-
Editorials
Brazilian guidelines in critical care: let’s face this challenge…
Rev Bras Ter Intensiva. 2016;28(3):213-214
Abstract
EditorialsBrazilian guidelines in critical care: let’s face this challenge…
Rev Bras Ter Intensiva. 2016;28(3):213-214
DOI 10.5935/0103-507X.20160046
Views0Clinical practice guidelines are useful tools to improve delivery of the best care, based on the best available evidence, for our patients. They help practitioners to make clinical decisions and might help to ensure the proper allocation of resources in public health policy.() Therefore, health care guidelines and their appropriate implementation are of interest to […]See moreViews0

Abstract
EditorialsBrazilian guidelines in critical care: let’s face this challenge…
Rev Bras Ter Intensiva. 2016;28(3):213-214
DOI 10.5935/0103-507X.20160046
Views0Clinical practice guidelines are useful tools to improve delivery of the best care, based on the best available evidence, for our patients. They help practitioners to make clinical decisions and might help to ensure the proper allocation of resources in public health policy.() Therefore, health care guidelines and their appropriate implementation are of interest to […]See more -
Editorials
Brazilian intensivists: exhausted, but (still) happy with their choice?
Rev Bras Ter Intensiva. 2016;28(3):215-216
Abstract
EditorialsBrazilian intensivists: exhausted, but (still) happy with their choice?
Rev Bras Ter Intensiva. 2016;28(3):215-216
DOI 10.5935/0103-507X.20160047
Views0Burnout syndrome has gained increasing attention since the term was coined by Freudenberger in 1974.() It is amazing that the first systematic description of occupational physical or mental burnout was provided more than two centuries after the modern contextualization of work.() It is even more astonishing that more than 40 years have passed without any […]See moreViews0Abstract
EditorialsBrazilian intensivists: exhausted, but (still) happy with their choice?
Rev Bras Ter Intensiva. 2016;28(3):215-216
DOI 10.5935/0103-507X.20160047
Views0Burnout syndrome has gained increasing attention since the term was coined by Freudenberger in 1974.() It is amazing that the first systematic description of occupational physical or mental burnout was provided more than two centuries after the modern contextualization of work.() It is even more astonishing that more than 40 years have passed without any […]See more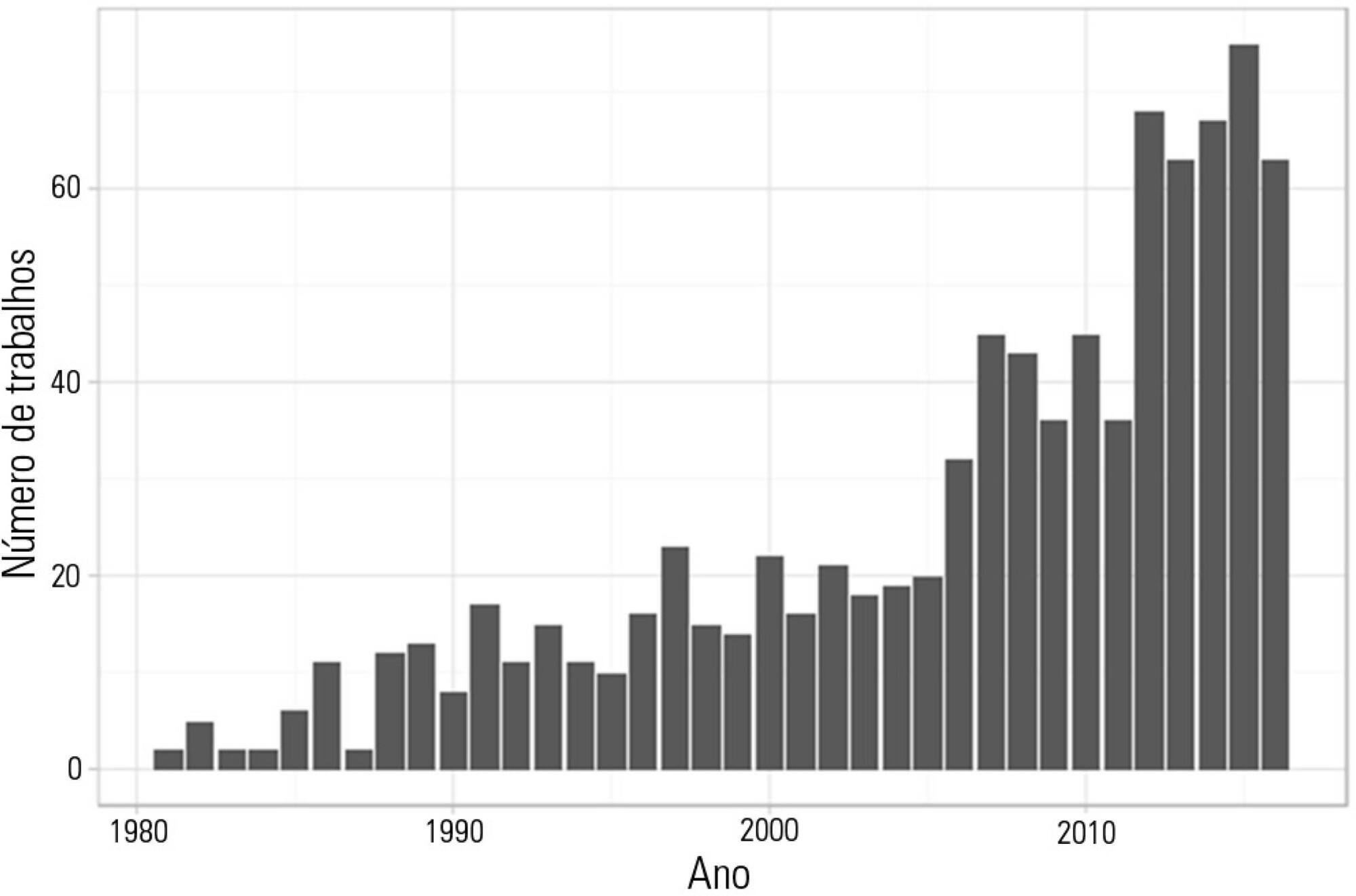
-
Editorials
Advances in performance, more benefits… the perspectives of rapid response teams
Rev Bras Ter Intensiva. 2016;28(3):217-219
Abstract
EditorialsAdvances in performance, more benefits… the perspectives of rapid response teams
Rev Bras Ter Intensiva. 2016;28(3):217-219
DOI 10.5935/0103-507X.20160048
Views0Rapid response teams (RRT) emerged in 1990 with the goals of improving the identification of ward patients with clinical deterioration and offering, based on this identification, early intervention.(–) An RRT is activated according to previously defined triggers, traditionally vital signs, by themselves or as part of aggregated scores, other clinical changes, such as seizures, or […]See moreViews0Abstract
EditorialsAdvances in performance, more benefits… the perspectives of rapid response teams
Rev Bras Ter Intensiva. 2016;28(3):217-219
DOI 10.5935/0103-507X.20160048
Views0Rapid response teams (RRT) emerged in 1990 with the goals of improving the identification of ward patients with clinical deterioration and offering, based on this identification, early intervention.(–) An RRT is activated according to previously defined triggers, traditionally vital signs, by themselves or as part of aggregated scores, other clinical changes, such as seizures, or […]See more -
Special Articles
Guidelines for the assessment and acceptance of potential brain-dead organ donors
Rev Bras Ter Intensiva. 2016;28(3):220-255
Abstract
Special ArticlesGuidelines for the assessment and acceptance of potential brain-dead organ donors
Rev Bras Ter Intensiva. 2016;28(3):220-255
DOI 10.5935/0103-507X.20160049
Views0See moreABSTRACT
Organ transplantation is the only alternative for many patients with terminal diseases. The increasing disproportion between the high demand for organ transplants and the low rate of transplants actually performed is worrisome. Some of the causes of this disproportion are errors in the identification of potential organ donors and in the determination of contraindications by the attending staff. Therefore, the aim of the present document is to provide guidelines for intensive care multi-professional staffs for the recognition, assessment and acceptance of potential organ donors.
Views0Abstract
Special ArticlesGuidelines for the assessment and acceptance of potential brain-dead organ donors
Rev Bras Ter Intensiva. 2016;28(3):220-255
DOI 10.5935/0103-507X.20160049
Views0See moreABSTRACT
Organ transplantation is the only alternative for many patients with terminal diseases. The increasing disproportion between the high demand for organ transplants and the low rate of transplants actually performed is worrisome. Some of the causes of this disproportion are errors in the identification of potential organ donors and in the determination of contraindications by the attending staff. Therefore, the aim of the present document is to provide guidelines for intensive care multi-professional staffs for the recognition, assessment and acceptance of potential organ donors.
-
Special Articles
Different research designs and their characteristics in intensive care
Rev Bras Ter Intensiva. 2016;28(3):256-260
Abstract
Special ArticlesDifferent research designs and their characteristics in intensive care
Rev Bras Ter Intensiva. 2016;28(3):256-260
DOI 10.5935/0103-507X.20160050
Views0See moreABSTRACT
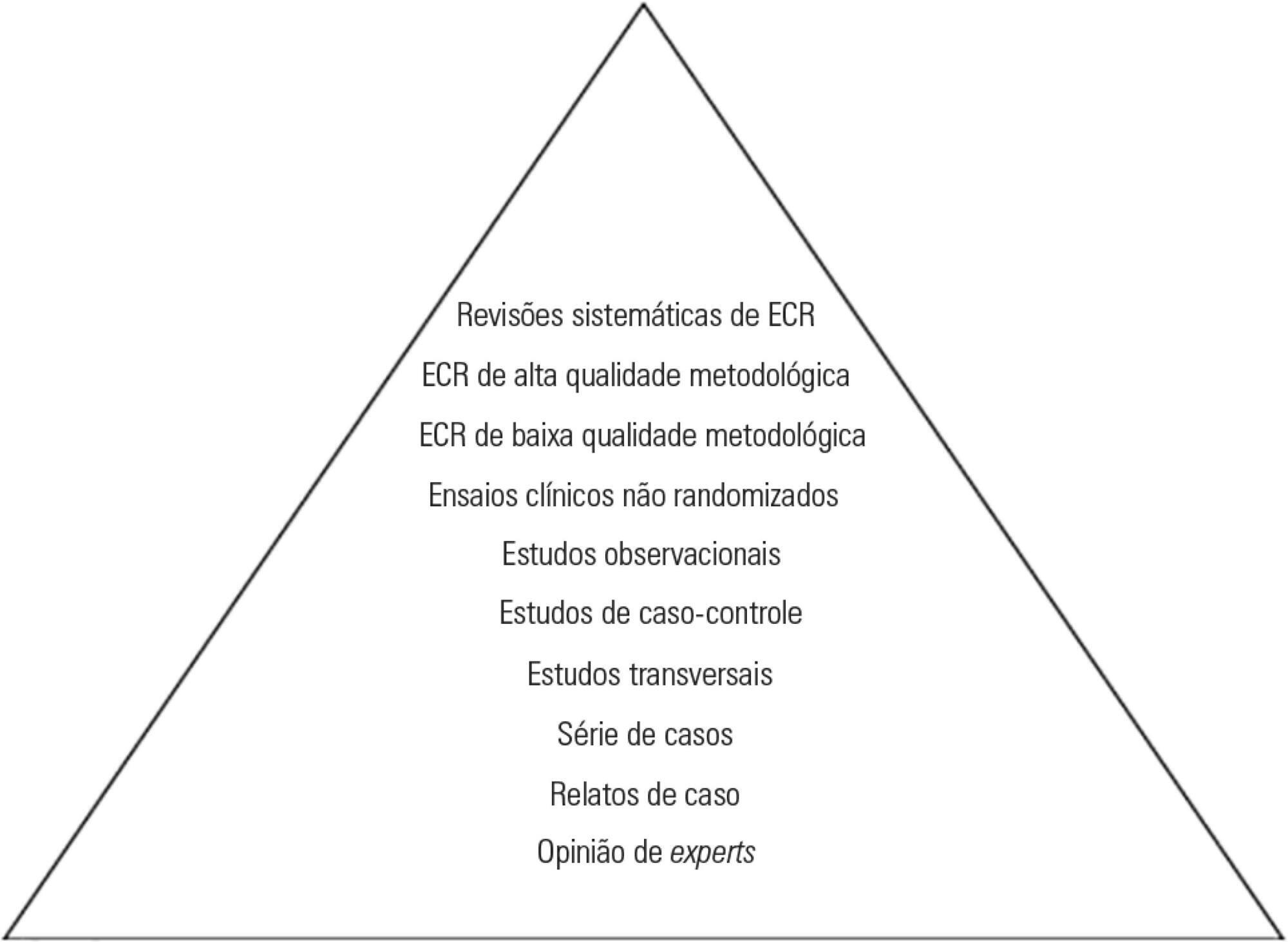
Different research designs have various advantages and limitations inherent to their main characteristics. Knowledge of the proper use of each design is of great importance to understanding the applicability of research findings to clinical epidemiology.
In intensive care, a hierarchical classification of designs can often be misleading if the characteristics of the design in this context are not understood. One must therefore be alert to common problems in randomized clinical trials and systematic reviews/meta-analyses that address clinical issues related to the care of the critically ill patient.
Views0Abstract
Special ArticlesDifferent research designs and their characteristics in intensive care
Rev Bras Ter Intensiva. 2016;28(3):256-260
DOI 10.5935/0103-507X.20160050
Views0See moreABSTRACT
Different research designs have various advantages and limitations inherent to their main characteristics. Knowledge of the proper use of each design is of great importance to understanding the applicability of research findings to clinical epidemiology.
In intensive care, a hierarchical classification of designs can often be misleading if the characteristics of the design in this context are not understood. One must therefore be alert to common problems in randomized clinical trials and systematic reviews/meta-analyses that address clinical issues related to the care of the critically ill patient.
-
Commentaries
Epidemiology of severe infections in Latin American intensive care units
Rev Bras Ter Intensiva. 2016;28(3):261-263
Abstract
CommentariesEpidemiology of severe infections in Latin American intensive care units
Rev Bras Ter Intensiva. 2016;28(3):261-263
DOI 10.5935/0103-507X.20160051
Views0Latin American perspectiveThe majority of the representative epidemiologic reports of sepsis are from developed countries; in Latin America, the clinical and epidemiological approaches to the problem have sometimes been inappropriate in terms of research design, study population, and clinical outcomes.() Cities are expanding rapidly in middle-income countries, but their supply of acute care services is […]See moreViews0Abstract
CommentariesEpidemiology of severe infections in Latin American intensive care units
Rev Bras Ter Intensiva. 2016;28(3):261-263
DOI 10.5935/0103-507X.20160051
Views0Latin American perspectiveThe majority of the representative epidemiologic reports of sepsis are from developed countries; in Latin America, the clinical and epidemiological approaches to the problem have sometimes been inappropriate in terms of research design, study population, and clinical outcomes.() Cities are expanding rapidly in middle-income countries, but their supply of acute care services is […]See more -
Commentaries
What every intensivist should know about prognostic scoring systems and risk-adjusted mortality
Rev Bras Ter Intensiva. 2016;28(3):264-269
Abstract
CommentariesWhat every intensivist should know about prognostic scoring systems and risk-adjusted mortality
Rev Bras Ter Intensiva. 2016;28(3):264-269
DOI 10.5935/0103-507X.20160052
Views0Sequential Organ Failure Assessment: an organ dysfunction scoreMultiple organ dysfunction syndrome is a major cause of ICU morbidity and mortality. The extent and severity of organ dysfunction may be quantified in a number of organ dysfunction scores, the most prominent of which is the SOFA.() Originally designed to be used in patients with sepsis, the […]See moreViews0Abstract
CommentariesWhat every intensivist should know about prognostic scoring systems and risk-adjusted mortality
Rev Bras Ter Intensiva. 2016;28(3):264-269
DOI 10.5935/0103-507X.20160052
Views0Sequential Organ Failure Assessment: an organ dysfunction scoreMultiple organ dysfunction syndrome is a major cause of ICU morbidity and mortality. The extent and severity of organ dysfunction may be quantified in a number of organ dysfunction scores, the most prominent of which is the SOFA.() Originally designed to be used in patients with sepsis, the […]See more
-
Original Articles
Prevalence of burnout syndrome in intensivist doctors in five Brazilian capitals
Rev Bras Ter Intensiva. 2016;28(3):270-277
Abstract
Original ArticlesPrevalence of burnout syndrome in intensivist doctors in five Brazilian capitals
Rev Bras Ter Intensiva. 2016;28(3):270-277
DOI 10.5935/0103-507X.20160053
Views0ABSTRACT
Objective:
To estimate the prevalence of burnout in intensivist doctors working in adult, pediatric and neonatal intensive care units in five Brazilian capitals.
Methods:
Descriptive epidemiological study with a random sample stratified by conglomerate with 180 intensivist doctors from five capitals representing the Brazilian geographic regions: Porto Alegre (RS), Sao Paulo (SP), Salvador (BA), Goiania (GO) and Belem (PA). A self-administered questionnaire examining sociodemographic data and the level of burnout was evaluated through the Maslach Burnout Inventory.
Results:
A total of 180 doctors were evaluated, of which 54.4% were female. The average age was 39 ± 8.1 years, 63.4% had specialization as the highest degree, 55.7% had up to 10 years of work experience in an intensive care unit, and 46.1% had the title intensive care specialist. Most (50.3%) had weekly workloads between 49 and 72 hours, and the most frequent employee type was salaried. High levels of emotional exhaustion, depersonalization and inefficacy were found (50.6%, 26.1% and 15.0%, respectively). The prevalence of burnout was 61.7% when considering a high level in at least one dimension and 5% with a high level in three dimensions simultaneously.
Conclusion:
A high prevalence of burnout syndrome among intensivist doctors was observed. Strategies for the promotion and protection of health in these workers must be discussed and implemented in hospitals.
Keywords:Burnout, professional/epidemiologyIntensive care unitsIntensive care units, pediatricIntensive care, neonatalOccupational diseases/epidemiologyPhysicians/psychologyprevalenceWorking conditionsSee moreViews0Abstract
Original ArticlesPrevalence of burnout syndrome in intensivist doctors in five Brazilian capitals
Rev Bras Ter Intensiva. 2016;28(3):270-277
DOI 10.5935/0103-507X.20160053
Views0ABSTRACT
Objective:
To estimate the prevalence of burnout in intensivist doctors working in adult, pediatric and neonatal intensive care units in five Brazilian capitals.
Methods:
Descriptive epidemiological study with a random sample stratified by conglomerate with 180 intensivist doctors from five capitals representing the Brazilian geographic regions: Porto Alegre (RS), Sao Paulo (SP), Salvador (BA), Goiania (GO) and Belem (PA). A self-administered questionnaire examining sociodemographic data and the level of burnout was evaluated through the Maslach Burnout Inventory.
Results:
A total of 180 doctors were evaluated, of which 54.4% were female. The average age was 39 ± 8.1 years, 63.4% had specialization as the highest degree, 55.7% had up to 10 years of work experience in an intensive care unit, and 46.1% had the title intensive care specialist. Most (50.3%) had weekly workloads between 49 and 72 hours, and the most frequent employee type was salaried. High levels of emotional exhaustion, depersonalization and inefficacy were found (50.6%, 26.1% and 15.0%, respectively). The prevalence of burnout was 61.7% when considering a high level in at least one dimension and 5% with a high level in three dimensions simultaneously.
Conclusion:
A high prevalence of burnout syndrome among intensivist doctors was observed. Strategies for the promotion and protection of health in these workers must be discussed and implemented in hospitals.
Keywords:Burnout, professional/epidemiologyIntensive care unitsIntensive care units, pediatricIntensive care, neonatalOccupational diseases/epidemiologyPhysicians/psychologyprevalenceWorking conditionsSee more -
Original Articles
Evaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
Abstract
Original ArticlesEvaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
DOI 10.5935/0103-507X.20160045
Views1ABSTRACT
Objective:
To evaluate the implementation of a multidisciplinary rapid response team led by an intensive care physician at a university hospital.
Methods:
This retrospective cohort study analyzed assessment forms that were completed during the assessments made by the rapid response team of a university hospital between March 2009 and February 2014.
Results:
Data were collected from 1,628 assessments performed by the rapid response team for 1,024 patients and included 1,423 code yellow events and 205 code blue events. The number of assessments was higher in the first year of operation of the rapid response team. The multivariate analysis indicated that age (OR 1.02; 95%CI 1.02 – 1.03; p < 0.001), being male (OR 1.48; 95%CI 1.09 - 2.01; p = 0.01), having more than one assessment (OR 3.31; 95%CI, 2.32 - 4.71; p < 0.001), hospitalization for clinical care (OR 1.77; 95%CI 1.29 - 2.42; p < 0.001), the request of admission to the intensive care unit after the code event (OR 4.75; 95%CI 3.43 - 6.59; p < 0.001), and admission to the intensive care unit before the code event (OR 2.13; 95%CI 1.41 - 3.21; p = 0.001) were risk factors for hospital mortality in patients who were seen for code yellow events.
Conclusion:
The hospital mortality rates were higher than those found in previous studies. The number of assessments was higher in the first year of operation of the rapid response team. Moreover, hospital mortality was higher among patients admitted for clinical care.
Keywords:Hospital mortalityHospital rapid response teamHospital, universitiesIntensive care unitsPatient safetySee moreViews1Abstract
Original ArticlesEvaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
DOI 10.5935/0103-507X.20160045
Views1ABSTRACT
Objective:
To evaluate the implementation of a multidisciplinary rapid response team led by an intensive care physician at a university hospital.
Methods:
This retrospective cohort study analyzed assessment forms that were completed during the assessments made by the rapid response team of a university hospital between March 2009 and February 2014.
Results:
Data were collected from 1,628 assessments performed by the rapid response team for 1,024 patients and included 1,423 code yellow events and 205 code blue events. The number of assessments was higher in the first year of operation of the rapid response team. The multivariate analysis indicated that age (OR 1.02; 95%CI 1.02 – 1.03; p < 0.001), being male (OR 1.48; 95%CI 1.09 - 2.01; p = 0.01), having more than one assessment (OR 3.31; 95%CI, 2.32 - 4.71; p < 0.001), hospitalization for clinical care (OR 1.77; 95%CI 1.29 - 2.42; p < 0.001), the request of admission to the intensive care unit after the code event (OR 4.75; 95%CI 3.43 - 6.59; p < 0.001), and admission to the intensive care unit before the code event (OR 2.13; 95%CI 1.41 - 3.21; p = 0.001) were risk factors for hospital mortality in patients who were seen for code yellow events.
Conclusion:
The hospital mortality rates were higher than those found in previous studies. The number of assessments was higher in the first year of operation of the rapid response team. Moreover, hospital mortality was higher among patients admitted for clinical care.
Keywords:Hospital mortalityHospital rapid response teamHospital, universitiesIntensive care unitsPatient safetySee more
-
Original Articles
Analysis of knowledge of the general population and health professionals on organ donation after cardiac death
Rev Bras Ter Intensiva. 2016;28(3):285-293
Abstract
Original ArticlesAnalysis of knowledge of the general population and health professionals on organ donation after cardiac death
Rev Bras Ter Intensiva. 2016;28(3):285-293
DOI 10.5935/0103-507X.20160043
Views0ABSTRACT
Objective:
To evaluate the knowledge and acceptance of the public and professionals working in intensive care units regarding organ donation after cardiac death.
Methods:
The three hospitals with the most brain death notifications in Curitiba were selected, and two groups of respondents were established for application of the same questionnaire: the general public (i.e., visitors of patients in intensive care units) and health professionals working in the same intensive care unit. The questionnaire contained questions concerning demographics, intention to donate organs and knowledge of current legislation regarding brain death and donation after cardiac death.
Results:
In total, 543 questionnaires were collected, including 442 from family members and 101 from health professionals. There was a predominance of women and Catholics in both groups. More females intended to donate. Health professionals performed better in the knowledge comparison. The intention to donate organs was significantly higher in the health professionals group (p = 0.01). There was no significant difference in the intention to donate in terms of education level or income. There was a greater acceptance of donation after uncontrolled cardiac death among Catholics than among evangelicals (p < 0.001).
Conclusion:
Most of the general population intended to donate, with greater intentions expressed by females. Education and income did not affect the decision. The type of transplant that used a donation after uncontrolled cardiac death was not well accepted in the study population, indicating the need for more clarification for its use in our setting.
Keywords:Intensive care unitsOrgan donationPublic healthPublic opinionTissue and organ procurementTransplantationSee moreViews0Abstract
Original ArticlesAnalysis of knowledge of the general population and health professionals on organ donation after cardiac death
Rev Bras Ter Intensiva. 2016;28(3):285-293
DOI 10.5935/0103-507X.20160043
Views0ABSTRACT
Objective:
To evaluate the knowledge and acceptance of the public and professionals working in intensive care units regarding organ donation after cardiac death.
Methods:
The three hospitals with the most brain death notifications in Curitiba were selected, and two groups of respondents were established for application of the same questionnaire: the general public (i.e., visitors of patients in intensive care units) and health professionals working in the same intensive care unit. The questionnaire contained questions concerning demographics, intention to donate organs and knowledge of current legislation regarding brain death and donation after cardiac death.
Results:
In total, 543 questionnaires were collected, including 442 from family members and 101 from health professionals. There was a predominance of women and Catholics in both groups. More females intended to donate. Health professionals performed better in the knowledge comparison. The intention to donate organs was significantly higher in the health professionals group (p = 0.01). There was no significant difference in the intention to donate in terms of education level or income. There was a greater acceptance of donation after uncontrolled cardiac death among Catholics than among evangelicals (p < 0.001).
Conclusion:
Most of the general population intended to donate, with greater intentions expressed by females. Education and income did not affect the decision. The type of transplant that used a donation after uncontrolled cardiac death was not well accepted in the study population, indicating the need for more clarification for its use in our setting.
Keywords:Intensive care unitsOrgan donationPublic healthPublic opinionTissue and organ procurementTransplantationSee more -
Original Articles
Limitation to Advanced Life Support in patients admitted to intensive care unit with integrated palliative care
Rev Bras Ter Intensiva. 2016;28(3):294-300
Abstract
Original ArticlesLimitation to Advanced Life Support in patients admitted to intensive care unit with integrated palliative care
Rev Bras Ter Intensiva. 2016;28(3):294-300
DOI 10.5935/0103-507X.20160042
Views1See moreABSTRACT
Objective:
To estimate the incidence of limitations to Advanced Life Support in critically ill patients admitted to an intensive care unit with integrated palliative care.
Methods:
This retrospective cohort study included patients in the palliative care program of the intensive care unit of Hospital Paulistano over 18 years of age from May 1, 2011, to January 31, 2014. The limitations to Advanced Life Support that were analyzed included do-not-resuscitate orders, mechanical ventilation, dialysis and vasoactive drugs. Central tendency measures were calculated for quantitative variables. The chi-squared test was used to compare the characteristics of patients with or without limits to Advanced Life Support, and the Wilcoxon test was used to compare length of stay after Advanced Life Support. Confidence intervals reflecting p ≤ 0.05 were considered for statistical significance.
Results:
A total of 3,487 patients were admitted to the intensive care unit, of whom 342 were included in the palliative care program. It was observed that after entering the palliative care program, it took a median of 2 (1 – 4) days for death to occur in the intensive care unit and 4 (2 – 11) days for hospital death to occur. Many of the limitations to Advanced Life Support (42.7%) took place on the first day of hospitalization. Cardiopulmonary resuscitation (96.8%) and ventilatory support (73.6%) were the most adopted limitations.
Conclusion:
The contribution of palliative care integrated into the intensive care unit was important for the practice of orthothanasia, i.e., the non-extension of the life of a critically ill patient by artificial means.
Views1Abstract
Original ArticlesLimitation to Advanced Life Support in patients admitted to intensive care unit with integrated palliative care
Rev Bras Ter Intensiva. 2016;28(3):294-300
DOI 10.5935/0103-507X.20160042
Views1See moreABSTRACT
Objective:
To estimate the incidence of limitations to Advanced Life Support in critically ill patients admitted to an intensive care unit with integrated palliative care.
Methods:
This retrospective cohort study included patients in the palliative care program of the intensive care unit of Hospital Paulistano over 18 years of age from May 1, 2011, to January 31, 2014. The limitations to Advanced Life Support that were analyzed included do-not-resuscitate orders, mechanical ventilation, dialysis and vasoactive drugs. Central tendency measures were calculated for quantitative variables. The chi-squared test was used to compare the characteristics of patients with or without limits to Advanced Life Support, and the Wilcoxon test was used to compare length of stay after Advanced Life Support. Confidence intervals reflecting p ≤ 0.05 were considered for statistical significance.
Results:
A total of 3,487 patients were admitted to the intensive care unit, of whom 342 were included in the palliative care program. It was observed that after entering the palliative care program, it took a median of 2 (1 – 4) days for death to occur in the intensive care unit and 4 (2 – 11) days for hospital death to occur. Many of the limitations to Advanced Life Support (42.7%) took place on the first day of hospitalization. Cardiopulmonary resuscitation (96.8%) and ventilatory support (73.6%) were the most adopted limitations.
Conclusion:
The contribution of palliative care integrated into the intensive care unit was important for the practice of orthothanasia, i.e., the non-extension of the life of a critically ill patient by artificial means.
-
Original Articles
Palliative care for patients with HIV/AIDS admitted to intensive care units
Rev Bras Ter Intensiva. 2016;28(3):301-309
Abstract
Original ArticlesPalliative care for patients with HIV/AIDS admitted to intensive care units
Rev Bras Ter Intensiva. 2016;28(3):301-309
DOI 10.5935/0103-507X.20160054
Views0See moreABSTRACT
Objective:
To describe the characteristics of patients with HIV/AIDS and to compare the therapeutic interventions and end-of-life care before and after evaluation by the palliative care team.
Methods:
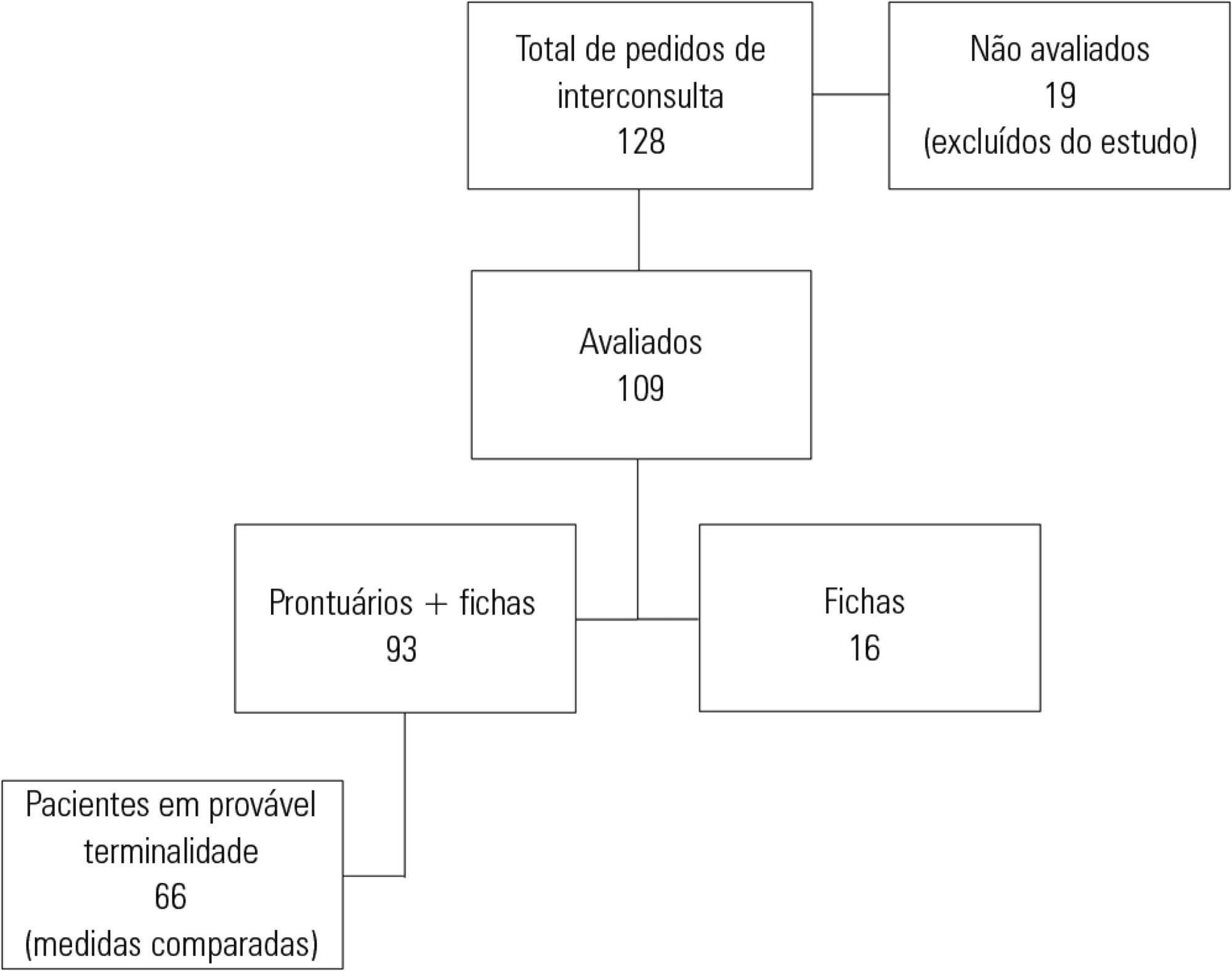
This retrospective cohort study included all patients with HIV/AIDS admitted to the intensive care unit of the Instituto de Infectologia Emílio Ribas who were evaluated by a palliative care team between January 2006 and December 2012.
Results:
Of the 109 patients evaluated, 89% acquired opportunistic infections, 70% had CD4 counts lower than 100 cells/mm3, and only 19% adhered to treatment. The overall mortality rate was 88%. Among patients predicted with a terminally ill (68%), the use of highly active antiretroviral therapy decreased from 50.0% to 23.1% (p = 0.02), the use of antibiotics decreased from 100% to 63.6% (p < 0.001), the use of vasoactive drugs decreased from 62.1% to 37.8% (p = 0.009), the use of renal replacement therapy decreased from 34.8% to 23.0% (p < 0.0001), and the number of blood product transfusions decreased from 74.2% to 19.7% (p < 0.0001). Meetings with the family were held in 48 cases, and 23% of the terminally ill patients were discharged from the intensive care unit.
Conclusion:
Palliative care was required in patients with severe illnesses and high mortality. The number of potentially inappropriate interventions in terminally ill patients monitored by the palliative care team significantly decreased, and 26% of the patients were discharged from the intensive care unit.
Views0Abstract
Original ArticlesPalliative care for patients with HIV/AIDS admitted to intensive care units
Rev Bras Ter Intensiva. 2016;28(3):301-309
DOI 10.5935/0103-507X.20160054
Views0See moreABSTRACT
Objective:
To describe the characteristics of patients with HIV/AIDS and to compare the therapeutic interventions and end-of-life care before and after evaluation by the palliative care team.
Methods:
This retrospective cohort study included all patients with HIV/AIDS admitted to the intensive care unit of the Instituto de Infectologia Emílio Ribas who were evaluated by a palliative care team between January 2006 and December 2012.
Results:
Of the 109 patients evaluated, 89% acquired opportunistic infections, 70% had CD4 counts lower than 100 cells/mm3, and only 19% adhered to treatment. The overall mortality rate was 88%. Among patients predicted with a terminally ill (68%), the use of highly active antiretroviral therapy decreased from 50.0% to 23.1% (p = 0.02), the use of antibiotics decreased from 100% to 63.6% (p < 0.001), the use of vasoactive drugs decreased from 62.1% to 37.8% (p = 0.009), the use of renal replacement therapy decreased from 34.8% to 23.0% (p < 0.0001), and the number of blood product transfusions decreased from 74.2% to 19.7% (p < 0.0001). Meetings with the family were held in 48 cases, and 23% of the terminally ill patients were discharged from the intensive care unit.
Conclusion:
Palliative care was required in patients with severe illnesses and high mortality. The number of potentially inappropriate interventions in terminally ill patients monitored by the palliative care team significantly decreased, and 26% of the patients were discharged from the intensive care unit.
-
Original Articles
Possible stressors in a neonatal intensive care unit at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):310-314
Abstract
Original ArticlesPossible stressors in a neonatal intensive care unit at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):310-314
DOI 10.5935/0103-507X.20160041
Views0See moreABSTRACT
Objective:
To investigate possible stressors to which newborns are exposed in the neonatal intensive care unit.
Methods:
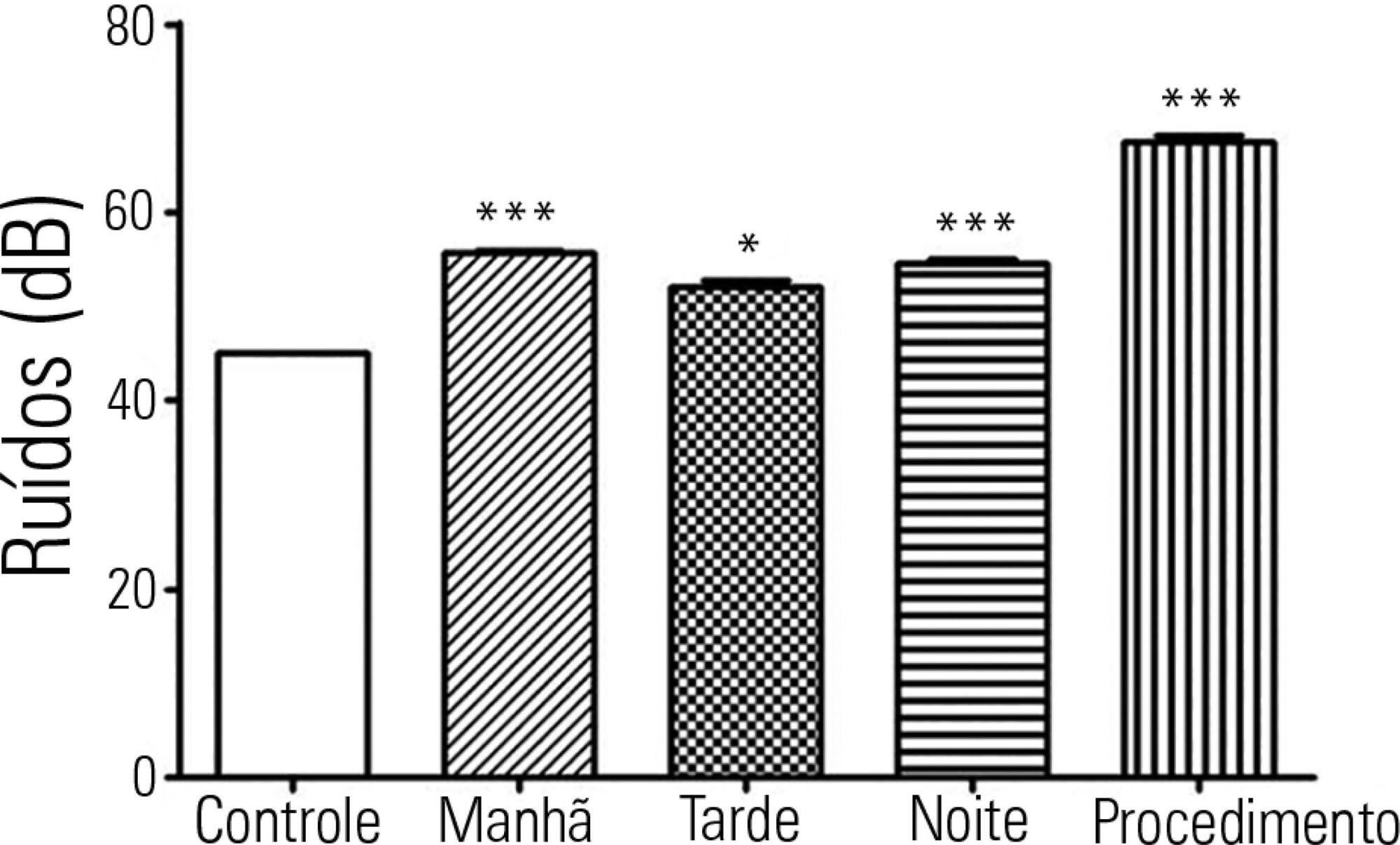
The levels of continuous noise were checked by a decibel meter positioned near the ear of the newborn, brightness was observed by a light meter positioned in the incubator in front of the newborn’s eyes, and temperature was checked through the incubator display. The evaluations were performed in three periods of the day, with ten measurements taken at one-minute intervals during each shift for the subsequent statistical analysis.
Results:
All shifts showed noise above acceptable levels. Morning (p < 0.001), afternoon (p < 0.05) and night (p < 0.001) showed a significant increase compared to the control. The brightness significantly exceeded the normal range (p < 0.01) in the morning. We observed that only one of the incubators was within the normal temperature limits.
Conclusion:
The noise, brightness and temperature intensities were not in accordance with regulatory standards and thus might be possible stressors to newborns.
Views0Abstract
Original ArticlesPossible stressors in a neonatal intensive care unit at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):310-314
DOI 10.5935/0103-507X.20160041
Views0See moreABSTRACT
Objective:
To investigate possible stressors to which newborns are exposed in the neonatal intensive care unit.
Methods:
The levels of continuous noise were checked by a decibel meter positioned near the ear of the newborn, brightness was observed by a light meter positioned in the incubator in front of the newborn’s eyes, and temperature was checked through the incubator display. The evaluations were performed in three periods of the day, with ten measurements taken at one-minute intervals during each shift for the subsequent statistical analysis.
Results:
All shifts showed noise above acceptable levels. Morning (p < 0.001), afternoon (p < 0.05) and night (p < 0.001) showed a significant increase compared to the control. The brightness significantly exceeded the normal range (p < 0.01) in the morning. We observed that only one of the incubators was within the normal temperature limits.
Conclusion:
The noise, brightness and temperature intensities were not in accordance with regulatory standards and thus might be possible stressors to newborns.
-
Original Articles
De-escalation, adequacy of antibiotic therapy and culture positivity in septic patients: an observational study
Rev Bras Ter Intensiva. 2016;28(3):315-322
Abstract
Original ArticlesDe-escalation, adequacy of antibiotic therapy and culture positivity in septic patients: an observational study
Rev Bras Ter Intensiva. 2016;28(3):315-322
DOI 10.5935/0103-507X.20160044
Views0ABSTRACT
Objective:
To evaluate the prevalence of antibiotic de-escalation in patients diagnosed with severe sepsis or septic shock at a public academic tertiary hospital and to evaluate antibiotic adequacy and culture positivity.
Methods:
The prevalence of antibiotic de-escalation, the adequacy of antibiotic treatment and the rates of culture positivity were analyzed in patients with severe sepsis and septic shock between April and December 2013 at an intensive care unit in a tertiary university hospital.
Results:
Among the 224 patients included in the study, de-escalation was appropriate in 66 patients (29.4%) but was implemented in 44 patients (19.6%). Among the patients who underwent de-escalation, half experienced narrowing of the antimicrobial spectrum. The mortality rate was 56.3%, with no differences between the patients with or without de-escalation (56.8% versus 56.1%; p = 0.999) nor in the length of hospital stay. Empirical antibiotic therapy was appropriate in 89% of cases. Microorganisms were isolated from total cultures in 30% of cases and from blood cultures in 26.3% of cases.
Conclusion:
The adequacy rate of empirical antibiotic therapy was high, reflecting an active institutional policy of monitoring epidemiological profiles and institutional protocols on antimicrobial use. However, antibiotic de-escalation could have been implemented in a greater number of patients. De-escalation did not affect mortality rates.
Keywords:Anti-bacterial agents/administration & dosageIntensive care unitsShock, septic/drug therapySee moreViews0Abstract
Original ArticlesDe-escalation, adequacy of antibiotic therapy and culture positivity in septic patients: an observational study
Rev Bras Ter Intensiva. 2016;28(3):315-322
DOI 10.5935/0103-507X.20160044
Views0ABSTRACT
Objective:
To evaluate the prevalence of antibiotic de-escalation in patients diagnosed with severe sepsis or septic shock at a public academic tertiary hospital and to evaluate antibiotic adequacy and culture positivity.
Methods:
The prevalence of antibiotic de-escalation, the adequacy of antibiotic treatment and the rates of culture positivity were analyzed in patients with severe sepsis and septic shock between April and December 2013 at an intensive care unit in a tertiary university hospital.
Results:
Among the 224 patients included in the study, de-escalation was appropriate in 66 patients (29.4%) but was implemented in 44 patients (19.6%). Among the patients who underwent de-escalation, half experienced narrowing of the antimicrobial spectrum. The mortality rate was 56.3%, with no differences between the patients with or without de-escalation (56.8% versus 56.1%; p = 0.999) nor in the length of hospital stay. Empirical antibiotic therapy was appropriate in 89% of cases. Microorganisms were isolated from total cultures in 30% of cases and from blood cultures in 26.3% of cases.
Conclusion:
The adequacy rate of empirical antibiotic therapy was high, reflecting an active institutional policy of monitoring epidemiological profiles and institutional protocols on antimicrobial use. However, antibiotic de-escalation could have been implemented in a greater number of patients. De-escalation did not affect mortality rates.
Keywords:Anti-bacterial agents/administration & dosageIntensive care unitsShock, septic/drug therapySee more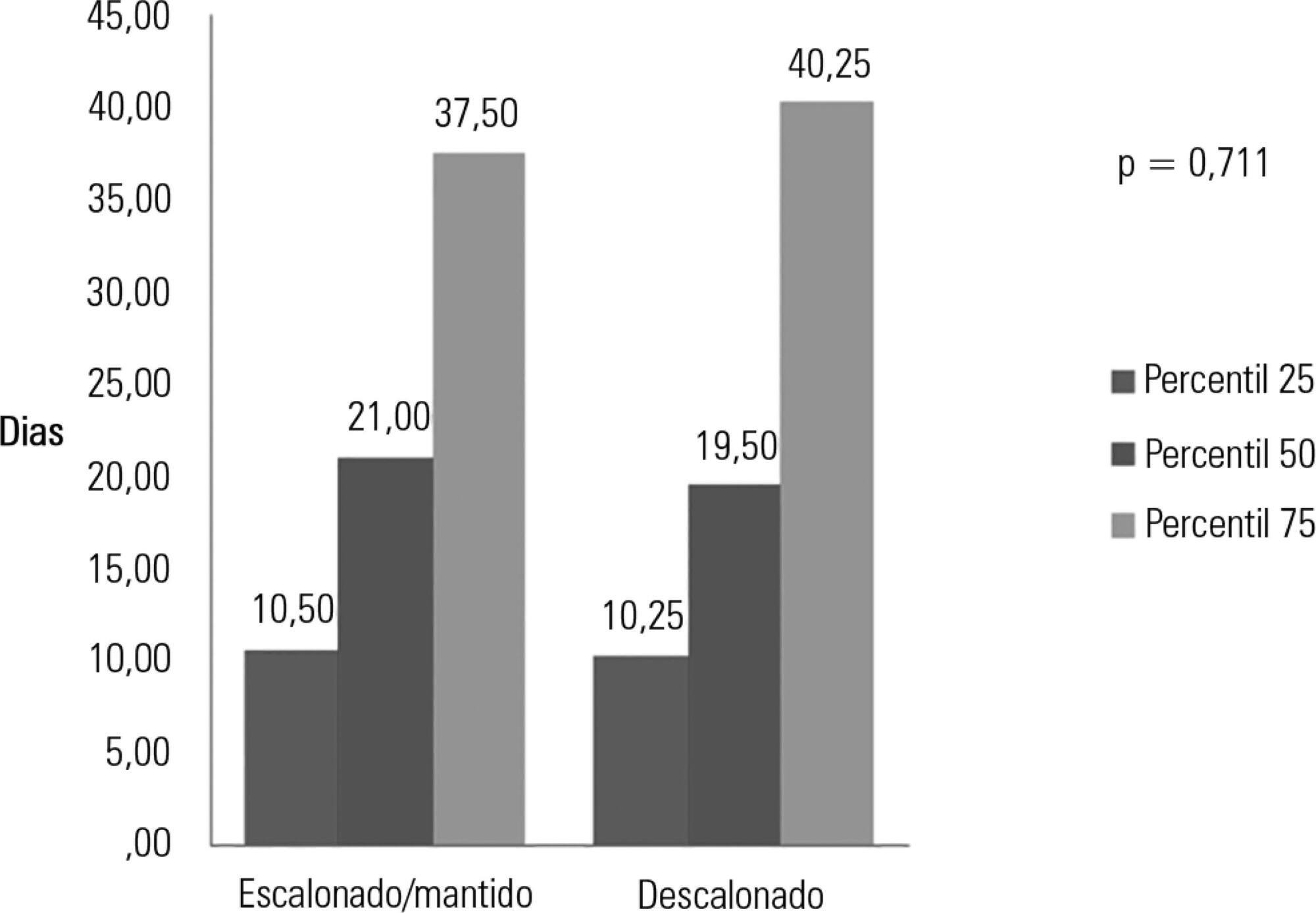
-
Original Articles
Stressors in the relatives of patients admitted to an intensive care unit
Rev Bras Ter Intensiva. 2016;28(3):323-329
Abstract
Original ArticlesStressors in the relatives of patients admitted to an intensive care unit
Rev Bras Ter Intensiva. 2016;28(3):323-329
DOI 10.5935/0103-507X.20160055
Views1ABSTRACT
Objective:
To identify and stratify the main stressors for the relatives of patients admitted to the adult intensive care unit of a teaching hospital.
Methods:
Cross-sectional descriptive study conducted with relatives of patients admitted to an intensive care unit from April to October 2014. The following materials were used: a questionnaire containing identification information and demographic data of the relatives, clinical data of the patients, and 25 stressors adapted from the Intensive Care Unit Environmental Stressor Scale. The degree of stress caused by each factor was determined on a scale of values from 1 to 4. The stressors were ranked based on the average score obtained.
Results:
The main cause of admission to the intensive care unit was clinical in 36 (52.2%) cases. The main stressors were the patient being in a state of coma (3.15 ± 1.23), the patient being unable to speak (3.15 ± 1.20), and the reason for admission (3.00 ± 1.27). After removing the 27 (39.1%) coma patients from the analysis, the main stressors for the relatives were the reason for admission (2.75 ± 1.354), seeing the patient in the intensive care unit (2.51 ± 1.227), and the patient being unable to speak (2.50 ± 1.269).
Conclusion:
Difficulties in communication and in the relationship with the patient admitted to the intensive care unit were identified as the main stressors by their relatives, with the state of coma being predominant. By contrast, the environment, work routines, and relationship between the relatives and intensive care unit team had the least impact as stressors.
Keywords:ComaCritical careFamilyHumanization of assistanceIntensive care unitsstressVisits to patientsSee moreViews1Abstract
Original ArticlesStressors in the relatives of patients admitted to an intensive care unit
Rev Bras Ter Intensiva. 2016;28(3):323-329
DOI 10.5935/0103-507X.20160055
Views1ABSTRACT
Objective:
To identify and stratify the main stressors for the relatives of patients admitted to the adult intensive care unit of a teaching hospital.
Methods:
Cross-sectional descriptive study conducted with relatives of patients admitted to an intensive care unit from April to October 2014. The following materials were used: a questionnaire containing identification information and demographic data of the relatives, clinical data of the patients, and 25 stressors adapted from the Intensive Care Unit Environmental Stressor Scale. The degree of stress caused by each factor was determined on a scale of values from 1 to 4. The stressors were ranked based on the average score obtained.
Results:
The main cause of admission to the intensive care unit was clinical in 36 (52.2%) cases. The main stressors were the patient being in a state of coma (3.15 ± 1.23), the patient being unable to speak (3.15 ± 1.20), and the reason for admission (3.00 ± 1.27). After removing the 27 (39.1%) coma patients from the analysis, the main stressors for the relatives were the reason for admission (2.75 ± 1.354), seeing the patient in the intensive care unit (2.51 ± 1.227), and the patient being unable to speak (2.50 ± 1.269).
Conclusion:
Difficulties in communication and in the relationship with the patient admitted to the intensive care unit were identified as the main stressors by their relatives, with the state of coma being predominant. By contrast, the environment, work routines, and relationship between the relatives and intensive care unit team had the least impact as stressors.
Keywords:ComaCritical careFamilyHumanization of assistanceIntensive care unitsstressVisits to patientsSee more -
Original Articles
Evaluation of medical devices in thoracic radiograms in intensive care unit – time to pay attention!
Rev Bras Ter Intensiva. 2016;28(3):330-334
Abstract
Original ArticlesEvaluation of medical devices in thoracic radiograms in intensive care unit – time to pay attention!
Rev Bras Ter Intensiva. 2016;28(3):330-334
DOI 10.5935/0103-507X.20160056
Views0ABSTRACT
Objective:
To identify and evaluate the correct positioning of the most commonly used medical devices as visualized in thoracic radiograms of patients in the intensive care unit of our center.
Methods:
A literature search was conducted for the criteria used to evaluate the correct positioning of medical devices on thoracic radiograms. All the thoracic radiograms performed in the intensive care unit of our center over an 18-month period were analyzed. All admissions in which at least one thoracic radiogram was performed in the intensive care unit and in which at least one medical device was identifiable in the thoracic radiogram were included. One radiogram per admission was selected for analysis. The radiograms were evaluated by an independent observer.
Results:
Out of the 2,312 thoracic radiograms analyzed, 568 were included in this study. Several medical devices were identified, including monitoring leads, endotracheal and tracheostomy tubes, central venous catheters, pacemakers and prosthetic cardiac valves. Of the central venous catheters that were identified, 33.6% of the subclavian and 23.8% of the jugular were malpositioned. Of the endotracheal tubes, 19.9% were malpositioned, while all the tracheostomy tubes were correctly positioned.
Conclusion:
Malpositioning of central venous catheters and endotracheal tubes is frequently identified in radiograms of patients in an intensive care unit. This is relevant because malpositioned devices may be related to adverse events. In future studies, an association between malpositioning and adverse events should be investigated.
Keywords:Central venous catheters/utilizationEquipment and suppliesIntensive care unitsIntubation, intratracheal/instrumentationRadiography, thoracicSee moreViews0Abstract
Original ArticlesEvaluation of medical devices in thoracic radiograms in intensive care unit – time to pay attention!
Rev Bras Ter Intensiva. 2016;28(3):330-334
DOI 10.5935/0103-507X.20160056
Views0ABSTRACT
Objective:
To identify and evaluate the correct positioning of the most commonly used medical devices as visualized in thoracic radiograms of patients in the intensive care unit of our center.
Methods:
A literature search was conducted for the criteria used to evaluate the correct positioning of medical devices on thoracic radiograms. All the thoracic radiograms performed in the intensive care unit of our center over an 18-month period were analyzed. All admissions in which at least one thoracic radiogram was performed in the intensive care unit and in which at least one medical device was identifiable in the thoracic radiogram were included. One radiogram per admission was selected for analysis. The radiograms were evaluated by an independent observer.
Results:
Out of the 2,312 thoracic radiograms analyzed, 568 were included in this study. Several medical devices were identified, including monitoring leads, endotracheal and tracheostomy tubes, central venous catheters, pacemakers and prosthetic cardiac valves. Of the central venous catheters that were identified, 33.6% of the subclavian and 23.8% of the jugular were malpositioned. Of the endotracheal tubes, 19.9% were malpositioned, while all the tracheostomy tubes were correctly positioned.
Conclusion:
Malpositioning of central venous catheters and endotracheal tubes is frequently identified in radiograms of patients in an intensive care unit. This is relevant because malpositioned devices may be related to adverse events. In future studies, an association between malpositioning and adverse events should be investigated.
Keywords:Central venous catheters/utilizationEquipment and suppliesIntensive care unitsIntubation, intratracheal/instrumentationRadiography, thoracicSee more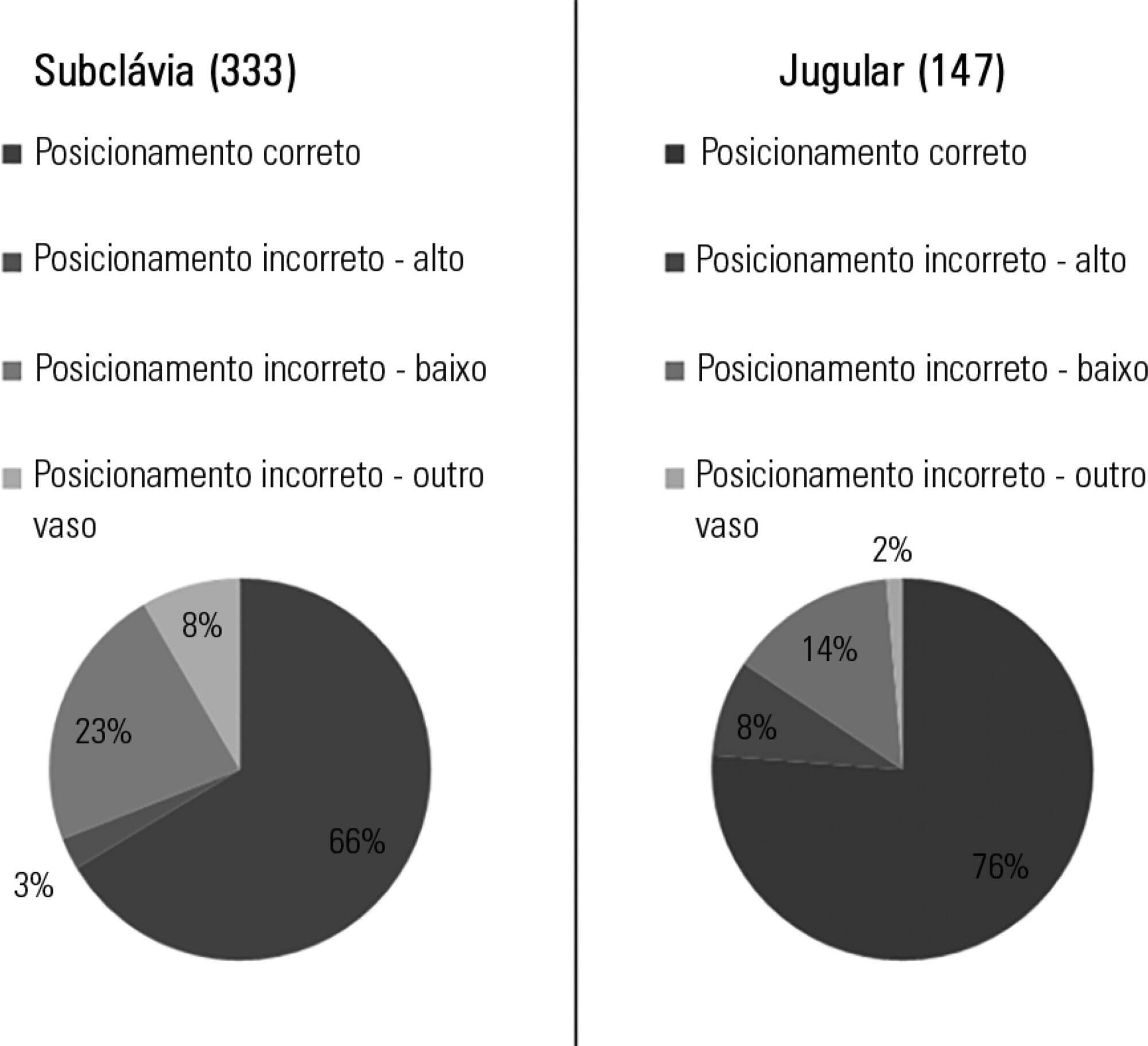
-
Original Articles
Health professionals’ perceptions about the decision-making process in the care of pediatric patients
Rev Bras Ter Intensiva. 2016;28(3):335-340
Abstract
Original ArticlesHealth professionals’ perceptions about the decision-making process in the care of pediatric patients
Rev Bras Ter Intensiva. 2016;28(3):335-340
DOI 10.5935/0103-507X.20160057
Views0ABSTRACT
Objective:
To evaluate the perceptions of physicians, nurses and nursing technicians of their participation in the decision-making process surrounding life support limitation in terminally ill pediatric patients, with comparisons by professional category.
Methods:
A cross-sectional study was conducted in the pediatric intensive care unit of a tertiary public university hospital with the participation of physicians, nurses and nursing technicians. The MacArthur Admission Experience Survey Voice Scale was used to assess and quantify the perceptions of professionals who assisted 17 pediatric patients with life support limitation within 24 hours after the outcome of each patient was determined. All professionals working in the unit (n = 117) who were potentially eligible for the study received a free and informed consent form prior to the occurrence of the cases studied.
Results:
Study participants included 25/40 (62.5%) physicians, 10/17 (58.8%) nurses and 41/60 (68.3%) nursing technicians, representing 65% of the eligible professionals identified. The questionnaire return rate was higher for physicians than technicians (p = 0.0258). A perceived lack of voice was reported in all three professional categories at varying rates that were lower for physicians than for nurses and nursing technicians (p < 0.00001); there was no difference between the latter (p = 0.7016). In the three professional categories studied, three subscale items were reported. For two of the three statements, there were significant differences between physicians and nurses (p = 0.004) and between physicians and nursing technicians (p = 0.001). For one of the statements, there was no difference among the three professional categories.
Conclusion:
Respondents perceived a lack of voice in the decision-making process at varying rates across the three categories of studied professionals who assisted terminally ill pediatric patients with life support limitation, with physicians expressing lowered rates of perceived coercion.
Keywords:CoercionDecision MakingEthics, professionalIntensive care units, pediatricPatient careResuscitation orders/psychologySurveys and questionnairesSee moreViews0Abstract
Original ArticlesHealth professionals’ perceptions about the decision-making process in the care of pediatric patients
Rev Bras Ter Intensiva. 2016;28(3):335-340
DOI 10.5935/0103-507X.20160057
Views0ABSTRACT
Objective:
To evaluate the perceptions of physicians, nurses and nursing technicians of their participation in the decision-making process surrounding life support limitation in terminally ill pediatric patients, with comparisons by professional category.
Methods:
A cross-sectional study was conducted in the pediatric intensive care unit of a tertiary public university hospital with the participation of physicians, nurses and nursing technicians. The MacArthur Admission Experience Survey Voice Scale was used to assess and quantify the perceptions of professionals who assisted 17 pediatric patients with life support limitation within 24 hours after the outcome of each patient was determined. All professionals working in the unit (n = 117) who were potentially eligible for the study received a free and informed consent form prior to the occurrence of the cases studied.
Results:
Study participants included 25/40 (62.5%) physicians, 10/17 (58.8%) nurses and 41/60 (68.3%) nursing technicians, representing 65% of the eligible professionals identified. The questionnaire return rate was higher for physicians than technicians (p = 0.0258). A perceived lack of voice was reported in all three professional categories at varying rates that were lower for physicians than for nurses and nursing technicians (p < 0.00001); there was no difference between the latter (p = 0.7016). In the three professional categories studied, three subscale items were reported. For two of the three statements, there were significant differences between physicians and nurses (p = 0.004) and between physicians and nursing technicians (p = 0.001). For one of the statements, there was no difference among the three professional categories.
Conclusion:
Respondents perceived a lack of voice in the decision-making process at varying rates across the three categories of studied professionals who assisted terminally ill pediatric patients with life support limitation, with physicians expressing lowered rates of perceived coercion.
Keywords:CoercionDecision MakingEthics, professionalIntensive care units, pediatricPatient careResuscitation orders/psychologySurveys and questionnairesSee more -
Original Articles
Effects of manual hyperinflation in preterm newborns under mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(3):341-347
Abstract
Original ArticlesEffects of manual hyperinflation in preterm newborns under mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(3):341-347
DOI 10.5935/0103-507X.20160058
Views0ABSTRACT
Objective:
To assess the effects of manual hyperinflation, performed with a manual resuscitator with and without the positive end-expiratory pressure valve, on the respiratory function of preterm newborns under mechanical ventilation.
Methods:
Cross-sectional study of hemodynamically stable preterm newborns with gestational age of less than 32 weeks, under mechanical ventilation and dependent on it at 28 days of life. Manual hyperinflation was applied randomly, alternating the use or not of the positive end-expiratory pressure valve, followed by tracheal aspiration for ending the maneuver. For nominal data, the two-tailed Wilcoxon test was applied at the 5% significance level and 80% power.
Results:
Twenty-eight preterm newborns, with an average birth weight of 1,005.71 ± 372.16g, an average gestational age of 28.90 ± 1.79 weeks, an average corrected age of 33.26 ± 1.78 weeks, and an average mechanical ventilation time of 29.5 (15 – 53) days, were studied. Increases in inspiratory and expiratory volumes occurred between time-points A5 (before the maneuver) and C1 (immediately after tracheal aspiration) in both the maneuver with the valve (p = 0.001 and p = 0.009) and without the valve (p = 0.026 and p = 0.001), respectively. There was also an increase in expiratory resistance between time-points A5 and C1 (p = 0.044).
Conclusion:
Lung volumes increased when performing the maneuver with and without the valve, with a significant difference in the first minute after aspiration. There was a significant difference in expiratory resistance between the time-points A5 (before the maneuver) and C1 (immediately after tracheal aspiration) in the first minute after aspiration within each maneuver.
Keywords:Infant, newbornIntensive care, neonatalPositive pressure respirationRespiration, artificialRespiratory therapySee moreViews0Abstract
Original ArticlesEffects of manual hyperinflation in preterm newborns under mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(3):341-347
DOI 10.5935/0103-507X.20160058
Views0ABSTRACT
Objective:
To assess the effects of manual hyperinflation, performed with a manual resuscitator with and without the positive end-expiratory pressure valve, on the respiratory function of preterm newborns under mechanical ventilation.
Methods:
Cross-sectional study of hemodynamically stable preterm newborns with gestational age of less than 32 weeks, under mechanical ventilation and dependent on it at 28 days of life. Manual hyperinflation was applied randomly, alternating the use or not of the positive end-expiratory pressure valve, followed by tracheal aspiration for ending the maneuver. For nominal data, the two-tailed Wilcoxon test was applied at the 5% significance level and 80% power.
Results:
Twenty-eight preterm newborns, with an average birth weight of 1,005.71 ± 372.16g, an average gestational age of 28.90 ± 1.79 weeks, an average corrected age of 33.26 ± 1.78 weeks, and an average mechanical ventilation time of 29.5 (15 – 53) days, were studied. Increases in inspiratory and expiratory volumes occurred between time-points A5 (before the maneuver) and C1 (immediately after tracheal aspiration) in both the maneuver with the valve (p = 0.001 and p = 0.009) and without the valve (p = 0.026 and p = 0.001), respectively. There was also an increase in expiratory resistance between time-points A5 and C1 (p = 0.044).
Conclusion:
Lung volumes increased when performing the maneuver with and without the valve, with a significant difference in the first minute after aspiration. There was a significant difference in expiratory resistance between the time-points A5 (before the maneuver) and C1 (immediately after tracheal aspiration) in the first minute after aspiration within each maneuver.
Keywords:Infant, newbornIntensive care, neonatalPositive pressure respirationRespiration, artificialRespiratory therapySee more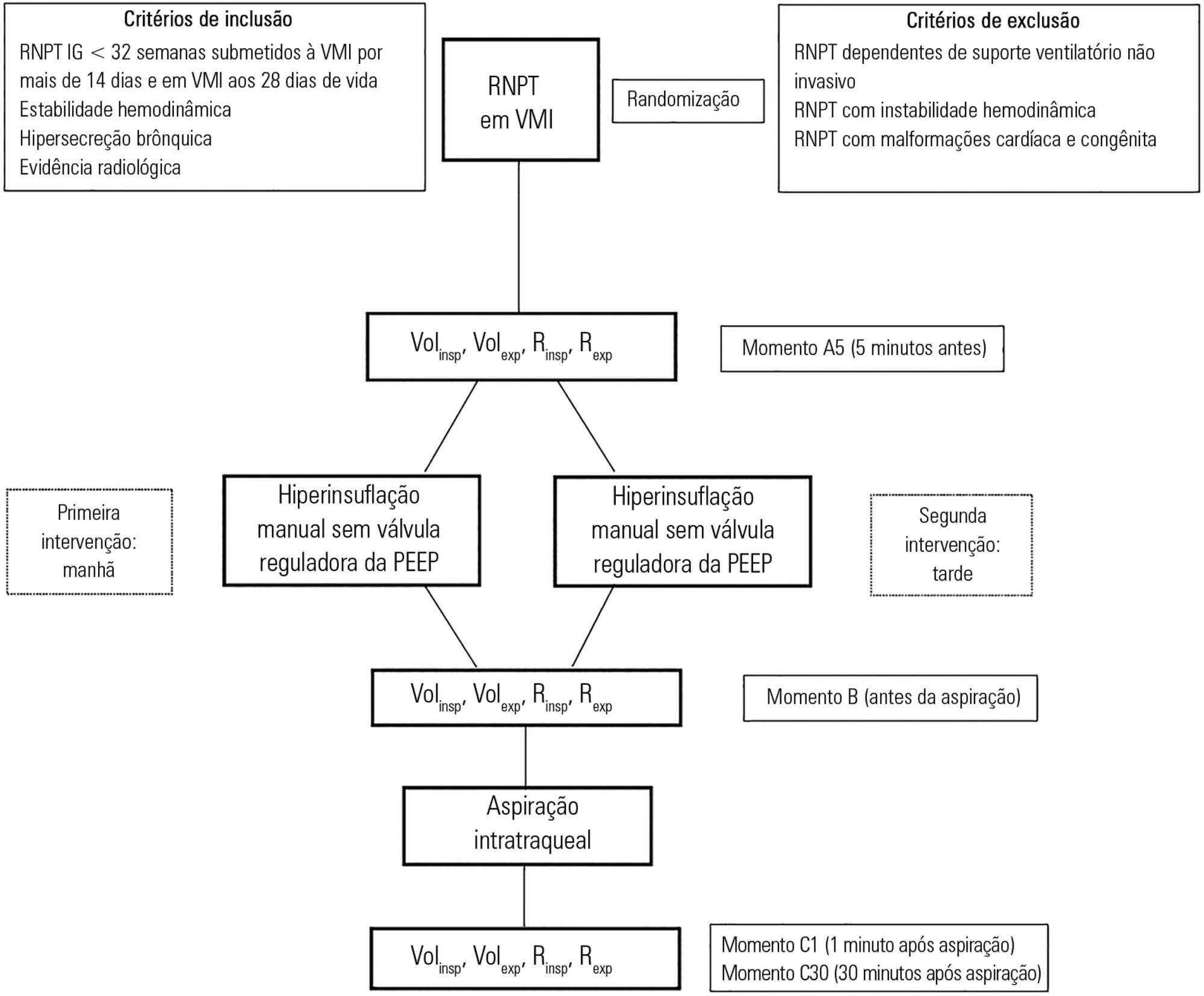
-
Letters to the Editor
To: Heliox in the treatment of status asthmaticus: case reports
Rev Bras Ter Intensiva. 2016;28(3):348-349
Abstract
Letters to the EditorTo: Heliox in the treatment of status asthmaticus: case reports
Rev Bras Ter Intensiva. 2016;28(3):348-349
DOI 10.5935/0103-507X.20160059
Views0To the Editor Bronchodilators and corticosteroids are used in clinical practice() to increase airway caliber and decrease resistance, wherein heliotherapy (heliox) may play key role. Heliox is insoluble in human tissues and has no bronchodilator or anti-inflammatory effects. However, its low density (one tenth of air density) enables a decrease in airflow resistance, regardless of […]See moreViews0Abstract
Letters to the EditorTo: Heliox in the treatment of status asthmaticus: case reports
Rev Bras Ter Intensiva. 2016;28(3):348-349
DOI 10.5935/0103-507X.20160059
Views0To the Editor Bronchodilators and corticosteroids are used in clinical practice() to increase airway caliber and decrease resistance, wherein heliotherapy (heliox) may play key role. Heliox is insoluble in human tissues and has no bronchodilator or anti-inflammatory effects. However, its low density (one tenth of air density) enables a decrease in airflow resistance, regardless of […]See more -
Letters to the Editor
To: Admission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(3):352-353
Abstract
Letters to the EditorTo: Admission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(3):352-353
DOI 10.5935/0103-507X.20160061
Views0To the editor We read the manuscript by Rodrigues et al. in the latest issue of Revista Brasileira de Terapia Intensiva Journal with great interest.() In this single-center, retrospective, observational cohort study, Rodrigues et al. aimed to identify risk factors associated with later readmission to the intensive care unit (ICU) among critically ill oncohematological patients […]See moreViews0Abstract
Letters to the EditorTo: Admission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(3):352-353
DOI 10.5935/0103-507X.20160061
Views0To the editor We read the manuscript by Rodrigues et al. in the latest issue of Revista Brasileira de Terapia Intensiva Journal with great interest.() In this single-center, retrospective, observational cohort study, Rodrigues et al. aimed to identify risk factors associated with later readmission to the intensive care unit (ICU) among critically ill oncohematological patients […]See more -
Letters to the Editor
Reply to: Admission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(3):354-355
Abstract
Letters to the EditorReply to: Admission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(3):354-355
DOI 10.5935/0103-507X.20160062
Views0We would like to thank you for the interest in our study about admission factors associated with later readmission to the intensive care unit (ICU) in an oncohematological cohort.() Aydoğdu and Esquinas correctly acknowledged that only evaluating ICU admission factors limited our analysis. Unfortunately, we evaluated an administrative database, which only had some physiological information […]See moreViews0Abstract
Letters to the EditorReply to: Admission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(3):354-355
DOI 10.5935/0103-507X.20160062
Views0We would like to thank you for the interest in our study about admission factors associated with later readmission to the intensive care unit (ICU) in an oncohematological cohort.() Aydoğdu and Esquinas correctly acknowledged that only evaluating ICU admission factors limited our analysis. Unfortunately, we evaluated an administrative database, which only had some physiological information […]See more -
Letters to the Editor
To: Contemporary treatment of children with critical and near-fatal asthma
Rev Bras Ter Intensiva. 2016;28(3):356-357
Abstract
Letters to the EditorTo: Contemporary treatment of children with critical and near-fatal asthma
Rev Bras Ter Intensiva. 2016;28(3):356-357
DOI 10.5935/0103-507X.20160063
Views1To the Editor The review article by Shein et al.() on the treatment of acute severe asthma in children is timely due to the prevalence of the disease and often variable and inconsistent disease management, which includes adjuvant therapies and depends on the availability of resources, the local practices and the preference of doctors. The […]See moreViews1Abstract
Letters to the EditorTo: Contemporary treatment of children with critical and near-fatal asthma
Rev Bras Ter Intensiva. 2016;28(3):356-357
DOI 10.5935/0103-507X.20160063
Views1To the Editor The review article by Shein et al.() on the treatment of acute severe asthma in children is timely due to the prevalence of the disease and often variable and inconsistent disease management, which includes adjuvant therapies and depends on the availability of resources, the local practices and the preference of doctors. The […]See more
Volume Articles - Critical Care Science (CCS)
