-
Commentaries
β-blockers in septic shock: are we there yet?
Rev Bras Ter Intensiva. 2017;29(1):1-3
Abstract
Commentariesβ-blockers in septic shock: are we there yet?
Rev Bras Ter Intensiva. 2017;29(1):1-3
DOI 10.5935/0103-507X.20170001
Views0Background Septic shock is characterized by circulatory collapse and diminished tissue perfusion, leading to organ dysfunction in the setting of systemic infection. The mechanisms of septic shock are incompletely understood; moreover, its incidence is increasing, and its mortality remains unacceptably high. In addition to antimicrobial and supportive treatments, no other therapy has a survival benefit, […]See moreViews0

Abstract
Commentariesβ-blockers in septic shock: are we there yet?
Rev Bras Ter Intensiva. 2017;29(1):1-3
DOI 10.5935/0103-507X.20170001
Views0BackgroundSeptic shock is characterized by circulatory collapse and diminished tissue perfusion, leading to organ dysfunction in the setting of systemic infection. The mechanisms of septic shock are incompletely understood; moreover, its incidence is increasing, and its mortality remains unacceptably high. In addition to antimicrobial and supportive treatments, no other therapy has a survival benefit, despite […]See more -
Commentaries
Dear Sepsis-3, we are sorry to say that we don’t like you
Rev Bras Ter Intensiva. 2017;29(1):4-8
Abstract
CommentariesDear Sepsis-3, we are sorry to say that we don’t like you
Rev Bras Ter Intensiva. 2017;29(1):4-8
DOI 10.5935/0103-507X.20170002
Views0The controversyThe medical community became divided over the clinical value of the new criteria (i.e., regarding their actual impact and safety when applied at the bedside). The criticism mainly focused on the following three aspects: (1) underlying theoretical concepts; (2) the methods used to define the criteria; and (3) their potential impacts on clinical practice.Regarding […]See moreViews0Abstract
CommentariesDear Sepsis-3, we are sorry to say that we don’t like you
Rev Bras Ter Intensiva. 2017;29(1):4-8
DOI 10.5935/0103-507X.20170002
Views0The controversyThe medical community became divided over the clinical value of the new criteria (i.e., regarding their actual impact and safety when applied at the bedside). The criticism mainly focused on the following three aspects: (1) underlying theoretical concepts; (2) the methods used to define the criteria; and (3) their potential impacts on clinical practice.Regarding […]See more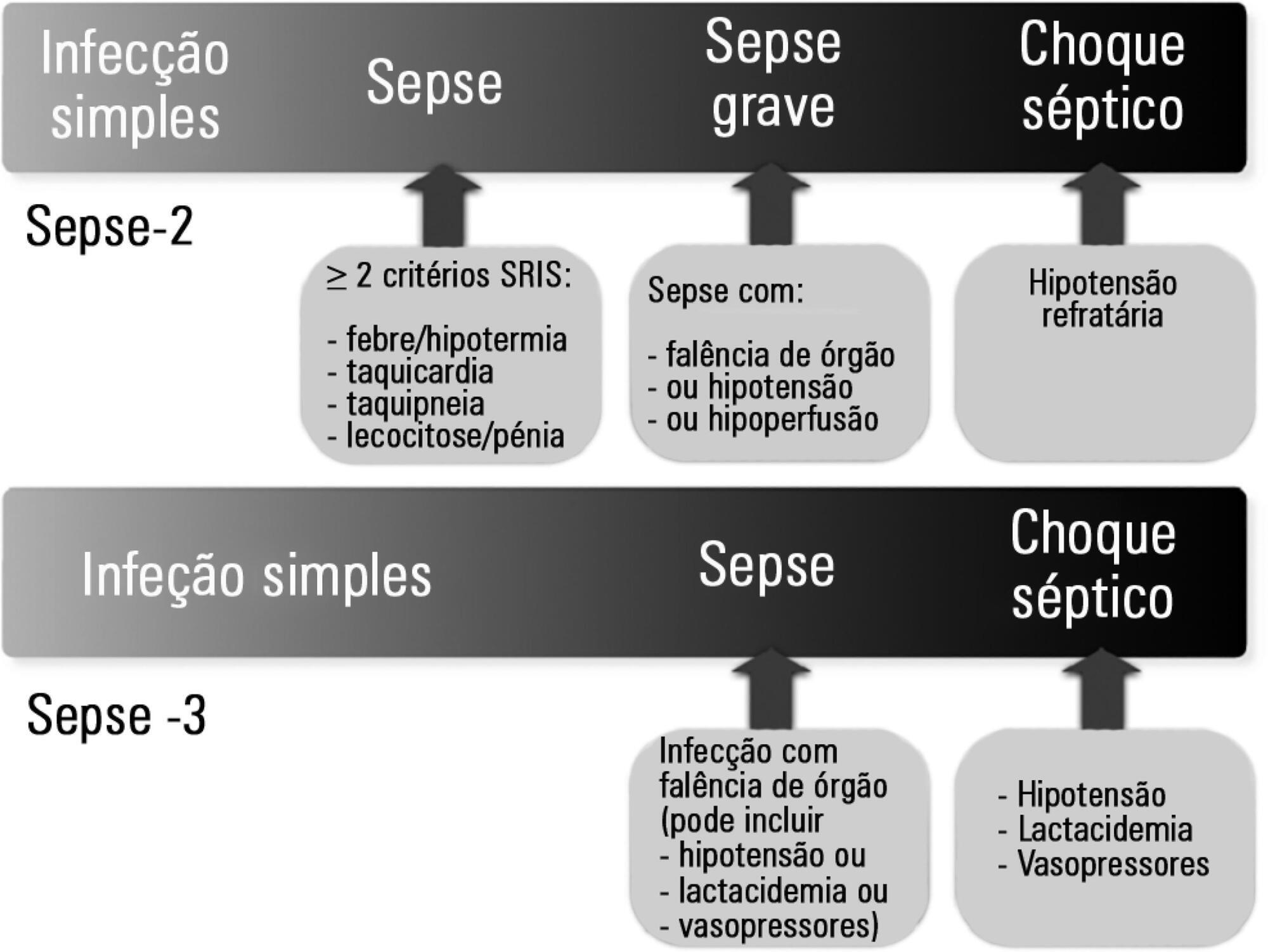
-
Commentaries
Seeking to humanize intensive care
Rev Bras Ter Intensiva. 2017;29(1):9-13
Abstract
CommentariesSeeking to humanize intensive care
Rev Bras Ter Intensiva. 2017;29(1):9-13
DOI 10.5935/0103-507X.20170003
Views0IntroductionThe scientific and technical evolution of critical patient care has dramatically improved clinical practice and survival, but this progress has not been matched equally in the more human aspects of critical patient care. In many cases, the organizational and architectural characteristics of intensive care units (ICU) make them hostile environments for patients and their families […]See moreViews0Abstract
CommentariesSeeking to humanize intensive care
Rev Bras Ter Intensiva. 2017;29(1):9-13
DOI 10.5935/0103-507X.20170003
Views0IntroductionThe scientific and technical evolution of critical patient care has dramatically improved clinical practice and survival, but this progress has not been matched equally in the more human aspects of critical patient care. In many cases, the organizational and architectural characteristics of intensive care units (ICU) make them hostile environments for patients and their families […]See more
-
Original Articles
Acute bag-valve breathing maneuvers plus manual chest compression is safe during stable septic shock: a randomized clinical trial
Rev Bras Ter Intensiva. 2017;29(1):14-22
Abstract
Original ArticlesAcute bag-valve breathing maneuvers plus manual chest compression is safe during stable septic shock: a randomized clinical trial
Rev Bras Ter Intensiva. 2017;29(1):14-22
DOI 10.5935/0103-507X.20170004
Views1See moreABSTRACT
Objective:
To evaluate the effects of bag-valve breathing maneuvers combined with standard manual chest compression techniques on safety, hemodynamics and oxygenation in stable septic shock patients.
Design:
A parallel, assessor-blinded, randomized trial of two groups. A computer-generated list of random numbers was prepared by an independent researcher to allocate treatments.
Setting:
The Intensive Care Unit at Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul.
Participants:
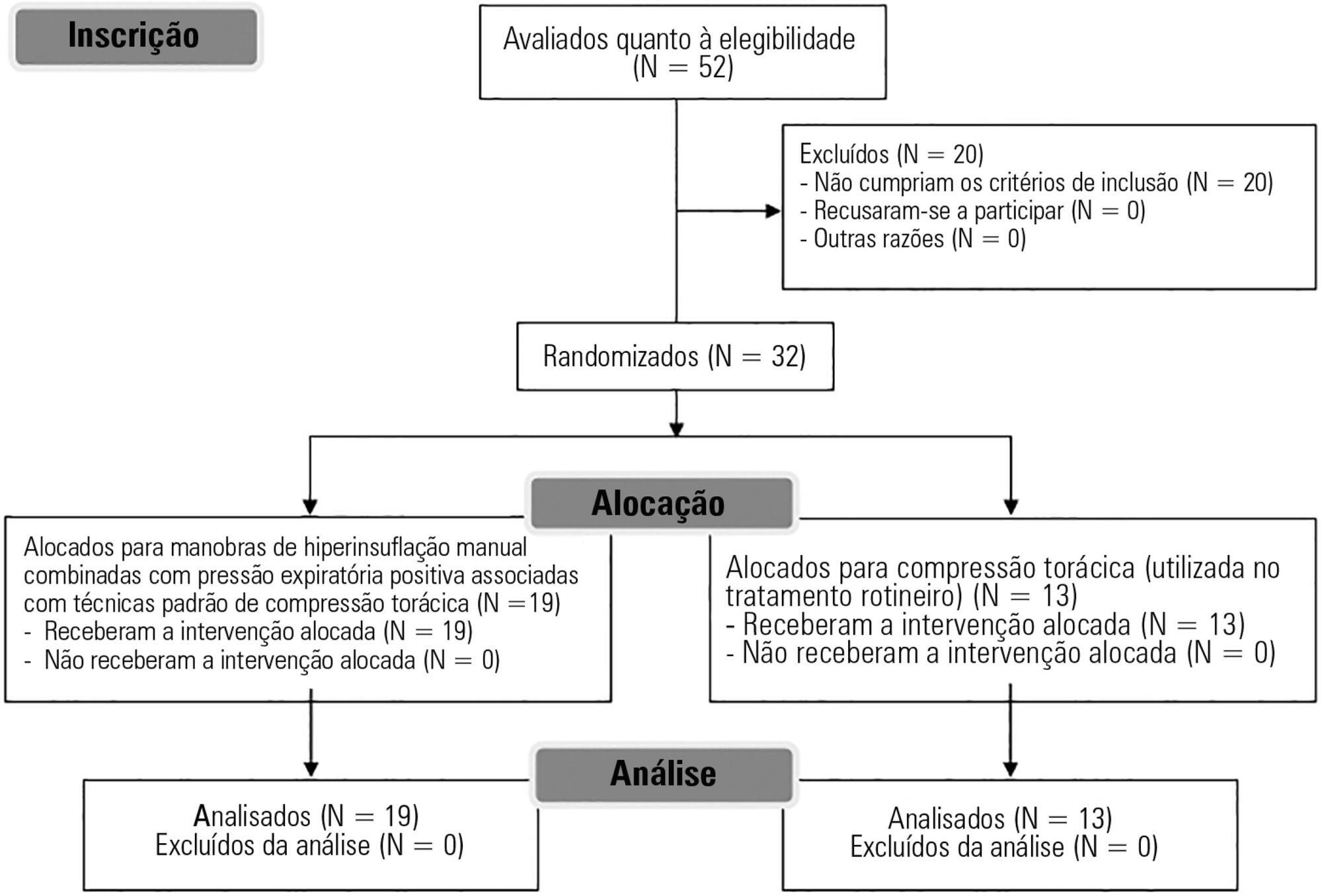
Fifty-two subjects were assessed for eligibility, and 32 were included. All included subjects (n = 32) received the allocated intervention (n = 19 for the Experimental Group and n = 13 for the Control Group).
Intervention:
Twenty minutes of bag-valve breathing maneuvers combined with manual chest compression techniques (Experimental Group) or chest compression, as routinely used at our intensive care unit (Control Group). Follow-up was performed immediately after and at 30 minutes after the intervention.
Main outcome measure:
Mean artery pressure.
Results:
All included subjects completed the trial (N = 32). We found no relevant effects on mean artery pressure (p = 0.17), heart rate (p = 0.50) or mean pulmonary artery pressure (p = 0.89) after adjusting for subject age and weight. Both groups were identical regarding oxygen consumption after the data adjustment (p = 0.84). Peripheral oxygen saturation tended to increase over time in both groups (p = 0.05), and there was no significant association between cardiac output and venous oxygen saturation (p = 0.813). No clinical deterioration was observed.
Conclusion:
A single session of bag-valve breathing maneuvers combined with manual chest compression is hemodynamically safe for stable septic-shocked subjects over the short-term.
Views1Abstract
Original ArticlesAcute bag-valve breathing maneuvers plus manual chest compression is safe during stable septic shock: a randomized clinical trial
Rev Bras Ter Intensiva. 2017;29(1):14-22
DOI 10.5935/0103-507X.20170004
Views1See moreABSTRACT
Objective:
To evaluate the effects of bag-valve breathing maneuvers combined with standard manual chest compression techniques on safety, hemodynamics and oxygenation in stable septic shock patients.
Design:
A parallel, assessor-blinded, randomized trial of two groups. A computer-generated list of random numbers was prepared by an independent researcher to allocate treatments.
Setting:
The Intensive Care Unit at Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul.
Participants:
Fifty-two subjects were assessed for eligibility, and 32 were included. All included subjects (n = 32) received the allocated intervention (n = 19 for the Experimental Group and n = 13 for the Control Group).
Intervention:
Twenty minutes of bag-valve breathing maneuvers combined with manual chest compression techniques (Experimental Group) or chest compression, as routinely used at our intensive care unit (Control Group). Follow-up was performed immediately after and at 30 minutes after the intervention.
Main outcome measure:
Mean artery pressure.
Results:
All included subjects completed the trial (N = 32). We found no relevant effects on mean artery pressure (p = 0.17), heart rate (p = 0.50) or mean pulmonary artery pressure (p = 0.89) after adjusting for subject age and weight. Both groups were identical regarding oxygen consumption after the data adjustment (p = 0.84). Peripheral oxygen saturation tended to increase over time in both groups (p = 0.05), and there was no significant association between cardiac output and venous oxygen saturation (p = 0.813). No clinical deterioration was observed.
Conclusion:
A single session of bag-valve breathing maneuvers combined with manual chest compression is hemodynamically safe for stable septic-shocked subjects over the short-term.
-
Original Articles
Predictors and pattern of weaning and long-term outcome of patients with prolonged mechanical ventilation at an acute intensive care unit in North India
Rev Bras Ter Intensiva. 2017;29(1):23-33
Abstract
Original ArticlesPredictors and pattern of weaning and long-term outcome of patients with prolonged mechanical ventilation at an acute intensive care unit in North India
Rev Bras Ter Intensiva. 2017;29(1):23-33
DOI 10.5935/0103-507X.20170005
Views1See moreABSTRACT
Objective:
This study aimed to examine the clinical characteristics, weaning pattern, and outcome of patients requiring prolonged mechanical ventilation in acute intensive care unit settings in a resource-limited country.
Methods:
This was a prospective single-center observational study in India, where all adult patients requiring prolonged ventilation were followed for weaning duration and pattern and for survival at both intensive care unit discharge and at 12 months. The definition of prolonged mechanical ventilation used was that of the National Association for Medical Direction of Respiratory Care.
Results:
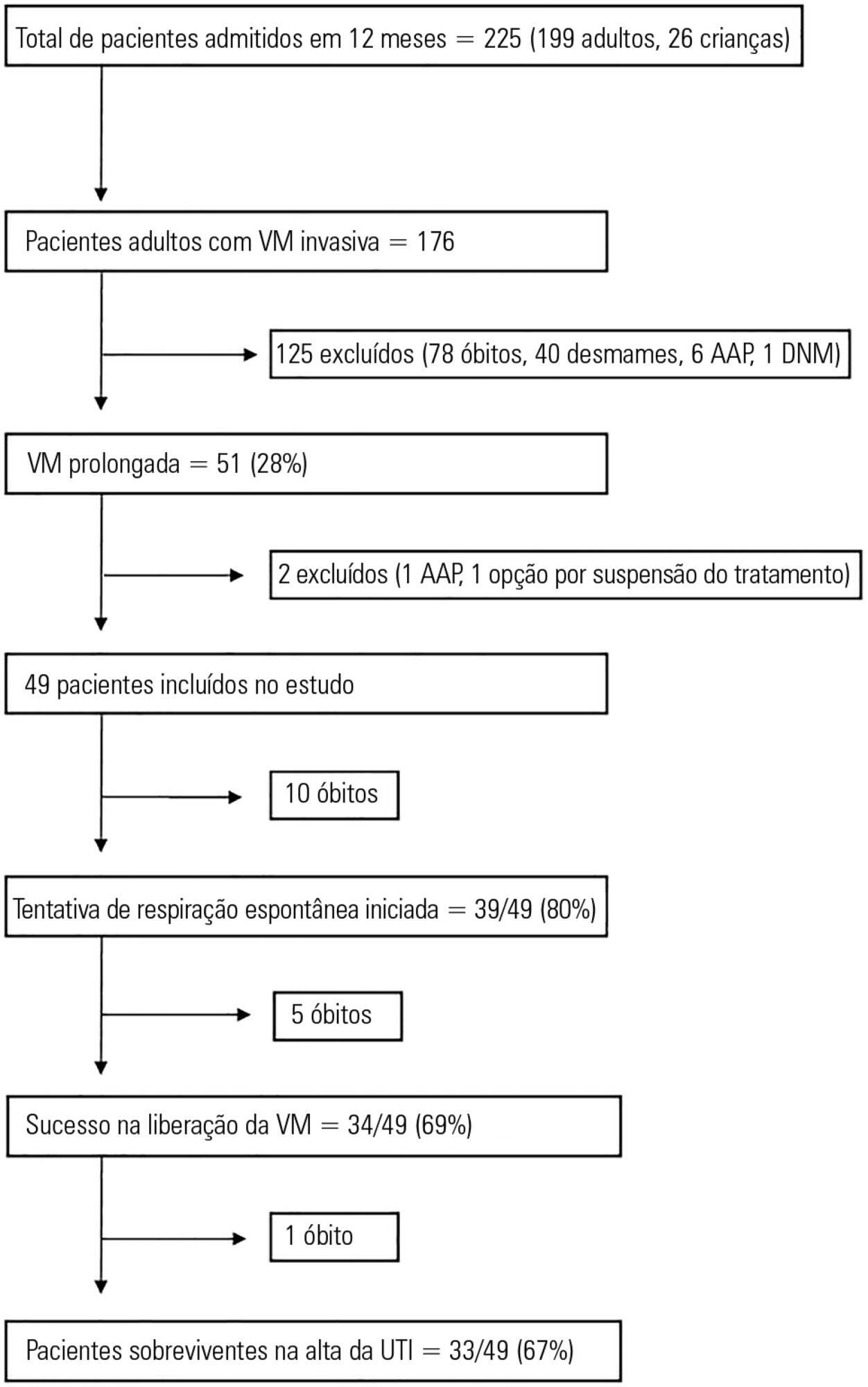
During the one-year period, 49 patients with a mean age of 49.7 years had prolonged ventilation; 63% were male, and 84% had a medical illness. The median APACHE II and SOFA scores on admission were 17 and 9, respectively. The median number of ventilation days was 37. The most common reason for starting ventilation was respiratory failure secondary to sepsis (67%). Weaning was initiated in 39 (79.5%) patients, with success in 34 (87%). The median weaning duration was 14 (9.5 – 19) days, and the median length of intensive care unit stay was 39 (32 – 58.5) days. Duration of vasopressor support and need for hemodialysis were significant independent predictors of unsuccessful ventilator liberation. At the 12-month follow-up, 65% had survived.
Conclusion:
In acute intensive care units, more than one-fourth of patients with invasive ventilation required prolonged ventilation. Successful weaning was achieved in two-thirds of patients, and most survived at the 12-month follow-up.
Views1Abstract
Original ArticlesPredictors and pattern of weaning and long-term outcome of patients with prolonged mechanical ventilation at an acute intensive care unit in North India
Rev Bras Ter Intensiva. 2017;29(1):23-33
DOI 10.5935/0103-507X.20170005
Views1See moreABSTRACT
Objective:
This study aimed to examine the clinical characteristics, weaning pattern, and outcome of patients requiring prolonged mechanical ventilation in acute intensive care unit settings in a resource-limited country.
Methods:
This was a prospective single-center observational study in India, where all adult patients requiring prolonged ventilation were followed for weaning duration and pattern and for survival at both intensive care unit discharge and at 12 months. The definition of prolonged mechanical ventilation used was that of the National Association for Medical Direction of Respiratory Care.
Results:
During the one-year period, 49 patients with a mean age of 49.7 years had prolonged ventilation; 63% were male, and 84% had a medical illness. The median APACHE II and SOFA scores on admission were 17 and 9, respectively. The median number of ventilation days was 37. The most common reason for starting ventilation was respiratory failure secondary to sepsis (67%). Weaning was initiated in 39 (79.5%) patients, with success in 34 (87%). The median weaning duration was 14 (9.5 – 19) days, and the median length of intensive care unit stay was 39 (32 – 58.5) days. Duration of vasopressor support and need for hemodialysis were significant independent predictors of unsuccessful ventilator liberation. At the 12-month follow-up, 65% had survived.
Conclusion:
In acute intensive care units, more than one-fourth of patients with invasive ventilation required prolonged ventilation. Successful weaning was achieved in two-thirds of patients, and most survived at the 12-month follow-up.
-
Original Articles
Brazilian version of the Functional Status Score for the ICU: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2017;29(1):34-38
Abstract
Original ArticlesBrazilian version of the Functional Status Score for the ICU: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2017;29(1):34-38
DOI 10.5935/0103-507X.20170006
Views0See moreABSTRACT
Objective:
The aim of the present study was to translate and cross-culturally adapt the Functional Status Score for the intensive care unit (FSS-ICU) into Brazilian Portuguese.
Methods:
This study consisted of the following steps: translation (performed by two independent translators), synthesis of the initial translation, back-translation (by two independent translators who were unaware of the original FSS-ICU), and testing to evaluate the target audience’s understanding. An Expert Committee supervised all steps and was responsible for the modifications made throughout the process and the final translated version.
Results:
The testing phase included two experienced physiotherapists who assessed a total of 30 critical care patients (mean FSS-ICU score = 25 ± 6). As the physiotherapists did not report any uncertainties or problems with interpretation affecting their performance, no additional adjustments were made to the Brazilian Portuguese version after the testing phase. Good interobserver reliability between the two assessors was obtained for each of the 5 FSS-ICU tasks and for the total FSS-ICU score (intraclass correlation coefficients ranged from 0.88 to 0.91).
Conclusion:
The adapted version of the FSS-ICU in Brazilian Portuguese was easy to understand and apply in an intensive care unit environment.
Views0Abstract
Original ArticlesBrazilian version of the Functional Status Score for the ICU: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2017;29(1):34-38
DOI 10.5935/0103-507X.20170006
Views0See moreABSTRACT
Objective:
The aim of the present study was to translate and cross-culturally adapt the Functional Status Score for the intensive care unit (FSS-ICU) into Brazilian Portuguese.
Methods:
This study consisted of the following steps: translation (performed by two independent translators), synthesis of the initial translation, back-translation (by two independent translators who were unaware of the original FSS-ICU), and testing to evaluate the target audience’s understanding. An Expert Committee supervised all steps and was responsible for the modifications made throughout the process and the final translated version.
Results:
The testing phase included two experienced physiotherapists who assessed a total of 30 critical care patients (mean FSS-ICU score = 25 ± 6). As the physiotherapists did not report any uncertainties or problems with interpretation affecting their performance, no additional adjustments were made to the Brazilian Portuguese version after the testing phase. Good interobserver reliability between the two assessors was obtained for each of the 5 FSS-ICU tasks and for the total FSS-ICU score (intraclass correlation coefficients ranged from 0.88 to 0.91).
Conclusion:
The adapted version of the FSS-ICU in Brazilian Portuguese was easy to understand and apply in an intensive care unit environment.
-
Original Articles
Reducing pressure ulcers in patients with prolonged acute mechanical ventilation: a quasi-experimental study
Rev Bras Ter Intensiva. 2017;29(1):39-46
Abstract
Original ArticlesReducing pressure ulcers in patients with prolonged acute mechanical ventilation: a quasi-experimental study
Rev Bras Ter Intensiva. 2017;29(1):39-46
DOI 10.5935/0103-507X.20170007
Views1ABSTRACT
Objective:
To determine the effectiveness of a quality management program in reducing the incidence and severity of pressure ulcers in critical care patients.
Methods:
This was a quasi-experimental, before-and-after study that was conducted in a medical-surgical intensive care unit. Consecutive patients who had received mechanical ventilation for ≥ 96 hours were included. A “Process Improvement” team designed a multifaceted interventional process that consisted of an educational session, a pressure ulcer checklist, a smartphone application for lesion monitoring and decision-making, and a “family prevention bundle”.
Results:
Fifty-five patients were included in Pre-I group, and 69 were included in the Post-I group, and the incidence of pressure ulcers in these groups was 41 (75%) and 37 (54%), respectively. The median time for pressure ulcers to develop was 4.5 [4 – 5] days in the Pre-I group and 9 [6 – 20] days in the Post-I group after admission for each period. The incidence of advanced-grade pressure ulcers was 27 (49%) in the Pre-I group and 7 (10%) in the Post-I group, and finally, the presence of pressure ulcers at discharge was 38 (69%) and 18 (26%), respectively (p < 0.05 for all comparisons). Family participation totaled 9% in the Pre-I group and increased to 57% in the Post-I group (p < 0.05). A logistic regression model was used to analyze the predictors of advanced-grade pressure ulcers. The duration of mechanical ventilation and the presence of organ failure were positively associated with the development of pressure ulcers, while the multifaceted intervention program acted as a protective factor.
Conclusion:
A quality program based on both a smartphone application and family participation can reduce the incidence and severity of pressure ulcers in patients on prolonged acute mechanical ventilation.
Keywords:Intensive care unitsLength of stayMobile applications/standardsPressure ulcer/prevention & controlRespiration, artificialSmartphoneTelemedicine/methodsSee moreViews1Abstract
Original ArticlesReducing pressure ulcers in patients with prolonged acute mechanical ventilation: a quasi-experimental study
Rev Bras Ter Intensiva. 2017;29(1):39-46
DOI 10.5935/0103-507X.20170007
Views1ABSTRACT
Objective:
To determine the effectiveness of a quality management program in reducing the incidence and severity of pressure ulcers in critical care patients.
Methods:
This was a quasi-experimental, before-and-after study that was conducted in a medical-surgical intensive care unit. Consecutive patients who had received mechanical ventilation for ≥ 96 hours were included. A “Process Improvement” team designed a multifaceted interventional process that consisted of an educational session, a pressure ulcer checklist, a smartphone application for lesion monitoring and decision-making, and a “family prevention bundle”.
Results:
Fifty-five patients were included in Pre-I group, and 69 were included in the Post-I group, and the incidence of pressure ulcers in these groups was 41 (75%) and 37 (54%), respectively. The median time for pressure ulcers to develop was 4.5 [4 – 5] days in the Pre-I group and 9 [6 – 20] days in the Post-I group after admission for each period. The incidence of advanced-grade pressure ulcers was 27 (49%) in the Pre-I group and 7 (10%) in the Post-I group, and finally, the presence of pressure ulcers at discharge was 38 (69%) and 18 (26%), respectively (p < 0.05 for all comparisons). Family participation totaled 9% in the Pre-I group and increased to 57% in the Post-I group (p < 0.05). A logistic regression model was used to analyze the predictors of advanced-grade pressure ulcers. The duration of mechanical ventilation and the presence of organ failure were positively associated with the development of pressure ulcers, while the multifaceted intervention program acted as a protective factor.
Conclusion:
A quality program based on both a smartphone application and family participation can reduce the incidence and severity of pressure ulcers in patients on prolonged acute mechanical ventilation.
Keywords:Intensive care unitsLength of stayMobile applications/standardsPressure ulcer/prevention & controlRespiration, artificialSmartphoneTelemedicine/methodsSee more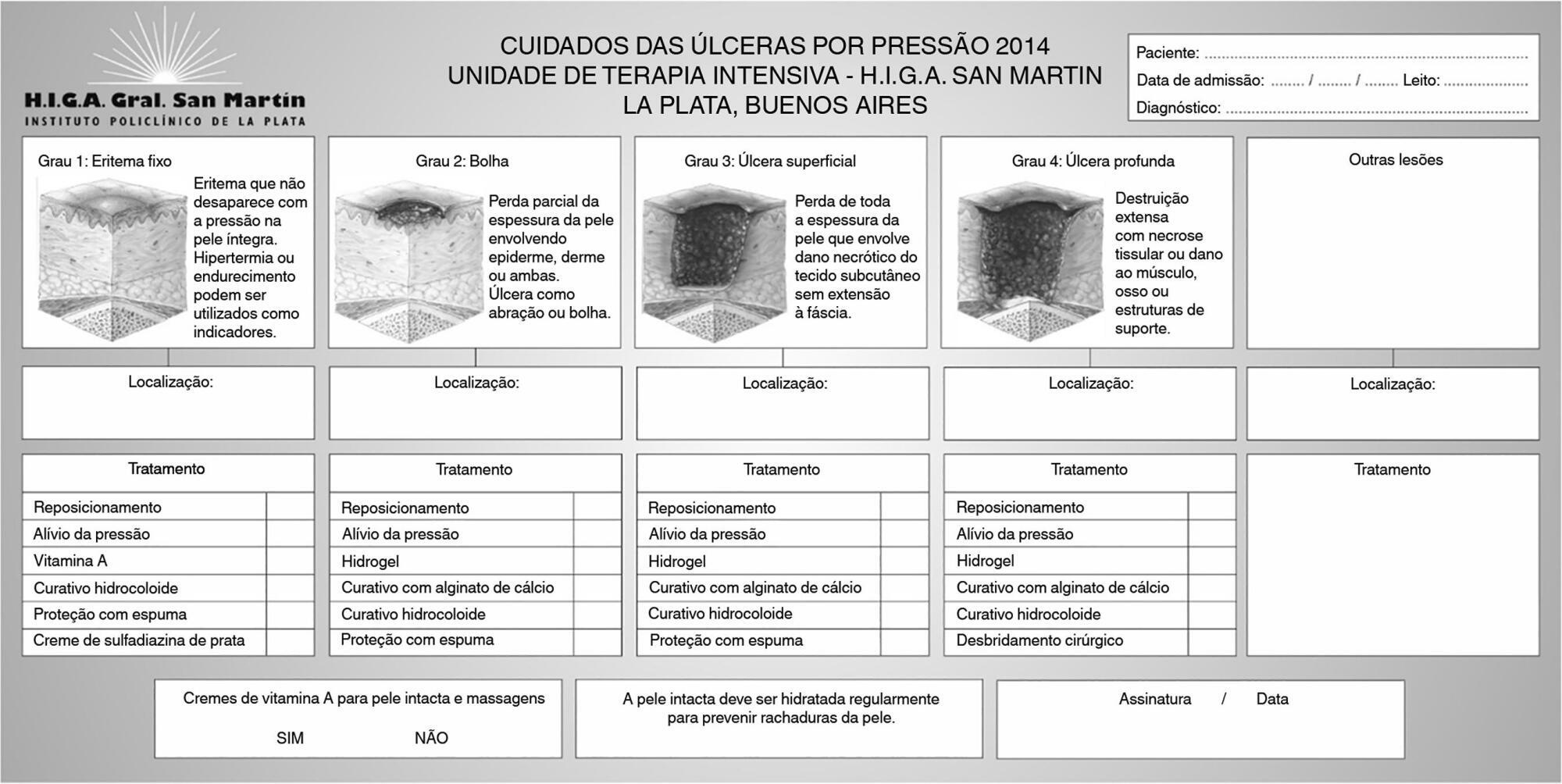
-
Original Articles
Chronic obstructive pulmonary disease exacerbation in the intensive care unit: clinical, functional and quality of life at discharge and 3 months of follow up
Rev Bras Ter Intensiva. 2017;29(1):47-54
Abstract
Original ArticlesChronic obstructive pulmonary disease exacerbation in the intensive care unit: clinical, functional and quality of life at discharge and 3 months of follow up
Rev Bras Ter Intensiva. 2017;29(1):47-54
DOI 10.5935/0103-507X.20170008
Views0ABSTRACT
Objective:
The purpose of this study was to evaluate the clinical/functional aspects and quality of life of chronic obstructive pulmonary disease patients who were discharged after an intensive care unit admission for acute respiratory failure.
Methods:
This prospective study included chronic obstructive pulmonary disease patients who were admitted to two intensive care units between December of 2010 and August of 2011 and evaluated over three visits after discharge. Thirty patients were included, and 20 patients completed the three-month follow up.
Results:
There was a significant improvement in the following: forced expiratory flow in one second (L) (1.1/1.4/1.4; p = 0.019), six-minute walk test (m) (- /232.8 /272.6; p = 0.04), BODE score (7.5/5.0/3.8; p = 0.001), cognition measured by the Mini Mental State Examination (21/23.5/23.5; p = 0.008) and quality of life measured by the total Saint George Respiratory Questionnaire score (63.3/56.8/51, p = 0.02). The mean difference in the total score was 12.3 (between visits 1 and three). Important clinical differences were observed for the symptom score (18.8), activities score (5.2) and impact score (14.3). The majority of participants (80%) reported they would be willing to undergo a new intensive care unit admission.
Conclusion:
Despite the disease severity, there was a significant clinical, functional and quality of life improvement at the end of the third month. Most patients would be willing to undergo a new intensive care unit admission.
Keywords:Chronic obstructive pulmonary diseaseCognitionPulmonary function testsQuality of lifeTreatment outcomeSee moreViews0Abstract
Original ArticlesChronic obstructive pulmonary disease exacerbation in the intensive care unit: clinical, functional and quality of life at discharge and 3 months of follow up
Rev Bras Ter Intensiva. 2017;29(1):47-54
DOI 10.5935/0103-507X.20170008
Views0ABSTRACT
Objective:
The purpose of this study was to evaluate the clinical/functional aspects and quality of life of chronic obstructive pulmonary disease patients who were discharged after an intensive care unit admission for acute respiratory failure.
Methods:
This prospective study included chronic obstructive pulmonary disease patients who were admitted to two intensive care units between December of 2010 and August of 2011 and evaluated over three visits after discharge. Thirty patients were included, and 20 patients completed the three-month follow up.
Results:
There was a significant improvement in the following: forced expiratory flow in one second (L) (1.1/1.4/1.4; p = 0.019), six-minute walk test (m) (- /232.8 /272.6; p = 0.04), BODE score (7.5/5.0/3.8; p = 0.001), cognition measured by the Mini Mental State Examination (21/23.5/23.5; p = 0.008) and quality of life measured by the total Saint George Respiratory Questionnaire score (63.3/56.8/51, p = 0.02). The mean difference in the total score was 12.3 (between visits 1 and three). Important clinical differences were observed for the symptom score (18.8), activities score (5.2) and impact score (14.3). The majority of participants (80%) reported they would be willing to undergo a new intensive care unit admission.
Conclusion:
Despite the disease severity, there was a significant clinical, functional and quality of life improvement at the end of the third month. Most patients would be willing to undergo a new intensive care unit admission.
Keywords:Chronic obstructive pulmonary diseaseCognitionPulmonary function testsQuality of lifeTreatment outcomeSee more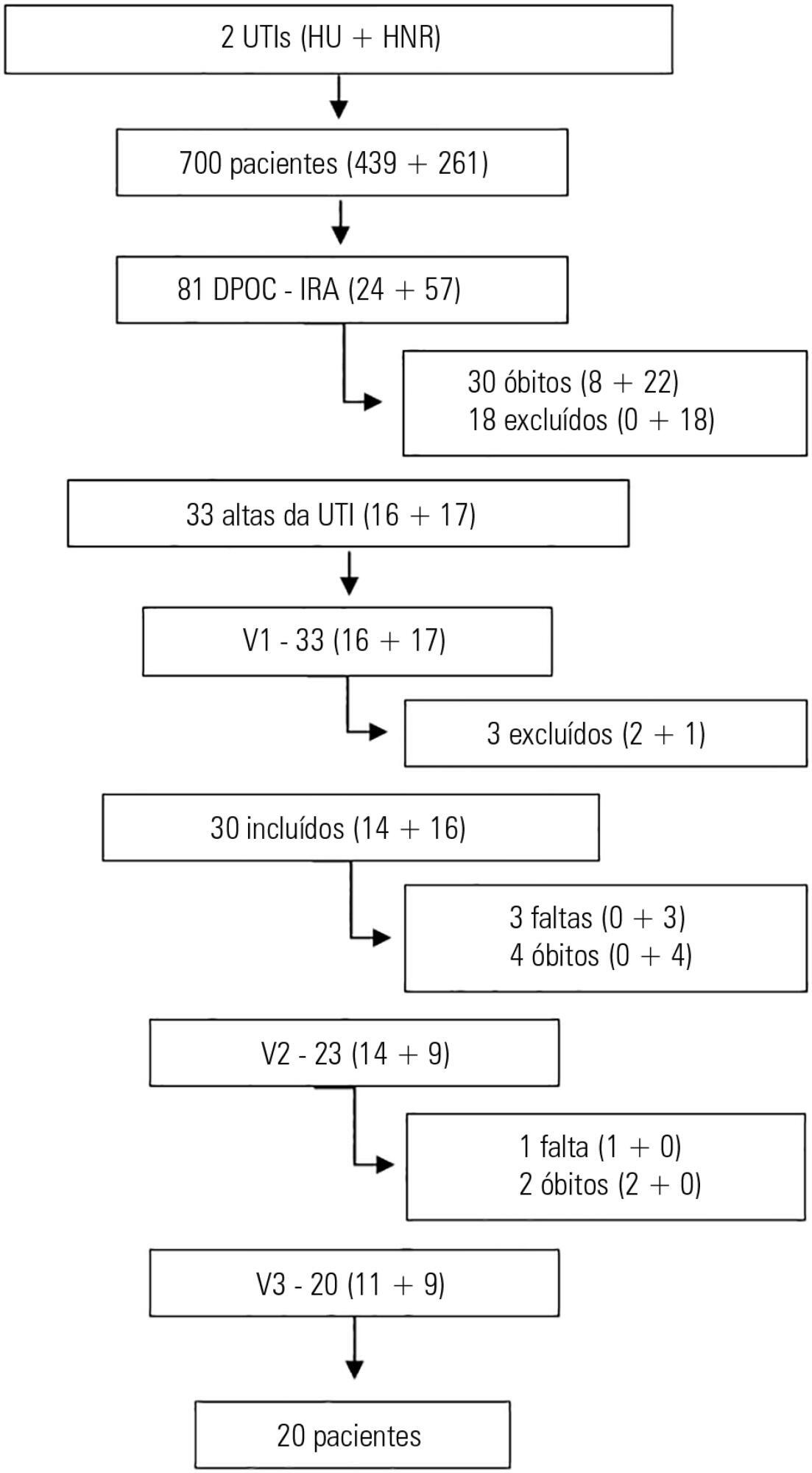
-
Original Articles
Antibacterial activity of standard and N-doped titanium dioxide-coated endotracheal tubes: an in vitro study
Rev Bras Ter Intensiva. 2017;29(1):55-62
Abstract
Original ArticlesAntibacterial activity of standard and N-doped titanium dioxide-coated endotracheal tubes: an in vitro study
Rev Bras Ter Intensiva. 2017;29(1):55-62
DOI 10.5935/0103-507X.20170009
Views0ABSTRACT
Objective:
The aim of this study was to assess the antibacterial activity against Staphylococcus aureus and Pseudomonas aeruginosa of two nanoparticle endotracheal tube coatings with visible light-induced photocatalysis.
Methods:
Two types of titanium dioxide nanoparticles were tested: standard anatase (TiO2) and N-doped TiO2 (N-TiO2). Nanoparticles were placed on the internal surface of a segment of commercial endotracheal tubes, which were loaded on a cellulose acetate filter; control endotracheal tubes were left without a nanoparticle coating. A bacterial inoculum of 150 colony forming units was placed in the endotracheal tubes and then exposed to a fluorescent light source (3700 lux, 300-700 nm wavelength) for 5, 10, 20, 40, 60 and 80 minutes. Colony forming units were counted after 24 hours of incubation at 37°C. Bacterial inactivation was calculated as the percentage reduction of bacterial growth compared to endotracheal tubes not exposed to light.
Results:
In the absence of light, no relevant antibacterial activity was shown against neither strain. For P. aeruginosa, both coatings had a higher bacterial inactivation than controls at any time point (p < 0.001), and no difference was observed between TiO2 and N-TiO2. For S. aureus, inactivation was higher than for controls starting at 5 minutes for N-TiO2 (p = 0.018) and 10 minutes for TiO2 (p = 0.014); inactivation with N-TiO2 was higher than that with TiO2 at 20 minutes (p < 0.001), 40 minutes (p < 0.001) and 60 minutes (p < 0.001).
Conclusions:
Nanosized commercial and N-doped TiO2 inhibit bacterial growth under visible fluorescent light. N-TiO2 has higher antibacterial activity against S. aureus compared to TiO2.
Keywords:Antibacterial agentsCoated materials, biocompatibleIntubation, intratracheal/instrumentationPneumonia, ventilator-associatedTitaniumSee moreViews0Abstract
Original ArticlesAntibacterial activity of standard and N-doped titanium dioxide-coated endotracheal tubes: an in vitro study
Rev Bras Ter Intensiva. 2017;29(1):55-62
DOI 10.5935/0103-507X.20170009
Views0ABSTRACT
Objective:
The aim of this study was to assess the antibacterial activity against Staphylococcus aureus and Pseudomonas aeruginosa of two nanoparticle endotracheal tube coatings with visible light-induced photocatalysis.
Methods:
Two types of titanium dioxide nanoparticles were tested: standard anatase (TiO2) and N-doped TiO2 (N-TiO2). Nanoparticles were placed on the internal surface of a segment of commercial endotracheal tubes, which were loaded on a cellulose acetate filter; control endotracheal tubes were left without a nanoparticle coating. A bacterial inoculum of 150 colony forming units was placed in the endotracheal tubes and then exposed to a fluorescent light source (3700 lux, 300-700 nm wavelength) for 5, 10, 20, 40, 60 and 80 minutes. Colony forming units were counted after 24 hours of incubation at 37°C. Bacterial inactivation was calculated as the percentage reduction of bacterial growth compared to endotracheal tubes not exposed to light.
Results:
In the absence of light, no relevant antibacterial activity was shown against neither strain. For P. aeruginosa, both coatings had a higher bacterial inactivation than controls at any time point (p < 0.001), and no difference was observed between TiO2 and N-TiO2. For S. aureus, inactivation was higher than for controls starting at 5 minutes for N-TiO2 (p = 0.018) and 10 minutes for TiO2 (p = 0.014); inactivation with N-TiO2 was higher than that with TiO2 at 20 minutes (p < 0.001), 40 minutes (p < 0.001) and 60 minutes (p < 0.001).
Conclusions:
Nanosized commercial and N-doped TiO2 inhibit bacterial growth under visible fluorescent light. N-TiO2 has higher antibacterial activity against S. aureus compared to TiO2.
Keywords:Antibacterial agentsCoated materials, biocompatibleIntubation, intratracheal/instrumentationPneumonia, ventilator-associatedTitaniumSee more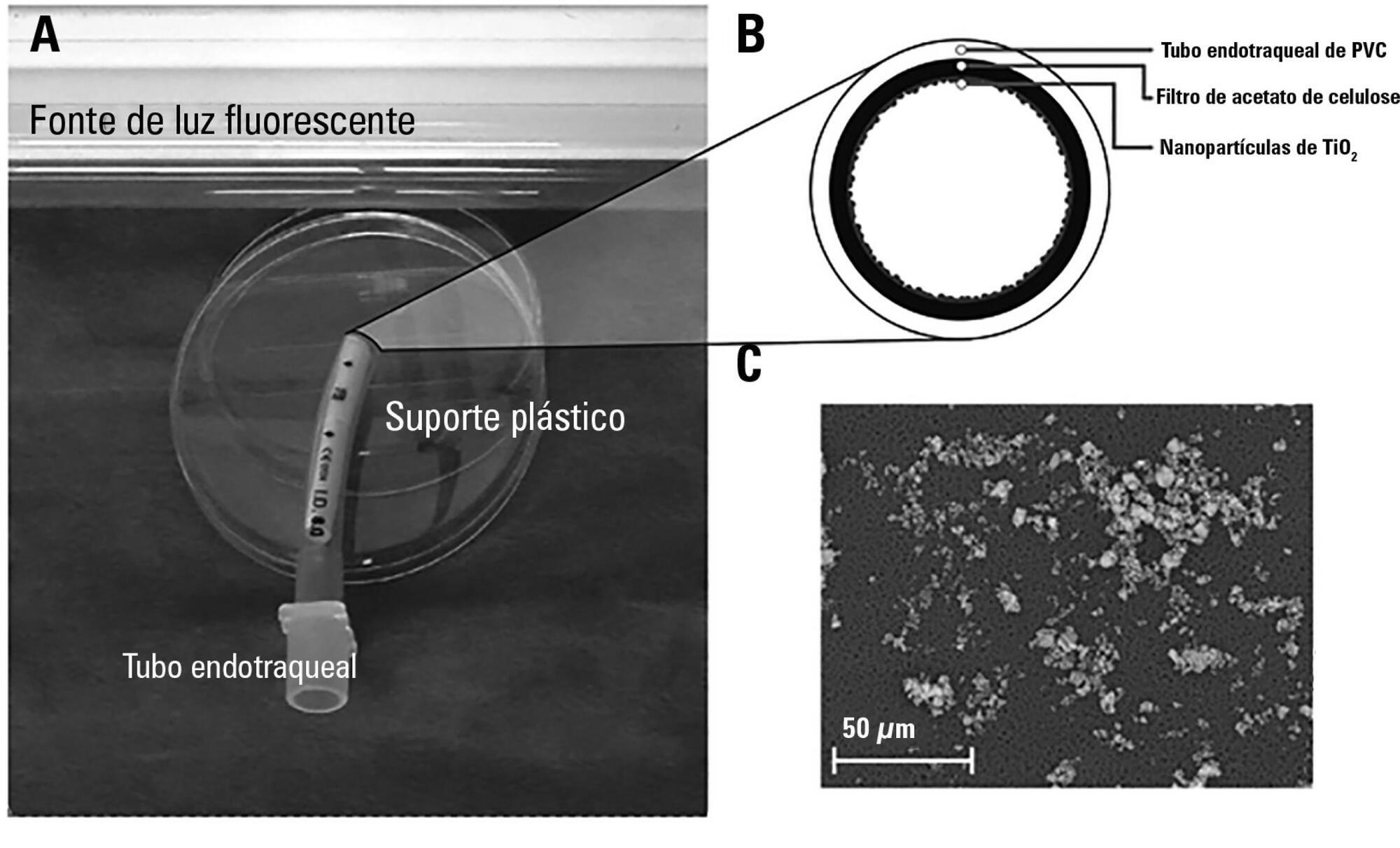
-
Original Articles
Prognostic impact of the time of admission and discharge from the intensive care unit
Rev Bras Ter Intensiva. 2017;29(1):63-69
Abstract
Original ArticlesPrognostic impact of the time of admission and discharge from the intensive care unit
Rev Bras Ter Intensiva. 2017;29(1):63-69
DOI 10.5935/0103-507X.20170010
Views0See moreABSTRACT
Objective:
To determine the impact of the day and time of admission and discharge from the intensive care unit on mortality.
Methods:
Prospective observational study that included patients admitted to the intensive care unit of the Hospital Maciel in Montevideo between April and November 2014.
Results:
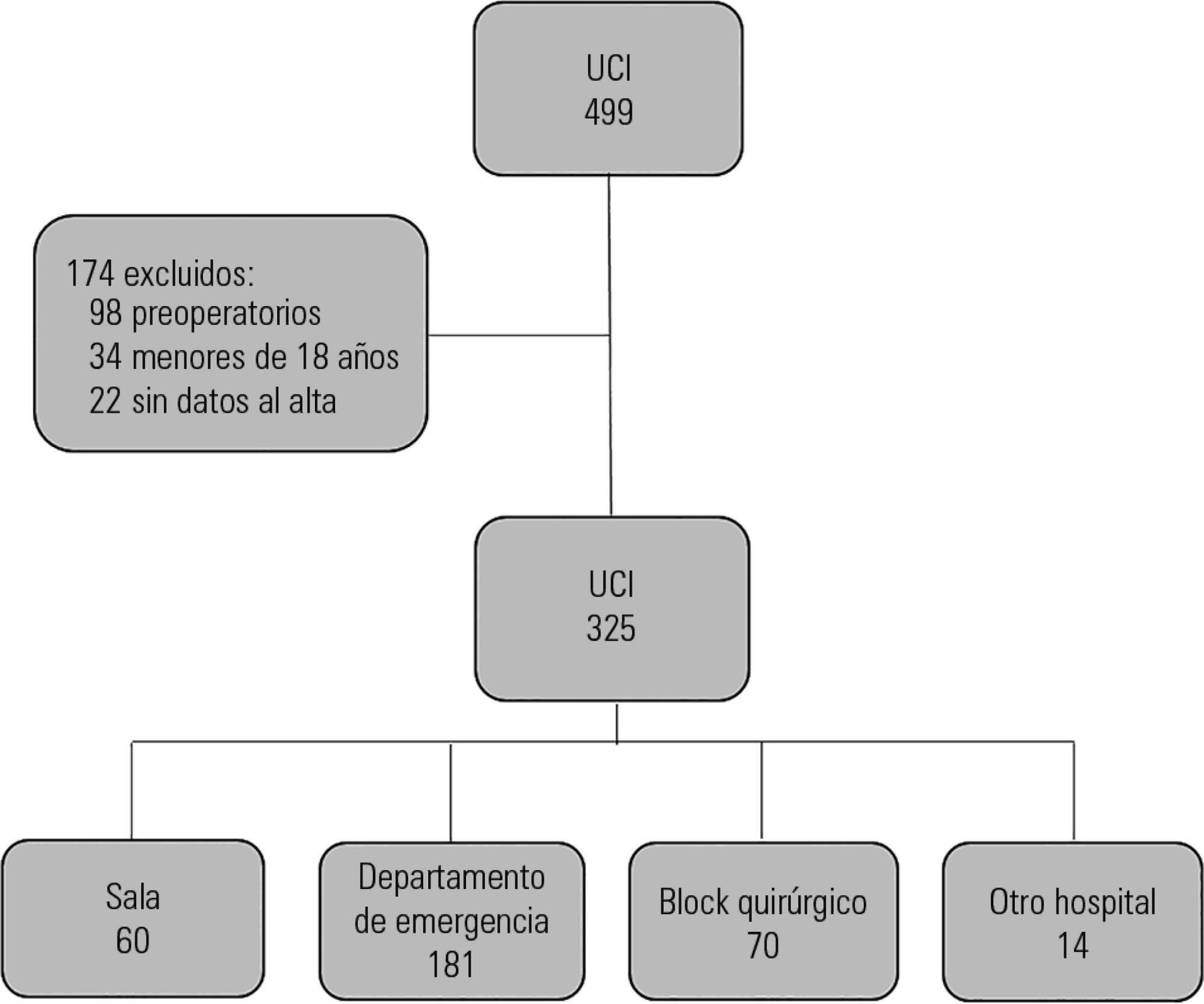
We analyzed 325 patients with an average age of 55 (36 – 71) years and a SAPS II value of 43 (29 – 58) points. No differences were found in the mortality of patients in the intensive care unit when time of admission (35% on the weekend versus 31% on weekdays, p = ns) or the hour of entry (35% at night versus 31% in the daytime, p = ns) were compared. The time of discharge was associated with higher hospital mortality rates (57% for weekend discharges versus 14% for weekday discharges, p = 0.000). The factors independently associated with hospital mortality after discharge from the intensive care unit were age > 50 years (OR 2.4, 95%CI, 1.1 – 5.4) and weekend discharge (OR 7.7, 95%CI, 3.8-15.6).
Conclusion:
This study identified the time of discharge from the intensive care unit as a factor that was independently associated with hospital mortality.
Views0Abstract
Original ArticlesPrognostic impact of the time of admission and discharge from the intensive care unit
Rev Bras Ter Intensiva. 2017;29(1):63-69
DOI 10.5935/0103-507X.20170010
Views0See moreABSTRACT
Objective:
To determine the impact of the day and time of admission and discharge from the intensive care unit on mortality.
Methods:
Prospective observational study that included patients admitted to the intensive care unit of the Hospital Maciel in Montevideo between April and November 2014.
Results:
We analyzed 325 patients with an average age of 55 (36 – 71) years and a SAPS II value of 43 (29 – 58) points. No differences were found in the mortality of patients in the intensive care unit when time of admission (35% on the weekend versus 31% on weekdays, p = ns) or the hour of entry (35% at night versus 31% in the daytime, p = ns) were compared. The time of discharge was associated with higher hospital mortality rates (57% for weekend discharges versus 14% for weekday discharges, p = 0.000). The factors independently associated with hospital mortality after discharge from the intensive care unit were age > 50 years (OR 2.4, 95%CI, 1.1 – 5.4) and weekend discharge (OR 7.7, 95%CI, 3.8-15.6).
Conclusion:
This study identified the time of discharge from the intensive care unit as a factor that was independently associated with hospital mortality.
-
Review Articles
Applicability of respiratory variations in stroke volume and its surrogates for dynamic fluid responsiveness prediction in critically ill patients: a systematic review of the prevalence of required conditions
Rev Bras Ter Intensiva. 2017;29(1):70-76
Abstract
Review ArticlesApplicability of respiratory variations in stroke volume and its surrogates for dynamic fluid responsiveness prediction in critically ill patients: a systematic review of the prevalence of required conditions
Rev Bras Ter Intensiva. 2017;29(1):70-76
DOI 10.5935/0103-507X.20170011
Views0See moreABSTRACT
Objective:
The present systematic review searched for published data on the prevalence of required conditions for proper assessment in critically ill patients.
Methods:
The Medline, Scopus and Web of Science databases were searched to identify studies that evaluated the prevalence of validated conditions for the fluid responsiveness assessment using respiratory variations in the stroke volume or another surrogate in adult critically ill patients. The primary outcome was the suitability of the fluid responsiveness evaluation. The secondary objectives were the type and prevalence of pre-requisites evaluated to define the suitability.
Results:
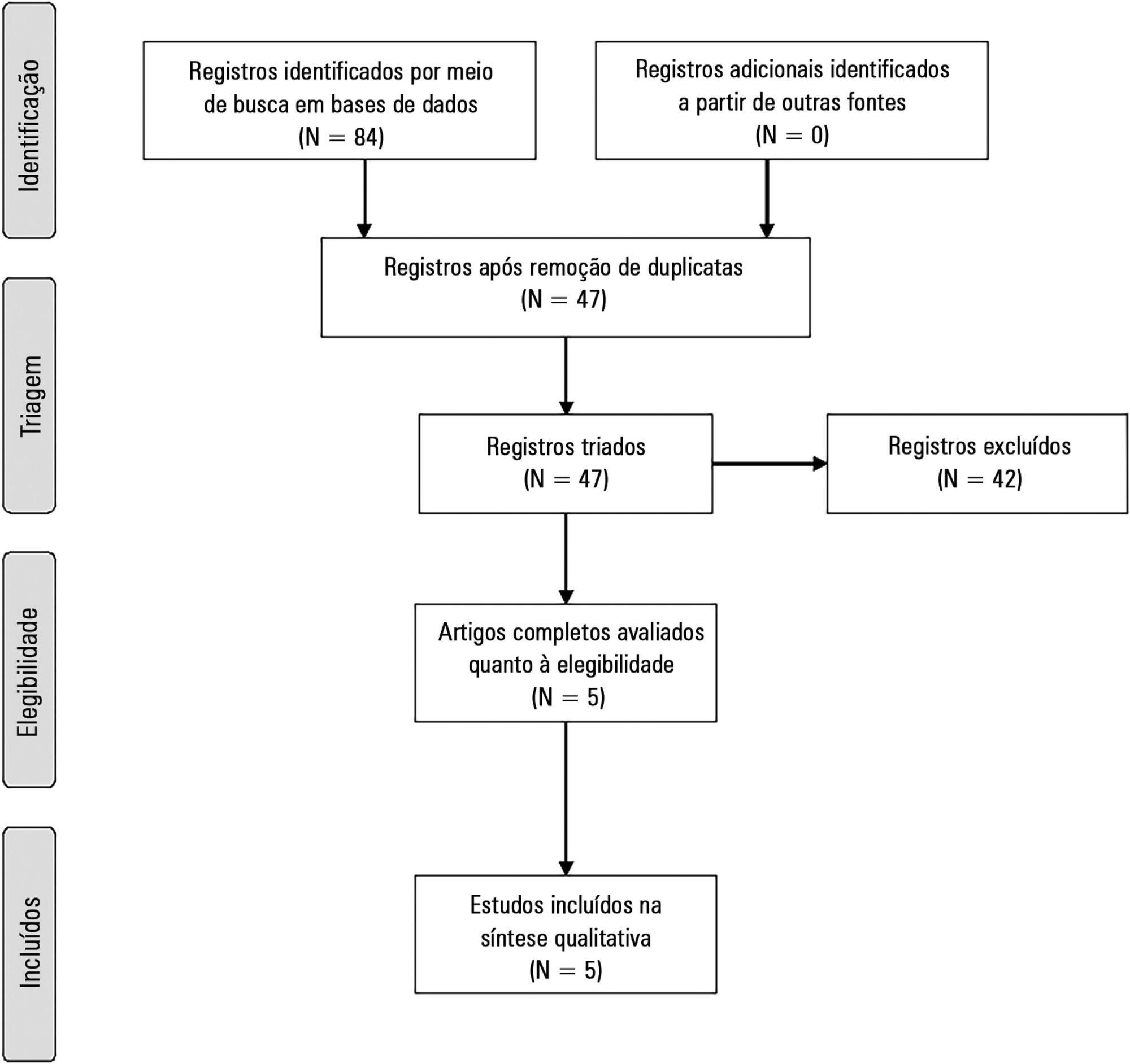
Five studies were included (14,804 patients). High clinical and statistical heterogeneity was observed (I2 = 98.6%), which prevented us from pooling the results into a meaningful summary conclusion. The most frequent limitation identified is the absence of invasive mechanical ventilation with a tidal volume ≥ 8mL/kg. The final suitability for the fluid responsiveness assessment was low (in four studies, it varied between 1.9 to 8.3%, in one study, it was 42.4%).
Conclusion:
Applicability of the dynamic indices of preload responsiveness requiring heart-lung interactions might be limited in daily practice.
Views0Abstract
Review ArticlesApplicability of respiratory variations in stroke volume and its surrogates for dynamic fluid responsiveness prediction in critically ill patients: a systematic review of the prevalence of required conditions
Rev Bras Ter Intensiva. 2017;29(1):70-76
DOI 10.5935/0103-507X.20170011
Views0See moreABSTRACT
Objective:
The present systematic review searched for published data on the prevalence of required conditions for proper assessment in critically ill patients.
Methods:
The Medline, Scopus and Web of Science databases were searched to identify studies that evaluated the prevalence of validated conditions for the fluid responsiveness assessment using respiratory variations in the stroke volume or another surrogate in adult critically ill patients. The primary outcome was the suitability of the fluid responsiveness evaluation. The secondary objectives were the type and prevalence of pre-requisites evaluated to define the suitability.
Results:
Five studies were included (14,804 patients). High clinical and statistical heterogeneity was observed (I2 = 98.6%), which prevented us from pooling the results into a meaningful summary conclusion. The most frequent limitation identified is the absence of invasive mechanical ventilation with a tidal volume ≥ 8mL/kg. The final suitability for the fluid responsiveness assessment was low (in four studies, it varied between 1.9 to 8.3%, in one study, it was 42.4%).
Conclusion:
Applicability of the dynamic indices of preload responsiveness requiring heart-lung interactions might be limited in daily practice.
-
Review Articles
Variable mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(1):77-86
Abstract
Review ArticlesVariable mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(1):77-86
DOI 10.5935/0103-507X.20170012
Views0ABSTRACT
Objective:
To review the literature on the use of variable mechanical ventilation and the main outcomes of this technique.
Methods:
Search, selection, and analysis of all original articles on variable ventilation, without restriction on the period of publication and language, available in the electronic databases LILACS, MEDLINE®, and PubMed, by searching the terms “variable ventilation” OR “noisy ventilation” OR “biologically variable ventilation”.
Results:
A total of 36 studies were selected. Of these, 24 were original studies, including 21 experimental studies and three clinical studies.
Conclusion:
Several experimental studies reported the beneficial effects of distinct variable ventilation strategies on lung function using different models of lung injury and healthy lungs. Variable ventilation seems to be a viable strategy for improving gas exchange and respiratory mechanics and preventing lung injury associated with mechanical ventilation. However, further clinical studies are necessary to assess the potential of variable ventilation strategies for the clinical improvement of patients undergoing mechanical ventilation.
Keywords:acute respiratory distress syndromePulmonary gas exchange/methodsPulmonary ventilation/physiologyVentilation, artificial/methodsSee moreViews0Abstract
Review ArticlesVariable mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(1):77-86
DOI 10.5935/0103-507X.20170012
Views0ABSTRACT
Objective:
To review the literature on the use of variable mechanical ventilation and the main outcomes of this technique.
Methods:
Search, selection, and analysis of all original articles on variable ventilation, without restriction on the period of publication and language, available in the electronic databases LILACS, MEDLINE®, and PubMed, by searching the terms “variable ventilation” OR “noisy ventilation” OR “biologically variable ventilation”.
Results:
A total of 36 studies were selected. Of these, 24 were original studies, including 21 experimental studies and three clinical studies.
Conclusion:
Several experimental studies reported the beneficial effects of distinct variable ventilation strategies on lung function using different models of lung injury and healthy lungs. Variable ventilation seems to be a viable strategy for improving gas exchange and respiratory mechanics and preventing lung injury associated with mechanical ventilation. However, further clinical studies are necessary to assess the potential of variable ventilation strategies for the clinical improvement of patients undergoing mechanical ventilation.
Keywords:acute respiratory distress syndromePulmonary gas exchange/methodsPulmonary ventilation/physiologyVentilation, artificial/methodsSee more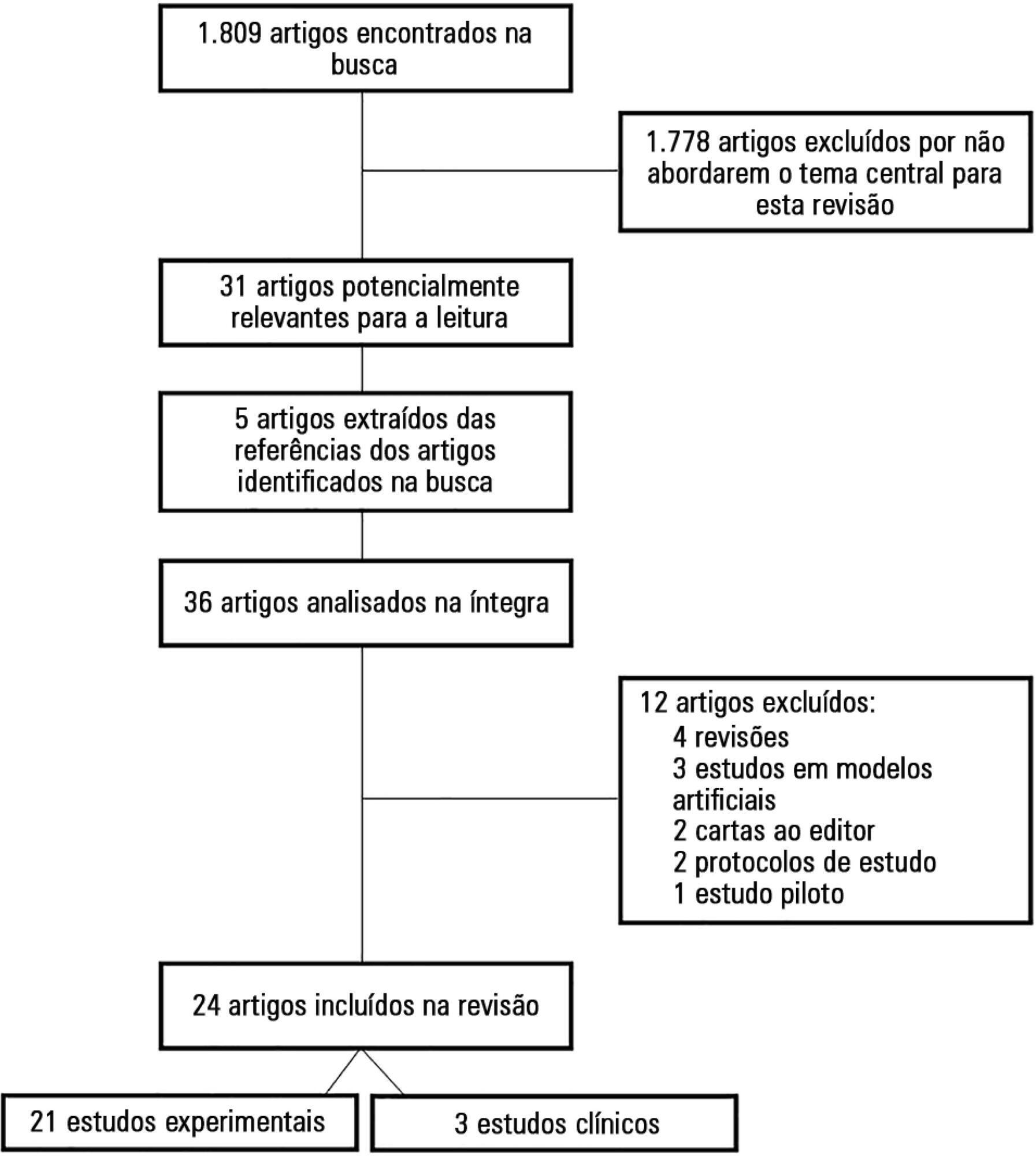
-
Review Articles
Chronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
Abstract
Review ArticlesChronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
DOI 10.5935/0103-507X.20170013
Views1See moreABSTRACT
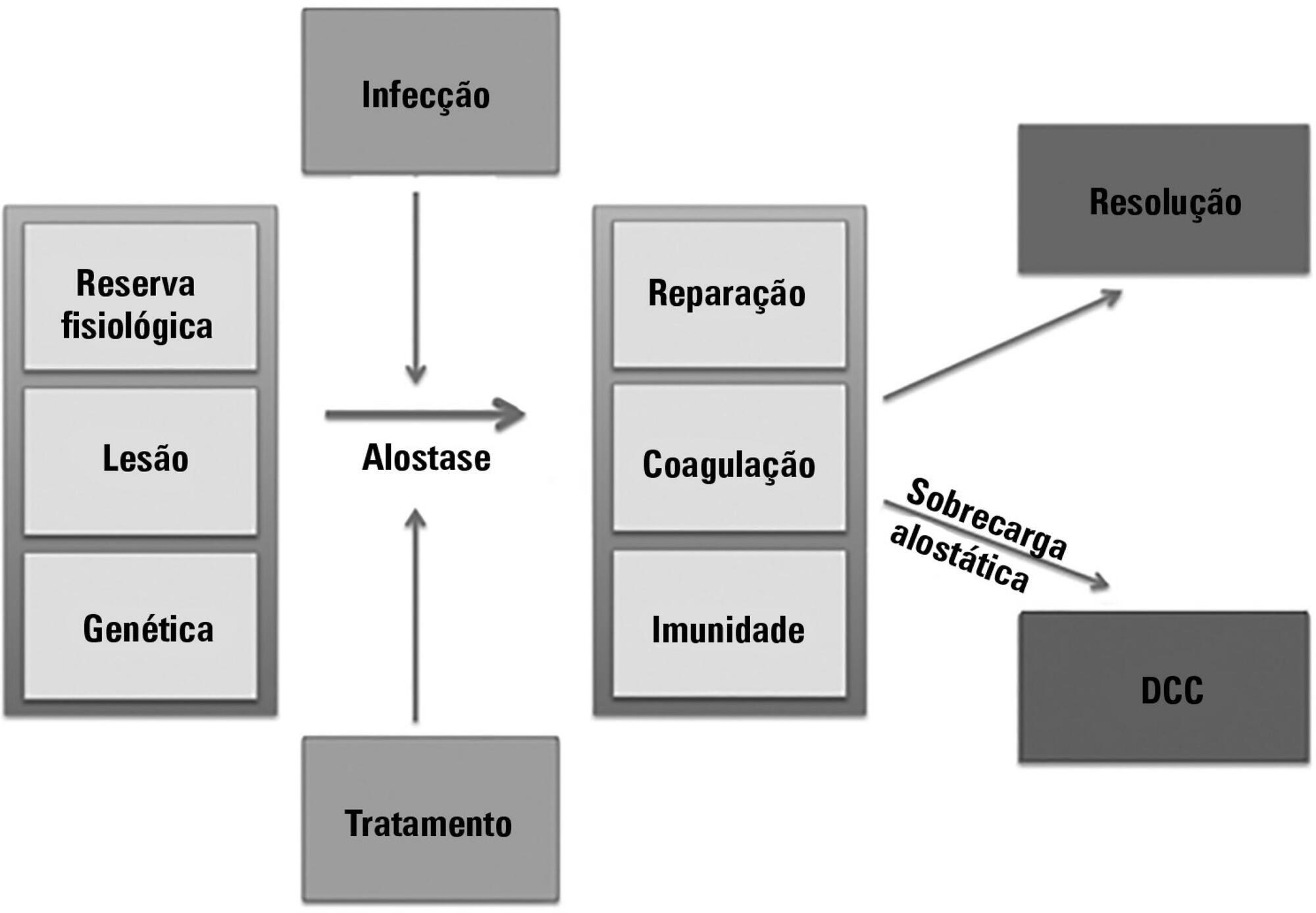
The technological advancements that allow support for organ dysfunction have led to an increase in survival rates for the most critically ill patients. Some of these patients survive the initial acute critical condition but continue to suffer from organ dysfunction and remain in an inflammatory state for long periods of time. This group of critically ill patients has been described since the 1980s and has had different diagnostic criteria over the years. These patients are known to have lengthy hospital stays, undergo significant alterations in muscle and bone metabolism, show immunodeficiency, consume substantial health resources, have reduced functional and cognitive capacity after discharge, create a sizable workload for caregivers, and present high long-term mortality rates. The aim of this review is to report on the most current evidence in terms of the definition, pathophysiology, clinical manifestations, treatment, and prognosis of persistent critical illness.
Views1Abstract
Review ArticlesChronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
DOI 10.5935/0103-507X.20170013
Views1See moreABSTRACT
The technological advancements that allow support for organ dysfunction have led to an increase in survival rates for the most critically ill patients. Some of these patients survive the initial acute critical condition but continue to suffer from organ dysfunction and remain in an inflammatory state for long periods of time. This group of critically ill patients has been described since the 1980s and has had different diagnostic criteria over the years. These patients are known to have lengthy hospital stays, undergo significant alterations in muscle and bone metabolism, show immunodeficiency, consume substantial health resources, have reduced functional and cognitive capacity after discharge, create a sizable workload for caregivers, and present high long-term mortality rates. The aim of this review is to report on the most current evidence in terms of the definition, pathophysiology, clinical manifestations, treatment, and prognosis of persistent critical illness.
-
Review Articles
Expiratory rib cage compression in mechanically ventilated adults: systematic review with meta-analysis
Rev Bras Ter Intensiva. 2017;29(1):96-104
Abstract
Review ArticlesExpiratory rib cage compression in mechanically ventilated adults: systematic review with meta-analysis
Rev Bras Ter Intensiva. 2017;29(1):96-104
DOI 10.5935/0103-507X.20170014
Views0See moreABSTRACT
Objective:
To review the literature on the effects of expiratory rib cage compression on ventilatory mechanics, airway clearance, and oxygen and hemodynamic indices in mechanically ventilated adults.
Methods:
Systematic review with meta-analysis of randomized clinical trials in the databases MEDLINE (via PubMed), EMBASE, Cochrane CENTRAL, PEDro, and LILACS. Studies on adult patients hospitalized in intensive care units and under mechanical ventilation that analyzed the effects of expiratory rib cage compression with respect to a control group (without expiratory rib cage compression) and evaluated the outcomes static and dynamic compliance, sputum volume, systolic blood pressure, diastolic blood pressure, mean arterial pressure, heart rate, peripheral oxygen saturation, and ratio of arterial oxygen partial pressure to fraction of inspired oxygen were included. Experimental studies with animals and those with incomplete data were excluded.
Results:
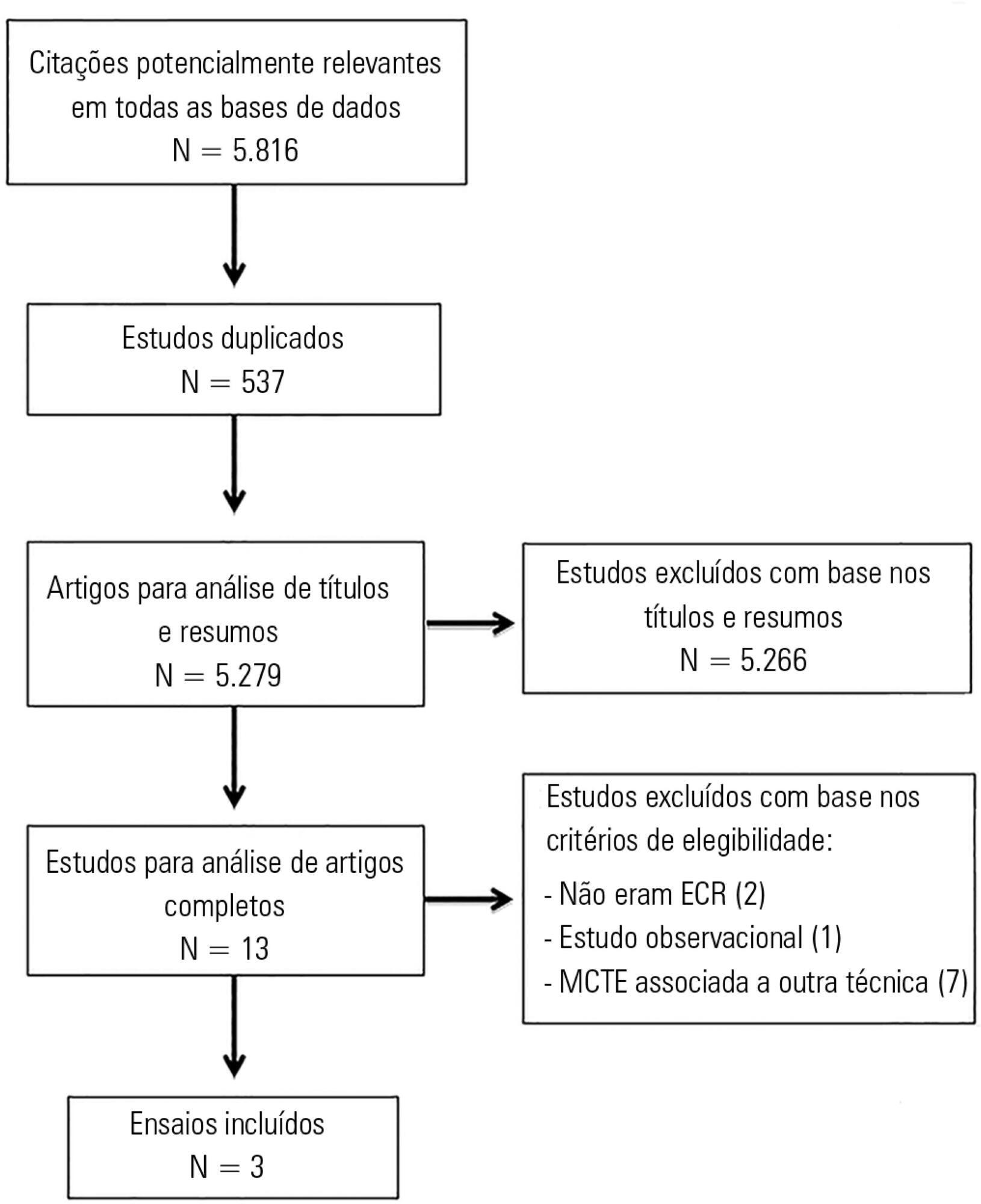
The search strategy produced 5,816 studies, of which only three randomized crossover trials were included, totaling 93 patients. With respect to the outcome of heart rate, values were reduced in the expiratory rib cage compression group compared with the control group [-2.81 bpm (95% confidence interval [95%CI]: -4.73 to 0.89; I2: 0%)]. Regarding dynamic compliance, there was no significant difference between groups [-0.58mL/cmH2O (95%CI: -2.98 to 1.82; I2: 1%)]. Regarding the variables systolic blood pressure and diastolic blood pressure, significant differences were found after descriptive evaluation. However, there was no difference between groups regarding the variables secretion volume, static compliance, ratio of arterial oxygen partial pressure to fraction of inspired oxygen, and peripheral oxygen saturation.
Conclusion:
There is a lack of evidence to support the use of expiratory rib cage compression in routine care, given that the literature on this topic offers low methodological quality and is inconclusive.
Views0Abstract
Review ArticlesExpiratory rib cage compression in mechanically ventilated adults: systematic review with meta-analysis
Rev Bras Ter Intensiva. 2017;29(1):96-104
DOI 10.5935/0103-507X.20170014
Views0See moreABSTRACT
Objective:
To review the literature on the effects of expiratory rib cage compression on ventilatory mechanics, airway clearance, and oxygen and hemodynamic indices in mechanically ventilated adults.
Methods:
Systematic review with meta-analysis of randomized clinical trials in the databases MEDLINE (via PubMed), EMBASE, Cochrane CENTRAL, PEDro, and LILACS. Studies on adult patients hospitalized in intensive care units and under mechanical ventilation that analyzed the effects of expiratory rib cage compression with respect to a control group (without expiratory rib cage compression) and evaluated the outcomes static and dynamic compliance, sputum volume, systolic blood pressure, diastolic blood pressure, mean arterial pressure, heart rate, peripheral oxygen saturation, and ratio of arterial oxygen partial pressure to fraction of inspired oxygen were included. Experimental studies with animals and those with incomplete data were excluded.
Results:
The search strategy produced 5,816 studies, of which only three randomized crossover trials were included, totaling 93 patients. With respect to the outcome of heart rate, values were reduced in the expiratory rib cage compression group compared with the control group [-2.81 bpm (95% confidence interval [95%CI]: -4.73 to 0.89; I2: 0%)]. Regarding dynamic compliance, there was no significant difference between groups [-0.58mL/cmH2O (95%CI: -2.98 to 1.82; I2: 1%)]. Regarding the variables systolic blood pressure and diastolic blood pressure, significant differences were found after descriptive evaluation. However, there was no difference between groups regarding the variables secretion volume, static compliance, ratio of arterial oxygen partial pressure to fraction of inspired oxygen, and peripheral oxygen saturation.
Conclusion:
There is a lack of evidence to support the use of expiratory rib cage compression in routine care, given that the literature on this topic offers low methodological quality and is inconclusive.
-
Case Reports
Use of noninvasive ventilation in severe acute respiratory distress syndrome due to accidental chlorine inhalation: a case report
Rev Bras Ter Intensiva. 2017;29(1):105-110
Abstract
Case ReportsUse of noninvasive ventilation in severe acute respiratory distress syndrome due to accidental chlorine inhalation: a case report
Rev Bras Ter Intensiva. 2017;29(1):105-110
DOI 10.5935/0103-507X.20170015
Views0See moreABSTRACT
Acute respiratory distress syndrome is characterized by diffuse inflammatory lung injury and is classified as mild, moderate, and severe. Clinically, hypoxemia, bilateral opacities in lung images, and decreased pulmonary compliance are observed. Sepsis is one of the most prevalent causes of this condition (30 – 50%). Among the direct causes of acute respiratory distress syndrome, chlorine inhalation is an uncommon cause, generating mucosal and airway irritation in most cases. We present a case of severe acute respiratory distress syndrome after accidental inhalation of chlorine in a swimming pool, with noninvasive ventilation used as a treatment with good response in this case. We classified severe acute respiratory distress syndrome based on an oxygen partial pressure/oxygen inspired fraction ratio <100, although the Berlin classification is limited in considering patients with severe hypoxemia managed exclusively with noninvasive ventilation. The failure rate of noninvasive ventilation in cases of acute respiratory distress syndrome is approximately 52% and is associated with higher mortality. The possible complications of using noninvasive positive-pressure mechanical ventilation in cases of acute respiratory distress syndrome include delays in orotracheal intubation, which is performed in cases of poor clinical condition and with high support pressure levels, and deep inspiratory efforts, generating high tidal volumes and excessive transpulmonary pressures, which contribute to ventilation-related lung injury. Despite these complications, some studies have shown a decrease in the rates of orotracheal intubation in patients with acute respiratory distress syndrome with low severity scores, hemodynamic stability, and the absence of other organ dysfunctions.
Views0Abstract
Case ReportsUse of noninvasive ventilation in severe acute respiratory distress syndrome due to accidental chlorine inhalation: a case report
Rev Bras Ter Intensiva. 2017;29(1):105-110
DOI 10.5935/0103-507X.20170015
Views0See moreABSTRACT
Acute respiratory distress syndrome is characterized by diffuse inflammatory lung injury and is classified as mild, moderate, and severe. Clinically, hypoxemia, bilateral opacities in lung images, and decreased pulmonary compliance are observed. Sepsis is one of the most prevalent causes of this condition (30 – 50%). Among the direct causes of acute respiratory distress syndrome, chlorine inhalation is an uncommon cause, generating mucosal and airway irritation in most cases. We present a case of severe acute respiratory distress syndrome after accidental inhalation of chlorine in a swimming pool, with noninvasive ventilation used as a treatment with good response in this case. We classified severe acute respiratory distress syndrome based on an oxygen partial pressure/oxygen inspired fraction ratio <100, although the Berlin classification is limited in considering patients with severe hypoxemia managed exclusively with noninvasive ventilation. The failure rate of noninvasive ventilation in cases of acute respiratory distress syndrome is approximately 52% and is associated with higher mortality. The possible complications of using noninvasive positive-pressure mechanical ventilation in cases of acute respiratory distress syndrome include delays in orotracheal intubation, which is performed in cases of poor clinical condition and with high support pressure levels, and deep inspiratory efforts, generating high tidal volumes and excessive transpulmonary pressures, which contribute to ventilation-related lung injury. Despite these complications, some studies have shown a decrease in the rates of orotracheal intubation in patients with acute respiratory distress syndrome with low severity scores, hemodynamic stability, and the absence of other organ dysfunctions.

-
Case Reports
Rhabdomyolysis as a manifestation of a metabolic disease: a case report
Rev Bras Ter Intensiva. 2017;29(1):111-114
Abstract
Case ReportsRhabdomyolysis as a manifestation of a metabolic disease: a case report
Rev Bras Ter Intensiva. 2017;29(1):111-114
DOI 10.5935/0103-507X.20170016
Views1ABSTRACT
Rhabdomyolysis is a process of muscle destruction that can present with varying clinical manifestations. In pediatric patients, its main etiology is infectious diseases. We present a previously healthy adolescent who was admitted to our emergency department with a four-day history of myalgia, muscle weakness and dark urine. At presentation, she was dehydrated. Blood analysis revealed acute renal failure and increased muscular enzymes.
She was transferred to our pediatric intensive care unit. Medical therapies for correction of dehydration and the ionic and metabolic consequences of renal failure were performed. Due to oliguria, renal replacement therapy was initiated. An etiological investigation revealed a beta-oxidation defect. Metabolic diseases are a known cause of rhabdomyolysis. Muscular destruction should be diagnosed early in order to avoid its potential consequences. Generally, the treatment of rhabdomyolysis is conservative, although in some situations, a more invasive approach is needed.
Keywords:Case reportsMetabolic diseasesOxidation-reductionRenal insufficiencyRhabdomyolysis/diagnosisRhabdomyolysis/etiologySee moreViews1Abstract
Case ReportsRhabdomyolysis as a manifestation of a metabolic disease: a case report
Rev Bras Ter Intensiva. 2017;29(1):111-114
DOI 10.5935/0103-507X.20170016
Views1ABSTRACT
Rhabdomyolysis is a process of muscle destruction that can present with varying clinical manifestations. In pediatric patients, its main etiology is infectious diseases. We present a previously healthy adolescent who was admitted to our emergency department with a four-day history of myalgia, muscle weakness and dark urine. At presentation, she was dehydrated. Blood analysis revealed acute renal failure and increased muscular enzymes.
She was transferred to our pediatric intensive care unit. Medical therapies for correction of dehydration and the ionic and metabolic consequences of renal failure were performed. Due to oliguria, renal replacement therapy was initiated. An etiological investigation revealed a beta-oxidation defect. Metabolic diseases are a known cause of rhabdomyolysis. Muscular destruction should be diagnosed early in order to avoid its potential consequences. Generally, the treatment of rhabdomyolysis is conservative, although in some situations, a more invasive approach is needed.
Keywords:Case reportsMetabolic diseasesOxidation-reductionRenal insufficiencyRhabdomyolysis/diagnosisRhabdomyolysis/etiologySee more -
Brief Communication
High prevalence of burnout syndrome among intensivists of the city of Porto Alegre
Rev Bras Ter Intensiva. 2017;29(1):115-120
Abstract
Brief CommunicationHigh prevalence of burnout syndrome among intensivists of the city of Porto Alegre
Rev Bras Ter Intensiva. 2017;29(1):115-120
DOI 10.5935/0103-507X.20170017
Views0INTRODUCTIONBurnout syndrome involves emotional exhaustion (EE), depersonalization (DP) and reduced personal achievement (PA).(,) Burnout is associated with absenteeism, physical illnesses, emotional problems, poor work performance and negative attitudes() and may result in decreased quality of medical care.The most widely used burnout syndrome measurement tool is the Maslach Burnout Inventory (MBI).() Variations in burnout prevalence and […]See moreViews0Abstract
Brief CommunicationHigh prevalence of burnout syndrome among intensivists of the city of Porto Alegre
Rev Bras Ter Intensiva. 2017;29(1):115-120
DOI 10.5935/0103-507X.20170017
Views0INTRODUCTIONBurnout syndrome involves emotional exhaustion (EE), depersonalization (DP) and reduced personal achievement (PA).(,) Burnout is associated with absenteeism, physical illnesses, emotional problems, poor work performance and negative attitudes() and may result in decreased quality of medical care.The most widely used burnout syndrome measurement tool is the Maslach Burnout Inventory (MBI).() Variations in burnout prevalence and […]See more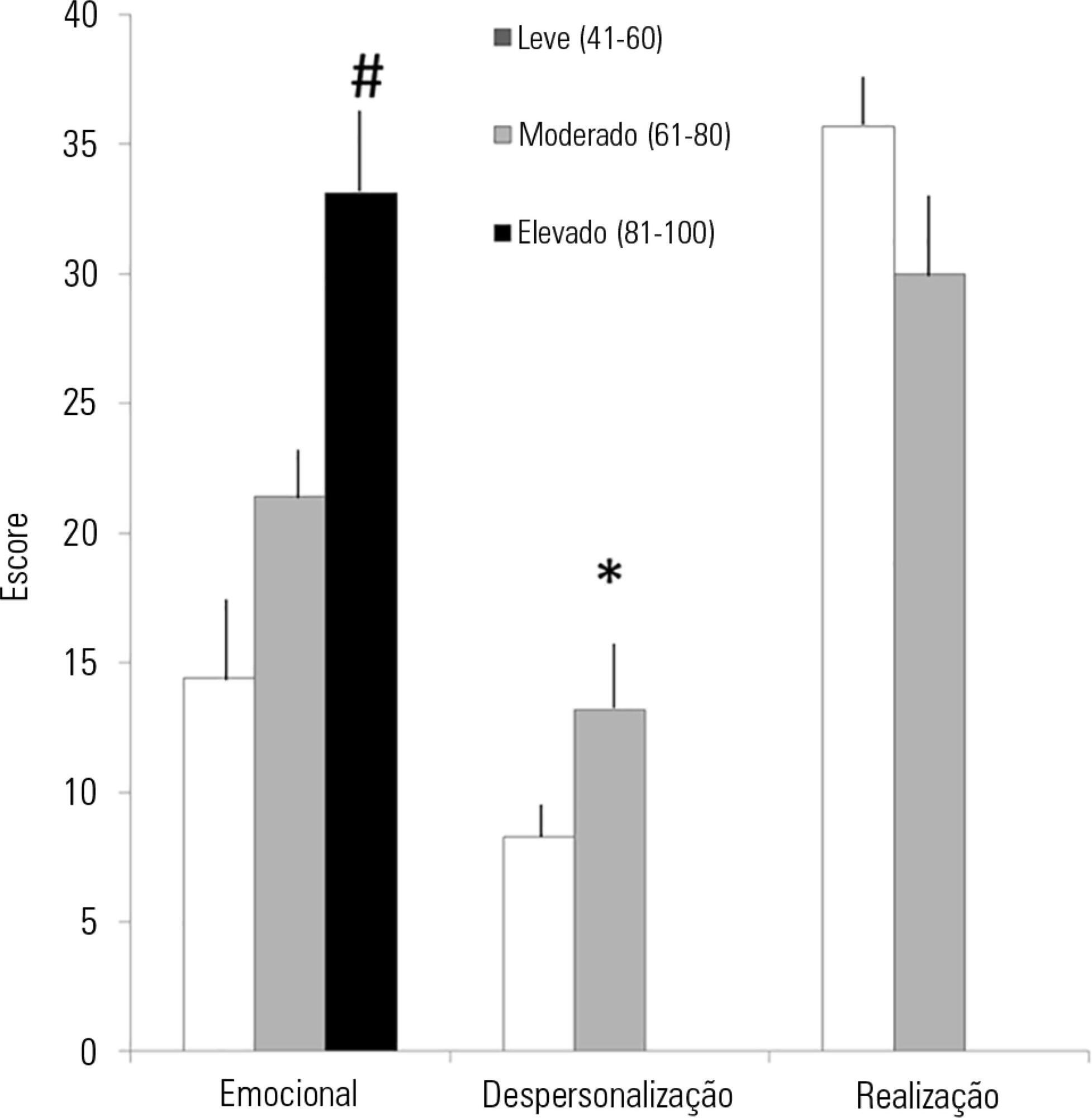
Volume Articles - Critical Care Science (CCS)
