-
Editoriais
Prevention of delirium in critically ill patients: a new beginning?
Rev Bras Ter Intensiva. 2012;24(1):1-3
Abstract
EditoriaisPrevention of delirium in critically ill patients: a new beginning?
Rev Bras Ter Intensiva. 2012;24(1):1-3
Views2

Abstract
EditoriaisPrevention of delirium in critically ill patients: a new beginning?
Rev Bras Ter Intensiva. 2012;24(1):1-3
-
Editoriais
Immunoinflammatory prognostic markers of early-onset neonatal sepsis in critically ill preterm newborns
Rev Bras Ter Intensiva. 2012;24(1):4-5
Abstract
EditoriaisImmunoinflammatory prognostic markers of early-onset neonatal sepsis in critically ill preterm newborns
Rev Bras Ter Intensiva. 2012;24(1):4-5
DOI 10.1590/S0103-507X2012000100002
Views1EDITORIAL Immunoinflammatory prognostic markers of early-onset neonatal sepsis in critically ill preterm newborns[…]See moreViews1Abstract
EditoriaisImmunoinflammatory prognostic markers of early-onset neonatal sepsis in critically ill preterm newborns
Rev Bras Ter Intensiva. 2012;24(1):4-5
DOI 10.1590/S0103-507X2012000100002
Views1EDITORIAL Immunoinflammatory prognostic markers of early-onset neonatal sepsis in critically ill preterm newborns[…]See more -
Special Articles
Physical therapy in critically ill adult patients: recommendations from the Brazilian Association of Intensive Care Medicine Department of Physical Therapy
Rev Bras Ter Intensiva. 2012;24(1):6-22
Abstract
Special ArticlesPhysical therapy in critically ill adult patients: recommendations from the Brazilian Association of Intensive Care Medicine Department of Physical Therapy
Rev Bras Ter Intensiva. 2012;24(1):6-22
DOI 10.1590/S0103-507X2012000100003
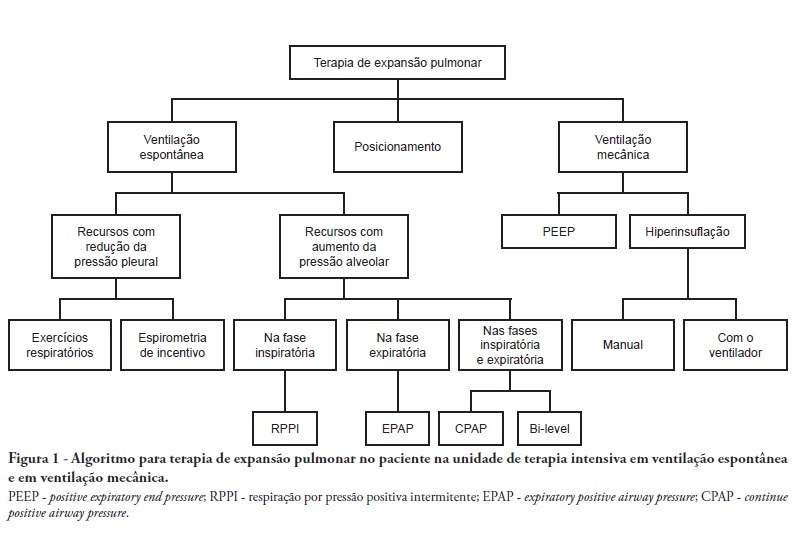
Views5See moreComplications from immobility in intensive care unit patients contribute to functional decline, increased healthcare costs, reduced quality of life and higher post-discharge mortality. Physical therapy focuses on promoting recovery and preserving function, and it may minimize the impact of these complications. A group of Brazilian Association of Intensive Care Medicine physical therapy experts developed this document that contains minimal physical therapy recommendations appropriate to the Brazilian real-world clinical situation. Prevention and treatment of atelectasis, procedures related to the removal of secretions and treatment of conditions related to physical deconditioning and functional decline are discussed. Equally important is the consideration that prescribing and executing activities, mobilizations and exercises are roles of the physical therapist, whose diagnosis should precede any intervention.
Views5Abstract
Special ArticlesPhysical therapy in critically ill adult patients: recommendations from the Brazilian Association of Intensive Care Medicine Department of Physical Therapy
Rev Bras Ter Intensiva. 2012;24(1):6-22
DOI 10.1590/S0103-507X2012000100003
Views5See moreComplications from immobility in intensive care unit patients contribute to functional decline, increased healthcare costs, reduced quality of life and higher post-discharge mortality. Physical therapy focuses on promoting recovery and preserving function, and it may minimize the impact of these complications. A group of Brazilian Association of Intensive Care Medicine physical therapy experts developed this document that contains minimal physical therapy recommendations appropriate to the Brazilian real-world clinical situation. Prevention and treatment of atelectasis, procedures related to the removal of secretions and treatment of conditions related to physical deconditioning and functional decline are discussed. Equally important is the consideration that prescribing and executing activities, mobilizations and exercises are roles of the physical therapist, whose diagnosis should precede any intervention.
-
Original Articles – Basic Research
The effects of mechanical ventilation on oxidative stress
Rev Bras Ter Intensiva. 2012;24(1):23-29
Abstract
Original Articles – Basic ResearchThe effects of mechanical ventilation on oxidative stress
Rev Bras Ter Intensiva. 2012;24(1):23-29
DOI 10.1590/S0103-507X2012000100004
Views0OBJECTIVE: Mechanical ventilation is a mainstay of therapy in intensive care units; however, its deleterious effects need to be assessed. Therefore, we aimed to assess oxidative stress in patients admitted to an intensive care unit undergoing invasive mechanical ventilation. METHODS: This cross-sectional study included 12 invasive mechanical ventilation patients. Blood samples (3 mL) were collected on the first and last days on invasive mechanical ventilation. Thiobarbituric acid-reacting substances (TBARS) were assessed in plasma, and superoxide dismutase (SOD) and catalase (CAT) were assessed in erythrocytes. RESULTS: The mean age was 64.8 ± 17.6 years, the tidal volume (VT) 382 ± 44.5 mL, and the APACHE II score 15 ± 7. When initial and final TBARS were compared, a significant difference was identified (3.54 ± 0.74 vs. 4.96 ± 1.47, p = 0.04). Antioxidant enzymes showed no significant differences. Correlations between PaO2/FiO2 and TBARS (r = 0.4), SOD and PaO2/FiO2 (r = 0.51) and APACHE II and SOD (r = 0.56) were identified. Six patients died. CONCLUSION: Patients undergoing invasive mechanical ventilation can develop redox state changes, showing increased TBARS and reduced antioxidant enzymes.
Keywords:Intensive care unitsOxidative stressRespiration, artificialThiobarbituric acid reactive substancesSee moreViews0Abstract
Original Articles – Basic ResearchThe effects of mechanical ventilation on oxidative stress
Rev Bras Ter Intensiva. 2012;24(1):23-29
DOI 10.1590/S0103-507X2012000100004
Views0OBJECTIVE: Mechanical ventilation is a mainstay of therapy in intensive care units; however, its deleterious effects need to be assessed. Therefore, we aimed to assess oxidative stress in patients admitted to an intensive care unit undergoing invasive mechanical ventilation. METHODS: This cross-sectional study included 12 invasive mechanical ventilation patients. Blood samples (3 mL) were collected on the first and last days on invasive mechanical ventilation. Thiobarbituric acid-reacting substances (TBARS) were assessed in plasma, and superoxide dismutase (SOD) and catalase (CAT) were assessed in erythrocytes. RESULTS: The mean age was 64.8 ± 17.6 years, the tidal volume (VT) 382 ± 44.5 mL, and the APACHE II score 15 ± 7. When initial and final TBARS were compared, a significant difference was identified (3.54 ± 0.74 vs. 4.96 ± 1.47, p = 0.04). Antioxidant enzymes showed no significant differences. Correlations between PaO2/FiO2 and TBARS (r = 0.4), SOD and PaO2/FiO2 (r = 0.51) and APACHE II and SOD (r = 0.56) were identified. Six patients died. CONCLUSION: Patients undergoing invasive mechanical ventilation can develop redox state changes, showing increased TBARS and reduced antioxidant enzymes.
Keywords:Intensive care unitsOxidative stressRespiration, artificialThiobarbituric acid reactive substancesSee more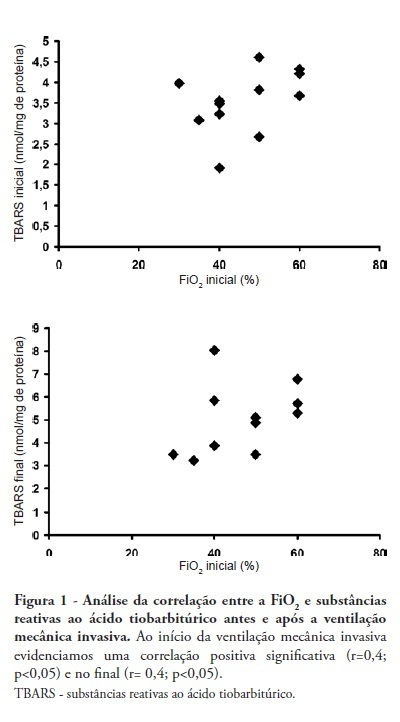
-
Original Articles – Basic Research
Inflammatory and oxidative cord blood parameters as predictors of neonatal sepsis severity
Rev Bras Ter Intensiva. 2012;24(1):30-34
Abstract
Original Articles – Basic ResearchInflammatory and oxidative cord blood parameters as predictors of neonatal sepsis severity
Rev Bras Ter Intensiva. 2012;24(1):30-34
DOI 10.1590/S0103-507X2012000100005
Views0OBJECTIVES: Neonatal sepsis is a complex syndrome involving an uncontrolled systemic inflammatory response associated with an infection. It may result in the dysfunction or failure of one or more organs or even death. Given its high incidence in premature neonates, the identification of prognostic factors to optimize the early diagnosis and therapeutic interventions are highly desirable. This objective study determine the relationship between inflammatory markers and oxidative parameters as prognostic factors in early neonatal sepsis. METHODS: We conducted a prospective observational study by collecting data from 120 patients in the maternity unit of a university hospital. Preterm (<37 weeks of pregnancy) infants with at least one additional risk factor for neonatal sepsis were included. The levels of interleukin (IL)-6, IL-10, thiobarbituric acid reactive species (TBARS) and protein carbonyls and their association with sepsis severity were determined in the cord blood. RESULTS: Levels of IL-6 and TBARS, but not IL-10 and protein carbonyls, demonstrated a mild to moderate correlation with the SNAPPE-II severity score (r=0.435, p=0.02 and r = 0.385, p = 0.017, respectively). No correlations were found between these markers and mortality. CONCLUSION: TBARS and IL-6 have a mild to moderate correlation with SNAPPE-II, but none of the studied markers were able to predict mortality in our sample.
Keywords:Fetal bloodInfant, newbornIntensive care units, neonatalInterleukin-10Interleukin-6Oxidative stressSepsisSee moreViews0Abstract
Original Articles – Basic ResearchInflammatory and oxidative cord blood parameters as predictors of neonatal sepsis severity
Rev Bras Ter Intensiva. 2012;24(1):30-34
DOI 10.1590/S0103-507X2012000100005
Views0OBJECTIVES: Neonatal sepsis is a complex syndrome involving an uncontrolled systemic inflammatory response associated with an infection. It may result in the dysfunction or failure of one or more organs or even death. Given its high incidence in premature neonates, the identification of prognostic factors to optimize the early diagnosis and therapeutic interventions are highly desirable. This objective study determine the relationship between inflammatory markers and oxidative parameters as prognostic factors in early neonatal sepsis. METHODS: We conducted a prospective observational study by collecting data from 120 patients in the maternity unit of a university hospital. Preterm (<37 weeks of pregnancy) infants with at least one additional risk factor for neonatal sepsis were included. The levels of interleukin (IL)-6, IL-10, thiobarbituric acid reactive species (TBARS) and protein carbonyls and their association with sepsis severity were determined in the cord blood. RESULTS: Levels of IL-6 and TBARS, but not IL-10 and protein carbonyls, demonstrated a mild to moderate correlation with the SNAPPE-II severity score (r=0.435, p=0.02 and r = 0.385, p = 0.017, respectively). No correlations were found between these markers and mortality. CONCLUSION: TBARS and IL-6 have a mild to moderate correlation with SNAPPE-II, but none of the studied markers were able to predict mortality in our sample.
Keywords:Fetal bloodInfant, newbornIntensive care units, neonatalInterleukin-10Interleukin-6Oxidative stressSepsisSee more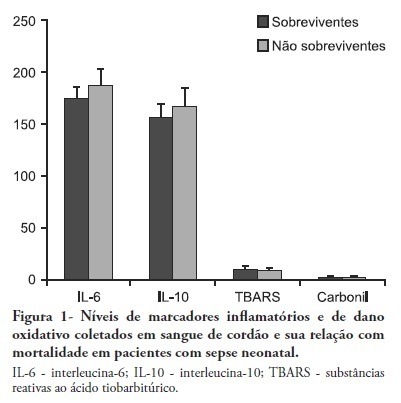
-
Original Articles – Clinical Research
Thrombocitopenia in sepsis: an important prognosis factor
Rev Bras Ter Intensiva. 2012;24(1):35-42
Abstract
Original Articles – Clinical ResearchThrombocitopenia in sepsis: an important prognosis factor
Rev Bras Ter Intensiva. 2012;24(1):35-42
DOI 10.1590/S0103-507X2012000100006
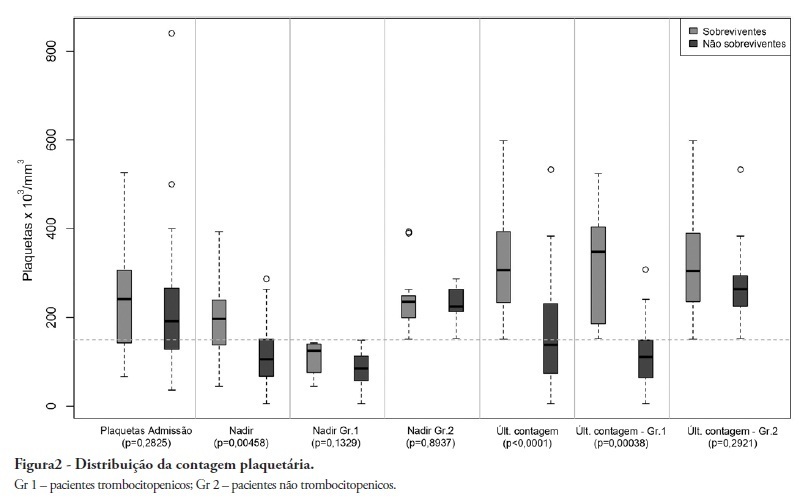
Views0See moreOBJECTIVE: To demonstrate an association between thrombocytopenia and platelet behavior in predicting mortality in septic patients. METHODS: Patients with criteria for sepsis at admission or at any time during hospitalization were selected; patients hospitalized for less than 24 hours were excluded. Thrombocytopenia was defined as a platelet count lower than 150.000/mm³, and recovery was defined as returning to levels above 150.000/mm³ after showing thrombocytopenia. We assessed the admission prognosis variables (APACHE II), platelet counts during the hospitalization and outcomes. RESULTS: Of the 56 patients included, 34 developed thrombocytopenia during sepsis (Group 1) and had a 76.4% mortality rate. The mortality rate among patients not showing thrombocytopenia (Group 2) was 40.9% (RR 1.87; 95% CI 1.12 – 3.12; p = 0.0163). In 44.1% of Group 1 patients, the platelet counts drops by >50% compared with the admission counts; 93.3% of these patients eventually died (RR 1.48; 95% CI 0.93 – 2.36; p = 0.0528). Among the Group 1 patients showing recovered platelet counts, 53.3% survived; 100% of the patients with unrecovered thrombocytopenia died (RR 2.14; 95% CI 1.35 – 3.39; p = 0.0003). Among the patients with APACHE II scores > 22, the thrombocytopenic patients had an 81.8% mortality rate (p = 0.25), while no deaths occurred among the non-thrombocytopenic patients. For the patients with APACHE II scores ≤ 22, the mortality rate of the thrombocytopenic patients was 74% (p = 0.0741), versus 42.8% for the non-thrombocytopenic patients. CONCLUSION: For this sample of septic patients, thrombocytopenia and its progression, defined as a >50% drop or failure to recover platelet count, were shown to be markers of poor prognosis.
Views0Abstract
Original Articles – Clinical ResearchThrombocitopenia in sepsis: an important prognosis factor
Rev Bras Ter Intensiva. 2012;24(1):35-42
DOI 10.1590/S0103-507X2012000100006
Views0See moreOBJECTIVE: To demonstrate an association between thrombocytopenia and platelet behavior in predicting mortality in septic patients. METHODS: Patients with criteria for sepsis at admission or at any time during hospitalization were selected; patients hospitalized for less than 24 hours were excluded. Thrombocytopenia was defined as a platelet count lower than 150.000/mm³, and recovery was defined as returning to levels above 150.000/mm³ after showing thrombocytopenia. We assessed the admission prognosis variables (APACHE II), platelet counts during the hospitalization and outcomes. RESULTS: Of the 56 patients included, 34 developed thrombocytopenia during sepsis (Group 1) and had a 76.4% mortality rate. The mortality rate among patients not showing thrombocytopenia (Group 2) was 40.9% (RR 1.87; 95% CI 1.12 – 3.12; p = 0.0163). In 44.1% of Group 1 patients, the platelet counts drops by >50% compared with the admission counts; 93.3% of these patients eventually died (RR 1.48; 95% CI 0.93 – 2.36; p = 0.0528). Among the Group 1 patients showing recovered platelet counts, 53.3% survived; 100% of the patients with unrecovered thrombocytopenia died (RR 2.14; 95% CI 1.35 – 3.39; p = 0.0003). Among the patients with APACHE II scores > 22, the thrombocytopenic patients had an 81.8% mortality rate (p = 0.25), while no deaths occurred among the non-thrombocytopenic patients. For the patients with APACHE II scores ≤ 22, the mortality rate of the thrombocytopenic patients was 74% (p = 0.0741), versus 42.8% for the non-thrombocytopenic patients. CONCLUSION: For this sample of septic patients, thrombocytopenia and its progression, defined as a >50% drop or failure to recover platelet count, were shown to be markers of poor prognosis.
-
Original Articles – Clinical Research
Positive end-expiratory pressure increases strain in patients with ALI/ARDS
Rev Bras Ter Intensiva. 2012;24(1):43-51
Abstract
Original Articles – Clinical ResearchPositive end-expiratory pressure increases strain in patients with ALI/ARDS
Rev Bras Ter Intensiva. 2012;24(1):43-51
DOI 10.1590/S0103-507X2012000100007
Views0OBJECTIVE: The objective of this study was to assess the effects of positive end-expiratory pressure on recruitment, cyclic recruitment and derecruitment and strain in patients with acute lung injury and acute respiratory distress syndrome using lung computed tomography. METHODS: This is an open, controlled, non-randomized interventional study of ten patients with acute lung injury and acute respiratory distress syndrome. Using computed tomography, single, basal slices of the lung were obtained during inspiratory and expiratory pauses at a tidal volume of 6 ml/kg and a positive end-expiratory pressure of 5, 10, 15 and 20 cmH2O. The densities of the lung parenchyma were measured in Hounsfield units. The values for positive end-expiratory pressure-induced recruitment, cyclic recruitment and derecruitment and strain were then calculated. RESULTS: Increasing levels of positive end-expiratory pressure were correlated with increased recruitment and global strain (p < 0.01), which was significantly correlated with plateau pressure (r² = 0.97, p < 0.01). In addition, increasing levels of positive end-expiratory pressure systematically increased strain along the sternovertebral axis. CONCLUSION: While strain is an adverse effect of positive end-expiratory pressure, the decision use positive end-expiratory pressure with any patient should be balanced against the potential benefits of recruitment. Due to the small number of patients in this study, the present data should be treated as hypothesis generating and is not intended to limit the clinical application of a high level of positive end-expiratory pressure in patients with severe hypoxemia.
Keywords:Positive end-expiratory pressureRespiration, artificialRespiratory distress syndrome, adultTomography, X-ray computedSee moreViews0Abstract
Original Articles – Clinical ResearchPositive end-expiratory pressure increases strain in patients with ALI/ARDS
Rev Bras Ter Intensiva. 2012;24(1):43-51
DOI 10.1590/S0103-507X2012000100007
Views0OBJECTIVE: The objective of this study was to assess the effects of positive end-expiratory pressure on recruitment, cyclic recruitment and derecruitment and strain in patients with acute lung injury and acute respiratory distress syndrome using lung computed tomography. METHODS: This is an open, controlled, non-randomized interventional study of ten patients with acute lung injury and acute respiratory distress syndrome. Using computed tomography, single, basal slices of the lung were obtained during inspiratory and expiratory pauses at a tidal volume of 6 ml/kg and a positive end-expiratory pressure of 5, 10, 15 and 20 cmH2O. The densities of the lung parenchyma were measured in Hounsfield units. The values for positive end-expiratory pressure-induced recruitment, cyclic recruitment and derecruitment and strain were then calculated. RESULTS: Increasing levels of positive end-expiratory pressure were correlated with increased recruitment and global strain (p < 0.01), which was significantly correlated with plateau pressure (r² = 0.97, p < 0.01). In addition, increasing levels of positive end-expiratory pressure systematically increased strain along the sternovertebral axis. CONCLUSION: While strain is an adverse effect of positive end-expiratory pressure, the decision use positive end-expiratory pressure with any patient should be balanced against the potential benefits of recruitment. Due to the small number of patients in this study, the present data should be treated as hypothesis generating and is not intended to limit the clinical application of a high level of positive end-expiratory pressure in patients with severe hypoxemia.
Keywords:Positive end-expiratory pressureRespiration, artificialRespiratory distress syndrome, adultTomography, X-ray computedSee more
-
Original Articles – Clinical Research
The incidence of delirium in patients pretreated with statins who remain in an intensive care unit after cardiac surgery
Rev Bras Ter Intensiva. 2012;24(1):52-57
Abstract
Original Articles – Clinical ResearchThe incidence of delirium in patients pretreated with statins who remain in an intensive care unit after cardiac surgery
Rev Bras Ter Intensiva. 2012;24(1):52-57
DOI 10.1590/S0103-507X2012000100008
Views0OBJECTIVE: To determine the association between the preoperative administration of statins and postoperative delirium in a prospective cohort of patients undergoing cardiac surgery. METHODS: All adult patients who were admitted to the intensive care unit following cardiac surgery between January and June 2011 were included. Delirium was screened during the postoperative period using the Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Intensive Care Delirium Screening Checklist (ICDSC). RESULTS: A total of 169 patients underwent elective cardiac surgery, and 40.2% of the patients were treated preoperatively with statins. Delirium was identified using the CAM-ICU in 14.9% of patients not taking preoperative statins in comparison with 11.8% of the patients taking statins (p = 0.817). Using the ICDSC, delirium was identified in 18.8% of patients not taking statins in comparison with 10.3% of the patients taking statins (p = 0.191). CONCLUSION: The use of preoperative statins is not correlated with postoperative delirium in patients undergoing cardiac surgery.
Keywords:Cardiac surgeryDeliriumHydroxymethylglutaryl-CoA reductase inhibitorsIntensive care unitsPostoperative periodSee moreViews0Abstract
Original Articles – Clinical ResearchThe incidence of delirium in patients pretreated with statins who remain in an intensive care unit after cardiac surgery
Rev Bras Ter Intensiva. 2012;24(1):52-57
DOI 10.1590/S0103-507X2012000100008
Views0OBJECTIVE: To determine the association between the preoperative administration of statins and postoperative delirium in a prospective cohort of patients undergoing cardiac surgery. METHODS: All adult patients who were admitted to the intensive care unit following cardiac surgery between January and June 2011 were included. Delirium was screened during the postoperative period using the Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Intensive Care Delirium Screening Checklist (ICDSC). RESULTS: A total of 169 patients underwent elective cardiac surgery, and 40.2% of the patients were treated preoperatively with statins. Delirium was identified using the CAM-ICU in 14.9% of patients not taking preoperative statins in comparison with 11.8% of the patients taking statins (p = 0.817). Using the ICDSC, delirium was identified in 18.8% of patients not taking statins in comparison with 10.3% of the patients taking statins (p = 0.191). CONCLUSION: The use of preoperative statins is not correlated with postoperative delirium in patients undergoing cardiac surgery.
Keywords:Cardiac surgeryDeliriumHydroxymethylglutaryl-CoA reductase inhibitorsIntensive care unitsPostoperative periodSee more -
Original Articles – Clinical Research
Expiratory peak flow and respiratory system resistance in mechanically ventilated patients undergoing two different forms of manually assisted cough
Rev Bras Ter Intensiva. 2012;24(1):58-63
Abstract
Original Articles – Clinical ResearchExpiratory peak flow and respiratory system resistance in mechanically ventilated patients undergoing two different forms of manually assisted cough
Rev Bras Ter Intensiva. 2012;24(1):58-63
DOI 10.1590/S0103-507X2012000100009
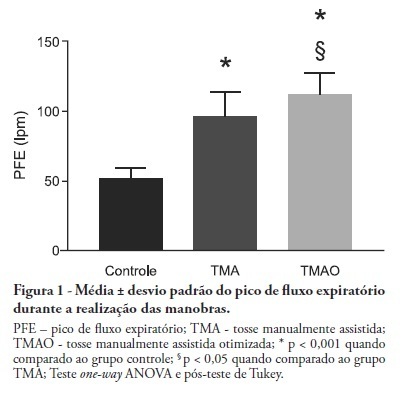
Views0See moreOBJECTIVE: Mechanical ventilation is associated with retained airway secretions. Manually assisted cough contributes to the displacement of bronchial mucus, whereas positive end-expiratory pressure increases collateral ventilation and maintains airway patency. This study aimed to assess the effects of manually assisted cough, either alone or added to increased positive end-expiratory pressure and inspiratory time (optimized manually assisted cough), on the expiratory peak flow and respiratory system mechanics in mechanically ventilated patients. METHODS: In this controlled and randomized clinical trial, respiratory mechanics and expiratory peak flow were assessed in male and female patients undergoing either tracheal suctioning alone, manually assisted cough followed by tracheal suctioning or optimized manually assisted cough followed by tracheal suctioning. RESULTS: Thirty-five patients completed the trial. Respiratory system resistance was significantly reduced after optimized manually assisted cough (16.0 ± 3.6 versus 12.4 ± 3.1 cmH2O/L/s; p = 0.04). The expiratory peak flow during optimized manually assisted cough was significantly higher in comparison with the values observed during manually assisted cough (112.3 ± 15.6 versus 95.8 ± 18.3 Lpm; p < 0.05). Both values were significantly higher than the values observed in the group undergoing tracheal suctioning alone (52.0 ± 7.6 Lpm; p < 0.001). CONCLUSION: Optimized manually assisted cough increases the expiratory peak flow in comparison with manually assisted cough; in addition, this procedure reduces respiratory system resistance.
Views0Abstract
Original Articles – Clinical ResearchExpiratory peak flow and respiratory system resistance in mechanically ventilated patients undergoing two different forms of manually assisted cough
Rev Bras Ter Intensiva. 2012;24(1):58-63
DOI 10.1590/S0103-507X2012000100009
Views0See moreOBJECTIVE: Mechanical ventilation is associated with retained airway secretions. Manually assisted cough contributes to the displacement of bronchial mucus, whereas positive end-expiratory pressure increases collateral ventilation and maintains airway patency. This study aimed to assess the effects of manually assisted cough, either alone or added to increased positive end-expiratory pressure and inspiratory time (optimized manually assisted cough), on the expiratory peak flow and respiratory system mechanics in mechanically ventilated patients. METHODS: In this controlled and randomized clinical trial, respiratory mechanics and expiratory peak flow were assessed in male and female patients undergoing either tracheal suctioning alone, manually assisted cough followed by tracheal suctioning or optimized manually assisted cough followed by tracheal suctioning. RESULTS: Thirty-five patients completed the trial. Respiratory system resistance was significantly reduced after optimized manually assisted cough (16.0 ± 3.6 versus 12.4 ± 3.1 cmH2O/L/s; p = 0.04). The expiratory peak flow during optimized manually assisted cough was significantly higher in comparison with the values observed during manually assisted cough (112.3 ± 15.6 versus 95.8 ± 18.3 Lpm; p < 0.05). Both values were significantly higher than the values observed in the group undergoing tracheal suctioning alone (52.0 ± 7.6 Lpm; p < 0.001). CONCLUSION: Optimized manually assisted cough increases the expiratory peak flow in comparison with manually assisted cough; in addition, this procedure reduces respiratory system resistance.
-
Original Articles – Clinical Research
The effects of orthostatism in adult intensive care unit patients
Rev Bras Ter Intensiva. 2012;24(1):64-70
Abstract
Original Articles – Clinical ResearchThe effects of orthostatism in adult intensive care unit patients
Rev Bras Ter Intensiva. 2012;24(1):64-70
DOI 10.1590/S0103-507X2012000100010
Views0See moreOBJECTIVE: To assess the consciousness level, pulmonary and hemodynamic effects of orthostatic position in intensive care patients. METHODS: This study was conducted from April 2008 to July 2009 in the Adult Intensive Care Unit, Hospital das Clínicas, Universidade Estadual de Campinas, São Paulo, Brazil. Fifteen patients were included who were mechanically ventilated for more than seven days and had the following characteristics: tracheotomized; receiving intermittent nebulization; maximal inspiratory pressure of less than -25 cm H2O; Tobin score less than 105; preserved respiratory drive; not sedated; partial arterial oxygen pressure greater than 70 mm Hg; oxygen saturation greater than 90%; and hemodynamically stable. With inclinations of 0º, 30º and 50º, the following parameters were recorded: consciousness level; blinking reflex; thoracoabdominal cirtometry; vital capacity; tidal volume; minute volume; respiratory muscle strength; and vital signs. RESULTS: No neurological level changes were observed. Respiratory rate and minute volume (V E) decreased at 30% and later increased at 50%; however, these changes were not statistically significant. Abdominal cirtometry and maximal expiratory pressure increased, but again, the changes were not statistically significant. Regarding maximal inspiratory pressure and vital capacity, statistically significant increases were seen in the comparison between the 50º and 0º inclinations. However, tidal volume increased with time in the comparisons between 30º and 0º and between 50º and 0º. Mean blood pressure increased only for the comparison of 50º versus 0º. Heart rate increased with time for the comparisons between 30º and 0º, between 50º and 0º and between 50º and 30º. CONCLUSION: Passive orthostatism resulted in improved tidal volume and vital capacity, maximal inspiratory pressure and increased heart rate and mean blood pressure in critically ill patients.
Views0Abstract
Original Articles – Clinical ResearchThe effects of orthostatism in adult intensive care unit patients
Rev Bras Ter Intensiva. 2012;24(1):64-70
DOI 10.1590/S0103-507X2012000100010
Views0See moreOBJECTIVE: To assess the consciousness level, pulmonary and hemodynamic effects of orthostatic position in intensive care patients. METHODS: This study was conducted from April 2008 to July 2009 in the Adult Intensive Care Unit, Hospital das Clínicas, Universidade Estadual de Campinas, São Paulo, Brazil. Fifteen patients were included who were mechanically ventilated for more than seven days and had the following characteristics: tracheotomized; receiving intermittent nebulization; maximal inspiratory pressure of less than -25 cm H2O; Tobin score less than 105; preserved respiratory drive; not sedated; partial arterial oxygen pressure greater than 70 mm Hg; oxygen saturation greater than 90%; and hemodynamically stable. With inclinations of 0º, 30º and 50º, the following parameters were recorded: consciousness level; blinking reflex; thoracoabdominal cirtometry; vital capacity; tidal volume; minute volume; respiratory muscle strength; and vital signs. RESULTS: No neurological level changes were observed. Respiratory rate and minute volume (V E) decreased at 30% and later increased at 50%; however, these changes were not statistically significant. Abdominal cirtometry and maximal expiratory pressure increased, but again, the changes were not statistically significant. Regarding maximal inspiratory pressure and vital capacity, statistically significant increases were seen in the comparison between the 50º and 0º inclinations. However, tidal volume increased with time in the comparisons between 30º and 0º and between 50º and 0º. Mean blood pressure increased only for the comparison of 50º versus 0º. Heart rate increased with time for the comparisons between 30º and 0º, between 50º and 0º and between 50º and 30º. CONCLUSION: Passive orthostatism resulted in improved tidal volume and vital capacity, maximal inspiratory pressure and increased heart rate and mean blood pressure in critically ill patients.
-
Original Articles – Clinical Research
Effects of passive mobilization on acute hemodynamic responses in mechanically ventilated patients
Rev Bras Ter Intensiva. 2012;24(1):72-78
Abstract
Original Articles – Clinical ResearchEffects of passive mobilization on acute hemodynamic responses in mechanically ventilated patients
Rev Bras Ter Intensiva. 2012;24(1):72-78
DOI 10.1590/S0103-507X2012000100011
Views0See moreOBJECTIVE: To assess the effects of passive mobilization on acute hemodynamic responses in mechanically ventilated patients. METHODS: This cross-sectional, quantitative, observational study enrolled patients who were admitted to the intensive care unit, sedated and mechanically ventilated. The infusion of sedative and analgesic drugs aimed to maintain a Ramsay scale sedation level of 4 to 6. Passive mobilization consisted of hip and knee flexion-extension movements for five minutes. After 10 minutes of rest, an additional five minutes of flexion-extension passive movements was performed for the shoulders. Hemodynamic assessments (heart rate and systolic, diastolic and mean blood pressure) were performed one minute before the mobilization protocol and one minute after each phase. The double product and myocardial oxygen consumption were calculated using appropriate formulas. RESULTS: A total of 13 patients (69.2% male, with a mean age of 69.1 ± 15.8 years) were admitted from June to December, 2011. Passive mobilization led to statistically significant increases in heart rate, double product and myocardial oxygen consumption. However, mean blood pressure was not significantly altered. CONCLUSIONS: Our results suggest that passive mobilization of mechanically ventilated and sedated patients is safe and provides beneficial effects on acute hemodynamic parameters, particularly heart rate, although mean blood pressure is not significantly altered
Views0Abstract
Original Articles – Clinical ResearchEffects of passive mobilization on acute hemodynamic responses in mechanically ventilated patients
Rev Bras Ter Intensiva. 2012;24(1):72-78
DOI 10.1590/S0103-507X2012000100011
Views0See moreOBJECTIVE: To assess the effects of passive mobilization on acute hemodynamic responses in mechanically ventilated patients. METHODS: This cross-sectional, quantitative, observational study enrolled patients who were admitted to the intensive care unit, sedated and mechanically ventilated. The infusion of sedative and analgesic drugs aimed to maintain a Ramsay scale sedation level of 4 to 6. Passive mobilization consisted of hip and knee flexion-extension movements for five minutes. After 10 minutes of rest, an additional five minutes of flexion-extension passive movements was performed for the shoulders. Hemodynamic assessments (heart rate and systolic, diastolic and mean blood pressure) were performed one minute before the mobilization protocol and one minute after each phase. The double product and myocardial oxygen consumption were calculated using appropriate formulas. RESULTS: A total of 13 patients (69.2% male, with a mean age of 69.1 ± 15.8 years) were admitted from June to December, 2011. Passive mobilization led to statistically significant increases in heart rate, double product and myocardial oxygen consumption. However, mean blood pressure was not significantly altered. CONCLUSIONS: Our results suggest that passive mobilization of mechanically ventilated and sedated patients is safe and provides beneficial effects on acute hemodynamic parameters, particularly heart rate, although mean blood pressure is not significantly altered
-
Original Articles – Clinical Research
Late-onset sepsis in preterm children in a neonatal intensive care unit: a three-year analysis
Rev Bras Ter Intensiva. 2012;24(1):79-85
Abstract
Original Articles – Clinical ResearchLate-onset sepsis in preterm children in a neonatal intensive care unit: a three-year analysis
Rev Bras Ter Intensiva. 2012;24(1):79-85
DOI 10.1590/S0103-507X2012000100012
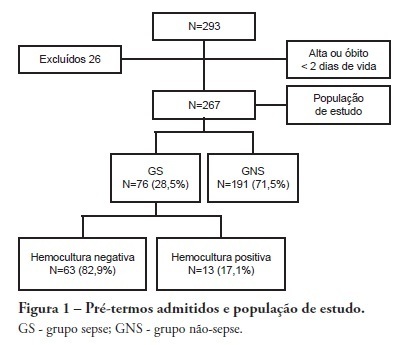
Views0See moreOBJECTIVE: To evaluate the prevalence factors and etiologies associated with late neonatal sepsis in preterm neonates in a neonatal intensive care unit. METHODS: This was a cross-sectional study of secondary data pertaining to preterm neonates admitted to the neonatal intensive care unit between 2008 and 2010 and was gathered from medical charts. The outcome variable, late neonatal sepsis, was characterized using the Brazilian national health surveillance agency criteria. Pearson’s Chi-squared test, Fisher’s exact test and the linear trend Chi-squared test were used to assess the qualitative variables for linear trends. The statistical significance level was set at p < 0.05. Bivariate and multivariate analyses of the independent and dependent variables were conducted to obtain a measure of the effect and prevalence ratios, considering a p-value of less than 0.20 to indicate statistical significance. RESULTS: This study included 267 preterm neonates. Of the participants, 28.5% were characterized as having late-onset sepsis. Positive blood cultures were recorded for 17.1% of the neonates. Death occurred in 8.2% of the total cases, and of these deaths, 68.2% occurred within the sepsis group. Three deaths were associated with positive blood cultures, all of which grew Gram-negative bacteria. The bivariate analysis demonstrated that as the gestational age and birth weight decreased, the prevalence of late-onset sepsis trended upward. Ten or more days on mechanical ventilation was associated with late-onset neonatal sepsis in 80.8% of cases. Peripherally inserted central catheters left in place for 11 or more days were associated with late-onset neonatal sepsis in 76.2% of cases. The multivariate analysis demonstrated that a peripherally inserted catheter left in place for less than 11 days was associated with late-onset neonatal sepsis. Gram-negative bacteria, including Klebsiella pneumoniae and Escherichia coli, were the most frequent causative agents. CONCLUSIONS: Late sepsis remains a concern because of its prevalence in intensive care units and because it increases the number of invasive procedures that preterm children usually undergo in these units. The authors emphasize the expanding role of Gram-negative bacteria in late-onset neonatal sepsis and the need for more efficient methods to identify confirmed sepsis.
Views0Abstract
Original Articles – Clinical ResearchLate-onset sepsis in preterm children in a neonatal intensive care unit: a three-year analysis
Rev Bras Ter Intensiva. 2012;24(1):79-85
DOI 10.1590/S0103-507X2012000100012
Views0See moreOBJECTIVE: To evaluate the prevalence factors and etiologies associated with late neonatal sepsis in preterm neonates in a neonatal intensive care unit. METHODS: This was a cross-sectional study of secondary data pertaining to preterm neonates admitted to the neonatal intensive care unit between 2008 and 2010 and was gathered from medical charts. The outcome variable, late neonatal sepsis, was characterized using the Brazilian national health surveillance agency criteria. Pearson’s Chi-squared test, Fisher’s exact test and the linear trend Chi-squared test were used to assess the qualitative variables for linear trends. The statistical significance level was set at p < 0.05. Bivariate and multivariate analyses of the independent and dependent variables were conducted to obtain a measure of the effect and prevalence ratios, considering a p-value of less than 0.20 to indicate statistical significance. RESULTS: This study included 267 preterm neonates. Of the participants, 28.5% were characterized as having late-onset sepsis. Positive blood cultures were recorded for 17.1% of the neonates. Death occurred in 8.2% of the total cases, and of these deaths, 68.2% occurred within the sepsis group. Three deaths were associated with positive blood cultures, all of which grew Gram-negative bacteria. The bivariate analysis demonstrated that as the gestational age and birth weight decreased, the prevalence of late-onset sepsis trended upward. Ten or more days on mechanical ventilation was associated with late-onset neonatal sepsis in 80.8% of cases. Peripherally inserted central catheters left in place for 11 or more days were associated with late-onset neonatal sepsis in 76.2% of cases. The multivariate analysis demonstrated that a peripherally inserted catheter left in place for less than 11 days was associated with late-onset neonatal sepsis. Gram-negative bacteria, including Klebsiella pneumoniae and Escherichia coli, were the most frequent causative agents. CONCLUSIONS: Late sepsis remains a concern because of its prevalence in intensive care units and because it increases the number of invasive procedures that preterm children usually undergo in these units. The authors emphasize the expanding role of Gram-negative bacteria in late-onset neonatal sepsis and the need for more efficient methods to identify confirmed sepsis.
-
Review Articles
Use of intravenous magnesium sulfate for the treatment of severe acute asthma in children in emergency department
Rev Bras Ter Intensiva. 2012;24(1):86-90
Abstract
Review ArticlesUse of intravenous magnesium sulfate for the treatment of severe acute asthma in children in emergency department
Rev Bras Ter Intensiva. 2012;24(1):86-90
DOI 10.1590/S0103-507X2012000100013
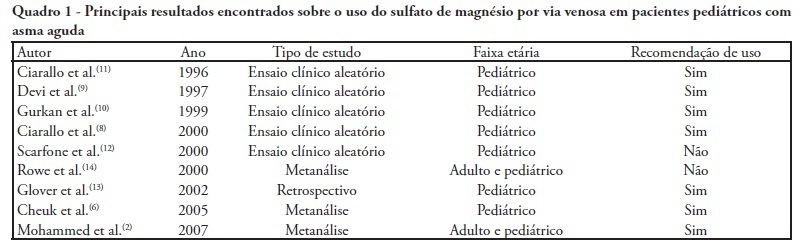
Views0See moreSevere acute asthma is a medical emergency that must be quickly diagnosed and treated. Initial treatment includes a bronchodilator agent and systemic corticosteroids. In severe cases with poor response to the standard treatment, intravenous magnesium sulfate is a therapeutic option. This article aimed a literature review on the use of intravenous magnesium sulfate in the emergency room treatment of children with acute asthma. The treatment parameters of effectiveness, indication, dosage, adverse effects and contraindications were assessed. A narrative review of the literature based on a search of the Medline and Lilacs databases and the Cochrane Database of Systematic Reviews for articles published between 2000 and 2010 was conducted. The keywords used included the following: asthma, children, emergency and magnesium sulfate. Eight controlled clinical trials, three meta-analyses, one retrospective study, eight review articles and one cross-sectional study were included. A total of 21 articles were analyzed. Several authors reported that intravenous magnesium was effective in the treatment of acute asthma in children. Adverse effects were rare. The use of intravenous magnesium sulfate was indicated for patients with moderate to severe acute asthma not responding to initial treatment with a bronchodilator agent and systemic corticosteroids. Few contraindications were reported but included kidney failure and atrioventricular block. Reports of adverse drug interactions with magnesium were rare. Although reported as safe, intravenous magnesium is infrequently used in children with acute asthma. Most often it is used in severe, progressed cases to prevent respiratory failure and/or admission to the intensive care unit. Intravenous magnesium was concluded to be effective and safe in children with severe acute asthma, although its use in the emergency room is still limited.
Views0Abstract
Review ArticlesUse of intravenous magnesium sulfate for the treatment of severe acute asthma in children in emergency department
Rev Bras Ter Intensiva. 2012;24(1):86-90
DOI 10.1590/S0103-507X2012000100013
Views0See moreSevere acute asthma is a medical emergency that must be quickly diagnosed and treated. Initial treatment includes a bronchodilator agent and systemic corticosteroids. In severe cases with poor response to the standard treatment, intravenous magnesium sulfate is a therapeutic option. This article aimed a literature review on the use of intravenous magnesium sulfate in the emergency room treatment of children with acute asthma. The treatment parameters of effectiveness, indication, dosage, adverse effects and contraindications were assessed. A narrative review of the literature based on a search of the Medline and Lilacs databases and the Cochrane Database of Systematic Reviews for articles published between 2000 and 2010 was conducted. The keywords used included the following: asthma, children, emergency and magnesium sulfate. Eight controlled clinical trials, three meta-analyses, one retrospective study, eight review articles and one cross-sectional study were included. A total of 21 articles were analyzed. Several authors reported that intravenous magnesium was effective in the treatment of acute asthma in children. Adverse effects were rare. The use of intravenous magnesium sulfate was indicated for patients with moderate to severe acute asthma not responding to initial treatment with a bronchodilator agent and systemic corticosteroids. Few contraindications were reported but included kidney failure and atrioventricular block. Reports of adverse drug interactions with magnesium were rare. Although reported as safe, intravenous magnesium is infrequently used in children with acute asthma. Most often it is used in severe, progressed cases to prevent respiratory failure and/or admission to the intensive care unit. Intravenous magnesium was concluded to be effective and safe in children with severe acute asthma, although its use in the emergency room is still limited.
-
Review Articles
Neurogenic pulmonary edema: a current literature review
Rev Bras Ter Intensiva. 2012;24(1):91-96
Abstract
Review ArticlesNeurogenic pulmonary edema: a current literature review
Rev Bras Ter Intensiva. 2012;24(1):91-96
DOI 10.1590/S0103-507X2012000100014
Views0See moreNeurogenic pulmonary edema in the setting of critically ill neurologic patients is a condition that is not fully understood, and it is a relatively rare condition. Severe brain damage, such as cerebral and subarachnoid hemorrhage, head injuries and seizures, represents a risk factor for developing neurogenic pulmonary edema. Misdiagnosis and inappropriate management may worsen cerebral damage because of secondary brain injury from hypoxemia or reduced cerebral perfusion pressure. These factors may increase morbidity and mortality. This study aimed to review the current concepts on pathophysiologic mechanisms involved in the development of neurogenic pulmonary edema and discuss the associated clinical and therapeutic aspects.
Views0Abstract
Review ArticlesNeurogenic pulmonary edema: a current literature review
Rev Bras Ter Intensiva. 2012;24(1):91-96
DOI 10.1590/S0103-507X2012000100014
Views0See moreNeurogenic pulmonary edema in the setting of critically ill neurologic patients is a condition that is not fully understood, and it is a relatively rare condition. Severe brain damage, such as cerebral and subarachnoid hemorrhage, head injuries and seizures, represents a risk factor for developing neurogenic pulmonary edema. Misdiagnosis and inappropriate management may worsen cerebral damage because of secondary brain injury from hypoxemia or reduced cerebral perfusion pressure. These factors may increase morbidity and mortality. This study aimed to review the current concepts on pathophysiologic mechanisms involved in the development of neurogenic pulmonary edema and discuss the associated clinical and therapeutic aspects.
-
Review Articles
Nutrition therapy in severe head trauma patients
Rev Bras Ter Intensiva. 2012;24(1):97-105
Abstract
Review ArticlesNutrition therapy in severe head trauma patients
Rev Bras Ter Intensiva. 2012;24(1):97-105
DOI 10.1590/S0103-507X2012000100015
Views0This article reviews the literature, organizes the major findings, and generates the best evidence-based recommendations on nutrition therapy for head trauma patients. Despite recent advances in head trauma diagnosis and therapy, the mortality associated with this condition remains high. Few therapeutic interventions have been proven to effectively improve this condition. Head trauma causes multiple metabolic and electrolytic disorders; it is characterized by a hypermetabolic state that is associated with intensive catabolism, leading to specific nutritional needs. The current literature lacks specific guidelines for nutrition therapy in severe head trauma patients, although a substantial amount of data has been reported and relevant issues are currently being studied; these data may allow better nutrition therapy guidelines for these patients. In addition to a well-trained multi-disciplinary team, the following recommendations appear to improve outcomes: introducing nutrition therapy early; preferred enteral administration; appropriate energy intake; formulations that are tailored to specific patients, including appropriate nutrients; and strict electrolytic and metabolic monitoring. Understanding the pathophysiology and the consequences of therapy is fundamental.
Keywords:Brain injuriescraniocerebral traumaenteral nutritionnutrition therapyNutritional supportparenteral nutritionSee moreViews0Abstract
Review ArticlesNutrition therapy in severe head trauma patients
Rev Bras Ter Intensiva. 2012;24(1):97-105
DOI 10.1590/S0103-507X2012000100015
Views0This article reviews the literature, organizes the major findings, and generates the best evidence-based recommendations on nutrition therapy for head trauma patients. Despite recent advances in head trauma diagnosis and therapy, the mortality associated with this condition remains high. Few therapeutic interventions have been proven to effectively improve this condition. Head trauma causes multiple metabolic and electrolytic disorders; it is characterized by a hypermetabolic state that is associated with intensive catabolism, leading to specific nutritional needs. The current literature lacks specific guidelines for nutrition therapy in severe head trauma patients, although a substantial amount of data has been reported and relevant issues are currently being studied; these data may allow better nutrition therapy guidelines for these patients. In addition to a well-trained multi-disciplinary team, the following recommendations appear to improve outcomes: introducing nutrition therapy early; preferred enteral administration; appropriate energy intake; formulations that are tailored to specific patients, including appropriate nutrients; and strict electrolytic and metabolic monitoring. Understanding the pathophysiology and the consequences of therapy is fundamental.
Keywords:Brain injuriescraniocerebral traumaenteral nutritionnutrition therapyNutritional supportparenteral nutritionSee more -
Case Report
Multidisciplinary care in the intensive care unit for a patient with Prader-Willi syndrome: a dental approach
Rev Bras Ter Intensiva. 2012;24(1):106-110
Abstract
Case ReportMultidisciplinary care in the intensive care unit for a patient with Prader-Willi syndrome: a dental approach
Rev Bras Ter Intensiva. 2012;24(1):106-110
DOI 10.1590/S0103-507X2012000100016
Views1Prader-Willi syndrome is a genetic neurobehavioral disease affecting children’s development and resulting in obesity, reduced height, hypotonia, endocrine disorders and cognitive deficits, which may impair oral integrity. This study aims to report on a case involving a white male 15-year-old patient with Prader-Willi syndrome whose oral examination revealed bacterial plaque, gingivitis, poor occlusion, viscous salivation and multiple lip, jugal mucosa, inserted gum and tongue ulcerations. An excision biopsy revealed oral ulcerations typical of herpes, which were considered to be likely to correlate with herpes encephalitis. This result demonstrates that a large portion of the deleterious effects of Prader-Willi syndrome can be attenuated by appropriate diagnosis and early therapeutic intervention, highlighting the role of an integrated multidisciplinary team in the development of therapeutic protocols for Prader-Willi syndrome patients.
Keywords:Case reportsDental care for person with disabilitiesHerpes simplexIntellectual disabilityIntensive careMorbid obesityPrader-Willi syndromeSee moreViews1Abstract
Case ReportMultidisciplinary care in the intensive care unit for a patient with Prader-Willi syndrome: a dental approach
Rev Bras Ter Intensiva. 2012;24(1):106-110
DOI 10.1590/S0103-507X2012000100016
Views1Prader-Willi syndrome is a genetic neurobehavioral disease affecting children’s development and resulting in obesity, reduced height, hypotonia, endocrine disorders and cognitive deficits, which may impair oral integrity. This study aims to report on a case involving a white male 15-year-old patient with Prader-Willi syndrome whose oral examination revealed bacterial plaque, gingivitis, poor occlusion, viscous salivation and multiple lip, jugal mucosa, inserted gum and tongue ulcerations. An excision biopsy revealed oral ulcerations typical of herpes, which were considered to be likely to correlate with herpes encephalitis. This result demonstrates that a large portion of the deleterious effects of Prader-Willi syndrome can be attenuated by appropriate diagnosis and early therapeutic intervention, highlighting the role of an integrated multidisciplinary team in the development of therapeutic protocols for Prader-Willi syndrome patients.
Keywords:Case reportsDental care for person with disabilitiesHerpes simplexIntellectual disabilityIntensive careMorbid obesityPrader-Willi syndromeSee more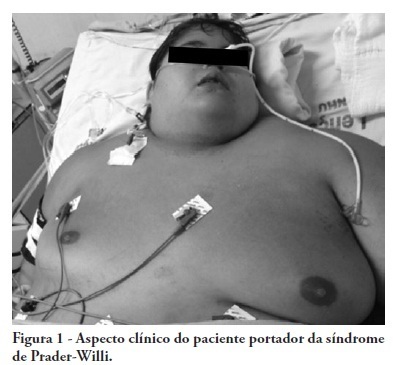
Volume Articles - Critical Care Science (CCS)
