-
Editorial
The new frontiers of acute kidney injury
Rev Bras Ter Intensiva. 2012;24(3):213-215
Abstract
Views0

-
Editorial
Why is it important to assess indications for red blood cell transfusion in premature infants?
Rev Bras Ter Intensiva. 2012;24(3):216-218
Abstract
EditorialWhy is it important to assess indications for red blood cell transfusion in premature infants?
Rev Bras Ter Intensiva. 2012;24(3):216-218
Views0Abstract
EditorialWhy is it important to assess indications for red blood cell transfusion in premature infants?
Rev Bras Ter Intensiva. 2012;24(3):216-218
-
Original Article – Basic Research
N-acetylcysteine and deferrioxamine protects against acute renal failure induced by ischemia/reperfusion in rats
Rev Bras Ter Intensiva. 2012;24(3):219-223
Abstract
Original Article – Basic ResearchN-acetylcysteine and deferrioxamine protects against acute renal failure induced by ischemia/reperfusion in rats
Rev Bras Ter Intensiva. 2012;24(3):219-223
DOI 10.1590/S0103-507X2012000300003
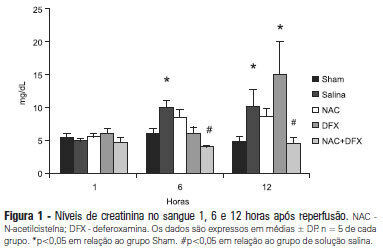
Views0See moreOBJECTIVE: Antioxidants are widely used in animal models to prevent renal injury after ischemia/reperfusion, but it is unknown if the benefits of antioxidants are additive. In this study, we aimed to investigate the protective effects of N-acetylcysteine plus deferoxamine in an animal model of kidney ischemia/reperfusion injury. METHODS: Bilateral kidney ischemia was mastintained for 45 minutes. N-acetylcysteine, deferoxamine or both were administered into the aorta above the renal arteries immediately prior to induction of ischemia. Five rats from each group were sacrificed 1, 6 or 12 hours after reperfusion for the determination of blood creatinine, kidney oxidative damage parameters and myeloperoxidase activity. RESULTS: The combination of N-acetylcysteine and deferoxamine, but not their isolated use, prevented the increase in creatinine after ischemia/reperfusion. This prevention was followed by a consistent decrease in myeloperoxidase activity and oxidative damage parameters both in the kidney cortex and medulla. CONCLUSION: Treatment with N-acetylcysteine and deferoxamine was superior to the isolated use of either compound in an animal model of kidney ischemia/reperfusion.
Views0Abstract
Original Article – Basic ResearchN-acetylcysteine and deferrioxamine protects against acute renal failure induced by ischemia/reperfusion in rats
Rev Bras Ter Intensiva. 2012;24(3):219-223
DOI 10.1590/S0103-507X2012000300003
Views0See moreOBJECTIVE: Antioxidants are widely used in animal models to prevent renal injury after ischemia/reperfusion, but it is unknown if the benefits of antioxidants are additive. In this study, we aimed to investigate the protective effects of N-acetylcysteine plus deferoxamine in an animal model of kidney ischemia/reperfusion injury. METHODS: Bilateral kidney ischemia was mastintained for 45 minutes. N-acetylcysteine, deferoxamine or both were administered into the aorta above the renal arteries immediately prior to induction of ischemia. Five rats from each group were sacrificed 1, 6 or 12 hours after reperfusion for the determination of blood creatinine, kidney oxidative damage parameters and myeloperoxidase activity. RESULTS: The combination of N-acetylcysteine and deferoxamine, but not their isolated use, prevented the increase in creatinine after ischemia/reperfusion. This prevention was followed by a consistent decrease in myeloperoxidase activity and oxidative damage parameters both in the kidney cortex and medulla. CONCLUSION: Treatment with N-acetylcysteine and deferoxamine was superior to the isolated use of either compound in an animal model of kidney ischemia/reperfusion.
-
Original Articles – Clinical Research
Factors associated with packed red blood cell transfusions in premature infants in an intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):224-229
Abstract
Original Articles – Clinical ResearchFactors associated with packed red blood cell transfusions in premature infants in an intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):224-229
DOI 10.1590/S0103-507X2012000300004
Views0See moreOBJECTIVE: This study analyzed the factors that are associated with the need for packed red blood cell transfusions in premature infants in a neonatal intensive care unit. METHODS: This study is a cross-sectional study of secondary data from premature infants who were admitted to a neonatal intensive care unit between 2008 and 2010. Premature infants with low birth weight were included. Packed red blood cell transfusion was the dependent variable. Pearson’s Chi-square or Fisher’s exact tests were used for data analysis, and the median, minimum, and maximum values were calculated. Prevalence ratios were calculated using the Poisson regression and Pearson correlation coefficient. Linear regression analyses were performed. P < 0.05 was considered to be significant. RESULTS: We examined 254 premature infants, and 39.4% of this sample received packed red blood cells. Transfusions were 70% less prevalent in premature infants who were born at >32 weeks of gestation, and 191% more prevalent in infants who exhibited late-onset neonatal sepsis. The number of transfusions per patient was negatively correlated with gestational age and positively correlated with late-onset neonatal sepsis. A gestational age <32 weeks and late-onset neonatal sepsis explained 45% of the transfusions (p<0.0001). CONCLUSIONS: Premature infants with a gestational age <32 weeks and who developed late-onset neonatal sepsis exhibited a greater need for packed red blood cell transfusions.
Views0Abstract
Original Articles – Clinical ResearchFactors associated with packed red blood cell transfusions in premature infants in an intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):224-229
DOI 10.1590/S0103-507X2012000300004
Views0See moreOBJECTIVE: This study analyzed the factors that are associated with the need for packed red blood cell transfusions in premature infants in a neonatal intensive care unit. METHODS: This study is a cross-sectional study of secondary data from premature infants who were admitted to a neonatal intensive care unit between 2008 and 2010. Premature infants with low birth weight were included. Packed red blood cell transfusion was the dependent variable. Pearson’s Chi-square or Fisher’s exact tests were used for data analysis, and the median, minimum, and maximum values were calculated. Prevalence ratios were calculated using the Poisson regression and Pearson correlation coefficient. Linear regression analyses were performed. P < 0.05 was considered to be significant. RESULTS: We examined 254 premature infants, and 39.4% of this sample received packed red blood cells. Transfusions were 70% less prevalent in premature infants who were born at >32 weeks of gestation, and 191% more prevalent in infants who exhibited late-onset neonatal sepsis. The number of transfusions per patient was negatively correlated with gestational age and positively correlated with late-onset neonatal sepsis. A gestational age <32 weeks and late-onset neonatal sepsis explained 45% of the transfusions (p<0.0001). CONCLUSIONS: Premature infants with a gestational age <32 weeks and who developed late-onset neonatal sepsis exhibited a greater need for packed red blood cell transfusions.
-
Original Articles – Clinical Research
Incidence and primary causes of unplanned extubation in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):230-235
Abstract
Original Articles – Clinical ResearchIncidence and primary causes of unplanned extubation in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):230-235
DOI 10.1590/S0103-507X2012000300005
Views0OBJECTIVE: This study established the incidence and primary causes of unplanned extubation in newborns in the neonatal intensive care units of the Hospital Sofia Feldman, Belo Horizonte (Minas Gerais). METHODS: This retrospective study was conducted between July 1, 2009 and April 30, 2010. Unplanned extubations and their primary causes were assessed using an adverse events form. The following variables were assessed: gender, corrected age, present weight, duration of mechanical ventilation time, and motives/causes of the event on the day of the unplanned extubation event. RESULTS: Fifty-four unplanned extubations occurred, which corresponded to an incidence of 1.0 event/100 days of mechanical ventilation. This rate was higher among newborns with a corrected age of 30 to 36 weeks and weight < 1,000 g. The primary causes of unplanned extubations included patient agitation, inappropriate handling of patients during the performance of procedures, and inappropriate fixation and positioning of the endotracheal tube. CONCLUSION: The incidence of unplanned extubation in the investigated neonatal intensive care units was low during the study period compared to previously reported data. Nevertheless, the assessment of the quality of procedures, the continuous follow-up of newborns, and the monitoring of the causes of extubation are required to further reduce this incidence.
Keywords:Airway extubationIncidenceInfant, newbornIntensive care units, neonatalPhysical therapy modalitiesSee moreViews0Abstract
Original Articles – Clinical ResearchIncidence and primary causes of unplanned extubation in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):230-235
DOI 10.1590/S0103-507X2012000300005
Views0OBJECTIVE: This study established the incidence and primary causes of unplanned extubation in newborns in the neonatal intensive care units of the Hospital Sofia Feldman, Belo Horizonte (Minas Gerais). METHODS: This retrospective study was conducted between July 1, 2009 and April 30, 2010. Unplanned extubations and their primary causes were assessed using an adverse events form. The following variables were assessed: gender, corrected age, present weight, duration of mechanical ventilation time, and motives/causes of the event on the day of the unplanned extubation event. RESULTS: Fifty-four unplanned extubations occurred, which corresponded to an incidence of 1.0 event/100 days of mechanical ventilation. This rate was higher among newborns with a corrected age of 30 to 36 weeks and weight < 1,000 g. The primary causes of unplanned extubations included patient agitation, inappropriate handling of patients during the performance of procedures, and inappropriate fixation and positioning of the endotracheal tube. CONCLUSION: The incidence of unplanned extubation in the investigated neonatal intensive care units was low during the study period compared to previously reported data. Nevertheless, the assessment of the quality of procedures, the continuous follow-up of newborns, and the monitoring of the causes of extubation are required to further reduce this incidence.
Keywords:Airway extubationIncidenceInfant, newbornIntensive care units, neonatalPhysical therapy modalitiesSee more -
Original Articles – Clinical Research
Urinary electrolyte monitoring in critically ill patients: a preliminary observational study
Rev Bras Ter Intensiva. 2012;24(3):236-245
Abstract
Original Articles – Clinical ResearchUrinary electrolyte monitoring in critically ill patients: a preliminary observational study
Rev Bras Ter Intensiva. 2012;24(3):236-245
DOI 10.1590/S0103-507X2012000300006
Views0OBJECTIVE: Intensive care unit survivors and non-survivors have distinct acid-base profiles. The kidney’s regulation of urinary electrolytes and the urinary strong ion difference plays a major role in acid-base homeostasis. The aim of this study was to evaluate the potential utility of daily spot urinary electrolyte measurement in acid-base and renal function monitoring. METHODS: We prospectively recorded daily plasma acid-base parameters and traditional markers of renal function in parallel with spot urinary electrolyte measurements in patients with urinary catheters admitted to our intensive care unit. Patients who remained in the intensive care unit for at least 4 days with a urinary catheter were included in the study. RESULTS: Of the 50 patients included in the study, 22% died during their intensive care unit stay. The incidence of acute kidney injury was significantly higher in non-survivors during the 4-day observation period (64% vs. 18% in survivors). Urinary chloride and sodium were lower and urinary strong ion difference was higher on day 1 in patients who developed acute kidney injury among both survivors and non-survivors. Both groups had similar urine output, although non-survivors had persistently higher urinary strong ion difference on all days. Survivors had a progressive improvement in metabolic acid-base profile due to increases in the plasma strong ion difference and decreases in weak acids. These changes were concomitant with decreases in urinary strong ion difference. In non-survivors, acid-base parameters did not significantly change during follow-up. CONCLUSIONS: Daily assessment of spot urinary electrolytes and strong ion difference are useful components of acid-base and renal function evaluations in critically ill patients, having distinct profiles between intensive care unit survivors and non-survivors.
Keywords:AcidosisAcute kidney injuryCritical careMonitoring, physiologicPrognosisWater-electrolyte imbalanceSee moreViews0Abstract
Original Articles – Clinical ResearchUrinary electrolyte monitoring in critically ill patients: a preliminary observational study
Rev Bras Ter Intensiva. 2012;24(3):236-245
DOI 10.1590/S0103-507X2012000300006
Views0OBJECTIVE: Intensive care unit survivors and non-survivors have distinct acid-base profiles. The kidney’s regulation of urinary electrolytes and the urinary strong ion difference plays a major role in acid-base homeostasis. The aim of this study was to evaluate the potential utility of daily spot urinary electrolyte measurement in acid-base and renal function monitoring. METHODS: We prospectively recorded daily plasma acid-base parameters and traditional markers of renal function in parallel with spot urinary electrolyte measurements in patients with urinary catheters admitted to our intensive care unit. Patients who remained in the intensive care unit for at least 4 days with a urinary catheter were included in the study. RESULTS: Of the 50 patients included in the study, 22% died during their intensive care unit stay. The incidence of acute kidney injury was significantly higher in non-survivors during the 4-day observation period (64% vs. 18% in survivors). Urinary chloride and sodium were lower and urinary strong ion difference was higher on day 1 in patients who developed acute kidney injury among both survivors and non-survivors. Both groups had similar urine output, although non-survivors had persistently higher urinary strong ion difference on all days. Survivors had a progressive improvement in metabolic acid-base profile due to increases in the plasma strong ion difference and decreases in weak acids. These changes were concomitant with decreases in urinary strong ion difference. In non-survivors, acid-base parameters did not significantly change during follow-up. CONCLUSIONS: Daily assessment of spot urinary electrolytes and strong ion difference are useful components of acid-base and renal function evaluations in critically ill patients, having distinct profiles between intensive care unit survivors and non-survivors.
Keywords:AcidosisAcute kidney injuryCritical careMonitoring, physiologicPrognosisWater-electrolyte imbalanceSee more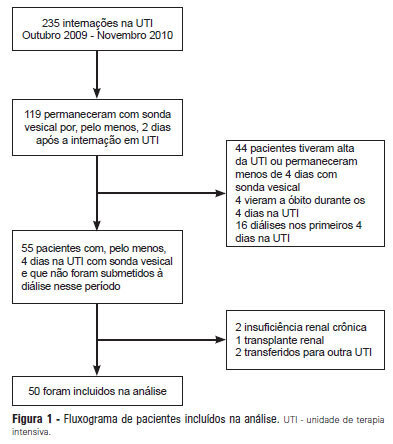
-
Original Articles – Clinical Research
Mortality assessment in patients with severe acute pancreatitis: a comparative study of specific and general severity indices
Rev Bras Ter Intensiva. 2012;24(3):246-251
Abstract
Original Articles – Clinical ResearchMortality assessment in patients with severe acute pancreatitis: a comparative study of specific and general severity indices
Rev Bras Ter Intensiva. 2012;24(3):246-251
DOI 10.1590/S0103-507X2012000300007
Views0OBJECTIVE: This study compared the general and specific severity indices to assess the prognosis of severe acute pancreatitis at a polyvalent intensive care unit. METHODS: This retrospective study included 108 patients who were diagnosed with severe acute pancreatitis from July 1, 1999 to March 31, 2012. Their demographic and clinical data were collected, and the following severity indices were calculated: Ranson, Osborne, Blamey and Imrie, Balthazar, POP, APACHE II, SAPS II, and SOFA. The discriminative power of these indices with regard to mortality at the intensive care unit and hospital was assessed using the area under the ROC curve. RESULTS: The demographic data of the surviving and deceased patients did not significantly differ at baseline. The mortality rates were 27% and 39% at the intensive care unit and hospital, respectively. The severity indices that exhibited the greatest discriminative power with regard to mortality at the intensive care unit and hospital were the POP 0, POP 24, SOFA (at admission, 24 hours, 48 hours, and discharge), SAPS II, and APACHE II. CONCLUSION: The POP performed better than the other indices (aROC>0.8) at admission and 24 hours later (as originally described). The general physiological dysfunction indices also exhibited reasonable discriminative power (aROC=0.75-0.8), which was unlike the remaining pancreatitis specific indices, whose discriminative power was lower.
Keywords:Acute pancreatitisCritical careHospital mortalityMortalityPrognosisSeverity of illness indexSee moreViews0Abstract
Original Articles – Clinical ResearchMortality assessment in patients with severe acute pancreatitis: a comparative study of specific and general severity indices
Rev Bras Ter Intensiva. 2012;24(3):246-251
DOI 10.1590/S0103-507X2012000300007
Views0OBJECTIVE: This study compared the general and specific severity indices to assess the prognosis of severe acute pancreatitis at a polyvalent intensive care unit. METHODS: This retrospective study included 108 patients who were diagnosed with severe acute pancreatitis from July 1, 1999 to March 31, 2012. Their demographic and clinical data were collected, and the following severity indices were calculated: Ranson, Osborne, Blamey and Imrie, Balthazar, POP, APACHE II, SAPS II, and SOFA. The discriminative power of these indices with regard to mortality at the intensive care unit and hospital was assessed using the area under the ROC curve. RESULTS: The demographic data of the surviving and deceased patients did not significantly differ at baseline. The mortality rates were 27% and 39% at the intensive care unit and hospital, respectively. The severity indices that exhibited the greatest discriminative power with regard to mortality at the intensive care unit and hospital were the POP 0, POP 24, SOFA (at admission, 24 hours, 48 hours, and discharge), SAPS II, and APACHE II. CONCLUSION: The POP performed better than the other indices (aROC>0.8) at admission and 24 hours later (as originally described). The general physiological dysfunction indices also exhibited reasonable discriminative power (aROC=0.75-0.8), which was unlike the remaining pancreatitis specific indices, whose discriminative power was lower.
Keywords:Acute pancreatitisCritical careHospital mortalityMortalityPrognosisSeverity of illness indexSee more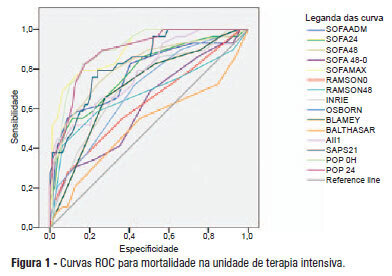
-
Original Articles – Clinical Research
Routine chest radiography in intensive care: impact on decision-making
Rev Bras Ter Intensiva. 2012;24(3):252-257
Abstract
Original Articles – Clinical ResearchRoutine chest radiography in intensive care: impact on decision-making
Rev Bras Ter Intensiva. 2012;24(3):252-257
DOI 10.1590/S0103-507X2012000300008
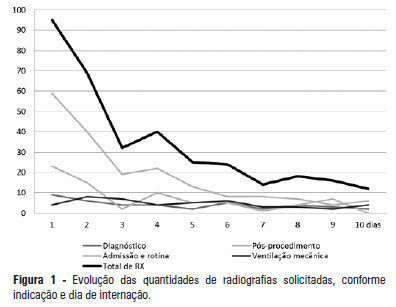
Views0See moreOBJECTIVE: This study determined the prevalence of clinical abnormalities in chest radiographs and its relationship with decision-making in intensive care. METHODS: This prospective cohort study involved nonconsecutive patients who were admitted to the intensive care unit at the Hospital Universitário Professor Polydoro Ernani de São Thiago of the Universidade Federal de Santa Catarina. Imaging tests in the intensive care unit (ICU) were assessed daily between February and May 2011 and divided according to the reason for hospitalization, the type of test requested, anatomical segment under assessment and the purpose of the request. The imaging tests were interpreted by intensivists and subsequently divided according to the detected abnormalities and changes in medical care. The chi-squared test was used for statistical analysis. RESULTS: The study sample included 106 patients. A total of 447 imaging tests were assessed, 425 of which were anteroposterior chest radiographs. An average of 4.01 radiographs per patient was obtained. Among the requested radiographs, 79.3% were normal, and 35.2% of abnormal radiographs did not prompt changes in medical care. CONCLUSION: Most of the radiographs performed in the intensive care unit exhibited no statistically significant clinical alterations, and the radiographs that revealed abnormalities did not necessarily lead to changes in medical care.
Views0Abstract
Original Articles – Clinical ResearchRoutine chest radiography in intensive care: impact on decision-making
Rev Bras Ter Intensiva. 2012;24(3):252-257
DOI 10.1590/S0103-507X2012000300008
Views0See moreOBJECTIVE: This study determined the prevalence of clinical abnormalities in chest radiographs and its relationship with decision-making in intensive care. METHODS: This prospective cohort study involved nonconsecutive patients who were admitted to the intensive care unit at the Hospital Universitário Professor Polydoro Ernani de São Thiago of the Universidade Federal de Santa Catarina. Imaging tests in the intensive care unit (ICU) were assessed daily between February and May 2011 and divided according to the reason for hospitalization, the type of test requested, anatomical segment under assessment and the purpose of the request. The imaging tests were interpreted by intensivists and subsequently divided according to the detected abnormalities and changes in medical care. The chi-squared test was used for statistical analysis. RESULTS: The study sample included 106 patients. A total of 447 imaging tests were assessed, 425 of which were anteroposterior chest radiographs. An average of 4.01 radiographs per patient was obtained. Among the requested radiographs, 79.3% were normal, and 35.2% of abnormal radiographs did not prompt changes in medical care. CONCLUSION: Most of the radiographs performed in the intensive care unit exhibited no statistically significant clinical alterations, and the radiographs that revealed abnormalities did not necessarily lead to changes in medical care.
-
Original Articles – Clinical Research
Is the intention to donate organs influenced by the public’s understanding of brain death?
Rev Bras Ter Intensiva. 2012;24(3):258-262
Abstract
Original Articles – Clinical ResearchIs the intention to donate organs influenced by the public’s understanding of brain death?
Rev Bras Ter Intensiva. 2012;24(3):258-262
DOI 10.1590/S0103-507X2012000300009
Views0OBJECTIVE: To evaluate the influence of the understanding of brain death in relation to organ donation in patients from the Marco School Health Center, which is linked to the Universidade do Estado do Pará. METHODS: A total of 136 patients were interviewed based on a research protocol. The interview results were subsequently analyzed with regard to the understanding of brain death and organ donation in addition to the collection of sociodemographic data. RESULTS: The majority of patients were female and were in favor of organ donation, with a mean age of 39 years being observed. Only 19.9% of the patients understood the meaning of brain death, and 85.3% believed that physicians may be mistaken in confirming the status of brain death of a patient, while 18.4% trusted the diagnosis of brain death. A statistically significant (p < 0.01) correlation was observed between the degree of confidence in the diagnosis of brain death and the person's agreement to donate his/her organs after death. CONCLUSION: The majority of the population under study did not understand the meaning of brain death and had a low degree of confidence in the diagnosis of brain death. This lack of understanding and confidence negatively influences the desire to donate organs.
Keywords:Assessmentbrain deathDirected tissue donationHealth centersKnowledgePopulationTeaching, hospitalsSee moreViews0Abstract
Original Articles – Clinical ResearchIs the intention to donate organs influenced by the public’s understanding of brain death?
Rev Bras Ter Intensiva. 2012;24(3):258-262
DOI 10.1590/S0103-507X2012000300009
Views0OBJECTIVE: To evaluate the influence of the understanding of brain death in relation to organ donation in patients from the Marco School Health Center, which is linked to the Universidade do Estado do Pará. METHODS: A total of 136 patients were interviewed based on a research protocol. The interview results were subsequently analyzed with regard to the understanding of brain death and organ donation in addition to the collection of sociodemographic data. RESULTS: The majority of patients were female and were in favor of organ donation, with a mean age of 39 years being observed. Only 19.9% of the patients understood the meaning of brain death, and 85.3% believed that physicians may be mistaken in confirming the status of brain death of a patient, while 18.4% trusted the diagnosis of brain death. A statistically significant (p < 0.01) correlation was observed between the degree of confidence in the diagnosis of brain death and the person's agreement to donate his/her organs after death. CONCLUSION: The majority of the population under study did not understand the meaning of brain death and had a low degree of confidence in the diagnosis of brain death. This lack of understanding and confidence negatively influences the desire to donate organs.
Keywords:Assessmentbrain deathDirected tissue donationHealth centersKnowledgePopulationTeaching, hospitalsSee more -
Original Articles – Clinical Research
Nutritional support and outcomes in critically ill patients after one week in the intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):263-269
Abstract
Original Articles – Clinical ResearchNutritional support and outcomes in critically ill patients after one week in the intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):263-269
DOI 10.1590/S0103-507X2012000300010
Views1OBJECTIVE: This study evaluated the relationship between nutritional intake and protein and caloric requirements and observed clinical outcomes on the 7th day of intensive care unit stay. METHODS: This was a retrospective cohort study of 126 patients who were admitted to the intensive care unit for >7 days. The patients were categorized according to the adequacy of energy and protein intake in relation to requirements (a >60% Adequate Intake Group and a <60% Inadequate Intake Group). The length of stay, ventilator free time and mortality in the intensive care unit and hospital were evaluated. RESULTS: Enteral nutrition was used in 95.6% of the 126 included patients, and nutrition was initiated 41 hours after admission to the intensive care unit. The adequacy of intake was 84% for energy and 72.5% for protein. No differences in the length of stay [16 (11-23) versus 15 (11-21) days, p=0.862], ventilator free time [2 (0-7) versus 3 (0-6) days, p=0.985] or mortality in the intensive care unit [12 (41.4%) versus 38 (39.1%), p=0.831] and hospital [15 (51.7%) versus 44 (45.4%), p=0.348] were observed between the adequate and inadequate energy intake groups, respectively. Similar results in protein intake and the length of hospital stay [15 (12-21) versus 15 (11-21) days, p=0.996], ventilator free time [2 (0-7) versus 3 (0-6) days, p=0.846], and mortality in the intensive care unit [15 (28.3%) versus 35 (47.9%), p=0.536)] and hospital [18 (52.9%) versus 41 (44.6%), p=0.262] were observed between groups. CONCLUSION: The results did not establish that energy and protein intakes of greater or less than 60% of nutritional requirements were reliable dividers of clinical outcomes.
Keywords:Energy requirementIntensive care unitsLength of stayMortalitynutrition therapyRespiration, artificialSee moreViews1Abstract
Original Articles – Clinical ResearchNutritional support and outcomes in critically ill patients after one week in the intensive care unit
Rev Bras Ter Intensiva. 2012;24(3):263-269
DOI 10.1590/S0103-507X2012000300010
Views1OBJECTIVE: This study evaluated the relationship between nutritional intake and protein and caloric requirements and observed clinical outcomes on the 7th day of intensive care unit stay. METHODS: This was a retrospective cohort study of 126 patients who were admitted to the intensive care unit for >7 days. The patients were categorized according to the adequacy of energy and protein intake in relation to requirements (a >60% Adequate Intake Group and a <60% Inadequate Intake Group). The length of stay, ventilator free time and mortality in the intensive care unit and hospital were evaluated. RESULTS: Enteral nutrition was used in 95.6% of the 126 included patients, and nutrition was initiated 41 hours after admission to the intensive care unit. The adequacy of intake was 84% for energy and 72.5% for protein. No differences in the length of stay [16 (11-23) versus 15 (11-21) days, p=0.862], ventilator free time [2 (0-7) versus 3 (0-6) days, p=0.985] or mortality in the intensive care unit [12 (41.4%) versus 38 (39.1%), p=0.831] and hospital [15 (51.7%) versus 44 (45.4%), p=0.348] were observed between the adequate and inadequate energy intake groups, respectively. Similar results in protein intake and the length of hospital stay [15 (12-21) versus 15 (11-21) days, p=0.996], ventilator free time [2 (0-7) versus 3 (0-6) days, p=0.846], and mortality in the intensive care unit [15 (28.3%) versus 35 (47.9%), p=0.536)] and hospital [18 (52.9%) versus 41 (44.6%), p=0.262] were observed between groups. CONCLUSION: The results did not establish that energy and protein intakes of greater or less than 60% of nutritional requirements were reliable dividers of clinical outcomes.
Keywords:Energy requirementIntensive care unitsLength of stayMortalitynutrition therapyRespiration, artificialSee more -
Original Articles – Clinical Research
Nutritional requirements of the critically ill patient
Rev Bras Ter Intensiva. 2012;24(3):270-277
Abstract
Original Articles – Clinical ResearchNutritional requirements of the critically ill patient
Rev Bras Ter Intensiva. 2012;24(3):270-277
DOI 10.1590/S0103-507X2012000300011
Views0OBJECTIVE: Given the inaccessibility of indirect calorimetry, intensive care units generally use predictive equations or recommendations that are established by international societies to determine energy expenditure. The aim of the present study was to compare the energy expenditure of critically ill patients, as determined using indirect calorimetry, to the values obtained using the Harris-Benedict equation. METHODS: A retrospective observational study was conducted at the Intensive Care Unit 1 of the Centro Hospitalar do Porto. The energy requirements of hospitalized critically ill patients as determined using indirect calorimetry were assessed between January 2003 and April 2012. The accuracy (± 10% difference between the measured and estimated values), the mean differences and the limits of agreement were determined for the studied equations. RESULTS: Eighty-five patients were assessed using 288 indirect calorimetry measurements. The following energy requirement values were obtained for the different methods: 1,753.98±391.13 kcal/day (24.48 ± 5.95 kcal/kg/day) for indirect calorimetry and 1,504.11 ± 266.99 kcal/day (20.72±2.43 kcal/kg/day) for the Harris-Benedict equation. The equation had a precision of 31.76% with a mean difference of -259.86 kcal/day and limits of agreement between -858.84 and 339.12 kcal/day. Sex (p=0.023), temperature (p=0.009) and body mass index (p<0.001) were found to significantly affect energy expenditure. CONCLUSION: The Harris-Benedict equation is inaccurate and tends to underestimate energy expenditure. In addition, the Harris-Benedict equation is associated with significant differences between the predicted and true energy expenditure at an individual level.
Keywords:Diet therapyEnergy metabolismIndirect calorimetryIntensive care unitsnutritional therapyRespiration, artificialSee moreViews0Abstract
Original Articles – Clinical ResearchNutritional requirements of the critically ill patient
Rev Bras Ter Intensiva. 2012;24(3):270-277
DOI 10.1590/S0103-507X2012000300011
Views0OBJECTIVE: Given the inaccessibility of indirect calorimetry, intensive care units generally use predictive equations or recommendations that are established by international societies to determine energy expenditure. The aim of the present study was to compare the energy expenditure of critically ill patients, as determined using indirect calorimetry, to the values obtained using the Harris-Benedict equation. METHODS: A retrospective observational study was conducted at the Intensive Care Unit 1 of the Centro Hospitalar do Porto. The energy requirements of hospitalized critically ill patients as determined using indirect calorimetry were assessed between January 2003 and April 2012. The accuracy (± 10% difference between the measured and estimated values), the mean differences and the limits of agreement were determined for the studied equations. RESULTS: Eighty-five patients were assessed using 288 indirect calorimetry measurements. The following energy requirement values were obtained for the different methods: 1,753.98±391.13 kcal/day (24.48 ± 5.95 kcal/kg/day) for indirect calorimetry and 1,504.11 ± 266.99 kcal/day (20.72±2.43 kcal/kg/day) for the Harris-Benedict equation. The equation had a precision of 31.76% with a mean difference of -259.86 kcal/day and limits of agreement between -858.84 and 339.12 kcal/day. Sex (p=0.023), temperature (p=0.009) and body mass index (p<0.001) were found to significantly affect energy expenditure. CONCLUSION: The Harris-Benedict equation is inaccurate and tends to underestimate energy expenditure. In addition, the Harris-Benedict equation is associated with significant differences between the predicted and true energy expenditure at an individual level.
Keywords:Diet therapyEnergy metabolismIndirect calorimetryIntensive care unitsnutritional therapyRespiration, artificialSee more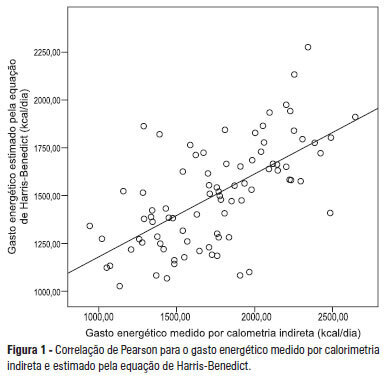
-
Original Articles – Clinical Research
Use of non-invasive ventilation in acute pulmonary edema and chronic obstructive pulmonary disease exacerbation in emergency medicine: predictors of failure
Rev Bras Ter Intensiva. 2012;24(3):278-283
Abstract
Original Articles – Clinical ResearchUse of non-invasive ventilation in acute pulmonary edema and chronic obstructive pulmonary disease exacerbation in emergency medicine: predictors of failure
Rev Bras Ter Intensiva. 2012;24(3):278-283
DOI 10.1590/S0103-507X2012000300012
Views0OBJECTIVE: This study analyzed acute respiratory failure caused by acute pulmonary edema, as well as chronic obstructive pulmonary disease exacerbation, that was treated with non-invasive mechanical ventilation to identify the factors that are associated with the success or failure non-invasive mechanical ventilation in urgent and emergency service. METHODS: This study was a prospective, descriptive and analytical study. We included patients of both genders aged >18 years who used non-invasive mechanical ventilation due to acute respiratory failure that was secondary to acute pulmonary edema or chronic obstructive pulmonary disease exacerbation. Patients with acute respiratory failure that was secondary to pathologies other than acute pulmonary edema and chronic obstructive pulmonary disease or who presented with contraindications for the technique were excluded. Expiratory pressures between 5 and 8 cmH2O and inspiratory pressures between 10 and 12 cmH2O were used. Supplemental oxygen maintained peripheral oxygen saturation at >90%. The primary outcome was endotracheal intubation. RESULTS: A total of 152 patients were included. The median non-invasive mechanical ventilation time was 6 hours (range 1 – 32 hours) for chronic obstructive pulmonary disease patients (n=60) and 5 hours (range 2 – 32 hours) for acute pulmonary edema patients (n=92). Most (75.7%) patients progressed successfully. However, reduced APACHE II scores and lower peripheral oxygen saturation were observed. These results were statistically significant in patients who progressed to intubation (p<0.001). BiPAP (Bi-level Positive Airway Pressure portable ventilator), as continuous positive airway pressure use increased the probability of endotracheal intubation 2.3 times (p=0.032). Patients with acute pulmonary edema and elevated GCS scores also increased the probability of success. CONCLUSION: Respiratory frequency >25 rpm, higher APACHE II scores, BiPAP use and chronic obstructive pulmonary disease diagnosis were associated with endotracheal intubation. Higher GCS and SpO2 values were associated with NIV success. Non-invasive mechanical ventilation can be used in emergency services in acute respiratory failure cases caused by acute pulmonary edema and chronic obstructive pulmonary disease exacerbation, but patients with variables related to a higher percentage of endotracheal intubation should be specially monitored.
Keywords:Continuous positive airway pressureEmergencyPulmonary disease, chronic obstructivePulmonary edemaRespiratory insufficiencySee moreViews0Abstract
Original Articles – Clinical ResearchUse of non-invasive ventilation in acute pulmonary edema and chronic obstructive pulmonary disease exacerbation in emergency medicine: predictors of failure
Rev Bras Ter Intensiva. 2012;24(3):278-283
DOI 10.1590/S0103-507X2012000300012
Views0OBJECTIVE: This study analyzed acute respiratory failure caused by acute pulmonary edema, as well as chronic obstructive pulmonary disease exacerbation, that was treated with non-invasive mechanical ventilation to identify the factors that are associated with the success or failure non-invasive mechanical ventilation in urgent and emergency service. METHODS: This study was a prospective, descriptive and analytical study. We included patients of both genders aged >18 years who used non-invasive mechanical ventilation due to acute respiratory failure that was secondary to acute pulmonary edema or chronic obstructive pulmonary disease exacerbation. Patients with acute respiratory failure that was secondary to pathologies other than acute pulmonary edema and chronic obstructive pulmonary disease or who presented with contraindications for the technique were excluded. Expiratory pressures between 5 and 8 cmH2O and inspiratory pressures between 10 and 12 cmH2O were used. Supplemental oxygen maintained peripheral oxygen saturation at >90%. The primary outcome was endotracheal intubation. RESULTS: A total of 152 patients were included. The median non-invasive mechanical ventilation time was 6 hours (range 1 – 32 hours) for chronic obstructive pulmonary disease patients (n=60) and 5 hours (range 2 – 32 hours) for acute pulmonary edema patients (n=92). Most (75.7%) patients progressed successfully. However, reduced APACHE II scores and lower peripheral oxygen saturation were observed. These results were statistically significant in patients who progressed to intubation (p<0.001). BiPAP (Bi-level Positive Airway Pressure portable ventilator), as continuous positive airway pressure use increased the probability of endotracheal intubation 2.3 times (p=0.032). Patients with acute pulmonary edema and elevated GCS scores also increased the probability of success. CONCLUSION: Respiratory frequency >25 rpm, higher APACHE II scores, BiPAP use and chronic obstructive pulmonary disease diagnosis were associated with endotracheal intubation. Higher GCS and SpO2 values were associated with NIV success. Non-invasive mechanical ventilation can be used in emergency services in acute respiratory failure cases caused by acute pulmonary edema and chronic obstructive pulmonary disease exacerbation, but patients with variables related to a higher percentage of endotracheal intubation should be specially monitored.
Keywords:Continuous positive airway pressureEmergencyPulmonary disease, chronic obstructivePulmonary edemaRespiratory insufficiencySee more -
Review Articles
Bleeding in non-ST-segment elevation acute coronary syndrome
Rev Bras Ter Intensiva. 2012;24(3):284-293
Abstract
Review ArticlesBleeding in non-ST-segment elevation acute coronary syndrome
Rev Bras Ter Intensiva. 2012;24(3):284-293
DOI 10.1590/S0103-507X2012000300013
Views0The development of antiplatelet and antithrombotic therapies, in addition to interventionist strategy, has resulted in great improvements in the outcomes of patients with non-ST-segment elevation acute coronary syndrome. Parallel to therapeutic advances, bleeding, which can be induced during management, increases the risk of recurrent ischemia, myocardial infarction and death. The present literature review describes the benefits and bleeding risks of each medication or intervention strategy and suggests guidelines for managing these patients.
Keywords:Acute coronary syndromeBleedingGastrointestinal bleedingIntracranial hemorrhagesThrombosisTransfusionSee moreViews0Abstract
Review ArticlesBleeding in non-ST-segment elevation acute coronary syndrome
Rev Bras Ter Intensiva. 2012;24(3):284-293
DOI 10.1590/S0103-507X2012000300013
Views0The development of antiplatelet and antithrombotic therapies, in addition to interventionist strategy, has resulted in great improvements in the outcomes of patients with non-ST-segment elevation acute coronary syndrome. Parallel to therapeutic advances, bleeding, which can be induced during management, increases the risk of recurrent ischemia, myocardial infarction and death. The present literature review describes the benefits and bleeding risks of each medication or intervention strategy and suggests guidelines for managing these patients.
Keywords:Acute coronary syndromeBleedingGastrointestinal bleedingIntracranial hemorrhagesThrombosisTransfusionSee more -
Review Articles
CD4+CD25+ T lymphocytes and regulation of the immune system: perspectives for a pathophysiological understanding of sepsis
Rev Bras Ter Intensiva. 2012;24(3):294-301
Abstract
Review ArticlesCD4+CD25+ T lymphocytes and regulation of the immune system: perspectives for a pathophysiological understanding of sepsis
Rev Bras Ter Intensiva. 2012;24(3):294-301
DOI 10.1590/S0103-507X2012000300014
Views0See moreThe systemic inflammatory response represents the core pathogenic event of sepsis, underlying clinical manifestations and laboratory findings in patients. Numerous studies have shown that CD4+CD25+ T lymphocytes, also known as regulatory T lymphocytes (Treg), participate in the development of sepsis due to their ability to suppress the immune response. The present article discusses the role of Treg lymphocytes in sepsis based on a specific search strategy (Latin American and Caribbean Health Sciences / Literatura Latino-americana e do Caribe em Ciências da Saúde – LILACS, PubMed, and Scientific Electronic Library Online – SciELO) focusing on two main topics: the participation of Treg cells in inflammation and immunity as well as perspectives in the computational physiological investigation of sepsis.
Views0Abstract
Review ArticlesCD4+CD25+ T lymphocytes and regulation of the immune system: perspectives for a pathophysiological understanding of sepsis
Rev Bras Ter Intensiva. 2012;24(3):294-301
DOI 10.1590/S0103-507X2012000300014
Views0See moreThe systemic inflammatory response represents the core pathogenic event of sepsis, underlying clinical manifestations and laboratory findings in patients. Numerous studies have shown that CD4+CD25+ T lymphocytes, also known as regulatory T lymphocytes (Treg), participate in the development of sepsis due to their ability to suppress the immune response. The present article discusses the role of Treg lymphocytes in sepsis based on a specific search strategy (Latin American and Caribbean Health Sciences / Literatura Latino-americana e do Caribe em Ciências da Saúde – LILACS, PubMed, and Scientific Electronic Library Online – SciELO) focusing on two main topics: the participation of Treg cells in inflammation and immunity as well as perspectives in the computational physiological investigation of sepsis.
-
Case Report
Plasmapheresis as a therapeutic approach for hypertriglyceridemia-induced acute pancreatitis
Rev Bras Ter Intensiva. 2012;24(3):302-307
Abstract
Case ReportPlasmapheresis as a therapeutic approach for hypertriglyceridemia-induced acute pancreatitis
Rev Bras Ter Intensiva. 2012;24(3):302-307
DOI 10.1590/S0103-507X2012000300015
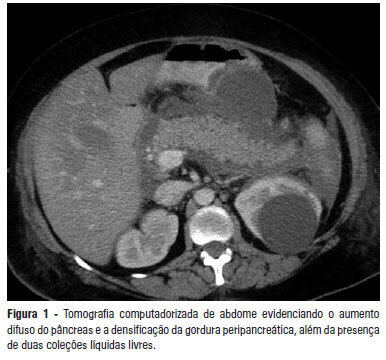
Views0See moreAcute pancreatitis is an inflammatory condition that is clinically manifested by abdominal pain and elevated serum levels of pancreatic enzymes. Hypertriglyceridemia is the third most common cause of acute pancreatitis. The present report aimed to describe a case of hypertriglyceridemia-induced acute pancreatitis, where the therapeutic approach was plasmapheresis. A 48-year-old female patient was admitted to the hospital with complaints of “severe abdominal pain”. She reported the onset of such symptoms as nausea, vomiting and abdominal pain with a burning feeling in the epigastric area. The patient denied having a fever. The initial examination revealed that she was obese, oriented, tachypneic, normotensive, tachycardic, dehydrated, afebrile, anicteric and acyanotic and had normal color. Her abdomen was distended with bowel sounds, tympanic and diffusely painful, which was mostly in the supramesocolic compartment. The initial laboratory exams showed 10.932 mg/dL triglycerides, 1.548 mg/dL cholesterol, 226 mg/dL amylase and 899 mg/dL lipase. The abdominal computed tomography exhibited increased pancreatic volume (Balthazar E). The patient’s condition worsened, and she was sent to the intensive care center. Plasmapheresis was performed with no complications. On the 14th day after admission, the patient was discharged from the intensive care center and was sent to the gastroenterology ward, where an oral diet was resumed with good acceptance. The patient progressed well and was discharged from the hospital on the 25th day after admission. High triglyceride levels are necessary to cause pancreatitis, and it is important to exclude the most common causes. Importantly, the therapeutic approach reduced the high hypertriglyceridemia quickly, thereby avoiding tissue damage.
Views0Abstract
Case ReportPlasmapheresis as a therapeutic approach for hypertriglyceridemia-induced acute pancreatitis
Rev Bras Ter Intensiva. 2012;24(3):302-307
DOI 10.1590/S0103-507X2012000300015
Views0See moreAcute pancreatitis is an inflammatory condition that is clinically manifested by abdominal pain and elevated serum levels of pancreatic enzymes. Hypertriglyceridemia is the third most common cause of acute pancreatitis. The present report aimed to describe a case of hypertriglyceridemia-induced acute pancreatitis, where the therapeutic approach was plasmapheresis. A 48-year-old female patient was admitted to the hospital with complaints of “severe abdominal pain”. She reported the onset of such symptoms as nausea, vomiting and abdominal pain with a burning feeling in the epigastric area. The patient denied having a fever. The initial examination revealed that she was obese, oriented, tachypneic, normotensive, tachycardic, dehydrated, afebrile, anicteric and acyanotic and had normal color. Her abdomen was distended with bowel sounds, tympanic and diffusely painful, which was mostly in the supramesocolic compartment. The initial laboratory exams showed 10.932 mg/dL triglycerides, 1.548 mg/dL cholesterol, 226 mg/dL amylase and 899 mg/dL lipase. The abdominal computed tomography exhibited increased pancreatic volume (Balthazar E). The patient’s condition worsened, and she was sent to the intensive care center. Plasmapheresis was performed with no complications. On the 14th day after admission, the patient was discharged from the intensive care center and was sent to the gastroenterology ward, where an oral diet was resumed with good acceptance. The patient progressed well and was discharged from the hospital on the 25th day after admission. High triglyceride levels are necessary to cause pancreatitis, and it is important to exclude the most common causes. Importantly, the therapeutic approach reduced the high hypertriglyceridemia quickly, thereby avoiding tissue damage.
-
Case Report
Meningitis as a complication of infective endocarditis
Rev Bras Ter Intensiva. 2012;24(3):308-311
Abstract
Case ReportMeningitis as a complication of infective endocarditis
Rev Bras Ter Intensiva. 2012;24(3):308-311
DOI 10.1590/S0103-507X2012000300016
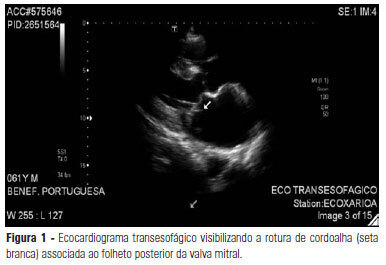
Views0See moreAlthough approximately 30% of patients with endocarditis present with neurological complications, the development of meningitis in these patients is rare. This case report describes a female patient who developed meningitis as a complication of mitral valve endocarditis, and surgery was required for this patient due to acute heart failure resulting from the rupture of the chordae tendineae.
Views0Abstract
Case ReportMeningitis as a complication of infective endocarditis
Rev Bras Ter Intensiva. 2012;24(3):308-311
DOI 10.1590/S0103-507X2012000300016
Views0See moreAlthough approximately 30% of patients with endocarditis present with neurological complications, the development of meningitis in these patients is rare. This case report describes a female patient who developed meningitis as a complication of mitral valve endocarditis, and surgery was required for this patient due to acute heart failure resulting from the rupture of the chordae tendineae.
-
Letter to the Editor
The incidence of delirium in patients pretreated with statins who remain in an intensive care unit after cardiac surgery
Rev Bras Ter Intensiva. 2012;24(3):312-313
Abstract
Letter to the EditorThe incidence of delirium in patients pretreated with statins who remain in an intensive care unit after cardiac surgery
Rev Bras Ter Intensiva. 2012;24(3):312-313
Views0Abstract
Letter to the EditorThe incidence of delirium in patients pretreated with statins who remain in an intensive care unit after cardiac surgery
Rev Bras Ter Intensiva. 2012;24(3):312-313
Volume Articles - Critical Care Science (CCS)
