantation were analyzed. Blood samples were collected for thrombin activatable fibrinolysis inhibitor analysis at three different time points: immediately before liver transplantation (preoperative thrombin activatable fibrinolysis inhibitor), immediately after the surgical procedure (immediate postoperative thrombin activatable fibrinolysis inhibitor), and 24 hours after surgery (thrombin activatable fibrinolysis inhibitor 24 hours after surgery). The primary outcome of the study was to correlate the preoperative and immediate postoperative levels of thrombin activatable fibrinolysis inhibitor with intraoperative blood loss.
Results:
There was a correlation between the preoperative thrombin activatable fibrinolysis inhibitor levels and bleeding volume (ρ = -0.469; p = 0.05) but no correlation between the immediate postoperative thrombin activatable fibrinolysis inhibitor and bleeding volume (ρ = -0.062; p = 0.79). No variable included in the linear regression analysis (prehemoglobin, prefibrinogen and preoperative thrombin activatable fibrinolysis inhibitor) was a bleeding predictor. There was a similar trend in the variation between the levels of thrombin activatable fibrinolysis inhibitor at the three different time points and fibrinogen levels. Patients who died within 6 months (14.3%) showed decreased preoperative and immediate postoperative levels of thrombin activatable fibrinolysis compared with survivors (preoperative: 1.3 ± 0.15 versus 2.55 ± 0.53, p = 0.06; immediate postoperative: 1.2 ± 0.15 versus 2.5 ± 0.42, p = 0.007).
Conclusion:
There was a moderate correlation between preoperative thrombin activatable fibrinolysis inhibitor and intraoperative bleeding in liver transplantation patients, although the predictive role of this variable independent of other variables remains uncertain. Preoperative and immediate postoperative thrombin activatable fibrinolysis inhibitor levels may have a role in the survival prognosis of this population; however, this possibility requires confirmation in further studies with larger sample sizes.
Views0Abstract
Original ArticleThrombin activatable fibrinolysis inhibitor as a bleeding predictor in liver transplantation: a pilot observational study
Rev Bras Ter Intensiva. 2016;28(2):161-166
DOI 10.5935/0103-507X.20160031
Views0See moreABSTRACT
Objective:
To correlate the levels of thrombin activatable fibrinolysis inhibitor in the immediate postoperative period and at 24 hours postoperatively with the volume of intraoperative bleeding.
Methods:
Twenty-one patients allocated immediately before (elective or emergency) liver transplantation were analyzed. Blood samples were collected for thrombin activatable fibrinolysis inhibitor analysis at three different time points: immediately before liver transplantation (preoperative thrombin activatable fibrinolysis inhibitor), immediately after the surgical procedure (immediate postoperative thrombin activatable fibrinolysis inhibitor), and 24 hours after surgery (thrombin activatable fibrinolysis inhibitor 24 hours after surgery). The primary outcome of the study was to correlate the preoperative and immediate postoperative levels of thrombin activatable fibrinolysis inhibitor with intraoperative blood loss.
Results:
There was a correlation between the preoperative thrombin activatable fibrinolysis inhibitor levels and bleeding volume (ρ = -0.469; p = 0.05) but no correlation between the immediate postoperative thrombin activatable fibrinolysis inhibitor and bleeding volume (ρ = -0.062; p = 0.79). No variable included in the linear regression analysis (prehemoglobin, prefibrinogen and preoperative thrombin activatable fibrinolysis inhibitor) was a bleeding predictor. There was a similar trend in the variation between the levels of thrombin activatable fibrinolysis inhibitor at the three different time points and fibrinogen levels. Patients who died within 6 months (14.3%) showed decreased preoperative and immediate postoperative levels of thrombin activatable fibrinolysis compared with survivors (preoperative: 1.3 ± 0.15 versus 2.55 ± 0.53, p = 0.06; immediate postoperative: 1.2 ± 0.15 versus 2.5 ± 0.42, p = 0.007).
Conclusion:
There was a moderate correlation between preoperative thrombin activatable fibrinolysis inhibitor and intraoperative bleeding in liver transplantation patients, although the predictive role of this variable independent of other variables remains uncertain. Preoperative and immediate postoperative thrombin activatable fibrinolysis inhibitor levels may have a role in the survival prognosis of this population; however, this possibility requires confirmation in further studies with larger sample sizes.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis