-
How do you prefer your resuscitation solution?: do you want a little bit more salt?
Rev Bras Ter Intensiva. 2012;24(4):315-315
Abstract
How do you prefer your resuscitation solution?: do you want a little bit more salt?
Rev Bras Ter Intensiva. 2012;24(4):315-315
DOI 10.1590/S0103-507X2012000400001
Views0EDITORIAL How do you prefer your resuscitation solution? Do you want a little bit more salt? […]See moreViews0

Abstract
How do you prefer your resuscitation solution?: do you want a little bit more salt?
Rev Bras Ter Intensiva. 2012;24(4):315-315
DOI 10.1590/S0103-507X2012000400001
Views0EDITORIAL How do you prefer your resuscitation solution? Do you want a little bit more salt?[…]See more -
Importance of intensive care professionals for organ donation and transplantation
Rev Bras Ter Intensiva. 2012;24(4):316-317
Abstract
Importance of intensive care professionals for organ donation and transplantation
Rev Bras Ter Intensiva. 2012;24(4):316-317
DOI 10.1590/S0103-507X2012000400002
Views0EDITORIAL Importance of intensive care professionals for organ donation and transplantation[…]See moreViews0Abstract
Importance of intensive care professionals for organ donation and transplantation
Rev Bras Ter Intensiva. 2012;24(4):316-317
DOI 10.1590/S0103-507X2012000400002
Views0EDITORIAL Importance of intensive care professionals for organ donation and transplantation[…]See more -
Moving beyond the assessment of mortality and severity of diseases in critical patients: we are just getting started…
Rev Bras Ter Intensiva. 2012;24(4):318-319
Abstract
Moving beyond the assessment of mortality and severity of diseases in critical patients: we are just getting started…
Rev Bras Ter Intensiva. 2012;24(4):318-319
DOI 10.1590/S0103-507X2012000400003
Views0EDITORIAL Moving beyond the assessment of mortality and severity of diseases in critical patients: we are just getting started…[…]See moreViews0Abstract
Moving beyond the assessment of mortality and severity of diseases in critical patients: we are just getting started…
Rev Bras Ter Intensiva. 2012;24(4):318-319
DOI 10.1590/S0103-507X2012000400003
Views0EDITORIAL Moving beyond the assessment of mortality and severity of diseases in critical patients: we are just getting started…[…]See more -
Do endotracheal tubes with suction above the cuff decrease the rate of ventilator-associated pneumonia, and are they cost-effective?
Rev Bras Ter Intensiva. 2012;24(4):320-321
Abstract
Do endotracheal tubes with suction above the cuff decrease the rate of ventilator-associated pneumonia, and are they cost-effective?
Rev Bras Ter Intensiva. 2012;24(4):320-321
DOI 10.1590/S0103-507X2012000400004
Views0EDITORIAL Do endotracheal tubes with suction above the cuff decrease the rate of ventilator-associated pneumonia, and are they cost-effective?[…]See moreViews0Abstract
Do endotracheal tubes with suction above the cuff decrease the rate of ventilator-associated pneumonia, and are they cost-effective?
Rev Bras Ter Intensiva. 2012;24(4):320-321
DOI 10.1590/S0103-507X2012000400004
Views0EDITORIAL Do endotracheal tubes with suction above the cuff decrease the rate of ventilator-associated pneumonia, and are they cost-effective?[…]See more -
Special Article
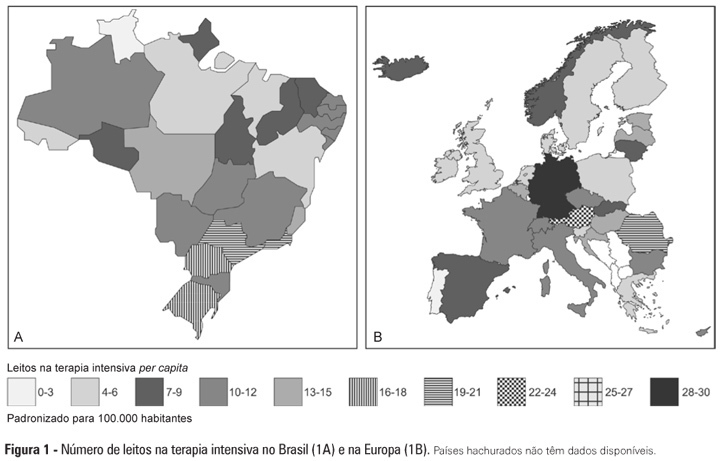
Intensive care provision: a global problem
Rev Bras Ter Intensiva. 2012;24(4):322-325
Abstract
Views0Abstract
-
Original Article – Basic Research
Volume replacement with saline solutions during pancreatitis in rats and the hepatic profiles of apoptotic proteins and heat-shock proteins
Rev Bras Ter Intensiva. 2012;24(4):326-333
Abstract
Original Article – Basic ResearchVolume replacement with saline solutions during pancreatitis in rats and the hepatic profiles of apoptotic proteins and heat-shock proteins
Rev Bras Ter Intensiva. 2012;24(4):326-333
DOI 10.1590/S0103-507X2012000400006
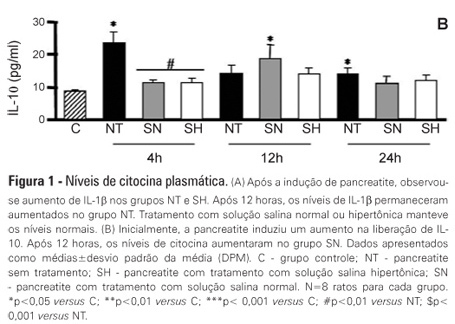
Views0See moreOBJECTIVE: Liver failure can occur as a consequence of the systemic inflammation after acute pancreatitis. We assessed the effect of volume repositioning with hypertonic saline solution or normal saline on hepatic cytokine production and the expression of heat-shock proteins and apoptotic proteins after acute pancreatitis. METHODS: Wistar rats were divided in four groups: C – control animals that were not subjected to insult or treatment; NT – animals that were subjected to acute pancreatitis and received no treatment; normal saline – animals that were subjected to acute pancreatitis and received normal saline (NaCl 0.9%); and HS – animals that were subjected to acute pancreatitis and received hypertonic saline solution (NaCl 7.5%). Acute pancreatitis was induced by retrograde transduodenal infusion of 2.5% sodium taurocholate into the pancreatic duct. At 4, 12 and 24 h following acute pancreatitis induction, TNF-alpha, IL-1-beta, IL-6 and IL-10, caspase-2 and -7, Apaf-1, AIF and HSP60 and 90 were analyzed in the liver. RESULTS: Casp2 decreased in the normal saline and hypertonic saline groups (p<0.05 versus. C) at 12 h. Apaf-1, AIF and HSP90 remained unchanged. At 4 h, Casp7 increased in the NT group (p<0.01 versus C), although it remained at the baseline levels in the reperfused groups. HSP60 increased in all of the groups at 4 h (p< 0.001 vs. C). However, the hypertonic saline group showed lower expression of HSP60 than the normal saline group (p<0.05). Hypertonic saline solution maintained the production of cytokines at normal levels. Volume reperfusion with normal or hypertonic saline significantly modulated the expression of Casp7. CONCLUSION: Volume replacement with hypertonic or normal saline was effective in reducing caspase 7. However, only hypertonic solution was capable of regulating cytokine production and HSP60 expression at all time points.
Views0Abstract
Original Article – Basic ResearchVolume replacement with saline solutions during pancreatitis in rats and the hepatic profiles of apoptotic proteins and heat-shock proteins
Rev Bras Ter Intensiva. 2012;24(4):326-333
DOI 10.1590/S0103-507X2012000400006
Views0See moreOBJECTIVE: Liver failure can occur as a consequence of the systemic inflammation after acute pancreatitis. We assessed the effect of volume repositioning with hypertonic saline solution or normal saline on hepatic cytokine production and the expression of heat-shock proteins and apoptotic proteins after acute pancreatitis. METHODS: Wistar rats were divided in four groups: C – control animals that were not subjected to insult or treatment; NT – animals that were subjected to acute pancreatitis and received no treatment; normal saline – animals that were subjected to acute pancreatitis and received normal saline (NaCl 0.9%); and HS – animals that were subjected to acute pancreatitis and received hypertonic saline solution (NaCl 7.5%). Acute pancreatitis was induced by retrograde transduodenal infusion of 2.5% sodium taurocholate into the pancreatic duct. At 4, 12 and 24 h following acute pancreatitis induction, TNF-alpha, IL-1-beta, IL-6 and IL-10, caspase-2 and -7, Apaf-1, AIF and HSP60 and 90 were analyzed in the liver. RESULTS: Casp2 decreased in the normal saline and hypertonic saline groups (p<0.05 versus. C) at 12 h. Apaf-1, AIF and HSP90 remained unchanged. At 4 h, Casp7 increased in the NT group (p<0.01 versus C), although it remained at the baseline levels in the reperfused groups. HSP60 increased in all of the groups at 4 h (p< 0.001 vs. C). However, the hypertonic saline group showed lower expression of HSP60 than the normal saline group (p<0.05). Hypertonic saline solution maintained the production of cytokines at normal levels. Volume reperfusion with normal or hypertonic saline significantly modulated the expression of Casp7. CONCLUSION: Volume replacement with hypertonic or normal saline was effective in reducing caspase 7. However, only hypertonic solution was capable of regulating cytokine production and HSP60 expression at all time points.
-
Original Articles – Clinical Research
A managed protocol for treatment of deceased potential donors reduces the incidence of cardiac arrest before organ explant
Rev Bras Ter Intensiva. 2012;24(4):334-340
Abstract
Original Articles – Clinical ResearchA managed protocol for treatment of deceased potential donors reduces the incidence of cardiac arrest before organ explant
Rev Bras Ter Intensiva. 2012;24(4):334-340
DOI 10.1590/S0103-507X2012000400007
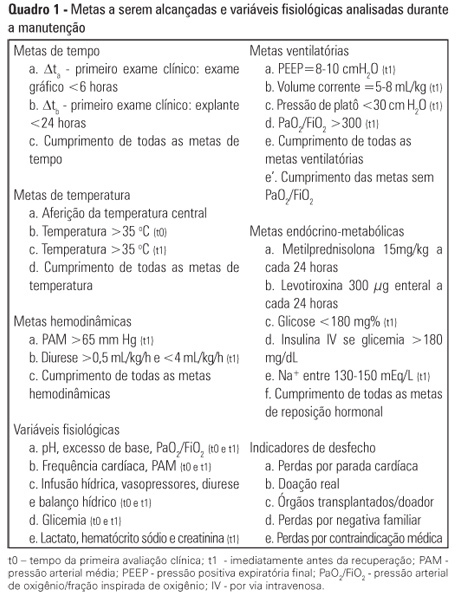
Views0See moreOBJECTIVE: To assess the effect of the application of a managed protocol for the maintenance care of deceased potential multiple organ donors at two hospitals. METHODS: A before (Phase 1)/after (Phase 2) study conducted at two general hospitals, which included consecutively potential donors admitted to two intensive care units. In Phase 1 (16 months), the data were collected retrospectively, and the maintenance care measures of the potential donors were instituted by the intensivists. In Phase 2 (12 months), the data collection was prospective, and a managed protocol was used for maintenance care. The two phases were compared in terms of their demographic variables, physiological variables at diagnosis of brain death and the end of the process, time to performance of brain death confirmatory test and end of the process, adherence to bundles of maintenance care essential measures, losses due to cardiac arrest, family refusal, contraindications, and the conversion rate of potential into actual donors. Student’s t- and chi-square tests were used, and p-value < 0.05 was considered to be significant. RESULTS: A total of 42 potential donors were identified (18 in Phase 1 and 24 in Phase 2). The time interval between the first clinical assessment and the recovery decreased in Phase 2 (Phase 1: 35.0±15.5 hours versus Phase 2: 24.6±6.2 hours; p = 0.023). Adherence increased to 10 out of the 19 essential items of maintenance care, and losses due to cardiac arrest also decreased in Phase 2 (Phase 1: 27.8 versus 0% in Phase 2; p = 0.006), while the convertion rate increased (Phase 1: 44.4 versus 75% in Phase 2; p = 0.044). The losses due to family refusal and medical contraindication did not vary. CONCLUSION: The adoption of a managed protocol focused on the application of essential measures for the care of potential deceased donors might reduce the loss of potential donors due to cardiac arrest.
Views0Abstract
Original Articles – Clinical ResearchA managed protocol for treatment of deceased potential donors reduces the incidence of cardiac arrest before organ explant
Rev Bras Ter Intensiva. 2012;24(4):334-340
DOI 10.1590/S0103-507X2012000400007
Views0See moreOBJECTIVE: To assess the effect of the application of a managed protocol for the maintenance care of deceased potential multiple organ donors at two hospitals. METHODS: A before (Phase 1)/after (Phase 2) study conducted at two general hospitals, which included consecutively potential donors admitted to two intensive care units. In Phase 1 (16 months), the data were collected retrospectively, and the maintenance care measures of the potential donors were instituted by the intensivists. In Phase 2 (12 months), the data collection was prospective, and a managed protocol was used for maintenance care. The two phases were compared in terms of their demographic variables, physiological variables at diagnosis of brain death and the end of the process, time to performance of brain death confirmatory test and end of the process, adherence to bundles of maintenance care essential measures, losses due to cardiac arrest, family refusal, contraindications, and the conversion rate of potential into actual donors. Student’s t- and chi-square tests were used, and p-value < 0.05 was considered to be significant. RESULTS: A total of 42 potential donors were identified (18 in Phase 1 and 24 in Phase 2). The time interval between the first clinical assessment and the recovery decreased in Phase 2 (Phase 1: 35.0±15.5 hours versus Phase 2: 24.6±6.2 hours; p = 0.023). Adherence increased to 10 out of the 19 essential items of maintenance care, and losses due to cardiac arrest also decreased in Phase 2 (Phase 1: 27.8 versus 0% in Phase 2; p = 0.006), while the convertion rate increased (Phase 1: 44.4 versus 75% in Phase 2; p = 0.044). The losses due to family refusal and medical contraindication did not vary. CONCLUSION: The adoption of a managed protocol focused on the application of essential measures for the care of potential deceased donors might reduce the loss of potential donors due to cardiac arrest.
-
Original Articles – Clinical Research
Quality of life before admission to the intensive care unit
Rev Bras Ter Intensiva. 2012;24(4):341-346
Abstract
Original Articles – Clinical ResearchQuality of life before admission to the intensive care unit
Rev Bras Ter Intensiva. 2012;24(4):341-346
DOI 10.1590/S0103-507X2012000400008
Views0See moreOBJECTIVE: To examine the reliability of the SF-36 general health questionnaire when used to evaluate the health status of critically ill patients before admission to intensive care and to measure their health-related quality of life prior to admission and its relation to severity of illness and length of stay in the intensive care unit. METHODS: Prospective cohort study conducted in the intensive care unit of a public teaching hospital. Over three months, communicative and oriented patients were interviewed within the first 72 hours of intensive care unit admission; 91 individuals participated. The APACHE II score was used to assess severity of illness, and the SF-36 questionnaire was used to measure health-related quality of life. RESULTS: The reliability of SF-36 was verified in all dimensions using Cronbach’s alpha coefficient. In six dimensions of eight domains the value exceeded 0.70. The average SF-36 scores of the health-related quality of life dimensions for the patients before admission to intensive care unit were 57.8 for physical functioning, 32.4 for role-physical, 53.0 for bodily pain, 63.2 for general health, 50.6 for vitality, 56.2 for social functioning, 54.6 for role-emotional and 60.3 for mental health. The correlations between severity of illness and length of stay and the health-related quality of life scores were very low, ranging from -0.152 to 0.175 and -0.158 to 0.152, respectively, which were not statistically significant. CONCLUSION: In the sample studied, the SF-36 demonstrated good reliability when used to measure health-related quality of life in critically ill patients before admission to the intensive care unit. The worst score was role-physical and the best was general health. Health-related quality of life of patients before admission was not correlated with severity of illness or length of stay in the intensive care unit.
Views0Abstract
Original Articles – Clinical ResearchQuality of life before admission to the intensive care unit
Rev Bras Ter Intensiva. 2012;24(4):341-346
DOI 10.1590/S0103-507X2012000400008
Views0See moreOBJECTIVE: To examine the reliability of the SF-36 general health questionnaire when used to evaluate the health status of critically ill patients before admission to intensive care and to measure their health-related quality of life prior to admission and its relation to severity of illness and length of stay in the intensive care unit. METHODS: Prospective cohort study conducted in the intensive care unit of a public teaching hospital. Over three months, communicative and oriented patients were interviewed within the first 72 hours of intensive care unit admission; 91 individuals participated. The APACHE II score was used to assess severity of illness, and the SF-36 questionnaire was used to measure health-related quality of life. RESULTS: The reliability of SF-36 was verified in all dimensions using Cronbach’s alpha coefficient. In six dimensions of eight domains the value exceeded 0.70. The average SF-36 scores of the health-related quality of life dimensions for the patients before admission to intensive care unit were 57.8 for physical functioning, 32.4 for role-physical, 53.0 for bodily pain, 63.2 for general health, 50.6 for vitality, 56.2 for social functioning, 54.6 for role-emotional and 60.3 for mental health. The correlations between severity of illness and length of stay and the health-related quality of life scores were very low, ranging from -0.152 to 0.175 and -0.158 to 0.152, respectively, which were not statistically significant. CONCLUSION: In the sample studied, the SF-36 demonstrated good reliability when used to measure health-related quality of life in critically ill patients before admission to the intensive care unit. The worst score was role-physical and the best was general health. Health-related quality of life of patients before admission was not correlated with severity of illness or length of stay in the intensive care unit.
-
Original Articles – Clinical Research
Diabetes mellitus and impaired glucose tolerance are underdiagnosed in intensive care units
Rev Bras Ter Intensiva. 2012;24(4):347-351
Abstract
Original Articles – Clinical ResearchDiabetes mellitus and impaired glucose tolerance are underdiagnosed in intensive care units
Rev Bras Ter Intensiva. 2012;24(4):347-351
DOI 10.1590/S0103-507X2012000400009
Views0OBJECTIVE: To evaluate the presence of diabetes mellitus and impaired glucose tolerance in intensive care unit inpatients. METHODS: The study included patients in post-surgical care for elective and emergency surgery and excluded those patients with known diabetes mellitus. To diagnose prior serum glucose level disorders, we considered the value of glycated hemoglobin (HbA1c) at the time of admission, classifying the patients as normal (<5.7%), glucose intolerant (5.7-6.4%) or diabetic (>6.4%). During the first 3 days of the patient’s hospital stay, glycemic control and clinical complications were assessed. Mortality was monitored for 28 days. For the statistical analyses, chi-square, ANOVA, student’s t, Kruskal-Wallis or Mann Whitney tests were used. RESULTS: Thirty patients were included in the present study, 53% of whom were women; the patients had a mean age of 53.4±19.7 years and an APACHE II score of 13.6±6.6. The majority of patients were admitted for severe sepsis or septic shock followed by post-operative care for elective surgery, oncological surgery, multiple traumas and emergency surgery. When classifying these patients according to HbA1c, despite the absence of a prior history of diabetes mellitus, only 13.3% had a normal HbA1c level, 23.3% had levels compatible with the diagnosis of diabetes mellitus and 63.3% had levels compatible with impaired glucose tolerance. We found a significant association between the diagnosis of diabetes mellitus or impaired glucose tolerance and the use of vasoactive drugs (p=0.04). CONCLUSION: A high prevalence of undiagnosed diabetes mellitus and impaired glucose tolerance was observed in inpatients at a general intensive care unit.
Keywords:Catecholaminesdiabetes mellitusGlucose metabolism disordersHemoglobina A, glycosylatedhyperglycemiaIntensive careSee moreViews0Abstract
Original Articles – Clinical ResearchDiabetes mellitus and impaired glucose tolerance are underdiagnosed in intensive care units
Rev Bras Ter Intensiva. 2012;24(4):347-351
DOI 10.1590/S0103-507X2012000400009
Views0OBJECTIVE: To evaluate the presence of diabetes mellitus and impaired glucose tolerance in intensive care unit inpatients. METHODS: The study included patients in post-surgical care for elective and emergency surgery and excluded those patients with known diabetes mellitus. To diagnose prior serum glucose level disorders, we considered the value of glycated hemoglobin (HbA1c) at the time of admission, classifying the patients as normal (<5.7%), glucose intolerant (5.7-6.4%) or diabetic (>6.4%). During the first 3 days of the patient’s hospital stay, glycemic control and clinical complications were assessed. Mortality was monitored for 28 days. For the statistical analyses, chi-square, ANOVA, student’s t, Kruskal-Wallis or Mann Whitney tests were used. RESULTS: Thirty patients were included in the present study, 53% of whom were women; the patients had a mean age of 53.4±19.7 years and an APACHE II score of 13.6±6.6. The majority of patients were admitted for severe sepsis or septic shock followed by post-operative care for elective surgery, oncological surgery, multiple traumas and emergency surgery. When classifying these patients according to HbA1c, despite the absence of a prior history of diabetes mellitus, only 13.3% had a normal HbA1c level, 23.3% had levels compatible with the diagnosis of diabetes mellitus and 63.3% had levels compatible with impaired glucose tolerance. We found a significant association between the diagnosis of diabetes mellitus or impaired glucose tolerance and the use of vasoactive drugs (p=0.04). CONCLUSION: A high prevalence of undiagnosed diabetes mellitus and impaired glucose tolerance was observed in inpatients at a general intensive care unit.
Keywords:Catecholaminesdiabetes mellitusGlucose metabolism disordersHemoglobina A, glycosylatedhyperglycemiaIntensive careSee more -
Original Articles – Clinical Research
Influence on prognosis and prevalence of stress hyperglycemia in a cohort of patients with acute coronary syndrome
Rev Bras Ter Intensiva. 2012;24(4):352-356
Abstract
Original Articles – Clinical ResearchInfluence on prognosis and prevalence of stress hyperglycemia in a cohort of patients with acute coronary syndrome
Rev Bras Ter Intensiva. 2012;24(4):352-356
DOI 10.1590/S0103-507X2012000400010
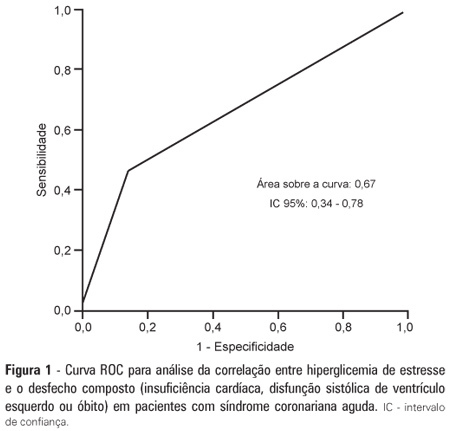
Views0See moreOBJECTIVE: To demonstrate the prevalence of stress hyperglycemia in a cohort of patients with acute coronary syndrome and to determine the correlation of stress hyperglycemia with death, heart failure and/or left ventricular systolic dysfunction during the intrahospital phase. METHODS: A prospective initial cohort study of hospitalized patients with acute coronary syndrome with or without ST segment elevation. The groups were compared to demonstrate the correlation between stress hyperglycemia and cardiovascular events. The chi-square test or Fisher’s exact test and student’s t-test were used to compare the groups with and without stress hyperglycemia. The variables with p<0.20 in the univariate analysis were submitted to logistic regression. RESULTS: In total, 363 patients with an average age of 12.45 ± 62.06 were studied. There was a predominance of males (64.2%). In total, 96 patients (26.4%) presented with stress hyperglycemia. There were no differences between the groups with or without stress hyperglycemia. The area under the ROC curve was 0.67 for the relationship between stress hyperglycemia and the composite outcome heart failure, left ventricular systolic dysfunction or death at the end of the hospital admission. The ROC curve proved that stress hyperglycemia was the predictor of the composite outcome (death, heart failure and/or ventricular dysfunction). The multivariate analysis did not indicate age, stress hyperglycemia or admission heart rate as risk factors. CONCLUSION: Stress hyperglycemia was common in the studied sample. In the univariate analysis, the presence of stress hyperglycemia was associated with such events as death, heart failure and/or intrahospital ventricular dysfunction in patients with acute coronary syndrome.
Views0Abstract
Original Articles – Clinical ResearchInfluence on prognosis and prevalence of stress hyperglycemia in a cohort of patients with acute coronary syndrome
Rev Bras Ter Intensiva. 2012;24(4):352-356
DOI 10.1590/S0103-507X2012000400010
Views0See moreOBJECTIVE: To demonstrate the prevalence of stress hyperglycemia in a cohort of patients with acute coronary syndrome and to determine the correlation of stress hyperglycemia with death, heart failure and/or left ventricular systolic dysfunction during the intrahospital phase. METHODS: A prospective initial cohort study of hospitalized patients with acute coronary syndrome with or without ST segment elevation. The groups were compared to demonstrate the correlation between stress hyperglycemia and cardiovascular events. The chi-square test or Fisher’s exact test and student’s t-test were used to compare the groups with and without stress hyperglycemia. The variables with p<0.20 in the univariate analysis were submitted to logistic regression. RESULTS: In total, 363 patients with an average age of 12.45 ± 62.06 were studied. There was a predominance of males (64.2%). In total, 96 patients (26.4%) presented with stress hyperglycemia. There were no differences between the groups with or without stress hyperglycemia. The area under the ROC curve was 0.67 for the relationship between stress hyperglycemia and the composite outcome heart failure, left ventricular systolic dysfunction or death at the end of the hospital admission. The ROC curve proved that stress hyperglycemia was the predictor of the composite outcome (death, heart failure and/or ventricular dysfunction). The multivariate analysis did not indicate age, stress hyperglycemia or admission heart rate as risk factors. CONCLUSION: Stress hyperglycemia was common in the studied sample. In the univariate analysis, the presence of stress hyperglycemia was associated with such events as death, heart failure and/or intrahospital ventricular dysfunction in patients with acute coronary syndrome.
-
Original Articles – Clinical Research
Financial impact of nosocomial infections in the intensive care units of a charitable hospital in Minas Gerais, Brazil
Rev Bras Ter Intensiva. 2012;24(4):357-361
Abstract
Original Articles – Clinical ResearchFinancial impact of nosocomial infections in the intensive care units of a charitable hospital in Minas Gerais, Brazil
Rev Bras Ter Intensiva. 2012;24(4):357-361
DOI 10.1590/S0103-507X2012000400011
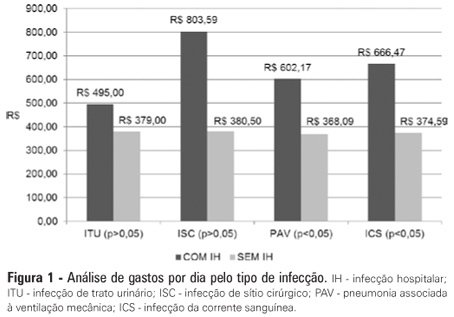
Views0See moreOBJECTIVE: Infections in intensive care units are often associated with a high morbidity and mortality in addition to high costs. An analysis of these aspects can assist in optimizing the allocation of relevant financial resources. METHODS: This retrospective study analyzed the hospital administration and quality in intensive care medical databases [Sistema de Gestão Hospitalar (SGH)] and RM Janus®. A cost analysis was performed by evaluating the medical products and materials used in direct medical care. The costs are reported in the Brazilian national currency (Real). The cost and length of stay analyses were performed for all the costs studied. The median was used to determine the costs involved. Costs were also adjusted by the patients’ length of stay in the intensive care unit. RESULTS: In total, 974 individuals were analyzed, of which 51% were male, and the mean age was 57±18.24 years. There were 87 patients (8.9%) identified who had nosocomial infections associated with the intensive care unit. The median cost per admission and the length of stay for all the patients sampled were R$1.257,53 and 3 days, respectively. Compared to the patients without an infection, the patients with an infection had longer hospital stays (15 [11-25] versus 3 [2-6] days, p<0.01), increased costs per patient in the intensive care unit (median R$9.763,78 [5445.64 - 18,007.90] versus R$1.093,94 [416.14 - 2755.90], p<0.01) and increased costs per day of hospitalization in the intensive care unit (R$618,00 [407.81 - 838.69] versus R$359,00 [174.59 - 719.12], p<0.01). CONCLUSION: Nosocomial infections associated with the intensive care unit were determinants of increased costs and longer hospital stays. However, the study design did not allow us to evaluate specific aspects of cause and effect.
Views0Abstract
Original Articles – Clinical ResearchFinancial impact of nosocomial infections in the intensive care units of a charitable hospital in Minas Gerais, Brazil
Rev Bras Ter Intensiva. 2012;24(4):357-361
DOI 10.1590/S0103-507X2012000400011
Views0See moreOBJECTIVE: Infections in intensive care units are often associated with a high morbidity and mortality in addition to high costs. An analysis of these aspects can assist in optimizing the allocation of relevant financial resources. METHODS: This retrospective study analyzed the hospital administration and quality in intensive care medical databases [Sistema de Gestão Hospitalar (SGH)] and RM Janus®. A cost analysis was performed by evaluating the medical products and materials used in direct medical care. The costs are reported in the Brazilian national currency (Real). The cost and length of stay analyses were performed for all the costs studied. The median was used to determine the costs involved. Costs were also adjusted by the patients’ length of stay in the intensive care unit. RESULTS: In total, 974 individuals were analyzed, of which 51% were male, and the mean age was 57±18.24 years. There were 87 patients (8.9%) identified who had nosocomial infections associated with the intensive care unit. The median cost per admission and the length of stay for all the patients sampled were R$1.257,53 and 3 days, respectively. Compared to the patients without an infection, the patients with an infection had longer hospital stays (15 [11-25] versus 3 [2-6] days, p<0.01), increased costs per patient in the intensive care unit (median R$9.763,78 [5445.64 - 18,007.90] versus R$1.093,94 [416.14 - 2755.90], p<0.01) and increased costs per day of hospitalization in the intensive care unit (R$618,00 [407.81 - 838.69] versus R$359,00 [174.59 - 719.12], p<0.01). CONCLUSION: Nosocomial infections associated with the intensive care unit were determinants of increased costs and longer hospital stays. However, the study design did not allow us to evaluate specific aspects of cause and effect.
-
Original Articles – Clinical Research
Relative adrenal insufficiency as a predictor of disease severity and mortality in severe septic shock
Rev Bras Ter Intensiva. 2012;24(4):362-368
Abstract
Original Articles – Clinical ResearchRelative adrenal insufficiency as a predictor of disease severity and mortality in severe septic shock
Rev Bras Ter Intensiva. 2012;24(4):362-368
DOI 10.1590/S0103-507X2012000400012
Views0OBJECTIVE: To evaluate if cortisol responses to 250 µg of intravenously administered adrenocorticotropic hormone are related to disease severity and, hence, mortality. METHODS: This is a retrospective study in a medical-surgical intensive care unit of a university hospital. We studied 69 consecutive patients with septic shock over a 1-yr period; these patients underwent a short 250-µg adrenocorticotropic hormone test because they exhibited >6 hours of progressive hemodynamic instability requiring repeated fluid challenges and vasopressor treatment to maintain blood pressure. The test was performed by intravenously injecting 250 µg of synthetic adrenocorticotropic hormone and measuring cortisol immediately before injection, 30 minutes post-injection and 60 minutes post-injection. RESULTS: The mean APACHE II score was 22±7. The intensive care unit mortality rate at day 28 was 55%. Median baseline cortisol levels (19 [11-27] µg/dL versus 24 [18-34] µg/dL, p=0.047) and median baseline cortisol/albumin ratios (7.6 [4.6-12.3] versus 13.9 [8.8-18.5]; p=0.01) were lower in survivors than in non-survivors. Responders and non-responders had similar baseline clinical data and outcomes. The variables that were significantly correlated with outcome based on the area under the ROC curves (AUC) were APACHE II (AUC=0.67 [0.535 to 0.781]), baseline cortisol (µg/dl) (AUC=0.662 [0.536 to 0.773], peak cortisol (µg/dl) (AUC=0.642 [0.515 to 0.755]) and baseline cortisol/albumin (AUC=0.75 [0.621 to 0.849]). CONCLUSIONS: Increased basal cortisol is associated with mortality and disease severity. Cortisol responses upon adrenocorticotropic hormone stimulation were not related to outcome. The cortisol/albumin ratio does not predict unfavorable outcomes better than total cortisol levels or help to improve the accuracy of the adrenocorticotropic hormone test.
Keywords:adrenal insufficiencyAdrenocorticotropic hormoneCritical illnessHydrocortisoneShock, septicSee moreViews0Abstract
Original Articles – Clinical ResearchRelative adrenal insufficiency as a predictor of disease severity and mortality in severe septic shock
Rev Bras Ter Intensiva. 2012;24(4):362-368
DOI 10.1590/S0103-507X2012000400012
Views0OBJECTIVE: To evaluate if cortisol responses to 250 µg of intravenously administered adrenocorticotropic hormone are related to disease severity and, hence, mortality. METHODS: This is a retrospective study in a medical-surgical intensive care unit of a university hospital. We studied 69 consecutive patients with septic shock over a 1-yr period; these patients underwent a short 250-µg adrenocorticotropic hormone test because they exhibited >6 hours of progressive hemodynamic instability requiring repeated fluid challenges and vasopressor treatment to maintain blood pressure. The test was performed by intravenously injecting 250 µg of synthetic adrenocorticotropic hormone and measuring cortisol immediately before injection, 30 minutes post-injection and 60 minutes post-injection. RESULTS: The mean APACHE II score was 22±7. The intensive care unit mortality rate at day 28 was 55%. Median baseline cortisol levels (19 [11-27] µg/dL versus 24 [18-34] µg/dL, p=0.047) and median baseline cortisol/albumin ratios (7.6 [4.6-12.3] versus 13.9 [8.8-18.5]; p=0.01) were lower in survivors than in non-survivors. Responders and non-responders had similar baseline clinical data and outcomes. The variables that were significantly correlated with outcome based on the area under the ROC curves (AUC) were APACHE II (AUC=0.67 [0.535 to 0.781]), baseline cortisol (µg/dl) (AUC=0.662 [0.536 to 0.773], peak cortisol (µg/dl) (AUC=0.642 [0.515 to 0.755]) and baseline cortisol/albumin (AUC=0.75 [0.621 to 0.849]). CONCLUSIONS: Increased basal cortisol is associated with mortality and disease severity. Cortisol responses upon adrenocorticotropic hormone stimulation were not related to outcome. The cortisol/albumin ratio does not predict unfavorable outcomes better than total cortisol levels or help to improve the accuracy of the adrenocorticotropic hormone test.
Keywords:adrenal insufficiencyAdrenocorticotropic hormoneCritical illnessHydrocortisoneShock, septicSee more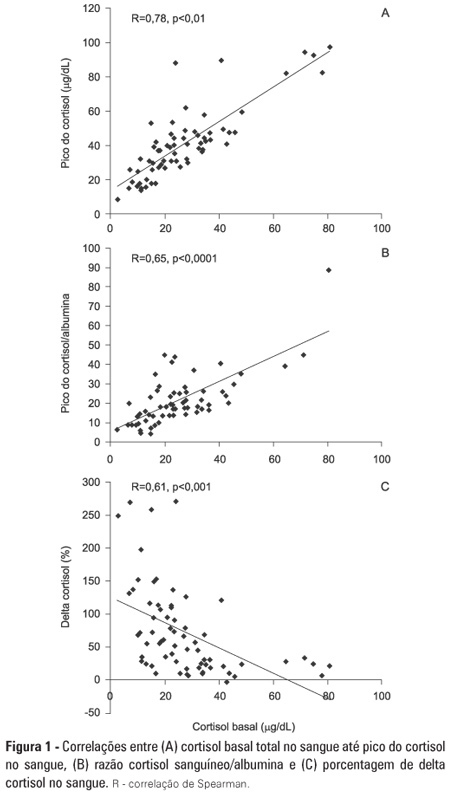
-
Original Articles – Clinical Research
The use of 2% chlorhexidine gel and toothbrushing for oral hygiene of patients receiving mechanical ventilation: effects on ventilator-associated pneumonia
Rev Bras Ter Intensiva. 2012;24(4):369-374
Abstract
Original Articles – Clinical ResearchThe use of 2% chlorhexidine gel and toothbrushing for oral hygiene of patients receiving mechanical ventilation: effects on ventilator-associated pneumonia
Rev Bras Ter Intensiva. 2012;24(4):369-374
DOI 10.1590/S0103-507X2012000400013
Views0OBJECTIVE: To evaluate the effects of oral chlorhexidine hygiene with toothbrushing on the rate of ventilator-associated pneumonia in a mixed population of critically ill patients under prolonged mechanical ventilation. METHODS: Prospective, randomized, and placebo-controlled pilot study. Patients who were receiving mechanical ventilation, had been admitted less than 24 hours prior, and were anticipated to require mechanical ventilation for more than 72 hours were included in the study. The patients were randomly divided into one of the following groups: chlorhexidine hygiene with toothbrushing or a placebo group (gel with the same color and consistency and toothbrushing). RESULTS: The planned interim analysis was conducted using 52 patients, and the study was terminated prematurely. In total, 28 patients were included in the chlorhexidine / toothbrushing group, and 24 patients were included in the placebo group. Ventilator-associated pneumonia occurred in 45.8% of the placebo group and in 64.3% of the chlorhexidine hygiene with toothbrushing group (RR=1.4; 95% CI=0.83-2.34; p=0.29). CONCLUSION: Because the study was terminated due to futility, it was not possible to evaluate the impact of oral hygiene using 2% chlorhexidine and toothbrushing on the incidence of ventilator-associated pneumonia in this heterogeneous population of critical patients receiving long-term mechanical ventilation, and no beneficial effect was observed for this intervention.
Keywords:ChlorhexidineIntensive care unitsManual brushingOral hygienePlacebosPneumonia, ventilator-associatedSee moreViews0Abstract
Original Articles – Clinical ResearchThe use of 2% chlorhexidine gel and toothbrushing for oral hygiene of patients receiving mechanical ventilation: effects on ventilator-associated pneumonia
Rev Bras Ter Intensiva. 2012;24(4):369-374
DOI 10.1590/S0103-507X2012000400013
Views0OBJECTIVE: To evaluate the effects of oral chlorhexidine hygiene with toothbrushing on the rate of ventilator-associated pneumonia in a mixed population of critically ill patients under prolonged mechanical ventilation. METHODS: Prospective, randomized, and placebo-controlled pilot study. Patients who were receiving mechanical ventilation, had been admitted less than 24 hours prior, and were anticipated to require mechanical ventilation for more than 72 hours were included in the study. The patients were randomly divided into one of the following groups: chlorhexidine hygiene with toothbrushing or a placebo group (gel with the same color and consistency and toothbrushing). RESULTS: The planned interim analysis was conducted using 52 patients, and the study was terminated prematurely. In total, 28 patients were included in the chlorhexidine / toothbrushing group, and 24 patients were included in the placebo group. Ventilator-associated pneumonia occurred in 45.8% of the placebo group and in 64.3% of the chlorhexidine hygiene with toothbrushing group (RR=1.4; 95% CI=0.83-2.34; p=0.29). CONCLUSION: Because the study was terminated due to futility, it was not possible to evaluate the impact of oral hygiene using 2% chlorhexidine and toothbrushing on the incidence of ventilator-associated pneumonia in this heterogeneous population of critical patients receiving long-term mechanical ventilation, and no beneficial effect was observed for this intervention.
Keywords:ChlorhexidineIntensive care unitsManual brushingOral hygienePlacebosPneumonia, ventilator-associatedSee more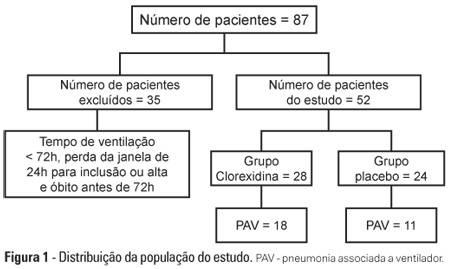
-
Original Articles – Clinical Research
Noninvasive ventilation in acute respiratory failure from respiratory syncytial virus bronchiolitis
Rev Bras Ter Intensiva. 2012;24(4):375-380
Abstract
Original Articles – Clinical ResearchNoninvasive ventilation in acute respiratory failure from respiratory syncytial virus bronchiolitis
Rev Bras Ter Intensiva. 2012;24(4):375-380
DOI 10.1590/S0103-507X2012000400014
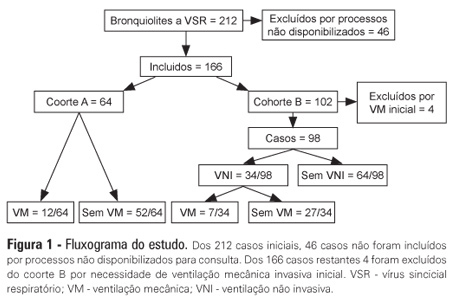
Views0See moreOBJECTIVES: The present study focused on respiratory syncytial virus bronchiolitis with respiratory failure. The aim of the study was to determine whether noninvasive ventilation reduces the need for endotracheal intubation or slows the clinical progression of acute respiratory syncytial virus bronchiolitis by reducing the incidence of infectious complications. METHODS: The present study was a retrospective cohort study. Cohort A was comprised of children who were admitted to the pediatric intensive and special care unit from 2003-2005 before starting noninvasive ventilation; cohort B was comprised of children who were admitted to the pediatric intensive and special care unit from 2006-2008 after starting noninvasive ventilation. With the exception of noninvasive ventilation, the therapeutic support was the same for the two groups. All children who were diagnosed with respiratory syncytial virus bronchiolitis and respiratory failure between November 2003 and March 2008 were included in the cohort. Demographic, clinical and blood gas variables were analyzed. RESULTS: A total of 162 children were included; 75% of the subjects were less than 3 months old. Group A included 64 children, and group B included 98 children. In group B, 34 of the children required noninvasive ventilation. The distributions of the variables age, preterm birth, congenital heart disease, cerebral palsy and chronic lung disease were similar between the two groups. On admission, the data for blood gas analysis and the number of apneas were not significantly different between the groups. In group B, fewer children required invasive ventilation (group A: 12/64 versus group B: 7/98; p=0.02), and there was a reduction in the number of cases of bacterial pneumonia (group A: 19/64 versus group B: 12/98; p=0.008). There was no record of mortality in either of the groups. CONCLUSION: By comparing children with the same disease both before and after noninvasive ventilation was used for ventilation support, we verified a reduction in infectious complications and cases requiring intubation.
Views0Abstract
Original Articles – Clinical ResearchNoninvasive ventilation in acute respiratory failure from respiratory syncytial virus bronchiolitis
Rev Bras Ter Intensiva. 2012;24(4):375-380
DOI 10.1590/S0103-507X2012000400014
Views0See moreOBJECTIVES: The present study focused on respiratory syncytial virus bronchiolitis with respiratory failure. The aim of the study was to determine whether noninvasive ventilation reduces the need for endotracheal intubation or slows the clinical progression of acute respiratory syncytial virus bronchiolitis by reducing the incidence of infectious complications. METHODS: The present study was a retrospective cohort study. Cohort A was comprised of children who were admitted to the pediatric intensive and special care unit from 2003-2005 before starting noninvasive ventilation; cohort B was comprised of children who were admitted to the pediatric intensive and special care unit from 2006-2008 after starting noninvasive ventilation. With the exception of noninvasive ventilation, the therapeutic support was the same for the two groups. All children who were diagnosed with respiratory syncytial virus bronchiolitis and respiratory failure between November 2003 and March 2008 were included in the cohort. Demographic, clinical and blood gas variables were analyzed. RESULTS: A total of 162 children were included; 75% of the subjects were less than 3 months old. Group A included 64 children, and group B included 98 children. In group B, 34 of the children required noninvasive ventilation. The distributions of the variables age, preterm birth, congenital heart disease, cerebral palsy and chronic lung disease were similar between the two groups. On admission, the data for blood gas analysis and the number of apneas were not significantly different between the groups. In group B, fewer children required invasive ventilation (group A: 12/64 versus group B: 7/98; p=0.02), and there was a reduction in the number of cases of bacterial pneumonia (group A: 19/64 versus group B: 12/98; p=0.008). There was no record of mortality in either of the groups. CONCLUSION: By comparing children with the same disease both before and after noninvasive ventilation was used for ventilation support, we verified a reduction in infectious complications and cases requiring intubation.
-
Original Articles – Clinical Research
Nosocomial infections in a neonatal intensive care unit in South Brazil
Rev Bras Ter Intensiva. 2012;24(4):381-385
Abstract
Original Articles – Clinical ResearchNosocomial infections in a neonatal intensive care unit in South Brazil
Rev Bras Ter Intensiva. 2012;24(4):381-385
DOI 10.1590/S0103-507X2012000400015
Views0See moreOBJECTIVE: The aim of this study was to describe the incidence and epidemiology of nosocomial infection in newborns who were admitted to a neonatal intensive care unit in a hospital in south Santa Catarina, Brazil. METHODS: A prospective cohort study was conducted for 1 year among 239 neonates who remained as in-patients 48 hours after admission. The criteria that were used to diagnose infection were in accordance with the Centers for Disease Control and Prevention and the National Health Surveillance Agency. RESULTS: The incidence of nosocomial infection was 45.8%. The primary reasons for admission were primary bloodstream infection (80.7%) and pneumonia (6.7%). Coagulase-negative Staphylococcus was the most commonly identified agent in the blood cultures and in the hospital unit. Prematurity was the most prevalent reason for admission. The general mortality rate was 12.1%, and mortality from nosocomial infection was 33.8%. CONCLUSIONS: The incidence of nosocomial infection in the hospital unit was higher than rates that have been reported in other national studies. The major types of nosocomial infection were primary bloodstream infection and pneumonia.
Views0Abstract
Original Articles – Clinical ResearchNosocomial infections in a neonatal intensive care unit in South Brazil
Rev Bras Ter Intensiva. 2012;24(4):381-385
DOI 10.1590/S0103-507X2012000400015
Views0See moreOBJECTIVE: The aim of this study was to describe the incidence and epidemiology of nosocomial infection in newborns who were admitted to a neonatal intensive care unit in a hospital in south Santa Catarina, Brazil. METHODS: A prospective cohort study was conducted for 1 year among 239 neonates who remained as in-patients 48 hours after admission. The criteria that were used to diagnose infection were in accordance with the Centers for Disease Control and Prevention and the National Health Surveillance Agency. RESULTS: The incidence of nosocomial infection was 45.8%. The primary reasons for admission were primary bloodstream infection (80.7%) and pneumonia (6.7%). Coagulase-negative Staphylococcus was the most commonly identified agent in the blood cultures and in the hospital unit. Prematurity was the most prevalent reason for admission. The general mortality rate was 12.1%, and mortality from nosocomial infection was 33.8%. CONCLUSIONS: The incidence of nosocomial infection in the hospital unit was higher than rates that have been reported in other national studies. The major types of nosocomial infection were primary bloodstream infection and pneumonia.
-
Original Articles – Clinical Research
Epidemiological characteristics and deaths of premature infants in a referral hospital for high-risk pregnancies
Rev Bras Ter Intensiva. 2012;24(4):386-392
Abstract
Original Articles – Clinical ResearchEpidemiological characteristics and deaths of premature infants in a referral hospital for high-risk pregnancies
Rev Bras Ter Intensiva. 2012;24(4):386-392
DOI 10.1590/S0103-507X2012000400016
Views0OBJECTIVE: To analyze the process of care provided to premature infants in a neonatal intensive care unit and the factors associated with their mortality. METHODS: Cross-sectional retrospective study of premature infants in an intensive care unit between 2008 and 2010. The characteristics of the mothers and premature infants were described, and a bivariate analysis was performed on the following characteristics: the study period and the “death” outcome (hospital, neonatal and early) using Pearson’s chi-square test, Fisher’s exact test or a chi-square test for linear trends. Bivariate and multivariable logistic regression analyses were performed using a stepwise backward logistic regression method between the variables with p<0.20 and the "death" outcome. A p value <0.05 was considered to be significant. RESULTS: In total, 293 preterm infants were studied. Increased access to complementary tests (transfontanellar ultrasound and Doppler echocardiogram) and breastfeeding rates were indicators of improving care. Mortality was concentrated in the neonatal period, especially in the early neonatal period, and was associated with extreme prematurity, small size for gestational age and an Apgar score <7 at 5 minutes after birth. The late-onset sepsis was also associated with a greater chance of neonatal death, and antenatal corticosteroids were protective against neonatal and early deaths. CONCLUSIONS: Although these results are comparable to previous findings regarding mortality among premature infants in Brazil, the study emphasizes the need to implement strategies that promote breastfeeding and reduce neonatal mortality and its early component.
Keywords:Breast feedingEarly neonatal mortalityInfant, prematureIntensive care, neonatalNeonatal mortality (Public Health)Perinatal careSepsisSee moreViews0Abstract
Original Articles – Clinical ResearchEpidemiological characteristics and deaths of premature infants in a referral hospital for high-risk pregnancies
Rev Bras Ter Intensiva. 2012;24(4):386-392
DOI 10.1590/S0103-507X2012000400016
Views0OBJECTIVE: To analyze the process of care provided to premature infants in a neonatal intensive care unit and the factors associated with their mortality. METHODS: Cross-sectional retrospective study of premature infants in an intensive care unit between 2008 and 2010. The characteristics of the mothers and premature infants were described, and a bivariate analysis was performed on the following characteristics: the study period and the “death” outcome (hospital, neonatal and early) using Pearson’s chi-square test, Fisher’s exact test or a chi-square test for linear trends. Bivariate and multivariable logistic regression analyses were performed using a stepwise backward logistic regression method between the variables with p<0.20 and the "death" outcome. A p value <0.05 was considered to be significant. RESULTS: In total, 293 preterm infants were studied. Increased access to complementary tests (transfontanellar ultrasound and Doppler echocardiogram) and breastfeeding rates were indicators of improving care. Mortality was concentrated in the neonatal period, especially in the early neonatal period, and was associated with extreme prematurity, small size for gestational age and an Apgar score <7 at 5 minutes after birth. The late-onset sepsis was also associated with a greater chance of neonatal death, and antenatal corticosteroids were protective against neonatal and early deaths. CONCLUSIONS: Although these results are comparable to previous findings regarding mortality among premature infants in Brazil, the study emphasizes the need to implement strategies that promote breastfeeding and reduce neonatal mortality and its early component.
Keywords:Breast feedingEarly neonatal mortalityInfant, prematureIntensive care, neonatalNeonatal mortality (Public Health)Perinatal careSepsisSee more -
Review Articles
Plasmodium falciparum malaria: proteomic studies
Rev Bras Ter Intensiva. 2012;24(4):394-400
Abstract
Review ArticlesPlasmodium falciparum malaria: proteomic studies
Rev Bras Ter Intensiva. 2012;24(4):394-400
DOI 10.1590/S0103-507X2012000400017
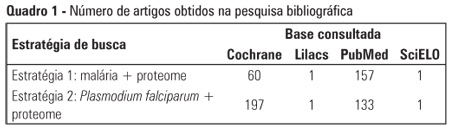
Views0See moreDespite advances in treatment and campaigns for prevention and control of malaria on the various continents where it is still rampant, this disease remains significantly relevant to the contemporary world. Plasmodium falciparum is the organism that is mainly responsible for severe malaria, which is characterized by disturbances in different organs and systems, with possibly fatal outcomes. Although incipient, proteomic studies of malaria have yielded favorable prospects for elucidating the biological aspects of Plasmodium as well as the pathophysiological, diagnostic, prophylactic, and therapeutic mechanisms of the disease. Thus, the aim of the present article is to present a brief review of the applications of proteomic analysis in P. falciparum malaria.
Views0Abstract
Review ArticlesPlasmodium falciparum malaria: proteomic studies
Rev Bras Ter Intensiva. 2012;24(4):394-400
DOI 10.1590/S0103-507X2012000400017
Views0See moreDespite advances in treatment and campaigns for prevention and control of malaria on the various continents where it is still rampant, this disease remains significantly relevant to the contemporary world. Plasmodium falciparum is the organism that is mainly responsible for severe malaria, which is characterized by disturbances in different organs and systems, with possibly fatal outcomes. Although incipient, proteomic studies of malaria have yielded favorable prospects for elucidating the biological aspects of Plasmodium as well as the pathophysiological, diagnostic, prophylactic, and therapeutic mechanisms of the disease. Thus, the aim of the present article is to present a brief review of the applications of proteomic analysis in P. falciparum malaria.
-
Review Articles
Impact of supra-cuff suction on ventilator-associated pneumonia prevention
Rev Bras Ter Intensiva. 2012;24(4):401-406
Abstract
Review ArticlesImpact of supra-cuff suction on ventilator-associated pneumonia prevention
Rev Bras Ter Intensiva. 2012;24(4):401-406
DOI 10.1590/S0103-507X2012000400018
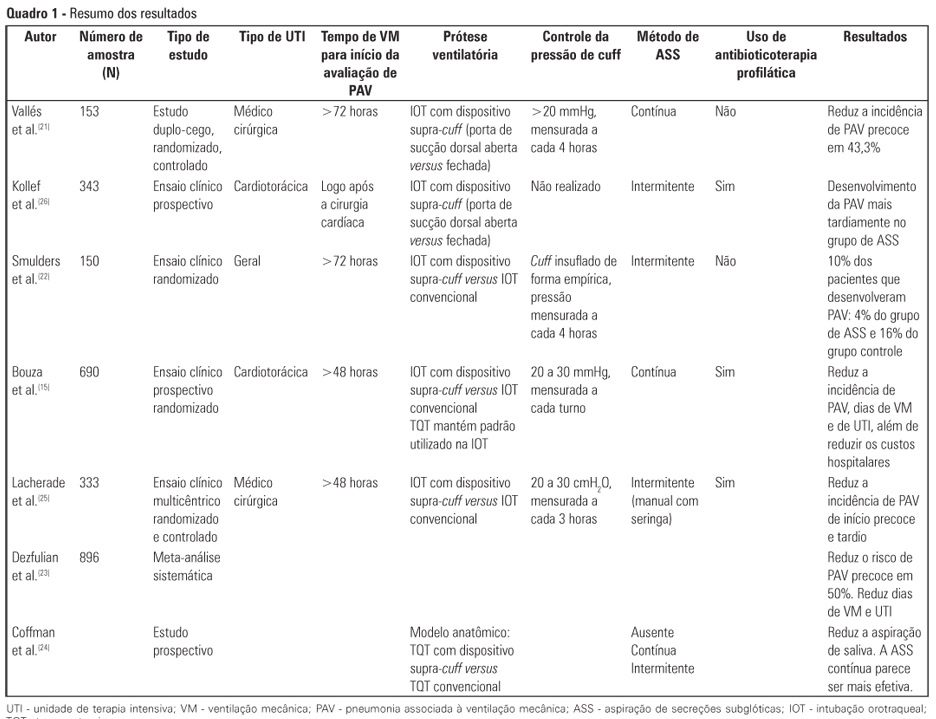
Views0See moreCritically ill patients are intubated or tracheostomized because, in most cases, these individuals require invasive mechanical ventilation. The cannulae that are used include the cuff, which can act as a reservoir for oropharyngeal secretions, predisposing to ventilator-associated pneumonia. Studies have revealed that the suction of subglottic secretions through the dorsal suction lumen above the endotracheal tube cuff delays the onset and reduces the incidence of ventilator-associated pneumonia. The aim of this review is to assess published studies regarding the significance of using suction with a supra-cuff device for the prevention of ventilator-associated pneumonia in critically ill patients treated with orotracheal intubation or tracheostomy. Therefore, by searching national and international databases, a literature review was undertaken of studies published between the years 1986 and 2011. Few results were found relating the suction of subglottic secretions to decreased duration of mechanical ventilation and length of stay in the intensive care unit. The suction of subglottic secretions is ineffective in decreasing mortality but is effective in reducing the incidence of early-onset ventilator-associated pneumonia and hospital costs. Techniques involving continuous suction of subglottic secretions may be particularly efficient in removing secretions; however, intermittent suction appears to be the least harmful method. In conclusion, cannulae with a supra-cuff suction device enable the aspiration of subglottic secretions, providing benefits to critically ill patients by reducing the incidence of ventilator-associated pneumonia and, consequently, hospital costs – with no large-scale adverse effects.
Views0Abstract
Review ArticlesImpact of supra-cuff suction on ventilator-associated pneumonia prevention
Rev Bras Ter Intensiva. 2012;24(4):401-406
DOI 10.1590/S0103-507X2012000400018
Views0See moreCritically ill patients are intubated or tracheostomized because, in most cases, these individuals require invasive mechanical ventilation. The cannulae that are used include the cuff, which can act as a reservoir for oropharyngeal secretions, predisposing to ventilator-associated pneumonia. Studies have revealed that the suction of subglottic secretions through the dorsal suction lumen above the endotracheal tube cuff delays the onset and reduces the incidence of ventilator-associated pneumonia. The aim of this review is to assess published studies regarding the significance of using suction with a supra-cuff device for the prevention of ventilator-associated pneumonia in critically ill patients treated with orotracheal intubation or tracheostomy. Therefore, by searching national and international databases, a literature review was undertaken of studies published between the years 1986 and 2011. Few results were found relating the suction of subglottic secretions to decreased duration of mechanical ventilation and length of stay in the intensive care unit. The suction of subglottic secretions is ineffective in decreasing mortality but is effective in reducing the incidence of early-onset ventilator-associated pneumonia and hospital costs. Techniques involving continuous suction of subglottic secretions may be particularly efficient in removing secretions; however, intermittent suction appears to be the least harmful method. In conclusion, cannulae with a supra-cuff suction device enable the aspiration of subglottic secretions, providing benefits to critically ill patients by reducing the incidence of ventilator-associated pneumonia and, consequently, hospital costs – with no large-scale adverse effects.
-
Review Articles
Vascular access through the intraosseous route in pediatric emergencies
Rev Bras Ter Intensiva. 2012;24(4):407-414
Abstract
Review ArticlesVascular access through the intraosseous route in pediatric emergencies
Rev Bras Ter Intensiva. 2012;24(4):407-414
DOI 10.1590/S0103-507X2012000400019
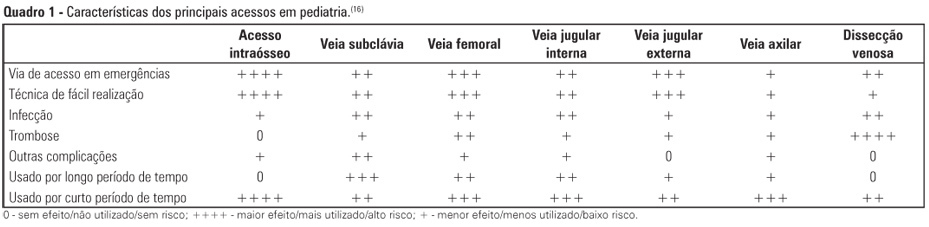
Views0See moreObtaining venous access in critically ill children is an essential procedure to restore blood volume and administer drugs during pediatric emergencies. The first option for vascular access is through a peripheral vein puncture. If this route cannot be used or if a prolonged period of access is necessary, then the intraosseous route is an effective option for rapid and safe venous access. The present work is a descriptive and exploratory literature review. The study’s aim was to describe the techniques, professional responsibilities, and care related to obtaining venous access via the intraosseous route in pediatric emergencies. We selected 22 articles (published between 2000 and 2011) that were available in the Latin American and Caribbean Health Sciences (LILACS) and MEDLINE databases and the SciELO electronic library, in addition to the current protocol of cardiopulmonary resuscitation from the American Heart Association (2010). After the literature search, data were pooled and grouped into the following categories of analysis: historical aspects and physiological principles; indications, benefits, and contraindications; professional assignments; technical principles; care during the access; and possible complications. The results of the present study revealed that the intraosseous route is considered the main secondary option for vascular access during the emergency response because the technique is quick and easily executed, presents several non-collapsible puncture sites, and enables the rapid and effective administration of drugs and fluid replacement.
Views0Abstract
Review ArticlesVascular access through the intraosseous route in pediatric emergencies
Rev Bras Ter Intensiva. 2012;24(4):407-414
DOI 10.1590/S0103-507X2012000400019
Views0See moreObtaining venous access in critically ill children is an essential procedure to restore blood volume and administer drugs during pediatric emergencies. The first option for vascular access is through a peripheral vein puncture. If this route cannot be used or if a prolonged period of access is necessary, then the intraosseous route is an effective option for rapid and safe venous access. The present work is a descriptive and exploratory literature review. The study’s aim was to describe the techniques, professional responsibilities, and care related to obtaining venous access via the intraosseous route in pediatric emergencies. We selected 22 articles (published between 2000 and 2011) that were available in the Latin American and Caribbean Health Sciences (LILACS) and MEDLINE databases and the SciELO electronic library, in addition to the current protocol of cardiopulmonary resuscitation from the American Heart Association (2010). After the literature search, data were pooled and grouped into the following categories of analysis: historical aspects and physiological principles; indications, benefits, and contraindications; professional assignments; technical principles; care during the access; and possible complications. The results of the present study revealed that the intraosseous route is considered the main secondary option for vascular access during the emergency response because the technique is quick and easily executed, presents several non-collapsible puncture sites, and enables the rapid and effective administration of drugs and fluid replacement.
-
Case Report
Acute respiratory failure caused by organizing pneumonia secondary to antineoplastic therapy for non-Hodgkin’s lymphoma
Rev Bras Ter Intensiva. 2012;24(4):415-419
Abstract
Case ReportAcute respiratory failure caused by organizing pneumonia secondary to antineoplastic therapy for non-Hodgkin’s lymphoma
Rev Bras Ter Intensiva. 2012;24(4):415-419
DOI 10.1590/S0103-507X2012000400020
Views0Interstitial lung diseases belong to a group of diseases that typically exhibit a subacute or chronic progression but that may cause acute respiratory failure. The male patient, who was 37 years of age and undergoing therapy for non-Hodgkin’s lymphoma, was admitted with cough, fever, dyspnea and acute hypoxemic respiratory failure. Mechanical ventilation and antibiotic therapy were initiated but were associated with unfavorable progression. Thoracic computed tomography showed bilateral pulmonary “ground glass” opacities. Methylprednisolone pulse therapy was initiated with satisfactory response because the patient had used three drugs related to organizing pneumonia (cyclophosphamide, doxorubicin and rituximab), and the clinical and radiological symptoms were suggestive. Organizing pneumonia may be idiopathic or linked to collagen diseases, drugs and cancer and usually responds to corticosteroid therapy. The diagnosis was anatomopathological, but the patient’s clinical condition precluded performing a lung biopsy. Organizing pneumonia should be a differential diagnosis in patients with apparent pneumonia and a progression that is unfavorable to antimicrobial treatment.
Keywords:Case reportsCryptogenic organizing pneumoniaDrug toxicityLung diseases, interstitialLymphoma, non-HodgkinRespiratory insufficiencyTomography, X-ray computedSee moreViews0Abstract
Case ReportAcute respiratory failure caused by organizing pneumonia secondary to antineoplastic therapy for non-Hodgkin’s lymphoma
Rev Bras Ter Intensiva. 2012;24(4):415-419
DOI 10.1590/S0103-507X2012000400020
Views0Interstitial lung diseases belong to a group of diseases that typically exhibit a subacute or chronic progression but that may cause acute respiratory failure. The male patient, who was 37 years of age and undergoing therapy for non-Hodgkin’s lymphoma, was admitted with cough, fever, dyspnea and acute hypoxemic respiratory failure. Mechanical ventilation and antibiotic therapy were initiated but were associated with unfavorable progression. Thoracic computed tomography showed bilateral pulmonary “ground glass” opacities. Methylprednisolone pulse therapy was initiated with satisfactory response because the patient had used three drugs related to organizing pneumonia (cyclophosphamide, doxorubicin and rituximab), and the clinical and radiological symptoms were suggestive. Organizing pneumonia may be idiopathic or linked to collagen diseases, drugs and cancer and usually responds to corticosteroid therapy. The diagnosis was anatomopathological, but the patient’s clinical condition precluded performing a lung biopsy. Organizing pneumonia should be a differential diagnosis in patients with apparent pneumonia and a progression that is unfavorable to antimicrobial treatment.
Keywords:Case reportsCryptogenic organizing pneumoniaDrug toxicityLung diseases, interstitialLymphoma, non-HodgkinRespiratory insufficiencyTomography, X-ray computedSee more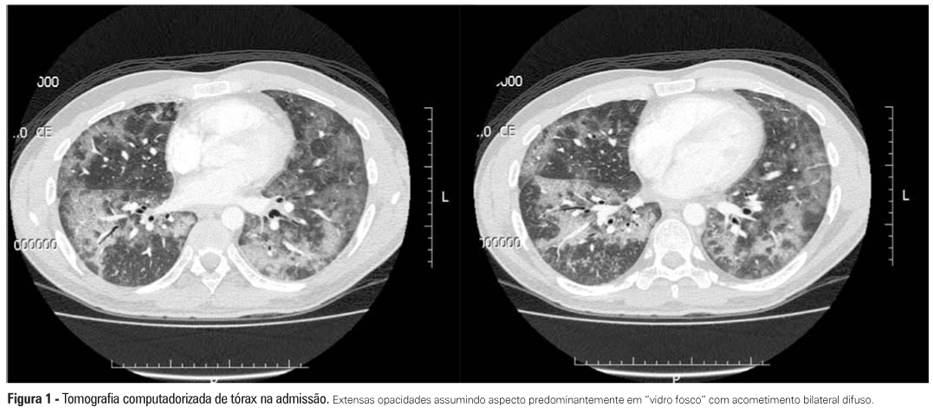
Volume Articles - Critical Care Science (CCS)
