-
Commentaries
Methods to safely implement hypothermia in the intensive care unit: a how-to guide
Rev Bras Ter Intensiva. 2016;28(1):1-4
Abstract
CommentariesMethods to safely implement hypothermia in the intensive care unit: a how-to guide
Rev Bras Ter Intensiva. 2016;28(1):1-4
DOI 10.5935/0103-507X.20160007
Views0TARGET TEMPERATURE MANAGEMENT IN 2016 Target temperature management (TTM) is well-known to reduce secondary cell damage after cardiac arrest in patients with presumed cerebral hypoxia. The treatment of this reperfusion syndrome, especially in terms of temperature management, is not fully understood. Several clinical randomized controlled trials and other studies have shown TTM’s effectiveness in improving […]See moreViews0

Abstract
CommentariesMethods to safely implement hypothermia in the intensive care unit: a how-to guide
Rev Bras Ter Intensiva. 2016;28(1):1-4
DOI 10.5935/0103-507X.20160007
Views0TARGET TEMPERATURE MANAGEMENT IN 2016Target temperature management (TTM) is well-known to reduce secondary cell damage after cardiac arrest in patients with presumed cerebral hypoxia. The treatment of this reperfusion syndrome, especially in terms of temperature management, is not fully understood. Several clinical randomized controlled trials and other studies have shown TTM’s effectiveness in improving neurological […]See more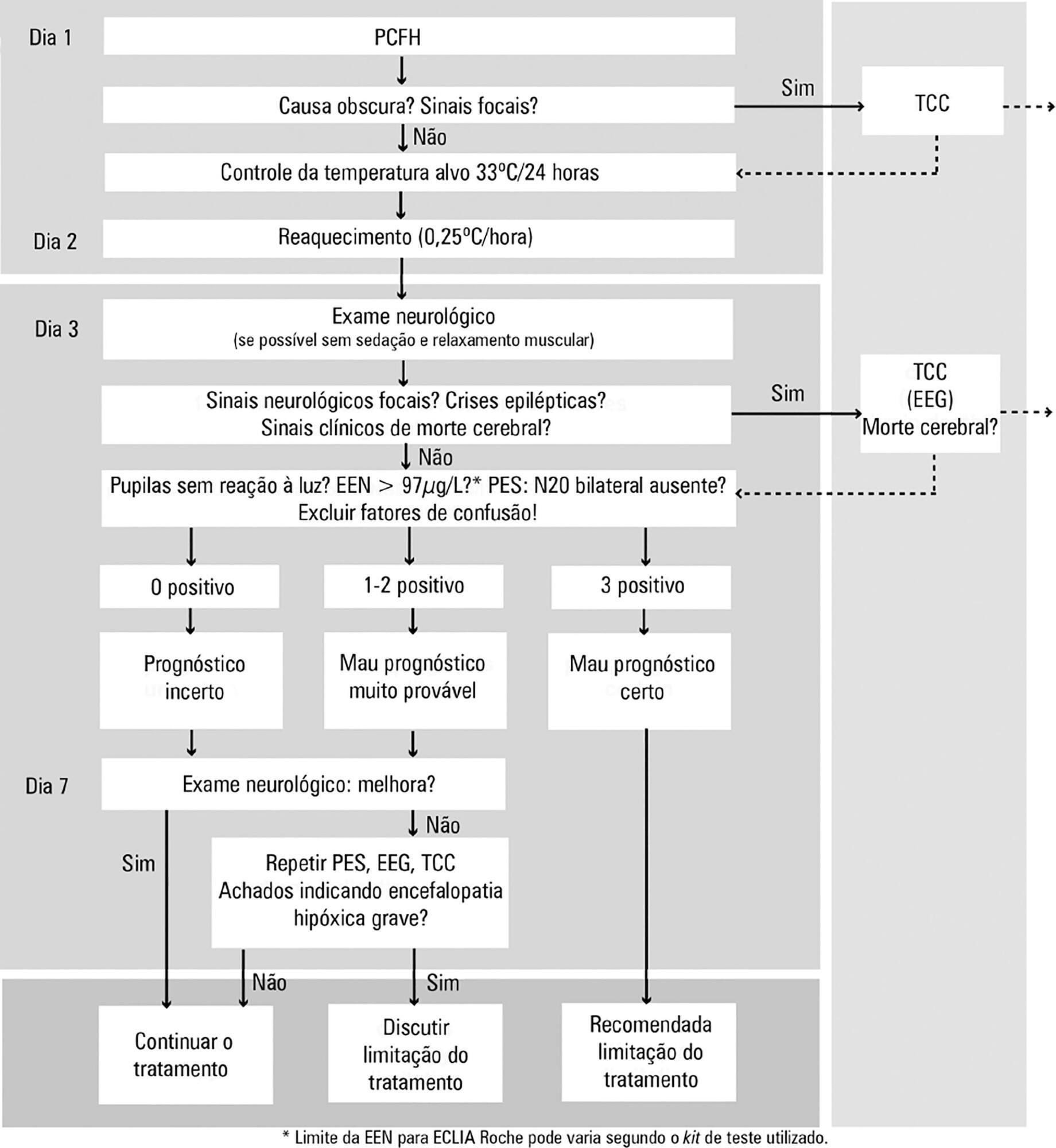
-
Commentaries
Lung ultrasound: a useful tool in the weaning process?
Rev Bras Ter Intensiva. 2016;28(1):5-7
Abstract
CommentariesLung ultrasound: a useful tool in the weaning process?
Rev Bras Ter Intensiva. 2016;28(1):5-7
DOI 10.5935/0103-507X.20160002
Views0INTRODUCTIONThe incidence of pulmonary complications related to mechanical ventilation is an important issue among critically ill patients. Reducing the duration of respiratory support is essential for minimizing these complications. The extubation of a patient marks the end of the weaning process. Unfortunately, even after a successful spontaneous breathing trial (SBT), approximately 30% of patients develop […]See moreViews0Abstract
CommentariesLung ultrasound: a useful tool in the weaning process?
Rev Bras Ter Intensiva. 2016;28(1):5-7
DOI 10.5935/0103-507X.20160002
Views0INTRODUCTIONThe incidence of pulmonary complications related to mechanical ventilation is an important issue among critically ill patients. Reducing the duration of respiratory support is essential for minimizing these complications. The extubation of a patient marks the end of the weaning process. Unfortunately, even after a successful spontaneous breathing trial (SBT), approximately 30% of patients develop […]See more
-
Commentaries
Big data in healthcare: are we close to it?
Rev Bras Ter Intensiva. 2016;28(1):08-10
Abstract
CommentariesBig data in healthcare: are we close to it?
Rev Bras Ter Intensiva. 2016;28(1):08-10
DOI 10.5935/0103-507X.20160008
Views0INTRODUCTIONTranslating medical research into clinical practice guidelines is not trivial. There has been a surge in the number of published biomedical articles,() but how clinicians adapt these articles into practice is not straightforward. In addition, the validity of biomedical research has recently been under scrutiny.() Bias in publication with emphasis on sensational discoveries over reproducibility, […]See moreViews0Abstract
CommentariesBig data in healthcare: are we close to it?
Rev Bras Ter Intensiva. 2016;28(1):08-10
DOI 10.5935/0103-507X.20160008
Views0INTRODUCTIONTranslating medical research into clinical practice guidelines is not trivial. There has been a surge in the number of published biomedical articles,() but how clinicians adapt these articles into practice is not straightforward. In addition, the validity of biomedical research has recently been under scrutiny.() Bias in publication with emphasis on sensational discoveries over reproducibility, […]See more -
Factors associated with blood oxygen partial pressure and carbon dioxide partial pressure regulation during respiratory extracorporeal membrane oxygenation support: data from a swine model
Rev Bras Ter Intensiva. 2016;28(1):11-18
Abstract
Factors associated with blood oxygen partial pressure and carbon dioxide partial pressure regulation during respiratory extracorporeal membrane oxygenation support: data from a swine model
Rev Bras Ter Intensiva. 2016;28(1):11-18
DOI 10.5935/0103-507X.20160006
Views0ABSTRACT
Objective:
The aim of this study was to explore the factors associated with blood oxygen partial pressure and carbon dioxide partial pressure.
Methods:
The factors associated with oxygen – and carbon dioxide regulation were investigated in an apneic pig model under veno-venous extracorporeal membrane oxygenation support. A predefined sequence of blood and sweep flows was tested.
Results:
Oxygenation was mainly associated with extracorporeal membrane oxygenation blood flow (beta coefficient = 0.036mmHg/mL/min), cardiac output (beta coefficient = -11.970mmHg/L/min) and pulmonary shunting (beta coefficient = -0.232mmHg/%). Furthermore, the initial oxygen partial pressure and carbon dioxide partial pressure measurements were also associated with oxygenation, with beta coefficients of 0.160 and 0.442mmHg/mmHg, respectively. Carbon dioxide partial pressure was associated with cardiac output (beta coefficient = 3.578mmHg/L/min), sweep gas flow (beta coefficient = -2.635mmHg/L/min), temperature (beta coefficient = 4.514mmHg/ºC), initial pH (beta coefficient = -66.065mmHg/0.01 unit) and hemoglobin (beta coefficient = 6.635mmHg/g/dL).
Conclusion:
In conclusion, elevations in blood and sweep gas flows in an apneic veno-venous extracorporeal membrane oxygenation model resulted in an increase in oxygen partial pressure and a reduction in carbon dioxide partial pressure 2, respectively. Furthermore, without the possibility of causal inference, oxygen partial pressure was negatively associated with pulmonary shunting and cardiac output, and carbon dioxide partial pressure was positively associated with cardiac output, core temperature and initial hemoglobin.
Keywords:Extracorporeal membrane oxygenationRespiration, artificialRespiratory distress syndrome, adultSwineSee moreViews0Abstract
Factors associated with blood oxygen partial pressure and carbon dioxide partial pressure regulation during respiratory extracorporeal membrane oxygenation support: data from a swine model
Rev Bras Ter Intensiva. 2016;28(1):11-18
DOI 10.5935/0103-507X.20160006
Views0ABSTRACT
Objective:
The aim of this study was to explore the factors associated with blood oxygen partial pressure and carbon dioxide partial pressure.
Methods:
The factors associated with oxygen – and carbon dioxide regulation were investigated in an apneic pig model under veno-venous extracorporeal membrane oxygenation support. A predefined sequence of blood and sweep flows was tested.
Results:
Oxygenation was mainly associated with extracorporeal membrane oxygenation blood flow (beta coefficient = 0.036mmHg/mL/min), cardiac output (beta coefficient = -11.970mmHg/L/min) and pulmonary shunting (beta coefficient = -0.232mmHg/%). Furthermore, the initial oxygen partial pressure and carbon dioxide partial pressure measurements were also associated with oxygenation, with beta coefficients of 0.160 and 0.442mmHg/mmHg, respectively. Carbon dioxide partial pressure was associated with cardiac output (beta coefficient = 3.578mmHg/L/min), sweep gas flow (beta coefficient = -2.635mmHg/L/min), temperature (beta coefficient = 4.514mmHg/ºC), initial pH (beta coefficient = -66.065mmHg/0.01 unit) and hemoglobin (beta coefficient = 6.635mmHg/g/dL).
Conclusion:
In conclusion, elevations in blood and sweep gas flows in an apneic veno-venous extracorporeal membrane oxygenation model resulted in an increase in oxygen partial pressure and a reduction in carbon dioxide partial pressure 2, respectively. Furthermore, without the possibility of causal inference, oxygen partial pressure was negatively associated with pulmonary shunting and cardiac output, and carbon dioxide partial pressure was positively associated with cardiac output, core temperature and initial hemoglobin.
Keywords:Extracorporeal membrane oxygenationRespiration, artificialRespiratory distress syndrome, adultSwineSee more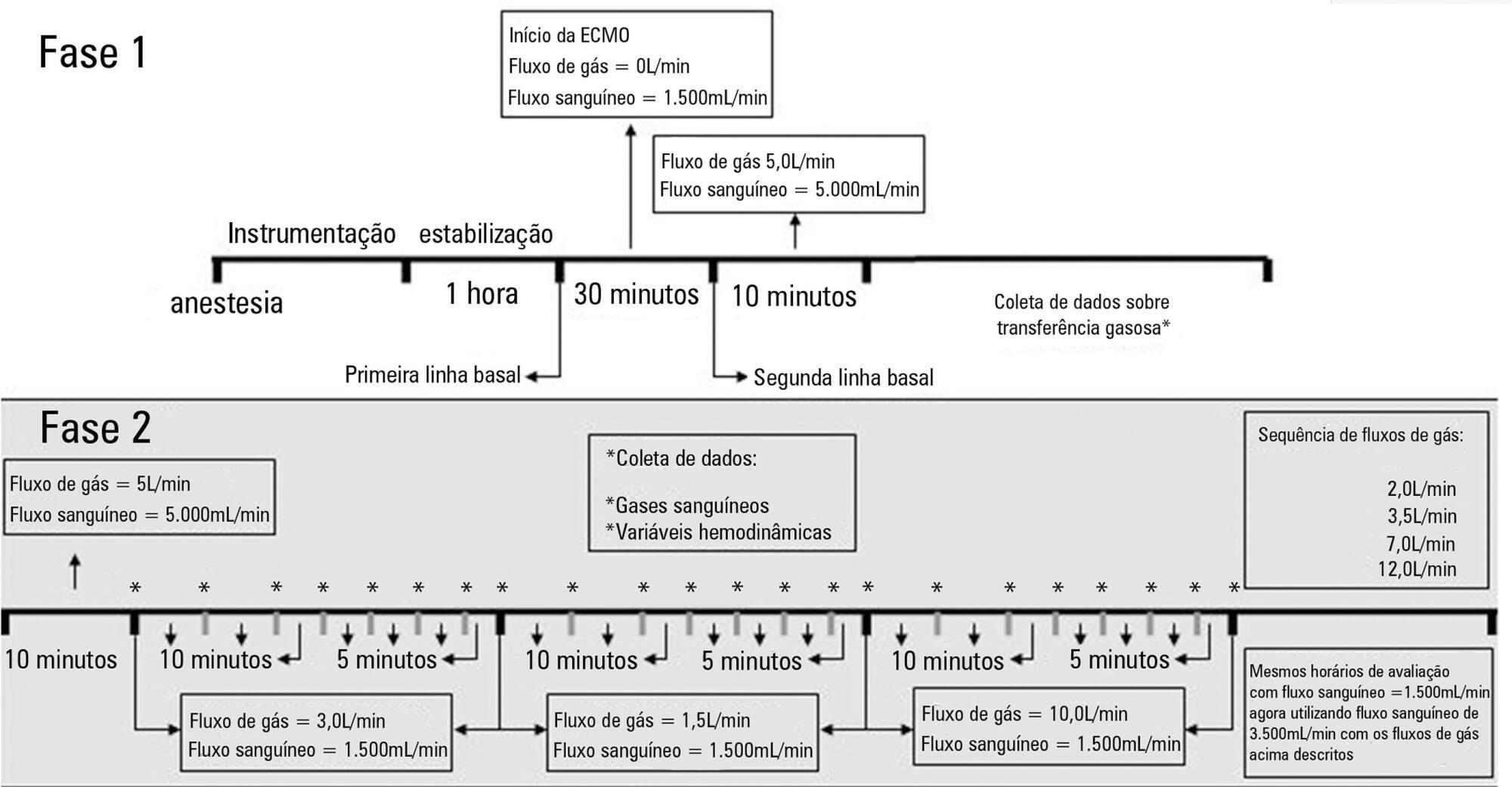
-
Original Article
Metabolic acid-base adaptation triggered by acute persistent hypercapnia in mechanically ventilated patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(1):19-26
Abstract
Original ArticleMetabolic acid-base adaptation triggered by acute persistent hypercapnia in mechanically ventilated patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(1):19-26
DOI 10.5935/0103-507X.20160009
Views0ABSTRACT
Objective:
Hypercapnia resulting from protective ventilation in acute respiratory distress syndrome triggers metabolic pH compensation, which is not entirely characterized. We aimed to describe this metabolic compensation.
Methods:
The data were retrieved from a prospective collected database. Variables from patients’ admission and from hypercapnia installation until the third day after installation were gathered. Forty-one patients with acute respiratory distress syndrome were analyzed, including twenty-six with persistent hypercapnia (PaCO2 > 50mmHg > 24 hours) and 15 non-hypercapnic (control group). An acid-base quantitative physicochemical approach was used for the analysis.
Results:
The mean ages in the hypercapnic and control groups were 48 ± 18 years and 44 ± 14 years, respectively. After the induction of hypercapnia, pH markedly decreased and gradually improved in the ensuing 72 hours, consistent with increases in the standard base excess. The metabolic acid-base adaptation occurred because of decreases in the serum lactate and strong ion gap and increases in the inorganic apparent strong ion difference. Furthermore, the elevation in the inorganic apparent strong ion difference occurred due to slight increases in serum sodium, magnesium, potassium and calcium. Serum chloride did not decrease for up to 72 hours after the initiation of hypercapnia.
Conclusion:
In this explanatory study, the results indicate that metabolic acid-base adaptation, which is triggered by acute persistent hypercapnia in patients with acute respiratory distress syndrome, is complex. Furthermore, further rapid increases in the standard base excess of hypercapnic patients involve decreases in serum lactate and unmeasured anions and increases in the inorganic apparent strong ion difference by means of slight increases in serum sodium, magnesium, calcium, and potassium. Serum chloride is not reduced.
Keywords:Acid-base equilibriumAcidosis, respiratoryIntensive care unitsRespiration, artificialRespiratory distress syndrome, adultSee moreViews0Abstract
Original ArticleMetabolic acid-base adaptation triggered by acute persistent hypercapnia in mechanically ventilated patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(1):19-26
DOI 10.5935/0103-507X.20160009
Views0ABSTRACT
Objective:
Hypercapnia resulting from protective ventilation in acute respiratory distress syndrome triggers metabolic pH compensation, which is not entirely characterized. We aimed to describe this metabolic compensation.
Methods:
The data were retrieved from a prospective collected database. Variables from patients’ admission and from hypercapnia installation until the third day after installation were gathered. Forty-one patients with acute respiratory distress syndrome were analyzed, including twenty-six with persistent hypercapnia (PaCO2 > 50mmHg > 24 hours) and 15 non-hypercapnic (control group). An acid-base quantitative physicochemical approach was used for the analysis.
Results:
The mean ages in the hypercapnic and control groups were 48 ± 18 years and 44 ± 14 years, respectively. After the induction of hypercapnia, pH markedly decreased and gradually improved in the ensuing 72 hours, consistent with increases in the standard base excess. The metabolic acid-base adaptation occurred because of decreases in the serum lactate and strong ion gap and increases in the inorganic apparent strong ion difference. Furthermore, the elevation in the inorganic apparent strong ion difference occurred due to slight increases in serum sodium, magnesium, potassium and calcium. Serum chloride did not decrease for up to 72 hours after the initiation of hypercapnia.
Conclusion:
In this explanatory study, the results indicate that metabolic acid-base adaptation, which is triggered by acute persistent hypercapnia in patients with acute respiratory distress syndrome, is complex. Furthermore, further rapid increases in the standard base excess of hypercapnic patients involve decreases in serum lactate and unmeasured anions and increases in the inorganic apparent strong ion difference by means of slight increases in serum sodium, magnesium, calcium, and potassium. Serum chloride is not reduced.
Keywords:Acid-base equilibriumAcidosis, respiratoryIntensive care unitsRespiration, artificialRespiratory distress syndrome, adultSee more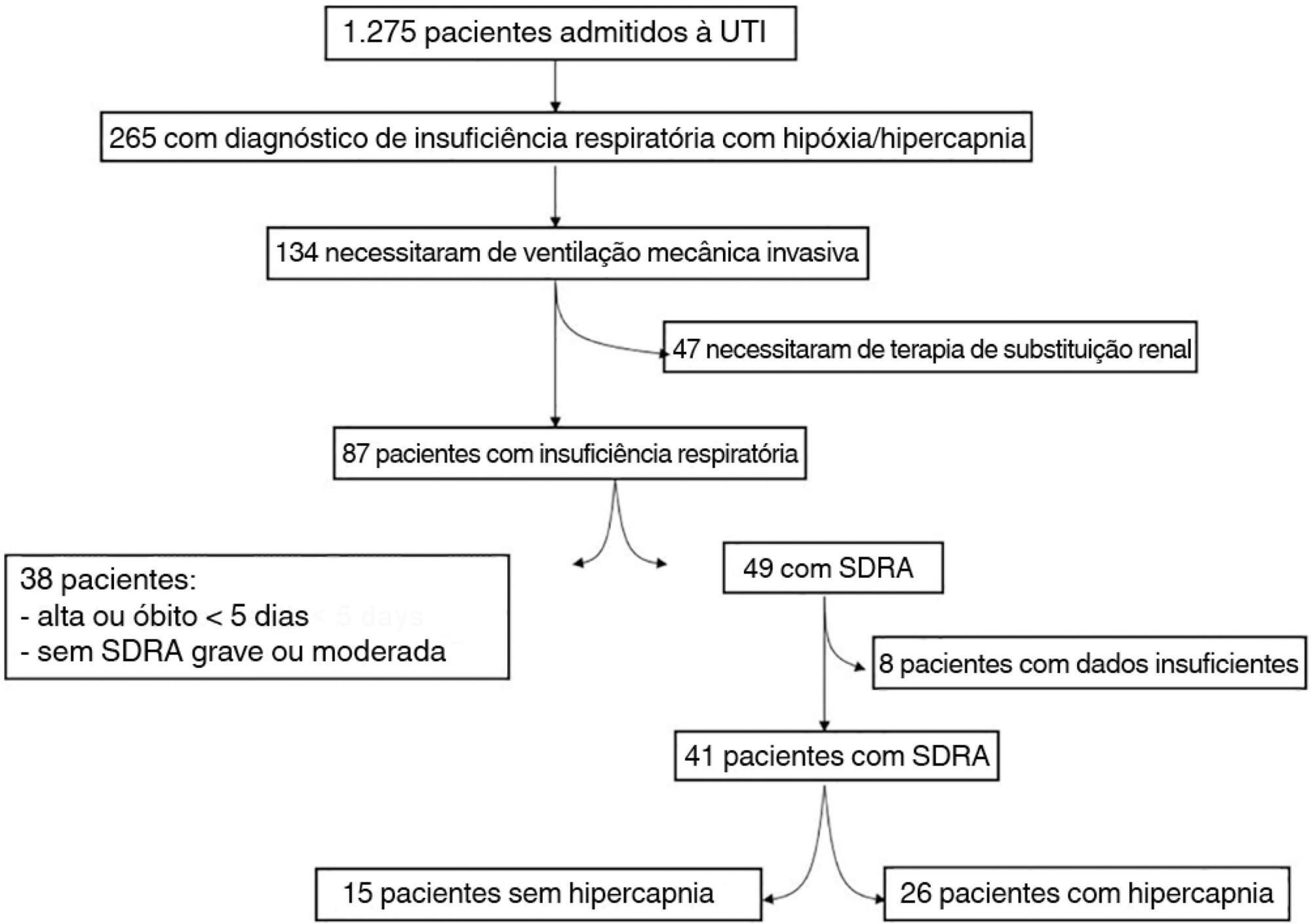
-
Original Article
Lung hyperinflation by mechanical ventilation versus isolated tracheal aspiration in the bronchial hygiene of patients undergoing mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(1):27-32
Abstract
Original ArticleLung hyperinflation by mechanical ventilation versus isolated tracheal aspiration in the bronchial hygiene of patients undergoing mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(1):27-32
DOI 10.5935/0103-507X.20160010
Views0See moreABSTRACT
Objective:
To determine the efficacy of lung hyperinflation maneuvers via a mechanical ventilator compared to isolated tracheal aspiration for removing secretions, normalizing hemodynamics and improving lung mechanics in patients on mechanical ventilation.
Methods:
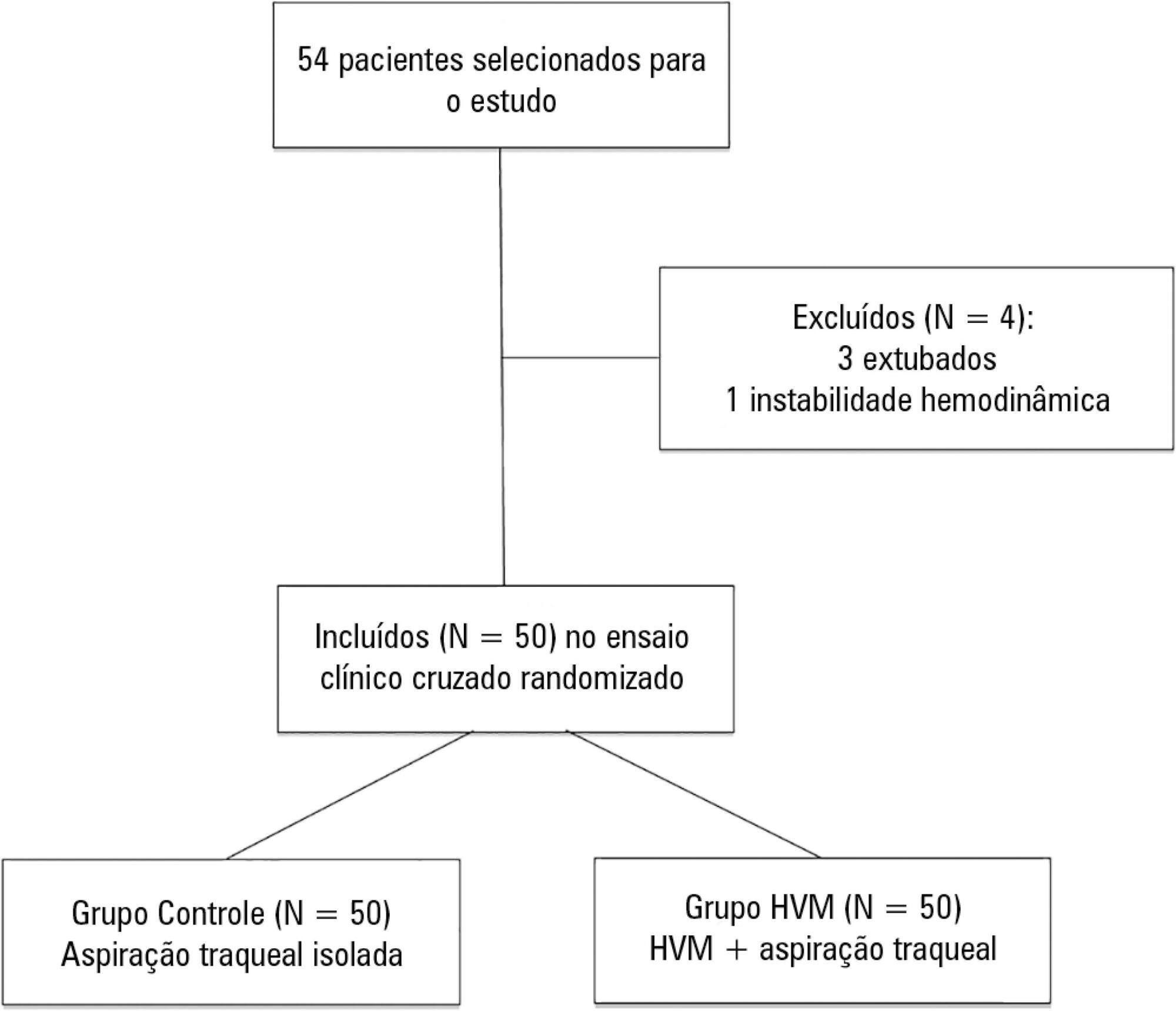
This was a randomized crossover clinical trial including patients admitted to the intensive care unit and on mechanical ventilation for more than 48 hours. Patients were randomized to receive either isolated tracheal aspiration (Control Group) or lung hyperinflation by mechanical ventilator (MVH Group). Hemodynamic and mechanical respiratory parameters were measured along with the amount of aspirated secretions.
Results:
A total of 50 patients were included. The mean age of the patients was 44.7 ± 21.6 years, and 31 were male. Compared to the Control Group, the MVH Group showed greater aspirated secretion amount (3.9g versus 6.4g, p = 0.0001), variation in mean dynamic compliance (-1.3 ± 2.3 versus -2.9 ± 2.3; p = 0.008), and expired tidal volume (-0.7 ± 0.0 versus -54.1 ± 38.8, p = 0.0001) as well as a significant decrease in peak inspiratory pressure (0.2 ± 0.1 versus 2.5 ± 0.1; p = 0.001).
Conclusion:
In the studied sample, the MVH technique led to a greater amount of aspirated secretions, significant increases in dynamic compliance and expired tidal volume and a significant reduction in peak inspiratory pressure.
Views0Abstract
Original ArticleLung hyperinflation by mechanical ventilation versus isolated tracheal aspiration in the bronchial hygiene of patients undergoing mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(1):27-32
DOI 10.5935/0103-507X.20160010
Views0See moreABSTRACT
Objective:
To determine the efficacy of lung hyperinflation maneuvers via a mechanical ventilator compared to isolated tracheal aspiration for removing secretions, normalizing hemodynamics and improving lung mechanics in patients on mechanical ventilation.
Methods:
This was a randomized crossover clinical trial including patients admitted to the intensive care unit and on mechanical ventilation for more than 48 hours. Patients were randomized to receive either isolated tracheal aspiration (Control Group) or lung hyperinflation by mechanical ventilator (MVH Group). Hemodynamic and mechanical respiratory parameters were measured along with the amount of aspirated secretions.
Results:
A total of 50 patients were included. The mean age of the patients was 44.7 ± 21.6 years, and 31 were male. Compared to the Control Group, the MVH Group showed greater aspirated secretion amount (3.9g versus 6.4g, p = 0.0001), variation in mean dynamic compliance (-1.3 ± 2.3 versus -2.9 ± 2.3; p = 0.008), and expired tidal volume (-0.7 ± 0.0 versus -54.1 ± 38.8, p = 0.0001) as well as a significant decrease in peak inspiratory pressure (0.2 ± 0.1 versus 2.5 ± 0.1; p = 0.001).
Conclusion:
In the studied sample, the MVH technique led to a greater amount of aspirated secretions, significant increases in dynamic compliance and expired tidal volume and a significant reduction in peak inspiratory pressure.
-
Original Article
Admission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(1):33-39
Abstract
Original ArticleAdmission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(1):33-39
DOI 10.5935/0103-507X.20160011
Views0See moreABSTRACT
Objective:
The purpose of our study was to determine the admission factors associated with intensive care unit readmission among oncohematological patients.
Methods:
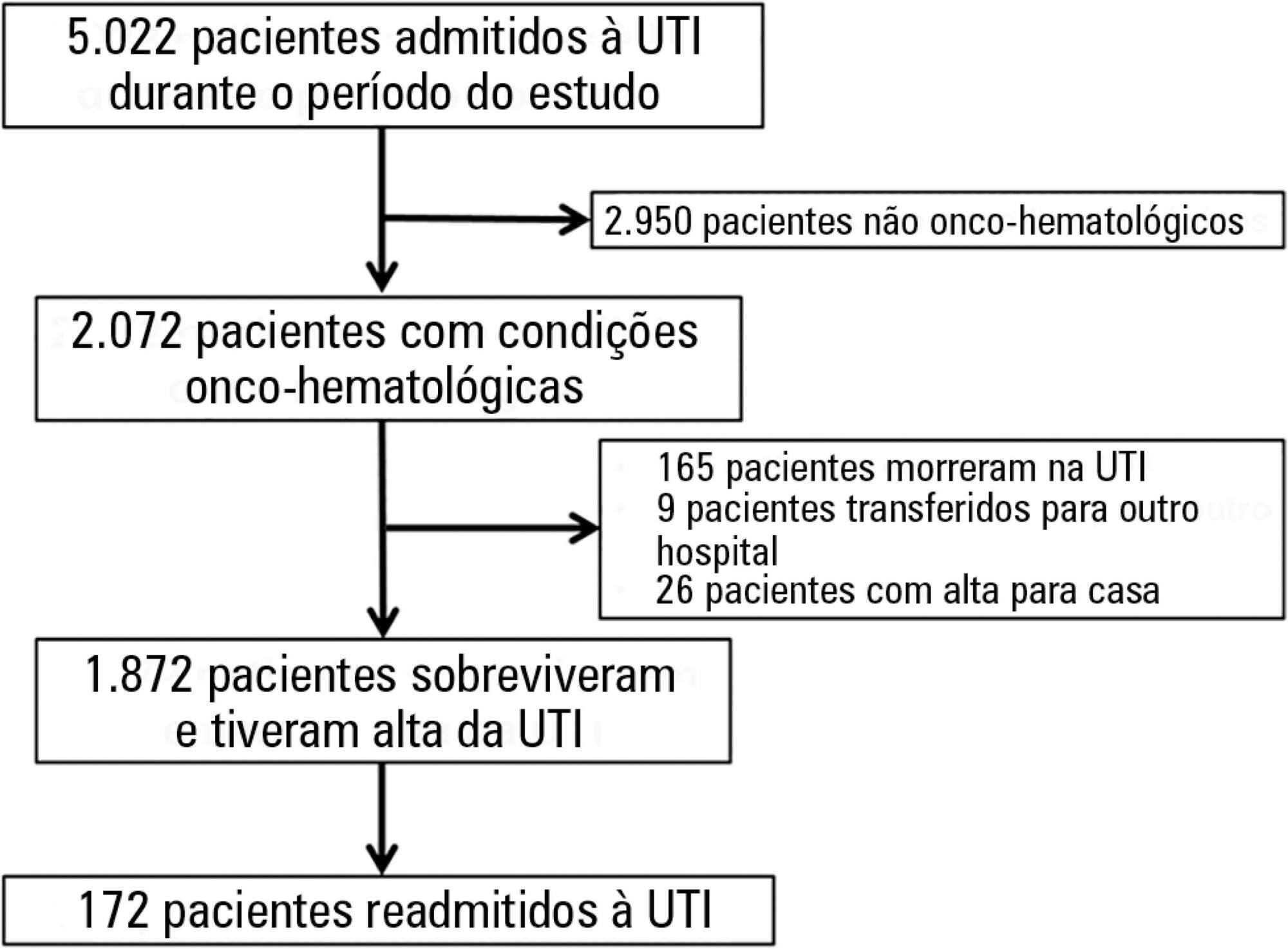
Retrospective cohort study using an intensive care unit database from a tertiary oncological center. The participants included 1,872 critically ill oncohematological patients who were admitted to the intensive care unit from January 2012 to December 2014 and who were subsequently discharged alive. We used univariate and multivariate analysis to identify the admission risk factors associated with later intensive care unit readmission.
Results:
One hundred seventy-two patients (9.2% of 1,872 oncohematological patients discharged alive from the intensive care unit) were readmitted after intensive care unit discharge. The readmitted patients were sicker compared with the non-readmitted group and had higher hospital mortality (32.6% versus 3.7%, respectively; p < 0.001). In the multivariate analysis, the independent risk factors for intensive care unit readmission were male sex (OR: 1.5, 95% CI: 1.07 - 2.12; p = 0.019), emergency surgery as the admission reason (OR: 2.91, 95%CI: 1.53 - 5.54; p = 0.001), longer hospital length of stay before intensive care unit transfer (OR: 1.02, 95%CI: 1.007 - 1.035; p = 0.003), and mechanical ventilation (OR: 2.31, 95%CI: 1.57 - 3.40; p < 0.001).
Conclusions:
In this cohort of oncohematological patients, we identified some risk factors associated with intensive care unit readmission, most of which are not amenable to interventions. The identification of risk factors at intensive care unit discharge might be a promising approach.
Views0Abstract
Original ArticleAdmission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2016;28(1):33-39
DOI 10.5935/0103-507X.20160011
Views0See moreABSTRACT
Objective:
The purpose of our study was to determine the admission factors associated with intensive care unit readmission among oncohematological patients.
Methods:
Retrospective cohort study using an intensive care unit database from a tertiary oncological center. The participants included 1,872 critically ill oncohematological patients who were admitted to the intensive care unit from January 2012 to December 2014 and who were subsequently discharged alive. We used univariate and multivariate analysis to identify the admission risk factors associated with later intensive care unit readmission.
Results:
One hundred seventy-two patients (9.2% of 1,872 oncohematological patients discharged alive from the intensive care unit) were readmitted after intensive care unit discharge. The readmitted patients were sicker compared with the non-readmitted group and had higher hospital mortality (32.6% versus 3.7%, respectively; p < 0.001). In the multivariate analysis, the independent risk factors for intensive care unit readmission were male sex (OR: 1.5, 95% CI: 1.07 - 2.12; p = 0.019), emergency surgery as the admission reason (OR: 2.91, 95%CI: 1.53 - 5.54; p = 0.001), longer hospital length of stay before intensive care unit transfer (OR: 1.02, 95%CI: 1.007 - 1.035; p = 0.003), and mechanical ventilation (OR: 2.31, 95%CI: 1.57 - 3.40; p < 0.001).
Conclusions:
In this cohort of oncohematological patients, we identified some risk factors associated with intensive care unit readmission, most of which are not amenable to interventions. The identification of risk factors at intensive care unit discharge might be a promising approach.
-
Original Article
Postoperative complications and clinical outcomes among patients undergoing thoracic and gastrointestinal cancer surgery: A prospective cohort study
Rev Bras Ter Intensiva. 2016;28(1):40-48
Abstract
Original ArticlePostoperative complications and clinical outcomes among patients undergoing thoracic and gastrointestinal cancer surgery: A prospective cohort study
Rev Bras Ter Intensiva. 2016;28(1):40-48
DOI 10.5935/0103-507X.20160012
Views0ABSTRACT
Objective:
This study sought to determine the influence of postoperative complications on the clinical outcomes of patients who underwent thoracic and gastrointestinal cancer surgery.
Methods:
A prospective cohort study was conducted regarding 179 consecutive patients who received thorax or digestive tract surgery due to cancer and were admitted to an oncological intensive care unit. The Postoperative Morbidity Survey was used to evaluate the incidence of postoperative complications. The influence of postoperative complications on both mortality and length of hospital stay were also assessed.
Results:
Postoperative complications were found for 54 patients (30.2%); the most common complications were respiratory problems (14.5%), pain (12.9%), cardiovascular problems (11.7%), infectious disease (11.2%), and surgical wounds (10.1%). A multivariate logistic regression found that respiratory complications (OR = 18.68; 95%CI = 5.59 – 62.39; p < 0.0001), cardiovascular problems (OR = 5.06, 95%CI = 1.49 - 17.13; p = 0.009), gastrointestinal problems (OR = 26.09; 95%CI = 6.80 - 100.16; p < 0.0001), infectious diseases (OR = 20.55; 95%CI = 5.99 - 70.56; p < 0.0001) and renal complications (OR = 18.27; 95%CI = 3.88 - 83.35; p < 0.0001) were independently associated with hospital mortality. The occurrence of at least one complication increased the likelihood of remaining hospitalized (log-rank test, p = 0.002).
Conclusions:
Postoperative complications are frequent disorders that are associated with poor clinical outcomes; thus, structural and procedural changes should be implemented to reduce postoperative morbidity and mortality.
Keywords:Gastrointestinal neoplasms/complicationsGastrointestinal neoplasms/surgeryHospital mortalityLength of hospital stayPostoperative complicationThoracic neoplasms/complicationsThoracic neoplasms/surgeryTreatment outcomeSee moreViews0Abstract
Original ArticlePostoperative complications and clinical outcomes among patients undergoing thoracic and gastrointestinal cancer surgery: A prospective cohort study
Rev Bras Ter Intensiva. 2016;28(1):40-48
DOI 10.5935/0103-507X.20160012
Views0ABSTRACT
Objective:
This study sought to determine the influence of postoperative complications on the clinical outcomes of patients who underwent thoracic and gastrointestinal cancer surgery.
Methods:
A prospective cohort study was conducted regarding 179 consecutive patients who received thorax or digestive tract surgery due to cancer and were admitted to an oncological intensive care unit. The Postoperative Morbidity Survey was used to evaluate the incidence of postoperative complications. The influence of postoperative complications on both mortality and length of hospital stay were also assessed.
Results:
Postoperative complications were found for 54 patients (30.2%); the most common complications were respiratory problems (14.5%), pain (12.9%), cardiovascular problems (11.7%), infectious disease (11.2%), and surgical wounds (10.1%). A multivariate logistic regression found that respiratory complications (OR = 18.68; 95%CI = 5.59 – 62.39; p < 0.0001), cardiovascular problems (OR = 5.06, 95%CI = 1.49 - 17.13; p = 0.009), gastrointestinal problems (OR = 26.09; 95%CI = 6.80 - 100.16; p < 0.0001), infectious diseases (OR = 20.55; 95%CI = 5.99 - 70.56; p < 0.0001) and renal complications (OR = 18.27; 95%CI = 3.88 - 83.35; p < 0.0001) were independently associated with hospital mortality. The occurrence of at least one complication increased the likelihood of remaining hospitalized (log-rank test, p = 0.002).
Conclusions:
Postoperative complications are frequent disorders that are associated with poor clinical outcomes; thus, structural and procedural changes should be implemented to reduce postoperative morbidity and mortality.
Keywords:Gastrointestinal neoplasms/complicationsGastrointestinal neoplasms/surgeryHospital mortalityLength of hospital stayPostoperative complicationThoracic neoplasms/complicationsThoracic neoplasms/surgeryTreatment outcomeSee more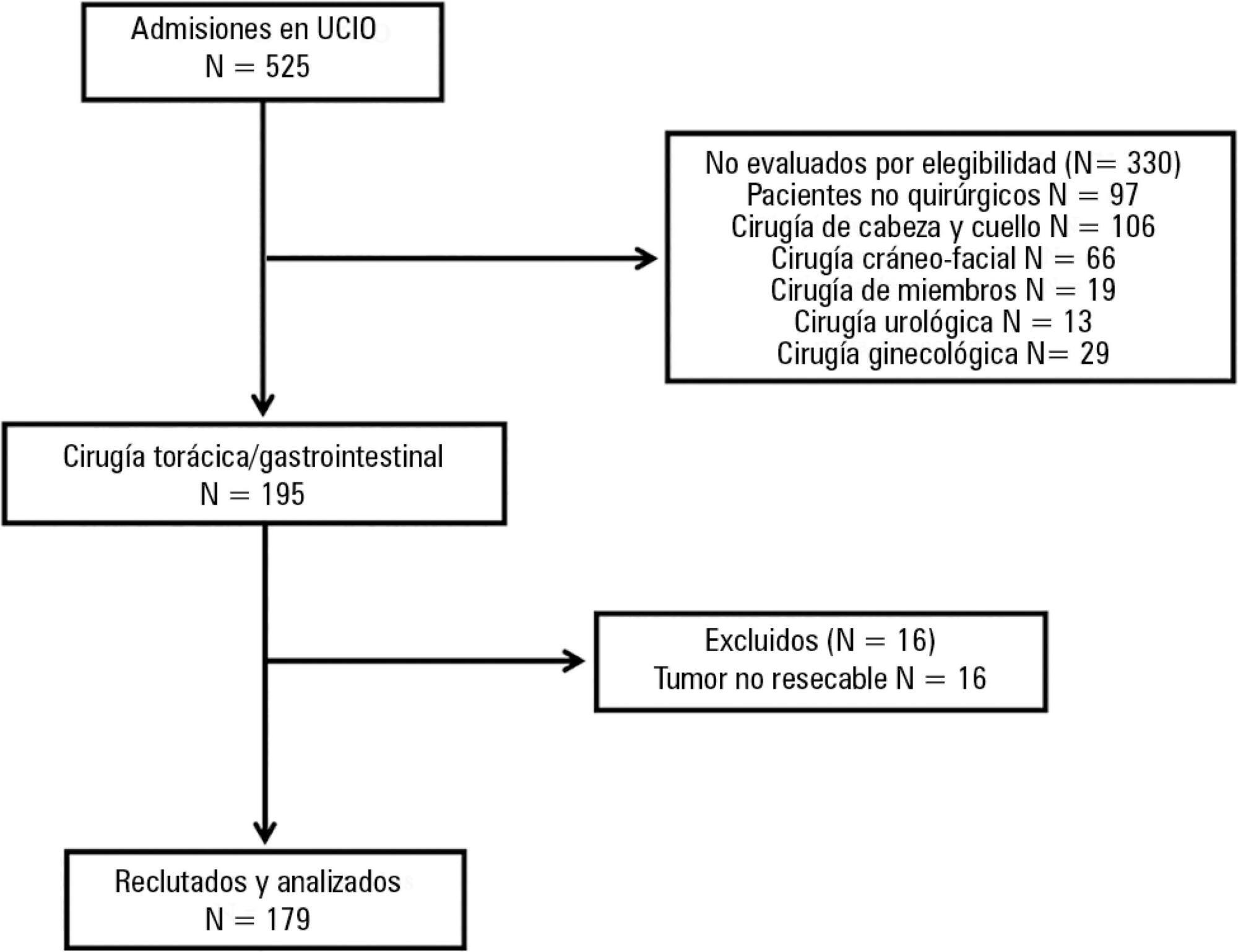
-
Original Articles
Pain assessment during blood collection from sedated and mechanically ventilated children
Rev Bras Ter Intensiva. 2016;28(1):49-54
Abstract
Original ArticlesPain assessment during blood collection from sedated and mechanically ventilated children
Rev Bras Ter Intensiva. 2016;28(1):49-54
DOI 10.5935/0103-507X.20160013
Views0ABSTRACT
Objective:
This study assessed pain and observed physiological parameters in sedated and mechanically ventilated children during a routine procedure.
Methods:
This observational study was performed in a pediatric intensive care unit. Thirty-five children between 1 month and 12 years of age were assessed before, during, and five minutes after an arterial blood collection for gas analysis (painful procedure). Face, Legs, Activity, Cry and Consolability scale was used to assess pain. In addition, patients’ heart rate, respiratory rate, peripheral saturation of oxygen and blood pressure (diastolic and systolic) were recorded. COMFORT-B scale was applied before the pain and physiological parameter assessments to verify sedation level of the subjects.
Results:
There was an increase in Face, Legs, Activity, Cry and Consolability score (p = 0.0001) during painful stimuli. There was an increase in heart rate (p = 0.03), respiratory rate (p = 0.001) and diastolic blood pressure (p = 0.006) due to pain caused by the routine procedure.
Conclusions:
This study suggests that assessments of pain using standard scales, such as Face, Legs, Activity, Cry and Consolability score, and other physiological parameters should be consistently executed to optimize pain management in pediatric intensive care units.
Keywords:ChildChild, preschoolIntensive care units, pediatricPain measurementRespiration, artificialSee moreViews0Abstract
Original ArticlesPain assessment during blood collection from sedated and mechanically ventilated children
Rev Bras Ter Intensiva. 2016;28(1):49-54
DOI 10.5935/0103-507X.20160013
Views0ABSTRACT
Objective:
This study assessed pain and observed physiological parameters in sedated and mechanically ventilated children during a routine procedure.
Methods:
This observational study was performed in a pediatric intensive care unit. Thirty-five children between 1 month and 12 years of age were assessed before, during, and five minutes after an arterial blood collection for gas analysis (painful procedure). Face, Legs, Activity, Cry and Consolability scale was used to assess pain. In addition, patients’ heart rate, respiratory rate, peripheral saturation of oxygen and blood pressure (diastolic and systolic) were recorded. COMFORT-B scale was applied before the pain and physiological parameter assessments to verify sedation level of the subjects.
Results:
There was an increase in Face, Legs, Activity, Cry and Consolability score (p = 0.0001) during painful stimuli. There was an increase in heart rate (p = 0.03), respiratory rate (p = 0.001) and diastolic blood pressure (p = 0.006) due to pain caused by the routine procedure.
Conclusions:
This study suggests that assessments of pain using standard scales, such as Face, Legs, Activity, Cry and Consolability score, and other physiological parameters should be consistently executed to optimize pain management in pediatric intensive care units.
Keywords:ChildChild, preschoolIntensive care units, pediatricPain measurementRespiration, artificialSee more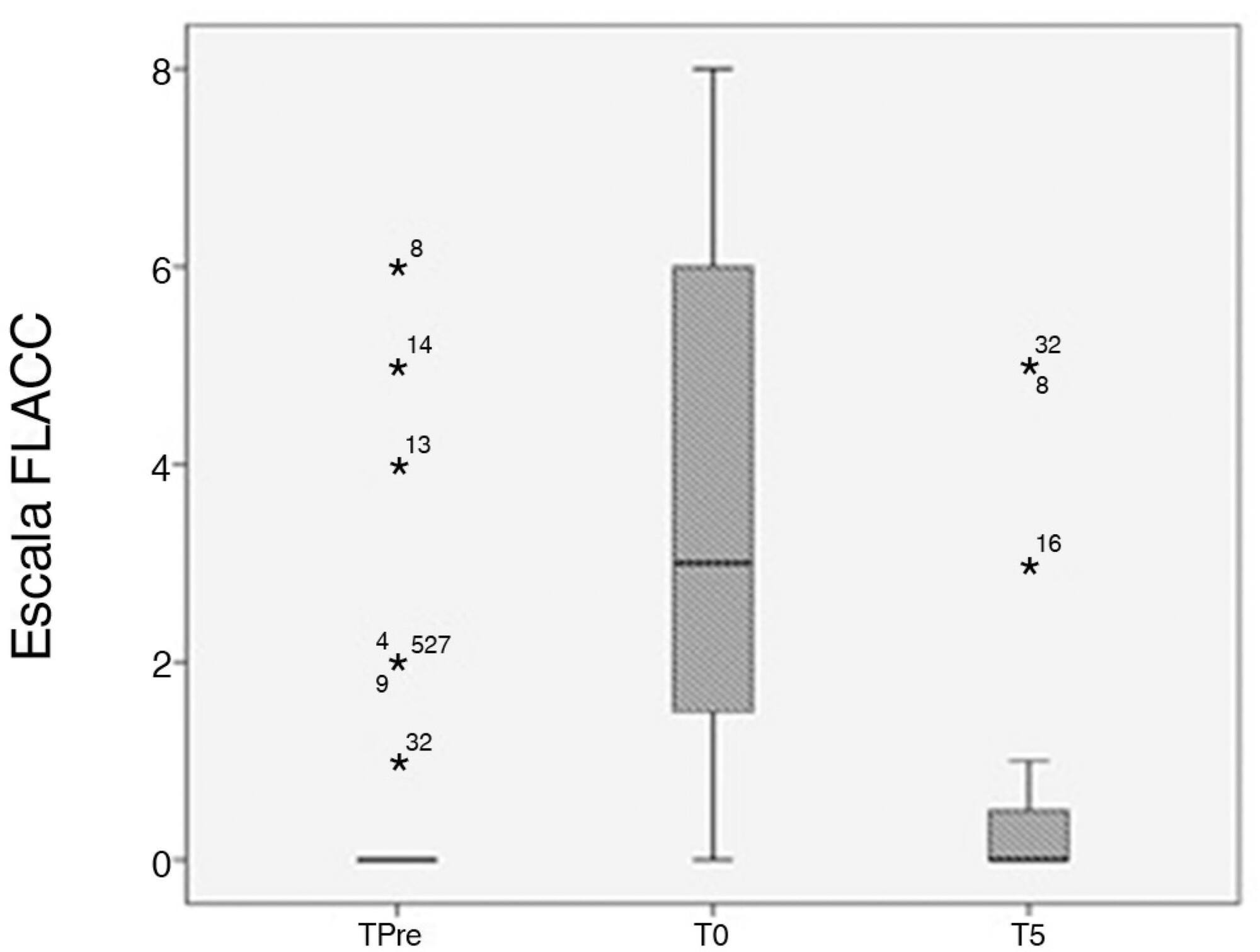
-
Original Articles
Characteristics and progression of children with acute viral bronchiolitis subjected to mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(1):55-61
Abstract
Original ArticlesCharacteristics and progression of children with acute viral bronchiolitis subjected to mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(1):55-61
DOI 10.5935/0103-507X.20160003
Views0ABSTRACT
Objective:
To analyze the characteristics of children with acute viral bronchiolitis subjected to mechanical ventilation for three consecutive years and to correlate their progression with mechanical ventilation parameters and fluid balance.
Methods:
Longitudinal study of a series of infants (< one year old) subjected to mechanical ventilation for acute viral bronchitis from January 2012 to September 2014 in the pediatric intensive care unit. The children's clinical records were reviewed, and their anthropometric data, mechanical ventilation parameters, fluid balance, clinical progression, and major complications were recorded.
Results:
Sixty-six infants (3.0 ± 2.0 months old and with an average weight of 4.7 ± 1.4kg) were included, of whom 62% were boys; a virus was identified in 86%. The average duration of mechanical ventilation was 6.5 ± 2.9 days, and the average length of stay in the pediatric intensive care unit was 9.1 ± 3.5 days; the mortality rate was 1.5% (1/66). The peak inspiratory pressure remained at 30cmH2O during the first four days of mechanical ventilation and then decreased before extubation (25 cmH2O; p < 0.05). Pneumothorax occurred in 10% of the sample and extubation failure in 9%, which was due to upper airway obstruction in half of the cases. The cumulative fluid balance on mechanical ventilation day four was 402 ± 254mL, which corresponds to an increase of 9.0 ± 5.9% in body weight. Thirty-seven patients (56%) exhibited a weight gain of 10% or more, which was not significantly associated with the ventilation parameters on mechanical ventilation day four, extubation failure, duration of mechanical ventilation or length of stay in the pediatric intensive care unit.
Conclusion:
The rate of mechanical ventilation for acute viral bronchiolitis remains constant, being associated with low mortality, few adverse effects, and positive cumulative fluid balance during the first days. Better fluid control might reduce the duration of mechanical ventilation.
Keywords:BronchiolitisChildEdemaIntensive care unitsRespiration, artificialRespiratory syncytial virusesSee moreViews0Abstract
Original ArticlesCharacteristics and progression of children with acute viral bronchiolitis subjected to mechanical ventilation
Rev Bras Ter Intensiva. 2016;28(1):55-61
DOI 10.5935/0103-507X.20160003
Views0ABSTRACT
Objective:
To analyze the characteristics of children with acute viral bronchiolitis subjected to mechanical ventilation for three consecutive years and to correlate their progression with mechanical ventilation parameters and fluid balance.
Methods:
Longitudinal study of a series of infants (< one year old) subjected to mechanical ventilation for acute viral bronchitis from January 2012 to September 2014 in the pediatric intensive care unit. The children's clinical records were reviewed, and their anthropometric data, mechanical ventilation parameters, fluid balance, clinical progression, and major complications were recorded.
Results:
Sixty-six infants (3.0 ± 2.0 months old and with an average weight of 4.7 ± 1.4kg) were included, of whom 62% were boys; a virus was identified in 86%. The average duration of mechanical ventilation was 6.5 ± 2.9 days, and the average length of stay in the pediatric intensive care unit was 9.1 ± 3.5 days; the mortality rate was 1.5% (1/66). The peak inspiratory pressure remained at 30cmH2O during the first four days of mechanical ventilation and then decreased before extubation (25 cmH2O; p < 0.05). Pneumothorax occurred in 10% of the sample and extubation failure in 9%, which was due to upper airway obstruction in half of the cases. The cumulative fluid balance on mechanical ventilation day four was 402 ± 254mL, which corresponds to an increase of 9.0 ± 5.9% in body weight. Thirty-seven patients (56%) exhibited a weight gain of 10% or more, which was not significantly associated with the ventilation parameters on mechanical ventilation day four, extubation failure, duration of mechanical ventilation or length of stay in the pediatric intensive care unit.
Conclusion:
The rate of mechanical ventilation for acute viral bronchiolitis remains constant, being associated with low mortality, few adverse effects, and positive cumulative fluid balance during the first days. Better fluid control might reduce the duration of mechanical ventilation.
Keywords:BronchiolitisChildEdemaIntensive care unitsRespiration, artificialRespiratory syncytial virusesSee more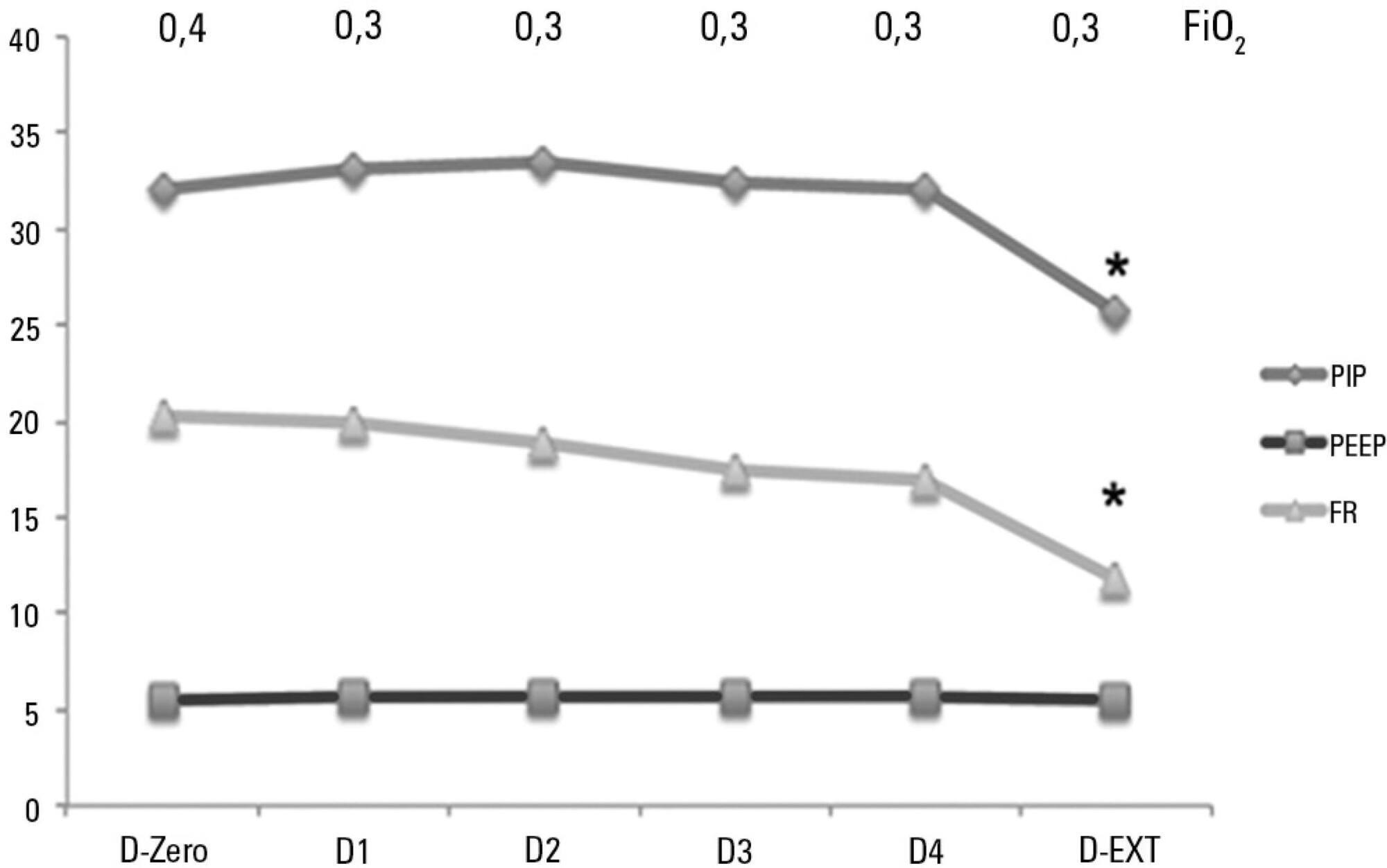
-
Original Articles
Evaluation of cost-effectiveness from the funding body’s point of view of ultrasound-guided central venous catheter insertion compared with the conventional technique
Rev Bras Ter Intensiva. 2016;28(1):62-69
Abstract
Original ArticlesEvaluation of cost-effectiveness from the funding body’s point of view of ultrasound-guided central venous catheter insertion compared with the conventional technique
Rev Bras Ter Intensiva. 2016;28(1):62-69
DOI 10.5935/0103-507X.20160014
Views0ABSTRACT
Objective:
To evaluate the cost-effectiveness, from the funding body’s point of view, of real-time ultrasound-guided central venous catheter insertion compared to the traditional method, which is based on the external anatomical landmark technique.
Methods:
A theoretical simulation based on international literature data was applied to the Brazilian context, i.e., the Unified Health System (Sistema Único de Saúde – SUS). A decision tree was constructed that showed the two central venous catheter insertion techniques: real-time ultrasonography versus external anatomical landmarks. The probabilities of failure and complications were extracted from a search on the PubMed and Embase databases, and values associated with the procedure and with complications were taken from market research and the Department of Information Technology of the Unified Health System (DATASUS). Each central venous catheter insertion alternative had a cost that could be calculated by following each of the possible paths on the decision tree. The incremental cost-effectiveness ratio was calculated by dividing the mean incremental cost of real-time ultrasound compared to the external anatomical landmark technique by the mean incremental benefit, in terms of avoided complications.
Results:
When considering the incorporation of real-time ultrasound and the concomitant lower cost due to the reduced number of complications, the decision tree revealed a final mean cost for the external anatomical landmark technique of 262.27 Brazilian reals (R$) and for real-time ultrasound of R$187.94. The final incremental cost of the real-time ultrasound-guided technique was -R$74.33 per central venous catheter. The incremental cost-effectiveness ratio was -R$2,494.34 due to the pneumothorax avoided.
Conclusion:
Real-time ultrasound-guided central venous catheter insertion was associated with decreased failure and complication rates and hypothetically reduced costs from the view of the funding body, which in this case was the SUS.
Keywords:Central venous cateteres/ economicsCosts and cost analysisDiagnostic techniques and proceduresHelath care costsUltrasonography/economicsUnified Health System/economicsSee moreViews0Abstract
Original ArticlesEvaluation of cost-effectiveness from the funding body’s point of view of ultrasound-guided central venous catheter insertion compared with the conventional technique
Rev Bras Ter Intensiva. 2016;28(1):62-69
DOI 10.5935/0103-507X.20160014
Views0ABSTRACT
Objective:
To evaluate the cost-effectiveness, from the funding body’s point of view, of real-time ultrasound-guided central venous catheter insertion compared to the traditional method, which is based on the external anatomical landmark technique.
Methods:
A theoretical simulation based on international literature data was applied to the Brazilian context, i.e., the Unified Health System (Sistema Único de Saúde – SUS). A decision tree was constructed that showed the two central venous catheter insertion techniques: real-time ultrasonography versus external anatomical landmarks. The probabilities of failure and complications were extracted from a search on the PubMed and Embase databases, and values associated with the procedure and with complications were taken from market research and the Department of Information Technology of the Unified Health System (DATASUS). Each central venous catheter insertion alternative had a cost that could be calculated by following each of the possible paths on the decision tree. The incremental cost-effectiveness ratio was calculated by dividing the mean incremental cost of real-time ultrasound compared to the external anatomical landmark technique by the mean incremental benefit, in terms of avoided complications.
Results:
When considering the incorporation of real-time ultrasound and the concomitant lower cost due to the reduced number of complications, the decision tree revealed a final mean cost for the external anatomical landmark technique of 262.27 Brazilian reals (R$) and for real-time ultrasound of R$187.94. The final incremental cost of the real-time ultrasound-guided technique was -R$74.33 per central venous catheter. The incremental cost-effectiveness ratio was -R$2,494.34 due to the pneumothorax avoided.
Conclusion:
Real-time ultrasound-guided central venous catheter insertion was associated with decreased failure and complication rates and hypothetically reduced costs from the view of the funding body, which in this case was the SUS.
Keywords:Central venous cateteres/ economicsCosts and cost analysisDiagnostic techniques and proceduresHelath care costsUltrasonography/economicsUnified Health System/economicsSee more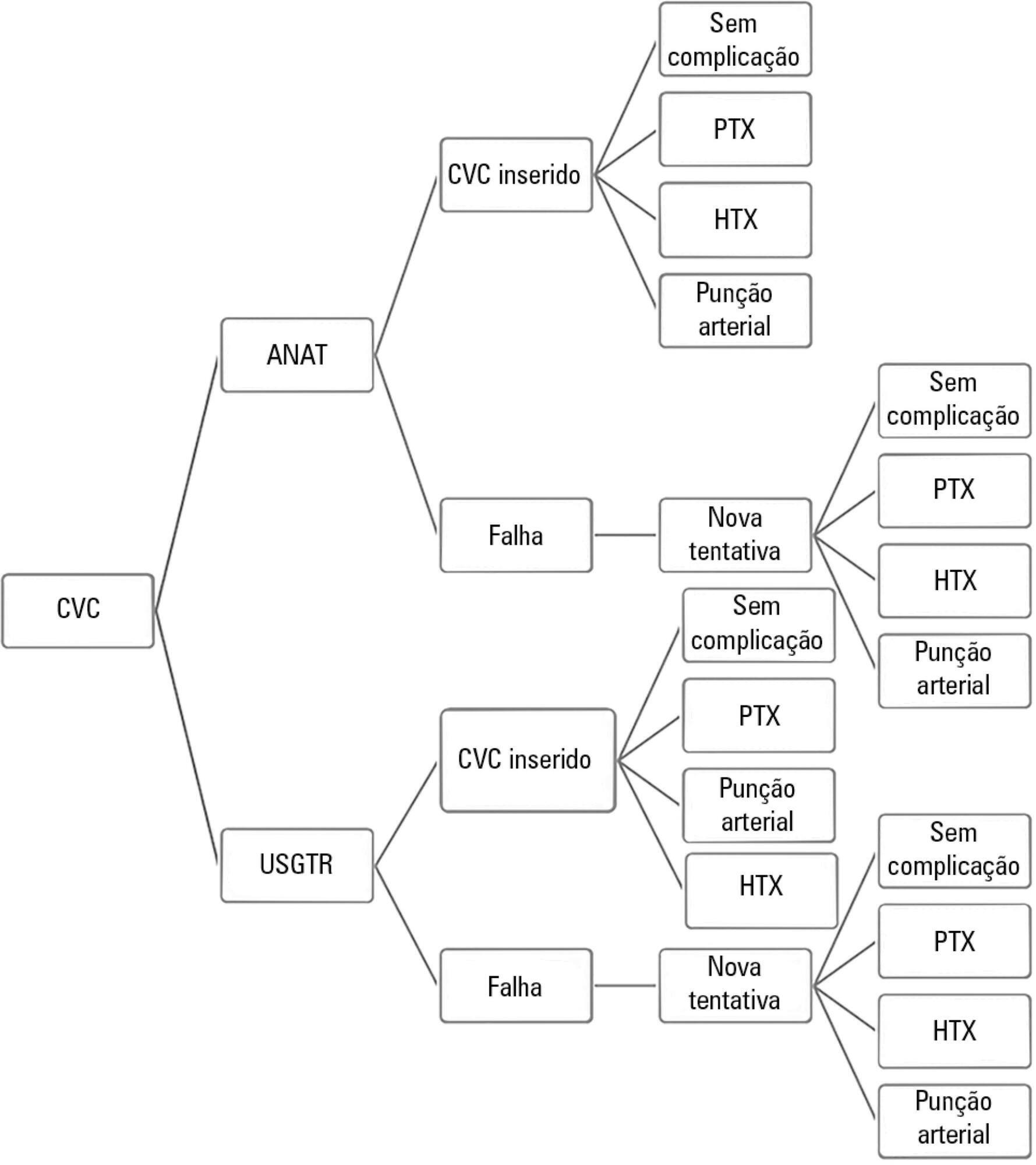
-
Original Articles
Prognostics factors for mortality and renal recovery in critically ill patients with acute kidney injury and renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(1):70-77
Abstract
Original ArticlesPrognostics factors for mortality and renal recovery in critically ill patients with acute kidney injury and renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(1):70-77
DOI 10.5935/0103-507X.20160015
Views0ABSTRACT
Objective:
Identify prognostic factors related to mortality and non-recovery of renal function.
Methods:
A prospective single-center study was conducted at the intensive care medicine department of a university hospital between 2012 and 2015. Patients with acute kidney injury receiving continuous renal replacement therapy were included in the study. Clinical and analytical parameters were collected, and the reasons for initiation and discontinuation of renal replacement therapy were examined.
Results:
A total of 41 patients were included in the study, of whom 43.9% had sepsis. The median Simplified Acute Physiology Score II (SAPSII) was 56 and the mortality was 53.7%, with a predicted mortality of 59.8%. The etiology of acute kidney injury was often multifactorial (56.1%). Survivors had lower cumulative fluid balance (median = 3,600mL, interquartile range [IQR] = 1,175 – 8,025) than non-survivors (median = 12,000mL, IQR = 6,625 – 17,875; p = 0.004). Patients who recovered renal function (median = 51.0, IQR = 45.8 – 56.2) had lower SAPS II than those who do not recover renal function (median = 73, IQR = 54 – 85; p = 0.005) as well as lower fluid balance (median = 3,850, IQR = 1,425 – 8,025 versus median = 11,500, IQR = 6,625 – 16,275; p = 0.004).
Conclusions:
SAPS II at admission and cumulative fluid balance during renal support therapy were risk factors for mortality and non-recovery of renal function among critically ill patients with acute kidney injury needing renal replacement therapy.
Keywords:Acute kidney injuryInsufficiency renal, chronicIntensive careRenal insufficiencyRenal replacement therapySee moreViews0Abstract
Original ArticlesPrognostics factors for mortality and renal recovery in critically ill patients with acute kidney injury and renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(1):70-77
DOI 10.5935/0103-507X.20160015
Views0ABSTRACT
Objective:
Identify prognostic factors related to mortality and non-recovery of renal function.
Methods:
A prospective single-center study was conducted at the intensive care medicine department of a university hospital between 2012 and 2015. Patients with acute kidney injury receiving continuous renal replacement therapy were included in the study. Clinical and analytical parameters were collected, and the reasons for initiation and discontinuation of renal replacement therapy were examined.
Results:
A total of 41 patients were included in the study, of whom 43.9% had sepsis. The median Simplified Acute Physiology Score II (SAPSII) was 56 and the mortality was 53.7%, with a predicted mortality of 59.8%. The etiology of acute kidney injury was often multifactorial (56.1%). Survivors had lower cumulative fluid balance (median = 3,600mL, interquartile range [IQR] = 1,175 – 8,025) than non-survivors (median = 12,000mL, IQR = 6,625 – 17,875; p = 0.004). Patients who recovered renal function (median = 51.0, IQR = 45.8 – 56.2) had lower SAPS II than those who do not recover renal function (median = 73, IQR = 54 – 85; p = 0.005) as well as lower fluid balance (median = 3,850, IQR = 1,425 – 8,025 versus median = 11,500, IQR = 6,625 – 16,275; p = 0.004).
Conclusions:
SAPS II at admission and cumulative fluid balance during renal support therapy were risk factors for mortality and non-recovery of renal function among critically ill patients with acute kidney injury needing renal replacement therapy.
Keywords:Acute kidney injuryInsufficiency renal, chronicIntensive careRenal insufficiencyRenal replacement therapySee more -
Case Reports
Use of a dual lumen cannula for venovenous extra corporeal membrane oxygenation in a patient with acute respiratory distress syndrome and a previously inserted inferior vena cava filter: a case report
Rev Bras Ter Intensiva. 2016;28(1):78-82
Abstract
Case ReportsUse of a dual lumen cannula for venovenous extra corporeal membrane oxygenation in a patient with acute respiratory distress syndrome and a previously inserted inferior vena cava filter: a case report
Rev Bras Ter Intensiva. 2016;28(1):78-82
DOI 10.5935/0103-507X.20160001
Views0ABSTRACT
Extracorporeal membrane oxygenation is used in refractory hypoxemia in many clinical settings. Thoracic trauma patients usually develop acute respiratory distress syndrome. Due to high risk of bleeding, thrombotic complications present in this context are particularly difficult to manage and usually require insertion of an inferior vena cava filter to prevent embolism from the distal veins to the pulmonary circulation. Here, we present a case of a thoracic trauma patient with severe acute respiratory distress syndrome requiring venovenous extracorporeal membrane oxygenation via a right internal jugular double lumen cannula due to a previously inserted inferior vena cava filter caused by distal bilateral calf muscle vein deep vein thrombosis.
Keywords:Case reportsExtracorporeal membrane oxygenationInferior vena cava filterRespiratory distress syndrome, adultThoracic injuryVena cava filtersVenous thrombosisSee moreViews0Abstract
Case ReportsUse of a dual lumen cannula for venovenous extra corporeal membrane oxygenation in a patient with acute respiratory distress syndrome and a previously inserted inferior vena cava filter: a case report
Rev Bras Ter Intensiva. 2016;28(1):78-82
DOI 10.5935/0103-507X.20160001
Views0ABSTRACT
Extracorporeal membrane oxygenation is used in refractory hypoxemia in many clinical settings. Thoracic trauma patients usually develop acute respiratory distress syndrome. Due to high risk of bleeding, thrombotic complications present in this context are particularly difficult to manage and usually require insertion of an inferior vena cava filter to prevent embolism from the distal veins to the pulmonary circulation. Here, we present a case of a thoracic trauma patient with severe acute respiratory distress syndrome requiring venovenous extracorporeal membrane oxygenation via a right internal jugular double lumen cannula due to a previously inserted inferior vena cava filter caused by distal bilateral calf muscle vein deep vein thrombosis.
Keywords:Case reportsExtracorporeal membrane oxygenationInferior vena cava filterRespiratory distress syndrome, adultThoracic injuryVena cava filtersVenous thrombosisSee more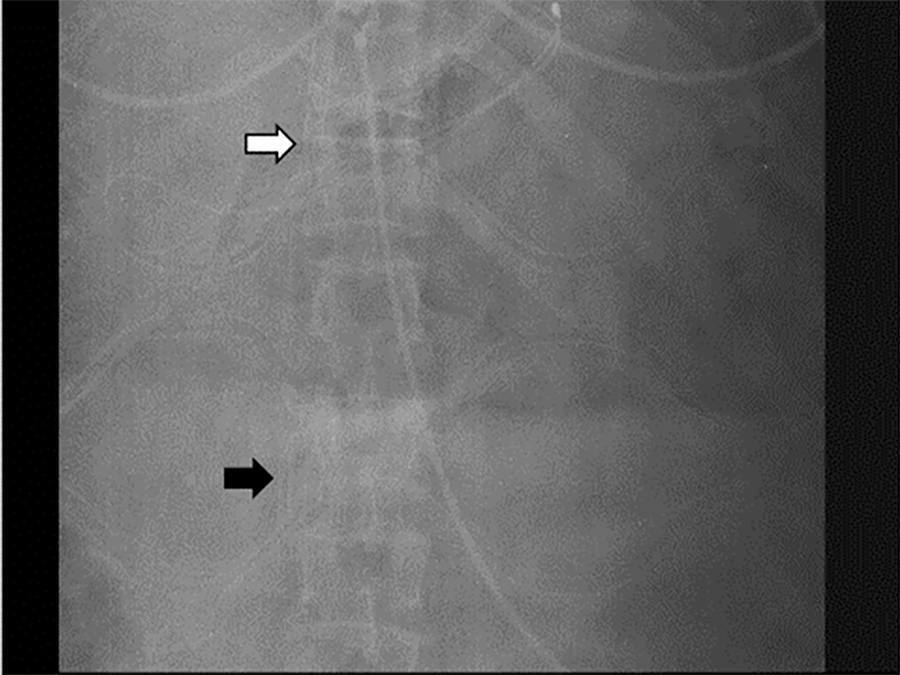
-
Case Reports
Native aortic valve pneumococcal endocarditis – fulminant presentation
Rev Bras Ter Intensiva. 2016;28(1):83-86
Abstract
Case ReportsNative aortic valve pneumococcal endocarditis – fulminant presentation
Rev Bras Ter Intensiva. 2016;28(1):83-86
DOI 10.5935/0103-507X.20160004
Views0See moreABSTRACT
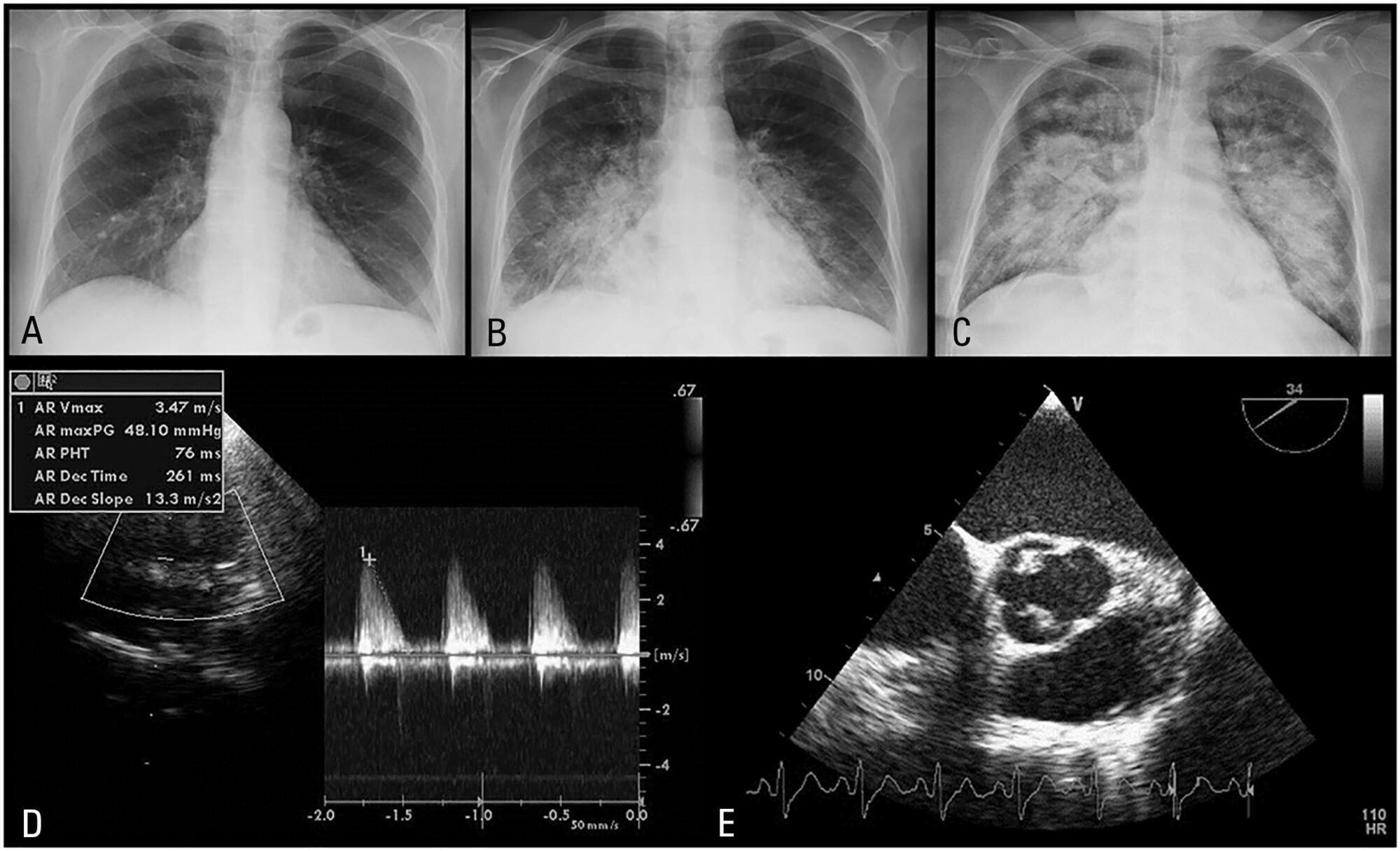
Pneumococcal endocarditis is a rare entity, corresponding to 1 to 3% of native valve endocarditis cases. It has a typically adverse prognosis, with high mortality. There is a reported predilection for the aortic valve; thus, a common presentation is acute left heart failure. We present a case of a 60-year-old woman with a history of sinusitis, who was admitted with the diagnosis of pneumonia. She rapidly deteriorated with signs of septic shock and was transferred to the critical care unit. The transesophageal echocardiogram revealed severe aortic regurgitation due to valve vegetations. Blood cultures were positive for Streptococcus pneumoniae. She underwent cardiac surgery and had multiple postoperative complications. Nonetheless, the patient made a slow and complete recovery. Infectious endocarditis should be ruled out if any suspicion arises, and echocardiography should be performed in an early stage in patients with poor response to vasopressors and inotropes. Patients with pneumococcal endocarditis benefit from an aggressive approach, with performance of early surgery.
Views0Abstract
Case ReportsNative aortic valve pneumococcal endocarditis – fulminant presentation
Rev Bras Ter Intensiva. 2016;28(1):83-86
DOI 10.5935/0103-507X.20160004
Views0See moreABSTRACT
Pneumococcal endocarditis is a rare entity, corresponding to 1 to 3% of native valve endocarditis cases. It has a typically adverse prognosis, with high mortality. There is a reported predilection for the aortic valve; thus, a common presentation is acute left heart failure. We present a case of a 60-year-old woman with a history of sinusitis, who was admitted with the diagnosis of pneumonia. She rapidly deteriorated with signs of septic shock and was transferred to the critical care unit. The transesophageal echocardiogram revealed severe aortic regurgitation due to valve vegetations. Blood cultures were positive for Streptococcus pneumoniae. She underwent cardiac surgery and had multiple postoperative complications. Nonetheless, the patient made a slow and complete recovery. Infectious endocarditis should be ruled out if any suspicion arises, and echocardiography should be performed in an early stage in patients with poor response to vasopressors and inotropes. Patients with pneumococcal endocarditis benefit from an aggressive approach, with performance of early surgery.
-
Case Reports
Heliox in the treatment of status asthmaticus: case reports
Rev Bras Ter Intensiva. 2016;28(1):87-91
Abstract
Case ReportsHeliox in the treatment of status asthmaticus: case reports
Rev Bras Ter Intensiva. 2016;28(1):87-91
DOI 10.5935/0103-507X.20160005
Views0See moreABSTRACT
Helium was discovered in 1868 by the French astronomer Pierre-Jules-César Janssen and was first used as a therapeutic treatment for airway obstruction by Barach almost 70 years later, in 1934. Heliox is characterized by its low density, which makes it more fluid under conditions of turbulence, thus minimizing airway pressure and facilitating the occurrence of laminar flow. The present article describes two clinical cases of patients with status asthmaticus subjected to mechanical ventilation and refractory to treatment in whom heliox was used, which allowed optimization of the efficacy of conventional pharmacological treatments. Although heliox is still used sporadically and its true efficacy has not been well demonstrated, the unique physical properties of helium and the theoretical improvement of the airflow in obstructed airways have produced scientific interest and stimulated research. Heliox can be used simultaneously with conventional therapies in cases of serious and refractory exacerbations of severe obstructive disease.
Views0Abstract
Case ReportsHeliox in the treatment of status asthmaticus: case reports
Rev Bras Ter Intensiva. 2016;28(1):87-91
DOI 10.5935/0103-507X.20160005
Views0See moreABSTRACT
Helium was discovered in 1868 by the French astronomer Pierre-Jules-César Janssen and was first used as a therapeutic treatment for airway obstruction by Barach almost 70 years later, in 1934. Heliox is characterized by its low density, which makes it more fluid under conditions of turbulence, thus minimizing airway pressure and facilitating the occurrence of laminar flow. The present article describes two clinical cases of patients with status asthmaticus subjected to mechanical ventilation and refractory to treatment in whom heliox was used, which allowed optimization of the efficacy of conventional pharmacological treatments. Although heliox is still used sporadically and its true efficacy has not been well demonstrated, the unique physical properties of helium and the theoretical improvement of the airflow in obstructed airways have produced scientific interest and stimulated research. Heliox can be used simultaneously with conventional therapies in cases of serious and refractory exacerbations of severe obstructive disease.

-
Letter to the Editor
To: Noninvasive positive pressure ventilation after extubation: features and outcomes in clinical practice
Rev Bras Ter Intensiva. 2016;28(1):92-93
Abstract
Letter to the EditorTo: Noninvasive positive pressure ventilation after extubation: features and outcomes in clinical practice
Rev Bras Ter Intensiva. 2016;28(1):92-93
DOI 10.5935/0103-507X.20160016
Views0To the editor, We carefully read the article by Yamauchi et al.() on using noninvasive positive pressure ventilation (NIPPV) after extubation and congratulate the authors on their study. However, in the last few years, several studies with conflicting results have been published.(–)[…]See moreViews0Abstract
Letter to the EditorTo: Noninvasive positive pressure ventilation after extubation: features and outcomes in clinical practice
Rev Bras Ter Intensiva. 2016;28(1):92-93
DOI 10.5935/0103-507X.20160016
Views0To the editor, We carefully read the article by Yamauchi et al.() on using noninvasive positive pressure ventilation (NIPPV) after extubation and congratulate the authors on their study. However, in the last few years, several studies with conflicting results have been published.(–)[…]See more -
Author’s Response
Reply to: Noninvasive positive pressure ventilation after extubation: features and outcomes in clinical practice
Rev Bras Ter Intensiva. 2016;28(1):94-95
Abstract
Author’s ResponseReply to: Noninvasive positive pressure ventilation after extubation: features and outcomes in clinical practice
Rev Bras Ter Intensiva. 2016;28(1):94-95
DOI 10.5935/0103-507X.20160017
Views0The authors gratefully acknowledge the comments made by the researchers. We will analyze the methodologies currently used by our group and the cited studies to understand the differences described in the letter. Additionally, we would like to emphasize that the study was a prospective cohort study, in which the researchers collected data on a daily […]See moreViews0Abstract
Author’s ResponseReply to: Noninvasive positive pressure ventilation after extubation: features and outcomes in clinical practice
Rev Bras Ter Intensiva. 2016;28(1):94-95
DOI 10.5935/0103-507X.20160017
Views0The authors gratefully acknowledge the comments made by the researchers. We will analyze the methodologies currently used by our group and the cited studies to understand the differences described in the letter. Additionally, we would like to emphasize that the study was a prospective cohort study, in which the researchers collected data on a daily […]See more -
Erratum
ERRATUM
Rev Bras Ter Intensiva. 2016;28(1):96-96
Abstract
ErratumERRATUM
Rev Bras Ter Intensiva. 2016;28(1):96-96
DOI 10.5935/0103-507X.20160018
Views0In the article Influence of different degrees of head elevation on respiratory mechanics in mechanically ventilated patients, DOI number: 10.5935/0103-507X.20150059, published in Revista Brasileira de Terapia Intensiva 2015;27(4):347-52, page 347 “Vanessa Silva Salgado” should be read as “Vanessa Salgado Silva”.In the article Delirium in intensive care unit patients under noninvasive ventilation: a multinational survey, DOI […]See moreViews0Abstract
ErratumERRATUM
Rev Bras Ter Intensiva. 2016;28(1):96-96
DOI 10.5935/0103-507X.20160018
Views0In the article Influence of different degrees of head elevation on respiratory mechanics in mechanically ventilated patients, DOI number: 10.5935/0103-507X.20150059, published in Revista Brasileira de Terapia Intensiva 2015;27(4):347-52, page 347 “Vanessa Silva Salgado” should be read as “Vanessa Salgado Silva”.In the article Delirium in intensive care unit patients under noninvasive ventilation: a multinational survey, DOI […]See more
Volume Articles - Critical Care Science (CCS)
