risk factors Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2016;28(4):405-412
DOI 10.5935/0103-507X.20160065
To compare patients without previously diagnosed cardiovascular risk factors) and patients with one or more risk factors admitted with acute coronary syndrome.
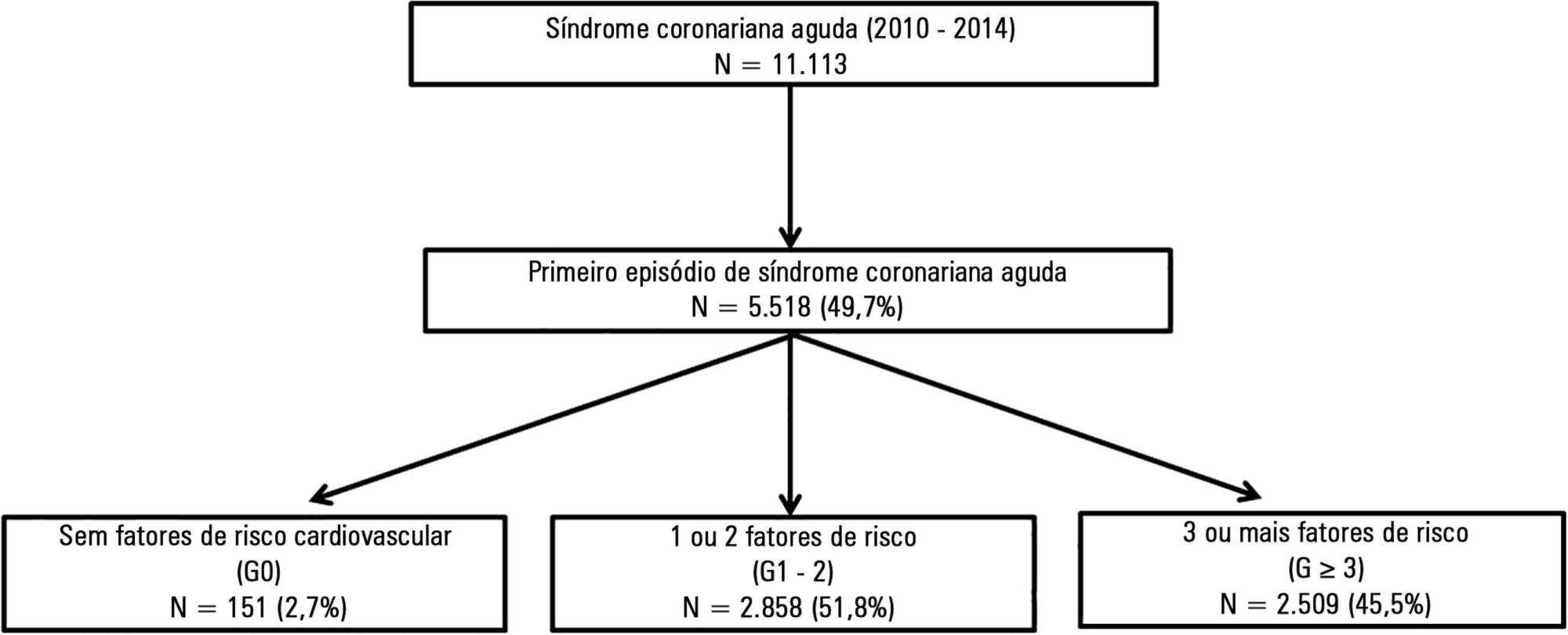
This was a retrospective analysis of patients admitted with first episode of acute coronary syndrome without previous heart disease, who were included in a national acute coronary syndrome registry. The patients were divided according to the number of risk factors, as follows: 0 risk factor (G0), 1 or 2 risk factors (G1 - 2) and 3 or more risk factors (G ≥ 3). Comparative analysis was performed between the three groups, and independent predictors of cardiac arrest and death were studied.
A total of 5,518 patients were studied, of which 72.2% were male and the mean age was 64 ± 14 years. G0 had a greater incidence of ST-segment elevation myocardial infarction, with the left anterior descending artery being the most frequently involved vessel, and a lower prevalence of multivessel disease. Even though G0 had a lower Killip class (96% in Killip I; p < 0.001) and higher ejection fraction (G0 56 ± 10% versus G1 - 2 and G ≥ 3 53 ± 12%; p = 0.024) on admission, there was a significant higher incidence of cardiac arrest. Multivariate analysis identified the absence of risk factors as an independent predictor of cardiac arrest (OR 2.78; p = 0.019). Hospital mortality was slightly higher in G0, although this difference was not significant. By Cox regression analysis, the number of risk factors was found not to be associated with mortality. Predictors of death at 1 year follow up included age (OR 1.05; p < 0.001), ST-segment elevation myocardial infarction (OR 1.94; p = 0.003) and ejection fraction < 50% (OR 2.34; p < 0.001).
Even though the group without risk factors was composed of younger patients with fewer comorbidities, better left ventricular function and less extensive coronary disease, the absence of risk factors was an independent predictor of cardiac arrest.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):405-412
DOI 10.5935/0103-507X.20160065
To compare patients without previously diagnosed cardiovascular risk factors) and patients with one or more risk factors admitted with acute coronary syndrome.
This was a retrospective analysis of patients admitted with first episode of acute coronary syndrome without previous heart disease, who were included in a national acute coronary syndrome registry. The patients were divided according to the number of risk factors, as follows: 0 risk factor (G0), 1 or 2 risk factors (G1 - 2) and 3 or more risk factors (G ≥ 3). Comparative analysis was performed between the three groups, and independent predictors of cardiac arrest and death were studied.
A total of 5,518 patients were studied, of which 72.2% were male and the mean age was 64 ± 14 years. G0 had a greater incidence of ST-segment elevation myocardial infarction, with the left anterior descending artery being the most frequently involved vessel, and a lower prevalence of multivessel disease. Even though G0 had a lower Killip class (96% in Killip I; p < 0.001) and higher ejection fraction (G0 56 ± 10% versus G1 - 2 and G ≥ 3 53 ± 12%; p = 0.024) on admission, there was a significant higher incidence of cardiac arrest. Multivariate analysis identified the absence of risk factors as an independent predictor of cardiac arrest (OR 2.78; p = 0.019). Hospital mortality was slightly higher in G0, although this difference was not significant. By Cox regression analysis, the number of risk factors was found not to be associated with mortality. Predictors of death at 1 year follow up included age (OR 1.05; p < 0.001), ST-segment elevation myocardial infarction (OR 1.94; p = 0.003) and ejection fraction < 50% (OR 2.34; p < 0.001).
Even though the group without risk factors was composed of younger patients with fewer comorbidities, better left ventricular function and less extensive coronary disease, the absence of risk factors was an independent predictor of cardiac arrest.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):33-39
DOI 10.5935/0103-507X.20160011
The purpose of our study was to determine the admission factors associated with intensive care unit readmission among oncohematological patients.
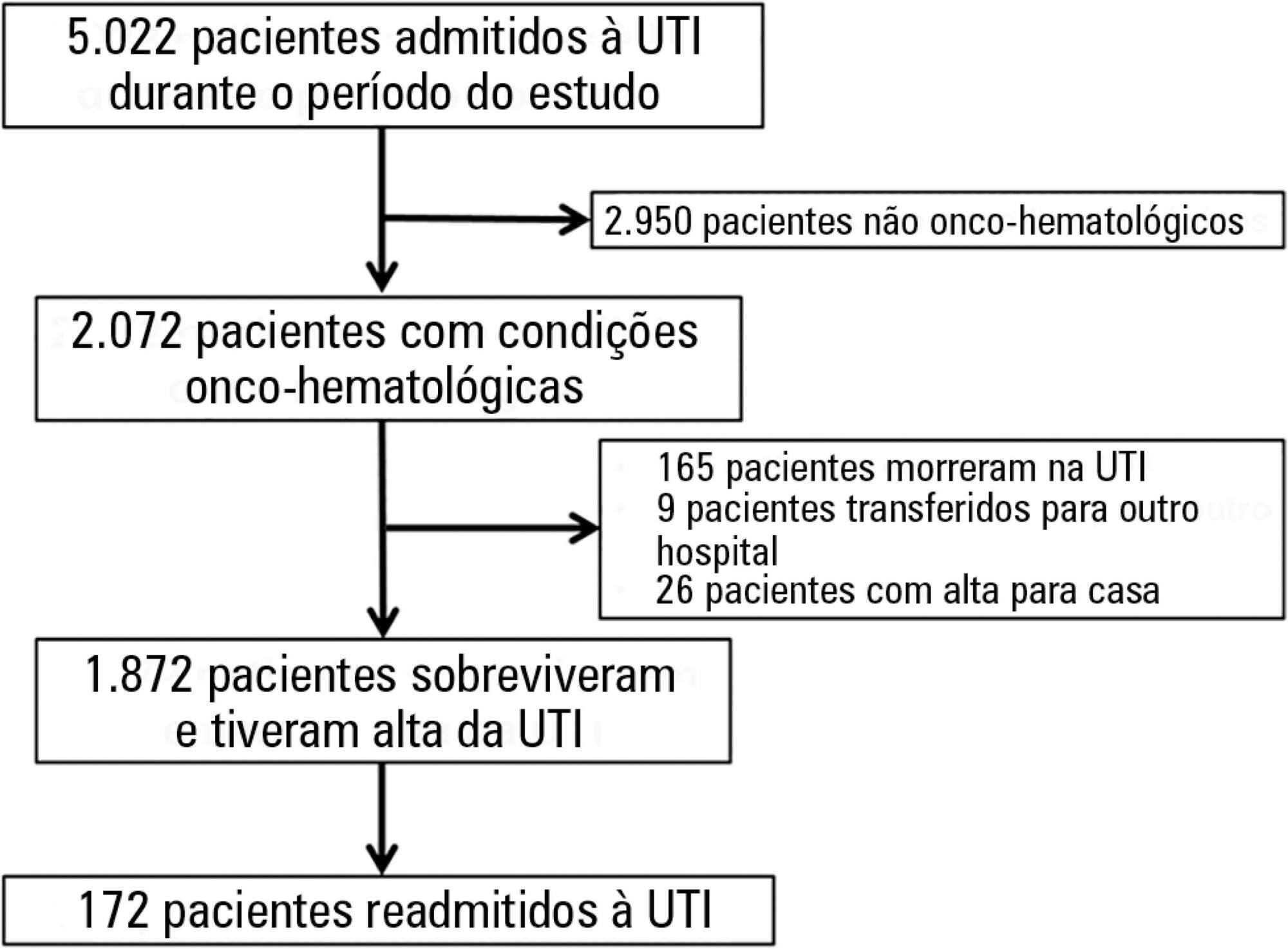
Retrospective cohort study using an intensive care unit database from a tertiary oncological center. The participants included 1,872 critically ill oncohematological patients who were admitted to the intensive care unit from January 2012 to December 2014 and who were subsequently discharged alive. We used univariate and multivariate analysis to identify the admission risk factors associated with later intensive care unit readmission.
One hundred seventy-two patients (9.2% of 1,872 oncohematological patients discharged alive from the intensive care unit) were readmitted after intensive care unit discharge. The readmitted patients were sicker compared with the non-readmitted group and had higher hospital mortality (32.6% versus 3.7%, respectively; p < 0.001). In the multivariate analysis, the independent risk factors for intensive care unit readmission were male sex (OR: 1.5, 95% CI: 1.07 - 2.12; p = 0.019), emergency surgery as the admission reason (OR: 2.91, 95%CI: 1.53 - 5.54; p = 0.001), longer hospital length of stay before intensive care unit transfer (OR: 1.02, 95%CI: 1.007 - 1.035; p = 0.003), and mechanical ventilation (OR: 2.31, 95%CI: 1.57 - 3.40; p < 0.001).
In this cohort of oncohematological patients, we identified some risk factors associated with intensive care unit readmission, most of which are not amenable to interventions. The identification of risk factors at intensive care unit discharge might be a promising approach.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):33-39
DOI 10.5935/0103-507X.20160011
The purpose of our study was to determine the admission factors associated with intensive care unit readmission among oncohematological patients.
Retrospective cohort study using an intensive care unit database from a tertiary oncological center. The participants included 1,872 critically ill oncohematological patients who were admitted to the intensive care unit from January 2012 to December 2014 and who were subsequently discharged alive. We used univariate and multivariate analysis to identify the admission risk factors associated with later intensive care unit readmission.
One hundred seventy-two patients (9.2% of 1,872 oncohematological patients discharged alive from the intensive care unit) were readmitted after intensive care unit discharge. The readmitted patients were sicker compared with the non-readmitted group and had higher hospital mortality (32.6% versus 3.7%, respectively; p < 0.001). In the multivariate analysis, the independent risk factors for intensive care unit readmission were male sex (OR: 1.5, 95% CI: 1.07 - 2.12; p = 0.019), emergency surgery as the admission reason (OR: 2.91, 95%CI: 1.53 - 5.54; p = 0.001), longer hospital length of stay before intensive care unit transfer (OR: 1.02, 95%CI: 1.007 - 1.035; p = 0.003), and mechanical ventilation (OR: 2.31, 95%CI: 1.57 - 3.40; p < 0.001).
In this cohort of oncohematological patients, we identified some risk factors associated with intensive care unit readmission, most of which are not amenable to interventions. The identification of risk factors at intensive care unit discharge might be a promising approach.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):397-404
DOI 10.5935/0103-507X.20160073
To identify factors associated with maternal death in patients admitted to an intensive care unit.
A cross-sectional study was conducted in a maternal intensive care unit. All medical records of patients admitted from January 2012 to December 2014 were reviewed. Pregnant and puerperal women were included; those with diagnoses of hydatidiform mole, ectopic pregnancy, or anembryonic pregnancy were excluded, as were patients admitted for non-obstetrical reasons. Death and hospital discharge were the outcomes subjected to comparative analysis.
A total of 373 patients aged 13 to 45 years were included. The causes for admission to the intensive care unit were hypertensive disorders of pregnancy, followed by heart disease, respiratory failure, and sepsis; complications included acute kidney injury (24.1%), hypotension (15.5%), bleeding (10.2%), and sepsis (6.7%). A total of 28 patients died (7.5%). Causes of death were hemorrhagic shock, multiple organ failure, respiratory failure, and sepsis. The independent risk factors associated with death were acute kidney injury (odds ratio [OR] = 6.77), hypotension (OR = 15.08), and respiratory failure (OR = 3.65).
The frequency of deaths was low. Acute kidney injury, hypotension, and respiratory insufficiency were independent risk factors for maternal death.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):397-404
DOI 10.5935/0103-507X.20160073
To identify factors associated with maternal death in patients admitted to an intensive care unit.
A cross-sectional study was conducted in a maternal intensive care unit. All medical records of patients admitted from January 2012 to December 2014 were reviewed. Pregnant and puerperal women were included; those with diagnoses of hydatidiform mole, ectopic pregnancy, or anembryonic pregnancy were excluded, as were patients admitted for non-obstetrical reasons. Death and hospital discharge were the outcomes subjected to comparative analysis.
A total of 373 patients aged 13 to 45 years were included. The causes for admission to the intensive care unit were hypertensive disorders of pregnancy, followed by heart disease, respiratory failure, and sepsis; complications included acute kidney injury (24.1%), hypotension (15.5%), bleeding (10.2%), and sepsis (6.7%). A total of 28 patients died (7.5%). Causes of death were hemorrhagic shock, multiple organ failure, respiratory failure, and sepsis. The independent risk factors associated with death were acute kidney injury (odds ratio [OR] = 6.77), hypotension (OR = 15.08), and respiratory failure (OR = 3.65).
The frequency of deaths was low. Acute kidney injury, hypotension, and respiratory insufficiency were independent risk factors for maternal death.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):413-419
DOI 10.5935/0103-507X.20160074
To evaluate the incidence of agitation in the first 7 days after intensive care unit admission, its risk factors and its associations with clinical outcomes.
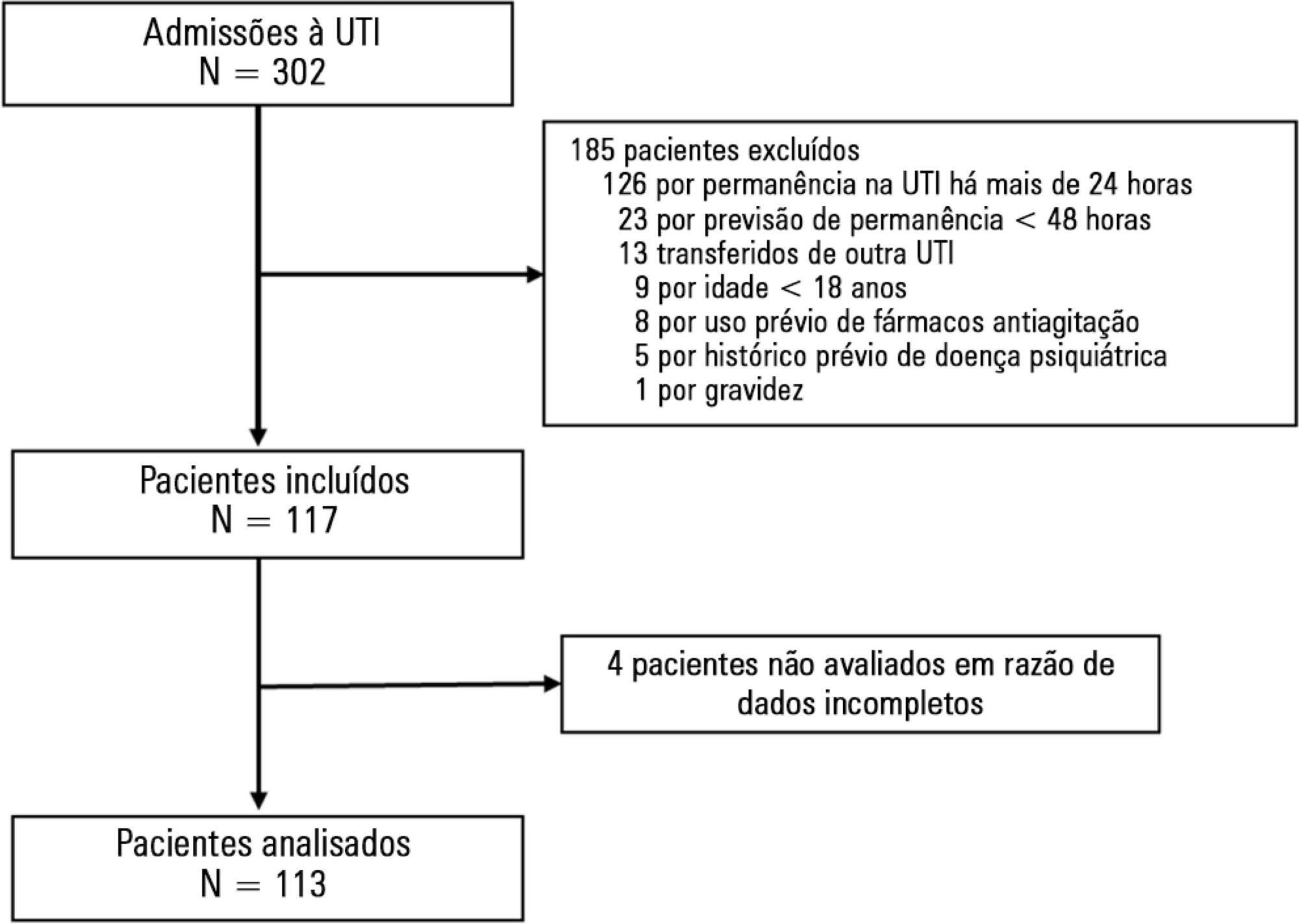
This single-center prospective cohort study included all patients older than 18 years with a predicted stay > 48 hours within the first 24 hours of intensive care unit admission. Agitation was defined as a Richmond Agitation Sedation Scale score ≥ +2, an episode of agitation or the use of a specific medication recorded in patient charts.
Agitation occurred in 31.8% of the 113 patients. Multivariate analysis showed that delirium [OR = 24.14; CI95% 5.15 - 113.14; p < 0.001], moderate or severe pain [OR = 5.74; CI95% 1.73 - 19.10; p = 0.004], mechanical ventilation [OR = 10.14; CI95% 2.93 - 35.10; p < 0.001], and smoking habits [OR = 4.49; CI95% 1.33 - 15.17; p = 0.015] were independent factors for agitation, while hyperlactatemia was associated with a lower risk [OR = 0.169; CI95% 0.04 - 0.77; p = 0.021]. Agitated patients had fewer mechanical ventilation-free days at day 7 (p = 0.003).
The incidence of agitation in the first 7 days after admission to the intensive care unit was high. Delirium, moderate/severe pain, mechanical ventilation, and smoking habits were independent risk factors. Agitated patients had fewer ventilator-free days in the first 7 days.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):413-419
DOI 10.5935/0103-507X.20160074
To evaluate the incidence of agitation in the first 7 days after intensive care unit admission, its risk factors and its associations with clinical outcomes.
This single-center prospective cohort study included all patients older than 18 years with a predicted stay > 48 hours within the first 24 hours of intensive care unit admission. Agitation was defined as a Richmond Agitation Sedation Scale score ≥ +2, an episode of agitation or the use of a specific medication recorded in patient charts.
Agitation occurred in 31.8% of the 113 patients. Multivariate analysis showed that delirium [OR = 24.14; CI95% 5.15 - 113.14; p < 0.001], moderate or severe pain [OR = 5.74; CI95% 1.73 - 19.10; p = 0.004], mechanical ventilation [OR = 10.14; CI95% 2.93 - 35.10; p < 0.001], and smoking habits [OR = 4.49; CI95% 1.33 - 15.17; p = 0.015] were independent factors for agitation, while hyperlactatemia was associated with a lower risk [OR = 0.169; CI95% 0.04 - 0.77; p = 0.021]. Agitated patients had fewer mechanical ventilation-free days at day 7 (p = 0.003).
The incidence of agitation in the first 7 days after admission to the intensive care unit was high. Delirium, moderate/severe pain, mechanical ventilation, and smoking habits were independent risk factors. Agitated patients had fewer ventilator-free days in the first 7 days.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):130-136
DOI 10.5935/0103-507X.20140019
To assess the performance of central venous oxygen saturation, lactate, base deficit, and C-reactive protein levels and SOFA and SWIFT scores on the day of discharge from the intensive care unit as predictors of patient readmission to the intensive care unit.
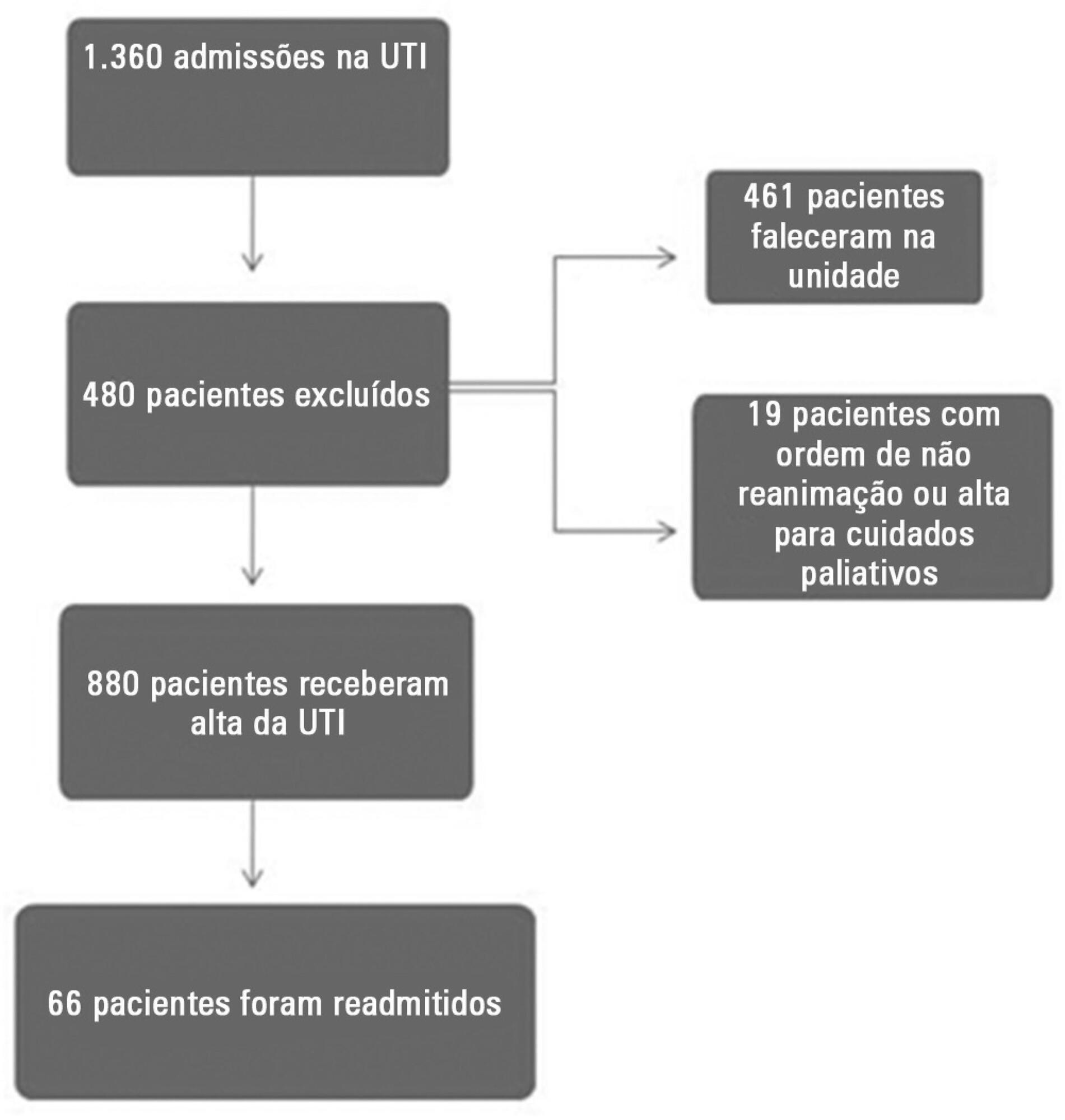
This prospective and observational study collected data from 1,360 patients who were admitted consecutively to a clinical-surgical intensive care unit from August 2011 to August 2012. The clinical characteristics and laboratory data of readmitted and non-readmitted patients after discharge from the intensive care unit were compared. Using a multivariate analysis, the risk factors independently associated with readmission were identified.
The C-reactive protein, central venous oxygen saturation, base deficit, and lactate levels and the SWIFT and SOFA scores did not correlate with the readmission of critically ill patients. Increased age and contact isolation because of multidrug-resistant organisms were identified as risk factors that were independently associated with readmission in this study group.
Inflammatory and perfusion parameters were not associated with patient readmission. Increased age and contact isolation because of multidrug-resistant organisms were identified as predictors of readmission to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):130-136
DOI 10.5935/0103-507X.20140019
To assess the performance of central venous oxygen saturation, lactate, base deficit, and C-reactive protein levels and SOFA and SWIFT scores on the day of discharge from the intensive care unit as predictors of patient readmission to the intensive care unit.
This prospective and observational study collected data from 1,360 patients who were admitted consecutively to a clinical-surgical intensive care unit from August 2011 to August 2012. The clinical characteristics and laboratory data of readmitted and non-readmitted patients after discharge from the intensive care unit were compared. Using a multivariate analysis, the risk factors independently associated with readmission were identified.
The C-reactive protein, central venous oxygen saturation, base deficit, and lactate levels and the SWIFT and SOFA scores did not correlate with the readmission of critically ill patients. Increased age and contact isolation because of multidrug-resistant organisms were identified as risk factors that were independently associated with readmission in this study group.
Inflammatory and perfusion parameters were not associated with patient readmission. Increased age and contact isolation because of multidrug-resistant organisms were identified as predictors of readmission to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):130-136
DOI 10.5935/0103-507X.20130024
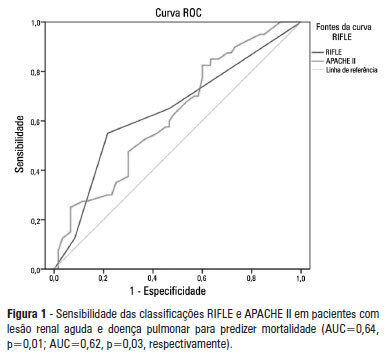
OBJECTIVE: To examine the factors associated with acute kidney injury and outcome in patients with lung disease. METHODS: A prospective study was conducted with 100 consecutive patients admitted to a respiratory intensive care unit in Fortaleza (CE), Brazil. The risk factors for acute kidney injury and mortality were investigated in a group of patients with lung diseases. RESULTS: The mean age of the study population was 57 years, and 50% were male. The incidence of acute kidney injury was higher in patients with PaO2/FiO2<200 mmHg (54% versus 23.7%; p=0.02). Death was observed in 40 cases and the rate of mortality of the acute kidney injury group was higher (62.8% versus 27.6%; p=0.01). The independent factor that was found to be associated with acute kidney injury was PaO2/FiO2<200 mmHg (p=0.01), and the independent risk factors for death were PEEP at admission (OR: 3.6; 95%CI: 1.3-9.6; p=0.009) and need for hemodialysis (OR: 7.9; 95%CI: 2.2-28.3; p=0.001). CONCLUSION: There was a higher mortality rate in the acute kidney injury group. Increased mortality was associated with mechanical ventilation, high PEEP, urea and need for dialysis. Further studies must be performed to better establish the relationship between kidney and lung injury and its impact on patient outcome.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):130-136
DOI 10.5935/0103-507X.20130024
OBJECTIVE: To examine the factors associated with acute kidney injury and outcome in patients with lung disease. METHODS: A prospective study was conducted with 100 consecutive patients admitted to a respiratory intensive care unit in Fortaleza (CE), Brazil. The risk factors for acute kidney injury and mortality were investigated in a group of patients with lung diseases. RESULTS: The mean age of the study population was 57 years, and 50% were male. The incidence of acute kidney injury was higher in patients with PaO2/FiO2<200 mmHg (54% versus 23.7%; p=0.02). Death was observed in 40 cases and the rate of mortality of the acute kidney injury group was higher (62.8% versus 27.6%; p=0.01). The independent factor that was found to be associated with acute kidney injury was PaO2/FiO2<200 mmHg (p=0.01), and the independent risk factors for death were PEEP at admission (OR: 3.6; 95%CI: 1.3-9.6; p=0.009) and need for hemodialysis (OR: 7.9; 95%CI: 2.2-28.3; p=0.001). CONCLUSION: There was a higher mortality rate in the acute kidney injury group. Increased mortality was associated with mechanical ventilation, high PEEP, urea and need for dialysis. Further studies must be performed to better establish the relationship between kidney and lung injury and its impact on patient outcome.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):245-250
DOI 10.5935/0103-507X.20130042
To analyze the incidence of early-onset nasal injury in infants with very low birth weight and indication for noninvasive ventilation via nasal prongs.
A prospective case series of infants with gestational age <37 weeks, weight <1.500 g and postnatal age <29 days. The patients were evaluated three times daily from the installation of nasal prongs to the 3rd day of use. The patients' clinical conditions and the device's characteristics and its application were analyzed. The initial analysis was descriptive, indicating the prevalence of nasal injury and factors associated with it. Categorical data were analyzed using the chi-squared test or Fisher's exact test, and numerical data were analyzed using the t-test or the Mann-Whitney test.
Eighteen infants were included; 12 (with a gestational age of 29.8±3.1 weeks, birth weight of 1.070±194 g and a Score for Neonatal Acute Physiology - Perinatal Extension (SNAPPE) of 15.4±17.5) developed nasal injuries (injury group), and 6 (with a gestational age of 28.0±1.9 weeks, weight of 1.003±317 g and SNAPPE of 26.2±7.5) showed no nasal injury (uninjured group). The injury group subjects were more often male (75% versus 17%), and their injuries appeared after an average of 18 hours, predominantly during the night (75%).
The incidence of nasal injury in preterm infants who experienced noninvasive ventilation via nasal prongs was high, and a study of associated factors may be planned based on this pilot.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):245-250
DOI 10.5935/0103-507X.20130042
To analyze the incidence of early-onset nasal injury in infants with very low birth weight and indication for noninvasive ventilation via nasal prongs.
A prospective case series of infants with gestational age <37 weeks, weight <1.500 g and postnatal age <29 days. The patients were evaluated three times daily from the installation of nasal prongs to the 3rd day of use. The patients' clinical conditions and the device's characteristics and its application were analyzed. The initial analysis was descriptive, indicating the prevalence of nasal injury and factors associated with it. Categorical data were analyzed using the chi-squared test or Fisher's exact test, and numerical data were analyzed using the t-test or the Mann-Whitney test.
Eighteen infants were included; 12 (with a gestational age of 29.8±3.1 weeks, birth weight of 1.070±194 g and a Score for Neonatal Acute Physiology - Perinatal Extension (SNAPPE) of 15.4±17.5) developed nasal injuries (injury group), and 6 (with a gestational age of 28.0±1.9 weeks, weight of 1.003±317 g and SNAPPE of 26.2±7.5) showed no nasal injury (uninjured group). The injury group subjects were more often male (75% versus 17%), and their injuries appeared after an average of 18 hours, predominantly during the night (75%).
The incidence of nasal injury in preterm infants who experienced noninvasive ventilation via nasal prongs was high, and a study of associated factors may be planned based on this pilot.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):321-326
DOI 10.1590/S0103-507X2011000300010
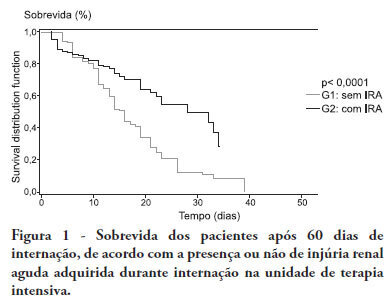
OBJECTIVE:To compare the clinical features and outcomes of patients with and without acute kidney injury in an intensive care unit of a tertiary university hospital and to identify acute kidney injury and mortality risk factors. METHODS: This was a prospective observational study of a cohort including 564 patients followed during their stay in the intensive care unit of Hospital das Clinicas da Faculdade de Medicina de Botucatu (Botucatu, São Paulo, Brazil) between May 2008 and May 2010. Patients were allocated to two different groups: with (G1) and without (G2) acute kidney injury. RESULTS: The incidence of acute kidney injury was 25.5%. The groups were different with respect to the reason for admission to the intensive care unit (sepsis, G1: 41.6% versus G2: 24.1%; P < 0.0001; neurosurgery, postoperative G1: 13.8% versus G2: 38.1%; P < 0.0001); age (G1: 56.8 ± 15.9 vs. G2: 49.8 ± 17.8 years; P < 0.0001); Acute Physiological Chronic Health Evaluation (APACHE) II score (G1: 21.9 ± 6.9 versus G2: 14.1 ± 4.6; P < 0.0001); use of mechanical ventilation (G1: 89.2% vs. G2: 69.1%; P < 0.0001) and use of vasoactive drugs (G1: 78.3% vs. G2: 56.1%; P < 0.0001). Higher rates of diabetes mellitus, congestive heart failure, chronic renal disease and use of non-steroidal anti-inflammatory drugs were more frequent in acute kidney injury patients (28.2% vs. 19.7%, P = 0.03; 23.6 vs. 11.6%, P = 0.0002; 21.5% vs. 11.5%, P < 0.0001 and 23.5% vs. 71.%, P < 0.0001, for G1 versus G2, respectively). Length of hospital stay and mortality were also higher for acute kidney injury patients (G1: 6.6 ± 2.7 days versus G2: 12.9 ±5.6 days, P < 0.0001 and G1: 62.5% versus G2: 16.4%, P < 0.0001). Multivariate analysis identified the following as risk factors for acute kidney injury: age above 55 years, APACHE II score above 16, baseline creatinine above 1.2 and use of non-steroidal anti-inflammatory drugs (odds ratio (OR) = 1.36, 95% confidence interval (95%CI): 1.22 - 1.85; OR = 1.2, 95%CI: 1.11 - 1.33; OR = 5.2, 95%CI: 2.3 - 11.6 and OR = 2.15, 95%CI: 1.1 - 4.2, respectively). Acute kidney injury was independently associated with longer hospital stay and increased mortality (OR = 1.18, 95%CI: 1.05 - 1.26 and OR = 1.24, 95%CI: 1.09 - 1.99, respectively). Analysis of the survival curve 30 days after admission showed 83.3% mortality for acute kidney injury patients and 45.2% for non-acute kidney injury patients (P < 0.0001). CONCLUSION: The incidence of acute kidney injury was high in this intensive care unit; the independent risk factors associated with acute kidney injury were age > 55 years, APACHE II > 16, baseline serum creatinine > 1.2 and use of non-steroidal anti-inflammatory drugs. Acute kidney injury is an independent risk factor for longer intensive care unit stay and mortality.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):321-326
DOI 10.1590/S0103-507X2011000300010
OBJECTIVE:To compare the clinical features and outcomes of patients with and without acute kidney injury in an intensive care unit of a tertiary university hospital and to identify acute kidney injury and mortality risk factors. METHODS: This was a prospective observational study of a cohort including 564 patients followed during their stay in the intensive care unit of Hospital das Clinicas da Faculdade de Medicina de Botucatu (Botucatu, São Paulo, Brazil) between May 2008 and May 2010. Patients were allocated to two different groups: with (G1) and without (G2) acute kidney injury. RESULTS: The incidence of acute kidney injury was 25.5%. The groups were different with respect to the reason for admission to the intensive care unit (sepsis, G1: 41.6% versus G2: 24.1%; P < 0.0001; neurosurgery, postoperative G1: 13.8% versus G2: 38.1%; P < 0.0001); age (G1: 56.8 ± 15.9 vs. G2: 49.8 ± 17.8 years; P < 0.0001); Acute Physiological Chronic Health Evaluation (APACHE) II score (G1: 21.9 ± 6.9 versus G2: 14.1 ± 4.6; P < 0.0001); use of mechanical ventilation (G1: 89.2% vs. G2: 69.1%; P < 0.0001) and use of vasoactive drugs (G1: 78.3% vs. G2: 56.1%; P < 0.0001). Higher rates of diabetes mellitus, congestive heart failure, chronic renal disease and use of non-steroidal anti-inflammatory drugs were more frequent in acute kidney injury patients (28.2% vs. 19.7%, P = 0.03; 23.6 vs. 11.6%, P = 0.0002; 21.5% vs. 11.5%, P < 0.0001 and 23.5% vs. 71.%, P < 0.0001, for G1 versus G2, respectively). Length of hospital stay and mortality were also higher for acute kidney injury patients (G1: 6.6 ± 2.7 days versus G2: 12.9 ±5.6 days, P < 0.0001 and G1: 62.5% versus G2: 16.4%, P < 0.0001). Multivariate analysis identified the following as risk factors for acute kidney injury: age above 55 years, APACHE II score above 16, baseline creatinine above 1.2 and use of non-steroidal anti-inflammatory drugs (odds ratio (OR) = 1.36, 95% confidence interval (95%CI): 1.22 - 1.85; OR = 1.2, 95%CI: 1.11 - 1.33; OR = 5.2, 95%CI: 2.3 - 11.6 and OR = 2.15, 95%CI: 1.1 - 4.2, respectively). Acute kidney injury was independently associated with longer hospital stay and increased mortality (OR = 1.18, 95%CI: 1.05 - 1.26 and OR = 1.24, 95%CI: 1.09 - 1.99, respectively). Analysis of the survival curve 30 days after admission showed 83.3% mortality for acute kidney injury patients and 45.2% for non-acute kidney injury patients (P < 0.0001). CONCLUSION: The incidence of acute kidney injury was high in this intensive care unit; the independent risk factors associated with acute kidney injury were age > 55 years, APACHE II > 16, baseline serum creatinine > 1.2 and use of non-steroidal anti-inflammatory drugs. Acute kidney injury is an independent risk factor for longer intensive care unit stay and mortality.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)