Respiration, artificial Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2012;24(2):167-172
DOI 10.1590/S0103-507X2012000200012
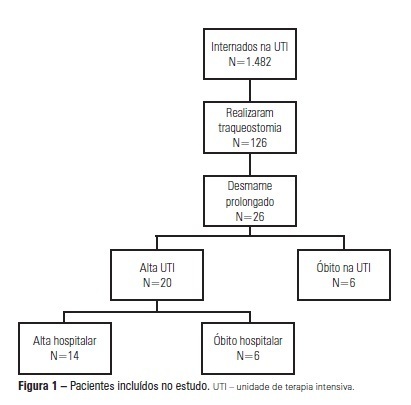
OBJECTIVE: We aimed to assess the use of noninvasive ventilation devices in patients with prolonged weaning following tracheotomy. METHODS: We performed a retrospective observational study using data collected from the clinical records of tracheotomized patients diagnosed with prolonged weaning. The participants were hospitalized in the adult intensive care unit of Moinhos de Vento Hospital, Porto Alegre (RS) between December 2007 and December 2008. RESULTS: In the data collection period, 1,482 patients were admitted to the intensive care unit. In total, 126 patients underwent tracheotomies, and 26 of these patients met the inclusion criteria for participating in the study. The average age of the patients in our sample was 73 ± 12 years. In our sample, 57.7% of the participants were female, and 80.8% were admitted as a result of acute hypoxemic respiratory failure. After the tracheotomy, the patients remained under mechanical ventilation for an average of 29.8 days. After the initiation of the experimental protocol, the tracheotomized patients remained under ventilation for an average of 53.5 days on a portable noninvasive device connected to the tracheotomy. There were three possible outcomes for the patients. They were discharged, were weaned from the noninvasive ventilation, or died in the intensive care unit or hospital ward. In total, 76.9% (20/26) of the patients were discharged from the intensive care unit, and 53.8% (14/26) of the patients were discharged from the hospital. CONCLUSION: The use of noninvasive portable ventilators connected to the tracheotomy may represent an alternative for discontinuing ventilationand discharging tracheotomized patients with prolonged ventilatory weaning from intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):167-172
DOI 10.1590/S0103-507X2012000200012
OBJECTIVE: We aimed to assess the use of noninvasive ventilation devices in patients with prolonged weaning following tracheotomy. METHODS: We performed a retrospective observational study using data collected from the clinical records of tracheotomized patients diagnosed with prolonged weaning. The participants were hospitalized in the adult intensive care unit of Moinhos de Vento Hospital, Porto Alegre (RS) between December 2007 and December 2008. RESULTS: In the data collection period, 1,482 patients were admitted to the intensive care unit. In total, 126 patients underwent tracheotomies, and 26 of these patients met the inclusion criteria for participating in the study. The average age of the patients in our sample was 73 ± 12 years. In our sample, 57.7% of the participants were female, and 80.8% were admitted as a result of acute hypoxemic respiratory failure. After the tracheotomy, the patients remained under mechanical ventilation for an average of 29.8 days. After the initiation of the experimental protocol, the tracheotomized patients remained under ventilation for an average of 53.5 days on a portable noninvasive device connected to the tracheotomy. There were three possible outcomes for the patients. They were discharged, were weaned from the noninvasive ventilation, or died in the intensive care unit or hospital ward. In total, 76.9% (20/26) of the patients were discharged from the intensive care unit, and 53.8% (14/26) of the patients were discharged from the hospital. CONCLUSION: The use of noninvasive portable ventilators connected to the tracheotomy may represent an alternative for discontinuing ventilationand discharging tracheotomized patients with prolonged ventilatory weaning from intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):119-129
DOI 10.1590/S0103-507X2012000200005
Developing guidelines for the role of the physiotherapist in neonatal and pediatric intensive care units is essential because these professionals are responsible for the rehabilitation of critically ill patients. Rehabilitation includes the evaluation and prevention of functional kinetic alterations, application of treatment interventions (respiratory and/or motor physiotherapy), control and application of medical gases, care of mechanical ventilation, weaning and extubation, tracheal gas insufflation, inflation/deflation of the endotracheal cuff protocol, and surfactant application, aiming to allow patients to have a full recovery and return to their functional activities. In this article, we present guidelines that are intended to guide the physiotherapist in some of the prevention/treatment interventions in respiratory therapy (airway clearance, lung expansion, position in bed, airway suction, drug inhalation, and cough assist), which help in the rehabilitation process of newborns and children in intensive care units during mechanical ventilation and up to 12 hours following extubation.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):119-129
DOI 10.1590/S0103-507X2012000200005
Developing guidelines for the role of the physiotherapist in neonatal and pediatric intensive care units is essential because these professionals are responsible for the rehabilitation of critically ill patients. Rehabilitation includes the evaluation and prevention of functional kinetic alterations, application of treatment interventions (respiratory and/or motor physiotherapy), control and application of medical gases, care of mechanical ventilation, weaning and extubation, tracheal gas insufflation, inflation/deflation of the endotracheal cuff protocol, and surfactant application, aiming to allow patients to have a full recovery and return to their functional activities. In this article, we present guidelines that are intended to guide the physiotherapist in some of the prevention/treatment interventions in respiratory therapy (airway clearance, lung expansion, position in bed, airway suction, drug inhalation, and cough assist), which help in the rehabilitation process of newborns and children in intensive care units during mechanical ventilation and up to 12 hours following extubation.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):137-142
DOI 10.1590/S0103-507X2012000200007
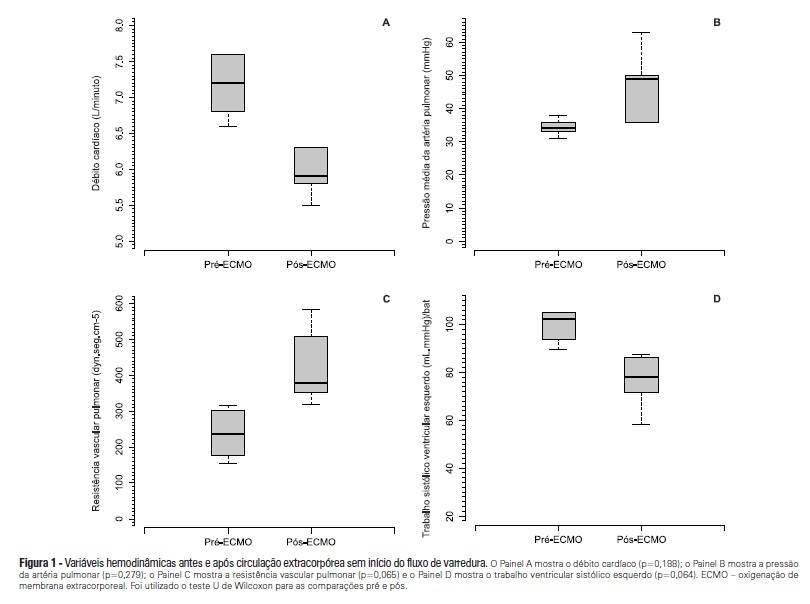
OBJECTIVE: To investigate the hemodynamic, respiratory and metabolic impact of blood contact with a priming volume and extracorporeal membrane oxygenation circuit, before the initiation of oxygenation and ventilation METHODS: Five animals were instrumented and submitted to extracorporeal membrane oxygenation. Data were collected at the baseline and 30 minutes after starting extracorporeal circulation, without membrane ventilatory (sweeper) flow. RESULTS: After starting extracorporeal membrane oxygenation, there was a non-significant elevation in pulmonary vascular resistance from 235 (178,303) to 379 (353,508) dyn.seg.(cm5)-1 (P=0.065), associated with an elevation in the alveolar arterial oxygen gradient from 235 (178,303) to 379 (353,508) mmHg (P=0.063). We also observed a reduction in the left ventricle stroke work from 102 (94,105) to 78 (71,87) (mL.mmHg)/beat (P=0.064), in addition to a reduction in cardiac output from 7.2 (6.8,7.6) to 5.9 (5.8,6.3) L/min (P=0.188). The right ventricle stroke work was counterbalanced between the pulmonary vascular resistance increment and the cardiac output reduction, maintaining a similar value. CONCLUSIONS: We presented an experimental model that is feasible and safe. Blood contact with the priming volume and extracorporeal membrane oxygenation circuit resulted in non-significant systemic or metabolic changes.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):137-142
DOI 10.1590/S0103-507X2012000200007
OBJECTIVE: To investigate the hemodynamic, respiratory and metabolic impact of blood contact with a priming volume and extracorporeal membrane oxygenation circuit, before the initiation of oxygenation and ventilation METHODS: Five animals were instrumented and submitted to extracorporeal membrane oxygenation. Data were collected at the baseline and 30 minutes after starting extracorporeal circulation, without membrane ventilatory (sweeper) flow. RESULTS: After starting extracorporeal membrane oxygenation, there was a non-significant elevation in pulmonary vascular resistance from 235 (178,303) to 379 (353,508) dyn.seg.(cm5)-1 (P=0.065), associated with an elevation in the alveolar arterial oxygen gradient from 235 (178,303) to 379 (353,508) mmHg (P=0.063). We also observed a reduction in the left ventricle stroke work from 102 (94,105) to 78 (71,87) (mL.mmHg)/beat (P=0.064), in addition to a reduction in cardiac output from 7.2 (6.8,7.6) to 5.9 (5.8,6.3) L/min (P=0.188). The right ventricle stroke work was counterbalanced between the pulmonary vascular resistance increment and the cardiac output reduction, maintaining a similar value. CONCLUSIONS: We presented an experimental model that is feasible and safe. Blood contact with the priming volume and extracorporeal membrane oxygenation circuit resulted in non-significant systemic or metabolic changes.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):162-166
DOI 10.1590/S0103-507X2012000200011
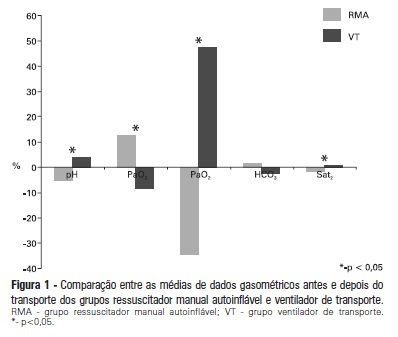
OBJECTIVE: To evaluate the effects on blood gases by two methods of ventilation (with transport ventilation or self-inflating manual resuscitator) during intra-hospital transport of patients after cardiac surgery. METHODS: Observational, longitudinal, prospective, randomized study. Two samples of arterial blood were collected at the end of the surgery and another at the end of patient transport. RESULTS: We included 23 patients: 13 in the Group with transport ventilation and 10 in the Group with self-inflating manual resuscitator. Baseline characteristics were similar between both groups, except for higher acute severity of illness in the Group with transport ventilation. We observed significant differences in comparisons of percentage variations of gasometric data: pH (transport ventilation + 4% x MR -5%, p=0.007), PaCO2 (-8% x +13%, p=0.006), PaO2 (+47% x -34%, p=0.01) and SatO2 (+0.6% x -1.7%, p=0.001). CONCLUSION: The use of mechanical ventilation results in fewer repercussions for blood gas analysis in the intra-hospital transport of cardiac surgery patients.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):162-166
DOI 10.1590/S0103-507X2012000200011
OBJECTIVE: To evaluate the effects on blood gases by two methods of ventilation (with transport ventilation or self-inflating manual resuscitator) during intra-hospital transport of patients after cardiac surgery. METHODS: Observational, longitudinal, prospective, randomized study. Two samples of arterial blood were collected at the end of the surgery and another at the end of patient transport. RESULTS: We included 23 patients: 13 in the Group with transport ventilation and 10 in the Group with self-inflating manual resuscitator. Baseline characteristics were similar between both groups, except for higher acute severity of illness in the Group with transport ventilation. We observed significant differences in comparisons of percentage variations of gasometric data: pH (transport ventilation + 4% x MR -5%, p=0.007), PaCO2 (-8% x +13%, p=0.006), PaO2 (+47% x -34%, p=0.01) and SatO2 (+0.6% x -1.7%, p=0.001). CONCLUSION: The use of mechanical ventilation results in fewer repercussions for blood gas analysis in the intra-hospital transport of cardiac surgery patients.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):23-29
DOI 10.1590/S0103-507X2012000100004
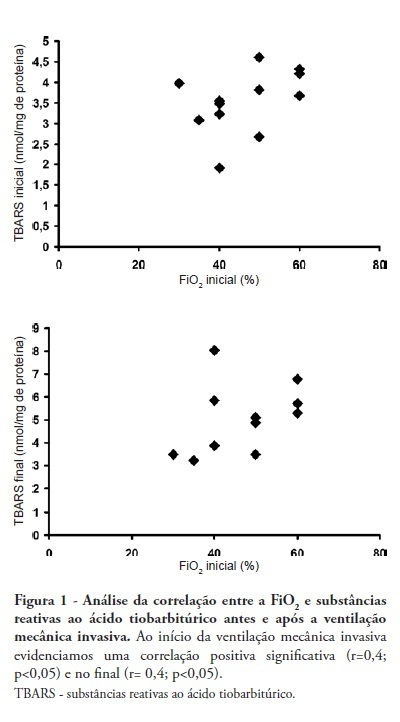
OBJECTIVE: Mechanical ventilation is a mainstay of therapy in intensive care units; however, its deleterious effects need to be assessed. Therefore, we aimed to assess oxidative stress in patients admitted to an intensive care unit undergoing invasive mechanical ventilation. METHODS: This cross-sectional study included 12 invasive mechanical ventilation patients. Blood samples (3 mL) were collected on the first and last days on invasive mechanical ventilation. Thiobarbituric acid-reacting substances (TBARS) were assessed in plasma, and superoxide dismutase (SOD) and catalase (CAT) were assessed in erythrocytes. RESULTS: The mean age was 64.8 ± 17.6 years, the tidal volume (VT) 382 ± 44.5 mL, and the APACHE II score 15 ± 7. When initial and final TBARS were compared, a significant difference was identified (3.54 ± 0.74 vs. 4.96 ± 1.47, p = 0.04). Antioxidant enzymes showed no significant differences. Correlations between PaO2/FiO2 and TBARS (r = 0.4), SOD and PaO2/FiO2 (r = 0.51) and APACHE II and SOD (r = 0.56) were identified. Six patients died. CONCLUSION: Patients undergoing invasive mechanical ventilation can develop redox state changes, showing increased TBARS and reduced antioxidant enzymes.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):23-29
DOI 10.1590/S0103-507X2012000100004
OBJECTIVE: Mechanical ventilation is a mainstay of therapy in intensive care units; however, its deleterious effects need to be assessed. Therefore, we aimed to assess oxidative stress in patients admitted to an intensive care unit undergoing invasive mechanical ventilation. METHODS: This cross-sectional study included 12 invasive mechanical ventilation patients. Blood samples (3 mL) were collected on the first and last days on invasive mechanical ventilation. Thiobarbituric acid-reacting substances (TBARS) were assessed in plasma, and superoxide dismutase (SOD) and catalase (CAT) were assessed in erythrocytes. RESULTS: The mean age was 64.8 ± 17.6 years, the tidal volume (VT) 382 ± 44.5 mL, and the APACHE II score 15 ± 7. When initial and final TBARS were compared, a significant difference was identified (3.54 ± 0.74 vs. 4.96 ± 1.47, p = 0.04). Antioxidant enzymes showed no significant differences. Correlations between PaO2/FiO2 and TBARS (r = 0.4), SOD and PaO2/FiO2 (r = 0.51) and APACHE II and SOD (r = 0.56) were identified. Six patients died. CONCLUSION: Patients undergoing invasive mechanical ventilation can develop redox state changes, showing increased TBARS and reduced antioxidant enzymes.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):43-51
DOI 10.1590/S0103-507X2012000100007
OBJECTIVE: The objective of this study was to assess the effects of positive end-expiratory pressure on recruitment, cyclic recruitment and derecruitment and strain in patients with acute lung injury and acute respiratory distress syndrome using lung computed tomography. METHODS: This is an open, controlled, non-randomized interventional study of ten patients with acute lung injury and acute respiratory distress syndrome. Using computed tomography, single, basal slices of the lung were obtained during inspiratory and expiratory pauses at a tidal volume of 6 ml/kg and a positive end-expiratory pressure of 5, 10, 15 and 20 cmH2O. The densities of the lung parenchyma were measured in Hounsfield units. The values for positive end-expiratory pressure-induced recruitment, cyclic recruitment and derecruitment and strain were then calculated. RESULTS: Increasing levels of positive end-expiratory pressure were correlated with increased recruitment and global strain (p < 0.01), which was significantly correlated with plateau pressure (r² = 0.97, p < 0.01). In addition, increasing levels of positive end-expiratory pressure systematically increased strain along the sternovertebral axis. CONCLUSION: While strain is an adverse effect of positive end-expiratory pressure, the decision use positive end-expiratory pressure with any patient should be balanced against the potential benefits of recruitment. Due to the small number of patients in this study, the present data should be treated as hypothesis generating and is not intended to limit the clinical application of a high level of positive end-expiratory pressure in patients with severe hypoxemia.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):43-51
DOI 10.1590/S0103-507X2012000100007
OBJECTIVE: The objective of this study was to assess the effects of positive end-expiratory pressure on recruitment, cyclic recruitment and derecruitment and strain in patients with acute lung injury and acute respiratory distress syndrome using lung computed tomography. METHODS: This is an open, controlled, non-randomized interventional study of ten patients with acute lung injury and acute respiratory distress syndrome. Using computed tomography, single, basal slices of the lung were obtained during inspiratory and expiratory pauses at a tidal volume of 6 ml/kg and a positive end-expiratory pressure of 5, 10, 15 and 20 cmH2O. The densities of the lung parenchyma were measured in Hounsfield units. The values for positive end-expiratory pressure-induced recruitment, cyclic recruitment and derecruitment and strain were then calculated. RESULTS: Increasing levels of positive end-expiratory pressure were correlated with increased recruitment and global strain (p < 0.01), which was significantly correlated with plateau pressure (r² = 0.97, p < 0.01). In addition, increasing levels of positive end-expiratory pressure systematically increased strain along the sternovertebral axis. CONCLUSION: While strain is an adverse effect of positive end-expiratory pressure, the decision use positive end-expiratory pressure with any patient should be balanced against the potential benefits of recruitment. Due to the small number of patients in this study, the present data should be treated as hypothesis generating and is not intended to limit the clinical application of a high level of positive end-expiratory pressure in patients with severe hypoxemia.

Abstract
Rev Bras Ter Intensiva. 2012;24(1):58-63
DOI 10.1590/S0103-507X2012000100009
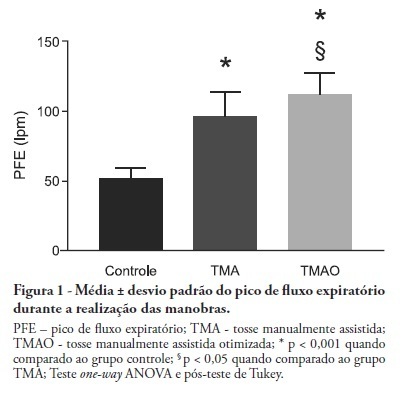
OBJECTIVE: Mechanical ventilation is associated with retained airway secretions. Manually assisted cough contributes to the displacement of bronchial mucus, whereas positive end-expiratory pressure increases collateral ventilation and maintains airway patency. This study aimed to assess the effects of manually assisted cough, either alone or added to increased positive end-expiratory pressure and inspiratory time (optimized manually assisted cough), on the expiratory peak flow and respiratory system mechanics in mechanically ventilated patients. METHODS: In this controlled and randomized clinical trial, respiratory mechanics and expiratory peak flow were assessed in male and female patients undergoing either tracheal suctioning alone, manually assisted cough followed by tracheal suctioning or optimized manually assisted cough followed by tracheal suctioning. RESULTS: Thirty-five patients completed the trial. Respiratory system resistance was significantly reduced after optimized manually assisted cough (16.0 ± 3.6 versus 12.4 ± 3.1 cmH2O/L/s; p = 0.04). The expiratory peak flow during optimized manually assisted cough was significantly higher in comparison with the values observed during manually assisted cough (112.3 ± 15.6 versus 95.8 ± 18.3 Lpm; p < 0.05). Both values were significantly higher than the values observed in the group undergoing tracheal suctioning alone (52.0 ± 7.6 Lpm; p < 0.001). CONCLUSION: Optimized manually assisted cough increases the expiratory peak flow in comparison with manually assisted cough; in addition, this procedure reduces respiratory system resistance.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):58-63
DOI 10.1590/S0103-507X2012000100009
OBJECTIVE: Mechanical ventilation is associated with retained airway secretions. Manually assisted cough contributes to the displacement of bronchial mucus, whereas positive end-expiratory pressure increases collateral ventilation and maintains airway patency. This study aimed to assess the effects of manually assisted cough, either alone or added to increased positive end-expiratory pressure and inspiratory time (optimized manually assisted cough), on the expiratory peak flow and respiratory system mechanics in mechanically ventilated patients. METHODS: In this controlled and randomized clinical trial, respiratory mechanics and expiratory peak flow were assessed in male and female patients undergoing either tracheal suctioning alone, manually assisted cough followed by tracheal suctioning or optimized manually assisted cough followed by tracheal suctioning. RESULTS: Thirty-five patients completed the trial. Respiratory system resistance was significantly reduced after optimized manually assisted cough (16.0 ± 3.6 versus 12.4 ± 3.1 cmH2O/L/s; p = 0.04). The expiratory peak flow during optimized manually assisted cough was significantly higher in comparison with the values observed during manually assisted cough (112.3 ± 15.6 versus 95.8 ± 18.3 Lpm; p < 0.05). Both values were significantly higher than the values observed in the group undergoing tracheal suctioning alone (52.0 ± 7.6 Lpm; p < 0.001). CONCLUSION: Optimized manually assisted cough increases the expiratory peak flow in comparison with manually assisted cough; in addition, this procedure reduces respiratory system resistance.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):164-169
DOI 10.1590/S0103-507X2011000200008
OBJECTIVE: To evaluate the effects of hemodynamic, respiratory and metabolic changes on intracranial pressure in a model of acute lung injury and abdominal compartment syndrome. METHODS: Eight Agroceres pigs were submitted to five different clinical scenarios after instrumentation: 1) a baseline condition with low intra-abdominal pressure and healthy lungs; 2) pneumoperitoneum with 20 mmHg intra-abdominal pressure; 3) acute lung injury induced by pulmonary lavage with surfactant deactivation; 4) pneumoperitoneum with 20 mmHg intra-abdominal pressure with lung pulmonary injury and low positive end-expiratory pressure; and 5) 27 cmH2O positive end-expiratory pressure with pneumoperitoneum and acute lung injury. Respiratory and hemodynamic variables were collected. A multivariate analysis was conducted to search for variables associated with increased intracranial pressure in the five scenarios. RESULTS: Only plateau airway pressure showed a positive correlation with intracranial pressure in the multivariate analysis. In the models with acute lung injury, plateau airway pressure, CO2 arterial pressure, end tidal CO2 and central venous pressure were positively correlated with increased intracranial pressure. CONCLUSION: In a model of multiple organ dysfunction with associated clinical conditions causing increased intra-thoracic and abdominal pressure, increased intracranial pressure triggered by elevated intra-abdominal pressure is apparently caused by worsened respiratory system compliance and a reduced brain venous drainage gradient due to increased central venous pressure.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):164-169
DOI 10.1590/S0103-507X2011000200008
OBJECTIVE: To evaluate the effects of hemodynamic, respiratory and metabolic changes on intracranial pressure in a model of acute lung injury and abdominal compartment syndrome. METHODS: Eight Agroceres pigs were submitted to five different clinical scenarios after instrumentation: 1) a baseline condition with low intra-abdominal pressure and healthy lungs; 2) pneumoperitoneum with 20 mmHg intra-abdominal pressure; 3) acute lung injury induced by pulmonary lavage with surfactant deactivation; 4) pneumoperitoneum with 20 mmHg intra-abdominal pressure with lung pulmonary injury and low positive end-expiratory pressure; and 5) 27 cmH2O positive end-expiratory pressure with pneumoperitoneum and acute lung injury. Respiratory and hemodynamic variables were collected. A multivariate analysis was conducted to search for variables associated with increased intracranial pressure in the five scenarios. RESULTS: Only plateau airway pressure showed a positive correlation with intracranial pressure in the multivariate analysis. In the models with acute lung injury, plateau airway pressure, CO2 arterial pressure, end tidal CO2 and central venous pressure were positively correlated with increased intracranial pressure. CONCLUSION: In a model of multiple organ dysfunction with associated clinical conditions causing increased intra-thoracic and abdominal pressure, increased intracranial pressure triggered by elevated intra-abdominal pressure is apparently caused by worsened respiratory system compliance and a reduced brain venous drainage gradient due to increased central venous pressure.