Intensive care units Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):499-506
DOI 10.5935/0103-507X.20220080-en
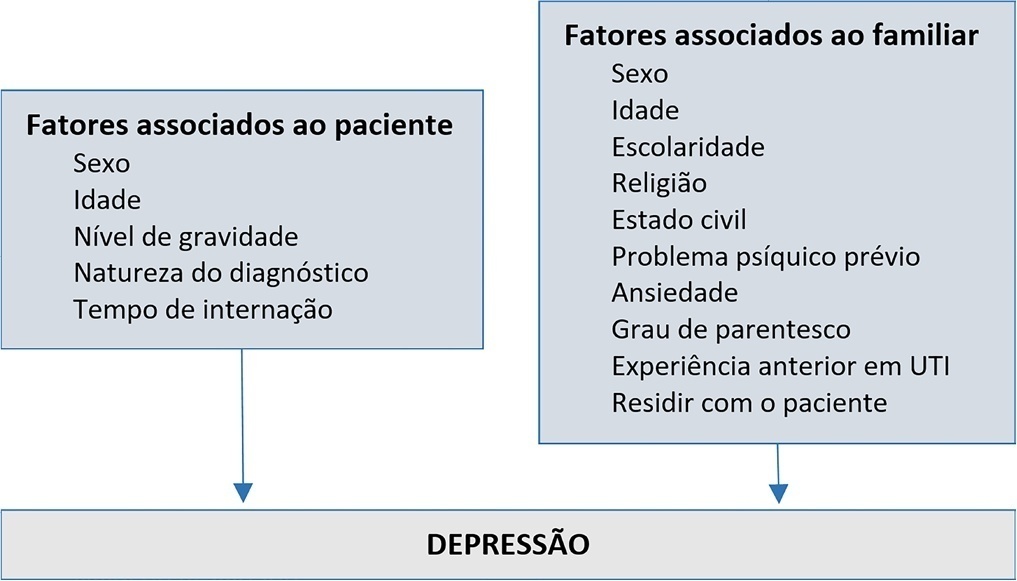
To evaluate the prevalence and factors associated with depression in family members of people hospitalized in intensive care units.
A cross-sectional study was conducted with 980 family members of patients admitted to the intensive care units of a large public hospital in the interior of Bahia. Depression was measured using the Patient Health Questionnaire-8. The multivariate model consisted of the following variables: sex and age of the patient, sex and age of the family member, education level, religion, living with the family member, previous mental illness and anxiety.
Depression had a prevalence of 43.5%. In the multivariate analysis, the model with the best representativeness indicated that factors associated with a higher prevalence of depression were being female (39%), age younger than 40 years (26%) and previous mental illness (38%). A higher education level was associated with a 19% lower prevalence of depression in family members.
The increase in the prevalence of depression was associated with female sex, age younger than 40 years and previous psychological problems. Such elements should be valued in actions aimed at family members of people hospitalized in intensive care.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):499-506
DOI 10.5935/0103-507X.20220080-en
To evaluate the prevalence and factors associated with depression in family members of people hospitalized in intensive care units.
A cross-sectional study was conducted with 980 family members of patients admitted to the intensive care units of a large public hospital in the interior of Bahia. Depression was measured using the Patient Health Questionnaire-8. The multivariate model consisted of the following variables: sex and age of the patient, sex and age of the family member, education level, religion, living with the family member, previous mental illness and anxiety.
Depression had a prevalence of 43.5%. In the multivariate analysis, the model with the best representativeness indicated that factors associated with a higher prevalence of depression were being female (39%), age younger than 40 years (26%) and previous mental illness (38%). A higher education level was associated with a 19% lower prevalence of depression in family members.
The increase in the prevalence of depression was associated with female sex, age younger than 40 years and previous psychological problems. Such elements should be valued in actions aimed at family members of people hospitalized in intensive care.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):507-518
DOI 10.5935/0103-507X.20220145-en
To verify strategies for the prevention and treatment of abstinence syndrome in a pediatric intensive care unit.
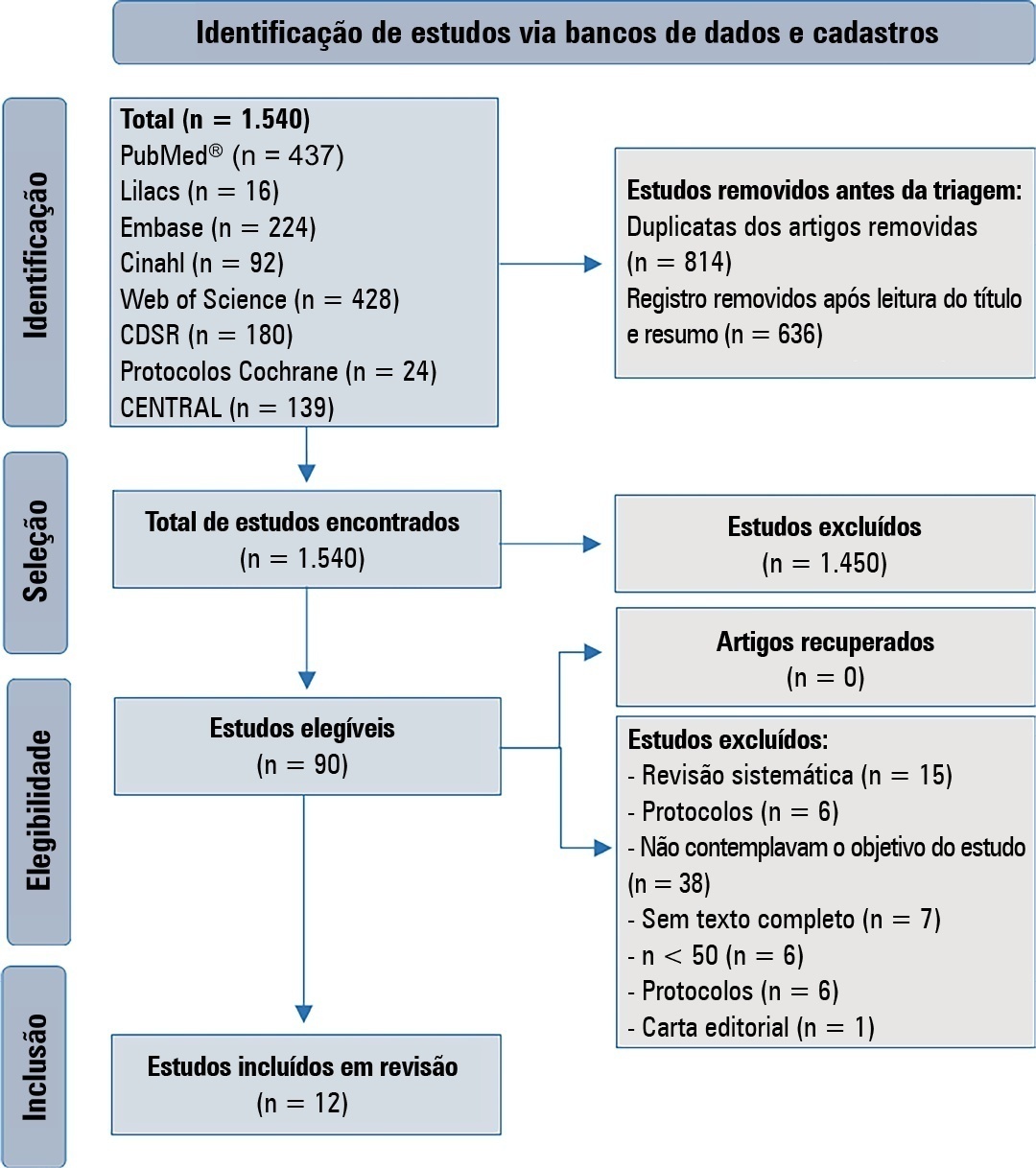
This is a systematic review in the PubMed database®, Lilacs, Embase, Web of Science, Cochrane, Cinahl, Cochrane Database Systematic Review and CENTRAL. A three-step search strategy was used for this review, and the protocol was approved in PROSPERO (CRD42021274670).
Twelve articles were included in the analysis. There was great heterogeneity among the studies included, especially regarding the therapeutic regimens used for sedation and analgesia. Midazolam doses ranged from 0.05mg/kg/hour to 0.3mg/kg/hour. Morphine also varied considerably, from 10mcg/kg/hour to 30mcg/kg/hour, between studies. Among the 12 selected studies, the most commonly used scale for the identification of withdrawal symptoms was the Sophia Observational Withdrawal Symptoms Scale. In three studies, there was a statistically significant difference in the prevention and management of the withdrawal syndrome due to the implementation of different protocols (p < 0.01 and p < 0.001).
There was great variation in the sedoanalgesia regimen used by the studies and the method of weaning and evaluation of withdrawal syndrome. More studies are needed to provide more robust evidence about the most appropriate treatment for the prevention and reduction of withdrawal signs and symptoms in critically ill children.
CRD 42021274670
Abstract
Rev Bras Ter Intensiva. 2022;34(4):507-518
DOI 10.5935/0103-507X.20220145-en
To verify strategies for the prevention and treatment of abstinence syndrome in a pediatric intensive care unit.
This is a systematic review in the PubMed database®, Lilacs, Embase, Web of Science, Cochrane, Cinahl, Cochrane Database Systematic Review and CENTRAL. A three-step search strategy was used for this review, and the protocol was approved in PROSPERO (CRD42021274670).
Twelve articles were included in the analysis. There was great heterogeneity among the studies included, especially regarding the therapeutic regimens used for sedation and analgesia. Midazolam doses ranged from 0.05mg/kg/hour to 0.3mg/kg/hour. Morphine also varied considerably, from 10mcg/kg/hour to 30mcg/kg/hour, between studies. Among the 12 selected studies, the most commonly used scale for the identification of withdrawal symptoms was the Sophia Observational Withdrawal Symptoms Scale. In three studies, there was a statistically significant difference in the prevention and management of the withdrawal syndrome due to the implementation of different protocols (p < 0.01 and p < 0.001).
There was great variation in the sedoanalgesia regimen used by the studies and the method of weaning and evaluation of withdrawal syndrome. More studies are needed to provide more robust evidence about the most appropriate treatment for the prevention and reduction of withdrawal signs and symptoms in critically ill children.
CRD 42021274670
Abstract
Rev Bras Ter Intensiva. 2022;34(3):386-392
DOI 10.5935/0103-507X.20220446-en
To analyze the association of patient safety culture perceived by nursing professionals with incidents recorded during nursing shifts in intensive care units.
This was a cross-sectional study that investigated patient safety culture measured by the Hospital Survey on Patient Safety Culture instrument. Descriptive statistics, chi-square tests, Student’s t-test and multiple linear regression models were analyzed considering a significance level of 5%.
The study reported a mean of 3.1 (standard deviation of 0.4) for the culture of patient safety in the perception of nursing professionals and 480 incidents with and without damage recorded during the nursing shifts. The variables patient safety culture with a difference between means of 0.543 (95%CI 0.022 - 1.065; p < 0.05) and nursing assistants with a difference between means of -0.133 (95%CI -0.192 - -0.074; p < 0.05) were associated with the incidents recorded during the nursing shifts. Further, nursing assistants had a lower tendency to record incidents than did the nurses.
The strengthening of the patient safety culture and the aspects tangential to the nursing professionals represent a possible target for interventions to encourage the recording of incidents during the nursing shift shifts and improve patient safety.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):386-392
DOI 10.5935/0103-507X.20220446-en
To analyze the association of patient safety culture perceived by nursing professionals with incidents recorded during nursing shifts in intensive care units.
This was a cross-sectional study that investigated patient safety culture measured by the Hospital Survey on Patient Safety Culture instrument. Descriptive statistics, chi-square tests, Student’s t-test and multiple linear regression models were analyzed considering a significance level of 5%.
The study reported a mean of 3.1 (standard deviation of 0.4) for the culture of patient safety in the perception of nursing professionals and 480 incidents with and without damage recorded during the nursing shifts. The variables patient safety culture with a difference between means of 0.543 (95%CI 0.022 - 1.065; p < 0.05) and nursing assistants with a difference between means of -0.133 (95%CI -0.192 - -0.074; p < 0.05) were associated with the incidents recorded during the nursing shifts. Further, nursing assistants had a lower tendency to record incidents than did the nurses.
The strengthening of the patient safety culture and the aspects tangential to the nursing professionals represent a possible target for interventions to encourage the recording of incidents during the nursing shift shifts and improve patient safety.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):360-366
DOI 10.5935/0103-507X.20220477-en
To investigate the applicability of the Respiratory Rate-Oxygenation Index to identify the risk of high-flow nasal cannula failure in post-extubation pneumonia patients.
This was a 2-year retrospective observational study conducted in a reference hospital in Bogotá, Colombia. All patients in whom post-extubation high-flow nasal cannula therapy was used as a bridge to extubation were included in the study. The Respiratory Rate-Oxygenation Index was calculated to assess the risk of post-extubation high-flow nasal cannula failure.
A total of 162 patients were included in the study. Of these, 23.5% developed high-flow nasal cannula failure. The Respiratory Rate-Oxygenation Index was significantly lower in patients who had high-flow nasal cannula failure [median (IQR): 10.0 (7.7 - 14.4) versus 12.6 (10.1 - 15.6); p = 0.006]. Respiratory Rate-Oxygenation Index > 4.88 showed a crude OR of 0.23 (95%CI 0.17 - 0.30) and an adjusted OR of 0.89 (95%CI 0.81 - 0.98) stratified by severity and comorbidity. After logistic regression analysis, the Respiratory Rate-Oxygenation Index had an adjusted OR of 0.90 (95%CI 0.82 - 0.98; p = 0.026). The area under the Receiver Operating Characteristic curve for extubation failure was 0.64 (95%CI 0.53 - 0.75; p = 0.06). The Respiratory Rate-Oxygenation Index did not show differences between patients who survived and those who died during the intensive care unit stay.
The Respiratory Rate-Oxygenation Index is an accessible tool to identify patients at risk of failing high-flow nasal cannula post-extubation treatment. Prospective studies are needed to broaden the utility in this scenario.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):360-366
DOI 10.5935/0103-507X.20220477-en
To investigate the applicability of the Respiratory Rate-Oxygenation Index to identify the risk of high-flow nasal cannula failure in post-extubation pneumonia patients.
This was a 2-year retrospective observational study conducted in a reference hospital in Bogotá, Colombia. All patients in whom post-extubation high-flow nasal cannula therapy was used as a bridge to extubation were included in the study. The Respiratory Rate-Oxygenation Index was calculated to assess the risk of post-extubation high-flow nasal cannula failure.
A total of 162 patients were included in the study. Of these, 23.5% developed high-flow nasal cannula failure. The Respiratory Rate-Oxygenation Index was significantly lower in patients who had high-flow nasal cannula failure [median (IQR): 10.0 (7.7 - 14.4) versus 12.6 (10.1 - 15.6); p = 0.006]. Respiratory Rate-Oxygenation Index > 4.88 showed a crude OR of 0.23 (95%CI 0.17 - 0.30) and an adjusted OR of 0.89 (95%CI 0.81 - 0.98) stratified by severity and comorbidity. After logistic regression analysis, the Respiratory Rate-Oxygenation Index had an adjusted OR of 0.90 (95%CI 0.82 - 0.98; p = 0.026). The area under the Receiver Operating Characteristic curve for extubation failure was 0.64 (95%CI 0.53 - 0.75; p = 0.06). The Respiratory Rate-Oxygenation Index did not show differences between patients who survived and those who died during the intensive care unit stay.
The Respiratory Rate-Oxygenation Index is an accessible tool to identify patients at risk of failing high-flow nasal cannula post-extubation treatment. Prospective studies are needed to broaden the utility in this scenario.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):327-334
DOI 10.5935/0103-507X.20220070-en
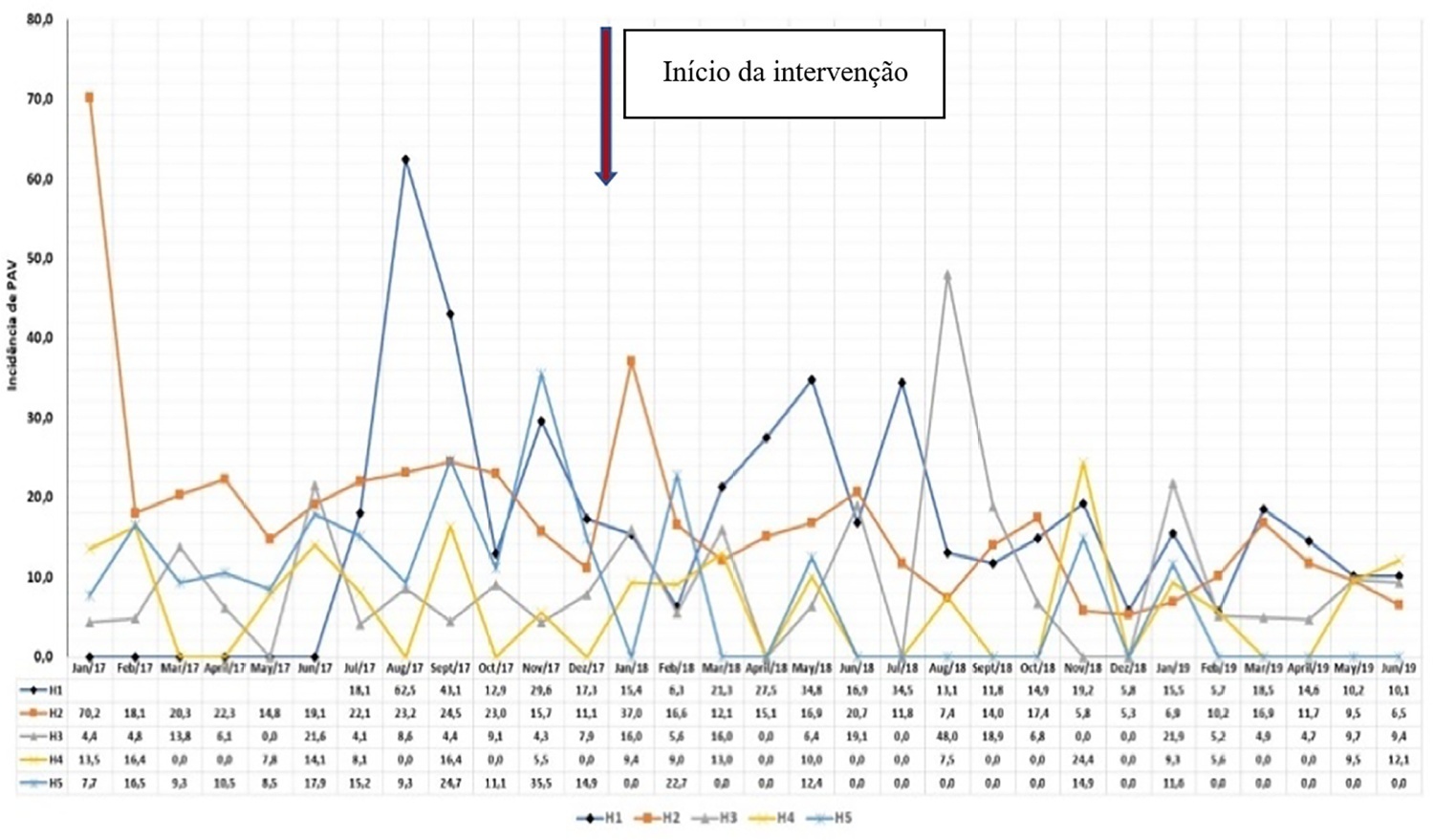
To describe the implementation and results of the collaborative PROADI-SUS project by the Brazilian Ministry of Health to reduce healthcare-associated infections: ventilator-associated pneumonia, primary central line-associated bloodstream infection and catheter-associated urinary tract infections.
This was a prospective observational study that investigated the implementation stages and outcomes during 18 months in five intensive care units in the city of Recife. Reductions in healthcare-associated infections in each unit were calculated using previous medians compared to those of the study period.
The goal of reducing the three healthcare-associated infections, i.e., 30% in 18 months, was achieved in at least one of the healthcare-associated infections and was also achieved for two healthcare-associated infections in two hospitals and three healthcare-associated infections in just one hospital; the latter reached the target of 36 months. Implementing the bundles and monitoring the results by the professionals were considered essential actions by the local management teams. In addition, the acquisition of supplies and their availability alongside the beds, signage, checklists, staff awareness, adaptation, team building, training and celebration of achievements were assessed as being relevant for reducing healthcare-associated infections.
The collaborative approach reduced healthcare-associated infections, despite partial adherence to the bundles. The hypothesis is that success is related to the project methodology and motivated multidisciplinary teams, especially nursing teams.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):327-334
DOI 10.5935/0103-507X.20220070-en
To describe the implementation and results of the collaborative PROADI-SUS project by the Brazilian Ministry of Health to reduce healthcare-associated infections: ventilator-associated pneumonia, primary central line-associated bloodstream infection and catheter-associated urinary tract infections.
This was a prospective observational study that investigated the implementation stages and outcomes during 18 months in five intensive care units in the city of Recife. Reductions in healthcare-associated infections in each unit were calculated using previous medians compared to those of the study period.
The goal of reducing the three healthcare-associated infections, i.e., 30% in 18 months, was achieved in at least one of the healthcare-associated infections and was also achieved for two healthcare-associated infections in two hospitals and three healthcare-associated infections in just one hospital; the latter reached the target of 36 months. Implementing the bundles and monitoring the results by the professionals were considered essential actions by the local management teams. In addition, the acquisition of supplies and their availability alongside the beds, signage, checklists, staff awareness, adaptation, team building, training and celebration of achievements were assessed as being relevant for reducing healthcare-associated infections.
The collaborative approach reduced healthcare-associated infections, despite partial adherence to the bundles. The hypothesis is that success is related to the project methodology and motivated multidisciplinary teams, especially nursing teams.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):220-226
DOI 10.5935/0103-507X.20220019-en
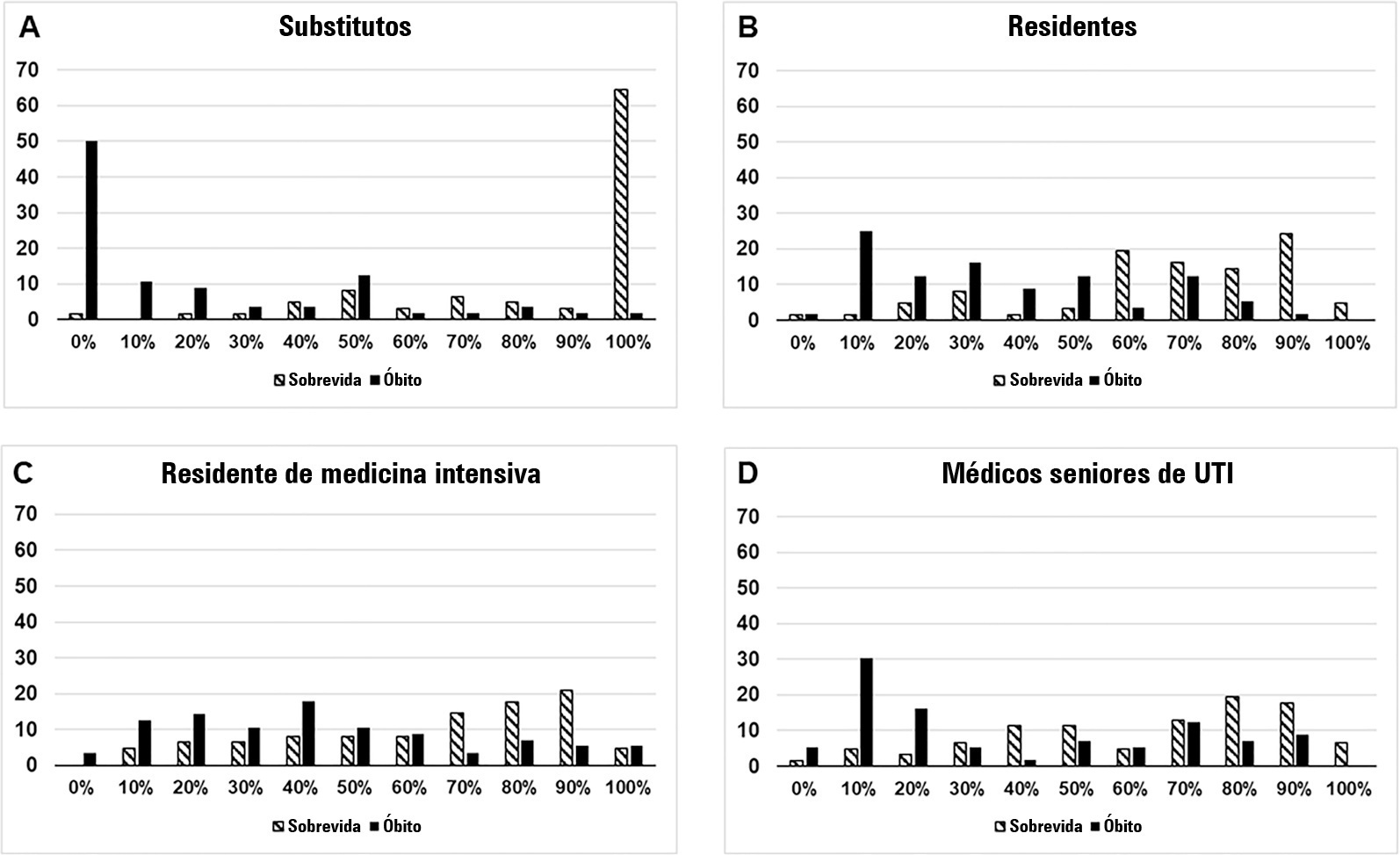
To compare the predictive performance of residents, senior intensive care unit physicians and surrogates early during intensive care unit stays and to evaluate whether different presentations of prognostic data (probability of survival versus probability of death) influenced their performance.
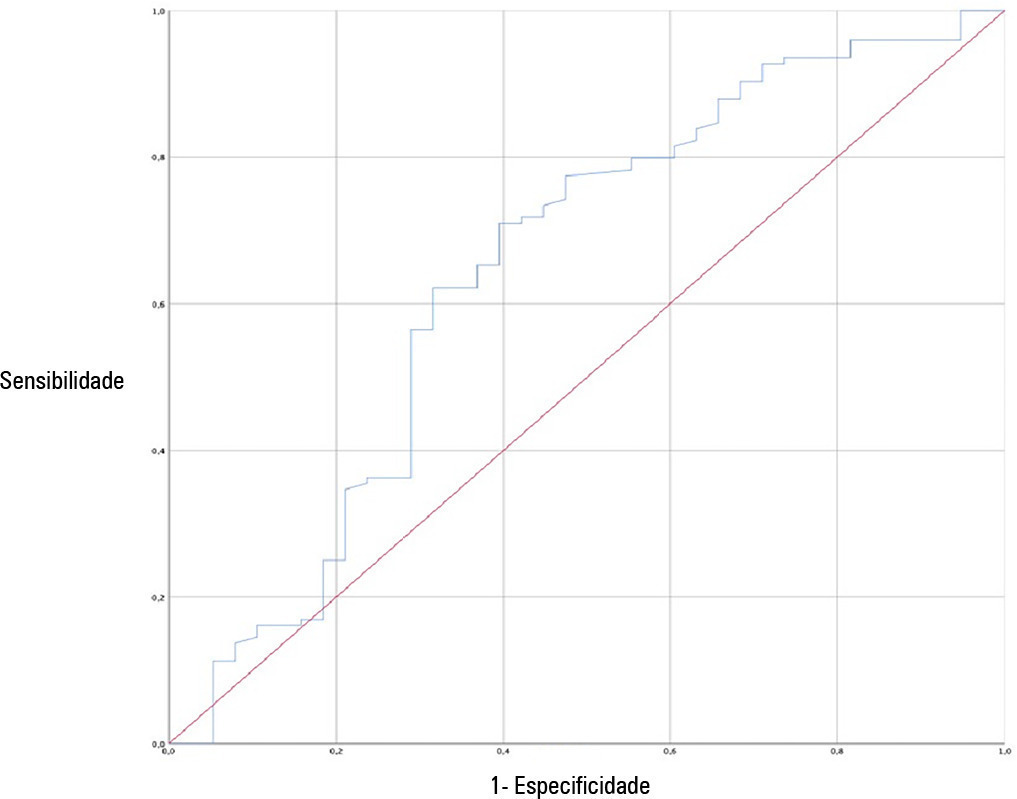
We questioned surrogates and physicians in charge of critically ill patients during the first 48 hours of intensive care unit admission on the patient’s probability of hospital outcome. The question framing (i.e., probability of survival versus probability of death during hospitalization) was randomized. To evaluate the predictive performance, we compared the areas under the ROC curves (AUCs) for hospital outcome between surrogates and physicians’ categories. We also stratified the results according to randomized question framing.
We interviewed surrogates and physicians on the hospital outcomes of 118 patients. The predictive performance of surrogate decisionmakers was significantly lower than that of physicians (AUC of 0.63 for surrogates, 0.82 for residents, 0.80 for intensive care unit fellows and 0.81 for intensive care unit senior physicians). There was no increase in predictive performance related to physicians’ experience (i.e., senior physicians did not predict outcomes better than junior physicians). Surrogate decisionmakers worsened their prediction performance when they were asked about probability of death instead of probability of survival, but there was no difference for physicians.
Different predictive performance was observed when comparing surrogate decision-makers and physicians, with no effect of experience on health care professionals’ prediction. Question framing affected the predictive performance of surrogates but not of physicians.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):220-226
DOI 10.5935/0103-507X.20220019-en
To compare the predictive performance of residents, senior intensive care unit physicians and surrogates early during intensive care unit stays and to evaluate whether different presentations of prognostic data (probability of survival versus probability of death) influenced their performance.
We questioned surrogates and physicians in charge of critically ill patients during the first 48 hours of intensive care unit admission on the patient’s probability of hospital outcome. The question framing (i.e., probability of survival versus probability of death during hospitalization) was randomized. To evaluate the predictive performance, we compared the areas under the ROC curves (AUCs) for hospital outcome between surrogates and physicians’ categories. We also stratified the results according to randomized question framing.
We interviewed surrogates and physicians on the hospital outcomes of 118 patients. The predictive performance of surrogate decisionmakers was significantly lower than that of physicians (AUC of 0.63 for surrogates, 0.82 for residents, 0.80 for intensive care unit fellows and 0.81 for intensive care unit senior physicians). There was no increase in predictive performance related to physicians’ experience (i.e., senior physicians did not predict outcomes better than junior physicians). Surrogate decisionmakers worsened their prediction performance when they were asked about probability of death instead of probability of survival, but there was no difference for physicians.
Different predictive performance was observed when comparing surrogate decision-makers and physicians, with no effect of experience on health care professionals’ prediction. Question framing affected the predictive performance of surrogates but not of physicians.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):262-271
DOI 10.5935/0103-507X.20220024-en
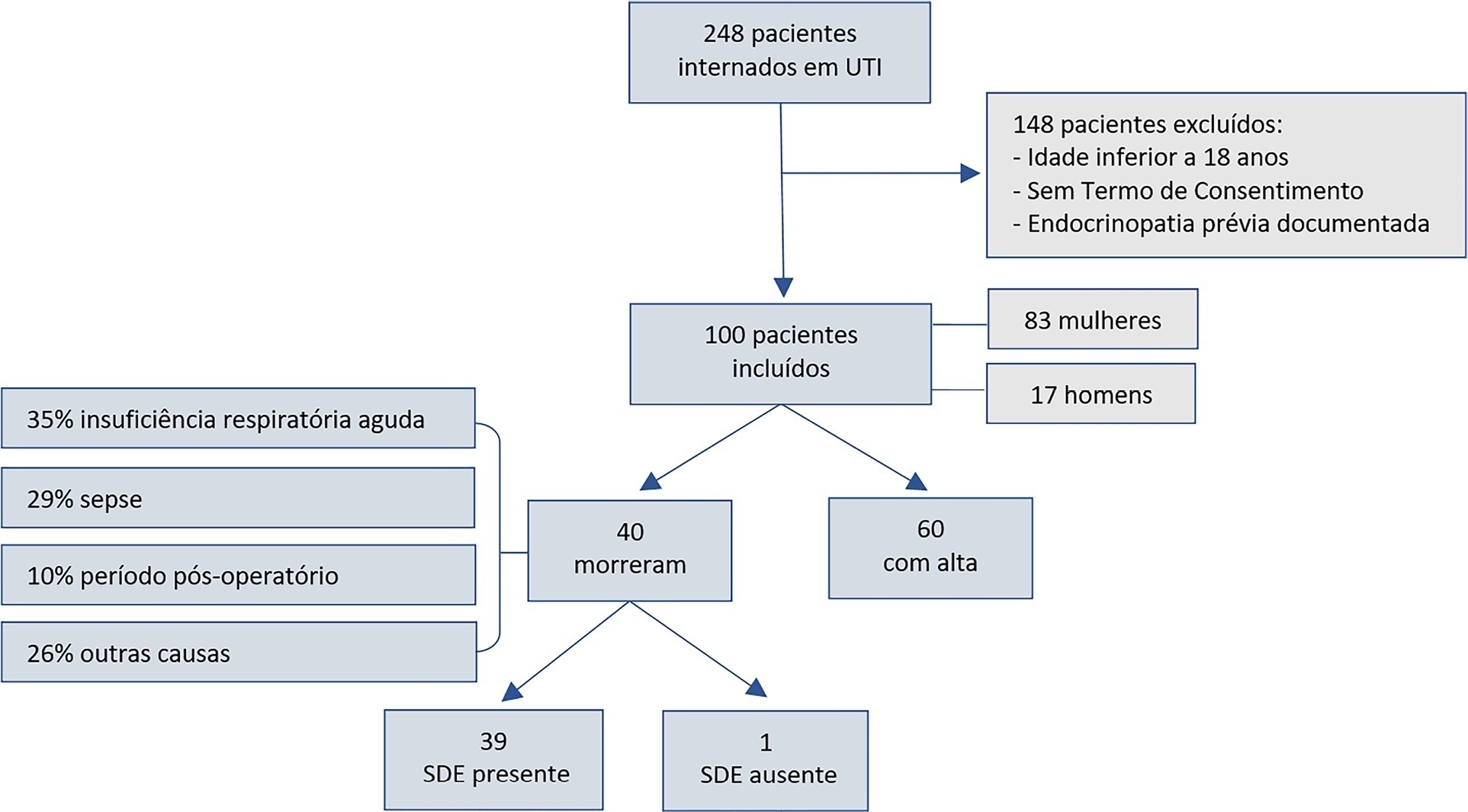
To assess euthyroid sick syndrome as a prognostic factor in patients in the intensive care unit; to detect factors that may affect mortality; and to develop an equation to calculate death probability.
This was a longitudinal, observational, nonconcurrent cohort study developed in the intensive care unit of Fundação Santa Casa de Misericórdia do Pará. One hundred adults with no prior documented endocrinopathy were submitted to a 20mL blood sample collection for the measurement of thyroid stimulating hormone, free tetraiodothyronine, free triiodothyronine and reverse triiodothyronine.
Most patients were female, aged 20 to 29 years. Most patients who died were older (median age of 48 years), and euthyroid sick syndrome was present in 97.5% of them. Euthyroid sick syndrome was related to death, comorbidities, age and length of stay in the intensive care unit (median of 7.5 days).
The main limitation of this study is the fact that it was conducted in a reference hospital for maternal and child care; therefore, there was a greater number of female patients and, consequently, a sampling bias existed. However, opportune measurement of free and reverse triiodothyronine levels in critical patients and application of the proposed equation are suggested.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):262-271
DOI 10.5935/0103-507X.20220024-en
To assess euthyroid sick syndrome as a prognostic factor in patients in the intensive care unit; to detect factors that may affect mortality; and to develop an equation to calculate death probability.
This was a longitudinal, observational, nonconcurrent cohort study developed in the intensive care unit of Fundação Santa Casa de Misericórdia do Pará. One hundred adults with no prior documented endocrinopathy were submitted to a 20mL blood sample collection for the measurement of thyroid stimulating hormone, free tetraiodothyronine, free triiodothyronine and reverse triiodothyronine.
Most patients were female, aged 20 to 29 years. Most patients who died were older (median age of 48 years), and euthyroid sick syndrome was present in 97.5% of them. Euthyroid sick syndrome was related to death, comorbidities, age and length of stay in the intensive care unit (median of 7.5 days).
The main limitation of this study is the fact that it was conducted in a reference hospital for maternal and child care; therefore, there was a greater number of female patients and, consequently, a sampling bias existed. However, opportune measurement of free and reverse triiodothyronine levels in critical patients and application of the proposed equation are suggested.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):272-278
DOI 10.5935/0103-507X.20220025-en
To translate, crossculturally adapt and evaluate the clinimetric properties of the Critical Care Functional Rehabilitation Outcome Measure for evaluating the functionality of patients admitted to intensive care units in Brazil.
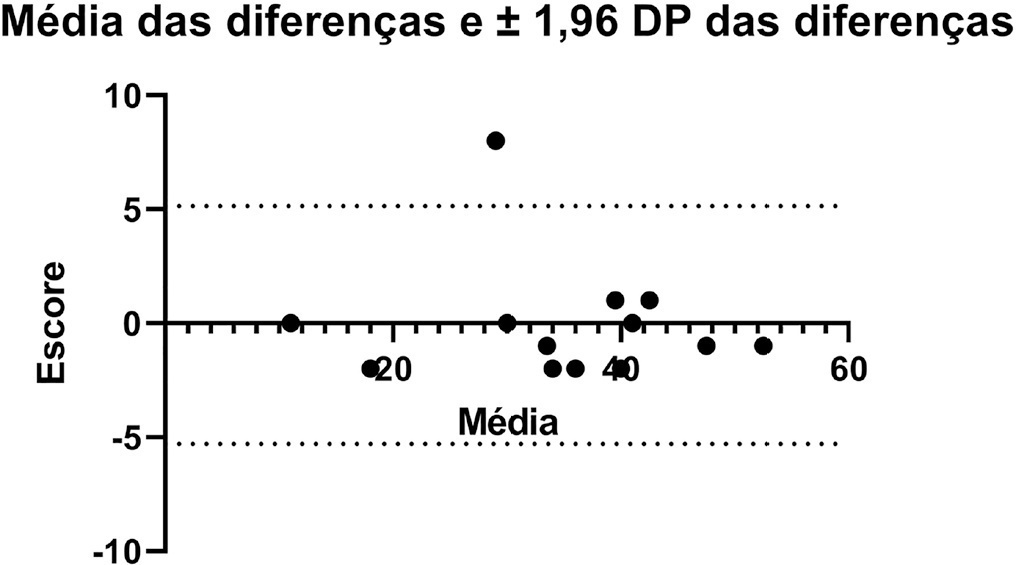
The process of translation and cross-cultural adaptation involved the following steps: initial translation, synthesis, back-translation, expert committee review and pretesting. The intra- and interrater reliability and agreement were analyzed between two physical therapists who evaluated the same group of patients (n = 35). The evaluations were performed by each therapist independently and blinded to the score assigned by the other professional. The qualitative analysis was performed by the review committee, and the experts adapted and synthesized the Portuguese translation of the Critical Care Functional Rehabilitation Outcome Measure.
There was agreement between the initial Brazilian translations of the Critical Care Functional Rehabilitation Outcome Measure scale. The conceptual, idiomatic, semantic and experimental equivalences between the original and translated versions were assessed, resulting in the final Brazilian version of the scale, called the Medida de Resultado da Reabilitação Funcional em Cuidados Intensivos. The evaluation of the clinimetric properties showed evidence of a high degree of agreement and reliability, as all had an intraclass correlation coefficient above 0.75. The overall intraclass correlation coefficient was 0.89.
The translated version of the Critical Care Functional Rehabilitation Outcome Measure scale for assessing the functionality of patients admitted to an intensive care unit can be used reliably in Brazil following translation and cross-cultural adaptation to Brazilian Portuguese and presents evidence of excellent interrater reliability.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):272-278
DOI 10.5935/0103-507X.20220025-en
To translate, crossculturally adapt and evaluate the clinimetric properties of the Critical Care Functional Rehabilitation Outcome Measure for evaluating the functionality of patients admitted to intensive care units in Brazil.
The process of translation and cross-cultural adaptation involved the following steps: initial translation, synthesis, back-translation, expert committee review and pretesting. The intra- and interrater reliability and agreement were analyzed between two physical therapists who evaluated the same group of patients (n = 35). The evaluations were performed by each therapist independently and blinded to the score assigned by the other professional. The qualitative analysis was performed by the review committee, and the experts adapted and synthesized the Portuguese translation of the Critical Care Functional Rehabilitation Outcome Measure.
There was agreement between the initial Brazilian translations of the Critical Care Functional Rehabilitation Outcome Measure scale. The conceptual, idiomatic, semantic and experimental equivalences between the original and translated versions were assessed, resulting in the final Brazilian version of the scale, called the Medida de Resultado da Reabilitação Funcional em Cuidados Intensivos. The evaluation of the clinimetric properties showed evidence of a high degree of agreement and reliability, as all had an intraclass correlation coefficient above 0.75. The overall intraclass correlation coefficient was 0.89.
The translated version of the Critical Care Functional Rehabilitation Outcome Measure scale for assessing the functionality of patients admitted to an intensive care unit can be used reliably in Brazil following translation and cross-cultural adaptation to Brazilian Portuguese and presents evidence of excellent interrater reliability.