-
Commentaries
Getting a consensus: advantages and disadvantages of Sepsis 3 in the context of middle-income settings
Rev Bras Ter Intensiva. 2016;28(4):361-365
Abstract
CommentariesGetting a consensus: advantages and disadvantages of Sepsis 3 in the context of middle-income settings
Rev Bras Ter Intensiva. 2016;28(4):361-365
DOI 10.5935/0103-507X.20160068
Views0What is new on the Sepsis 3 definitions? Recently the Society of Critical Care Medicine (SCCM) and the European Society of Critical Care Medicine (ESICM) promoted a new consensus conference and published the new sepsis definitions, known as Sepsis 3.() Briefly, the broad definition of sepsis is now “a life-threatening organ dysfunction caused by dysregulated […]See moreViews0

Abstract
CommentariesGetting a consensus: advantages and disadvantages of Sepsis 3 in the context of middle-income settings
Rev Bras Ter Intensiva. 2016;28(4):361-365
DOI 10.5935/0103-507X.20160068
Views0What is new on the Sepsis 3 definitions?Recently the Society of Critical Care Medicine (SCCM) and the European Society of Critical Care Medicine (ESICM) promoted a new consensus conference and published the new sepsis definitions, known as Sepsis 3.()Briefly, the broad definition of sepsis is now “a life-threatening organ dysfunction caused by dysregulated host response […]See more -
Commentaries
The implications of intensive care unit capacity strain for the care of critically ill patients
Rev Bras Ter Intensiva. 2016;28(4):366-368
Abstract
CommentariesThe implications of intensive care unit capacity strain for the care of critically ill patients
Rev Bras Ter Intensiva. 2016;28(4):366-368
DOI 10.5935/0103-507X.20160069
Views0IntroductionEvery intensive care unit (ICU) has an inherent “capacity” or “ability to provide high-quality care for everyone who is or could become a patient in that ICU on a given day”.() As with any operation, an ICU’s capacity is not without bounds. ICU capacity has been likened to a balloon – able to stretch to […]See moreViews0Abstract
CommentariesThe implications of intensive care unit capacity strain for the care of critically ill patients
Rev Bras Ter Intensiva. 2016;28(4):366-368
DOI 10.5935/0103-507X.20160069
Views0IntroductionEvery intensive care unit (ICU) has an inherent “capacity” or “ability to provide high-quality care for everyone who is or could become a patient in that ICU on a given day”.() As with any operation, an ICU’s capacity is not without bounds. ICU capacity has been likened to a balloon – able to stretch to […]See more -
Commentaries
How could we make nutrition in the intensive care unit simple?
Rev Bras Ter Intensiva. 2016;28(4):369-372
Abstract
CommentariesHow could we make nutrition in the intensive care unit simple?
Rev Bras Ter Intensiva. 2016;28(4):369-372
DOI 10.5935/0103-507X.20160070
Views0IntroductionA uniform approach may be applied to any process which may be defined as simple i.e. one which is orderly, easily understood, repeatable and reproducible and not complicated or complex. The approach to nutrition for critically ill patients in the intensive care unit (ICU) cannot be described as uniform or simple for a number of […]See moreViews0Abstract
CommentariesHow could we make nutrition in the intensive care unit simple?
Rev Bras Ter Intensiva. 2016;28(4):369-372
DOI 10.5935/0103-507X.20160070
Views0IntroductionA uniform approach may be applied to any process which may be defined as simple i.e. one which is orderly, easily understood, repeatable and reproducible and not complicated or complex. The approach to nutrition for critically ill patients in the intensive care unit (ICU) cannot be described as uniform or simple for a number of […]See more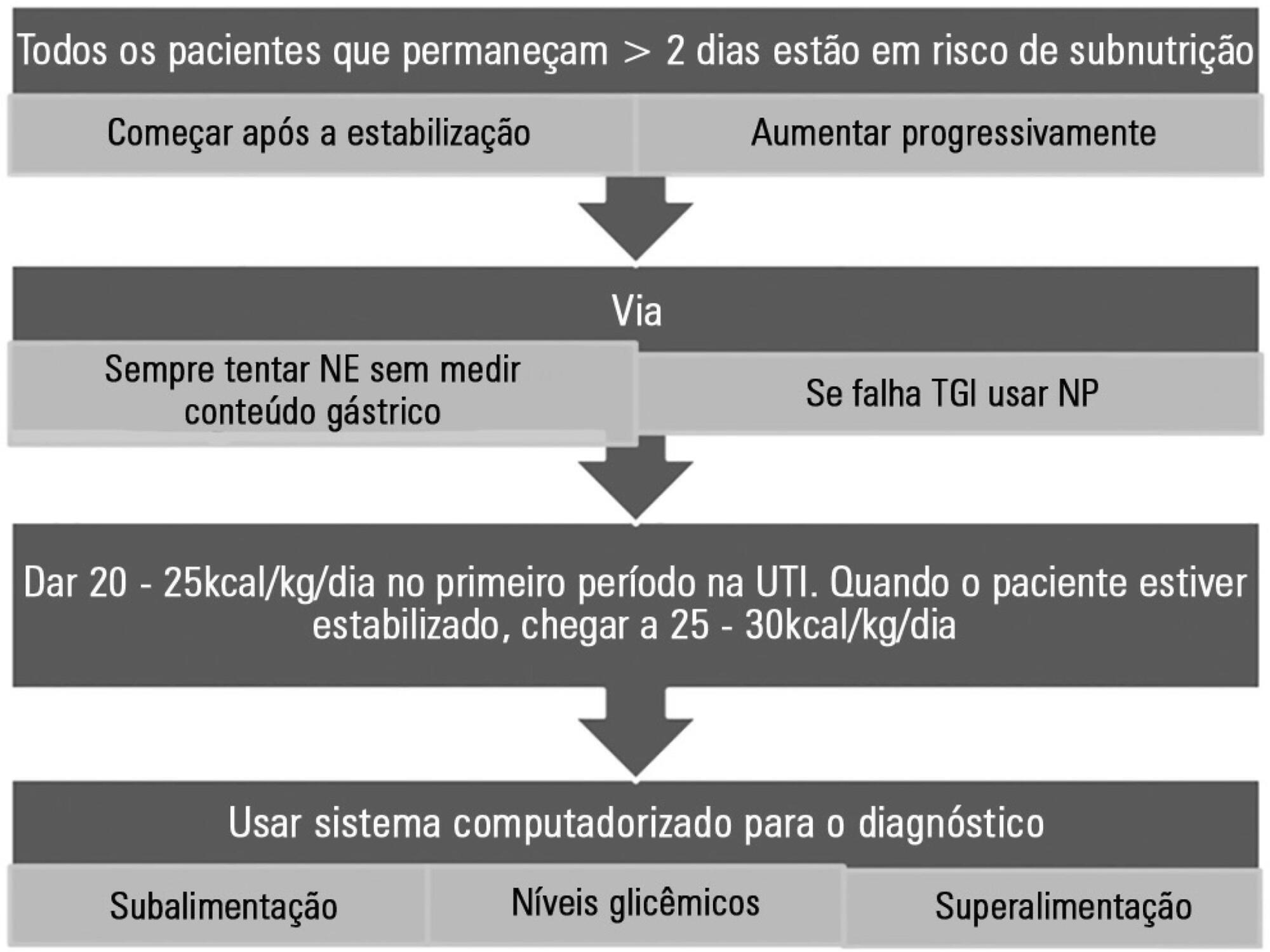
-
Lung protection: an intervention for tidal volume reduction in a teaching intensive care unit
Rev Bras Ter Intensiva. 2016;28(4):373-379
Abstract
Lung protection: an intervention for tidal volume reduction in a teaching intensive care unit
Rev Bras Ter Intensiva. 2016;28(4):373-379
DOI 10.5935/0103-507X.20160067
Views0See moreABSTRACT
Objective:
To determine the effect of feedback and education regarding the use of predicted body weight to adjust tidal volume in a lung-protective mechanical ventilation strategy.
Methods:
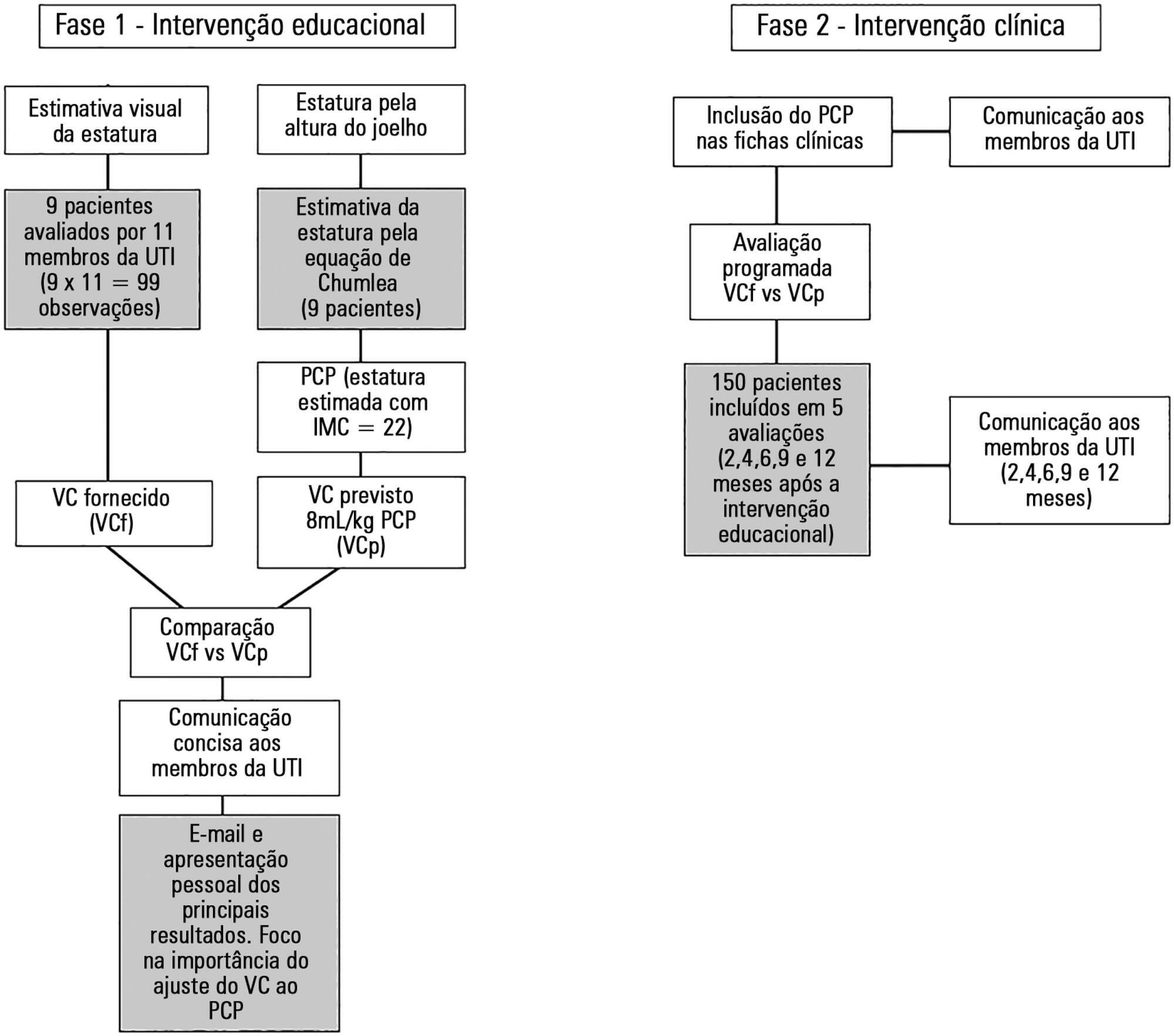
The study was performed from October 2014 to November 2015 (12 months) in a single university polyvalent intensive care unit. We developed a combined intervention (education and feedback), placing particular attention on the importance of adjusting tidal volumes to predicted body weight bedside. In parallel, predicted body weight was estimated from knee height and included in clinical charts.
Results:
One hundred fifty-nine patients were included. Predicted body weight assessed by knee height instead of visual evaluation revealed that the delivered tidal volume was significantly higher than predicted. After the inclusion of predicted body weight, we observed a sustained reduction in delivered tidal volume from a mean (standard error) of 8.97 ± 0.32 to 7.49 ± 0.19mL/kg (p < 0.002). Furthermore, the protocol adherence was subsequently sustained for 12 months (delivered tidal volume 7.49 ± 0.54 versus 7.62 ± 0.20mL/kg; p = 0.103).
Conclusion:
The lack of a reliable method to estimate the predicted body weight is a significant impairment for the application of a worldwide standard of care during mechanical ventilation. A combined intervention based on education and repeated feedbacks promoted sustained tidal volume education during the study period (12 months).
Views0Abstract
Lung protection: an intervention for tidal volume reduction in a teaching intensive care unit
Rev Bras Ter Intensiva. 2016;28(4):373-379
DOI 10.5935/0103-507X.20160067
Views0See moreABSTRACT
Objective:
To determine the effect of feedback and education regarding the use of predicted body weight to adjust tidal volume in a lung-protective mechanical ventilation strategy.
Methods:
The study was performed from October 2014 to November 2015 (12 months) in a single university polyvalent intensive care unit. We developed a combined intervention (education and feedback), placing particular attention on the importance of adjusting tidal volumes to predicted body weight bedside. In parallel, predicted body weight was estimated from knee height and included in clinical charts.
Results:
One hundred fifty-nine patients were included. Predicted body weight assessed by knee height instead of visual evaluation revealed that the delivered tidal volume was significantly higher than predicted. After the inclusion of predicted body weight, we observed a sustained reduction in delivered tidal volume from a mean (standard error) of 8.97 ± 0.32 to 7.49 ± 0.19mL/kg (p < 0.002). Furthermore, the protocol adherence was subsequently sustained for 12 months (delivered tidal volume 7.49 ± 0.54 versus 7.62 ± 0.20mL/kg; p = 0.103).
Conclusion:
The lack of a reliable method to estimate the predicted body weight is a significant impairment for the application of a worldwide standard of care during mechanical ventilation. A combined intervention based on education and repeated feedbacks promoted sustained tidal volume education during the study period (12 months).
-
Original Articles
Currently used dosage regimens of vancomycin fail to achieve therapeutic levels in approximately 40% of intensive care unit patients
Rev Bras Ter Intensiva. 2016;28(4):380-386
Abstract
Original ArticlesCurrently used dosage regimens of vancomycin fail to achieve therapeutic levels in approximately 40% of intensive care unit patients
Rev Bras Ter Intensiva. 2016;28(4):380-386
DOI 10.5935/0103-507X.20160071
Views2See moreABSTRACT
Objective:
This study aimed to assess whether currently used dosages of vancomycin for treatment of serious gram-positive bacterial infections in intensive care unit patients provided initial therapeutic vancomycin trough levels and to examine possible factors associated with the presence of adequate initial vancomycin trough levels in these patients.
Methods:
A prospective descriptive study with convenience sampling was performed. Nursing note and medical record data were collected from September 2013 to July 2014 for patients who met inclusion criteria. Eighty-three patients were included. Initial vancomycin trough levels were obtained immediately before vancomycin fourth dose. Acute kidney injury was defined as an increase of at least 0.3mg/dL in serum creatinine within 48 hours.
Results:
Considering vancomycin trough levels recommended for serious gram-positive infection treatment (15 – 20µg/mL), patients were categorized as presenting with low, adequate, and high vancomycin trough levels (35 [42.2%], 18 [21.7%], and 30 [36.1%] patients, respectively). Acute kidney injury patients had significantly greater vancomycin trough levels (p = 0.0055, with significance for a trend, p = 0.0023).
Conclusion:
Surprisingly, more than 40% of the patients did not reach an effective initial vancomycin trough level. Studies on pharmacokinetic and dosage regimens of vancomycin in intensive care unit patients are necessary to circumvent this high proportion of failures to obtain adequate initial vancomycin trough levels. Vancomycin use without trough serum level monitoring in critically ill patients should be discouraged.
Views2Abstract
Original ArticlesCurrently used dosage regimens of vancomycin fail to achieve therapeutic levels in approximately 40% of intensive care unit patients
Rev Bras Ter Intensiva. 2016;28(4):380-386
DOI 10.5935/0103-507X.20160071
Views2See moreABSTRACT
Objective:
This study aimed to assess whether currently used dosages of vancomycin for treatment of serious gram-positive bacterial infections in intensive care unit patients provided initial therapeutic vancomycin trough levels and to examine possible factors associated with the presence of adequate initial vancomycin trough levels in these patients.
Methods:
A prospective descriptive study with convenience sampling was performed. Nursing note and medical record data were collected from September 2013 to July 2014 for patients who met inclusion criteria. Eighty-three patients were included. Initial vancomycin trough levels were obtained immediately before vancomycin fourth dose. Acute kidney injury was defined as an increase of at least 0.3mg/dL in serum creatinine within 48 hours.
Results:
Considering vancomycin trough levels recommended for serious gram-positive infection treatment (15 – 20µg/mL), patients were categorized as presenting with low, adequate, and high vancomycin trough levels (35 [42.2%], 18 [21.7%], and 30 [36.1%] patients, respectively). Acute kidney injury patients had significantly greater vancomycin trough levels (p = 0.0055, with significance for a trend, p = 0.0023).
Conclusion:
Surprisingly, more than 40% of the patients did not reach an effective initial vancomycin trough level. Studies on pharmacokinetic and dosage regimens of vancomycin in intensive care unit patients are necessary to circumvent this high proportion of failures to obtain adequate initial vancomycin trough levels. Vancomycin use without trough serum level monitoring in critically ill patients should be discouraged.
-
Original Articles
Use of reactive hyperemia – peripheral arterial tonometry and circulating biological markers to predict outcomes in sepsis
Rev Bras Ter Intensiva. 2016;28(4):387-396
Abstract
Original ArticlesUse of reactive hyperemia – peripheral arterial tonometry and circulating biological markers to predict outcomes in sepsis
Rev Bras Ter Intensiva. 2016;28(4):387-396
DOI 10.5935/0103-507X.20160072
Views1See moreABSTRACT
Objective:
To evaluate the usefulness and prognostic value of reactive hyperemia – peripheral arterial tonometry in patients with sepsis. Moreover, we investigated the association of reactive hyperemia – peripheral arterial tonometry results with serum levels of certain inflammatory molecules.
Methods:
Prospective study, conducted in an 18-bed mixed intensive care unit for adults. The exclusion criteria included severe immunosuppression or antibiotic therapy initiated more than 48 hours before assessment. We measured the reactive hyperemia – peripheral arterial tonometry on inclusion (day 1) and on day 3. Interleukin-6, interleukin-10, high-mobility group box 1 protein and soluble ST2 levels were measured in the blood obtained upon inclusion.
Results:
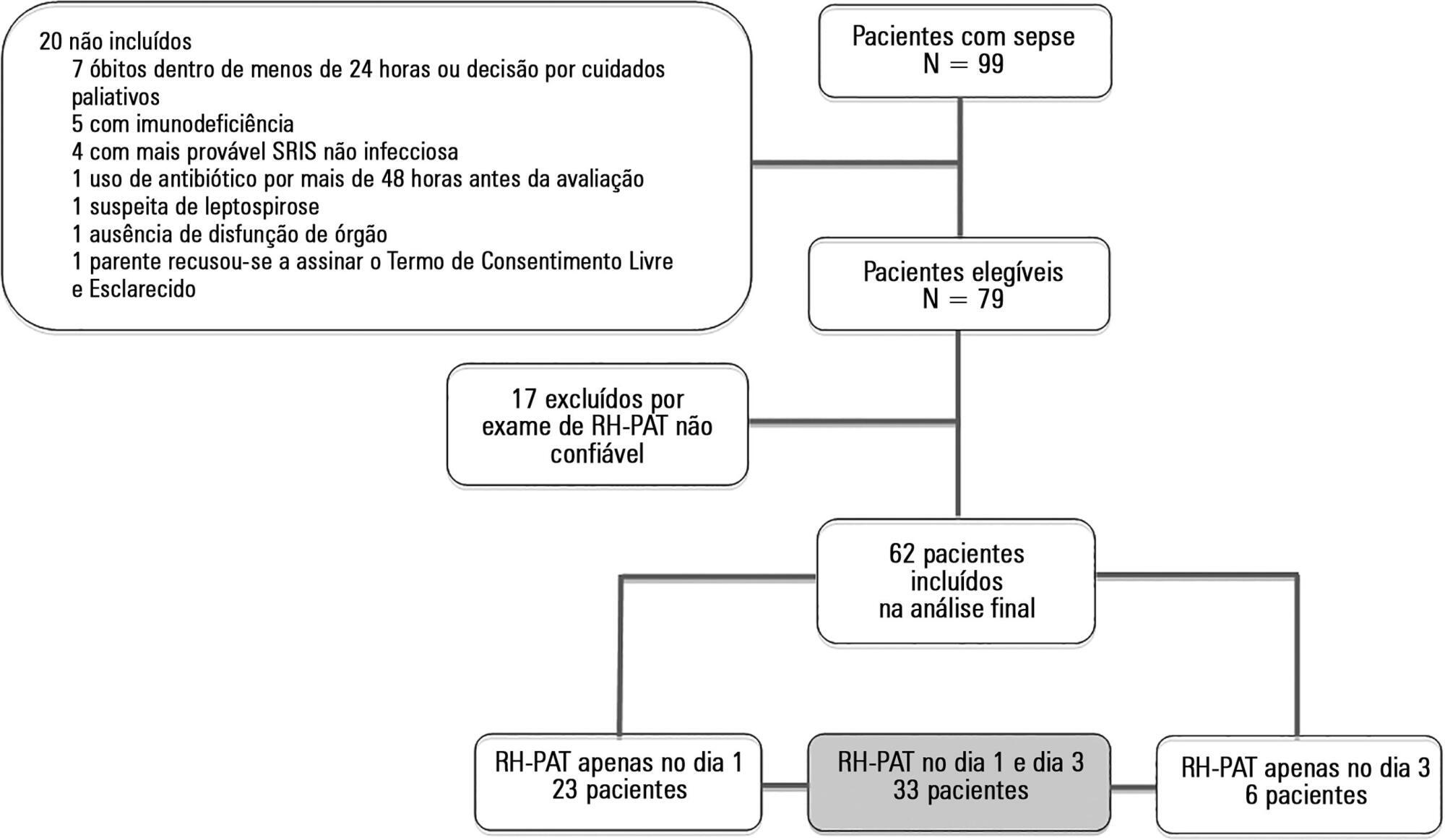
Seventeen of the 79 patients (21.6%) enrolled were determined to have reactive hyperemia – peripheral arterial tonometry signals considered technically unreliable and were excluded from the study. Thus, 62 patients were included in the final analysis, and they underwent a total of 95 reactive hyperemia – peripheral arterial tonometry exams within the first 48 hours after inclusion. The mean age was 51.5 (SD: 18.9), and 49 (62%) of the patients were male. Reactive hyperemia indexes from days 1 and 3 were not associated with vasopressor need, Sequential Organ Failure Assessment score, Acute Physiology and Chronic Health Evaluation II score, or 28-day mortality. Among the patients who died, compared with survivors, there was a significant increase in the day 3 reactive hyperemia index compared with day 1 (p = 0.045). There was a weak negative correlation between the day 1 reactive hyperemia – peripheral arterial tonometry index and the levels of high-mobility group box 1 protein (r = -0.287).
Conclusion:
Technical difficulties and the lack of clear associations between the exam results and clinical severity or outcomes strongly limits the utility of reactive hyperemia – peripheral arterial tonometry in septic patients admitted to the intensive care unit.
Views1Abstract
Original ArticlesUse of reactive hyperemia – peripheral arterial tonometry and circulating biological markers to predict outcomes in sepsis
Rev Bras Ter Intensiva. 2016;28(4):387-396
DOI 10.5935/0103-507X.20160072
Views1See moreABSTRACT
Objective:
To evaluate the usefulness and prognostic value of reactive hyperemia – peripheral arterial tonometry in patients with sepsis. Moreover, we investigated the association of reactive hyperemia – peripheral arterial tonometry results with serum levels of certain inflammatory molecules.
Methods:
Prospective study, conducted in an 18-bed mixed intensive care unit for adults. The exclusion criteria included severe immunosuppression or antibiotic therapy initiated more than 48 hours before assessment. We measured the reactive hyperemia – peripheral arterial tonometry on inclusion (day 1) and on day 3. Interleukin-6, interleukin-10, high-mobility group box 1 protein and soluble ST2 levels were measured in the blood obtained upon inclusion.
Results:
Seventeen of the 79 patients (21.6%) enrolled were determined to have reactive hyperemia – peripheral arterial tonometry signals considered technically unreliable and were excluded from the study. Thus, 62 patients were included in the final analysis, and they underwent a total of 95 reactive hyperemia – peripheral arterial tonometry exams within the first 48 hours after inclusion. The mean age was 51.5 (SD: 18.9), and 49 (62%) of the patients were male. Reactive hyperemia indexes from days 1 and 3 were not associated with vasopressor need, Sequential Organ Failure Assessment score, Acute Physiology and Chronic Health Evaluation II score, or 28-day mortality. Among the patients who died, compared with survivors, there was a significant increase in the day 3 reactive hyperemia index compared with day 1 (p = 0.045). There was a weak negative correlation between the day 1 reactive hyperemia – peripheral arterial tonometry index and the levels of high-mobility group box 1 protein (r = -0.287).
Conclusion:
Technical difficulties and the lack of clear associations between the exam results and clinical severity or outcomes strongly limits the utility of reactive hyperemia – peripheral arterial tonometry in septic patients admitted to the intensive care unit.
-
Original Articles
Factors associated with maternal death in an intensive care unit
Rev Bras Ter Intensiva. 2016;28(4):397-404
Abstract
Original ArticlesFactors associated with maternal death in an intensive care unit
Rev Bras Ter Intensiva. 2016;28(4):397-404
DOI 10.5935/0103-507X.20160073
Views3ABSTRACT
Objective:
To identify factors associated with maternal death in patients admitted to an intensive care unit.
Methods:
A cross-sectional study was conducted in a maternal intensive care unit. All medical records of patients admitted from January 2012 to December 2014 were reviewed. Pregnant and puerperal women were included; those with diagnoses of hydatidiform mole, ectopic pregnancy, or anembryonic pregnancy were excluded, as were patients admitted for non-obstetrical reasons. Death and hospital discharge were the outcomes subjected to comparative analysis.
Results:
A total of 373 patients aged 13 to 45 years were included. The causes for admission to the intensive care unit were hypertensive disorders of pregnancy, followed by heart disease, respiratory failure, and sepsis; complications included acute kidney injury (24.1%), hypotension (15.5%), bleeding (10.2%), and sepsis (6.7%). A total of 28 patients died (7.5%). Causes of death were hemorrhagic shock, multiple organ failure, respiratory failure, and sepsis. The independent risk factors associated with death were acute kidney injury (odds ratio [OR] = 6.77), hypotension (OR = 15.08), and respiratory failure (OR = 3.65).
Conclusion:
The frequency of deaths was low. Acute kidney injury, hypotension, and respiratory insufficiency were independent risk factors for maternal death.
Keywords:Hypertension, pregnancy-inducedIntensive care unitsMaternal death/epidemiologyrisk factorsWomen's healthSee moreViews3Abstract
Original ArticlesFactors associated with maternal death in an intensive care unit
Rev Bras Ter Intensiva. 2016;28(4):397-404
DOI 10.5935/0103-507X.20160073
Views3ABSTRACT
Objective:
To identify factors associated with maternal death in patients admitted to an intensive care unit.
Methods:
A cross-sectional study was conducted in a maternal intensive care unit. All medical records of patients admitted from January 2012 to December 2014 were reviewed. Pregnant and puerperal women were included; those with diagnoses of hydatidiform mole, ectopic pregnancy, or anembryonic pregnancy were excluded, as were patients admitted for non-obstetrical reasons. Death and hospital discharge were the outcomes subjected to comparative analysis.
Results:
A total of 373 patients aged 13 to 45 years were included. The causes for admission to the intensive care unit were hypertensive disorders of pregnancy, followed by heart disease, respiratory failure, and sepsis; complications included acute kidney injury (24.1%), hypotension (15.5%), bleeding (10.2%), and sepsis (6.7%). A total of 28 patients died (7.5%). Causes of death were hemorrhagic shock, multiple organ failure, respiratory failure, and sepsis. The independent risk factors associated with death were acute kidney injury (odds ratio [OR] = 6.77), hypotension (OR = 15.08), and respiratory failure (OR = 3.65).
Conclusion:
The frequency of deaths was low. Acute kidney injury, hypotension, and respiratory insufficiency were independent risk factors for maternal death.
Keywords:Hypertension, pregnancy-inducedIntensive care unitsMaternal death/epidemiologyrisk factorsWomen's healthSee more -
Risk factor paradox in the occurrence of cardiac arrest in acute coronary syndrome patients
Rev Bras Ter Intensiva. 2016;28(4):405-412
Abstract
Risk factor paradox in the occurrence of cardiac arrest in acute coronary syndrome patients
Rev Bras Ter Intensiva. 2016;28(4):405-412
DOI 10.5935/0103-507X.20160065
Views0See moreABSTRACT
Objective:
To compare patients without previously diagnosed cardiovascular risk factors) and patients with one or more risk factors admitted with acute coronary syndrome.
Methods:
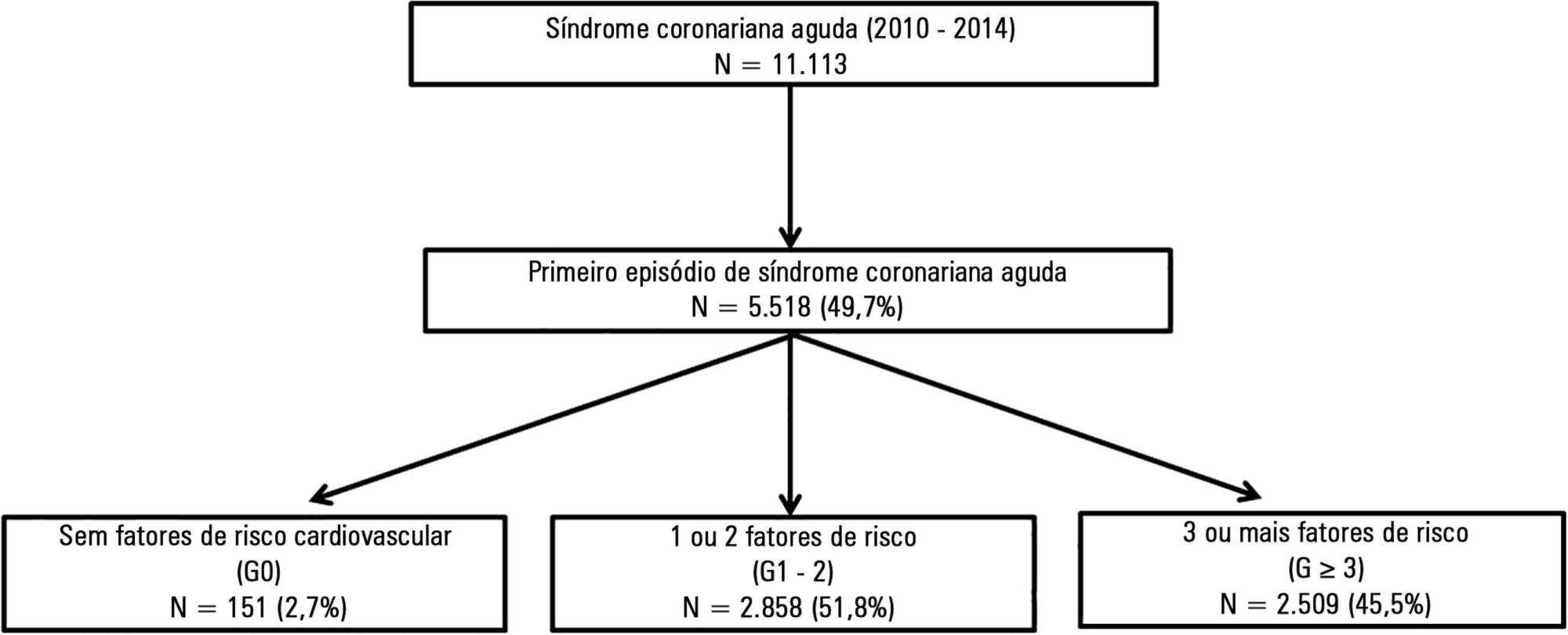
This was a retrospective analysis of patients admitted with first episode of acute coronary syndrome without previous heart disease, who were included in a national acute coronary syndrome registry. The patients were divided according to the number of risk factors, as follows: 0 risk factor (G0), 1 or 2 risk factors (G1 – 2) and 3 or more risk factors (G ≥ 3). Comparative analysis was performed between the three groups, and independent predictors of cardiac arrest and death were studied.
Results:
A total of 5,518 patients were studied, of which 72.2% were male and the mean age was 64 ± 14 years. G0 had a greater incidence of ST-segment elevation myocardial infarction, with the left anterior descending artery being the most frequently involved vessel, and a lower prevalence of multivessel disease. Even though G0 had a lower Killip class (96% in Killip I; p < 0.001) and higher ejection fraction (G0 56 ± 10% versus G1 – 2 and G ≥ 3 53 ± 12%; p = 0.024) on admission, there was a significant higher incidence of cardiac arrest. Multivariate analysis identified the absence of risk factors as an independent predictor of cardiac arrest (OR 2.78; p = 0.019). Hospital mortality was slightly higher in G0, although this difference was not significant. By Cox regression analysis, the number of risk factors was found not to be associated with mortality. Predictors of death at 1 year follow up included age (OR 1.05; p < 0.001), ST-segment elevation myocardial infarction (OR 1.94; p = 0.003) and ejection fraction < 50% (OR 2.34; p < 0.001).
Conclusion:
Even though the group without risk factors was composed of younger patients with fewer comorbidities, better left ventricular function and less extensive coronary disease, the absence of risk factors was an independent predictor of cardiac arrest.
Views0Abstract
Risk factor paradox in the occurrence of cardiac arrest in acute coronary syndrome patients
Rev Bras Ter Intensiva. 2016;28(4):405-412
DOI 10.5935/0103-507X.20160065
Views0See moreABSTRACT
Objective:
To compare patients without previously diagnosed cardiovascular risk factors) and patients with one or more risk factors admitted with acute coronary syndrome.
Methods:
This was a retrospective analysis of patients admitted with first episode of acute coronary syndrome without previous heart disease, who were included in a national acute coronary syndrome registry. The patients were divided according to the number of risk factors, as follows: 0 risk factor (G0), 1 or 2 risk factors (G1 – 2) and 3 or more risk factors (G ≥ 3). Comparative analysis was performed between the three groups, and independent predictors of cardiac arrest and death were studied.
Results:
A total of 5,518 patients were studied, of which 72.2% were male and the mean age was 64 ± 14 years. G0 had a greater incidence of ST-segment elevation myocardial infarction, with the left anterior descending artery being the most frequently involved vessel, and a lower prevalence of multivessel disease. Even though G0 had a lower Killip class (96% in Killip I; p < 0.001) and higher ejection fraction (G0 56 ± 10% versus G1 – 2 and G ≥ 3 53 ± 12%; p = 0.024) on admission, there was a significant higher incidence of cardiac arrest. Multivariate analysis identified the absence of risk factors as an independent predictor of cardiac arrest (OR 2.78; p = 0.019). Hospital mortality was slightly higher in G0, although this difference was not significant. By Cox regression analysis, the number of risk factors was found not to be associated with mortality. Predictors of death at 1 year follow up included age (OR 1.05; p < 0.001), ST-segment elevation myocardial infarction (OR 1.94; p = 0.003) and ejection fraction < 50% (OR 2.34; p < 0.001).
Conclusion:
Even though the group without risk factors was composed of younger patients with fewer comorbidities, better left ventricular function and less extensive coronary disease, the absence of risk factors was an independent predictor of cardiac arrest.
-
Original Articles
Risk factors for agitation in critically ill patients
Rev Bras Ter Intensiva. 2016;28(4):413-419
Abstract
Original ArticlesRisk factors for agitation in critically ill patients
Rev Bras Ter Intensiva. 2016;28(4):413-419
DOI 10.5935/0103-507X.20160074
Views0See moreABSTRACT
Objective:
To evaluate the incidence of agitation in the first 7 days after intensive care unit admission, its risk factors and its associations with clinical outcomes.
Methods:
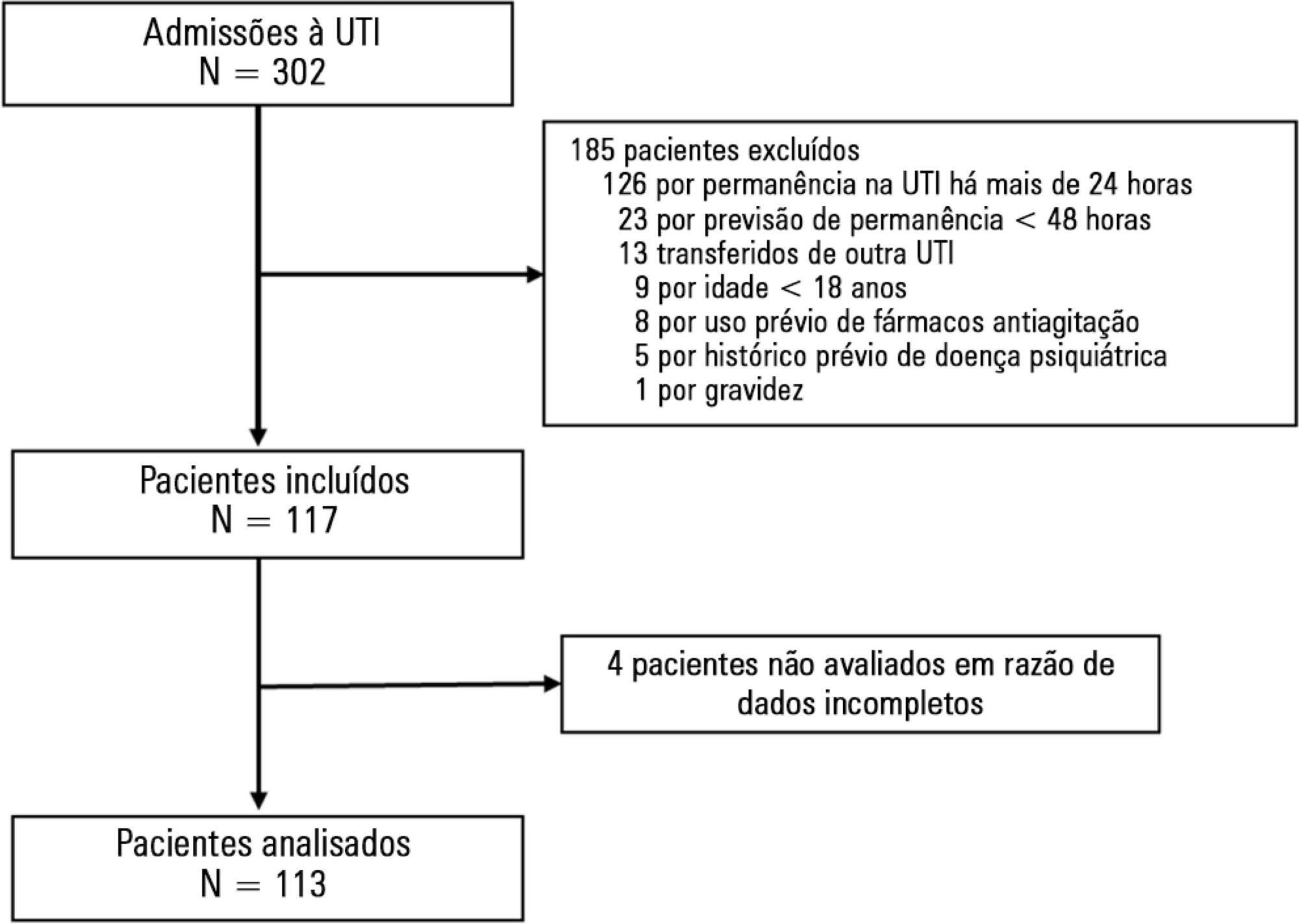
This single-center prospective cohort study included all patients older than 18 years with a predicted stay > 48 hours within the first 24 hours of intensive care unit admission. Agitation was defined as a Richmond Agitation Sedation Scale score ≥ +2, an episode of agitation or the use of a specific medication recorded in patient charts.
Results:
Agitation occurred in 31.8% of the 113 patients. Multivariate analysis showed that delirium [OR = 24.14; CI95% 5.15 – 113.14; p < 0.001], moderate or severe pain [OR = 5.74; CI95% 1.73 - 19.10; p = 0.004], mechanical ventilation [OR = 10.14; CI95% 2.93 - 35.10; p < 0.001], and smoking habits [OR = 4.49; CI95% 1.33 - 15.17; p = 0.015] were independent factors for agitation, while hyperlactatemia was associated with a lower risk [OR = 0.169; CI95% 0.04 - 0.77; p = 0.021]. Agitated patients had fewer mechanical ventilation-free days at day 7 (p = 0.003).
Conclusion:
The incidence of agitation in the first 7 days after admission to the intensive care unit was high. Delirium, moderate/severe pain, mechanical ventilation, and smoking habits were independent risk factors. Agitated patients had fewer ventilator-free days in the first 7 days.
Views0Abstract
Original ArticlesRisk factors for agitation in critically ill patients
Rev Bras Ter Intensiva. 2016;28(4):413-419
DOI 10.5935/0103-507X.20160074
Views0See moreABSTRACT
Objective:
To evaluate the incidence of agitation in the first 7 days after intensive care unit admission, its risk factors and its associations with clinical outcomes.
Methods:
This single-center prospective cohort study included all patients older than 18 years with a predicted stay > 48 hours within the first 24 hours of intensive care unit admission. Agitation was defined as a Richmond Agitation Sedation Scale score ≥ +2, an episode of agitation or the use of a specific medication recorded in patient charts.
Results:
Agitation occurred in 31.8% of the 113 patients. Multivariate analysis showed that delirium [OR = 24.14; CI95% 5.15 – 113.14; p < 0.001], moderate or severe pain [OR = 5.74; CI95% 1.73 - 19.10; p = 0.004], mechanical ventilation [OR = 10.14; CI95% 2.93 - 35.10; p < 0.001], and smoking habits [OR = 4.49; CI95% 1.33 - 15.17; p = 0.015] were independent factors for agitation, while hyperlactatemia was associated with a lower risk [OR = 0.169; CI95% 0.04 - 0.77; p = 0.021]. Agitated patients had fewer mechanical ventilation-free days at day 7 (p = 0.003).
Conclusion:
The incidence of agitation in the first 7 days after admission to the intensive care unit was high. Delirium, moderate/severe pain, mechanical ventilation, and smoking habits were independent risk factors. Agitated patients had fewer ventilator-free days in the first 7 days.
-
Original Articles
Failure to activate the in-hospital emergency team: causes and outcomes
Rev Bras Ter Intensiva. 2016;28(4):420-426
Abstract
Original ArticlesFailure to activate the in-hospital emergency team: causes and outcomes
Rev Bras Ter Intensiva. 2016;28(4):420-426
DOI 10.5935/0103-507X.20160075
Views0See moreABSTRACT
Objective:
To determine the incidence of afferent limb failure of the in-hospital Medical Emergency Team, characterizing it and comparing the mortality between the population experiencing afferent limb failure and the population not experiencing afferent limb failure.
Methods:
A total of 478 activations of the Medical Emergency Team of Hospital Pedro Hispano occurred from January 2013 to July 2015. A sample of 285 activations was obtained after excluding incomplete records and activations for patients with less than 6 hours of hospitalization. The sample was divided into two groups: the group experiencing afferent limb failure and the group not experiencing afferent limb failure of the Medical Emergency Team. Both populations were characterized and compared. Statistical significance was set at p ≤ 0.05.
Result:
Afferent limb failure was observed in 22.1% of activations. The causal analysis revealed significant differences in Medical Emergency Team activation criteria (p = 0.003) in the group experiencing afferent limb failure, with higher rates of Medical Emergency Team activation for cardiac arrest and cardiovascular dysfunction. Regarding patient outcomes, the group experiencing afferent limb failure had higher immediate mortality rates and higher mortality rates at hospital discharge, with no significant differences. No significant differences were found for the other parameters.
Conclusion:
The incidence of cardiac arrest and the mortality rate were higher in patients experiencing failure of the afferent limb of the Medical Emergency Team. This study highlights the need for health units to invest in the training of all healthcare professionals regarding the Medical Emergency Team activation criteria and emergency medical response system operations.
Views0Abstract
Original ArticlesFailure to activate the in-hospital emergency team: causes and outcomes
Rev Bras Ter Intensiva. 2016;28(4):420-426
DOI 10.5935/0103-507X.20160075
Views0See moreABSTRACT
Objective:
To determine the incidence of afferent limb failure of the in-hospital Medical Emergency Team, characterizing it and comparing the mortality between the population experiencing afferent limb failure and the population not experiencing afferent limb failure.
Methods:
A total of 478 activations of the Medical Emergency Team of Hospital Pedro Hispano occurred from January 2013 to July 2015. A sample of 285 activations was obtained after excluding incomplete records and activations for patients with less than 6 hours of hospitalization. The sample was divided into two groups: the group experiencing afferent limb failure and the group not experiencing afferent limb failure of the Medical Emergency Team. Both populations were characterized and compared. Statistical significance was set at p ≤ 0.05.
Result:
Afferent limb failure was observed in 22.1% of activations. The causal analysis revealed significant differences in Medical Emergency Team activation criteria (p = 0.003) in the group experiencing afferent limb failure, with higher rates of Medical Emergency Team activation for cardiac arrest and cardiovascular dysfunction. Regarding patient outcomes, the group experiencing afferent limb failure had higher immediate mortality rates and higher mortality rates at hospital discharge, with no significant differences. No significant differences were found for the other parameters.
Conclusion:
The incidence of cardiac arrest and the mortality rate were higher in patients experiencing failure of the afferent limb of the Medical Emergency Team. This study highlights the need for health units to invest in the training of all healthcare professionals regarding the Medical Emergency Team activation criteria and emergency medical response system operations.
-
Original Articles
Cardiopulmonary resuscitation of adults with in-hospital cardiac arrest using the Utstein style
Rev Bras Ter Intensiva. 2016;28(4):427-435
Abstract
Original ArticlesCardiopulmonary resuscitation of adults with in-hospital cardiac arrest using the Utstein style
Rev Bras Ter Intensiva. 2016;28(4):427-435
DOI 10.5935/0103-507X.20160076
Views0See moreABSTRACT
Objective:
The objective of this study was to analyze the clinical profile of patients with in-hospital cardiac arrest using the Utstein style.
Methods:
This study is an observational, prospective, longitudinal study of patients with cardiac arrest treated in intensive care units over a period of 1 year.
Results:
The study included 89 patients who underwent cardiopulmonary resuscitation maneuvers. The cohort was 51.6% male with a mean age 59.0 years. The episodes occurred during the daytime in 64.6% of cases. Asystole/bradyarrhythmia was the most frequent initial rhythm (42.7%). Most patients who exhibited a spontaneous return of circulation experienced recurrent cardiac arrest, especially within the first 24 hours (61.4%). The mean time elapsed between hospital admission and the occurrence of cardiac arrest was 10.3 days, the mean time between cardiac arrest and cardiopulmonary resuscitation was 0.68 min, the mean time between cardiac arrest and defibrillation was 7.1 min, and the mean duration of cardiopulmonary resuscitation was 16.3 min. Associations between gender and the duration of cardiopulmonary resuscitation (19.2 min in women versus 13.5 min in men, p = 0.02), the duration of cardiopulmonary resuscitation and the return of spontaneous circulation (10.8 min versus 30.7 min, p < 0.001) and heart disease and age (60.6 years versus 53.6, p < 0.001) were identified. The immediate survival rates after cardiac arrest, until hospital discharge and 6 months after discharge were 71%, 9% and 6%, respectively.
Conclusions:
The main initial rhythm detected was asystole/bradyarrhythmia; the interval between cardiac arrest and cardiopulmonary resuscitation was short, but defibrillation was delayed. Women received cardiopulmonary resuscitation for longer periods than men. The in-hospital survival rate was low.
Views0Abstract
Original ArticlesCardiopulmonary resuscitation of adults with in-hospital cardiac arrest using the Utstein style
Rev Bras Ter Intensiva. 2016;28(4):427-435
DOI 10.5935/0103-507X.20160076
Views0See moreABSTRACT
Objective:
The objective of this study was to analyze the clinical profile of patients with in-hospital cardiac arrest using the Utstein style.
Methods:
This study is an observational, prospective, longitudinal study of patients with cardiac arrest treated in intensive care units over a period of 1 year.
Results:
The study included 89 patients who underwent cardiopulmonary resuscitation maneuvers. The cohort was 51.6% male with a mean age 59.0 years. The episodes occurred during the daytime in 64.6% of cases. Asystole/bradyarrhythmia was the most frequent initial rhythm (42.7%). Most patients who exhibited a spontaneous return of circulation experienced recurrent cardiac arrest, especially within the first 24 hours (61.4%). The mean time elapsed between hospital admission and the occurrence of cardiac arrest was 10.3 days, the mean time between cardiac arrest and cardiopulmonary resuscitation was 0.68 min, the mean time between cardiac arrest and defibrillation was 7.1 min, and the mean duration of cardiopulmonary resuscitation was 16.3 min. Associations between gender and the duration of cardiopulmonary resuscitation (19.2 min in women versus 13.5 min in men, p = 0.02), the duration of cardiopulmonary resuscitation and the return of spontaneous circulation (10.8 min versus 30.7 min, p < 0.001) and heart disease and age (60.6 years versus 53.6, p < 0.001) were identified. The immediate survival rates after cardiac arrest, until hospital discharge and 6 months after discharge were 71%, 9% and 6%, respectively.
Conclusions:
The main initial rhythm detected was asystole/bradyarrhythmia; the interval between cardiac arrest and cardiopulmonary resuscitation was short, but defibrillation was delayed. Women received cardiopulmonary resuscitation for longer periods than men. The in-hospital survival rate was low.
-
Original Articles
Sepsis-related acute respiratory distress syndrome in children with cancer: the respiratory dynamics of a devastating condition
Rev Bras Ter Intensiva. 2016;28(4):436-443
Abstract
Original ArticlesSepsis-related acute respiratory distress syndrome in children with cancer: the respiratory dynamics of a devastating condition
Rev Bras Ter Intensiva. 2016;28(4):436-443
DOI 10.5935/0103-507X.20160077
Views0See moreABSTRACT
Objective:
To evaluate the clinical course and respiratory parameters of mechanically ventilated children with cancer suffering from sepsis-related acute respiratory distress syndrome.
Methods:
This 2-year prospective, longitudinal, observational cohort study enrolled 29 children and adolescents. Clinical data, measurements of blood gases and ventilation parameters were collected at four different time points. Fluctuations between measurements as well as differences in estimated means were analyzed by linear mixed models in which death within 28 days from the onset of acute respiratory distress syndrome was the primary endpoint.
Results:
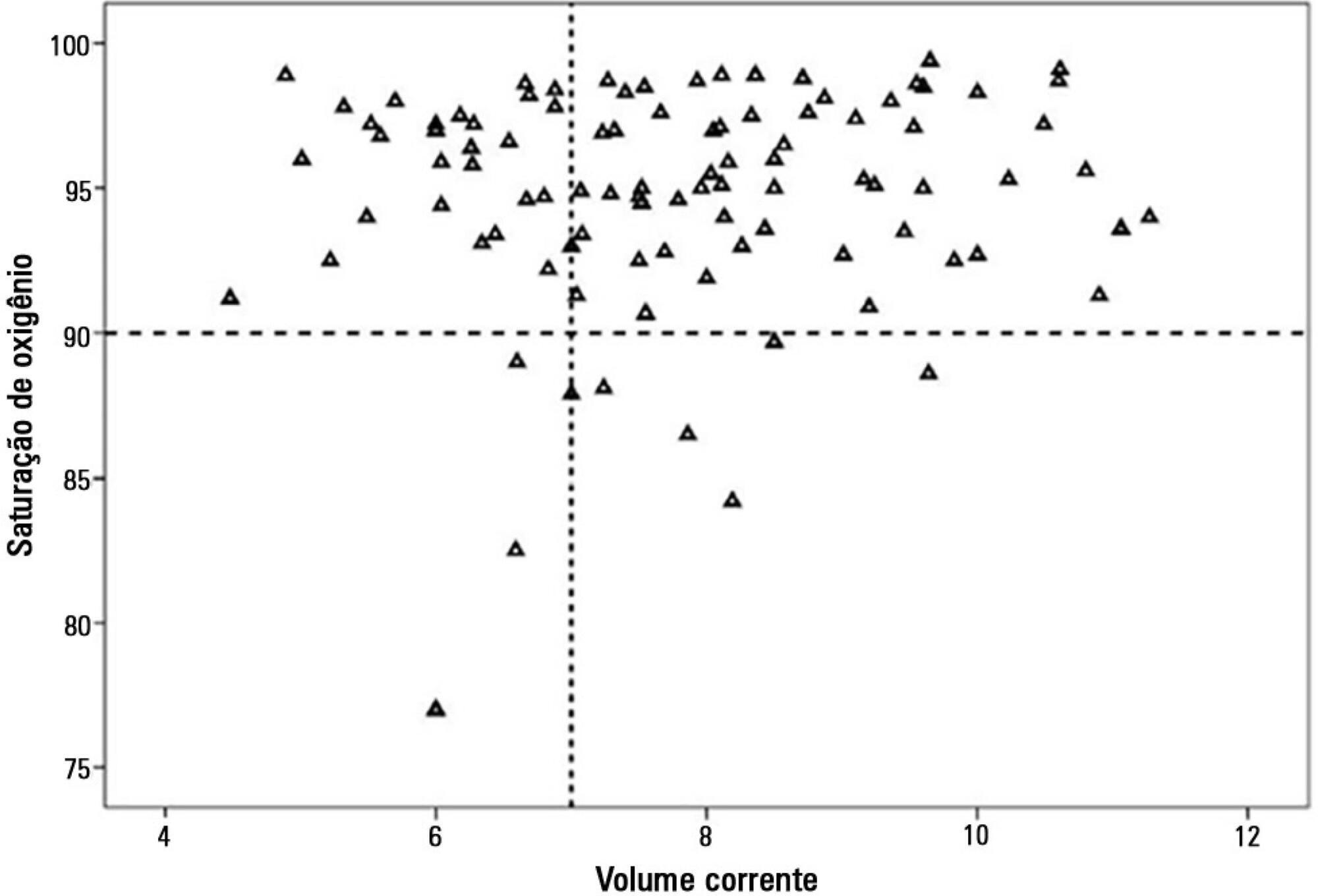
There were 17 deaths within 28 days of acute respiratory distress syndrome onset and another 7 between 29 – 60 days. Only 5 patients survived for more than 60 days. Nine (31%) patients died as a direct consequence of refractory hypoxemia, and the others died of multiple organ failure and catecholamine-refractory shock. In 66% of the measurements, the tidal volume required to obtain oxygen saturation equal to or above 90% was greater than 7mL/kg. The estimated means of dynamic compliance were low and were similar for survivors and non-survivors but with a negative slope between the first and final measurements, accompanied by a negative slope of the tidal volume for non-survivors. Non-survivors were significantly more hypoxemic, with PaO2/FiO2 ratios showing lower estimated means and a negative slope along the four measurements. Peak, expiratory and mean airway pressures showed positive slopes in the non-survivors, who also had more metabolic acidosis.
Conclusions:
In most of our children with cancer, sepsis and acute respiratory distress syndrome progressed with deteriorating ventilation indexes and escalating organic dysfunction, making this triad nearly fatal in children.
Views0Abstract
Original ArticlesSepsis-related acute respiratory distress syndrome in children with cancer: the respiratory dynamics of a devastating condition
Rev Bras Ter Intensiva. 2016;28(4):436-443
DOI 10.5935/0103-507X.20160077
Views0See moreABSTRACT
Objective:
To evaluate the clinical course and respiratory parameters of mechanically ventilated children with cancer suffering from sepsis-related acute respiratory distress syndrome.
Methods:
This 2-year prospective, longitudinal, observational cohort study enrolled 29 children and adolescents. Clinical data, measurements of blood gases and ventilation parameters were collected at four different time points. Fluctuations between measurements as well as differences in estimated means were analyzed by linear mixed models in which death within 28 days from the onset of acute respiratory distress syndrome was the primary endpoint.
Results:
There were 17 deaths within 28 days of acute respiratory distress syndrome onset and another 7 between 29 – 60 days. Only 5 patients survived for more than 60 days. Nine (31%) patients died as a direct consequence of refractory hypoxemia, and the others died of multiple organ failure and catecholamine-refractory shock. In 66% of the measurements, the tidal volume required to obtain oxygen saturation equal to or above 90% was greater than 7mL/kg. The estimated means of dynamic compliance were low and were similar for survivors and non-survivors but with a negative slope between the first and final measurements, accompanied by a negative slope of the tidal volume for non-survivors. Non-survivors were significantly more hypoxemic, with PaO2/FiO2 ratios showing lower estimated means and a negative slope along the four measurements. Peak, expiratory and mean airway pressures showed positive slopes in the non-survivors, who also had more metabolic acidosis.
Conclusions:
In most of our children with cancer, sepsis and acute respiratory distress syndrome progressed with deteriorating ventilation indexes and escalating organic dysfunction, making this triad nearly fatal in children.
-
Original Articles
Sedation protocols versus daily sedation interruption: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2016;28(4):444-451
Abstract
Original ArticlesSedation protocols versus daily sedation interruption: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2016;28(4):444-451
DOI 10.5935/0103-507X.20160078
Views0See moreABSTRACT
Objective:
The aim of this study was to systematically review studies that compared a mild target sedation protocol with daily sedation interruption and to perform a meta-analysis with the data presented in these studies.
Methods:
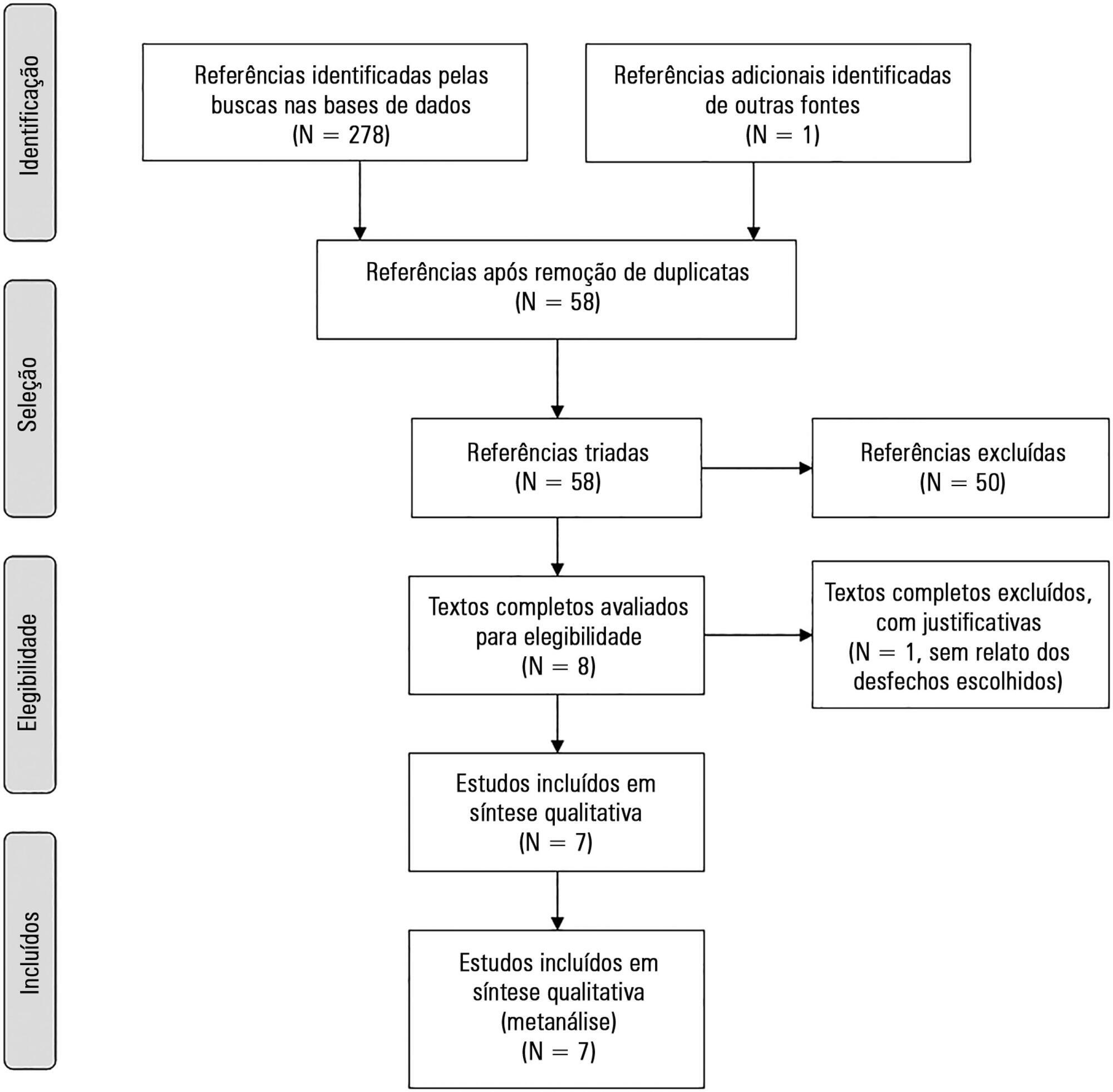
We searched Medline, Scopus and Web of Science databases to identify randomized clinical trials comparing sedation protocols with daily sedation interruption in critically ill patients requiring mechanical ventilation. The primary outcome was mortality in the intensive care unit.
Results:
Seven studies were included, with a total of 892 patients. Mortality in the intensive care unit did not differ between the sedation protocol and daily sedation interruption groups (odds ratio [OR] = 0.81; 95% confidence interval [CI] 0.60 – 1.10; I2 = 0%). Hospital mortality, duration of mechanical ventilation, intensive care unit and hospital length of stay did not differ between the groups either. Sedation protocols were associated with an increase in the number of days free of mechanical ventilation (mean difference = 6.70 days; 95%CI 1.09 – 12.31 days; I2 = 87.2%) and a shorter duration of hospital length of stay (mean difference = -5.05 days, 95%CI -9.98 – -0.11 days; I2 = 69%). There were no differences in regard to accidental extubation, extubation failure and the occurrence of delirium.
Conclusion:
Sedation protocols and daily sedation interruption do not appear to differ in regard to the majority of analyzed outcomes. The only differences found were small and had a high degree of heterogeneity.
Views0Abstract
Original ArticlesSedation protocols versus daily sedation interruption: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2016;28(4):444-451
DOI 10.5935/0103-507X.20160078
Views0See moreABSTRACT
Objective:
The aim of this study was to systematically review studies that compared a mild target sedation protocol with daily sedation interruption and to perform a meta-analysis with the data presented in these studies.
Methods:
We searched Medline, Scopus and Web of Science databases to identify randomized clinical trials comparing sedation protocols with daily sedation interruption in critically ill patients requiring mechanical ventilation. The primary outcome was mortality in the intensive care unit.
Results:
Seven studies were included, with a total of 892 patients. Mortality in the intensive care unit did not differ between the sedation protocol and daily sedation interruption groups (odds ratio [OR] = 0.81; 95% confidence interval [CI] 0.60 – 1.10; I2 = 0%). Hospital mortality, duration of mechanical ventilation, intensive care unit and hospital length of stay did not differ between the groups either. Sedation protocols were associated with an increase in the number of days free of mechanical ventilation (mean difference = 6.70 days; 95%CI 1.09 – 12.31 days; I2 = 87.2%) and a shorter duration of hospital length of stay (mean difference = -5.05 days, 95%CI -9.98 – -0.11 days; I2 = 69%). There were no differences in regard to accidental extubation, extubation failure and the occurrence of delirium.
Conclusion:
Sedation protocols and daily sedation interruption do not appear to differ in regard to the majority of analyzed outcomes. The only differences found were small and had a high degree of heterogeneity.
-
Prone position in patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(4):452-462
Abstract
Prone position in patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(4):452-462
DOI 10.5935/0103-507X.20160066
Views1ABSTRACT
Acute respiratory distress syndrome occupies a great deal of attention in intensive care units. Despite ample knowledge of the physiopathology of this syndrome, the focus in intensive care units consists mostly of life-supporting treatment and avoidance of the side effects of invasive treatments. Although great advances in mechanical ventilation have occurred in the past 20 years, with a significant impact on mortality, the incidence continues to be high. Patients with acute respiratory distress syndrome, especially the most severe cases, often present with refractory hypoxemia due to shunt, which can require additional treatments beyond mechanical ventilation, among which is mechanical ventilation in the prone position. This method, first recommended to improve oxygenation in 1974, can be easily implemented in any intensive care unit with trained personnel.
Prone position has extremely robust bibliographic support. Various randomized clinical studies have demonstrated the effect of prone decubitus on the oxygenation of patients with acute respiratory distress syndrome measured in terms of the PaO2/FiO2 ratio, including its effects on increasing patient survival.
The members of the Respiratory Therapists Committee of the Sociedad Argentina de Terapia Intensiva performed a narrative review with the objective of discovering the available evidence related to the implementation of prone position, changes produced in the respiratory system due to the application of this maneuver, and its impact on mortality. Finally, guidelines are suggested for decision-making.
Keywords:mechanical ventilationProne positionRefractory hypoxemia/etiologyRespiratory distress syndrome, acute/complicationsSee moreViews1Abstract
Prone position in patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(4):452-462
DOI 10.5935/0103-507X.20160066
Views1ABSTRACT
Acute respiratory distress syndrome occupies a great deal of attention in intensive care units. Despite ample knowledge of the physiopathology of this syndrome, the focus in intensive care units consists mostly of life-supporting treatment and avoidance of the side effects of invasive treatments. Although great advances in mechanical ventilation have occurred in the past 20 years, with a significant impact on mortality, the incidence continues to be high. Patients with acute respiratory distress syndrome, especially the most severe cases, often present with refractory hypoxemia due to shunt, which can require additional treatments beyond mechanical ventilation, among which is mechanical ventilation in the prone position. This method, first recommended to improve oxygenation in 1974, can be easily implemented in any intensive care unit with trained personnel.
Prone position has extremely robust bibliographic support. Various randomized clinical studies have demonstrated the effect of prone decubitus on the oxygenation of patients with acute respiratory distress syndrome measured in terms of the PaO2/FiO2 ratio, including its effects on increasing patient survival.
The members of the Respiratory Therapists Committee of the Sociedad Argentina de Terapia Intensiva performed a narrative review with the objective of discovering the available evidence related to the implementation of prone position, changes produced in the respiratory system due to the application of this maneuver, and its impact on mortality. Finally, guidelines are suggested for decision-making.
Keywords:mechanical ventilationProne positionRefractory hypoxemia/etiologyRespiratory distress syndrome, acute/complicationsSee more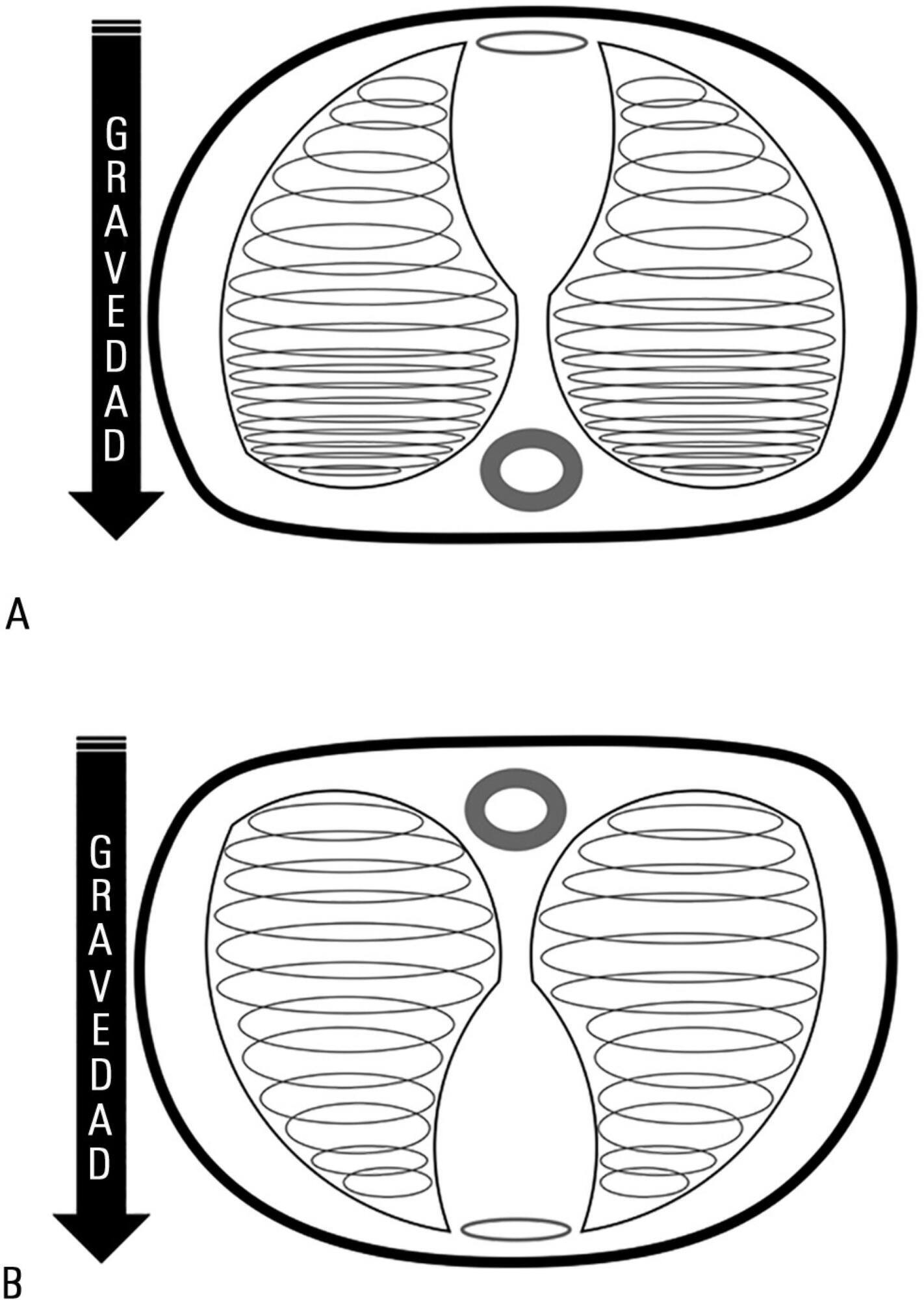
-
Review Articles
Balanced crystalloids for septic shock resuscitation
Rev Bras Ter Intensiva. 2016;28(4):463-471
Abstract
Review ArticlesBalanced crystalloids for septic shock resuscitation
Rev Bras Ter Intensiva. 2016;28(4):463-471
DOI 10.5935/0103-507X.20160079
Views0ABSTRACT
Timely fluid administration is crucial to maintain tissue perfusion in septic shock patients. However, the question concerning which fluid should be used for septic shock resuscitation remains a matter of debate. A growing body of evidence suggests that the type, amount and timing of fluid administration during the course of sepsis may affect patient outcomes. Crystalloids have been recommended as the first-line fluids for septic shock resuscitation. Nevertheless, given the inconclusive nature of the available literature, no definitive recommendations about the most appropriate crystalloid solution can be made. Resuscitation of septic and non-septic critically ill patients with unbalanced crystalloids, mainly 0.9% saline, has been associated with a higher incidence of acid-base balance and electrolyte disorders and might be associated with a higher incidence of acute kidney injury. This can result in greater demand for renal replacement therapy and increased mortality. Balanced crystalloids have been proposed as an alternative to unbalanced solutions in order to mitigate their detrimental effects. Nevertheless, the safety and effectiveness of balanced crystalloids for septic shock resuscitation need to be further addressed in a well-designed, multicenter, pragmatic, randomized controlled trial.
Keywords:Critical care/methodsCritical care/trendsFluid therapy/methodsIsotonic solutions/administration & dosageRehydration solutions/administration & dosageResuscitation/methodsShock, septicSee moreViews0Abstract
Review ArticlesBalanced crystalloids for septic shock resuscitation
Rev Bras Ter Intensiva. 2016;28(4):463-471
DOI 10.5935/0103-507X.20160079
Views0ABSTRACT
Timely fluid administration is crucial to maintain tissue perfusion in septic shock patients. However, the question concerning which fluid should be used for septic shock resuscitation remains a matter of debate. A growing body of evidence suggests that the type, amount and timing of fluid administration during the course of sepsis may affect patient outcomes. Crystalloids have been recommended as the first-line fluids for septic shock resuscitation. Nevertheless, given the inconclusive nature of the available literature, no definitive recommendations about the most appropriate crystalloid solution can be made. Resuscitation of septic and non-septic critically ill patients with unbalanced crystalloids, mainly 0.9% saline, has been associated with a higher incidence of acid-base balance and electrolyte disorders and might be associated with a higher incidence of acute kidney injury. This can result in greater demand for renal replacement therapy and increased mortality. Balanced crystalloids have been proposed as an alternative to unbalanced solutions in order to mitigate their detrimental effects. Nevertheless, the safety and effectiveness of balanced crystalloids for septic shock resuscitation need to be further addressed in a well-designed, multicenter, pragmatic, randomized controlled trial.
Keywords:Critical care/methodsCritical care/trendsFluid therapy/methodsIsotonic solutions/administration & dosageRehydration solutions/administration & dosageResuscitation/methodsShock, septicSee more -
Review Articles
Use of biomarkers in pediatric sepsis: literature review
Rev Bras Ter Intensiva. 2016;28(4):472-482
Abstract
Review ArticlesUse of biomarkers in pediatric sepsis: literature review
Rev Bras Ter Intensiva. 2016;28(4):472-482
DOI 10.5935/0103-507X.20160080
Views0See moreABSTRACT
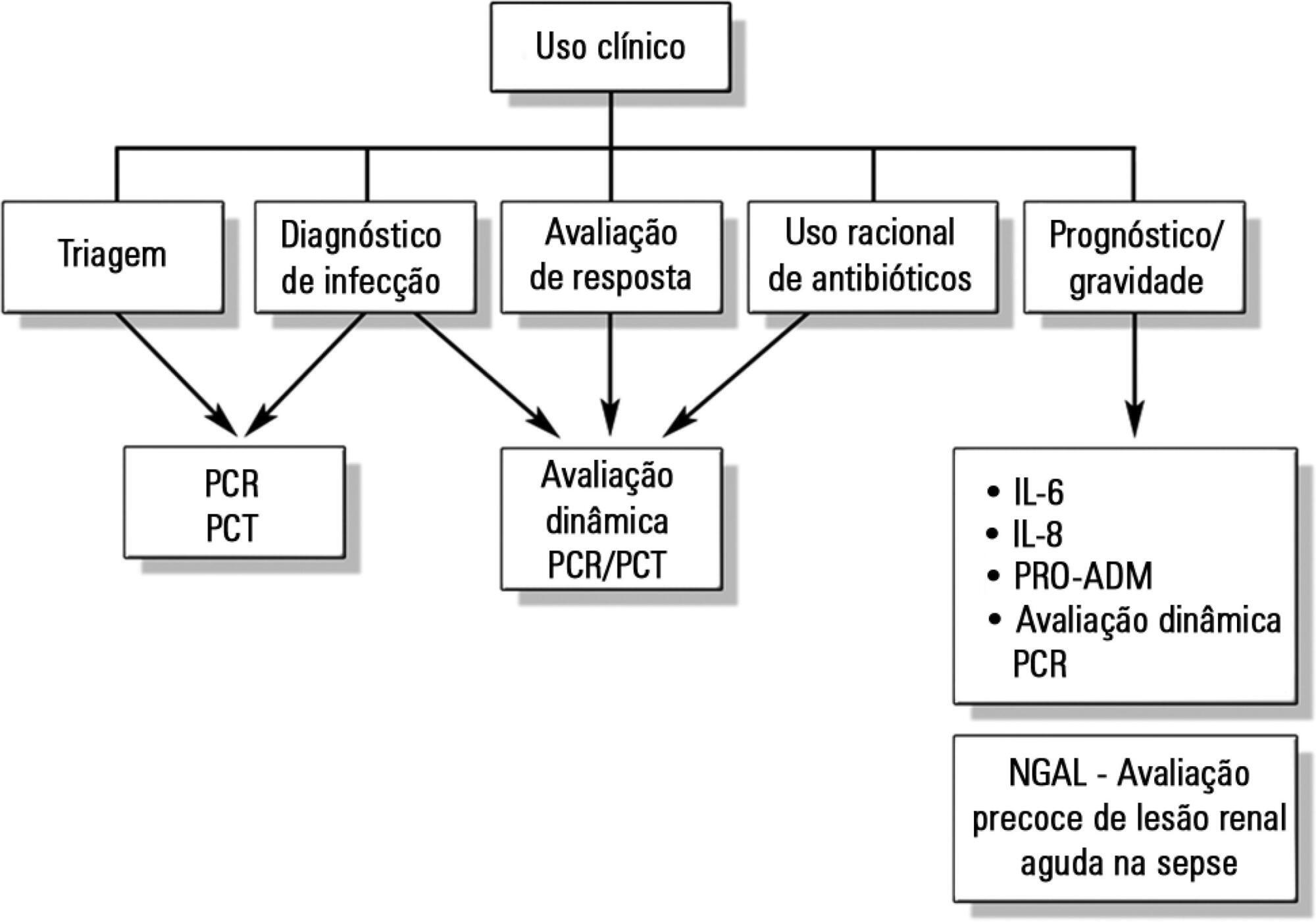
Despite advances in recent years, sepsis is still a leading cause of hospitalization and mortality in infants and children. The presence of biomarkers during the response to an infectious insult makes it possible to use such biomarkers in screening, diagnosis, prognosis (risk stratification), monitoring of therapeutic response, and rational use of antibiotics (for example, the determination of adequate treatment length). Studies of biomarkers in sepsis in children are still relatively scarce. This review addresses the use of biomarkers in sepsis in pediatric patients with emphasis on C-reactive protein, procalcitonin, interleukins 6, 8, and 18, human neutrophil gelatinase, and proadrenomedullin. Assessment of these biomarkers may be useful in the management of pediatric sepsis.
Views0Abstract
Review ArticlesUse of biomarkers in pediatric sepsis: literature review
Rev Bras Ter Intensiva. 2016;28(4):472-482
DOI 10.5935/0103-507X.20160080
Views0See moreABSTRACT
Despite advances in recent years, sepsis is still a leading cause of hospitalization and mortality in infants and children. The presence of biomarkers during the response to an infectious insult makes it possible to use such biomarkers in screening, diagnosis, prognosis (risk stratification), monitoring of therapeutic response, and rational use of antibiotics (for example, the determination of adequate treatment length). Studies of biomarkers in sepsis in children are still relatively scarce. This review addresses the use of biomarkers in sepsis in pediatric patients with emphasis on C-reactive protein, procalcitonin, interleukins 6, 8, and 18, human neutrophil gelatinase, and proadrenomedullin. Assessment of these biomarkers may be useful in the management of pediatric sepsis.
-
Case Reports
Mechanical ventilation in Coffin-Lowry syndrome: a case report
Rev Bras Ter Intensiva. 2016;28(4):483-487
Abstract
Case ReportsMechanical ventilation in Coffin-Lowry syndrome: a case report
Rev Bras Ter Intensiva. 2016;28(4):483-487
DOI 10.5935/0103-507X.20160081
Views0ABSTRACT
We describe a 27-year-old patient with Coffin-Lowry syndrome with severe community pneumonia, septic shock and respiratory failure. We summarize both the mechanical ventilatory assistance and the hospitalization period in the intensive care unit.
Keywords:Abnormalities, multiple/geneticsCase reportsCoffin-Lowry syndrome/diagnosisCoffin-Lowry syndrome/therapyMental retardation, X-linkedSee moreViews0Abstract
Case ReportsMechanical ventilation in Coffin-Lowry syndrome: a case report
Rev Bras Ter Intensiva. 2016;28(4):483-487
DOI 10.5935/0103-507X.20160081
Views0ABSTRACT
We describe a 27-year-old patient with Coffin-Lowry syndrome with severe community pneumonia, septic shock and respiratory failure. We summarize both the mechanical ventilatory assistance and the hospitalization period in the intensive care unit.
Keywords:Abnormalities, multiple/geneticsCase reportsCoffin-Lowry syndrome/diagnosisCoffin-Lowry syndrome/therapyMental retardation, X-linkedSee more
-
Letters to the Editor
To: Ralstonia pickettii bacteremia in hemodialysis patients: a report of two cases
Rev Bras Ter Intensiva. 2016;28(4):488-489
Abstract
Letters to the EditorTo: Ralstonia pickettii bacteremia in hemodialysis patients: a report of two cases
Rev Bras Ter Intensiva. 2016;28(4):488-489
DOI 10.5935/0103-507X.20160082
Views0To the Editor, I recently read the interesting report by Tejera et al. about Ralstonia pickettii, a gram-negative germ formerly of the Burkholderia group that infected two patients on hemodialyisis.() The first was a 65-year-old man with a chronic kidney disease and native arteriovenous fistula who, and was managed in the intensive care unit (ICU) […]See moreViews0Abstract
Letters to the EditorTo: Ralstonia pickettii bacteremia in hemodialysis patients: a report of two cases
Rev Bras Ter Intensiva. 2016;28(4):488-489
DOI 10.5935/0103-507X.20160082
Views0To the Editor, I recently read the interesting report by Tejera et al. about Ralstonia pickettii, a gram-negative germ formerly of the Burkholderia group that infected two patients on hemodialyisis.() The first was a 65-year-old man with a chronic kidney disease and native arteriovenous fistula who, and was managed in the intensive care unit (ICU) […]See more
Volume Articles - Critical Care Science (CCS)
