-
Intracranial pressure monitoring in the torture chambre
Rev Bras Ter Intensiva. 2015;27(4):303-304
Abstract
Intracranial pressure monitoring in the torture chambre
Rev Bras Ter Intensiva. 2015;27(4):303-304
DOI 10.5935/0103-507X.20150050
Views1After the BEST TRIP study appeared in December 2012 in the New England Journal of Medicine,() a large number of editorials, reviews, and new studies have addressed the issue of whether the monitoring of intracranial pressure (ICP) is relevant in the management of severe head injury and whether the costs are justified to achieve a […]See moreViews1

Abstract
Intracranial pressure monitoring in the torture chambre
Rev Bras Ter Intensiva. 2015;27(4):303-304
DOI 10.5935/0103-507X.20150050
Views1After the BEST TRIP study appeared in December 2012 in the New England Journal of Medicine,() a large number of editorials, reviews, and new studies have addressed the issue of whether the monitoring of intracranial pressure (ICP) is relevant in the management of severe head injury and whether the costs are justified to achieve a […]See more -
Editorial
Neurological outcomes after cardiac arrest: cold and dark issues
Rev Bras Ter Intensiva. 2015;27(4):305-306
Abstract
EditorialNeurological outcomes after cardiac arrest: cold and dark issues
Rev Bras Ter Intensiva. 2015;27(4):305-306
DOI 10.5935/0103-507X.20150051
Views0Prognostication after cardiac arrest is important for patients, families and health providers. It also has ethical and social implications. With the introduction of therapeutic hypothermia after recovery from cardiac arrest in comatose patients,(,) prognostication has become more complex and concerns have been raised, particularly about the amount of time and the number of tools required […]See moreViews0Abstract
EditorialNeurological outcomes after cardiac arrest: cold and dark issues
Rev Bras Ter Intensiva. 2015;27(4):305-306
DOI 10.5935/0103-507X.20150051
Views0Prognostication after cardiac arrest is important for patients, families and health providers. It also has ethical and social implications. With the introduction of therapeutic hypothermia after recovery from cardiac arrest in comatose patients,(,) prognostication has become more complex and concerns have been raised, particularly about the amount of time and the number of tools required […]See more -
A look at the diastolic function in severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):307-308
Abstract
A look at the diastolic function in severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):307-308
DOI 10.5935/0103-507X.20150052
Views0Myocardial dysfunction in sepsis is a complex entity due to the dynamic adaptation of the cardiovascular system to the disease process, the host response, and the effects of resuscitation. The pathophysiology of this entity is multifactorial; systemic, cellular, and extracellular mechanisms have been described, including maldistribution of coronary blood flow, myocardial injury, complement-triggered (C5a) myocyte […]See moreViews0Abstract
A look at the diastolic function in severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):307-308
DOI 10.5935/0103-507X.20150052
Views0Myocardial dysfunction in sepsis is a complex entity due to the dynamic adaptation of the cardiovascular system to the disease process, the host response, and the effects of resuscitation. The pathophysiology of this entity is multifactorial; systemic, cellular, and extracellular mechanisms have been described, including maldistribution of coronary blood flow, myocardial injury, complement-triggered (C5a) myocyte […]See more -
Commentary
Fluid resuscitation in the critically ill: what is the next challenge?
Rev Bras Ter Intensiva. 2015;27(4):309-311
Abstract
CommentaryFluid resuscitation in the critically ill: what is the next challenge?
Rev Bras Ter Intensiva. 2015;27(4):309-311
DOI 10.5935/0103-507X.20150053
Views1Fluid resuscitation in the critically ill: What are the remaining challenges?In 2010 the SAFE-TRIPS investigators reported on resuscitation fluid administration in 391 intensive care units (ICUs) in 25 countries.() The study found that more than one third of patients in the ICUs received resuscitation fluids on the study day and that the choice of fluid […]See moreViews1Abstract
CommentaryFluid resuscitation in the critically ill: what is the next challenge?
Rev Bras Ter Intensiva. 2015;27(4):309-311
DOI 10.5935/0103-507X.20150053
Views1Fluid resuscitation in the critically ill: What are the remaining challenges?In 2010 the SAFE-TRIPS investigators reported on resuscitation fluid administration in 391 intensive care units (ICUs) in 25 countries.() The study found that more than one third of patients in the ICUs received resuscitation fluids on the study day and that the choice of fluid […]See more -
Commentary
Improving outcomes for the critically ill in developing countries: what is next?
Rev Bras Ter Intensiva. 2015;27(4):312-314
Abstract
CommentaryImproving outcomes for the critically ill in developing countries: what is next?
Rev Bras Ter Intensiva. 2015;27(4):312-314
DOI 10.5935/0103-507X.20150054
Views0Critical care in developing countriesCritical care is a complicated, high risk, resource-dependent environment. Developing countries face common barriers to delivering quality emergent care due to the lack of supplies, coordination, infrastructure, technology, and human resources (e.g., competency-based education, multi-disciplinary staff and access to the most recent literature).() More importantly, the capacity to provide care for […]See moreViews0Abstract
CommentaryImproving outcomes for the critically ill in developing countries: what is next?
Rev Bras Ter Intensiva. 2015;27(4):312-314
DOI 10.5935/0103-507X.20150054
Views0Critical care in developing countriesCritical care is a complicated, high risk, resource-dependent environment. Developing countries face common barriers to delivering quality emergent care due to the lack of supplies, coordination, infrastructure, technology, and human resources (e.g., competency-based education, multi-disciplinary staff and access to the most recent literature).() More importantly, the capacity to provide care for […]See more -
Original Article
Measurement of intracranial pressure and short-term outcomes of patients with traumatic brain injury: a propensity-matched analysis
Rev Bras Ter Intensiva. 2015;27(4):315-321
Abstract
Original ArticleMeasurement of intracranial pressure and short-term outcomes of patients with traumatic brain injury: a propensity-matched analysis
Rev Bras Ter Intensiva. 2015;27(4):315-321
DOI 10.5935/0103-507X.20150055
Views0See moreABSTRACT
Objective:
To assess the impact of intracranial pressure monitoring on the short-term outcomes of traumatic brain injury patients.
Methods:
Retrospective observational study including 299 consecutive patients admitted due to traumatic brain injury from January 2011 through July 2012 at a Level 1 trauma center in São Paulo, Brazil. Patients were categorized in two groups according to the measurement of intracranial pressure (measured intracranial pressure and non-measured intracranial pressure groups). We applied a propensity-matched analysis to adjust for possible confounders (variables contained in the Crash Score prognostic algorithm).
Results:
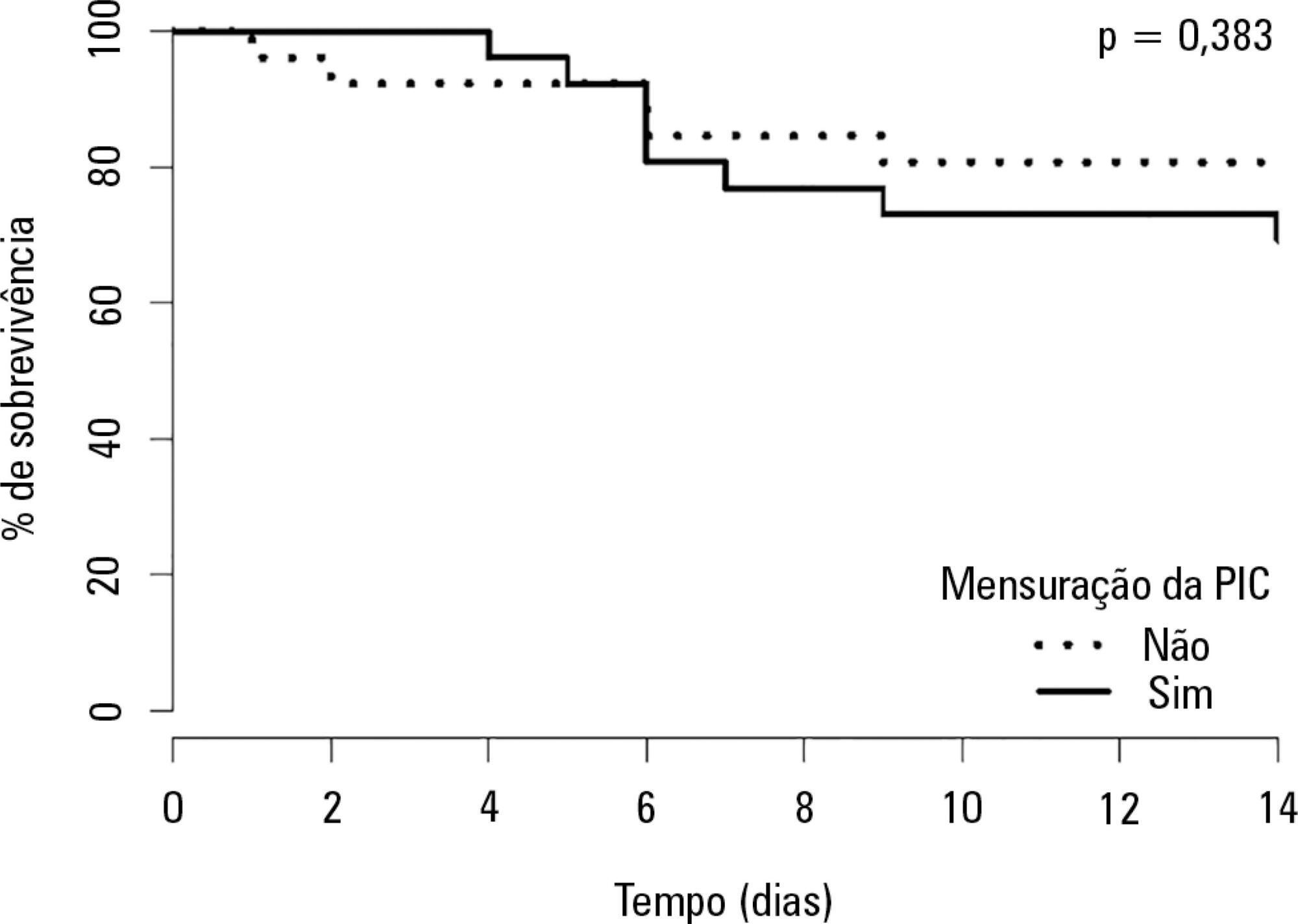
Global mortality at 14 days (16%) was equal to that observed in high-income countries in the CRASH Study and was better than expected based on the CRASH calculator score (20.6%), with a standardized mortality ratio of 0.77. A total of 28 patients received intracranial pressure monitoring (measured intracranial pressure group), of whom 26 were paired in a 1:1 fashion with patients from the non-measured intracranial pressure group. There was no improvement in the measured intracranial pressure group compared to the non-measured intracranial pressure group regarding hospital mortality, 14-day mortality, or combined hospital and chronic care facility mortality. Survival up to 14 days was also similar between groups.
Conclusion:
Patients receiving intracranial pressure monitoring tend to have more severe traumatic brain injuries. However, after adjusting for multiple confounders using propensity scoring, no benefits in terms of survival were observed among intracranial pressure-monitored patients and those managed with a systematic clinical protocol.
Views0Abstract
Original ArticleMeasurement of intracranial pressure and short-term outcomes of patients with traumatic brain injury: a propensity-matched analysis
Rev Bras Ter Intensiva. 2015;27(4):315-321
DOI 10.5935/0103-507X.20150055
Views0See moreABSTRACT
Objective:
To assess the impact of intracranial pressure monitoring on the short-term outcomes of traumatic brain injury patients.
Methods:
Retrospective observational study including 299 consecutive patients admitted due to traumatic brain injury from January 2011 through July 2012 at a Level 1 trauma center in São Paulo, Brazil. Patients were categorized in two groups according to the measurement of intracranial pressure (measured intracranial pressure and non-measured intracranial pressure groups). We applied a propensity-matched analysis to adjust for possible confounders (variables contained in the Crash Score prognostic algorithm).
Results:
Global mortality at 14 days (16%) was equal to that observed in high-income countries in the CRASH Study and was better than expected based on the CRASH calculator score (20.6%), with a standardized mortality ratio of 0.77. A total of 28 patients received intracranial pressure monitoring (measured intracranial pressure group), of whom 26 were paired in a 1:1 fashion with patients from the non-measured intracranial pressure group. There was no improvement in the measured intracranial pressure group compared to the non-measured intracranial pressure group regarding hospital mortality, 14-day mortality, or combined hospital and chronic care facility mortality. Survival up to 14 days was also similar between groups.
Conclusion:
Patients receiving intracranial pressure monitoring tend to have more severe traumatic brain injuries. However, after adjusting for multiple confounders using propensity scoring, no benefits in terms of survival were observed among intracranial pressure-monitored patients and those managed with a systematic clinical protocol.
-
Original Article
Therapeutic hypothermia after cardiac arrest: outcome predictors
Rev Bras Ter Intensiva. 2015;27(4):322-332
Abstract
Original ArticleTherapeutic hypothermia after cardiac arrest: outcome predictors
Rev Bras Ter Intensiva. 2015;27(4):322-332
DOI 10.5935/0103-507X.20150056
Views0ABSTRACT
Objective:
The determination of coma patient prognosis after cardiac arrest has clinical, ethical and social implications. Neurological examination, imaging and biochemical markers are helpful tools accepted as reliable in predicting recovery. With the advent of therapeutic hypothermia, these data need to be reconfirmed. In this study, we attempted to determine the validity of different markers, which can be used in the detection of patients with poor prognosis under hypothermia.
Methods:
Data from adult patients admitted to our intensive care unit for a hypothermia protocol after cardiac arrest were recorded prospectively to generate a descriptive and analytical study analyzing the relationship between clinical, neurophysiological, imaging and biochemical parameters with 6-month outcomes defined according to the Cerebral Performance Categories scale (good 1-2, poor 3-5). Neuron-specific enolase was collected at 72 hours. Imaging and neurophysiologic exams were carried out in the 24 hours after the rewarming period.
Results:
Sixty-seven patients were included in the study, of which 12 had good neurological outcomes. Ventricular fibrillation and electroencephalographic theta activity were associated with increased likelihood of survival and improved neurological outcomes. Patients who had more rapid cooling (mean time of 163 versus 312 minutes), hypoxic-ischemic brain injury on magnetic resonance imaging or neuron-specific enolase > 58ng/mL had poor neurological outcomes (p < 0.05).
Conclusion:
Hypoxic-ischemic brain injury on magnetic resonance imaging and neuron-specific enolase were strong predictors of poor neurological outcomes. Although there is the belief that early achievement of target temperature improves neurological prognoses, in our study, there were increased mortality and worse neurological outcomes with earlier target-temperature achievement.
Keywords:Cardiopulmonary ResuscitationHeart arrestHypothermia inducedHypoxia-ischemia, brainneuron-specific enolaseSee moreViews0Abstract
Original ArticleTherapeutic hypothermia after cardiac arrest: outcome predictors
Rev Bras Ter Intensiva. 2015;27(4):322-332
DOI 10.5935/0103-507X.20150056
Views0ABSTRACT
Objective:
The determination of coma patient prognosis after cardiac arrest has clinical, ethical and social implications. Neurological examination, imaging and biochemical markers are helpful tools accepted as reliable in predicting recovery. With the advent of therapeutic hypothermia, these data need to be reconfirmed. In this study, we attempted to determine the validity of different markers, which can be used in the detection of patients with poor prognosis under hypothermia.
Methods:
Data from adult patients admitted to our intensive care unit for a hypothermia protocol after cardiac arrest were recorded prospectively to generate a descriptive and analytical study analyzing the relationship between clinical, neurophysiological, imaging and biochemical parameters with 6-month outcomes defined according to the Cerebral Performance Categories scale (good 1-2, poor 3-5). Neuron-specific enolase was collected at 72 hours. Imaging and neurophysiologic exams were carried out in the 24 hours after the rewarming period.
Results:
Sixty-seven patients were included in the study, of which 12 had good neurological outcomes. Ventricular fibrillation and electroencephalographic theta activity were associated with increased likelihood of survival and improved neurological outcomes. Patients who had more rapid cooling (mean time of 163 versus 312 minutes), hypoxic-ischemic brain injury on magnetic resonance imaging or neuron-specific enolase > 58ng/mL had poor neurological outcomes (p < 0.05).
Conclusion:
Hypoxic-ischemic brain injury on magnetic resonance imaging and neuron-specific enolase were strong predictors of poor neurological outcomes. Although there is the belief that early achievement of target temperature improves neurological prognoses, in our study, there were increased mortality and worse neurological outcomes with earlier target-temperature achievement.
Keywords:Cardiopulmonary ResuscitationHeart arrestHypothermia inducedHypoxia-ischemia, brainneuron-specific enolaseSee more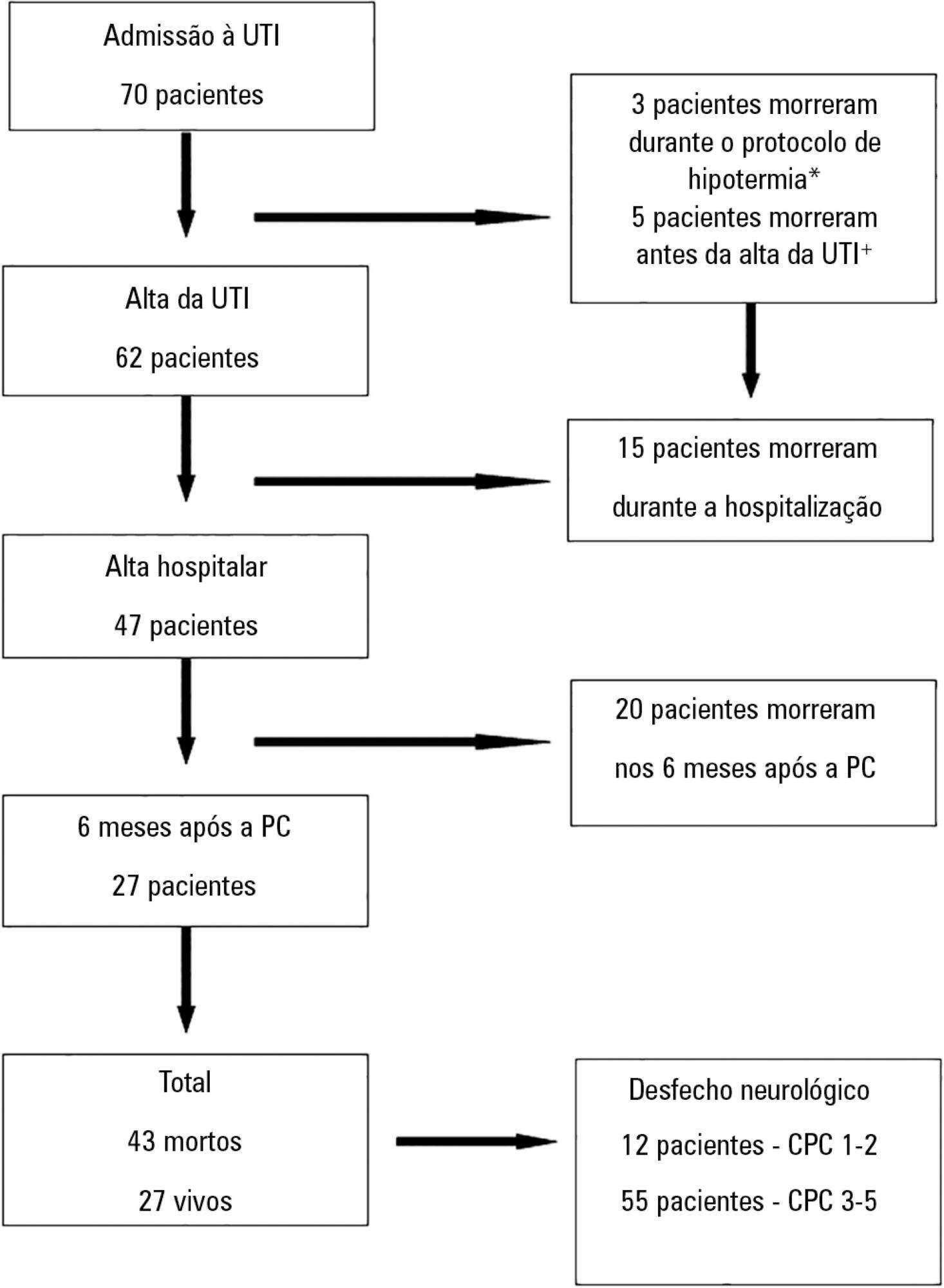
-
Original Article
Prognostic value of ventricular diastolic dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):333-339
Abstract
Original ArticlePrognostic value of ventricular diastolic dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):333-339
DOI 10.5935/0103-507X.20150057
Views0See moreABSTRACT
Objectives:
To evaluate the prevalence of myocardial dysfunction and its prognostic value in patients with severe sepsis and septic shock.
Methods:
Adult septic patients admitted to an intensive care unit were prospectively studied using transthoracic echocardiography within the first 48 hours after admission and thereafter on the 7th-10th days. Echocardiographic variables of biventricular function, including the E/e’ ratio, were compared between survivors and non-survivors.
Results:
A total of 99 echocardiograms (53 at admission and 46 between days 7 – 10) were performed on 53 patients with a mean age of 74 (SD 13) years. Systolic and diastolic dysfunction was present in 14 (26%) and 42 (83%) patients, respectively, and both types of dysfunction were present in 12 (23%) patients. The E/e’ ratio, an index of diastolic dysfunction, was the best predictor of hospital mortality according to the area under the ROC curve (0.71) and was an independent predictor of outcome, as determined by multivariate analysis (OR = 1.36 [1.05 – 1.76], p = 0.02).
Conclusion:
In septic patients admitted to an intensive care unit, echocardiographic systolic dysfunction is not associated with increased mortality. In contrast, diastolic dysfunction is an independent predictor of outcome.
Views0Abstract
Original ArticlePrognostic value of ventricular diastolic dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):333-339
DOI 10.5935/0103-507X.20150057
Views0See moreABSTRACT
Objectives:
To evaluate the prevalence of myocardial dysfunction and its prognostic value in patients with severe sepsis and septic shock.
Methods:
Adult septic patients admitted to an intensive care unit were prospectively studied using transthoracic echocardiography within the first 48 hours after admission and thereafter on the 7th-10th days. Echocardiographic variables of biventricular function, including the E/e’ ratio, were compared between survivors and non-survivors.
Results:
A total of 99 echocardiograms (53 at admission and 46 between days 7 – 10) were performed on 53 patients with a mean age of 74 (SD 13) years. Systolic and diastolic dysfunction was present in 14 (26%) and 42 (83%) patients, respectively, and both types of dysfunction were present in 12 (23%) patients. The E/e’ ratio, an index of diastolic dysfunction, was the best predictor of hospital mortality according to the area under the ROC curve (0.71) and was an independent predictor of outcome, as determined by multivariate analysis (OR = 1.36 [1.05 – 1.76], p = 0.02).
Conclusion:
In septic patients admitted to an intensive care unit, echocardiographic systolic dysfunction is not associated with increased mortality. In contrast, diastolic dysfunction is an independent predictor of outcome.
-
Original Article
Is venous blood drawn from femoral access adequate to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients?
Rev Bras Ter Intensiva. 2015;27(4):340-346
Abstract
Original ArticleIs venous blood drawn from femoral access adequate to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients?
Rev Bras Ter Intensiva. 2015;27(4):340-346
DOI 10.5935/0103-507X.20150058
Views0ABSTRACT
Objectives:
The purpose of this study was to test if venous blood drawn from femoral access can be used to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients.
Methods:
Bland-Altman analysis and Spearman correlations were used to compare the femoral venous oxygen saturation and central venous oxygen saturation as well as arterial lactate levels and femoral lactate. A pre-specified subgroup analysis was conducted in patients with signs of hypoperfusion. In addition, the clinical agreement was also investigated.
Results:
Blood samples were obtained in 26 patients. In 107 paired samples, there was a moderate correlation (r = 0.686, p < 0.0001) between the central venous oxygen saturation and femoral venous oxygen saturation with a bias of 8.24 ± 10.44 (95% limits of agreement: -12.23 to 28.70). In 102 paired samples, there was a strong correlation between the arterial lactate levels and femoral lactate levels (r = 0.972, p < 0.001) with a bias of -2.71 ± 9.86 (95% limits of agreement: -22.03 to 16.61). The presence of hypoperfusion did not significantly change these results. The clinical agreement for venous saturation was inadequate, with different therapeutic decisions in 22.4% of the situation; for lactate, this was the case only in 5.2% of the situations.
Conclusion:
Femoral venous oxygen saturation should not be used as a surrogate of central venous oxygen saturation. However, femoral lactate levels can be used in clinical practice, albeit with caution.
Keywords:Central venous pressure/physiologyFemoral vein/physiologyLactatesOxygen consumption/physiologySee moreViews0Abstract
Original ArticleIs venous blood drawn from femoral access adequate to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients?
Rev Bras Ter Intensiva. 2015;27(4):340-346
DOI 10.5935/0103-507X.20150058
Views0ABSTRACT
Objectives:
The purpose of this study was to test if venous blood drawn from femoral access can be used to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients.
Methods:
Bland-Altman analysis and Spearman correlations were used to compare the femoral venous oxygen saturation and central venous oxygen saturation as well as arterial lactate levels and femoral lactate. A pre-specified subgroup analysis was conducted in patients with signs of hypoperfusion. In addition, the clinical agreement was also investigated.
Results:
Blood samples were obtained in 26 patients. In 107 paired samples, there was a moderate correlation (r = 0.686, p < 0.0001) between the central venous oxygen saturation and femoral venous oxygen saturation with a bias of 8.24 ± 10.44 (95% limits of agreement: -12.23 to 28.70). In 102 paired samples, there was a strong correlation between the arterial lactate levels and femoral lactate levels (r = 0.972, p < 0.001) with a bias of -2.71 ± 9.86 (95% limits of agreement: -22.03 to 16.61). The presence of hypoperfusion did not significantly change these results. The clinical agreement for venous saturation was inadequate, with different therapeutic decisions in 22.4% of the situation; for lactate, this was the case only in 5.2% of the situations.
Conclusion:
Femoral venous oxygen saturation should not be used as a surrogate of central venous oxygen saturation. However, femoral lactate levels can be used in clinical practice, albeit with caution.
Keywords:Central venous pressure/physiologyFemoral vein/physiologyLactatesOxygen consumption/physiologySee more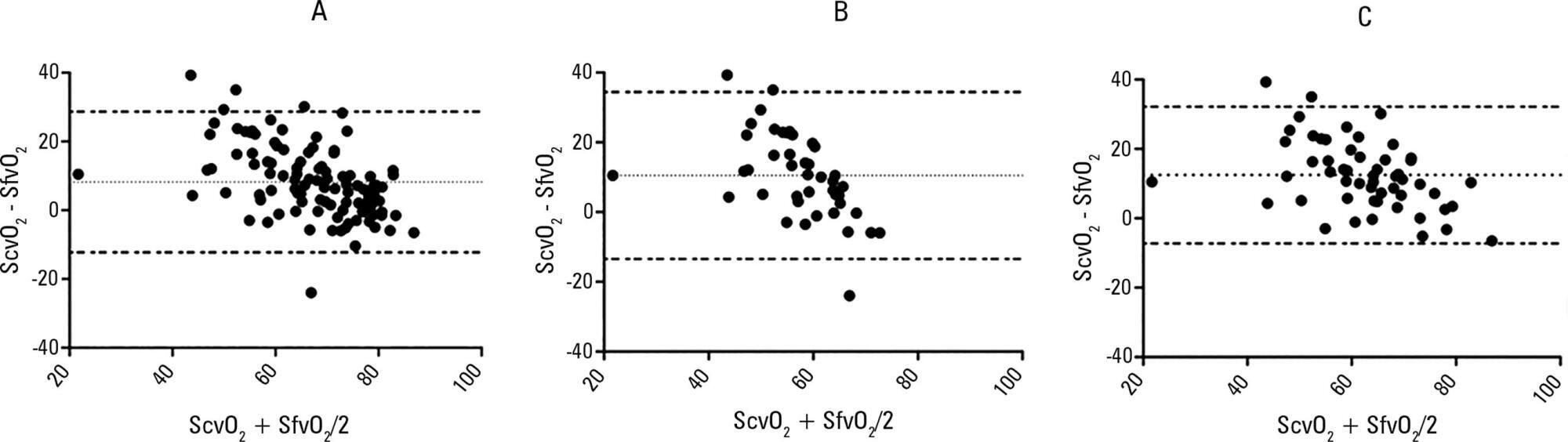
-
Original Article
Influence of different degrees of head elevation on respiratory mechanics in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(4):347-352
Abstract
Original ArticleInfluence of different degrees of head elevation on respiratory mechanics in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(4):347-352
DOI 10.5935/0103-507X.20150059
Views0See moreRESUMO
Objective:
The positioning of a patient in bed may directly affect their respiratory mechanics. The objective of this study was to evaluate the respiratory mechanics of mechanically ventilated patients positioned with different head angles hospitalized in an intensive care unit.
Methods:
This was a prospective physiological study in which static and dynamic compliance, resistive airway pressure, and peripheral oxygen saturation were measured with the head at four different positions (0° = P1, 30° = P2, 45° = P3, and 60° = P4). Repeated-measures analysis of variance (ANOVA) with a Bonferroni post-test and Friedman analysis were used to compare the values obtained at the different positions.
Results:
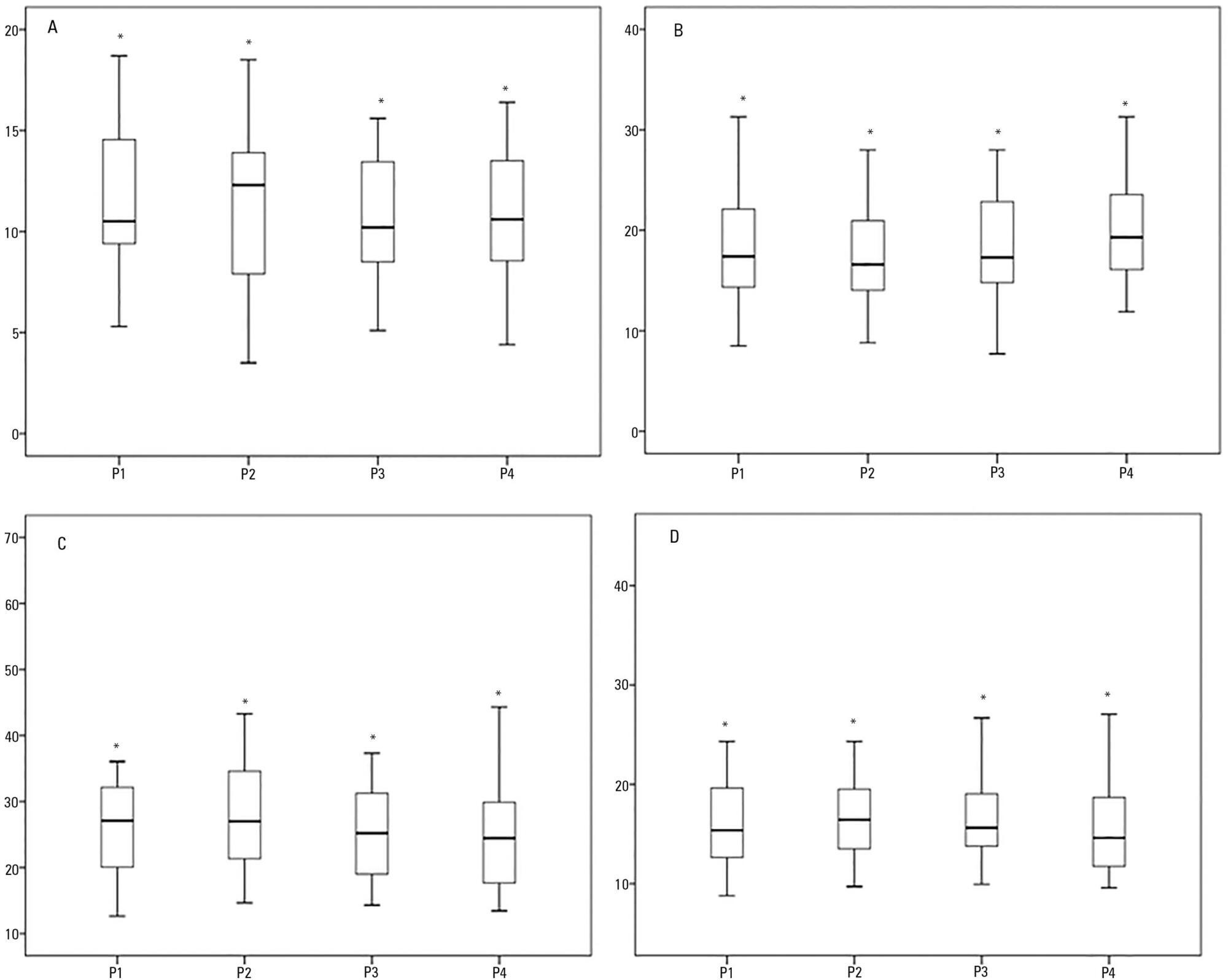
A comparison of the 35 evaluated patients revealed that the resistive airway pressure values in the 0° position were higher than those obtained when patients were positioned at greater angles. The elastic pressure analysis revealed that the 60° position produced the highest value relative to the other positions. Regarding static compliance, a reduction in values was observed from the 0° position to the 60° position. The dynamic compliance analysis revealed that the 30° angle produced the greatest value compared to the other positions. The peripheral oxygen saturation showed little variation, with the highest value obtained at the 0° position.
Conclusion:
The highest dynamic compliance value was observed at the 30° position, and the highest oxygenation value was observed at the 0° position.
Views0Abstract
Original ArticleInfluence of different degrees of head elevation on respiratory mechanics in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(4):347-352
DOI 10.5935/0103-507X.20150059
Views0See moreRESUMO
Objective:
The positioning of a patient in bed may directly affect their respiratory mechanics. The objective of this study was to evaluate the respiratory mechanics of mechanically ventilated patients positioned with different head angles hospitalized in an intensive care unit.
Methods:
This was a prospective physiological study in which static and dynamic compliance, resistive airway pressure, and peripheral oxygen saturation were measured with the head at four different positions (0° = P1, 30° = P2, 45° = P3, and 60° = P4). Repeated-measures analysis of variance (ANOVA) with a Bonferroni post-test and Friedman analysis were used to compare the values obtained at the different positions.
Results:
A comparison of the 35 evaluated patients revealed that the resistive airway pressure values in the 0° position were higher than those obtained when patients were positioned at greater angles. The elastic pressure analysis revealed that the 60° position produced the highest value relative to the other positions. Regarding static compliance, a reduction in values was observed from the 0° position to the 60° position. The dynamic compliance analysis revealed that the 30° angle produced the greatest value compared to the other positions. The peripheral oxygen saturation showed little variation, with the highest value obtained at the 0° position.
Conclusion:
The highest dynamic compliance value was observed at the 30° position, and the highest oxygenation value was observed at the 0° position.
-
Original Article
Adverse events caused by potential drug-drug interactions in an intensive care unit of a teaching hospital
Rev Bras Ter Intensiva. 2015;27(4):353-359
Abstract
Original ArticleAdverse events caused by potential drug-drug interactions in an intensive care unit of a teaching hospital
Rev Bras Ter Intensiva. 2015;27(4):353-359
DOI 10.5935/0103-507X.20150060
Views0ABSTRACT
Objective:
To evaluate the incidence of potential drug-drug interactions in an intensive care unit of a hospital, focusing on antimicrobial drugs.
Methods:
This cross-sectional study analyzed electronic prescriptions of patients admitted to the intensive care unit of a teaching hospital between January 1 and March 31, 2014 and assessed potential drug-drug interactions associated with antimicrobial drugs. Antimicrobial drug consumption levels were expressed in daily doses per 100 patient-days. The search and classification of the interactions were based on the Micromedex® system.
Results:
The daily prescriptions of 82 patients were analyzed, totaling 656 prescriptions. Antimicrobial drugs represented 25% of all prescription drugs, with meropenem, vancomycin and ceftriaxone being the most prescribed medications. According to the approach of daily dose per 100 patient-days, the most commonly used antimicrobial drugs were cefepime, meropenem, sulfamethoxazole + trimethoprim and ciprofloxacin. The mean number of interactions per patient was 2.6. Among the interactions, 51% were classified as contraindicated or significantly severe. Highly significant interactions (clinical value 1 and 2) were observed with a prevalence of 98%.
Conclusion:
The current study demonstrated that antimicrobial drugs are frequently prescribed in intensive care units and present a very high number of potential drug-drug interactions, with most of them being considered highly significant.
Keywords:Anti-infective agentsDrug interactionsDrug utilizationDrug-related side effects and adverse reactionsHospital, teachingIntensive carePharmaceutical preparationsSee moreViews0Abstract
Original ArticleAdverse events caused by potential drug-drug interactions in an intensive care unit of a teaching hospital
Rev Bras Ter Intensiva. 2015;27(4):353-359
DOI 10.5935/0103-507X.20150060
Views0ABSTRACT
Objective:
To evaluate the incidence of potential drug-drug interactions in an intensive care unit of a hospital, focusing on antimicrobial drugs.
Methods:
This cross-sectional study analyzed electronic prescriptions of patients admitted to the intensive care unit of a teaching hospital between January 1 and March 31, 2014 and assessed potential drug-drug interactions associated with antimicrobial drugs. Antimicrobial drug consumption levels were expressed in daily doses per 100 patient-days. The search and classification of the interactions were based on the Micromedex® system.
Results:
The daily prescriptions of 82 patients were analyzed, totaling 656 prescriptions. Antimicrobial drugs represented 25% of all prescription drugs, with meropenem, vancomycin and ceftriaxone being the most prescribed medications. According to the approach of daily dose per 100 patient-days, the most commonly used antimicrobial drugs were cefepime, meropenem, sulfamethoxazole + trimethoprim and ciprofloxacin. The mean number of interactions per patient was 2.6. Among the interactions, 51% were classified as contraindicated or significantly severe. Highly significant interactions (clinical value 1 and 2) were observed with a prevalence of 98%.
Conclusion:
The current study demonstrated that antimicrobial drugs are frequently prescribed in intensive care units and present a very high number of potential drug-drug interactions, with most of them being considered highly significant.
Keywords:Anti-infective agentsDrug interactionsDrug utilizationDrug-related side effects and adverse reactionsHospital, teachingIntensive carePharmaceutical preparationsSee more -
Original Article
Delirium in intensive care unit patients under noninvasive ventilation: a multinational survey
Rev Bras Ter Intensiva. 2015;27(4):360-368
Abstract
Original ArticleDelirium in intensive care unit patients under noninvasive ventilation: a multinational survey
Rev Bras Ter Intensiva. 2015;27(4):360-368
DOI 10.5935/0103-507X.20150061
Views0ABSTRACT
Objective:
To conduct a multinational survey of intensive care unit professionals to determine the practices on delirium assessment and management, in addition to their perceptions and attitudes toward the evaluation and impact of delirium in patients requiring noninvasive ventilation.
Methods:
An electronic questionnaire was created to evaluate the profiles of the respondents and their related intensive care units, the systematic delirium assessment and management and the respondents’ perceptions and attitudes regarding delirium in patients requiring noninvasive ventilation. The questionnaire was distributed to the cooperative network for research of the Associação de Medicina Intensiva Brasileira (AMIB-Net) mailing list and to researchers in different centers in Latin America and Europe.
Results:
Four hundred thirty-six questionnaires were available for analysis; the majority of the questionnaires were from Brazil (61.9%), followed by Turkey (8.7%) and Italy (4.8%). Approximately 61% of the respondents reported no delirium assessment in the intensive care unit, and 31% evaluated delirium in patients under noninvasive ventilation. The Confusion Assessment Method for the intensive care unit was the most reported validated diagnostic tool (66.9%). Concerning the indication of noninvasive ventilation in patients already presenting with delirium, 16.3% of respondents never allow the use of noninvasive ventilation in this clinical context.
Conclusion:
This survey provides data that strongly reemphasizes poor efforts toward delirium assessment and management in the intensive care unit setting, especially regarding patients requiring noninvasive ventilation.
Keywords:Attitude of health personnelCritical careDeliriumDiagnostic techniques, neurologicalNoninvasive ventilationQuestionnairesSee moreViews0Abstract
Original ArticleDelirium in intensive care unit patients under noninvasive ventilation: a multinational survey
Rev Bras Ter Intensiva. 2015;27(4):360-368
DOI 10.5935/0103-507X.20150061
Views0ABSTRACT
Objective:
To conduct a multinational survey of intensive care unit professionals to determine the practices on delirium assessment and management, in addition to their perceptions and attitudes toward the evaluation and impact of delirium in patients requiring noninvasive ventilation.
Methods:
An electronic questionnaire was created to evaluate the profiles of the respondents and their related intensive care units, the systematic delirium assessment and management and the respondents’ perceptions and attitudes regarding delirium in patients requiring noninvasive ventilation. The questionnaire was distributed to the cooperative network for research of the Associação de Medicina Intensiva Brasileira (AMIB-Net) mailing list and to researchers in different centers in Latin America and Europe.
Results:
Four hundred thirty-six questionnaires were available for analysis; the majority of the questionnaires were from Brazil (61.9%), followed by Turkey (8.7%) and Italy (4.8%). Approximately 61% of the respondents reported no delirium assessment in the intensive care unit, and 31% evaluated delirium in patients under noninvasive ventilation. The Confusion Assessment Method for the intensive care unit was the most reported validated diagnostic tool (66.9%). Concerning the indication of noninvasive ventilation in patients already presenting with delirium, 16.3% of respondents never allow the use of noninvasive ventilation in this clinical context.
Conclusion:
This survey provides data that strongly reemphasizes poor efforts toward delirium assessment and management in the intensive care unit setting, especially regarding patients requiring noninvasive ventilation.
Keywords:Attitude of health personnelCritical careDeliriumDiagnostic techniques, neurologicalNoninvasive ventilationQuestionnairesSee more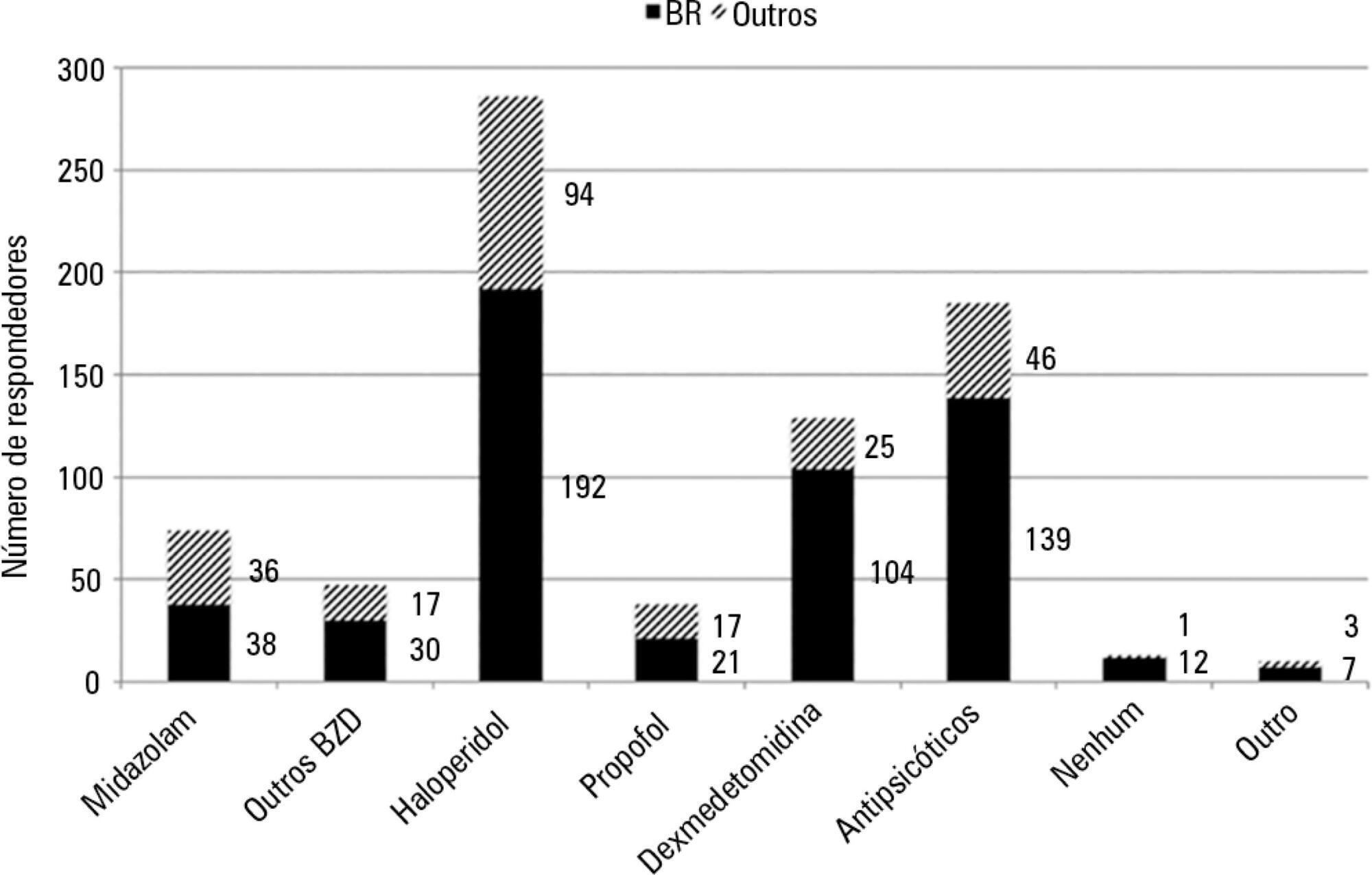
-
Original Article
Relationship between adductor pollicis muscle thickness and subjective global assessment in a cardiac intensive care unit
Rev Bras Ter Intensiva. 2015;27(4):369-375
Abstract
Original ArticleRelationship between adductor pollicis muscle thickness and subjective global assessment in a cardiac intensive care unit
Rev Bras Ter Intensiva. 2015;27(4):369-375
DOI 10.5935/0103-507X.20150062
Views0See moreABSTRACT
Objective:
To verify the relationship between the adductor pollicis muscle thickness test and the subjective global assessment and to correlate it with other anthropometric methods.
Methods:
This observational cross-sectional study was conducted in the intensive care unit of a cardiology hospital in the state of Rio Grande do Sul, Brazil. The hospitalized patients underwent subjective global assessment and adductor pollicis muscle thickness tests on both hands, along with measurement of the right calf circumference. Laboratory parameters, length of stay, vital signs and electronic medical record data and tests were all collected.
Results:
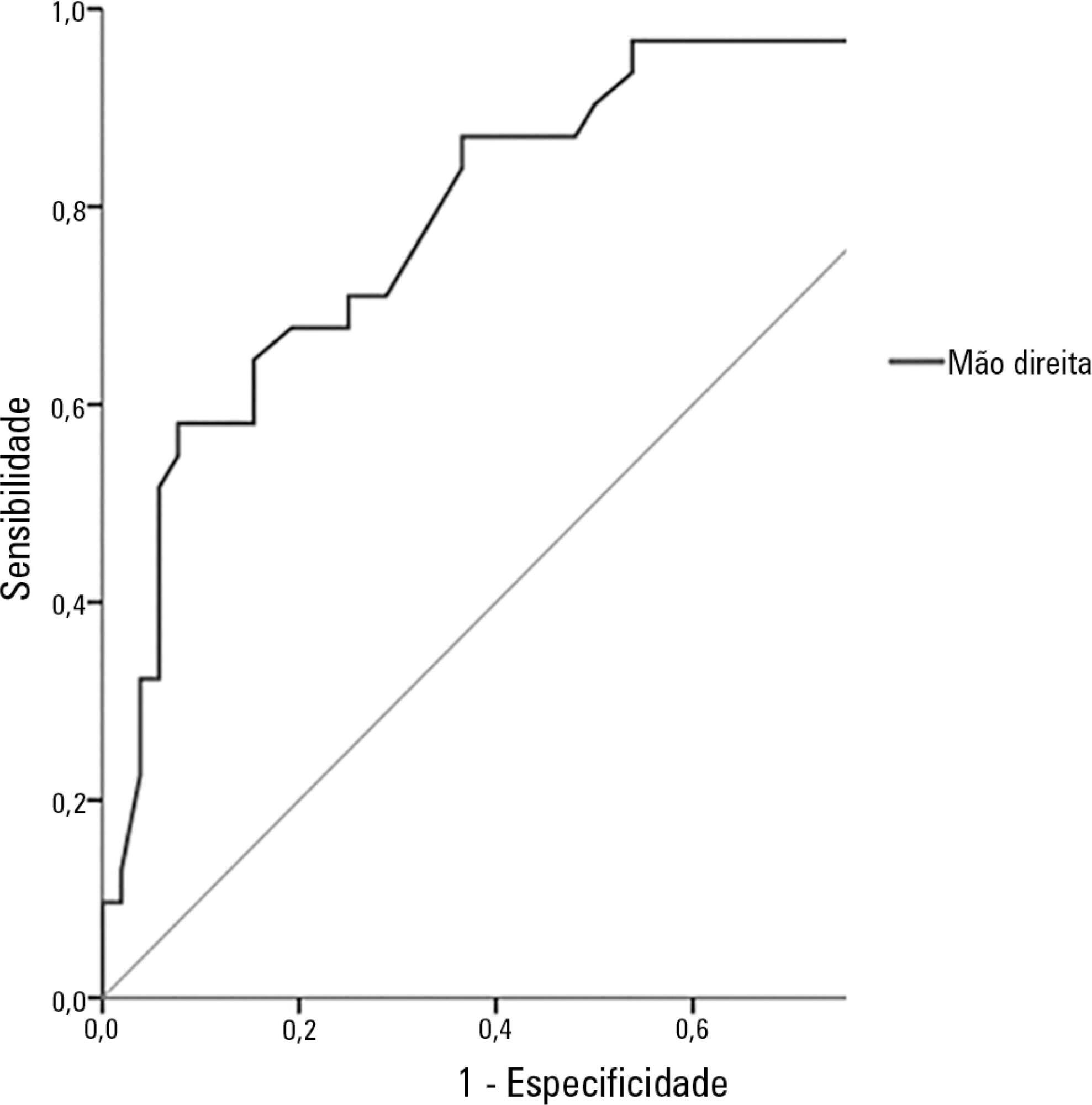
The study population included 83 patients, of whom 62% were men. The average age was 68.6 ± 12.5 years. The most common reason for hospitalization was acute myocardial infarction (34.9%), and the most common pathology was systolic blood pressure (63.9%), followed by diabetes mellitus (28.9%). According to subjective global assessment classifications, 62.7% of patients presented no nutritional risk, 20.5% were moderately malnourished and 16.9% were severely malnourished. Women had a higher nutritional risk, according to both the subjective global assessment and the adductor pollicis muscle thickness test, the cutoff for which was < 6.5mm (54.8%; p = 0.001). The pathology presenting the greatest nutritional risk was congestive heart failure (p = 0.001). Evaluation of the receiver operating characteristic (ROC) curve between adductor pollicis muscle thickness and subjective global assessment showed the accuracy of the former, with an area of 0.822.
Conclusion:
Adductor pollicis muscle thickness proved to be a good method for evaluating nutritional risk.
Views0Abstract
Original ArticleRelationship between adductor pollicis muscle thickness and subjective global assessment in a cardiac intensive care unit
Rev Bras Ter Intensiva. 2015;27(4):369-375
DOI 10.5935/0103-507X.20150062
Views0See moreABSTRACT
Objective:
To verify the relationship between the adductor pollicis muscle thickness test and the subjective global assessment and to correlate it with other anthropometric methods.
Methods:
This observational cross-sectional study was conducted in the intensive care unit of a cardiology hospital in the state of Rio Grande do Sul, Brazil. The hospitalized patients underwent subjective global assessment and adductor pollicis muscle thickness tests on both hands, along with measurement of the right calf circumference. Laboratory parameters, length of stay, vital signs and electronic medical record data and tests were all collected.
Results:
The study population included 83 patients, of whom 62% were men. The average age was 68.6 ± 12.5 years. The most common reason for hospitalization was acute myocardial infarction (34.9%), and the most common pathology was systolic blood pressure (63.9%), followed by diabetes mellitus (28.9%). According to subjective global assessment classifications, 62.7% of patients presented no nutritional risk, 20.5% were moderately malnourished and 16.9% were severely malnourished. Women had a higher nutritional risk, according to both the subjective global assessment and the adductor pollicis muscle thickness test, the cutoff for which was < 6.5mm (54.8%; p = 0.001). The pathology presenting the greatest nutritional risk was congestive heart failure (p = 0.001). Evaluation of the receiver operating characteristic (ROC) curve between adductor pollicis muscle thickness and subjective global assessment showed the accuracy of the former, with an area of 0.822.
Conclusion:
Adductor pollicis muscle thickness proved to be a good method for evaluating nutritional risk.
-
Original Article
Serum concentrations of vitamin D and organ dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):376-382
Abstract
Original ArticleSerum concentrations of vitamin D and organ dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):376-382
DOI 10.5935/0103-507X.20150063
Views0See moreABSTRACT
Objectives:
To evaluate the serum concentrations of vitamin D and their variations in patients with severe sepsis or septic shock and in control subjects upon admission and after 7 days of hospitalization in the intensive care unit and to correlate these concentrations with the severity of organ dysfunction.
Methods:
This case-control, prospective, observational study involved patients aged > 18 years with severe sepsis or septic shock paired with a control group. Serum vitamin D concentrations were measured at inclusion (D0) and on the seventh day after inclusion (D7). Severe deficiency was defined as vitamin D levels < 10ng/ml, deficiency as levels between 10 and 20ng/ml, insufficiency as levels between 20 and 30ng/ml, and sufficiency as levels ≥ 30ng/mL. We considered a change to a higher ranking, together with a 50% increase in the absolute concentration, to represent an improvement.
Results:
We included 51 patients (26 with septic shock and 25 controls). The prevalence of vitamin D concentration ≤ 30ng/ml was 98%. There was no correlation between the serum concentration of vitamin D at D0 and the SOFA score at D0 or D7 either in the general population or in the group with septic shock. Patients with improvement in vitamin D deficiency had an improved SOFA score at D7 (p = 0.013).
Conclusion:
In the population studied, patients with septic shock showed improvement in the serum concentrations of vitamin D on the seventh day compared with the controls. We also found a correlation between higher vitamin D concentrations and a greater decrease in the severity of organ dysfunction.
Views0Abstract
Original ArticleSerum concentrations of vitamin D and organ dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):376-382
DOI 10.5935/0103-507X.20150063
Views0See moreABSTRACT
Objectives:
To evaluate the serum concentrations of vitamin D and their variations in patients with severe sepsis or septic shock and in control subjects upon admission and after 7 days of hospitalization in the intensive care unit and to correlate these concentrations with the severity of organ dysfunction.
Methods:
This case-control, prospective, observational study involved patients aged > 18 years with severe sepsis or septic shock paired with a control group. Serum vitamin D concentrations were measured at inclusion (D0) and on the seventh day after inclusion (D7). Severe deficiency was defined as vitamin D levels < 10ng/ml, deficiency as levels between 10 and 20ng/ml, insufficiency as levels between 20 and 30ng/ml, and sufficiency as levels ≥ 30ng/mL. We considered a change to a higher ranking, together with a 50% increase in the absolute concentration, to represent an improvement.
Results:
We included 51 patients (26 with septic shock and 25 controls). The prevalence of vitamin D concentration ≤ 30ng/ml was 98%. There was no correlation between the serum concentration of vitamin D at D0 and the SOFA score at D0 or D7 either in the general population or in the group with septic shock. Patients with improvement in vitamin D deficiency had an improved SOFA score at D7 (p = 0.013).
Conclusion:
In the population studied, patients with septic shock showed improvement in the serum concentrations of vitamin D on the seventh day compared with the controls. We also found a correlation between higher vitamin D concentrations and a greater decrease in the severity of organ dysfunction.
-
Original Article
Evaluation of the role of the cannabidiol system in an animal model of ischemia/reperfusion kidney injury
Rev Bras Ter Intensiva. 2015;27(4):383-389
Abstract
Original ArticleEvaluation of the role of the cannabidiol system in an animal model of ischemia/reperfusion kidney injury
Rev Bras Ter Intensiva. 2015;27(4):383-389
DOI 10.5935/0103-507X.20150064
Views0ABSTRACT
Objective:
This work aimed to investigate the effects of the administration of cannabidiol in a kidney ischemia/reperfusion animal model.
Methods:
Kidney injury was induced by 45 minutes of renal ischemia followed by reperfusion. Cannabidiol (5mg/kg) was administered immediately after reperfusion.
Results:
Ischemia/reperfusion increased the IL-1 and TNF levels, and these levels were attenuated by cannabidiol treatment. Additionally, cannabidiol was able to decrease lipid and protein oxidative damage, but not the nitrite/nitrate levels. Kidney injury after ischemia/reperfusion seemed to be independent of the cannabidiol receptor 1 and cannabidiol receptor 2 (CB1 and CB2) expression levels, as there was no significant increase in these receptors after reperfusion.
Conclusion:
The cannabidiol treatment had a protective effect against inflammation and oxidative damage in the kidney ischemia/reperfusion model. These effects seemed to be independent of CB1/CB2 receptor activation.
Keywords:Cannabidiol/therapeutic useinflammationIschemia/metabolismKidney/injuriesReceptors, cannabinoidReperfusion injury/metabolismSee moreViews0Abstract
Original ArticleEvaluation of the role of the cannabidiol system in an animal model of ischemia/reperfusion kidney injury
Rev Bras Ter Intensiva. 2015;27(4):383-389
DOI 10.5935/0103-507X.20150064
Views0ABSTRACT
Objective:
This work aimed to investigate the effects of the administration of cannabidiol in a kidney ischemia/reperfusion animal model.
Methods:
Kidney injury was induced by 45 minutes of renal ischemia followed by reperfusion. Cannabidiol (5mg/kg) was administered immediately after reperfusion.
Results:
Ischemia/reperfusion increased the IL-1 and TNF levels, and these levels were attenuated by cannabidiol treatment. Additionally, cannabidiol was able to decrease lipid and protein oxidative damage, but not the nitrite/nitrate levels. Kidney injury after ischemia/reperfusion seemed to be independent of the cannabidiol receptor 1 and cannabidiol receptor 2 (CB1 and CB2) expression levels, as there was no significant increase in these receptors after reperfusion.
Conclusion:
The cannabidiol treatment had a protective effect against inflammation and oxidative damage in the kidney ischemia/reperfusion model. These effects seemed to be independent of CB1/CB2 receptor activation.
Keywords:Cannabidiol/therapeutic useinflammationIschemia/metabolismKidney/injuriesReceptors, cannabinoidReperfusion injury/metabolismSee more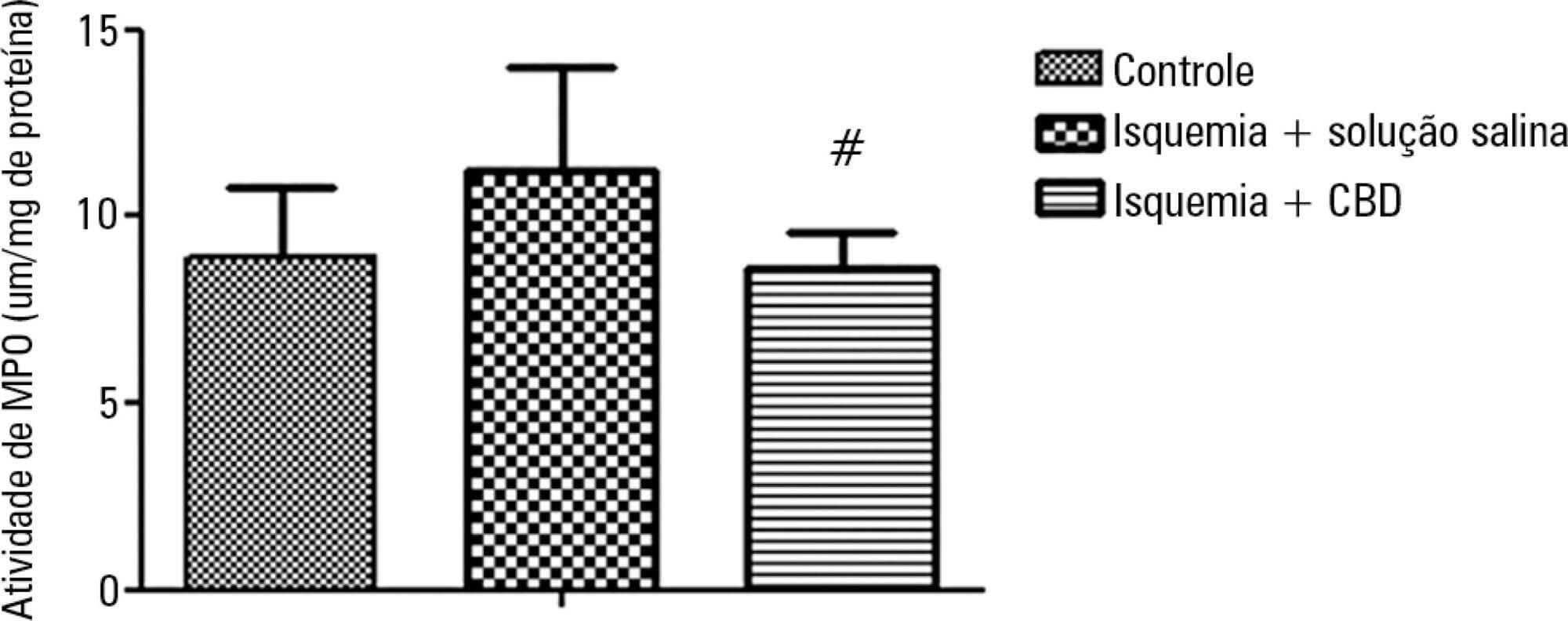
-
Review Article
Noninvasive ventilation in status asthmaticus in children: levels of evidence
Rev Bras Ter Intensiva. 2015;27(4):390-396
Abstract
Review ArticleNoninvasive ventilation in status asthmaticus in children: levels of evidence
Rev Bras Ter Intensiva. 2015;27(4):390-396
DOI 10.5935/0103-507X.20150065
Views0ABSTRACT
Objective:
To evaluate the quality of available evidence to establish guidelines for the use of noninvasive ventilation for the management of status asthmaticus in children unresponsive to standard treatment.
Methods:
Search, selection and analysis of all original articles on asthma and noninvasive ventilation in children, published until September 1, 2014 in all languages in the electronic databases PubMed, Web of Science, Cochrane Library, Scopus and SciELO, located using the search terms: “asthma”, “status asthmaticus”, “noninvasive ventilation”, “Bronchospasm”, “continuous positive airway pressure”, “child”, “infant”, “pediatrics”, “hypercapnia”, “respiratory failure” and the keywords “BIPAP”, “CPAP”, “Bilevel”, “acute asthma” and “near fatal asthma”. The articles were assessed based on the levels of evidence of the GRADE system.
Results:
Only nine original articles were located; two (22%) articles had level of evidence A, one (11%) had level of evidence B and six (67%) had level of evidence C.
Conclusion:
The results suggest that noninvasive ventilation is applicable for the treatment of status asthmaticus in most pediatric patients unresponsive to standard treatment. However, the available evidence cannot be considered as conclusive, as further high-quality research is likely to have an impact on and change the estimate of the effect.
Keywords:asthmaBronchial spasmusChildHypercapniaNoninvasive ventilationRespiratory insufficiencyStatus asmathicusSee moreViews0Abstract
Review ArticleNoninvasive ventilation in status asthmaticus in children: levels of evidence
Rev Bras Ter Intensiva. 2015;27(4):390-396
DOI 10.5935/0103-507X.20150065
Views0ABSTRACT
Objective:
To evaluate the quality of available evidence to establish guidelines for the use of noninvasive ventilation for the management of status asthmaticus in children unresponsive to standard treatment.
Methods:
Search, selection and analysis of all original articles on asthma and noninvasive ventilation in children, published until September 1, 2014 in all languages in the electronic databases PubMed, Web of Science, Cochrane Library, Scopus and SciELO, located using the search terms: “asthma”, “status asthmaticus”, “noninvasive ventilation”, “Bronchospasm”, “continuous positive airway pressure”, “child”, “infant”, “pediatrics”, “hypercapnia”, “respiratory failure” and the keywords “BIPAP”, “CPAP”, “Bilevel”, “acute asthma” and “near fatal asthma”. The articles were assessed based on the levels of evidence of the GRADE system.
Results:
Only nine original articles were located; two (22%) articles had level of evidence A, one (11%) had level of evidence B and six (67%) had level of evidence C.
Conclusion:
The results suggest that noninvasive ventilation is applicable for the treatment of status asthmaticus in most pediatric patients unresponsive to standard treatment. However, the available evidence cannot be considered as conclusive, as further high-quality research is likely to have an impact on and change the estimate of the effect.
Keywords:asthmaBronchial spasmusChildHypercapniaNoninvasive ventilationRespiratory insufficiencyStatus asmathicusSee more -
Case Report
Use of venoarterial extracorporeal membrane oxygenation in fulminant chagasic myocarditis as a bridge to heart transplant
Rev Bras Ter Intensiva. 2015;27(4):397-401
Abstract
Case ReportUse of venoarterial extracorporeal membrane oxygenation in fulminant chagasic myocarditis as a bridge to heart transplant
Rev Bras Ter Intensiva. 2015;27(4):397-401
DOI 10.5935/0103-507X.20150066
Views0See moreABSTRACT
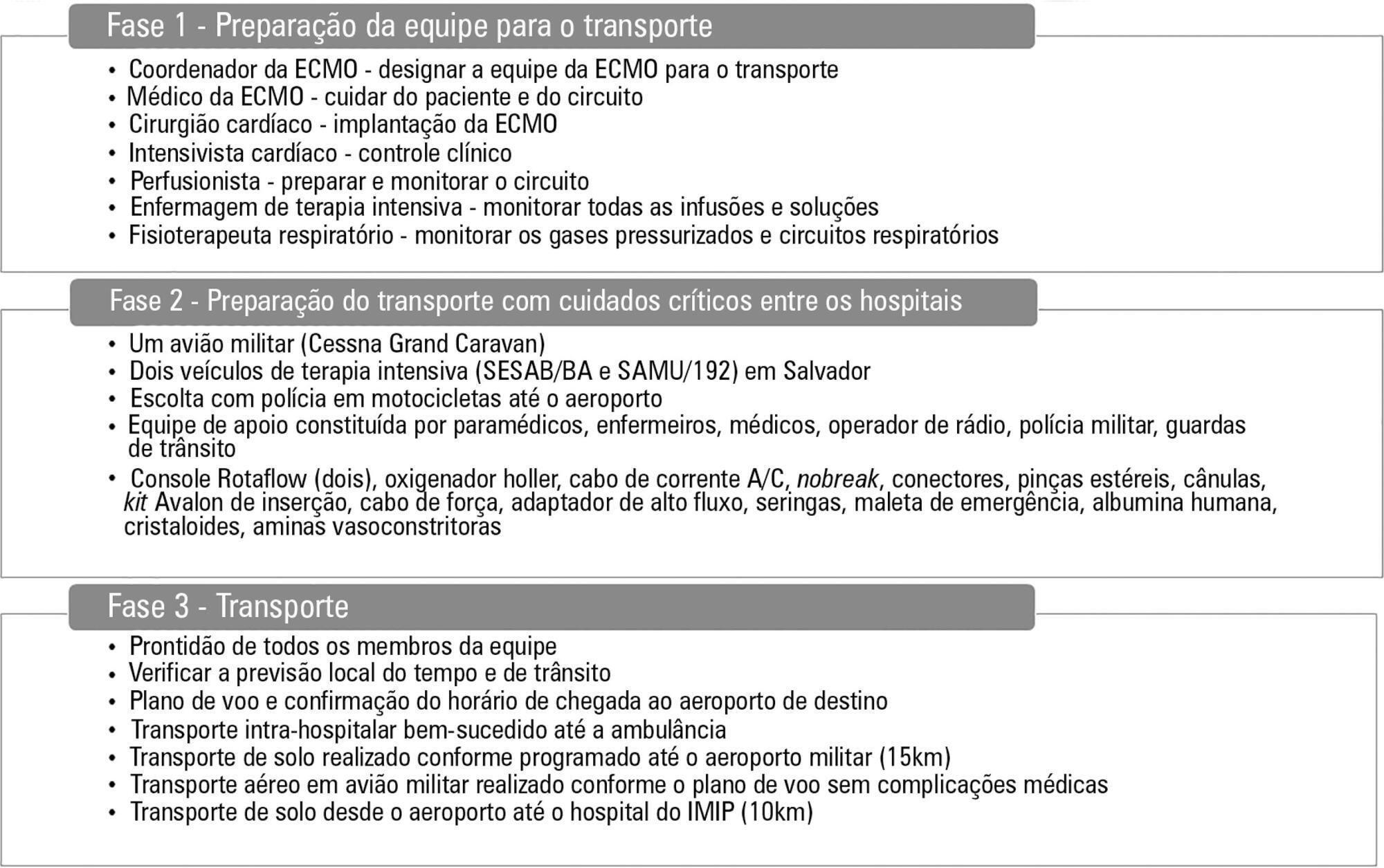
A 17-year-old Brazilian male presented with progressive dyspnea for 15 days, worsening in the last 24 hours, and was admitted in respiratory failure and cardiogenic shock, with multiple organ dysfunctions. Echocardiography showed a left ventricle ejection fraction of 11%, severe diffuse hypokinesia, and a systolic pulmonary artery pressure of 50mmHg, resulting in the need for hemodynamic support with dobutamine (20mcg/kg/min) and noradrenaline (1.7mcg/kg/min). After 48 hours with no clinical or hemodynamic improvement, an extracorporeal membrane oxygenation was implanted. The patient presented with hemodynamic, systemic perfusion and renal and liver function improvements; however, his cardiac function did not recover after 72 hours, and he was transfer to another hospital. Air transport was conducted from Salvador to Recife in Brazil. A heart transplant was performed with rapid recovery of both liver and kidney functions, as well as good graft function. Histopathology of the explanted heart showed chronic active myocarditis and amastigotes of Trypanosoma cruzi. The estimated global prevalence of T. cruzi infections declined from 18 million in 1991, when the first regional control initiative began, to 5.7 million in 2010. Myocarditis is an inflammatory disease due to infectious or non-infectious conditions. Clinical manifestation is variable, ranging from subclinical presentation to refractory heart failure and cardiogenic shock. Several reports suggest that the use of extracorporeal membrane oxygenation in patients presenting with severe refractory myocarditis is a potential bridging therapy to heart transplant when there is no spontaneous recovery of ventricular function. In a 6-month follow-up outpatient consult, the patient presented well and was asymptomatic.
Views0Abstract
Case ReportUse of venoarterial extracorporeal membrane oxygenation in fulminant chagasic myocarditis as a bridge to heart transplant
Rev Bras Ter Intensiva. 2015;27(4):397-401
DOI 10.5935/0103-507X.20150066
Views0See moreABSTRACT
A 17-year-old Brazilian male presented with progressive dyspnea for 15 days, worsening in the last 24 hours, and was admitted in respiratory failure and cardiogenic shock, with multiple organ dysfunctions. Echocardiography showed a left ventricle ejection fraction of 11%, severe diffuse hypokinesia, and a systolic pulmonary artery pressure of 50mmHg, resulting in the need for hemodynamic support with dobutamine (20mcg/kg/min) and noradrenaline (1.7mcg/kg/min). After 48 hours with no clinical or hemodynamic improvement, an extracorporeal membrane oxygenation was implanted. The patient presented with hemodynamic, systemic perfusion and renal and liver function improvements; however, his cardiac function did not recover after 72 hours, and he was transfer to another hospital. Air transport was conducted from Salvador to Recife in Brazil. A heart transplant was performed with rapid recovery of both liver and kidney functions, as well as good graft function. Histopathology of the explanted heart showed chronic active myocarditis and amastigotes of Trypanosoma cruzi. The estimated global prevalence of T. cruzi infections declined from 18 million in 1991, when the first regional control initiative began, to 5.7 million in 2010. Myocarditis is an inflammatory disease due to infectious or non-infectious conditions. Clinical manifestation is variable, ranging from subclinical presentation to refractory heart failure and cardiogenic shock. Several reports suggest that the use of extracorporeal membrane oxygenation in patients presenting with severe refractory myocarditis is a potential bridging therapy to heart transplant when there is no spontaneous recovery of ventricular function. In a 6-month follow-up outpatient consult, the patient presented well and was asymptomatic.
-
Case Report
Severe hypercalcemia as a form of acute lymphoblastic leukemia presentation in children
Rev Bras Ter Intensiva. 2015;27(4):402-405
Abstract
Case ReportSevere hypercalcemia as a form of acute lymphoblastic leukemia presentation in children
Rev Bras Ter Intensiva. 2015;27(4):402-405
DOI 10.5935/0103-507X.20150067
Views0See moreABSTRACT
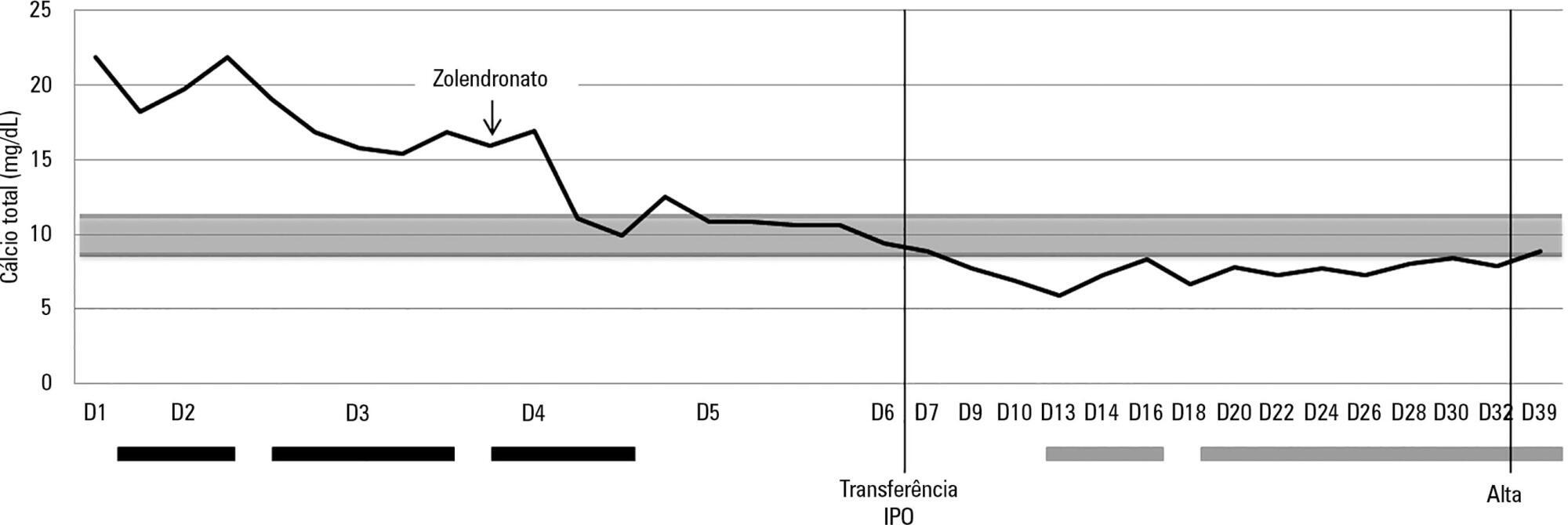
Hypercalcemia is a rare metabolic disorder in children and is potentially fatal. It has a wide differential diagnosis, including cancer. Here, we report the case of a previously healthy 3-year-old who was admitted to the emergency room with fatigue, hyporeactivity, fever and limping gait that had evolved over 5 days and that was progressively worsening. On examination the patient was unconscious (Glasgow coma score: 8). Laboratory tests indicated severe hypercalcemia (total calcium 21.39mg/dL, ionized calcium 2.93mmol/L) and microcytic anemia. Hyperhydration was initiated, and the child was transferred to the pediatric intensive care unit. Continuous venovenous hemodiafiltration with calcium-free solution was instituted, which brought progressive normalization of serum calcium and an improved state of consciousness. Zoledronate was administered, and metabolic and infectious causes and poisoning were excluded. The bone marrow smear revealed a diagnosis of acute lymphoblastic leukemia. Hypercalcemia associated with malignancy in children is rare and occurs as a form of cancer presentation or recurrence. Continuous venovenous hemodiafiltration should be considered in situations where there is imminent risk to life.
Views0Abstract
Case ReportSevere hypercalcemia as a form of acute lymphoblastic leukemia presentation in children
Rev Bras Ter Intensiva. 2015;27(4):402-405
DOI 10.5935/0103-507X.20150067
Views0See moreABSTRACT
Hypercalcemia is a rare metabolic disorder in children and is potentially fatal. It has a wide differential diagnosis, including cancer. Here, we report the case of a previously healthy 3-year-old who was admitted to the emergency room with fatigue, hyporeactivity, fever and limping gait that had evolved over 5 days and that was progressively worsening. On examination the patient was unconscious (Glasgow coma score: 8). Laboratory tests indicated severe hypercalcemia (total calcium 21.39mg/dL, ionized calcium 2.93mmol/L) and microcytic anemia. Hyperhydration was initiated, and the child was transferred to the pediatric intensive care unit. Continuous venovenous hemodiafiltration with calcium-free solution was instituted, which brought progressive normalization of serum calcium and an improved state of consciousness. Zoledronate was administered, and metabolic and infectious causes and poisoning were excluded. The bone marrow smear revealed a diagnosis of acute lymphoblastic leukemia. Hypercalcemia associated with malignancy in children is rare and occurs as a form of cancer presentation or recurrence. Continuous venovenous hemodiafiltration should be considered in situations where there is imminent risk to life.
-
Case Report
Use of thoracic electrical impedance tomography as an auxiliary tool for alveolar recruitment maneuvers in acute respiratory distress syndrome: case report and brief literature review
Rev Bras Ter Intensiva. 2015;27(4):406-411
Abstract
Case ReportUse of thoracic electrical impedance tomography as an auxiliary tool for alveolar recruitment maneuvers in acute respiratory distress syndrome: case report and brief literature review
Rev Bras Ter Intensiva. 2015;27(4):406-411
DOI 10.5935/0103-507X.20150068
Views0ABSTRACT
Thoracic electrical impedance tomography is a real-time, noninvasive monitoring tool of the regional pulmonary ventilation distribution. Its bedside use in patients with acute respiratory distress syndrome has the potential to aid in alveolar recruitment maneuvers, which are often necessary in cases of refractory hypoxemia. In this case report, we describe the monitoring results and interpretation of thoracic electrical impedance tomography used during alveolar recruitment maneuvers in a patient with acute respiratory distress syndrome, with transient application of high alveolar pressures and optimal positive end-expiratory pressure titration. Furthermore, we provide a brief literature review regarding the use of alveolar recruitment maneuvers and monitoring using thoracic electrical impedance tomography in patients with acute respiratory distress syndrome.
Keywords:Cardiography, impedanceCase reportsMonitoring, physiologicRespiratory insufficiency/physiopathologyRespiratory mechanicsSee moreViews0Abstract
Case ReportUse of thoracic electrical impedance tomography as an auxiliary tool for alveolar recruitment maneuvers in acute respiratory distress syndrome: case report and brief literature review
Rev Bras Ter Intensiva. 2015;27(4):406-411
DOI 10.5935/0103-507X.20150068
Views0ABSTRACT
Thoracic electrical impedance tomography is a real-time, noninvasive monitoring tool of the regional pulmonary ventilation distribution. Its bedside use in patients with acute respiratory distress syndrome has the potential to aid in alveolar recruitment maneuvers, which are often necessary in cases of refractory hypoxemia. In this case report, we describe the monitoring results and interpretation of thoracic electrical impedance tomography used during alveolar recruitment maneuvers in a patient with acute respiratory distress syndrome, with transient application of high alveolar pressures and optimal positive end-expiratory pressure titration. Furthermore, we provide a brief literature review regarding the use of alveolar recruitment maneuvers and monitoring using thoracic electrical impedance tomography in patients with acute respiratory distress syndrome.
Keywords:Cardiography, impedanceCase reportsMonitoring, physiologicRespiratory insufficiency/physiopathologyRespiratory mechanicsSee more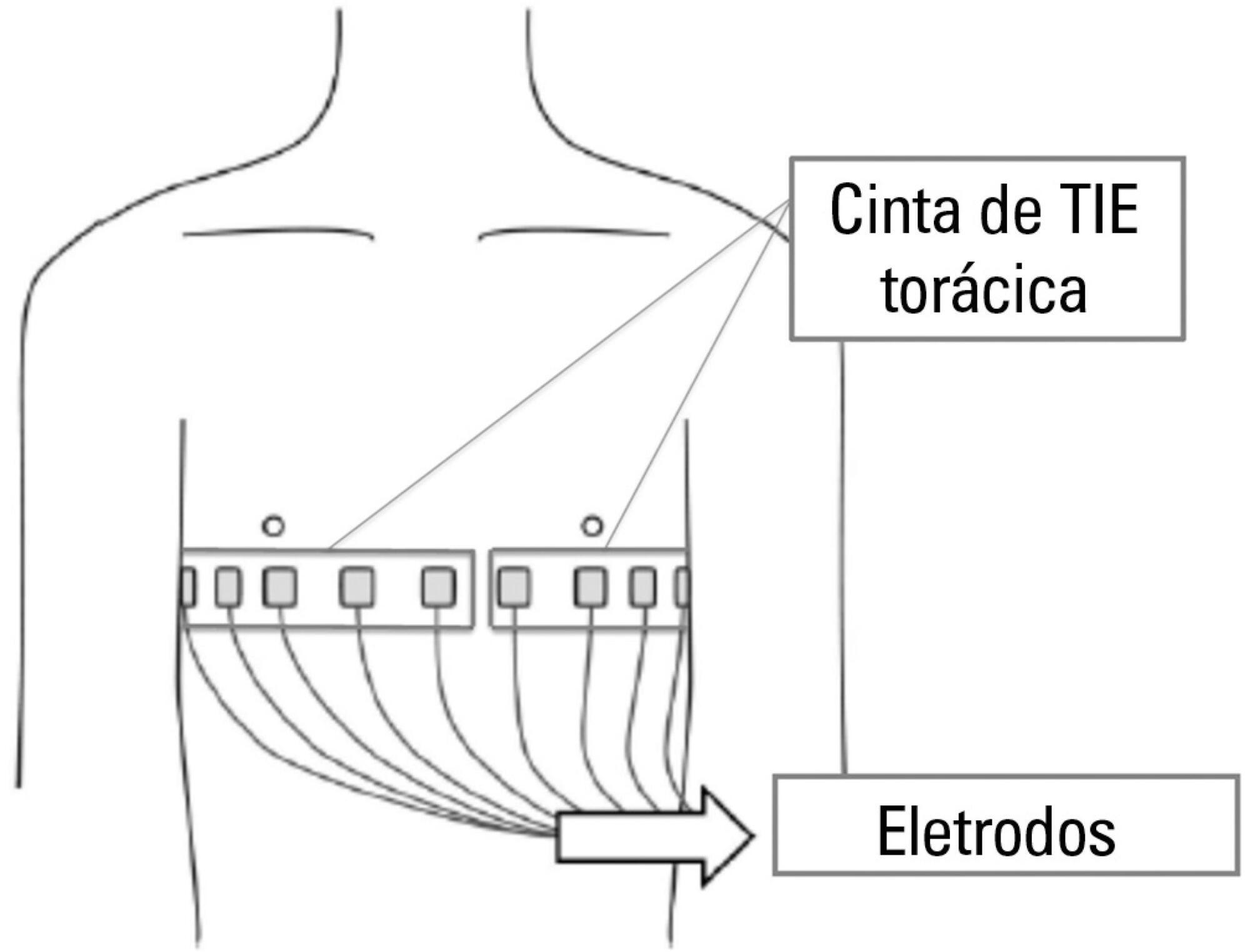
-
Case Report
Spontaneous intracranial hemorrhage in children: report of a hemophilia patient who survived due to a brain cyst
Rev Bras Ter Intensiva. 2015;27(4):412-415
Abstract
Case ReportSpontaneous intracranial hemorrhage in children: report of a hemophilia patient who survived due to a brain cyst
Rev Bras Ter Intensiva. 2015;27(4):412-415
DOI 10.5935/0103-507X.20150069
Views0ABSTRACT
We report the case of a 2-year-old child who survived an acute episode of severe spontaneous intracranial hemorrhage with clinical and radiological signs of intracranial hypertension and transtentorial herniation. The patient underwent emergency surgery to drain the hematoma, and a catheter was inserted to monitor intracranial pressure. In the initial computed tomography analysis performed prior to hematoma drainage, a brain cyst was evident contralateral to the hematoma, which, based on the analysis by the care team, possibly helped to avoid a worse outcome because the cyst accommodated the brain after the massive hemorrhage. After the investigation, the patient was determined to have previously undiagnosed hemophilia A. The patient underwent treatment in intensive care, which included the control of intracranial pressure, factor VIII replacement and discharge without signs of neurological impairment.
Keywords:Case reportsChildHemophilia A/complicationsIntracranial hemorrhagesIntracranial hypertension/etiologyIntracranial pressureTomography, X-ray computedSee moreViews0Abstract
Case ReportSpontaneous intracranial hemorrhage in children: report of a hemophilia patient who survived due to a brain cyst
Rev Bras Ter Intensiva. 2015;27(4):412-415
DOI 10.5935/0103-507X.20150069
Views0ABSTRACT
We report the case of a 2-year-old child who survived an acute episode of severe spontaneous intracranial hemorrhage with clinical and radiological signs of intracranial hypertension and transtentorial herniation. The patient underwent emergency surgery to drain the hematoma, and a catheter was inserted to monitor intracranial pressure. In the initial computed tomography analysis performed prior to hematoma drainage, a brain cyst was evident contralateral to the hematoma, which, based on the analysis by the care team, possibly helped to avoid a worse outcome because the cyst accommodated the brain after the massive hemorrhage. After the investigation, the patient was determined to have previously undiagnosed hemophilia A. The patient underwent treatment in intensive care, which included the control of intracranial pressure, factor VIII replacement and discharge without signs of neurological impairment.
Keywords:Case reportsChildHemophilia A/complicationsIntracranial hemorrhagesIntracranial hypertension/etiologyIntracranial pressureTomography, X-ray computedSee more
-
Letter to the Editor
To: The reality of patients requiring prolonged mechanical ventilation: a multicenter study
Rev Bras Ter Intensiva. 2015;27(4):416-418
Abstract
Letter to the EditorTo: The reality of patients requiring prolonged mechanical ventilation: a multicenter study
Rev Bras Ter Intensiva. 2015;27(4):416-418
DOI 10.5935/0103-507X.20150070
Views0To the Editor,From Averroes to Hippocrates and through Galen, Fleming or C. Venter, the history of medicine has been written as a constant stream of nonstop improvement on knowledge and clinical practice. Scientific production had not yet seen the momentum that we currently observe in the present era. With the astonishing amount of new data […]See moreViews0Abstract
Letter to the EditorTo: The reality of patients requiring prolonged mechanical ventilation: a multicenter study
Rev Bras Ter Intensiva. 2015;27(4):416-418
DOI 10.5935/0103-507X.20150070
Views0To the Editor,From Averroes to Hippocrates and through Galen, Fleming or C. Venter, the history of medicine has been written as a constant stream of nonstop improvement on knowledge and clinical practice. Scientific production had not yet seen the momentum that we currently observe in the present era. With the astonishing amount of new data […]See more -
Letter to the Editor
To: Out-of-bed extubation: a feasible study
Rev Bras Ter Intensiva. 2015;27(4):419-421
Abstract
Letter to the EditorTo: Out-of-bed extubation: a feasible study
Rev Bras Ter Intensiva. 2015;27(4):419-421
DOI 10.5935/0103-507X.20150071
Views0To the Editor, Weaning from mechanical ventilation represents one of the major challenges and concerns in intensive care units worldwide. The withdrawal time represents at least 40% of the overall mechanical ventilation period. Furthermore, in 30% of clinical cases some incidents will force the clinician to stop the attempt. Fortunately, there have been substantial improvements […]See moreViews0Abstract
Letter to the EditorTo: Out-of-bed extubation: a feasible study
Rev Bras Ter Intensiva. 2015;27(4):419-421
DOI 10.5935/0103-507X.20150071
Views0To the Editor, Weaning from mechanical ventilation represents one of the major challenges and concerns in intensive care units worldwide. The withdrawal time represents at least 40% of the overall mechanical ventilation period. Furthermore, in 30% of clinical cases some incidents will force the clinician to stop the attempt. Fortunately, there have been substantial improvements […]See more -
Letter to the Editor
To: Changes in respiratory mechanics during respiratory physiotherapy in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(4):422-423
Abstract
Letter to the EditorTo: Changes in respiratory mechanics during respiratory physiotherapy in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(4):422-423
DOI 10.5935/0103-507X.20150072
Views0To the Editor, We were very interested in the study by Moreira et al.() as it reflects common and routine respiratory physiotherapy practices in intensive care units in Brazil and other countries. We appreciate the author’s effort in examining the evidence for this type of therapy. In this study, an improvement was observed in the […]See moreViews0Abstract
Letter to the EditorTo: Changes in respiratory mechanics during respiratory physiotherapy in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(4):422-423
DOI 10.5935/0103-507X.20150072
Views0To the Editor, We were very interested in the study by Moreira et al.() as it reflects common and routine respiratory physiotherapy practices in intensive care units in Brazil and other countries. We appreciate the author’s effort in examining the evidence for this type of therapy. In this study, an improvement was observed in the […]See more
Volume Articles - Critical Care Science (CCS)
