Respiration, artificial Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(4):571-577
DOI 10.5935/0103-507X.20200095
To describe the results from the implementation of a respiratory care and mechanical ventilation protocol on potential lung donors who met the conditions for procurement. The secondary objective is to compare the results with historical data.
This was a retrospective, observational study. It included potential donors suitable for procurement of organs who had brain death and were hospitalized in critical care units of the Autonomous City of Buenos Aires from April 2017 to March 2018. Main variables: number of potential lung donors that reached the objective of procurement, rate of lungs procured, and rate of implanted lungs. Values of p < 0.05 were considered significant.
Thirty potential lung donors were included, and 23 (88.5%; 95%CI 69.8 - 97.6) met the oxygenation objective. Twenty potential lung donors donated organs, of whom eight donated lungs, with which four double lung transplants and eight single lung transplants were performed. Seven of 12 lungs were procured and implanted in the preprotocol period, while all 12 were under the protocol (p = 0.38). The implantation rate was 58.3% (7/12) in the historical control period and 100% (12/12) (p = 0.04) in the study period.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):571-577
DOI 10.5935/0103-507X.20200095
To describe the results from the implementation of a respiratory care and mechanical ventilation protocol on potential lung donors who met the conditions for procurement. The secondary objective is to compare the results with historical data.
This was a retrospective, observational study. It included potential donors suitable for procurement of organs who had brain death and were hospitalized in critical care units of the Autonomous City of Buenos Aires from April 2017 to March 2018. Main variables: number of potential lung donors that reached the objective of procurement, rate of lungs procured, and rate of implanted lungs. Values of p < 0.05 were considered significant.
Thirty potential lung donors were included, and 23 (88.5%; 95%CI 69.8 - 97.6) met the oxygenation objective. Twenty potential lung donors donated organs, of whom eight donated lungs, with which four double lung transplants and eight single lung transplants were performed. Seven of 12 lungs were procured and implanted in the preprotocol period, while all 12 were under the protocol (p = 0.38). The implantation rate was 58.3% (7/12) in the historical control period and 100% (12/12) (p = 0.04) in the study period.

Abstract
Rev Bras Ter Intensiva. 2020;32(4):487-492
DOI 10.5935/0103-507X.20200082
This study aims to describe the clinical characteristics and predictors of mechanical ventilation of adult inpatients with COVID-19 in a single center.
A retrospective cohort study was performed and included adult inpatients hospitalized from March 17th to May 3rd, 2020, who were diagnosed with SARS-CoV-2 infection. Clinical and demographic characteristics were extracted from electronic medical records.
Overall, 88 consecutive patients were included in this study. The median age of the patients was 63 years (IQR 49 - 71); 59 (67%) were male, 65 (86%) had a college degree and 67 (76%) had at least one comorbidity. Twenty-nine (33%) patients were admitted to the intensive care unit, 18 (20%) patients needed mechanical ventilation, and 9 (10.2%) died during hospitalization. The median length of stay in the intensive care unit and the median duration of mechanical ventilation was 23 and 29.5 days, respectively. An age ≥ 65 years was an independent risk factor for mechanical ventilation (OR 8.4 95%CI 1.3 - 55.6 p = 0.02).
Our findings describe the first wave of Brazilian patients hospitalized for COVID-19. Age was the strongest predictor of respiratory insufficiency and the need for mechanical ventilation in our population.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):487-492
DOI 10.5935/0103-507X.20200082
This study aims to describe the clinical characteristics and predictors of mechanical ventilation of adult inpatients with COVID-19 in a single center.
A retrospective cohort study was performed and included adult inpatients hospitalized from March 17th to May 3rd, 2020, who were diagnosed with SARS-CoV-2 infection. Clinical and demographic characteristics were extracted from electronic medical records.
Overall, 88 consecutive patients were included in this study. The median age of the patients was 63 years (IQR 49 - 71); 59 (67%) were male, 65 (86%) had a college degree and 67 (76%) had at least one comorbidity. Twenty-nine (33%) patients were admitted to the intensive care unit, 18 (20%) patients needed mechanical ventilation, and 9 (10.2%) died during hospitalization. The median length of stay in the intensive care unit and the median duration of mechanical ventilation was 23 and 29.5 days, respectively. An age ≥ 65 years was an independent risk factor for mechanical ventilation (OR 8.4 95%CI 1.3 - 55.6 p = 0.02).
Our findings describe the first wave of Brazilian patients hospitalized for COVID-19. Age was the strongest predictor of respiratory insufficiency and the need for mechanical ventilation in our population.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):444-457
DOI 10.5935/0103-507X.20200075
The COVID-19 pandemic has brought concerns to managers, healthcare professionals, and the general population related to the potential mechanical ventilators’ shortage for severely ill patients. In Brazil, there are several initiatives aimed at producing alternative ventilators to cover this gap. To assist the teams that work in these initiatives, we provide a discussion of some basic concepts on physiology and respiratory mechanics, commonly used mechanical ventilation terms, the differences between triggering and cycling, the basic ventilation modes and other relevant aspects, such as mechanisms of ventilator-induced lung injury, respiratory drive, airway heating and humidification, cross-contamination risks, and aerosol dissemination. After the prototype development phase, preclinical bench-tests and animal model trials are needed to determine the safety and performance of the ventilator, following the minimum technical requirements. Next, it is mandatory going through the regulatory procedures as required by the Brazilian Health Regulatory Agency (Agência Nacional de Vigilância Sanitária - ANVISA). The manufacturing company should be appropriately registered by ANVISA, which also must be notified about the conduction of clinical trials, following the research protocol approval by the Research Ethics Committee. The registration requisition of the ventilator with ANVISA should include a dossier containing the information described in this paper, which is not intended to cover all related matters but to provide guidance on the required procedures.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):444-457
DOI 10.5935/0103-507X.20200075
The COVID-19 pandemic has brought concerns to managers, healthcare professionals, and the general population related to the potential mechanical ventilators’ shortage for severely ill patients. In Brazil, there are several initiatives aimed at producing alternative ventilators to cover this gap. To assist the teams that work in these initiatives, we provide a discussion of some basic concepts on physiology and respiratory mechanics, commonly used mechanical ventilation terms, the differences between triggering and cycling, the basic ventilation modes and other relevant aspects, such as mechanisms of ventilator-induced lung injury, respiratory drive, airway heating and humidification, cross-contamination risks, and aerosol dissemination. After the prototype development phase, preclinical bench-tests and animal model trials are needed to determine the safety and performance of the ventilator, following the minimum technical requirements. Next, it is mandatory going through the regulatory procedures as required by the Brazilian Health Regulatory Agency (Agência Nacional de Vigilância Sanitária - ANVISA). The manufacturing company should be appropriately registered by ANVISA, which also must be notified about the conduction of clinical trials, following the research protocol approval by the Research Ethics Committee. The registration requisition of the ventilator with ANVISA should include a dossier containing the information described in this paper, which is not intended to cover all related matters but to provide guidance on the required procedures.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):348-353
DOI 10.5935/0103-507X.20200062
A novel coronavirus emerged this year as a cause of viral pneumonia. The main characteristics of the virus are rapid transmission, high contagion capacity and potential severity. The objective of this case series study is to describe the clinical characteristics of patients with confirmed coronavirus disease (COVID-19) admitted to different intensive care units in Argentina for mechanical ventilation.
A descriptive, prospective, multicenter case series study was conducted between April 1 and May 8, 2020. Data from patients older than 18 years who were admitted to the intensive care unit for mechanical ventilation for acute respiratory failure with a positive diagnosis of COVID-19 were included.
The variables for 47 patients from 31 intensive care units were recorded: 78.7% were men (median age of 61 years), with a SAPS II score of 43 and a Charlson index score of 3. The initial ventilatory mode was volume control - continuous mandatory ventilation with a tidal volume less than 8mL/kg in 100% of cases, with a median positive end-expiratory pressure of 10.5cmH2O. At the end of the study, 29 patients died, 8 were discharged, and 10 remained hospitalized. The SAPS II score was higher among patients who died (p = 0.046). Charlson comorbidity index was associated with higher mortality (OR = 2.27, 95% CI 1.13 - 4.55, p = 0.02).
Patients with COVID-19 and on mechanical ventilation in this series presented clinical variables similar to those described to date in other international reports. Our findings provide data that may predict outcomes.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):348-353
DOI 10.5935/0103-507X.20200062
A novel coronavirus emerged this year as a cause of viral pneumonia. The main characteristics of the virus are rapid transmission, high contagion capacity and potential severity. The objective of this case series study is to describe the clinical characteristics of patients with confirmed coronavirus disease (COVID-19) admitted to different intensive care units in Argentina for mechanical ventilation.
A descriptive, prospective, multicenter case series study was conducted between April 1 and May 8, 2020. Data from patients older than 18 years who were admitted to the intensive care unit for mechanical ventilation for acute respiratory failure with a positive diagnosis of COVID-19 were included.
The variables for 47 patients from 31 intensive care units were recorded: 78.7% were men (median age of 61 years), with a SAPS II score of 43 and a Charlson index score of 3. The initial ventilatory mode was volume control - continuous mandatory ventilation with a tidal volume less than 8mL/kg in 100% of cases, with a median positive end-expiratory pressure of 10.5cmH2O. At the end of the study, 29 patients died, 8 were discharged, and 10 remained hospitalized. The SAPS II score was higher among patients who died (p = 0.046). Charlson comorbidity index was associated with higher mortality (OR = 2.27, 95% CI 1.13 - 4.55, p = 0.02).
Patients with COVID-19 and on mechanical ventilation in this series presented clinical variables similar to those described to date in other international reports. Our findings provide data that may predict outcomes.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):398-404
DOI 10.5935/0103-507X.20200068
To evaluate the intra- and interexaminer reproducibility of measurements of the resistance and static and dynamic compliance of the respiratory system in patients on mechanical ventilation.
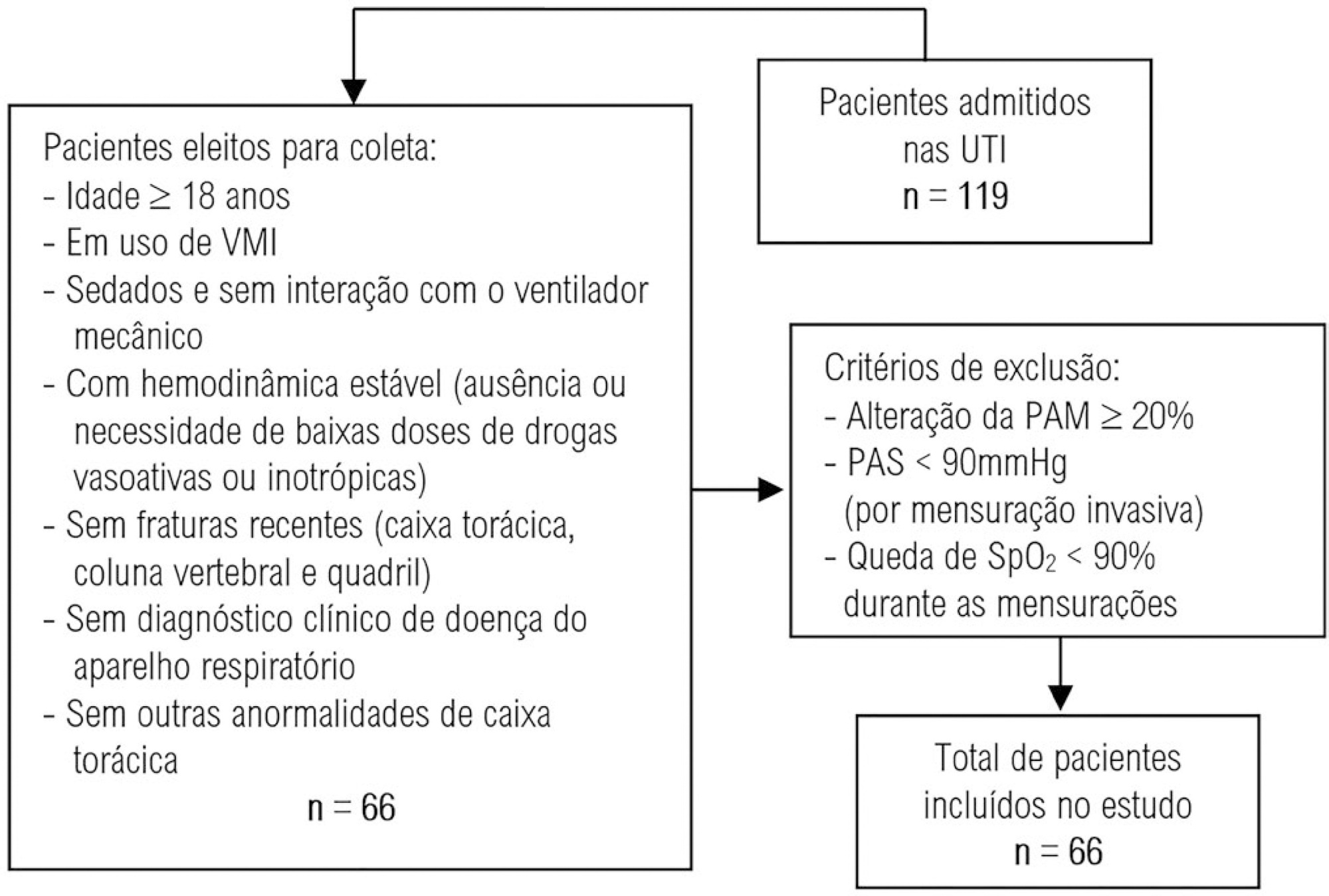
This was an analytical study conducted with individuals aged ≥ 18 years who were on invasive mechanical ventilation and had no clinical diagnosis of respiratory system disease and/or chest abnormality. Three measurements of respiratory mechanics were performed with a 1-minute interval between them. The first and third measurements were performed by examiner A, the second by examiner B. The values for the resistance and static and dynamic compliance of the respiratory system were compared using the intraclass correlation coefficient.
A total of 198 measurements of respiratory mechanics were performed for 66 patients on mechanical ventilation. The patients had a mean age of 52.6 ± 18.6 years and a mean body mass index of 21.6 ± 2.1kg/m2; a surgical profile (61.5%) and female sex (53.8%) were predominant. Mean values were obtained for the three measurements of respiratory system resistance (A1: 15.7 ± 6.8cmH2O/L/s; B1: 15.7 ± 6.4cmH2O/L/s and A2: 15.9 ± 6.2cmH2O/L/s), respiratory system static compliance (A1: 42.1 ± 13.7mL/cmH2O; B1: 42.4 ± 14.6mL/cmH2O and A2: 42.2 ± 14.5mL/cmH2O) and respiratory system dynamic compliance (A1: 21.3 ± 7.3mL/cmH2O; B1: 21.4 ± 7.5mL/cmH2O and A2: 21.3 ± 6.2mL/cmH2O). The intraclass correlation coefficient was also calculated for respiratory system resistance (R = 0.882 and p = 0.001; R = 0.949 and p = 0.001 - interexaminer A1 versus B and B versus A2, respectively; R = 0.932 and p = 0.001 - intraexaminer); respiratory system static compliance (R = 0.951 and p = 0.001; R = 0.958 and p = 0.001 - interexaminer A1 versus B and B versus A2, respectively; R = 0.965 and p = 0.001 - intraexaminer) and respiratory system dynamic compliance (R = 0.957 and p = 0.001; R = 0.946 and p = 0.001 - interexaminer A1 versus B and B versus A2, respectively; R = 0.926 and p = 0.001 - intraexaminer).
The measurements of resistance and static and dynamic compliance of the respiratory system show good intra- and interexaminer reproducibility for ventilated patients.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):398-404
DOI 10.5935/0103-507X.20200068
To evaluate the intra- and interexaminer reproducibility of measurements of the resistance and static and dynamic compliance of the respiratory system in patients on mechanical ventilation.
This was an analytical study conducted with individuals aged ≥ 18 years who were on invasive mechanical ventilation and had no clinical diagnosis of respiratory system disease and/or chest abnormality. Three measurements of respiratory mechanics were performed with a 1-minute interval between them. The first and third measurements were performed by examiner A, the second by examiner B. The values for the resistance and static and dynamic compliance of the respiratory system were compared using the intraclass correlation coefficient.
A total of 198 measurements of respiratory mechanics were performed for 66 patients on mechanical ventilation. The patients had a mean age of 52.6 ± 18.6 years and a mean body mass index of 21.6 ± 2.1kg/m2; a surgical profile (61.5%) and female sex (53.8%) were predominant. Mean values were obtained for the three measurements of respiratory system resistance (A1: 15.7 ± 6.8cmH2O/L/s; B1: 15.7 ± 6.4cmH2O/L/s and A2: 15.9 ± 6.2cmH2O/L/s), respiratory system static compliance (A1: 42.1 ± 13.7mL/cmH2O; B1: 42.4 ± 14.6mL/cmH2O and A2: 42.2 ± 14.5mL/cmH2O) and respiratory system dynamic compliance (A1: 21.3 ± 7.3mL/cmH2O; B1: 21.4 ± 7.5mL/cmH2O and A2: 21.3 ± 6.2mL/cmH2O). The intraclass correlation coefficient was also calculated for respiratory system resistance (R = 0.882 and p = 0.001; R = 0.949 and p = 0.001 - interexaminer A1 versus B and B versus A2, respectively; R = 0.932 and p = 0.001 - intraexaminer); respiratory system static compliance (R = 0.951 and p = 0.001; R = 0.958 and p = 0.001 - interexaminer A1 versus B and B versus A2, respectively; R = 0.965 and p = 0.001 - intraexaminer) and respiratory system dynamic compliance (R = 0.957 and p = 0.001; R = 0.946 and p = 0.001 - interexaminer A1 versus B and B versus A2, respectively; R = 0.926 and p = 0.001 - intraexaminer).
The measurements of resistance and static and dynamic compliance of the respiratory system show good intra- and interexaminer reproducibility for ventilated patients.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):229-234
DOI 10.5935/0103-507X.20200041
To depict the clinical presentation and outcomes of a cohort of critically ill patients with esophageal cancer.
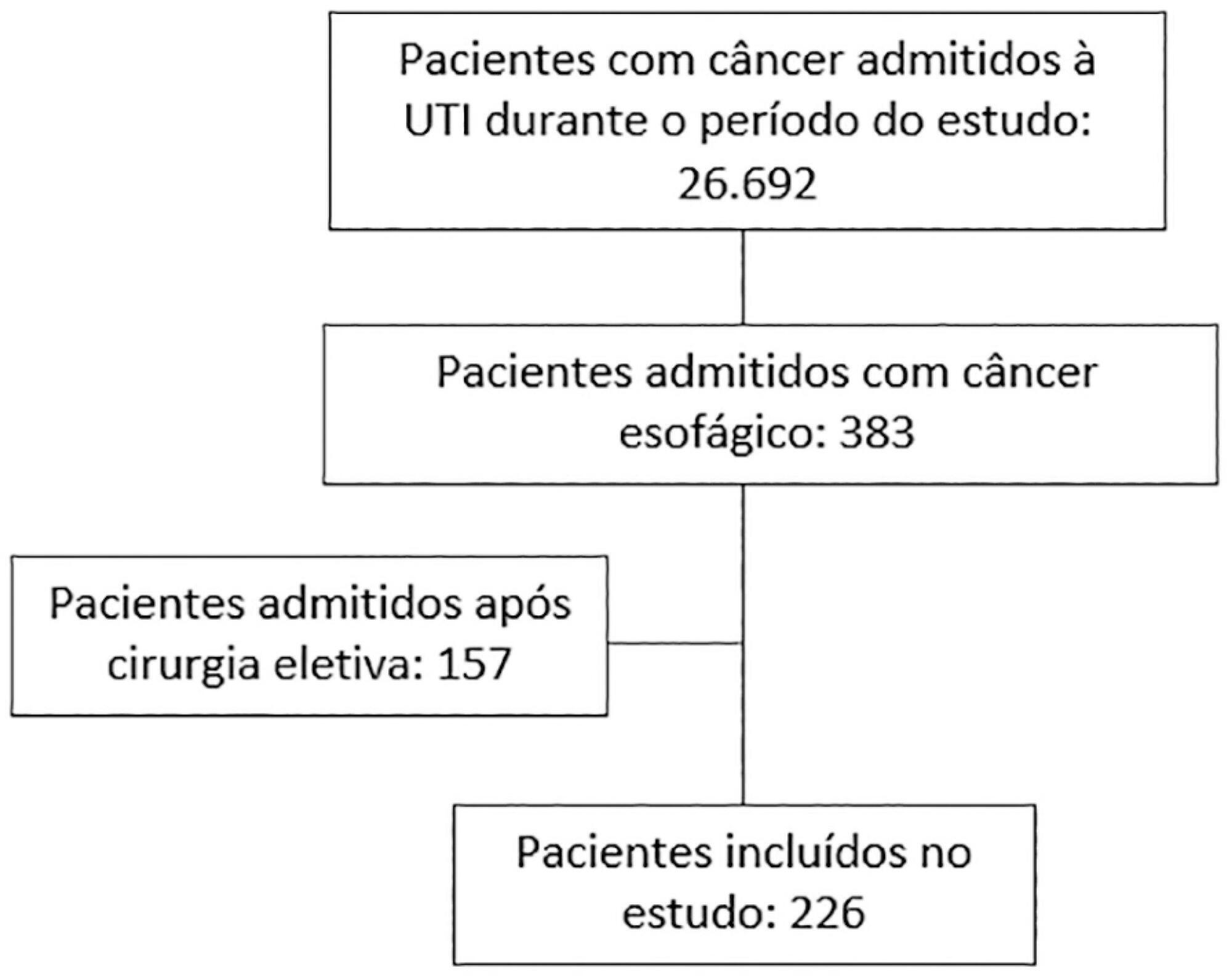
We carried out a multicenter retrospective study that included patients with esophageal cancer admitted to intensive care units with acute illness between September 2009 and December 2017. We collected the demographic and clinical characteristics of all included patients, as well as organ-support measures and hospital outcomes. We performed logistic regression analysis to identify independent factors associated with in-hospital mortality.
Of 226 patients included in the study, 131 (58.0%) patients died before hospital discharge. Squamous cell carcinoma was more frequent than adenocarcinoma, and 124 (54.9%) patients had metastatic cancer. The main reasons for admission were sepsis/septic shock and acute respiratory failure. Mechanical ventilation (OR = 6.18; 95%CI 2.86 - 13.35) and metastatic disease (OR = 7.10; 95%CI 3.35 - 15.05) were independently associated with in-hospital mortality.
In this cohort of patients with esophageal cancer admitted to intensive care units with acute illness, the in-hospital mortality rate was very high. The requirement for invasive mechanical ventilation and metastatic disease were independent prognostic factors and should be considered in discussions about the short-term outcomes of these patients.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):229-234
DOI 10.5935/0103-507X.20200041
To depict the clinical presentation and outcomes of a cohort of critically ill patients with esophageal cancer.
We carried out a multicenter retrospective study that included patients with esophageal cancer admitted to intensive care units with acute illness between September 2009 and December 2017. We collected the demographic and clinical characteristics of all included patients, as well as organ-support measures and hospital outcomes. We performed logistic regression analysis to identify independent factors associated with in-hospital mortality.
Of 226 patients included in the study, 131 (58.0%) patients died before hospital discharge. Squamous cell carcinoma was more frequent than adenocarcinoma, and 124 (54.9%) patients had metastatic cancer. The main reasons for admission were sepsis/septic shock and acute respiratory failure. Mechanical ventilation (OR = 6.18; 95%CI 2.86 - 13.35) and metastatic disease (OR = 7.10; 95%CI 3.35 - 15.05) were independently associated with in-hospital mortality.
In this cohort of patients with esophageal cancer admitted to intensive care units with acute illness, the in-hospital mortality rate was very high. The requirement for invasive mechanical ventilation and metastatic disease were independent prognostic factors and should be considered in discussions about the short-term outcomes of these patients.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):81-91
DOI 10.5935/0103-507X.20200013
To identify common practices related to the use and titration of pressure-support ventilation (PC-CSV - pressure control-continuous spontaneous ventilation) in patients under mechanical ventilation and to analyze diagnostic criteria for over-assistance and under-assistance. The secondary objective was to compare the responses provided by physician, physiotherapists and nurses related to diagnostic criteria for over-assistance and under-assistance.
An online survey was conducted using the Survey Monkey tool. Physicians, nurses and physiotherapists from Argentina with access to PC-CSV in their usual clinical practice were included.
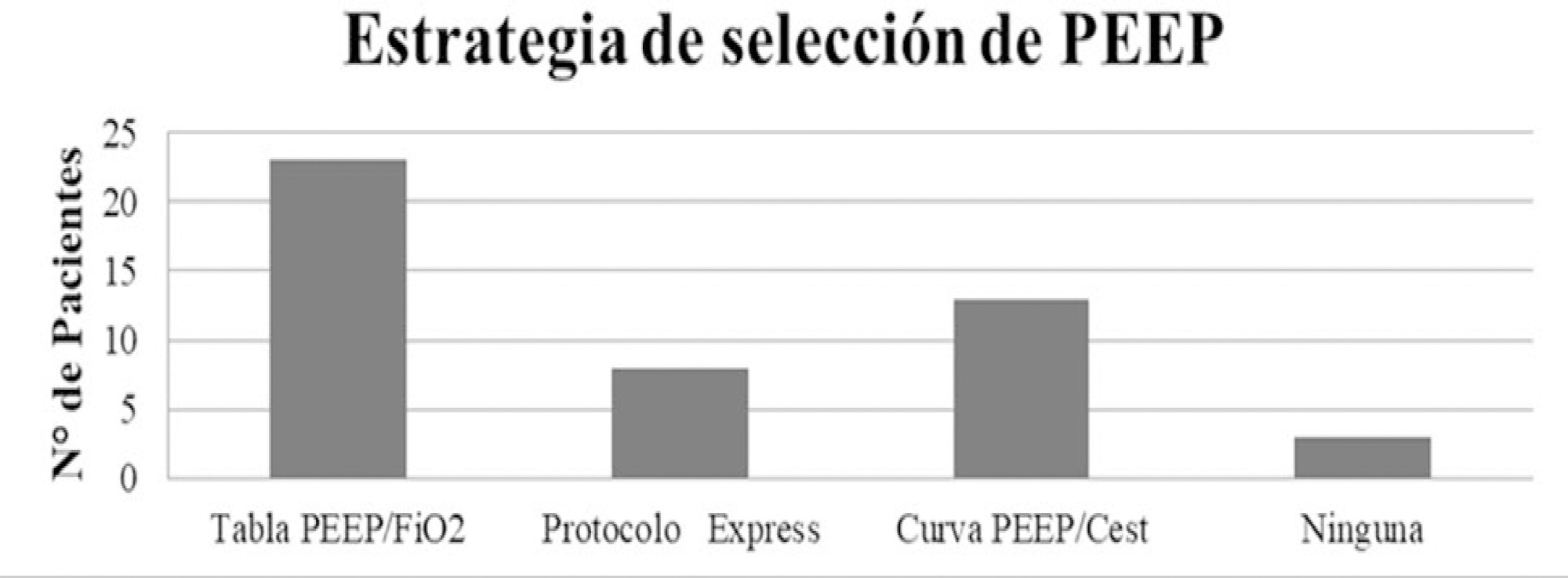
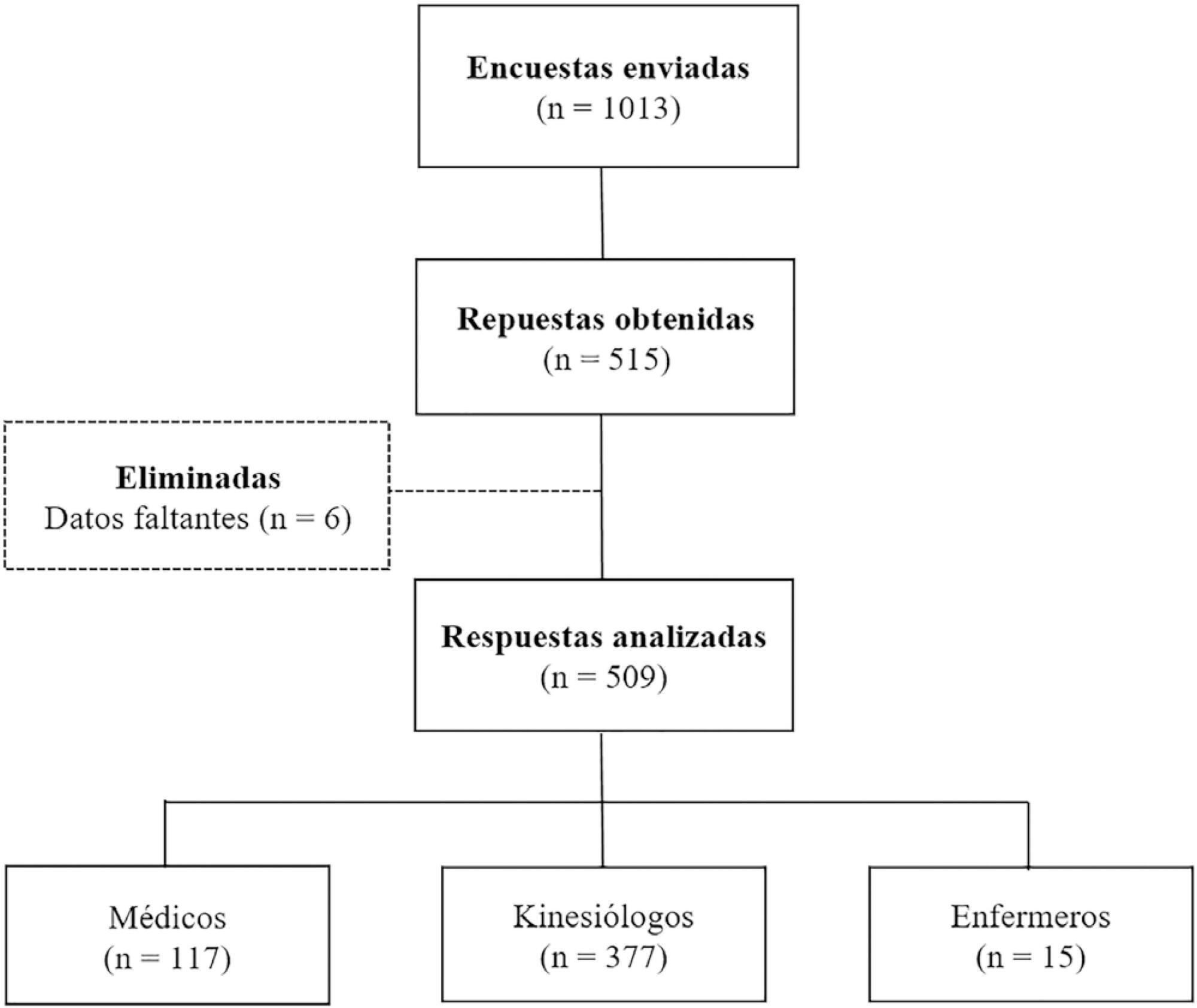
A total of 509 surveys were collected from October to December 2018. Of these, 74.1% were completed by physiotherapists. A total of 77.6% reported using PC-CSV to initiate the partial ventilatory support phase, and 43.8% of respondents select inspiratory pressure support level based on tidal volume. The main objective for selecting positive end-expiratory pressure (PEEP) level was to decrease the work of breathing. High tidal volume was the primary variable for detecting over-assistance, while the use of accessory respiratory muscles was the most commonly chosen for under-assistance. Discrepancies were observed between physicians and physiotherapists in relation to the diagnostic criteria for over-assistance.
The most commonly used mode to initiate the partial ventilatory support phase was PC-CSV. The most frequently selected variable to guide the titration of inspiratory pressure support level was tidal volume, and the main objective of PEEP was to decrease the work of breathing. Over-assistance was detected primarily by high tidal volume, while under-assistance by accessory respiratory muscles activation. Discrepancies were observed among professions in relation to the diagnostic criteria for over-assistance, but not for under-assistance.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):81-91
DOI 10.5935/0103-507X.20200013
To identify common practices related to the use and titration of pressure-support ventilation (PC-CSV - pressure control-continuous spontaneous ventilation) in patients under mechanical ventilation and to analyze diagnostic criteria for over-assistance and under-assistance. The secondary objective was to compare the responses provided by physician, physiotherapists and nurses related to diagnostic criteria for over-assistance and under-assistance.
An online survey was conducted using the Survey Monkey tool. Physicians, nurses and physiotherapists from Argentina with access to PC-CSV in their usual clinical practice were included.
A total of 509 surveys were collected from October to December 2018. Of these, 74.1% were completed by physiotherapists. A total of 77.6% reported using PC-CSV to initiate the partial ventilatory support phase, and 43.8% of respondents select inspiratory pressure support level based on tidal volume. The main objective for selecting positive end-expiratory pressure (PEEP) level was to decrease the work of breathing. High tidal volume was the primary variable for detecting over-assistance, while the use of accessory respiratory muscles was the most commonly chosen for under-assistance. Discrepancies were observed between physicians and physiotherapists in relation to the diagnostic criteria for over-assistance.
The most commonly used mode to initiate the partial ventilatory support phase was PC-CSV. The most frequently selected variable to guide the titration of inspiratory pressure support level was tidal volume, and the main objective of PEEP was to decrease the work of breathing. Over-assistance was detected primarily by high tidal volume, while under-assistance by accessory respiratory muscles activation. Discrepancies were observed among professions in relation to the diagnostic criteria for over-assistance, but not for under-assistance.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):58-65
DOI 10.5935/0103-507X.20200010
To determine whether adalimumab administration before mechanical ventilation reduces ventilator-induced lung injury (VILI).
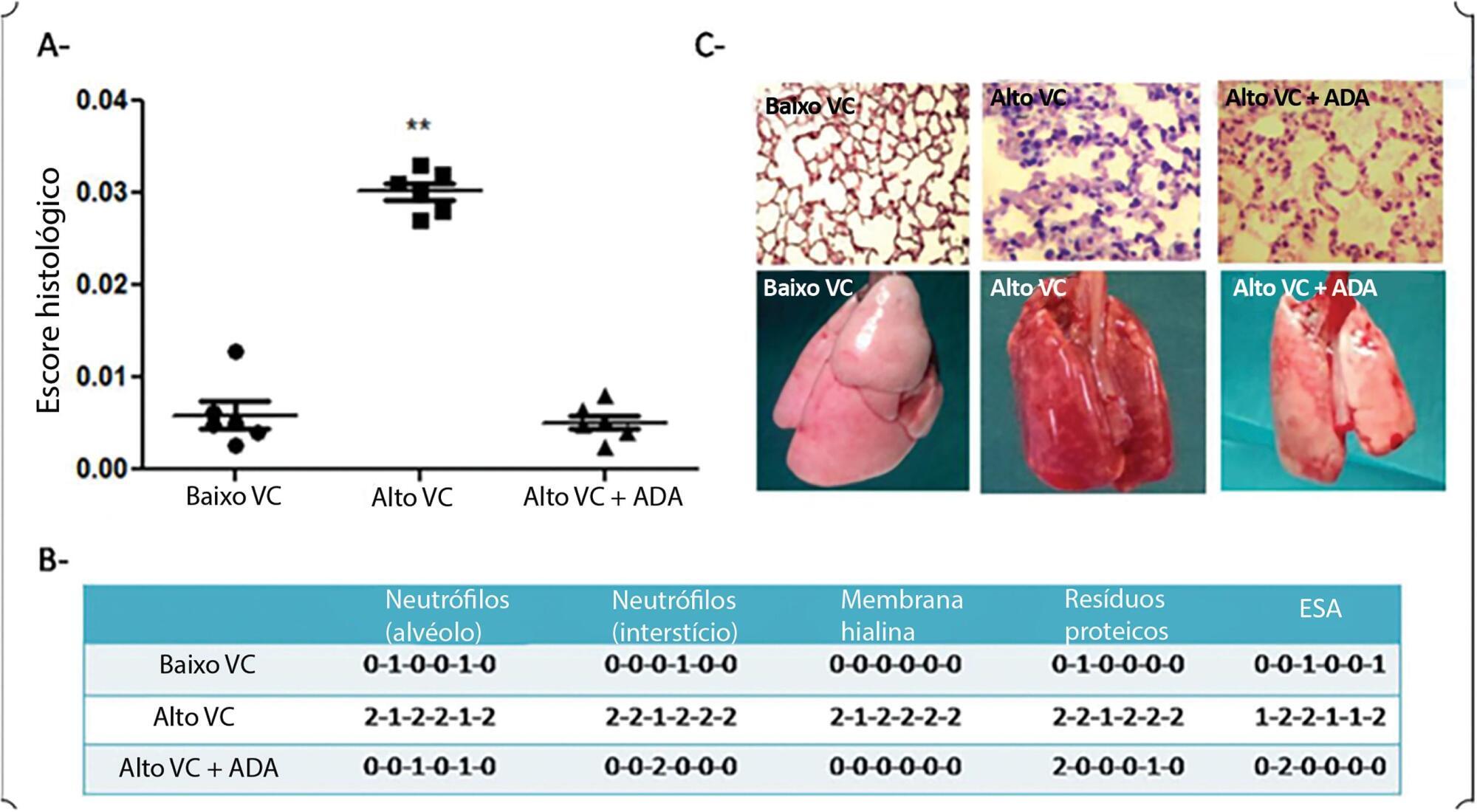
Eighteen rats randomized into 3 groups underwent mechanical ventilation for 3 hours with a fraction of inspired oxygen = 0.40% including a low tidal volume group (n = 6), where tidal volume = 8mL/kg and positive end-expiratory pressure = 5cmH2O; a high tidal volume group (n = 6), where tidal volume = 35mL/kg and positive end-expiratory pressure = 0; and a pretreated + high tidal volume group (n = 6) where adalimumab (100ug/kg) was administered intraperitoneally 24 hours before mechanical ventilation + tidal volume = 35mL/kg and positive end-expiratory pressure = 0. ANOVA was used to compare histological damage (ATS 2010 Lung Injury Scoring System), pulmonary edema, lung compliance, arterial partial pressure of oxygen, and mean arterial pressure among the groups.
After 3 hours of ventilation, the mean histological lung injury score was higher in the high tidal volume group than in the low tidal volume group (0.030 versus 0.0051, respectively, p = 0.003). The high tidal volume group showed diminished lung compliance at 3 hours (p = 0.04) and hypoxemia (p = 0,018 versus control). Pretreated HVt group had an improved histological score, mainly due to a significant reduction in leukocyte infiltration (p = 0.003).
Histological examination after 3 hours of injurious ventilation revealed ventilator-induced lung injury in the absence of measurable changes in lung mechanics or oxygenation; administering adalimumab before mechanical ventilation reduced lung edema and histological damage.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):58-65
DOI 10.5935/0103-507X.20200010
To determine whether adalimumab administration before mechanical ventilation reduces ventilator-induced lung injury (VILI).
Eighteen rats randomized into 3 groups underwent mechanical ventilation for 3 hours with a fraction of inspired oxygen = 0.40% including a low tidal volume group (n = 6), where tidal volume = 8mL/kg and positive end-expiratory pressure = 5cmH2O; a high tidal volume group (n = 6), where tidal volume = 35mL/kg and positive end-expiratory pressure = 0; and a pretreated + high tidal volume group (n = 6) where adalimumab (100ug/kg) was administered intraperitoneally 24 hours before mechanical ventilation + tidal volume = 35mL/kg and positive end-expiratory pressure = 0. ANOVA was used to compare histological damage (ATS 2010 Lung Injury Scoring System), pulmonary edema, lung compliance, arterial partial pressure of oxygen, and mean arterial pressure among the groups.
After 3 hours of ventilation, the mean histological lung injury score was higher in the high tidal volume group than in the low tidal volume group (0.030 versus 0.0051, respectively, p = 0.003). The high tidal volume group showed diminished lung compliance at 3 hours (p = 0.04) and hypoxemia (p = 0,018 versus control). Pretreated HVt group had an improved histological score, mainly due to a significant reduction in leukocyte infiltration (p = 0.003).
Histological examination after 3 hours of injurious ventilation revealed ventilator-induced lung injury in the absence of measurable changes in lung mechanics or oxygenation; administering adalimumab before mechanical ventilation reduced lung edema and histological damage.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)