-
Commentary
Tuberculosis is always a possibility (even in the intensive care unit)
Rev Bras Ter Intensiva. 2016;28(2):97-99
Abstract
CommentaryTuberculosis is always a possibility (even in the intensive care unit)
Rev Bras Ter Intensiva. 2016;28(2):97-99
DOI 10.5935/0103-507X.20160021
Views0INTRODUCTION Community-acquired pneumonia (CAP) requiring hospitalization is mainly caused by Streptococcus pneumoniae and respiratory viruses.() Among patients with severe CAP, including those requiring admission to an intensive care unit, additional important pathogens include Staphylococcus aureus, Gram-negative bacteria, and Legionella pneumophila.(,) Typically, Mycobacterium tuberculosis is not a pathogen that is strongly considered in patients with CAP […]See moreViews0

Abstract
CommentaryTuberculosis is always a possibility (even in the intensive care unit)
Rev Bras Ter Intensiva. 2016;28(2):97-99
DOI 10.5935/0103-507X.20160021
Views0INTRODUCTIONCommunity-acquired pneumonia (CAP) requiring hospitalization is mainly caused by Streptococcus pneumoniae and respiratory viruses.() Among patients with severe CAP, including those requiring admission to an intensive care unit, additional important pathogens include Staphylococcus aureus, Gram-negative bacteria, and Legionella pneumophila.(,)Typically, Mycobacterium tuberculosis is not a pathogen that is strongly considered in patients with CAP because it […]See more -
Commentary
Glutamine in critically ill patients: is it a fundamental nutritional supplement?
Rev Bras Ter Intensiva. 2016;28(2):100-103
Abstract
CommentaryGlutamine in critically ill patients: is it a fundamental nutritional supplement?
Rev Bras Ter Intensiva. 2016;28(2):100-103
DOI 10.5935/0103-507X.20160022
Views0What should the researchers of glutamine effects on the intensive care unit population be aware of in the future?In future studies, we need to learn more about glutamine kinetics, the relationship between plasma glutamine concentration, and endogenous glutamine production along the evolution of critically ill patients. It will be important to know whether glutamine kinetics […]See moreViews0Abstract
CommentaryGlutamine in critically ill patients: is it a fundamental nutritional supplement?
Rev Bras Ter Intensiva. 2016;28(2):100-103
DOI 10.5935/0103-507X.20160022
Views0What should the researchers of glutamine effects on the intensive care unit population be aware of in the future?In future studies, we need to learn more about glutamine kinetics, the relationship between plasma glutamine concentration, and endogenous glutamine production along the evolution of critically ill patients. It will be important to know whether glutamine kinetics […]See more -
Commentary
Recruitment maneuvers for acute respiratory distress syndrome: the panorama in 2016
Rev Bras Ter Intensiva. 2016;28(2):104-106
Abstract
CommentaryRecruitment maneuvers for acute respiratory distress syndrome: the panorama in 2016
Rev Bras Ter Intensiva. 2016;28(2):104-106
DOI 10.5935/0103-507X.20160023
Views0CONCLUSIONEven though experimental studies, systematic reviews, and meta-analyses have suggested that RMs are associated with beneficial effects for lung function and morphology in ARDS, their impact on clinical outcomes is still being debated. Different methods with different benefit and risk profiles have been used to recruit the lungs, and further studies are required to identify […]See moreViews0Abstract
CommentaryRecruitment maneuvers for acute respiratory distress syndrome: the panorama in 2016
Rev Bras Ter Intensiva. 2016;28(2):104-106
DOI 10.5935/0103-507X.20160023
Views0CONCLUSIONEven though experimental studies, systematic reviews, and meta-analyses have suggested that RMs are associated with beneficial effects for lung function and morphology in ARDS, their impact on clinical outcomes is still being debated. Different methods with different benefit and risk profiles have been used to recruit the lungs, and further studies are required to identify […]See more -
Original Article
Factors associated with job and personal satisfaction in adult Brazilian intensivists
Rev Bras Ter Intensiva. 2016;28(2):107-113
Abstract
Original ArticleFactors associated with job and personal satisfaction in adult Brazilian intensivists
Rev Bras Ter Intensiva. 2016;28(2):107-113
DOI 10.5935/0103-507X.20160024
Views0See moreABSTRACT
Objective:
To evaluate job and personal satisfaction rates in physicians who work in adult intensive care units and to identify the factors associated with satisfaction.
Methods:
A cross-sectional study performed with physicians who participated in two intensive medicine online discussion groups. A questionnaire designed to assess the physician’s sociodemographic profile and job was available for both groups for 3 months. At the end of the questionnaire, the participants addressed their degrees of job and personal satisfaction using a Likert scale in which 1 represented “very dissatisfied” and 5 represented “very satisfied”. The association between sociodemographic and job characteristics with job and personal satisfaction was evaluated. Variables independently associated with satisfaction were identified using a logistic regression model.
Results:
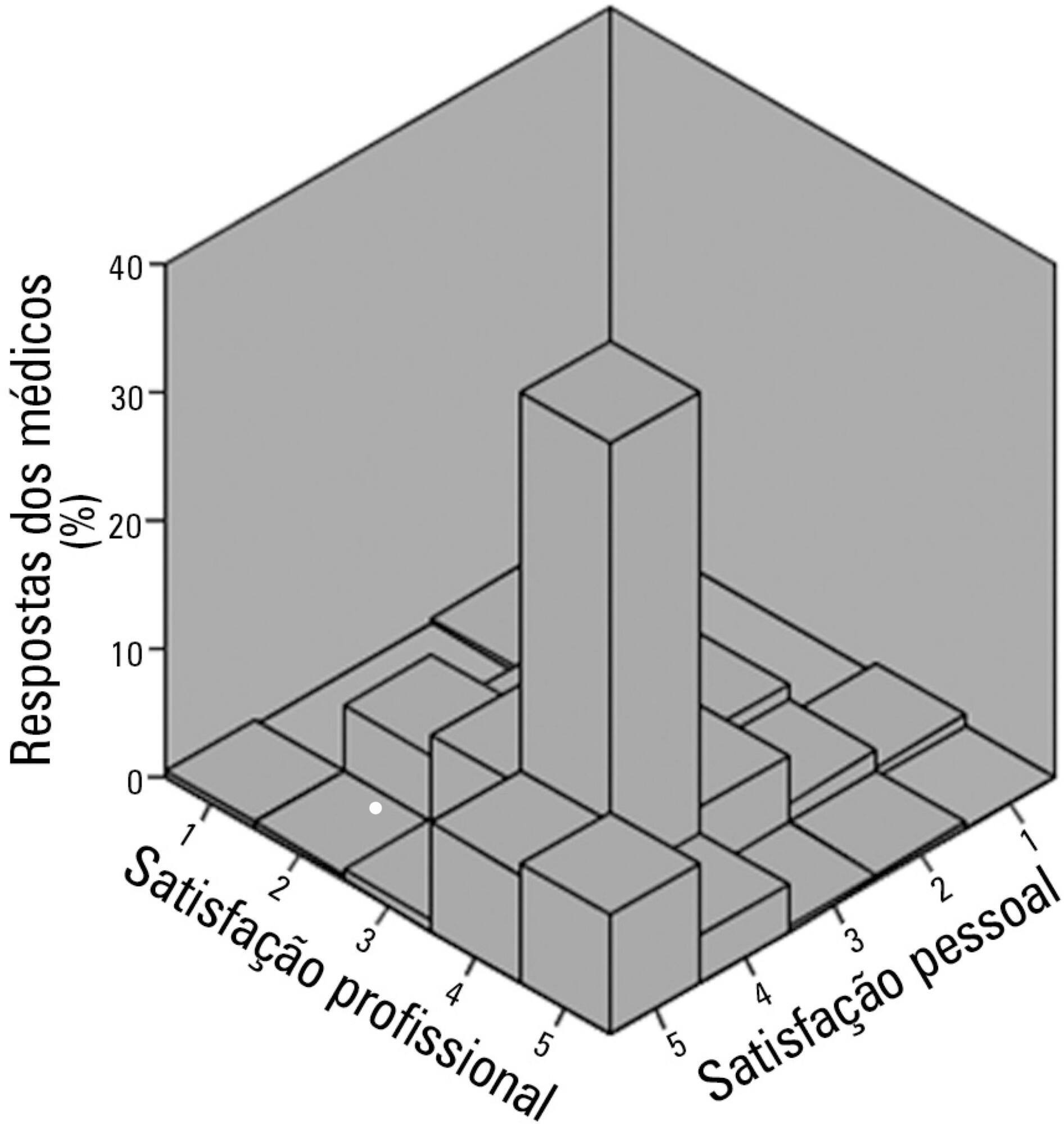
The questionnaire was answered by 250 physicians, of which 137 (54.8%) declared they were satisfied with their jobs and 34 (13.5%) were very satisfied. None of the evaluated characteristics were independently associated with job satisfaction. Regarding personal satisfaction, 136 (54.4%) physicians reported being satisfied, and 48 (19.9%) reported being very satisfied. Job satisfaction (OR = 7.21; 95%CI 3.21 – 16.20) and working in a university hospital (OR = 3.24; 95%CI 1.29 – 8.15) were factors independently associated with the personal satisfaction of the participants.
Conclusion:
The participant physicians reported job and personal satisfaction with their work in intensive care. Job satisfaction and working in a university hospital were independently associated with greater personal satisfaction.
Views0Abstract
Original ArticleFactors associated with job and personal satisfaction in adult Brazilian intensivists
Rev Bras Ter Intensiva. 2016;28(2):107-113
DOI 10.5935/0103-507X.20160024
Views0See moreABSTRACT
Objective:
To evaluate job and personal satisfaction rates in physicians who work in adult intensive care units and to identify the factors associated with satisfaction.
Methods:
A cross-sectional study performed with physicians who participated in two intensive medicine online discussion groups. A questionnaire designed to assess the physician’s sociodemographic profile and job was available for both groups for 3 months. At the end of the questionnaire, the participants addressed their degrees of job and personal satisfaction using a Likert scale in which 1 represented “very dissatisfied” and 5 represented “very satisfied”. The association between sociodemographic and job characteristics with job and personal satisfaction was evaluated. Variables independently associated with satisfaction were identified using a logistic regression model.
Results:
The questionnaire was answered by 250 physicians, of which 137 (54.8%) declared they were satisfied with their jobs and 34 (13.5%) were very satisfied. None of the evaluated characteristics were independently associated with job satisfaction. Regarding personal satisfaction, 136 (54.4%) physicians reported being satisfied, and 48 (19.9%) reported being very satisfied. Job satisfaction (OR = 7.21; 95%CI 3.21 – 16.20) and working in a university hospital (OR = 3.24; 95%CI 1.29 – 8.15) were factors independently associated with the personal satisfaction of the participants.
Conclusion:
The participant physicians reported job and personal satisfaction with their work in intensive care. Job satisfaction and working in a university hospital were independently associated with greater personal satisfaction.
-
Original Article
Mobility decline in patients hospitalized in an intensive care unit
Rev Bras Ter Intensiva. 2016;28(2):114-119
Abstract
Original ArticleMobility decline in patients hospitalized in an intensive care unit
Rev Bras Ter Intensiva. 2016;28(2):114-119
DOI 10.5935/0103-507X.20160025
Views0See moreABSTRACT
Objective:
To evaluate the variation in mobility during hospitalization in an intensive care unit and its association with hospital mortality.
Methods:
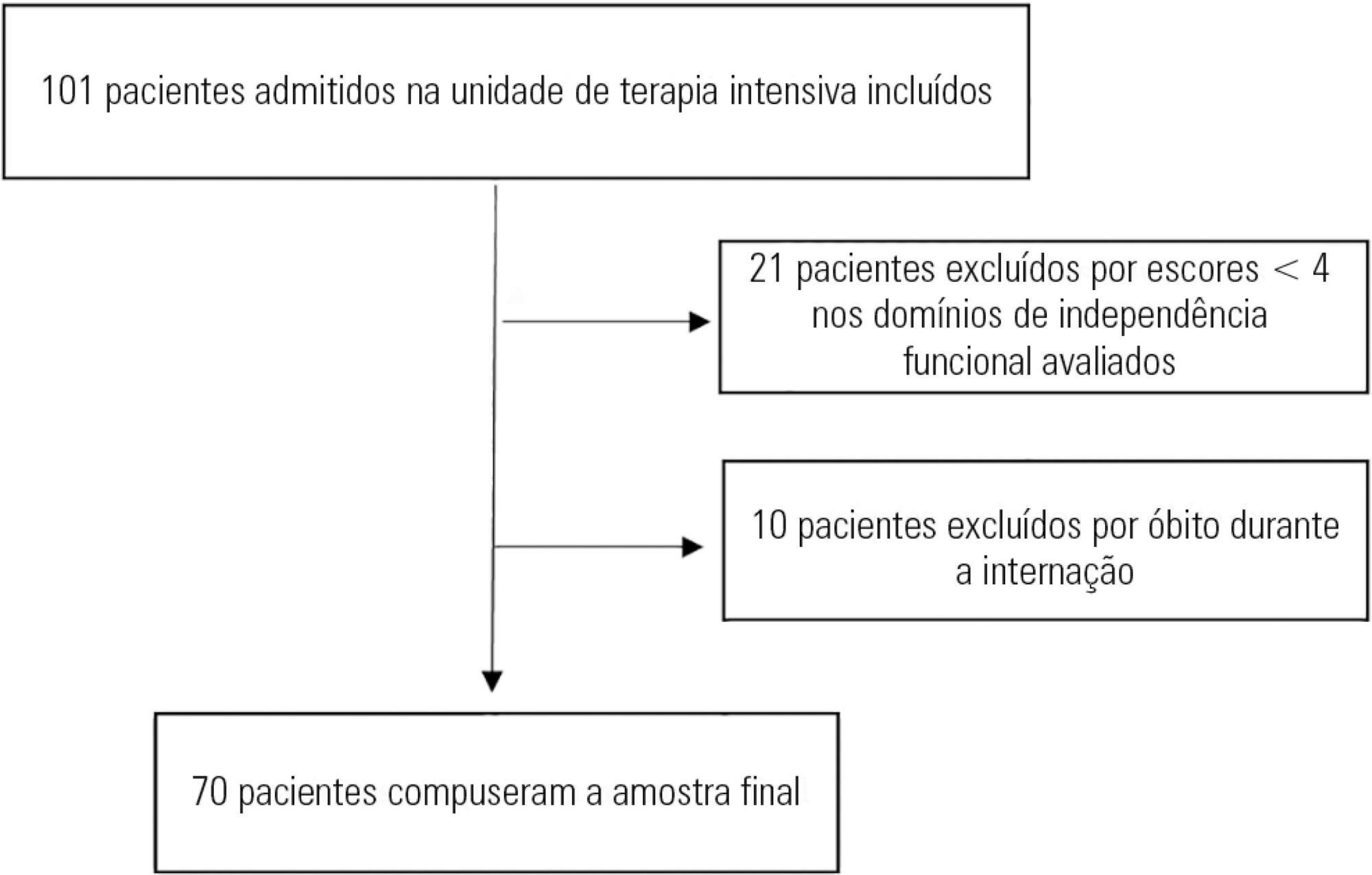
This prospective study was conducted in an intensive care unit. The inclusion criteria included patients admitted with an independence score of ≥ 4 for both bed-chair transfer and locomotion, with the score based on the Functional Independence Measure. Patients with cardiac arrest and/or those who died during hospitalization were excluded. To measure the loss of mobility, the value obtained at discharge was calculated and subtracted from the value obtained on admission, which was then divided by the admission score and recorded as a percentage.
Results:
The comparison of these two variables indicated that the loss of mobility during hospitalization was 14.3% (p < 0.001). Loss of mobility was greater in patients hospitalized for more than 48 hours in the intensive care unit (p < 0.02) and in patients who used vasopressor drugs (p = 0.041). However, the comparison between subjects aged 60 years or older and those younger than 60 years indicated no significant differences in the loss of mobility (p = 0.332), reason for hospitalization (p = 0.265), SAPS 3 score (p = 0.224), use of mechanical ventilation (p = 0.117), or hospital mortality (p = 0.063).
Conclusion:
There was loss of mobility during hospitalization in the intensive care unit. This loss was greater in patients who were hospitalized for more than 48 hours and in those who used vasopressors; however, the causal and prognostic factors associated with this decline need to be elucidated.
Views0Abstract
Original ArticleMobility decline in patients hospitalized in an intensive care unit
Rev Bras Ter Intensiva. 2016;28(2):114-119
DOI 10.5935/0103-507X.20160025
Views0See moreABSTRACT
Objective:
To evaluate the variation in mobility during hospitalization in an intensive care unit and its association with hospital mortality.
Methods:
This prospective study was conducted in an intensive care unit. The inclusion criteria included patients admitted with an independence score of ≥ 4 for both bed-chair transfer and locomotion, with the score based on the Functional Independence Measure. Patients with cardiac arrest and/or those who died during hospitalization were excluded. To measure the loss of mobility, the value obtained at discharge was calculated and subtracted from the value obtained on admission, which was then divided by the admission score and recorded as a percentage.
Results:
The comparison of these two variables indicated that the loss of mobility during hospitalization was 14.3% (p < 0.001). Loss of mobility was greater in patients hospitalized for more than 48 hours in the intensive care unit (p < 0.02) and in patients who used vasopressor drugs (p = 0.041). However, the comparison between subjects aged 60 years or older and those younger than 60 years indicated no significant differences in the loss of mobility (p = 0.332), reason for hospitalization (p = 0.265), SAPS 3 score (p = 0.224), use of mechanical ventilation (p = 0.117), or hospital mortality (p = 0.063).
Conclusion:
There was loss of mobility during hospitalization in the intensive care unit. This loss was greater in patients who were hospitalized for more than 48 hours and in those who used vasopressors; however, the causal and prognostic factors associated with this decline need to be elucidated.
-
Original Article
Insights about serum sodium behavior after 24 hours of continuous renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(2):120-131
Abstract
Original ArticleInsights about serum sodium behavior after 24 hours of continuous renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(2):120-131
DOI 10.5935/0103-507X.20160026
Views0See moreABSTRACT
Objective:
The aim of this study was to investigate the clinical and laboratorial factors associated with serum sodium variation during continuous renal replacement therapy and to assess whether the perfect admixture formula could predict 24-hour sodium variation.
Methods:
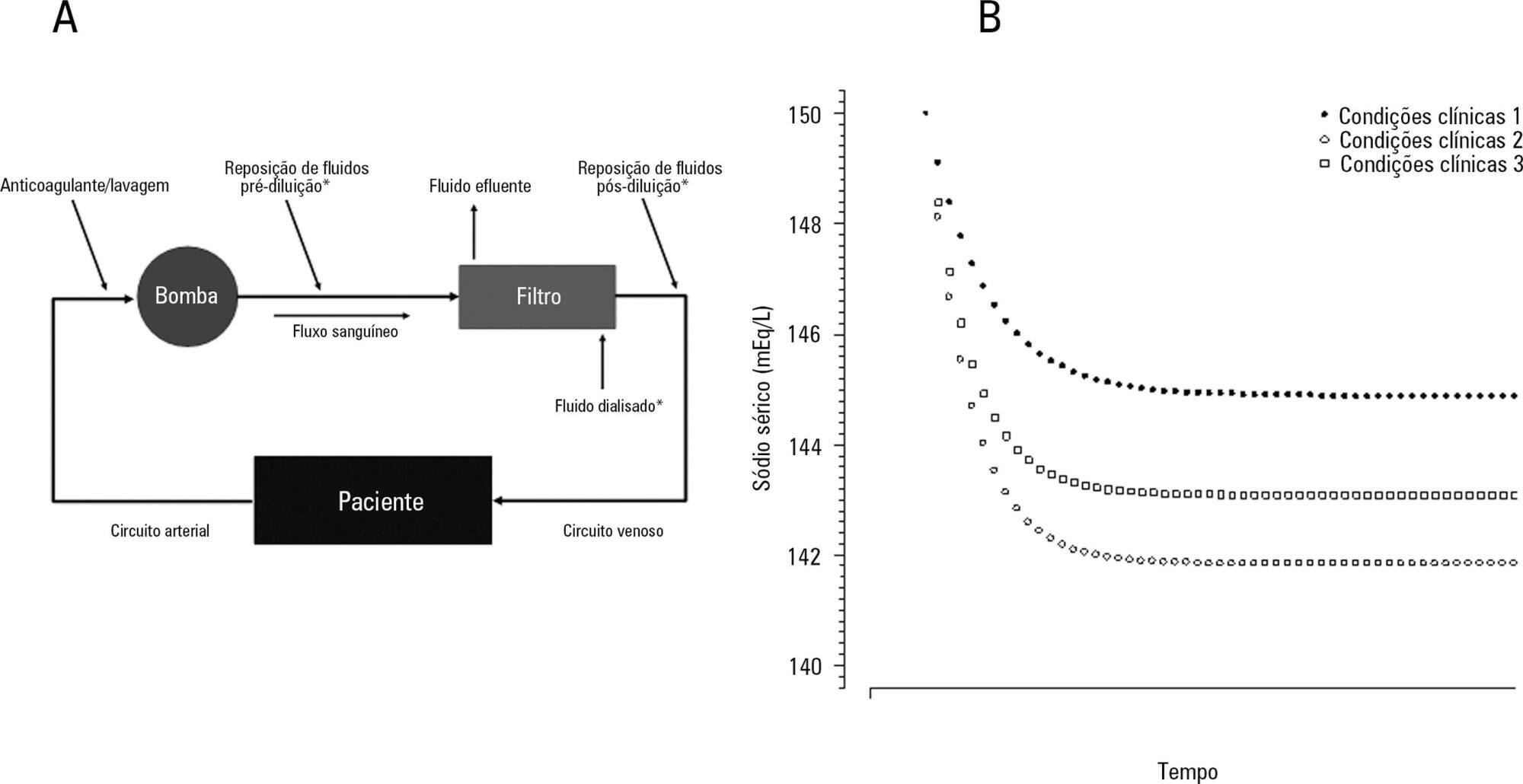
Thirty-six continuous renal replacement therapy sessions of 33 patients, in which the affluent prescription was unchanged during the first 24 hours, were retrieved from a prospective collected database and then analyzed. A mixed linear model was performed to investigate the factors associated with large serum sodium variations (≥ 8mEq/L), and a Bland-Altman plot was generated to assess the agreement between the predicted and observed variations.
Results:
In continuous renal replacement therapy 24-hour sessions, SAPS 3 (p = 0.022) and baseline hypernatremia (p = 0.023) were statistically significant predictors of serum sodium variations ≥ 8mEq/L in univariate analysis, but only hypernatremia demonstrated an independent association (β = 0.429, p < 0.001). The perfect admixture formula for sodium prediction at 24 hours demonstrated poor agreement with the observed values.
Conclusions:
Hypernatremia at the time of continuous renal replacement therapy initiation is an important factor associated with clinically significant serum sodium variation. The use of 4% citrate or acid citrate dextrose – formula A 2.2% as anticoagulants was not associated with higher serum sodium variations. A mathematical prediction for the serum sodium concentration after 24 hours was not feasible.
Views0Abstract
Original ArticleInsights about serum sodium behavior after 24 hours of continuous renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(2):120-131
DOI 10.5935/0103-507X.20160026
Views0See moreABSTRACT
Objective:
The aim of this study was to investigate the clinical and laboratorial factors associated with serum sodium variation during continuous renal replacement therapy and to assess whether the perfect admixture formula could predict 24-hour sodium variation.
Methods:
Thirty-six continuous renal replacement therapy sessions of 33 patients, in which the affluent prescription was unchanged during the first 24 hours, were retrieved from a prospective collected database and then analyzed. A mixed linear model was performed to investigate the factors associated with large serum sodium variations (≥ 8mEq/L), and a Bland-Altman plot was generated to assess the agreement between the predicted and observed variations.
Results:
In continuous renal replacement therapy 24-hour sessions, SAPS 3 (p = 0.022) and baseline hypernatremia (p = 0.023) were statistically significant predictors of serum sodium variations ≥ 8mEq/L in univariate analysis, but only hypernatremia demonstrated an independent association (β = 0.429, p < 0.001). The perfect admixture formula for sodium prediction at 24 hours demonstrated poor agreement with the observed values.
Conclusions:
Hypernatremia at the time of continuous renal replacement therapy initiation is an important factor associated with clinically significant serum sodium variation. The use of 4% citrate or acid citrate dextrose – formula A 2.2% as anticoagulants was not associated with higher serum sodium variations. A mathematical prediction for the serum sodium concentration after 24 hours was not feasible.
-
Original Article
Communication of mechanically ventilated patients in intensive care units
Rev Bras Ter Intensiva. 2016;28(2):132-140
Abstract
Original ArticleCommunication of mechanically ventilated patients in intensive care units
Rev Bras Ter Intensiva. 2016;28(2):132-140
DOI 10.5935/0103-507X.20160027
Views0ABSTRACT
Objective:
The aim of this study was to translate and culturally and linguistically adapt the Ease of Communication Scale and to assess the level of communication difficulties for patients undergoing mechanical ventilation with orotracheal intubation, relating these difficulties to clinical and sociodemographic variables.
Methods:
This study had three stages: (1) cultural and linguistic adaptation of the Ease of Communication Scale; (2) preliminary assessment of its psychometric properties; and (3) observational, descriptive-correlational and cross-sectional study, conducted from March to August 2015, based on the Ease of Communication Scale – after extubation answers and clinical and sociodemographic variables of 31 adult patients who were extubated, clinically stable and admitted to five Portuguese intensive care units.
Results:
Expert analysis showed high agreement on content (100%) and relevance (75%). The pretest scores showed a high acceptability regarding the completion of the instrument and its usefulness. The Ease of Communication Scale showed excellent internal consistency (0.951 Cronbach’s alpha). The factor analysis explained approximately 81% of the total variance with two scale components. On average, the patients considered the communication experiences during intubation to be “quite hard” (2.99). No significant correlation was observed between the communication difficulties reported and the studied sociodemographic and clinical variables, except for the clinical variable “number of hours after extubation” (p < 0.05).
Conclusion:
This study translated and adapted the first assessment instrument of communication difficulties for mechanically ventilated patients in intensive care units into European Portuguese. The preliminary scale validation suggested high reliability. Patients undergoing mechanical ventilation reported that communication during intubation was “quite hard”, and these communication difficulties apparently existed regardless of the presence of other clinical and/or sociodemographic variables.
Keywords:CommunicationCommunication barriersIntensive care unitsmechanical ventilationNonverbal communicationSpeech-language pathologySee moreViews0Abstract
Original ArticleCommunication of mechanically ventilated patients in intensive care units
Rev Bras Ter Intensiva. 2016;28(2):132-140
DOI 10.5935/0103-507X.20160027
Views0ABSTRACT
Objective:
The aim of this study was to translate and culturally and linguistically adapt the Ease of Communication Scale and to assess the level of communication difficulties for patients undergoing mechanical ventilation with orotracheal intubation, relating these difficulties to clinical and sociodemographic variables.
Methods:
This study had three stages: (1) cultural and linguistic adaptation of the Ease of Communication Scale; (2) preliminary assessment of its psychometric properties; and (3) observational, descriptive-correlational and cross-sectional study, conducted from March to August 2015, based on the Ease of Communication Scale – after extubation answers and clinical and sociodemographic variables of 31 adult patients who were extubated, clinically stable and admitted to five Portuguese intensive care units.
Results:
Expert analysis showed high agreement on content (100%) and relevance (75%). The pretest scores showed a high acceptability regarding the completion of the instrument and its usefulness. The Ease of Communication Scale showed excellent internal consistency (0.951 Cronbach’s alpha). The factor analysis explained approximately 81% of the total variance with two scale components. On average, the patients considered the communication experiences during intubation to be “quite hard” (2.99). No significant correlation was observed between the communication difficulties reported and the studied sociodemographic and clinical variables, except for the clinical variable “number of hours after extubation” (p < 0.05).
Conclusion:
This study translated and adapted the first assessment instrument of communication difficulties for mechanically ventilated patients in intensive care units into European Portuguese. The preliminary scale validation suggested high reliability. Patients undergoing mechanical ventilation reported that communication during intubation was “quite hard”, and these communication difficulties apparently existed regardless of the presence of other clinical and/or sociodemographic variables.
Keywords:CommunicationCommunication barriersIntensive care unitsmechanical ventilationNonverbal communicationSpeech-language pathologySee more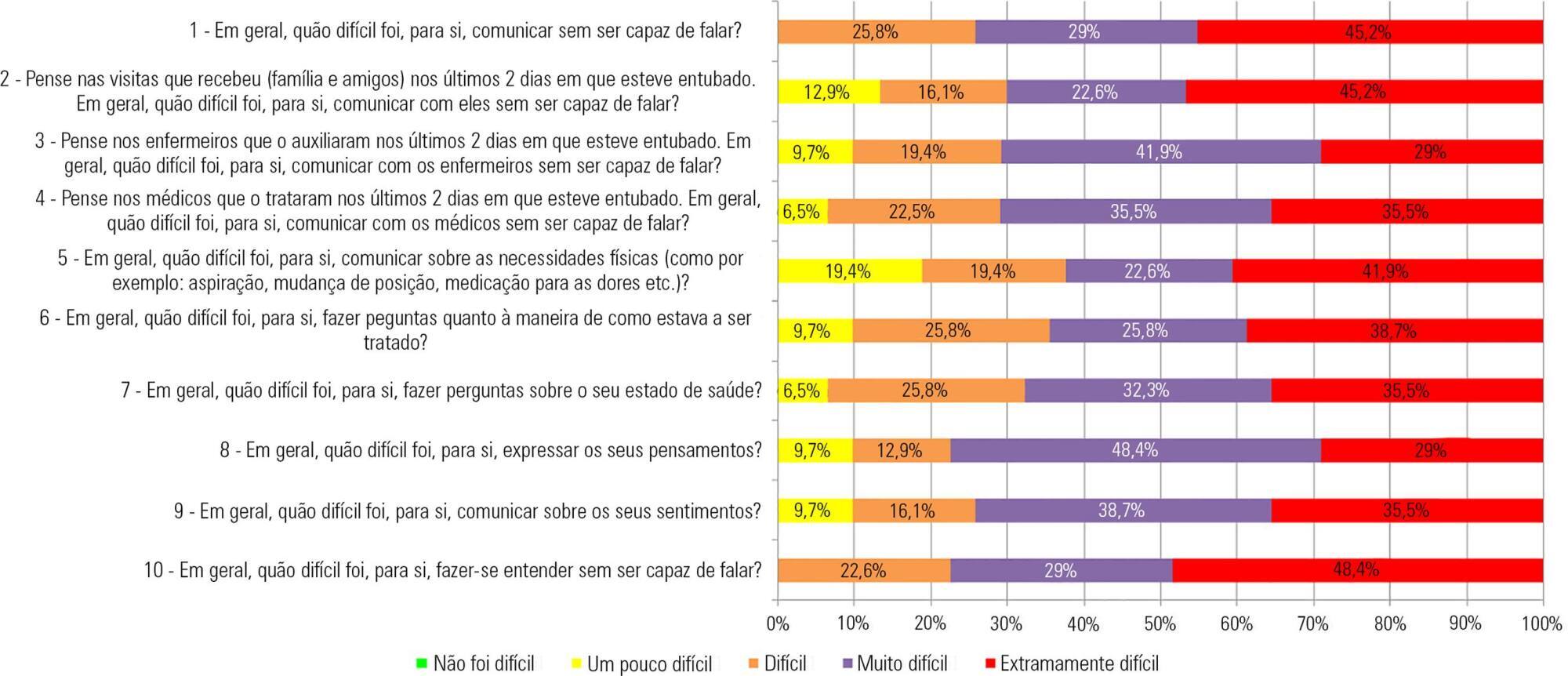
-
Original Article
Non-aneurysmal spontaneous subarachnoid hemorrhage: perimesencephalic versus non-perimesencephalic
Rev Bras Ter Intensiva. 2016;28(2):141-146
Abstract
Original ArticleNon-aneurysmal spontaneous subarachnoid hemorrhage: perimesencephalic versus non-perimesencephalic
Rev Bras Ter Intensiva. 2016;28(2):141-146
DOI 10.5935/0103-507X.20160028
Views0ABSTRACT
Objective:
To compare the clinical evolution of perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage.
Methods:
The study was conducted retrospectively in a tertiary hospital center in the north region of Portugal. Included patients had no identifiable cause for subarachnoid hemorrhage. Several epidemiologic, clinical and imaging aspects were statistically analyzed, taking into account the differences in perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage.
Results:
Sixty-two patients met the inclusion criteria (46.8% – perimesencephalic subarachnoid hemorrhage; 53.2% – non-perimesencephalic subarachnoid hemorrhage). Demographic and clinical background characteristics were similar in both groups. Complications were more frequent in patients with non-perimesencephalic subarachnoid hemorrhage – 84.8% of the patients had at least one complication versus 48.3% in perimesencephalic subarachnoid hemorrhage. Vasospasm, infection and hydrocephaly were the most common complications (each was detected more frequently in the non-perimesencephalic subarachnoid hemorrhage group than in perimesencephalic subarachnoid hemorrhage group). Two patients died, both had a non-perimesencephalic subarachnoid hemorrhage. The median inpatient time was longer in the non-perimesencephalic subarachnoid hemorrhage group (21 versus 14 days). No incidents of rebleeding were reported during the follow-up period (mean time of 15 ± 10.3 months).
Conclusion:
Perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage are two different entities that have different clinical outcomes, namely in terms of complication rate and median inpatient time. The management of these patients should respect this difference to improve treatment and optimize health care resources.
Keywords:Angiography, digital subtractionHydrocephalyInpatientsSubarachnoid hemorrhageTomography, X-ray computedVasospasm, intracranialSee moreViews0Abstract
Original ArticleNon-aneurysmal spontaneous subarachnoid hemorrhage: perimesencephalic versus non-perimesencephalic
Rev Bras Ter Intensiva. 2016;28(2):141-146
DOI 10.5935/0103-507X.20160028
Views0ABSTRACT
Objective:
To compare the clinical evolution of perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage.
Methods:
The study was conducted retrospectively in a tertiary hospital center in the north region of Portugal. Included patients had no identifiable cause for subarachnoid hemorrhage. Several epidemiologic, clinical and imaging aspects were statistically analyzed, taking into account the differences in perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage.
Results:
Sixty-two patients met the inclusion criteria (46.8% – perimesencephalic subarachnoid hemorrhage; 53.2% – non-perimesencephalic subarachnoid hemorrhage). Demographic and clinical background characteristics were similar in both groups. Complications were more frequent in patients with non-perimesencephalic subarachnoid hemorrhage – 84.8% of the patients had at least one complication versus 48.3% in perimesencephalic subarachnoid hemorrhage. Vasospasm, infection and hydrocephaly were the most common complications (each was detected more frequently in the non-perimesencephalic subarachnoid hemorrhage group than in perimesencephalic subarachnoid hemorrhage group). Two patients died, both had a non-perimesencephalic subarachnoid hemorrhage. The median inpatient time was longer in the non-perimesencephalic subarachnoid hemorrhage group (21 versus 14 days). No incidents of rebleeding were reported during the follow-up period (mean time of 15 ± 10.3 months).
Conclusion:
Perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage are two different entities that have different clinical outcomes, namely in terms of complication rate and median inpatient time. The management of these patients should respect this difference to improve treatment and optimize health care resources.
Keywords:Angiography, digital subtractionHydrocephalyInpatientsSubarachnoid hemorrhageTomography, X-ray computedVasospasm, intracranialSee more -
Original Article
Drug incompatibilities in the adult intensive care unit of a university hospital
Rev Bras Ter Intensiva. 2016;28(2):147-153
Abstract
Original ArticleDrug incompatibilities in the adult intensive care unit of a university hospital
Rev Bras Ter Intensiva. 2016;28(2):147-153
DOI 10.5935/0103-507X.20160029
Views0ABSTRACT
Objectives:
This study sought to identify the physical and chemical incompatibilities among the drugs administered intravenously to patients admitted to an adult intensive care unit. We also aimed to establish pharmaceutical guidelines for administering incompatible drugs.
Methods:
This cross-sectional, prospective, and quantitative study was conducted from July to September 2015. Drug incompatibilities were identified based on an analysis of the patient prescriptions available in the hospital online management system. A pharmaceutical intervention was performed using the guidelines on the preparation and administration of incompatible drugs. Adherence to those guidelines was subsequently assessed among the nursing staff.
Results:
A total of 100 prescriptions were analyzed; 68 were incompatible with the intravenous drugs prescribed. A total of 271 drug incompatibilities were found, averaging 4.0 ± 3.3 incompatibilities per prescription. The most commonly found drug incompatibilities were between midazolam and hydrocortisone (8.9%), between cefepime and midazolam (5.2%), and between hydrocortisone and vancomycin (5.2%). The drugs most commonly involved in incompatibilities were midazolam, hydrocortisone, and vancomycin. The most common incompatibilities occurred when a drug was administered via continuous infusion and another was administered intermittently (50%). Of the 68 prescriptions that led to pharmaceutical guidelines, 45 (66.2%) were fully adhered to by the nursing staff.
Conclusion:
Patients under intensive care were subjected to a high rate of incompatibilities. Drug incompatibilities can be identified and eliminated by the pharmacist on the multidisciplinary team, thereby reducing undesirable effects among patients.
Keywords:Administration, intravenousCritical careDrug incompatibilityIntensive care unitsPharmaceutical servicesSee moreViews0Abstract
Original ArticleDrug incompatibilities in the adult intensive care unit of a university hospital
Rev Bras Ter Intensiva. 2016;28(2):147-153
DOI 10.5935/0103-507X.20160029
Views0ABSTRACT
Objectives:
This study sought to identify the physical and chemical incompatibilities among the drugs administered intravenously to patients admitted to an adult intensive care unit. We also aimed to establish pharmaceutical guidelines for administering incompatible drugs.
Methods:
This cross-sectional, prospective, and quantitative study was conducted from July to September 2015. Drug incompatibilities were identified based on an analysis of the patient prescriptions available in the hospital online management system. A pharmaceutical intervention was performed using the guidelines on the preparation and administration of incompatible drugs. Adherence to those guidelines was subsequently assessed among the nursing staff.
Results:
A total of 100 prescriptions were analyzed; 68 were incompatible with the intravenous drugs prescribed. A total of 271 drug incompatibilities were found, averaging 4.0 ± 3.3 incompatibilities per prescription. The most commonly found drug incompatibilities were between midazolam and hydrocortisone (8.9%), between cefepime and midazolam (5.2%), and between hydrocortisone and vancomycin (5.2%). The drugs most commonly involved in incompatibilities were midazolam, hydrocortisone, and vancomycin. The most common incompatibilities occurred when a drug was administered via continuous infusion and another was administered intermittently (50%). Of the 68 prescriptions that led to pharmaceutical guidelines, 45 (66.2%) were fully adhered to by the nursing staff.
Conclusion:
Patients under intensive care were subjected to a high rate of incompatibilities. Drug incompatibilities can be identified and eliminated by the pharmacist on the multidisciplinary team, thereby reducing undesirable effects among patients.
Keywords:Administration, intravenousCritical careDrug incompatibilityIntensive care unitsPharmaceutical servicesSee more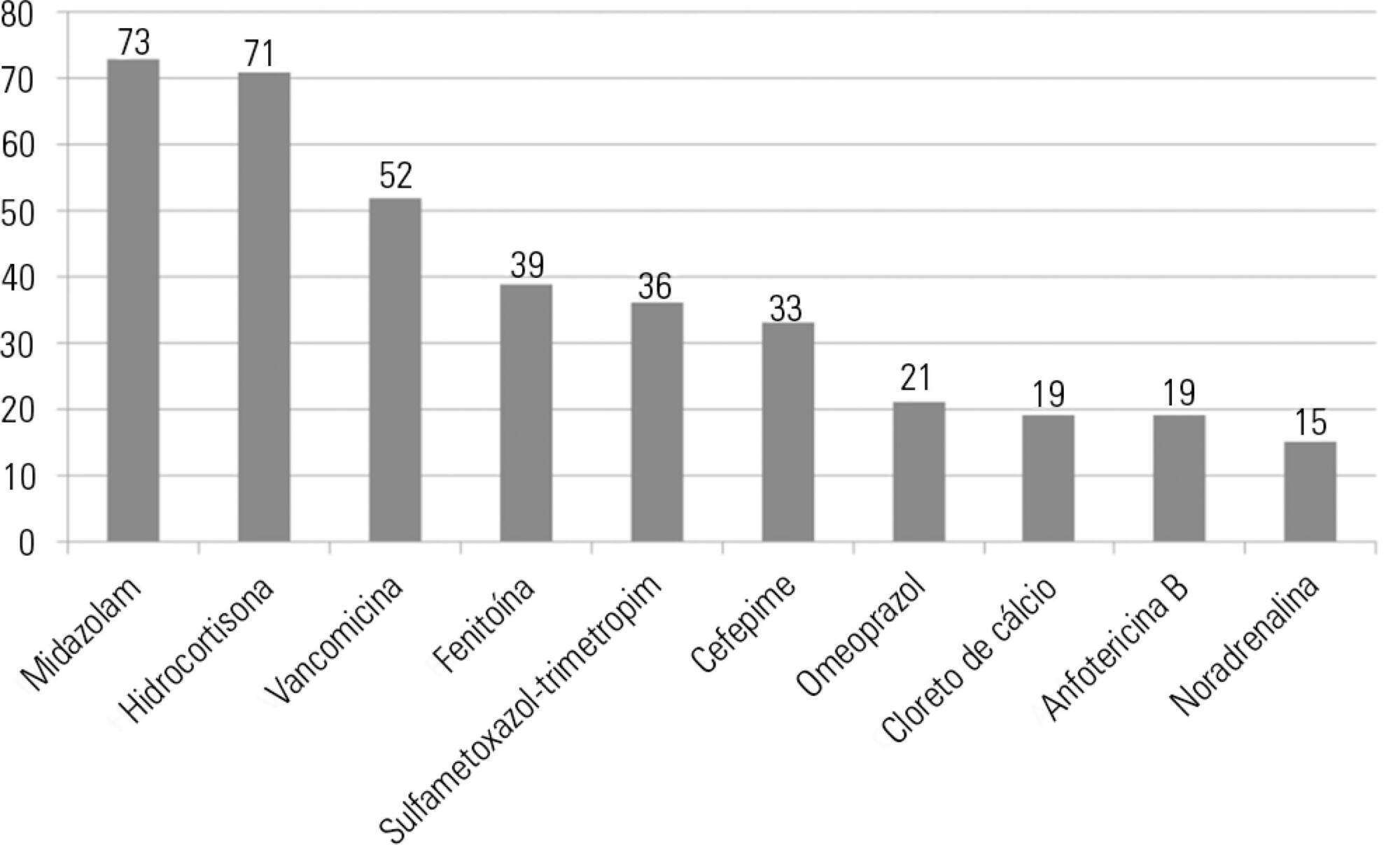
-
Original Article
Atrial natriuretic factor: is it responsible for hyponatremia and natriuresis in neurosurgery?
Rev Bras Ter Intensiva. 2016;28(2):154-160
Abstract
Original ArticleAtrial natriuretic factor: is it responsible for hyponatremia and natriuresis in neurosurgery?
Rev Bras Ter Intensiva. 2016;28(2):154-160
DOI 10.5935/0103-507X.20160030
Views0See moreABSTRACT
Objective:
To evaluate the presence of hyponatremia and natriuresis and their association with atrial natriuretic factor in neurosurgery patients.
Methods:
The study included 30 patients who had been submitted to intracranial tumor resection and cerebral aneurism clipping. Both plasma and urinary sodium and plasma atrial natriuretic factor were measured during the preoperative and postoperative time periods.
Results:
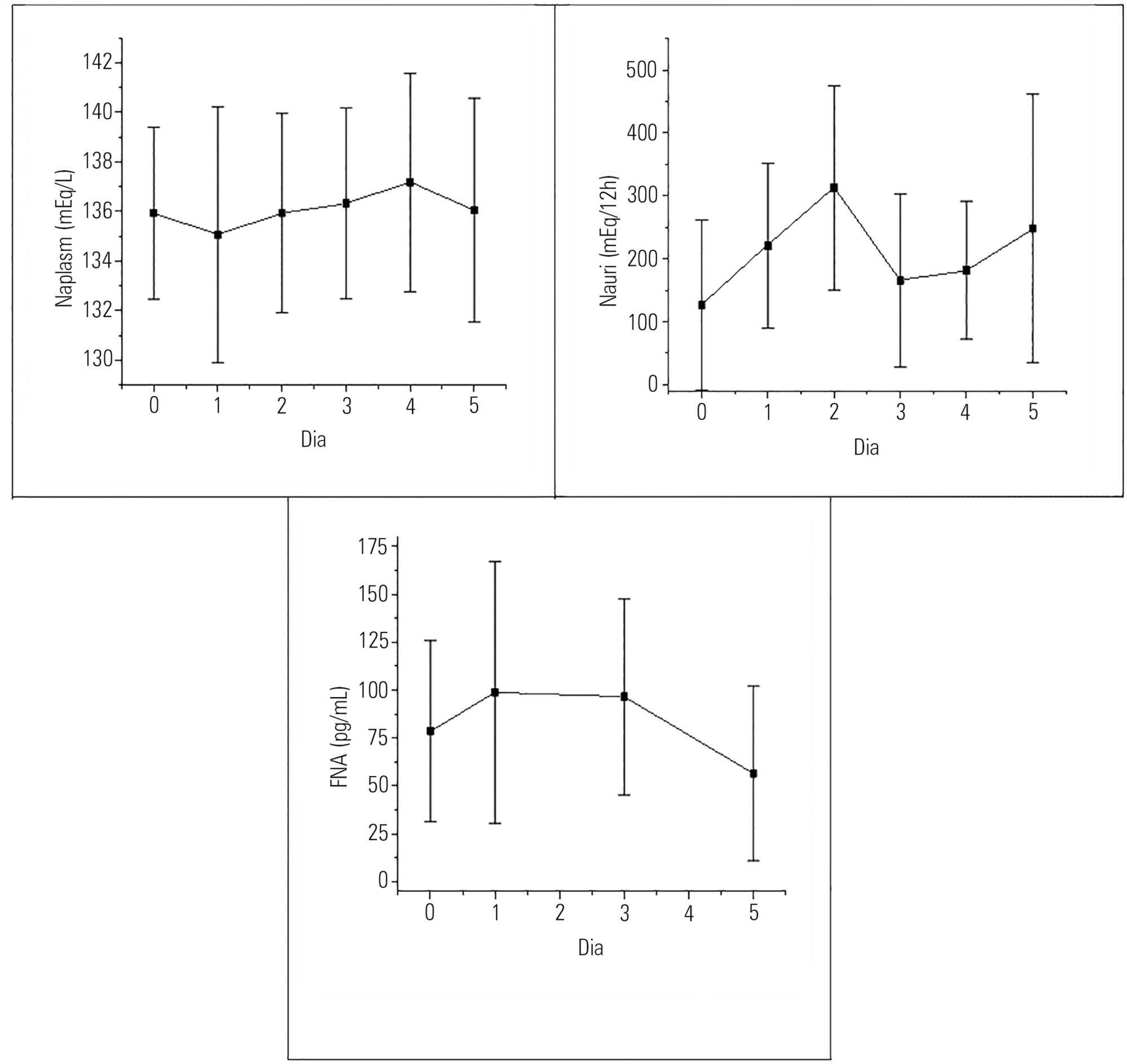
Hyponatremia was present in 63.33% of the patients, particularly on the first postoperative day. Natriuresis was present in 93.33% of the patients, particularly on the second postoperative day. Plasma atrial natriuretic factor was increased in 92.60% of the patients in at least one of the postoperative days; however, there was no statistically significant association between the atrial natriuretic factor and plasma sodium and between the atrial natriuretic factor and urinary sodium.
Conclusion:
Hyponatremia and natriuresis were present in most patients after neurosurgery; however, the atrial natriuretic factor cannot be considered to be directly responsible for these alterations in neurosurgery patients. Other natriuretic factors are likely to be involved.
Views0Abstract
Original ArticleAtrial natriuretic factor: is it responsible for hyponatremia and natriuresis in neurosurgery?
Rev Bras Ter Intensiva. 2016;28(2):154-160
DOI 10.5935/0103-507X.20160030
Views0See moreABSTRACT
Objective:
To evaluate the presence of hyponatremia and natriuresis and their association with atrial natriuretic factor in neurosurgery patients.
Methods:
The study included 30 patients who had been submitted to intracranial tumor resection and cerebral aneurism clipping. Both plasma and urinary sodium and plasma atrial natriuretic factor were measured during the preoperative and postoperative time periods.
Results:
Hyponatremia was present in 63.33% of the patients, particularly on the first postoperative day. Natriuresis was present in 93.33% of the patients, particularly on the second postoperative day. Plasma atrial natriuretic factor was increased in 92.60% of the patients in at least one of the postoperative days; however, there was no statistically significant association between the atrial natriuretic factor and plasma sodium and between the atrial natriuretic factor and urinary sodium.
Conclusion:
Hyponatremia and natriuresis were present in most patients after neurosurgery; however, the atrial natriuretic factor cannot be considered to be directly responsible for these alterations in neurosurgery patients. Other natriuretic factors are likely to be involved.
-
Original Article
Thrombin activatable fibrinolysis inhibitor as a bleeding predictor in liver transplantation: a pilot observational study
Rev Bras Ter Intensiva. 2016;28(2):161-166
Abstract
Original ArticleThrombin activatable fibrinolysis inhibitor as a bleeding predictor in liver transplantation: a pilot observational study
Rev Bras Ter Intensiva. 2016;28(2):161-166
DOI 10.5935/0103-507X.20160031
Views0See moreABSTRACT
Objective:
To correlate the levels of thrombin activatable fibrinolysis inhibitor in the immediate postoperative period and at 24 hours postoperatively with the volume of intraoperative bleeding.
Methods:
Twenty-one patients allocated immediately before (elective or emergency) liver transplantation were analyzed. Blood samples were collected for thrombin activatable fibrinolysis inhibitor analysis at three different time points: immediately before liver transplantation (preoperative thrombin activatable fibrinolysis inhibitor), immediately after the surgical procedure (immediate postoperative thrombin activatable fibrinolysis inhibitor), and 24 hours after surgery (thrombin activatable fibrinolysis inhibitor 24 hours after surgery). The primary outcome of the study was to correlate the preoperative and immediate postoperative levels of thrombin activatable fibrinolysis inhibitor with intraoperative blood loss.
Results:
There was a correlation between the preoperative thrombin activatable fibrinolysis inhibitor levels and bleeding volume (ρ = -0.469; p = 0.05) but no correlation between the immediate postoperative thrombin activatable fibrinolysis inhibitor and bleeding volume (ρ = -0.062; p = 0.79). No variable included in the linear regression analysis (prehemoglobin, prefibrinogen and preoperative thrombin activatable fibrinolysis inhibitor) was a bleeding predictor. There was a similar trend in the variation between the levels of thrombin activatable fibrinolysis inhibitor at the three different time points and fibrinogen levels. Patients who died within 6 months (14.3%) showed decreased preoperative and immediate postoperative levels of thrombin activatable fibrinolysis compared with survivors (preoperative: 1.3 ± 0.15 versus 2.55 ± 0.53, p = 0.06; immediate postoperative: 1.2 ± 0.15 versus 2.5 ± 0.42, p = 0.007).
Conclusion:
There was a moderate correlation between preoperative thrombin activatable fibrinolysis inhibitor and intraoperative bleeding in liver transplantation patients, although the predictive role of this variable independent of other variables remains uncertain. Preoperative and immediate postoperative thrombin activatable fibrinolysis inhibitor levels may have a role in the survival prognosis of this population; however, this possibility requires confirmation in further studies with larger sample sizes.
Views0Abstract
Original ArticleThrombin activatable fibrinolysis inhibitor as a bleeding predictor in liver transplantation: a pilot observational study
Rev Bras Ter Intensiva. 2016;28(2):161-166
DOI 10.5935/0103-507X.20160031
Views0See moreABSTRACT
Objective:
To correlate the levels of thrombin activatable fibrinolysis inhibitor in the immediate postoperative period and at 24 hours postoperatively with the volume of intraoperative bleeding.
Methods:
Twenty-one patients allocated immediately before (elective or emergency) liver transplantation were analyzed. Blood samples were collected for thrombin activatable fibrinolysis inhibitor analysis at three different time points: immediately before liver transplantation (preoperative thrombin activatable fibrinolysis inhibitor), immediately after the surgical procedure (immediate postoperative thrombin activatable fibrinolysis inhibitor), and 24 hours after surgery (thrombin activatable fibrinolysis inhibitor 24 hours after surgery). The primary outcome of the study was to correlate the preoperative and immediate postoperative levels of thrombin activatable fibrinolysis inhibitor with intraoperative blood loss.
Results:
There was a correlation between the preoperative thrombin activatable fibrinolysis inhibitor levels and bleeding volume (ρ = -0.469; p = 0.05) but no correlation between the immediate postoperative thrombin activatable fibrinolysis inhibitor and bleeding volume (ρ = -0.062; p = 0.79). No variable included in the linear regression analysis (prehemoglobin, prefibrinogen and preoperative thrombin activatable fibrinolysis inhibitor) was a bleeding predictor. There was a similar trend in the variation between the levels of thrombin activatable fibrinolysis inhibitor at the three different time points and fibrinogen levels. Patients who died within 6 months (14.3%) showed decreased preoperative and immediate postoperative levels of thrombin activatable fibrinolysis compared with survivors (preoperative: 1.3 ± 0.15 versus 2.55 ± 0.53, p = 0.06; immediate postoperative: 1.2 ± 0.15 versus 2.5 ± 0.42, p = 0.007).
Conclusion:
There was a moderate correlation between preoperative thrombin activatable fibrinolysis inhibitor and intraoperative bleeding in liver transplantation patients, although the predictive role of this variable independent of other variables remains uncertain. Preoperative and immediate postoperative thrombin activatable fibrinolysis inhibitor levels may have a role in the survival prognosis of this population; however, this possibility requires confirmation in further studies with larger sample sizes.
-
Review Article
Contemporary treatment of children with critical and near-fatal asthma
Rev Bras Ter Intensiva. 2016;28(2):167-178
Abstract
Review ArticleContemporary treatment of children with critical and near-fatal asthma
Rev Bras Ter Intensiva. 2016;28(2):167-178
DOI 10.5935/0103-507X.20160020
Views0See moreABSTRACT
Asthma is the most common chronic illness in childhood. Although the vast majority of children with acute asthma exacerbations do not require critical care, some fail to respond to standard treatment and require escalation of support. Children with critical or near-fatal asthma require close monitoring for deterioration and may require aggressive treatment strategies. This review examines the available evidence supporting therapies for critical and near-fatal asthma and summarizes the contemporary clinical care of these children. Typical treatment includes parenteral corticosteroids and inhaled or intravenous beta-agonist drugs. For children with an inadequate response to standard therapy, inhaled ipratropium bromide, intravenous magnesium sulfate, methylxanthines, helium-oxygen mixtures, and non-invasive mechanical support can be used. Patients with progressive respiratory failure benefit from mechanical ventilation with a strategy that employs large tidal volumes and low ventilator rates to minimize dynamic hyperinflation, barotrauma, and hypotension. Sedatives, analgesics and a neuromuscular blocker are often necessary in the early phase of treatment to facilitate a state of controlled hypoventilation and permissive hypercapnia. Patients who fail to improve with mechanical ventilation may be considered for less common approaches, such as inhaled anesthetics, bronchoscopy, and extracorporeal life support. This contemporary approach has resulted in extremely low mortality rates, even in children requiring mechanical support.
Views0Abstract
Review ArticleContemporary treatment of children with critical and near-fatal asthma
Rev Bras Ter Intensiva. 2016;28(2):167-178
DOI 10.5935/0103-507X.20160020
Views0See moreABSTRACT
Asthma is the most common chronic illness in childhood. Although the vast majority of children with acute asthma exacerbations do not require critical care, some fail to respond to standard treatment and require escalation of support. Children with critical or near-fatal asthma require close monitoring for deterioration and may require aggressive treatment strategies. This review examines the available evidence supporting therapies for critical and near-fatal asthma and summarizes the contemporary clinical care of these children. Typical treatment includes parenteral corticosteroids and inhaled or intravenous beta-agonist drugs. For children with an inadequate response to standard therapy, inhaled ipratropium bromide, intravenous magnesium sulfate, methylxanthines, helium-oxygen mixtures, and non-invasive mechanical support can be used. Patients with progressive respiratory failure benefit from mechanical ventilation with a strategy that employs large tidal volumes and low ventilator rates to minimize dynamic hyperinflation, barotrauma, and hypotension. Sedatives, analgesics and a neuromuscular blocker are often necessary in the early phase of treatment to facilitate a state of controlled hypoventilation and permissive hypercapnia. Patients who fail to improve with mechanical ventilation may be considered for less common approaches, such as inhaled anesthetics, bronchoscopy, and extracorporeal life support. This contemporary approach has resulted in extremely low mortality rates, even in children requiring mechanical support.
-
Review Article
Prognostic value of procalcitonin in hospitalized patients with lower respiratory tract infections
Rev Bras Ter Intensiva. 2016;28(2):179-189
Abstract
Review ArticlePrognostic value of procalcitonin in hospitalized patients with lower respiratory tract infections
Rev Bras Ter Intensiva. 2016;28(2):179-189
DOI 10.5935/0103-507X.20160019
Views0See moreABSTRACT
Lower respiratory tract infections are common and potentially lethal conditions and are a major cause of inadequate antibiotic prescriptions. Characterization of disease severity and prognostic prediction in affected patients can aid disease management and can increase accuracy in determining the need for and place of hospitalization. The inclusion of biomarkers, particularly procalcitonin, in the decision taken process is a promising strategy. This study aims to present a narrative review of the potential applications and limitations of procalcitonin as a prognostic marker in hospitalized patients with lower respiratory tract infections. The studies on this topic are heterogeneous with respect to procalcitonin measurement techniques, cutoff values, clinical settings, and disease severity. The results show that procalcitonin delivers moderate performance for prognostic prediction in patients with lower respiratory tract infections; its predictive performance was not higher than that of classical methods, and knowledge of procalcitonin levels is most useful when interpreted together with other clinical and laboratory results. Overall, repeated measurement of the procalcitonin levels during the first days of treatment provides more prognostic information than a single measurement; however, information on the cost-effectiveness of this procedure in intensive care patients is lacking. The results of studies that evaluated the prognostic value of initial procalcitonin levels in patients with community-acquired pneumonia are more consistent and have greater potential for practical application; in this case, low procalcitonin levels identify those patients with a low risk of adverse outcomes.
Views0Abstract
Review ArticlePrognostic value of procalcitonin in hospitalized patients with lower respiratory tract infections
Rev Bras Ter Intensiva. 2016;28(2):179-189
DOI 10.5935/0103-507X.20160019
Views0See moreABSTRACT
Lower respiratory tract infections are common and potentially lethal conditions and are a major cause of inadequate antibiotic prescriptions. Characterization of disease severity and prognostic prediction in affected patients can aid disease management and can increase accuracy in determining the need for and place of hospitalization. The inclusion of biomarkers, particularly procalcitonin, in the decision taken process is a promising strategy. This study aims to present a narrative review of the potential applications and limitations of procalcitonin as a prognostic marker in hospitalized patients with lower respiratory tract infections. The studies on this topic are heterogeneous with respect to procalcitonin measurement techniques, cutoff values, clinical settings, and disease severity. The results show that procalcitonin delivers moderate performance for prognostic prediction in patients with lower respiratory tract infections; its predictive performance was not higher than that of classical methods, and knowledge of procalcitonin levels is most useful when interpreted together with other clinical and laboratory results. Overall, repeated measurement of the procalcitonin levels during the first days of treatment provides more prognostic information than a single measurement; however, information on the cost-effectiveness of this procedure in intensive care patients is lacking. The results of studies that evaluated the prognostic value of initial procalcitonin levels in patients with community-acquired pneumonia are more consistent and have greater potential for practical application; in this case, low procalcitonin levels identify those patients with a low risk of adverse outcomes.
-
Case Report
Hantavirus cardiopulmonary syndrome successfully treated with high-volume hemofiltration
Rev Bras Ter Intensiva. 2016;28(2):190-194
Abstract
Case ReportHantavirus cardiopulmonary syndrome successfully treated with high-volume hemofiltration
Rev Bras Ter Intensiva. 2016;28(2):190-194
DOI 10.5935/0103-507X.20160032
Views0See moreABSTRACT
Hantavirus cardiopulmonary syndrome has a high mortality rate, and early connection to extracorporeal membrane oxygenation has been suggested to improve outcomes. We report the case of a patient with demonstrated Hantavirus cardiopulmonary syndrome and refractory shock who fulfilled the criteria for extracorporeal membrane oxygenation and responded successfully to high volume continuous hemofiltration. The implementation of high volume continuous hemofiltration along with protective ventilation reversed the shock within a few hours and may have prompted recovery. In patients with Hantavirus cardiopulmonary syndrome, a short course of high volume continuous hemofiltration may help differentiate patients who can be treated with conventional intensive care unit management from those who will require more complex therapies, such as extracorporeal membrane oxygenation.
Views0Abstract
Case ReportHantavirus cardiopulmonary syndrome successfully treated with high-volume hemofiltration
Rev Bras Ter Intensiva. 2016;28(2):190-194
DOI 10.5935/0103-507X.20160032
Views0See moreABSTRACT
Hantavirus cardiopulmonary syndrome has a high mortality rate, and early connection to extracorporeal membrane oxygenation has been suggested to improve outcomes. We report the case of a patient with demonstrated Hantavirus cardiopulmonary syndrome and refractory shock who fulfilled the criteria for extracorporeal membrane oxygenation and responded successfully to high volume continuous hemofiltration. The implementation of high volume continuous hemofiltration along with protective ventilation reversed the shock within a few hours and may have prompted recovery. In patients with Hantavirus cardiopulmonary syndrome, a short course of high volume continuous hemofiltration may help differentiate patients who can be treated with conventional intensive care unit management from those who will require more complex therapies, such as extracorporeal membrane oxygenation.
-
Case Report
Ralstonia pickettii bacteremia in hemodialysis patients: a report of two cases
Rev Bras Ter Intensiva. 2016;28(2):195-198
Abstract
Case ReportRalstonia pickettii bacteremia in hemodialysis patients: a report of two cases
Rev Bras Ter Intensiva. 2016;28(2):195-198
DOI 10.5935/0103-507X.20160033
Views0See moreABSTRACT
Ralstonia pickettii is a low-virulence gram-negative bacillus that may be associated with infections related to health care and may cause bacteremia. Ralstonia pickettii bacteremia is uncommon but is related to the contamination of medical products, mainly in immunodepressed patients. We present two cases of patients on chronic hemodialysis with Ralstonia pickettii bacteremia linked to contamination of the dialysis water. Similar cases have been published with links to intravenous fluid administration, medication ampules, and the use of extracorporeal oxygenation membranes, among other factors. The detection of Ralstonia pickettii bacteremia should provoke suspicion and a search for contaminated medical products, fluids, and/or medications.
Views0Abstract
Case ReportRalstonia pickettii bacteremia in hemodialysis patients: a report of two cases
Rev Bras Ter Intensiva. 2016;28(2):195-198
DOI 10.5935/0103-507X.20160033
Views0See moreABSTRACT
Ralstonia pickettii is a low-virulence gram-negative bacillus that may be associated with infections related to health care and may cause bacteremia. Ralstonia pickettii bacteremia is uncommon but is related to the contamination of medical products, mainly in immunodepressed patients. We present two cases of patients on chronic hemodialysis with Ralstonia pickettii bacteremia linked to contamination of the dialysis water. Similar cases have been published with links to intravenous fluid administration, medication ampules, and the use of extracorporeal oxygenation membranes, among other factors. The detection of Ralstonia pickettii bacteremia should provoke suspicion and a search for contaminated medical products, fluids, and/or medications.
-
Letters to the Editor
To: Severe hypercalcemia as a form of acute lymphoblastic leukemia presentation in children
Rev Bras Ter Intensiva. 2016;28(2):199-200
Abstract
Letters to the EditorTo: Severe hypercalcemia as a form of acute lymphoblastic leukemia presentation in children
Rev Bras Ter Intensiva. 2016;28(2):199-200
DOI 10.5935/0103-507X.20160034
Views1To the Editor, Severe hypercalcemia of malignancy in children has been extensively described in the medical literature.() However, this complication usually presents as a late symptom of acute lymphoblastic disease and not as an early manifestation, as described in a case report by Martins et al.() Colleti Junior et al.() also observed that hypercalcemia was […]See moreViews1Abstract
Letters to the EditorTo: Severe hypercalcemia as a form of acute lymphoblastic leukemia presentation in children
Rev Bras Ter Intensiva. 2016;28(2):199-200
DOI 10.5935/0103-507X.20160034
Views1To the Editor, Severe hypercalcemia of malignancy in children has been extensively described in the medical literature.() However, this complication usually presents as a late symptom of acute lymphoblastic disease and not as an early manifestation, as described in a case report by Martins et al.() Colleti Junior et al.() also observed that hypercalcemia was […]See more
-
Letters to the Editor
To: Measurement of intracranial pressure and short-term outcomes of patients with traumatic brain injury: a propensity-matched analysis
Rev Bras Ter Intensiva. 2016;28(2):203-204
Abstract
Letters to the EditorTo: Measurement of intracranial pressure and short-term outcomes of patients with traumatic brain injury: a propensity-matched analysis
Rev Bras Ter Intensiva. 2016;28(2):203-204
Views0Abstract
Letters to the EditorTo: Measurement of intracranial pressure and short-term outcomes of patients with traumatic brain injury: a propensity-matched analysis
Rev Bras Ter Intensiva. 2016;28(2):203-204
-
Letters to the Editor
To: Therapeutic hypothermia after cardiac arrest: outcome predictors
Rev Bras Ter Intensiva. 2016;28(2):207-208
Abstract
Letters to the EditorTo: Therapeutic hypothermia after cardiac arrest: outcome predictors
Rev Bras Ter Intensiva. 2016;28(2):207-208
DOI 10.5935/0103-507X.20160038
Views0To the Editor, Determining the neurological prognosis of patients who have suffered cardiac arrest is extremely important because it allows the physician to inform the family about the life expectancy of their beloved relative, as well as to wisely plan for the allocation of available resources. We read with great interest the study performed by […]See moreViews0Abstract
Letters to the EditorTo: Therapeutic hypothermia after cardiac arrest: outcome predictors
Rev Bras Ter Intensiva. 2016;28(2):207-208
DOI 10.5935/0103-507X.20160038
Views0To the Editor, Determining the neurological prognosis of patients who have suffered cardiac arrest is extremely important because it allows the physician to inform the family about the life expectancy of their beloved relative, as well as to wisely plan for the allocation of available resources. We read with great interest the study performed by […]See more
Volume Articles - Critical Care Science (CCS)
