Intensive care units Archives - Page 3 of 26 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2015;27(3):235-239
DOI 10.5935/0103-507X.20150043
To evaluate the association between the in-hospital mortality of patients hospitalized due to respiratory diseases and the availability of intensive care units.
This retrospective cohort study evaluated a database from a hospital medicine service involving patients hospitalized due to respiratory non-terminal diseases. Data on clinical characteristics and risk factors associated with mortality, such as Charlson score and length of hospital stay, were collected. The following analyses were performed: univariate analysis with simple stratification using the Mantel Haenszel test, chi squared test, Student’s t test, Mann-Whitney test, and logistic regression.
Three hundred thirteen patients were selected, including 98 (31.3%) before installation of the intensive care unit and 215 (68.7%) after installation of the intensive care unit. No significant differences in the clinical and anthropometric characteristics or risk factors were observed between the groups. The mortality rate was 18/95 (18.9%) before the installation of the intensive care unit and 21/206 (10.2%) after the installation of the intensive care unit. Logistic regression analysis indicated that the probability of death after the installation of the intensive care unit decreased by 58% (OR: 0.42; 95%CI 0.205 -0.879; p = 0.021).
Considering the limitations of the study, the results suggest a benefit, with a decrease of one death per every 11 patients treated for respiratory diseases after the installation of an intensive care unit in our hospital. The results corroborate the benefits of the implementation of intensive care units in secondary hospitals.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):235-239
DOI 10.5935/0103-507X.20150043
To evaluate the association between the in-hospital mortality of patients hospitalized due to respiratory diseases and the availability of intensive care units.
This retrospective cohort study evaluated a database from a hospital medicine service involving patients hospitalized due to respiratory non-terminal diseases. Data on clinical characteristics and risk factors associated with mortality, such as Charlson score and length of hospital stay, were collected. The following analyses were performed: univariate analysis with simple stratification using the Mantel Haenszel test, chi squared test, Student’s t test, Mann-Whitney test, and logistic regression.
Three hundred thirteen patients were selected, including 98 (31.3%) before installation of the intensive care unit and 215 (68.7%) after installation of the intensive care unit. No significant differences in the clinical and anthropometric characteristics or risk factors were observed between the groups. The mortality rate was 18/95 (18.9%) before the installation of the intensive care unit and 21/206 (10.2%) after the installation of the intensive care unit. Logistic regression analysis indicated that the probability of death after the installation of the intensive care unit decreased by 58% (OR: 0.42; 95%CI 0.205 -0.879; p = 0.021).
Considering the limitations of the study, the results suggest a benefit, with a decrease of one death per every 11 patients treated for respiratory diseases after the installation of an intensive care unit in our hospital. The results corroborate the benefits of the implementation of intensive care units in secondary hospitals.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):247-251
DOI 10.5935/0103-507X.20150045
To evaluate the incidence of urinary tract infections due to Trichosporon spp. in an intensive care unit.
This descriptive observational study was conducted in an intensive care unit between 2007 and 2009. All consecutive patients admitted to the intensive care unit with a confirmed diagnosis were evaluated.
Twenty patients presented with urinary tract infections due to Trichosporon spp. The prevalence was higher among men (65%) and among individuals > 70 years of age (55%). The mortality rate was 20%. The average intensive care unit stay was 19.8 days. The onset of infection was associated with prior use of antibiotics and was more frequent in the fall and winter.
Infection due to Trichosporon spp. was more common in men and among those > 70 years of age and was associated with the use of an indwelling urinary catheter for more than 20 days and with the use of broadspectrum antibiotics for more than 14 days. In addition, patients with urinary infection due to Trichosporon spp. were most often hospitalized in intensive care units in the fall and winter periods.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):247-251
DOI 10.5935/0103-507X.20150045
To evaluate the incidence of urinary tract infections due to Trichosporon spp. in an intensive care unit.
This descriptive observational study was conducted in an intensive care unit between 2007 and 2009. All consecutive patients admitted to the intensive care unit with a confirmed diagnosis were evaluated.
Twenty patients presented with urinary tract infections due to Trichosporon spp. The prevalence was higher among men (65%) and among individuals > 70 years of age (55%). The mortality rate was 20%. The average intensive care unit stay was 19.8 days. The onset of infection was associated with prior use of antibiotics and was more frequent in the fall and winter.
Infection due to Trichosporon spp. was more common in men and among those > 70 years of age and was associated with the use of an indwelling urinary catheter for more than 20 days and with the use of broadspectrum antibiotics for more than 14 days. In addition, patients with urinary infection due to Trichosporon spp. were most often hospitalized in intensive care units in the fall and winter periods.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):252-259
DOI 10.5935/0103-507X.20150046
To describe postextubation noninvasive positive pressure ventilation use in intensive care unit clinical practice and to identify factors associated with noninvasive positive pressure ventilation failure.
This prospective cohort study included patients aged ≥ 18 years consecutively admitted to the intensive care unit who required noninvasive positive pressure ventilation within 48 hours of extubation. The primary outcome was noninvasive positive pressure ventilation failure.
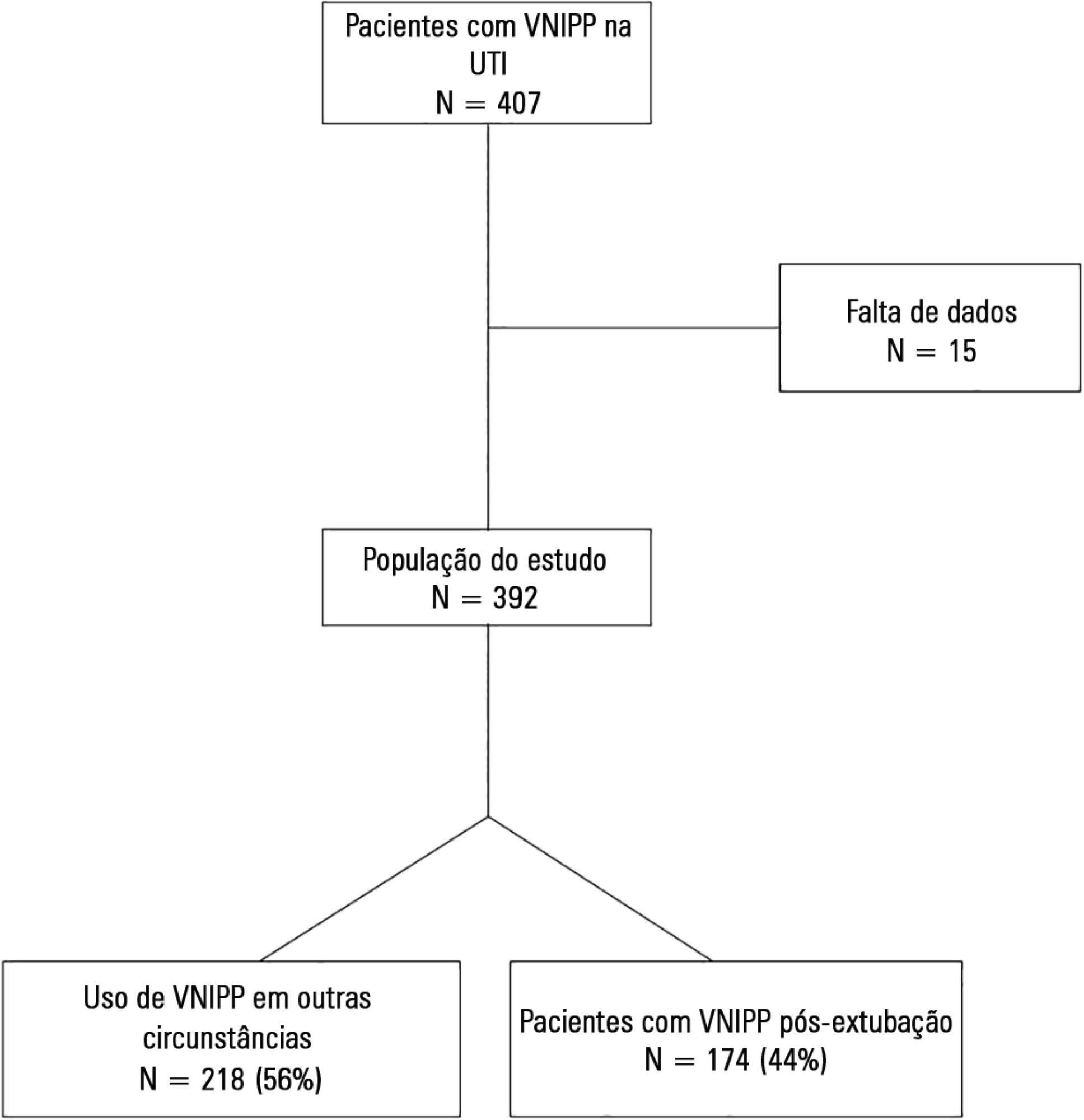
We included 174 patients in the study. The overall noninvasive positive pressure ventilation use rate was 15%. Among the patients who used noninvasive positive pressure ventilation, 44% used it after extubation. The failure rate of noninvasive positive pressure ventilation was 34%. The overall mean ± SD age was 56 ± 18 years, and 55% of participants were male. Demographics; baseline pH, PaCO2 and HCO3; and type of equipment used were similar between groups. All of the noninvasive positive pressure ventilation final parameters were higher in the noninvasive positive pressure ventilation failure group [inspiratory positive airway pressure: 15.0 versus 13.7cmH2O (p = 0.015), expiratory positive airway pressure: 10.0 versus 8.9cmH2O (p = 0.027), and FiO2: 41 versus 33% (p = 0.014)]. The mean intensive care unit length of stay was longer (24 versus 13 days), p < 0.001, and the intensive care unit mortality rate was higher (55 versus 10%), p < 0.001 in the noninvasive positive pressure ventilation failure group. After fitting, the logistic regression model allowed us to state that patients with inspiratory positive airway pressure ≥ 13.5cmH2O on the last day of noninvasive positive pressure ventilation support are three times more likely to experience noninvasive positive pressure ventilation failure compared with individuals with inspiratory positive airway pressure < 13.5 (OR = 3.02, 95%CI = 1.01 - 10.52, p value = 0.040).
The noninvasive positive pressure ventilation failure group had a longer intensive care unit length of stay and a higher mortality rate. Logistic regression analysis identified that patients with inspiratory positive airway pressure ≥ 13.5cmH2O on the last day of noninvasive positive pressure ventilation support are three times more likely to experience noninvasive positive pressure ventilation failure.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):252-259
DOI 10.5935/0103-507X.20150046
To describe postextubation noninvasive positive pressure ventilation use in intensive care unit clinical practice and to identify factors associated with noninvasive positive pressure ventilation failure.
This prospective cohort study included patients aged ≥ 18 years consecutively admitted to the intensive care unit who required noninvasive positive pressure ventilation within 48 hours of extubation. The primary outcome was noninvasive positive pressure ventilation failure.
We included 174 patients in the study. The overall noninvasive positive pressure ventilation use rate was 15%. Among the patients who used noninvasive positive pressure ventilation, 44% used it after extubation. The failure rate of noninvasive positive pressure ventilation was 34%. The overall mean ± SD age was 56 ± 18 years, and 55% of participants were male. Demographics; baseline pH, PaCO2 and HCO3; and type of equipment used were similar between groups. All of the noninvasive positive pressure ventilation final parameters were higher in the noninvasive positive pressure ventilation failure group [inspiratory positive airway pressure: 15.0 versus 13.7cmH2O (p = 0.015), expiratory positive airway pressure: 10.0 versus 8.9cmH2O (p = 0.027), and FiO2: 41 versus 33% (p = 0.014)]. The mean intensive care unit length of stay was longer (24 versus 13 days), p < 0.001, and the intensive care unit mortality rate was higher (55 versus 10%), p < 0.001 in the noninvasive positive pressure ventilation failure group. After fitting, the logistic regression model allowed us to state that patients with inspiratory positive airway pressure ≥ 13.5cmH2O on the last day of noninvasive positive pressure ventilation support are three times more likely to experience noninvasive positive pressure ventilation failure compared with individuals with inspiratory positive airway pressure < 13.5 (OR = 3.02, 95%CI = 1.01 - 10.52, p value = 0.040).
The noninvasive positive pressure ventilation failure group had a longer intensive care unit length of stay and a higher mortality rate. Logistic regression analysis identified that patients with inspiratory positive airway pressure ≥ 13.5cmH2O on the last day of noninvasive positive pressure ventilation support are three times more likely to experience noninvasive positive pressure ventilation failure.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):260-265
DOI 10.5935/0103-507X.20150047
>To evaluate the agreement between a new epidemiological surveillance method of the Center for Disease Control and Prevention and the clinical pulmonary infection score for mechanical ventilator-associated pneumonia detection.
This was a prospective cohort study that evaluated patients in the intensive care units of two hospitals who were intubated for more than 48 hours between August 2013 and June 2014. Patients were evaluated daily by physical therapist using the clinical pulmonary infection score. A nurse independently applied the new surveillance method proposed by the Center for Disease Control and Prevention. The diagnostic agreement between the methods was evaluated. A clinical pulmonary infection score of ≥ 7 indicated a clinical diagnosis of mechanical ventilator-associated pneumonia, and the association of a clinical pulmonary infection score ≥ 7 with an isolated semiquantitative culture consisting of ≥ 104 colony-forming units indicated a definitive diagnosis.
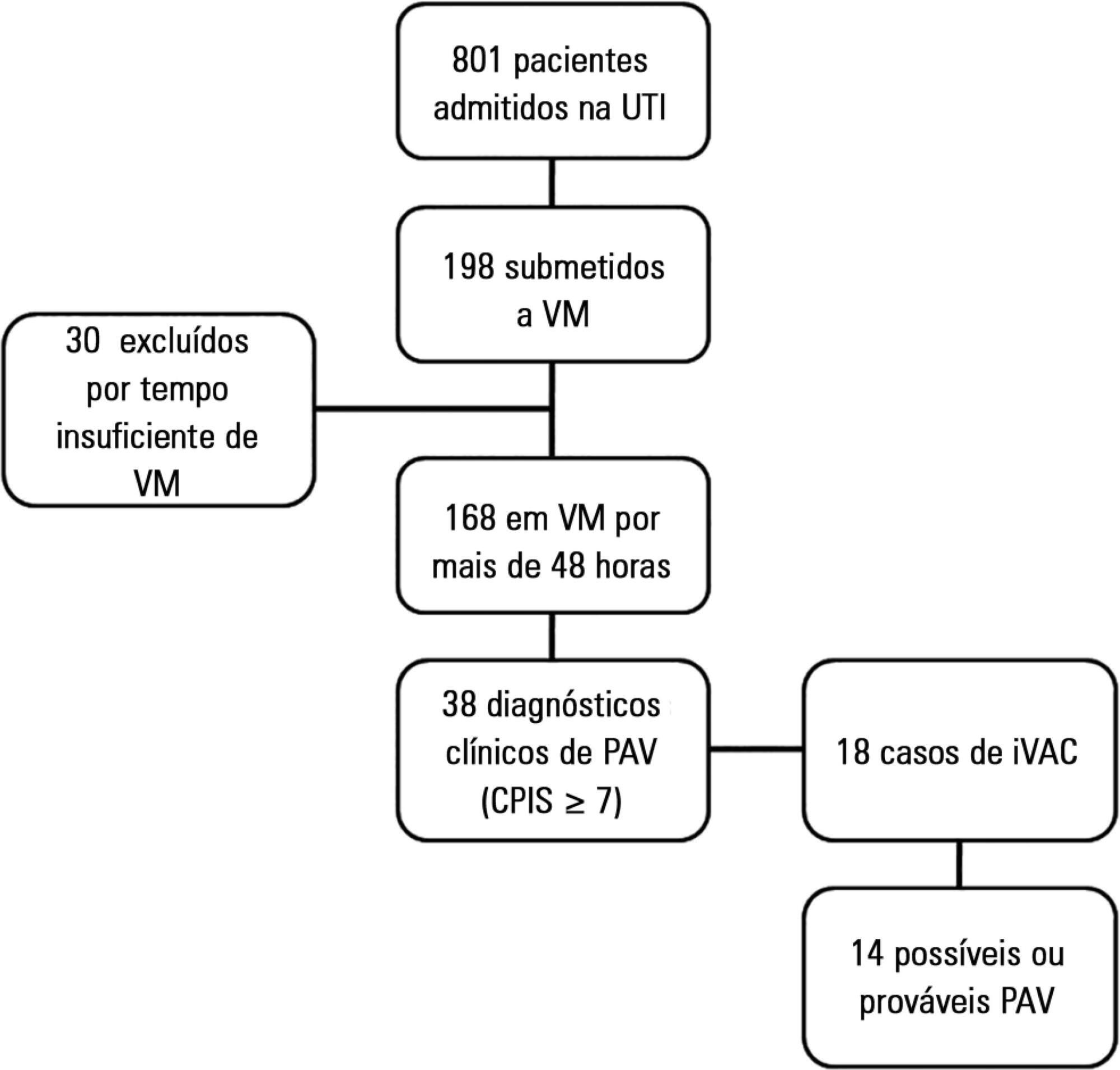
Of the 801 patients admitted to the intensive care units, 198 required mechanical ventilation. Of these, 168 were intubated for more than 48 hours. A total of 18 (10.7%) cases of mechanical ventilation-associated infectious conditions were identified, 14 (8.3%) of which exhibited possible or probable mechanical ventilatorassociated pneumonia, which represented 35% (14/38) of mechanical ventilator-associated pneumonia cases. The Center for Disease Control and Prevention method identified cases of mechanical ventilator-associated pneumonia with a sensitivity of 0.37, specificity of 1.0, positive predictive value of 1.0, and negative predictive value of 0.84. The differences resulted in discrepancies in the mechanical ventilator-associated pneumonia incidence density (CDC, 5.2/1000 days of mechanical ventilation; clinical pulmonary infection score ≥ 7, 13.1/1000 days of mechanical ventilation).
The Center for Disease Control and Prevention method failed to detect mechanical ventilatorassociated pneumonia cases and may not be satisfactory as a surveillance method.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):260-265
DOI 10.5935/0103-507X.20150047
>To evaluate the agreement between a new epidemiological surveillance method of the Center for Disease Control and Prevention and the clinical pulmonary infection score for mechanical ventilator-associated pneumonia detection.
This was a prospective cohort study that evaluated patients in the intensive care units of two hospitals who were intubated for more than 48 hours between August 2013 and June 2014. Patients were evaluated daily by physical therapist using the clinical pulmonary infection score. A nurse independently applied the new surveillance method proposed by the Center for Disease Control and Prevention. The diagnostic agreement between the methods was evaluated. A clinical pulmonary infection score of ≥ 7 indicated a clinical diagnosis of mechanical ventilator-associated pneumonia, and the association of a clinical pulmonary infection score ≥ 7 with an isolated semiquantitative culture consisting of ≥ 104 colony-forming units indicated a definitive diagnosis.
Of the 801 patients admitted to the intensive care units, 198 required mechanical ventilation. Of these, 168 were intubated for more than 48 hours. A total of 18 (10.7%) cases of mechanical ventilation-associated infectious conditions were identified, 14 (8.3%) of which exhibited possible or probable mechanical ventilatorassociated pneumonia, which represented 35% (14/38) of mechanical ventilator-associated pneumonia cases. The Center for Disease Control and Prevention method identified cases of mechanical ventilator-associated pneumonia with a sensitivity of 0.37, specificity of 1.0, positive predictive value of 1.0, and negative predictive value of 0.84. The differences resulted in discrepancies in the mechanical ventilator-associated pneumonia incidence density (CDC, 5.2/1000 days of mechanical ventilation; clinical pulmonary infection score ≥ 7, 13.1/1000 days of mechanical ventilation).
The Center for Disease Control and Prevention method failed to detect mechanical ventilatorassociated pneumonia cases and may not be satisfactory as a surveillance method.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):212-219
DOI 10.5935/0103-507X.20150034
To evaluate the clinical characteristics of patients with hematological disease admitted to the intensive care unit and the use of noninvasive mechanical ventilation in a subgroup with respiratory dysfunction.
A retrospective observational study from September 2011 to January 2014.
Overall, 157 patients were included. The mean age was 45.13 (± 17.2) years and 46.5% of the patients were female. Sixty-seven (48.4%) patients had sepsis, and 90 (57.3%) patients required vasoactive vasopressors. The main cause for admission to the intensive care unit was acute respiratory failure (94.3%). Among the 157 studied patients, 47 (29.9%) were intubated within the first 24 hours, and 38 (24.2%) underwent noninvasive mechanical ventilation. Among the 38 patients who initially received noninvasive mechanical ventilation, 26 (68.4%) were subsequently intubated, and 12 (31.6%) responded to this mode of ventilation. Patients who failed to respond to noninvasive mechanical ventilation had higher intensive care unit mortality (66.7% versus 16.7%; p = 0.004) and a longer stay in the intensive care unit (9.6 days versus 4.6 days, p = 0.02) compared with the successful cases. Baseline severity scores (SOFA and SAPS 3) and the total leukocyte count were not significantly different between these two subgroups. In a multivariate logistic regression model including the 157 patients, intubation at any time during the stay in the intensive care unit and SAPS 3 were independently associated with intensive care unit mortality, while using noninvasive mechanical ventilation was not.
In this retrospective study with severely ill hematologic patients, those who underwent noninvasive mechanical ventilation at admission and failed to respond to it presented elevated intensive care unit mortality. However, only intubation during the intensive care unit stay was independently associated with a poor outcome. Further studies are needed to define predictors of noninvasive mechanical ventilation failure.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):212-219
DOI 10.5935/0103-507X.20150034
To evaluate the clinical characteristics of patients with hematological disease admitted to the intensive care unit and the use of noninvasive mechanical ventilation in a subgroup with respiratory dysfunction.
A retrospective observational study from September 2011 to January 2014.
Overall, 157 patients were included. The mean age was 45.13 (± 17.2) years and 46.5% of the patients were female. Sixty-seven (48.4%) patients had sepsis, and 90 (57.3%) patients required vasoactive vasopressors. The main cause for admission to the intensive care unit was acute respiratory failure (94.3%). Among the 157 studied patients, 47 (29.9%) were intubated within the first 24 hours, and 38 (24.2%) underwent noninvasive mechanical ventilation. Among the 38 patients who initially received noninvasive mechanical ventilation, 26 (68.4%) were subsequently intubated, and 12 (31.6%) responded to this mode of ventilation. Patients who failed to respond to noninvasive mechanical ventilation had higher intensive care unit mortality (66.7% versus 16.7%; p = 0.004) and a longer stay in the intensive care unit (9.6 days versus 4.6 days, p = 0.02) compared with the successful cases. Baseline severity scores (SOFA and SAPS 3) and the total leukocyte count were not significantly different between these two subgroups. In a multivariate logistic regression model including the 157 patients, intubation at any time during the stay in the intensive care unit and SAPS 3 were independently associated with intensive care unit mortality, while using noninvasive mechanical ventilation was not.
In this retrospective study with severely ill hematologic patients, those who underwent noninvasive mechanical ventilation at admission and failed to respond to it presented elevated intensive care unit mortality. However, only intubation during the intensive care unit stay was independently associated with a poor outcome. Further studies are needed to define predictors of noninvasive mechanical ventilation failure.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):220-227
DOI 10.5935/0103-507X.20150033
To analyze the epidemiological clinical profile of women with maternal near miss according to the new World Health Organization criteria.
A descriptive crosssectional study was conducted, in which the records of patients admitted to the obstetric intensive care unit of a tertiary hospital in Recife (Brazil) over a period of four years were analyzed. Women who presented at least one near miss criterion were included. The variables studied were age, race/color, civil status, education, place of origin, number of pregnancies and prenatal consultations, complications and procedures performed, mode of delivery, gestational age at delivery, and maternal near miss criteria. The descriptive analysis was performed using the program Epi-Info 3.5.1.
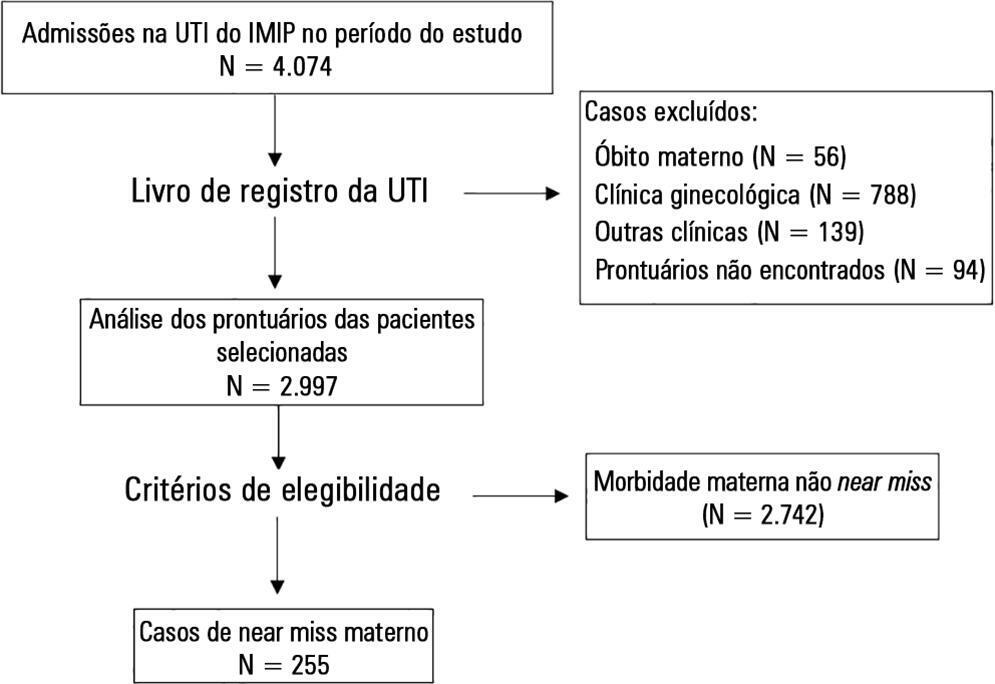
Two hundred fifty-five cases of maternal near miss were identified, with an overall ratio of maternal near miss of 12.8/1,000 live births. Among these cases, 43.2% of the women had incomplete primary education, 44.7% were primiparous, and 20.5% had undergone a previous cesarean section. Regarding specific diagnoses, there was a predominance of hypertensive disorders (62.7%), many of which were complicated by HELLP (hemolysis, elevated liver enzymes, and low platelets) syndrome (41.2%). The laboratory near miss criteria were the most often observed (59.6%), due mainly to the high frequency of acute thrombocytopenia (32.5%).
A high frequency of women who had a low level of education and who were primiparous was observed. According to the new criteria proposed by the World Health Organization, hypertensive pregnancy disorders are still the most common among maternal near miss cases. The high frequency of HELLP syndrome was also striking, which contributed to acute thrombocytopenia being the most frequent near miss criterion.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):220-227
DOI 10.5935/0103-507X.20150033
To analyze the epidemiological clinical profile of women with maternal near miss according to the new World Health Organization criteria.
A descriptive crosssectional study was conducted, in which the records of patients admitted to the obstetric intensive care unit of a tertiary hospital in Recife (Brazil) over a period of four years were analyzed. Women who presented at least one near miss criterion were included. The variables studied were age, race/color, civil status, education, place of origin, number of pregnancies and prenatal consultations, complications and procedures performed, mode of delivery, gestational age at delivery, and maternal near miss criteria. The descriptive analysis was performed using the program Epi-Info 3.5.1.
Two hundred fifty-five cases of maternal near miss were identified, with an overall ratio of maternal near miss of 12.8/1,000 live births. Among these cases, 43.2% of the women had incomplete primary education, 44.7% were primiparous, and 20.5% had undergone a previous cesarean section. Regarding specific diagnoses, there was a predominance of hypertensive disorders (62.7%), many of which were complicated by HELLP (hemolysis, elevated liver enzymes, and low platelets) syndrome (41.2%). The laboratory near miss criteria were the most often observed (59.6%), due mainly to the high frequency of acute thrombocytopenia (32.5%).
A high frequency of women who had a low level of education and who were primiparous was observed. According to the new criteria proposed by the World Health Organization, hypertensive pregnancy disorders are still the most common among maternal near miss cases. The high frequency of HELLP syndrome was also striking, which contributed to acute thrombocytopenia being the most frequent near miss criterion.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):51-56
DOI 10.5935/0103-507X.20150009
To assess the causes and factors associated with the death of patients between intensive care unit discharge and hospital discharge.
The present is a pilot, retrospective, observational cohort study. The records of all patients admitted to two units of a public/private university hospital from February 1, 2013 to April 30, 2013 were assessed. Demographic and clinical data, risk scores and outcomes were obtained from the Epimed monitoring system and confirmed in the electronic record system of the hospital. The relative risk and respective confidence intervals were calculated.
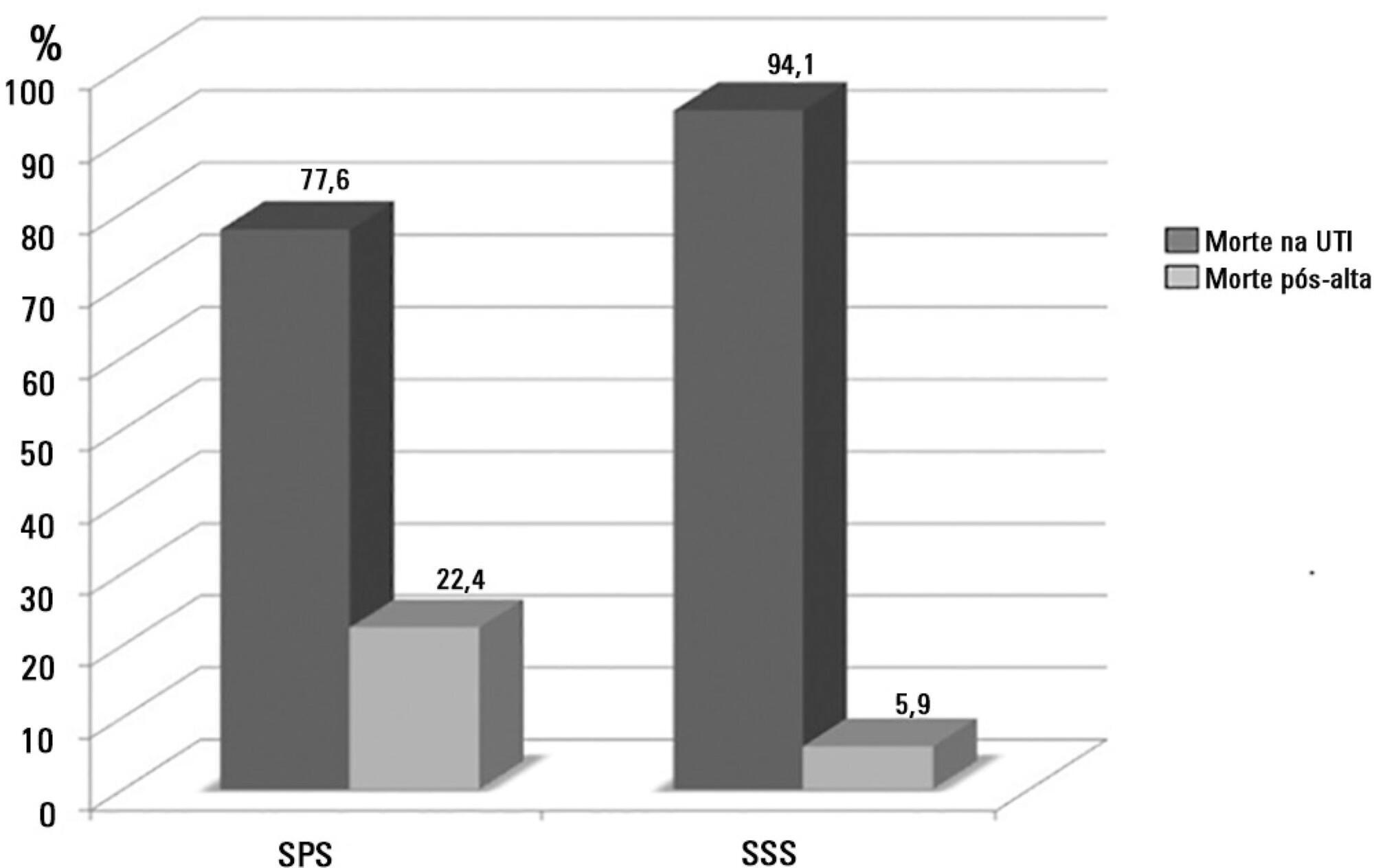
A total of 581 patients were evaluated. The mortality rate in the intensive care unit was 20.8% and in the hospital was 24.9%. Septic shock was the cause of death in 58.3% of patients who died after being discharged from the intensive care unit. Of the patients from the public health system, 73 (77.6%) died in the intensive care unit and 21 (22.4%) died in the hospital after being discharged from the unit. Of the patients from the Supplementary Health System, 48 (94.1%) died in the intensive care unit and 3 (5.9%) died in the hospital after being discharged from the unit (relative risk, 3.87%; 95% confidence interval, 1.21 - 12.36; p < 0.05). The post-discharge mortality rate was significantly higher in patients with intensive care unit hospitalization time longer than 6 days.
The main cause of death of patients who were discharged from the intensive care unit and died in the ward before hospital discharge was septic shock. Coverage by the public healthcare system and longer hospitalization time in the intensive care unit were factors associated with death after discharge from the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):51-56
DOI 10.5935/0103-507X.20150009
To assess the causes and factors associated with the death of patients between intensive care unit discharge and hospital discharge.
The present is a pilot, retrospective, observational cohort study. The records of all patients admitted to two units of a public/private university hospital from February 1, 2013 to April 30, 2013 were assessed. Demographic and clinical data, risk scores and outcomes were obtained from the Epimed monitoring system and confirmed in the electronic record system of the hospital. The relative risk and respective confidence intervals were calculated.
A total of 581 patients were evaluated. The mortality rate in the intensive care unit was 20.8% and in the hospital was 24.9%. Septic shock was the cause of death in 58.3% of patients who died after being discharged from the intensive care unit. Of the patients from the public health system, 73 (77.6%) died in the intensive care unit and 21 (22.4%) died in the hospital after being discharged from the unit. Of the patients from the Supplementary Health System, 48 (94.1%) died in the intensive care unit and 3 (5.9%) died in the hospital after being discharged from the unit (relative risk, 3.87%; 95% confidence interval, 1.21 - 12.36; p < 0.05). The post-discharge mortality rate was significantly higher in patients with intensive care unit hospitalization time longer than 6 days.
The main cause of death of patients who were discharged from the intensive care unit and died in the ward before hospital discharge was septic shock. Coverage by the public healthcare system and longer hospitalization time in the intensive care unit were factors associated with death after discharge from the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
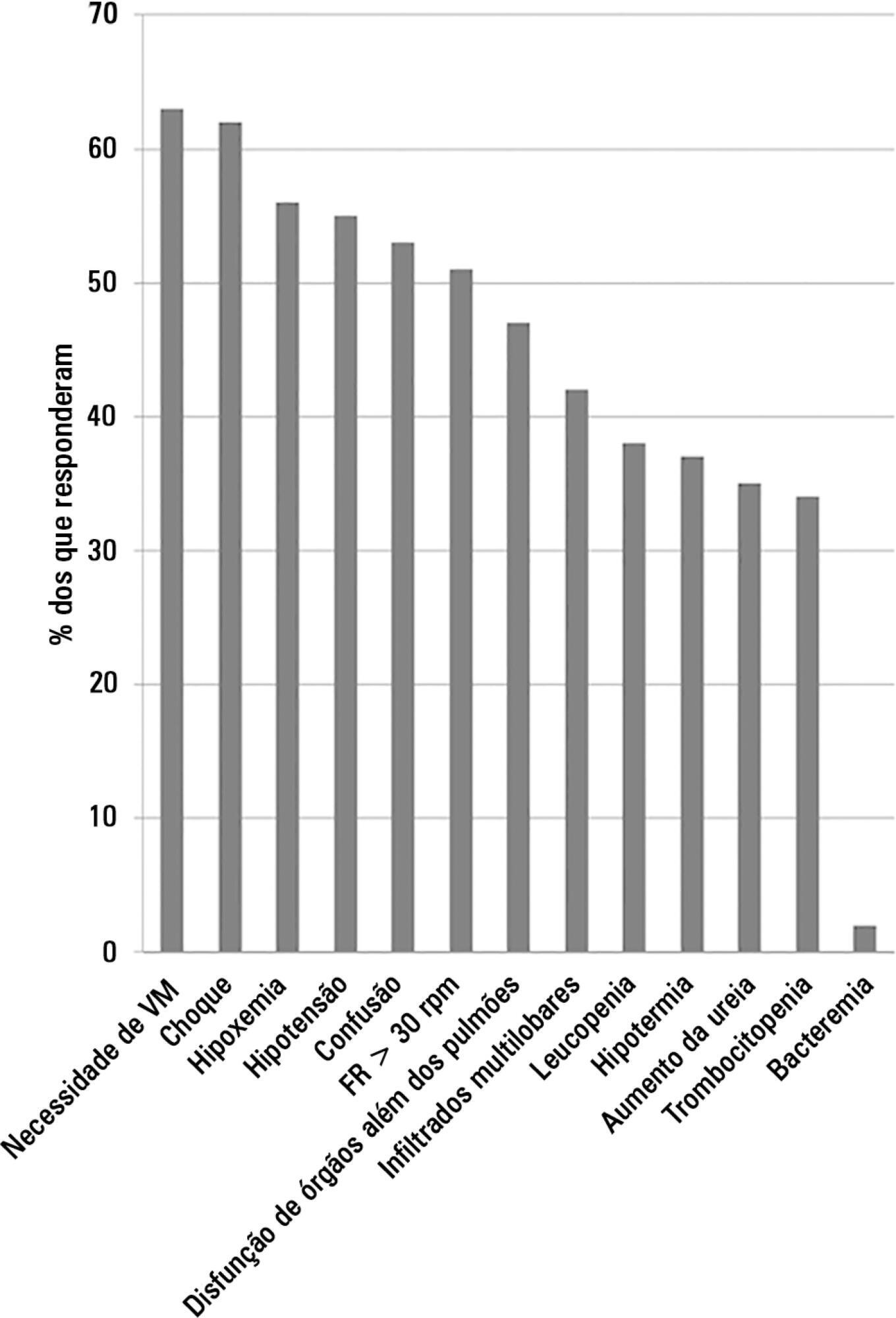
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.