Aortic valve Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2016;28(1):83-86
DOI 10.5935/0103-507X.20160004
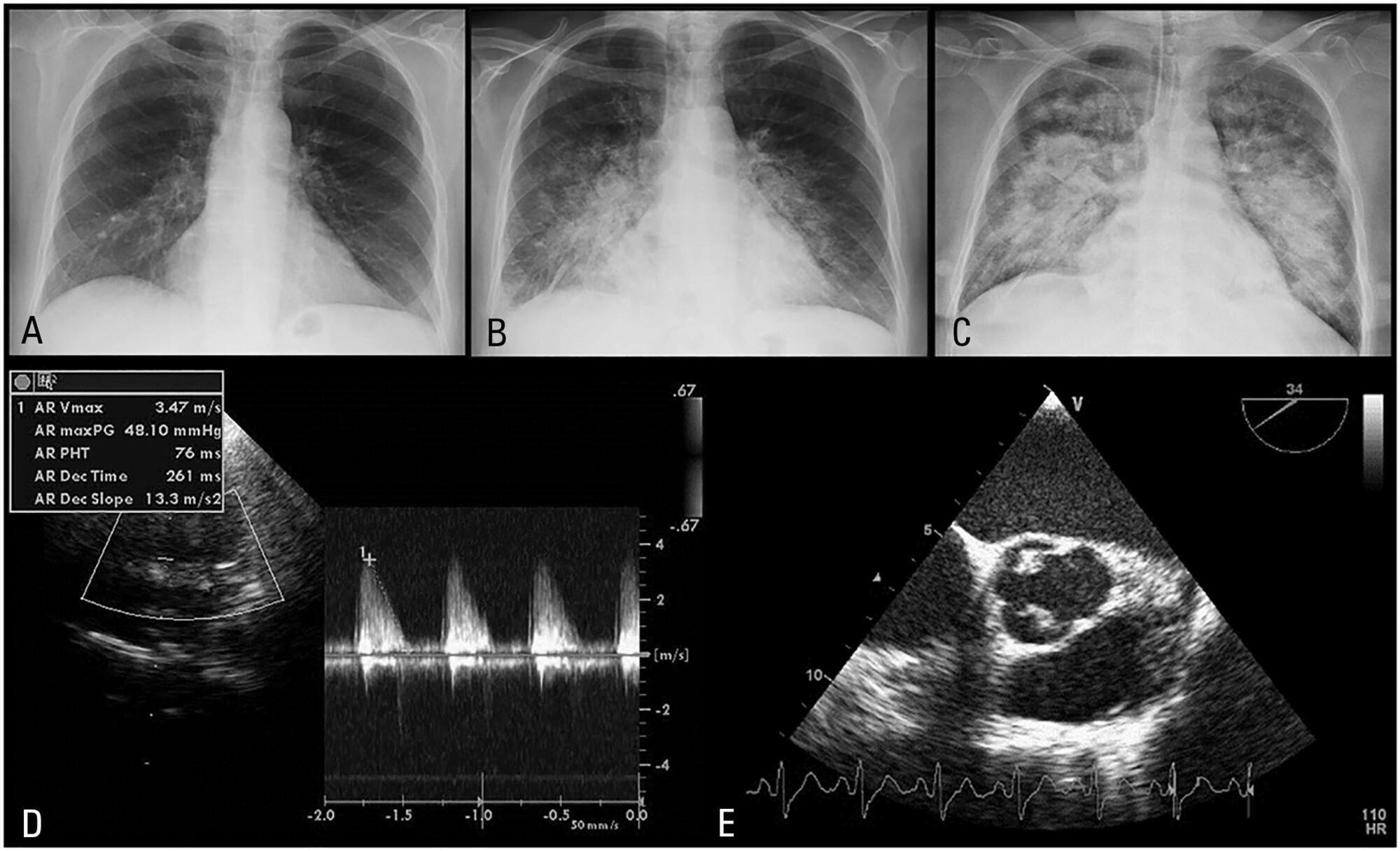
Pneumococcal endocarditis is a rare entity, corresponding to 1 to 3% of native valve endocarditis cases. It has a typically adverse prognosis, with high mortality. There is a reported predilection for the aortic valve; thus, a common presentation is acute left heart failure. We present a case of a 60-year-old woman with a history of sinusitis, who was admitted with the diagnosis of pneumonia. She rapidly deteriorated with signs of septic shock and was transferred to the critical care unit. The transesophageal echocardiogram revealed severe aortic regurgitation due to valve vegetations. Blood cultures were positive for Streptococcus pneumoniae. She underwent cardiac surgery and had multiple postoperative complications. Nonetheless, the patient made a slow and complete recovery. Infectious endocarditis should be ruled out if any suspicion arises, and echocardiography should be performed in an early stage in patients with poor response to vasopressors and inotropes. Patients with pneumococcal endocarditis benefit from an aggressive approach, with performance of early surgery.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):83-86
DOI 10.5935/0103-507X.20160004
Pneumococcal endocarditis is a rare entity, corresponding to 1 to 3% of native valve endocarditis cases. It has a typically adverse prognosis, with high mortality. There is a reported predilection for the aortic valve; thus, a common presentation is acute left heart failure. We present a case of a 60-year-old woman with a history of sinusitis, who was admitted with the diagnosis of pneumonia. She rapidly deteriorated with signs of septic shock and was transferred to the critical care unit. The transesophageal echocardiogram revealed severe aortic regurgitation due to valve vegetations. Blood cultures were positive for Streptococcus pneumoniae. She underwent cardiac surgery and had multiple postoperative complications. Nonetheless, the patient made a slow and complete recovery. Infectious endocarditis should be ruled out if any suspicion arises, and echocardiography should be performed in an early stage in patients with poor response to vasopressors and inotropes. Patients with pneumococcal endocarditis benefit from an aggressive approach, with performance of early surgery.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):185-189
DOI 10.5935/0103-507X.20150031
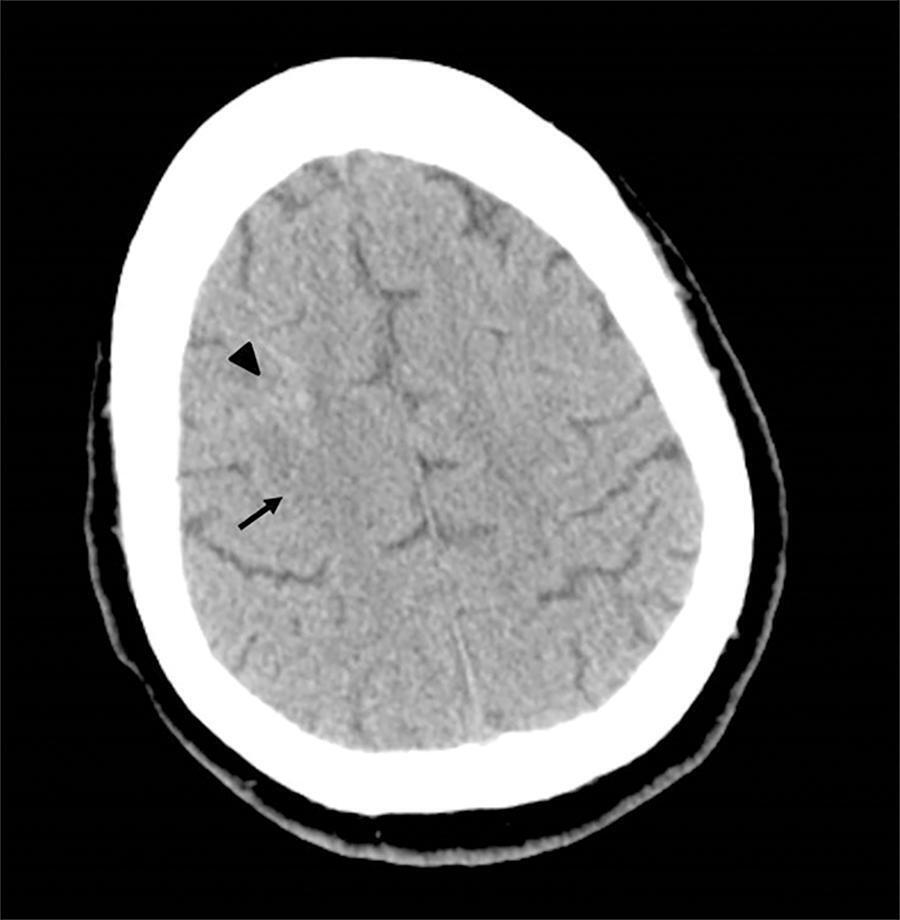
This is a case report of a 43-year-old Caucasian male with end-stage renal disease being treated with hemodialysis and infective endocarditis in the aortic and tricuspid valves. The clinical presentation was dominated by neurologic impairment with cerebral embolism and hemorrhagic components. A thoracoabdominal computerized tomography scan revealed septic pulmonary embolus. The patient underwent empirical antibiotherapy with ceftriaxone, gentamicin and vancomycin, and the therapy was changed to flucloxacilin and gentamicin after the isolation of S. aureus in blood cultures. The multidisciplinary team determined that the patient should undergo valve replacement after the stabilization of the intracranial hemorrhage; however, on the 8th day of hospitalization, the patient entered cardiac arrest due to a massive septic pulmonary embolism and died. Despite the risk of aggravation of the hemorrhagic cerebral lesion, early surgical intervention should be considered in high-risk patients.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):185-189
DOI 10.5935/0103-507X.20150031
This is a case report of a 43-year-old Caucasian male with end-stage renal disease being treated with hemodialysis and infective endocarditis in the aortic and tricuspid valves. The clinical presentation was dominated by neurologic impairment with cerebral embolism and hemorrhagic components. A thoracoabdominal computerized tomography scan revealed septic pulmonary embolus. The patient underwent empirical antibiotherapy with ceftriaxone, gentamicin and vancomycin, and the therapy was changed to flucloxacilin and gentamicin after the isolation of S. aureus in blood cultures. The multidisciplinary team determined that the patient should undergo valve replacement after the stabilization of the intracranial hemorrhage; however, on the 8th day of hospitalization, the patient entered cardiac arrest due to a massive septic pulmonary embolism and died. Despite the risk of aggravation of the hemorrhagic cerebral lesion, early surgical intervention should be considered in high-risk patients.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):339-345
DOI 10.1590/S0103-507X2010000400005
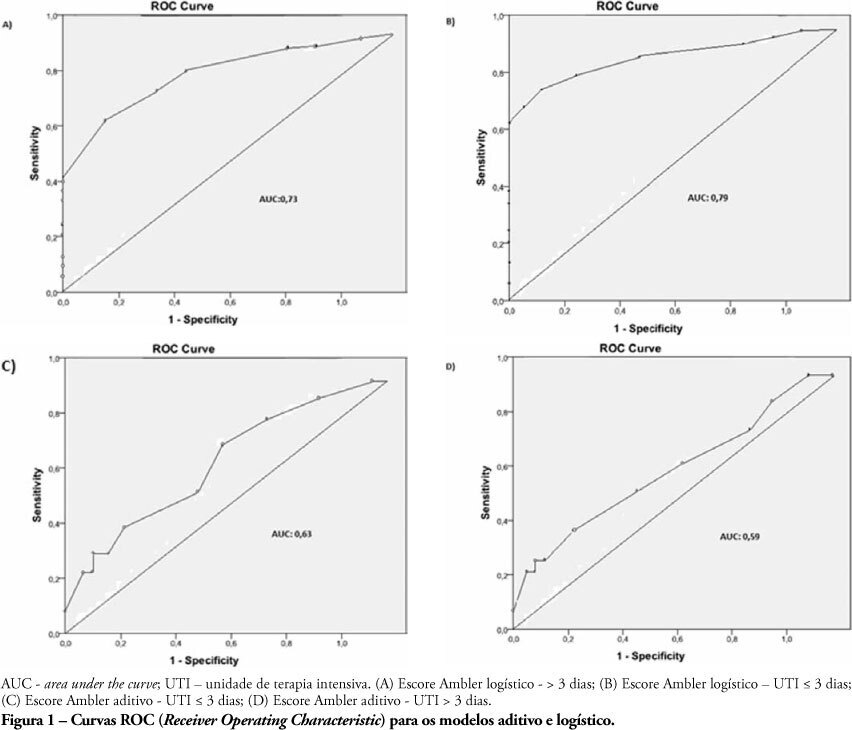
OBJECTIVES: The length of stay after prolonged cardiac surgery has been associated with poor immediate outcomes and increased costs. This study aimed to evaluate the predictive power of the Ambler Score to anticipate the length of stay in the intensive care unit. METHODS: This was a retrospective cohort study based on data collected from 110 patients undergoing valve replacement surgery alone or in combination with other procedures. Additive and logistic Ambler Scores were obtained and their predictive performances calculated using the Receiver Operating Characteristic curve. The normal length stay in the intensive care unit was assumed to be <3 days and prolonged >3 days. The areas under the receiver operating curves for both the additive and logistic models were compared using the Hanley-MacNeil test. RESULTS: The mean intensive care unit length of stay was 4.2 days. Sixty-three patients were male. The logistic model showed areas under the receiver operating characteristic curve of 0.73 and 0.79 for hospitalization > 3 days and < 3 days, respectively, showing good discriminative power. For the additive model, the areas were 0.63 and 0.59 for hospitalization > 3 days and < 3 days, respectively, a poor discriminative power. CONCLUSIONS: In our database, prolonged length of stay in the intensive care unit was positively correlated with the logistic Ambler score. The performance of the logistic Ambler Score had good discriminative power for correlation with the intensive care unit length of stay.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):339-345
DOI 10.1590/S0103-507X2010000400005
OBJECTIVES: The length of stay after prolonged cardiac surgery has been associated with poor immediate outcomes and increased costs. This study aimed to evaluate the predictive power of the Ambler Score to anticipate the length of stay in the intensive care unit. METHODS: This was a retrospective cohort study based on data collected from 110 patients undergoing valve replacement surgery alone or in combination with other procedures. Additive and logistic Ambler Scores were obtained and their predictive performances calculated using the Receiver Operating Characteristic curve. The normal length stay in the intensive care unit was assumed to be <3 days and prolonged >3 days. The areas under the receiver operating curves for both the additive and logistic models were compared using the Hanley-MacNeil test. RESULTS: The mean intensive care unit length of stay was 4.2 days. Sixty-three patients were male. The logistic model showed areas under the receiver operating characteristic curve of 0.73 and 0.79 for hospitalization > 3 days and < 3 days, respectively, showing good discriminative power. For the additive model, the areas were 0.63 and 0.59 for hospitalization > 3 days and < 3 days, respectively, a poor discriminative power. CONCLUSIONS: In our database, prolonged length of stay in the intensive care unit was positively correlated with the logistic Ambler score. The performance of the logistic Ambler Score had good discriminative power for correlation with the intensive care unit length of stay.